Burning Issues in the Esophagus
|
|
|
- Oswin Randall
- 5 years ago
- Views:
Transcription

![Squamous Epithelium Muscularis Mucosae Submucosa Mucosa [What a biopsy gets] Muscularis](/docs-images/81/83357797/images/1-1.jpg "Propria Layers of The Esophagus Lamina propria (note vessels) Submucosal gland Duct")
1 Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis Mucosae Submucosa Mucosa [What a biopsy gets] Muscularis Propria Layers of The Esophagus Lamina propria (note vessels) Submucosal gland Duct Muscularis mucosae 1
2 Barrett Esophagus - Epidemiology 5th and 6th decade M:F - 2:1-4:1 White: African-American - 10:1-20:1 Risk of cancer about 0.5%/year pooled data mostly US Study from Denmark Hvid-Jensen F, Pedersen L, Drewes AM, Sørensen HT, Funch-Jensen P. Incidence of Adenocarcinoma among Patients with Barrett's Esophagus. N Engl J Med Oct 13;365(15): Annual risk of progression to adenocarcinoma 0.12% Therefore surveillance pointless (at least in Denmark) Denmark Life expectancy (WHO) M 77y/ F 81y Obese population estimate: 7% United States Life expectancy M 76y/ F 81y Obese population estimate: 33% 2
3 Barrett s Esophagus ~ Overall incidence of progression in BE patients is 0.1 to 0.3 %/year in first five years but 9-9.5% at 20 years Kroep S, Lansdorp-Vogelaar I, Rubenstein JH, de Koning HJ, Meester R, Inadomi JM, van Ballegooijen M. An Accurate Cancer Incidence in Barrett's Esophagus: A Best Estimate Using Published Data and Modeling. Gastroenterology Sep;149(3): Prevalence of BE Swedish Study Columnar lined esophagus in about 10.3% BE found in [1.6%] [with goblet cells] Alcohol, smoking were risk factors [Gastroenterology 2005; 129: 1825] American College of Gastroenterology (ACG) Criteria for Barrett s Esophagus 2008 Barrett s mucosa is a change of the esophageal epithelium of any length that 1) can be recognized at endoscopy and 2) is confirmed to have intestinal metaplasia on biopsy 3
4 (ACG) Criteria for Barrett s Esophagus 2016 Barrett s esophagus should be diagnosed when there is extension of salmon-colored mucosa into the tubular esophagus extending > 1 cm proximal to the gastroesophageal junction with biopsy confirmation of intestinal metaplasia The authors further suggested that endoscopic biopsy should not be performed in the presence of a normal Z line or a Z line with <1 cm of variability Oh dear Length Requirement??? How the heck do we know how much they saw? The ACG suggested the term specialized IM of the esophagogastric junction for things <1cm Daily life Biopsy labeled esophagus Note: The above diagnosis of Barrett esophagus is made due to presence of goblet cells (intestinal metaplasia) with the assumption that the biopsies were obtained from columnar mucosa in the distal esophagus located at least 1 cm proximal to the top of the gastric folds as per 2016 American College of Gastroenterology (ACG) guidelines. Reference: Shaheen NJ, Falk GW, Iyer PG, Gerson LB; American College of Gastroenterology. ACG Clinical Guideline: Diagnosis and Management of Barrett's Esophagus. Am J Gastroenterol Jan;111(1):


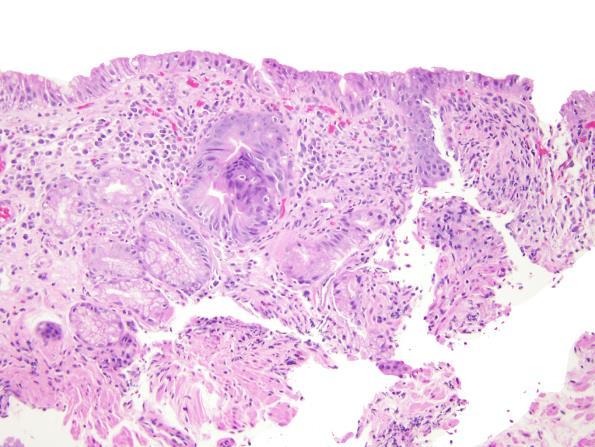
5 Daily life Biopsy labeled GEJ Note: This biopsy shows gastric-type mucosa with scattered goblet cells. The diagnosis in this case depends on the location of this biopsy. If this biopsy was taken from the tubular esophagus at least 1 cm above the gastric folds, it shows Barrett mucosa of the distinctive type. If this biopsy was taken from the gastric cardia, it shows intestinal metaplasia of the gastric cardia. Reference: Shaheen NJ, Falk GW, Iyer PG, Gerson LB; American College of Gastroenterology. ACG Clinical Guideline: Diagnosis and Management of Barrett's Esophagus. Am J Gastroenterol Jan;111(1):30-50 Tongue Island Classic Barrett mucosa with incomplete intestinal metaplasia 5


6 Normal small intestinal mucosa Normal small intestinal mucosa, PAS/AB stain?us Will Stop Requiring Goblet Cells? Example: Takubo et al Hum Pathol 2009;40:65-74 used German cases and found that intestinal metaplasia accompanied only 43% of early esophageal adenocarcinomas and believed that most cases arose in association with cardiac type mucosa. Stay tuned! ACG did not remove the requirement for goblet cells in 2008 OR 2016; AGA did not in position paper
7 2012 and 2016 Studies from USC ONLY FOUND DYSPLASIA OR CARCINOMA IN PATIENTS WITH INTESTINAL METAPLASIA AND EARLY CANCERS WERE ACCOMPANIED BY INTESTINAL METAPLASIA BUT these patients were all biopsied using systematic protocols ( perfect world ) by highly experienced colleagues Chandrasoma P, Wijetunge S, DeMeester S, Ma Y, Hagen J, Zamis L, DeMeester T. Columnar-lined esophagus without intestinal metaplasia has no proven risk of adenocarcinoma. Am J Surg Pathol Jan;36(1):1-7. Smith J, Garcia A, Zhang R, DeMeester S, Vallone J, Chandrasoma P. Intestinal Metaplasia is Present in Most if Not All Patients Who Have Undergone endoscopic Mucosal Resection for Esophageal Adenocarcinoma. Am J Surg Pathol Apr;40(4): PubMed PMID: Cases with staging data Johns Hopkins In our material at Johns Hopkins, we found that >90% of patients with treatment naïve esophageal adenocarcinomas had background intestinal metaplasia Salimian KJ, Waters KM, Eze O, Pezhouh MK, Tarabishy Y, Shin EJ, Canto MI, Voltaggio L, Montgomery EA. Definition of Barrett Esophagus in the United States: Support for Retention of a Requirement for Goblet Cells. Am J Surg Pathol Feb;42(2): PubMed PMID: However That s OUR population It may be reasonable in other populations 7
8 Dysplasia Neoplastic Epithelium Confined within the basement membrane of the gland within which it arose. Diagnostic Categories Negative for dysplasia Indefinite for dysplasia Dysplasia, low-grade Dysplasia, high-grade Intra-mucosal carcinoma Grading Dysplasia in Barrett s - Algorithm SURFACE MATURATION [COMPARED TO UNDERLYING GLANDS] ARCHITECTURE CYTOLOGIC FEATURES INFLAMMATION 8

9 BE - Negative for Dysplasia Surface - More mature than glands Architecture - Abundant lamina propria Cytology - Normal with mitoses confined to deeper glands. Nuclei with smooth nuclear membranes. Normal nuclear polarity Inflammation - Variable A fantastic clue A great clue to reactive epithelium in Barrett mucosa is looking for the four lines This feature is present in cardiac mucosa and remains in Barrett mucosa Let s have a look Gastric cardiac type mucosa 9


10 Gastric cardiac mucosa 10


11 Barrett mucosa no dysplasia Barrett mucosa no dysplasia 11



12 BE - Negative for Dysplasia Look at those lines! 12



13 LGD no lines, abrupt transition see at arrow at left LGD no lines 13
 Is this epithelium unequivocally neoplastic/adenomatous The answer NO to both questions = IFD But.")
14 Indefinite for dysplasia Originally defined in IBD and diagnosed by answering the questions a) Is this epithelium unequivocally benign or reactive? b) Is this epithelium unequivocally neoplastic/adenomatous The answer NO to both questions = IFD But.. Montgomery 2001 study on dysplasia in BE Deliberately defined any epithelium that looked dysplastic in the bases of the pits but had surface maturation as IFD i.e. impossible to have dysplasia with maturation Rationale maturation is a major feature of regenerating mucosa, so will exclude all reactive changes. 14


15 BE, Indefinite for Dysplasia Surface often more mature than glands Architecture - slight glandular crowding Cytology - hyperchromasia, nuclear membrane irregularities, increased mitoses in deep glands. Maintained nuclear polarity Inflammation - Frequently a factor Nice to see an abrupt transition to be sure something is dysplastic and thus clonal You might call indefinite for stratification. Neutrophils No abrupt transition But using the lines, it s reactive Kevin Waters 15


16 Changes in Proportion of NFD and IFD NFD IFD 16



17 17


18 Low Grade Dysplasia Clearly neoplastic Minimal loss of nuclear polarity Surface involved Only mild architectural crowding. 18


19 LGD, adenoma-like Where is the Minimum Abrupt transition appears divergent and clonal compared to adjacent epithelium But without inflammation in the specific abnormal focus Our lines obscured 19



20 Reactive - Unclear, gradual demarcation between zone of monolayered nuclei and stratification AND LINES Sharp demarcation of zone of abnormal nuclei 20
.")

21 Does Dysplasia Start Here?? Basal crypt dysplasia Lomo et al (R. Odze senior au). Crypt dysplasia with surface maturation: a clinical, pathologic, and molecular study of a Barrett's esophagus cohort. Am J Surg Pathol Apr;30(4):



22 Basal crypt dysplasia 22



23 Intramucosal carcinoma with basal crypt pattern Basal pattern dysplasia Basal pattern dysplasia, P53 23



24 High-Grade Dysplasia Surface - No maturation Architecture - Crowded glands overrunning lamina propria Cytology - Nuclear membrane irregularities, extending to surface and loss of nuclear polarity Inflammation - Typically not abundant 24



25 High- Grade Dysplasia HGD Inflammation 25



26 HGD - Inflammation Inflamed HGD Inflamed HGD Inflamed HGD, p53 26



27 Barrett, intramucosal carcinoma, P53 null pattern Barrett, intramucosal carcinoma, P53 null pattern Barrett mucosa, Reactive changes 27



28 Barrett reactive changes, wilt type pattern p53 Wild type pattern Dysplastic pattern TP53 HGD, small cell pattern non-adenomatous dysplasia 28



29 HGD, small Cell pattern nonadenomatous dysplasia HGD small cell pattern/ nonadenomatous dysplasia Lateral spread 29


30 Intramucosal Carcinoma Surface - No maturation Architecture - Effacement of lamina propria and syncytial growth pattern of glands. Back-to-back microglands, dirty necrosis in glands, DESMOPLASIA not yet developed Cytology - as in HG but often with nucleoli Inflammation - variable Lamina Propria Invasion, Esophageal Adenocarcinoma Early intramucosal invasion 30



31 Intramucosal carcinoma, lateral spread of atypical glands Intramucosal carcinoma, Budding and lateral growth Well developed desmoplasia Invasion into at least submucosa 31

32 Finding Pagetoid extension of single cells ALWAYS means there is a cancer underneath Additionally There are variant forms of dysplasia initial studies were all using criterial for intestinal type dysplasia but variant patterns are less well recognized and less well understood Intestinal type low-grade dysplasia 32



33 Look! Kulchitsky cells! HGD Foveolar Type LGD Foveolar type HGD 33


34 Pyloric type Our Experience at Johns Hopkins About 7% of our dysplasias had pyloric/cardiac type differentiation and about 10% had more foveolar type differentiation. N0 difference in rate of progression for the various types About 15% of our early cancers had no background intestinal metaplasia although we eventually found IM in many of these 34
35 Changing the game New endoscopic treatments and ability to visualize the mucosa (even with molecular markers) might slowly reduce the mortalility of esophagus cancer.assuming we can figure out how to get the right patients screened in a better way Known Risk Factors for Presence of BE Chronic GERD Advancing age (>50 y) Male gender Tobacco use Central obesity (waist >40 inches) Caucasian race Known Risk Factors for Developing Neoplasia in BE Advanced age Increasing length of BE Central obesity Tobacco use Lack of NSAID use Lack of PPI use Lack of statin use 35
 Endoscopic Resections For Barrett, endoscopic mucosal resections can be more practical than submucosal")
36 Estimates for Progression Risk No dysplasia %/year LGD 0.7%/yr HGD 7%/year Most patients with BE WITHOUT DYSPLASIA die of something else (>90%) Endoscopic Resections For Barrett, endoscopic mucosal resections can be more practical than submucosal dissections since they are fast and several can be performed to achieve coverage Subclassification of Depth of Invasion by Superficial Carcinoma Proposed by the Japan Esophageal Society 36

 12:1749-1756, 1997; Endo M et al.")
37 Relationships among Depths of Invasion and Vessel Invasion and Lymph Node Metastasis in Superficial SQUAMOUS Carcinoma Depth m1 0% m2 0% m3 8% sm1 17% sm2 28% sm3 49% % Lymph node metastases on resection Makuuchi H et al. Rinsho-Shokakinaika (Clin Gastroenterol) 12: , 1997; Endo M et al. Endoscopic treatment for early carcinoma of the esophagus. Shokaki-Shinyo Practice. Bunkodo, Tokyo,



38 Original muscularis mucosae Duplicated Muscularis mucosae Endoscopic Mucosal Resection [EMR] showing duplicated muscularis mucosae [Ref; Abraham et al. Am J Surg Pathol 2007; 31:1718.] 38



39 Endoscopic mucosal resection note damaged surface from plastic cap and suction 39


40 Original muscularis mucosae Endoscopic mucosal resection - layers 40


41 Duplicated muscularis mucosae 41



42 Early submucosal invasion measure the depth from the bottom of the muscularis mucosae to the deepest part of the cancer 42
 Tumor cells invading beyond basement membrane into")
 original muscularis mucosae m1 HGD HGD m2 m1 LP m2 m2 IMM m2 m3 BMM m3")
43 Reported Subclassification Schemes for Intramucosal Carcinoma (T1a) Designation, Weserterp et al Designation, Vieth et al Degsignation, Kaneshiro et al Description of Depth of Invasion None (Tis, high-grade dysplasia, HGD) Tumor cells invading beyond basement membrane into lamina propria Tumor cells invading (inner) duplicated muscularis mucosae Tumor cells in the space between the duplicated muscularis mucosae and original muscularis mucosae Tumor cells into (outer) original muscularis mucosae m1 HGD HGD m2 m1 LP m2 m2 IMM m2 m3 BMM m3 m4 OMM 43
44 Studies Early Esophagus Adenocarcinomas Liu. Am J Surg Pathol 2005; 29: 1079 Liu. Am J Surg Pathol 2005; 1079 Westertwerp. Virchow s Arch 2005;446:497 Westertwerp. Virchow s Arch 2005;446:497 Depth Lamina propria MM or superficial SM M1-M3, SM1 SM2, SM3 Outcome No mets 22% mets 1/79 LN mets, 83% 5 yr surv 44% LN mets; 42% 5 yr surv Kaneshiro Am J Surg Pathol 2011; 35:697 M1-M3 SM1 0.7% LN mets 8.6% LN mets Guidelines ACG 2016 Surveillance NFD every 3-5 years IFD repeat after optimization of acid suppression for 3-6 mos; if repeat IFD rebiopsy in 1 year LGD confirmation followed by consideration of ablation or surveillance every year HGD confirmation followed by endosopic therapy Follow-up After Ablation If for HGD or IMC every 3 months for a year then every 6 months for a year then annually If for LGD every 6 months for first year, then annually 44

45 Thank you! Mr. Barrett says thank you 45
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions
 Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
American Journal of Gastroenterology. Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma
 Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Ablation for Barrett s Esophagus: Burn or Freeze
 Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Earlyoesophagealcancer. dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia
 Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s Esophagus. Case Presentation
 Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Barrett esophagus. Bible class Inselspital
 Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Present Day Management of Barrett s Esophagus
 Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Barrett s Esophagus: Ablate Everyone?
 Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
SAM PROVIDER TOOLKIT
 THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
 Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful in characterizing esophageal location
 Diseases of the Esophagus (2005) 18, 87 92 2005 ISDE Blackwell Publishing, Ltd. Original article Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful
Diseases of the Esophagus (2005) 18, 87 92 2005 ISDE Blackwell Publishing, Ltd. Original article Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful
Barrett s esophagus. Barrett s neoplasia treatment trends
 Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Gastrointestinal pathology 2018 lecture 2. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD?
 Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Division of Anatomic Pathology & Molecular Oncology, University of Utah and ARUP Laboratories, Huntsman Cancer Institute, Salt Lake City, UT, USA
 REVIEW ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2014.14.3.131 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2014;14(3):131-162 Barrett s Esophagus Mary P. Bronner Division
REVIEW ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2014.14.3.131 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2014;14(3):131-162 Barrett s Esophagus Mary P. Bronner Division
Current Management: Role of Radiofrequency Ablation
 Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Part 1. A pragmatic approach to common problems in esophageal biopsy pathology
 Part 1 A pragmatic approach to common problems in esophageal biopsy pathology How I can help more patients than I hurt Barbara J McKenna University of Michigan barbmcke@med.umich.edu Case 1 The following
Part 1 A pragmatic approach to common problems in esophageal biopsy pathology How I can help more patients than I hurt Barbara J McKenna University of Michigan barbmcke@med.umich.edu Case 1 The following
Current Management of Low-Grade Dysplasia in Barrett Esophagus
 Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment Barrett s esophagus
 E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
From reflux to esophageal cancer. Josh Boys, MD TCV 2 nd year indentured servant
 From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL
 THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL PATHOLOGY SOCIETY Amitabh Srivastava 1, Henry Appelman
THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL PATHOLOGY SOCIETY Amitabh Srivastava 1, Henry Appelman
Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of the distal esophagus, gastroesophageal junction and gastric cardia?
 Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST QUESTIONS. Ver. #
 SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
One of the more common specimens encountered by
 Controversies in the Diagnosis of Barrett Esophagus and Barrett-Related Dysplasia One Pathologist s Perspective John R. Goldblum, MD N Context. Pathologists frequently assess esophageal biopsy specimens
Controversies in the Diagnosis of Barrett Esophagus and Barrett-Related Dysplasia One Pathologist s Perspective John R. Goldblum, MD N Context. Pathologists frequently assess esophageal biopsy specimens
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
Barrett s s Dysplasia
 Barrett s s Dysplasia Mary P. Bronner,, MD Director, GI Pathology Section Head, Molecular Pathology Cleveland Clinic Foundation Neoplastic Progression in Barrett s s Esophagus Chronic Reflux GERD Metaplasia
Barrett s s Dysplasia Mary P. Bronner,, MD Director, GI Pathology Section Head, Molecular Pathology Cleveland Clinic Foundation Neoplastic Progression in Barrett s s Esophagus Chronic Reflux GERD Metaplasia
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ
 - Project manual + FAQ") Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Gastrooesophageal reflux disease. Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia
 Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
In 1998, the American College of Gastroenterology issued ALIMENTARY TRACT
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Case in discussion. Common diagnostic problems in gallbladder pathology 62, F
 Common diagnostic problems in gallbladder pathology N. Volkan Adsay, M.D. 62, F Case in discussion Underwent cholecystectomy with the diagnosis of chronic cholecystititis and cholelithiasis Professor and
Common diagnostic problems in gallbladder pathology N. Volkan Adsay, M.D. 62, F Case in discussion Underwent cholecystectomy with the diagnosis of chronic cholecystititis and cholelithiasis Professor and
Everything Esophagus: Barrett s Esophagus. Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina
 Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
DIGESTIVE TRACT ESOPHAGUS
 DIGESTIVE TRACT From the lower esophagus to the lower rectum four fundamental layers comprise the wall of the digestive tube: mucosa, submucosa, muscularis propria (externa), and adventitia or serosa (see
DIGESTIVE TRACT From the lower esophagus to the lower rectum four fundamental layers comprise the wall of the digestive tube: mucosa, submucosa, muscularis propria (externa), and adventitia or serosa (see
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Changes to the diagnosis and management of Barrett s Oesophagus
 Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations
 Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert
Henry Moon was one of the giants in academic pathology during my early years.
 Henry Moon was one of the giants in academic pathology during my early years. Controversial stuff that occurs slightly above, within or slightly below the gastroesophageal junction, including Barrett s
Henry Moon was one of the giants in academic pathology during my early years. Controversial stuff that occurs slightly above, within or slightly below the gastroesophageal junction, including Barrett s
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
RFA and Cyrotherapy for Esophageal Disease
 RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
Diagnosis and grading of dysplasia in Barrett s oesophagus ... J Clin Pathol 2006;59: doi: /jcp
 1029 MY APPROACH Diagnosis and grading of dysplasia in Barrett s oesophagus R D Odze... This review focuses on the pathological features of dysplasia in Barrett s oesophagus. Two categorisation schemes
1029 MY APPROACH Diagnosis and grading of dysplasia in Barrett s oesophagus R D Odze... This review focuses on the pathological features of dysplasia in Barrett s oesophagus. Two categorisation schemes
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, by Am. Coll. of Gastroenterology ISSN /02/$22.00
 THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, 2002 2002 by Am. Coll. of Gastroenterology ISSN 0002-9270/02/$22.00 Published by Elsevier Science Inc. PII S0002-9270(01)03982-X ORIGINAL CONTRIBUTIONS
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, 2002 2002 by Am. Coll. of Gastroenterology ISSN 0002-9270/02/$22.00 Published by Elsevier Science Inc. PII S0002-9270(01)03982-X ORIGINAL CONTRIBUTIONS
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series
 E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS
 COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Medicare Advantage Medical Policy
 Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 30 PRACTICE GUIDELINES nature publishing group CME ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G.
30 PRACTICE GUIDELINES nature publishing group CME ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G.
Tumor location is a risk factor for lymph node metastasis in superficial Barrett s adenocarcinoma
 Tumor location is a risk factor for lymph node metastasis in superficial Barrett s adenocarcinoma Authors Masayoshi Yamada 1,IchiroOda 1,HirohitoTanaka 1, Seiichiro Abe 1, Satoru Nonaka 1, Haruhisa Suzuki
Tumor location is a risk factor for lymph node metastasis in superficial Barrett s adenocarcinoma Authors Masayoshi Yamada 1,IchiroOda 1,HirohitoTanaka 1, Seiichiro Abe 1, Satoru Nonaka 1, Haruhisa Suzuki
Adenocarcinoma of the distal esophagus is a recognized
 ORIGINAL ARTICLE Adenocarcinomas of the Distal Esophagus and Gastric Cardia Are Predominantly Esophageal Carcinomas Parakrama Chandrasoma, MD, Kumari Wickramasinghe, MD, PhD, Yanling Ma, MD, and Tom DeMeester,
ORIGINAL ARTICLE Adenocarcinomas of the Distal Esophagus and Gastric Cardia Are Predominantly Esophageal Carcinomas Parakrama Chandrasoma, MD, Kumari Wickramasinghe, MD, PhD, Yanling Ma, MD, and Tom DeMeester,
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
RADIOFREQUENCY ABLATION OR CRYOABLATION FOR ESOPHAGEAL DISORDERS
 DISORDERS Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs are dependent
DISORDERS Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs are dependent
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications
 and Clinicoradiologic Implications") Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications Poster No.: E-0060 Congress: ESTI 2012 Type: Scientific Exhibit Authors: K. Lee, T. J.
Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications Poster No.: E-0060 Congress: ESTI 2012 Type: Scientific Exhibit Authors: K. Lee, T. J.
Histopathology: Cervical HPV and neoplasia
 Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
Professor, Department of Endoscopic Diagnostic and Therapeutics, Chiba University School of Medicine
 Gastrointestinal Diseases Esophageal Disorders JMAJ 47(): 41 47, 24 Teruo KOUZU Professor, Department of Endoscopic Diagnostic and Therapeutics, Chiba University School of Medicine Abstract: Recent trends
Gastrointestinal Diseases Esophageal Disorders JMAJ 47(): 41 47, 24 Teruo KOUZU Professor, Department of Endoscopic Diagnostic and Therapeutics, Chiba University School of Medicine Abstract: Recent trends
Barrett esophagus is a premalignant condition resulting
 Diagnostic Challenges in the Pathologic Evaluation of Barrett Esophagus Rhonda K. Yantiss, MD N Context. Barrett esophagus represents an unstable epithelium resulting from chronic gastroesophageal reflux
Diagnostic Challenges in the Pathologic Evaluation of Barrett Esophagus Rhonda K. Yantiss, MD N Context. Barrett esophagus represents an unstable epithelium resulting from chronic gastroesophageal reflux
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Alimentary Canal (I)
") Alimentary Canal (I) Esophagus and Stomach (Objectives) By the end of this lecture, the student should be able to discuss the microscopic structure in correlation with the function of the following organs:
Alimentary Canal (I) Esophagus and Stomach (Objectives) By the end of this lecture, the student should be able to discuss the microscopic structure in correlation with the function of the following organs:
Barrett s Esophagus: Are We Making any Progress?
 3/22/217 arrett s Esophagus: re We Making any Progress? Stuart Jon Spechler, M.D. hief, Division of Gastroenterology, V North Texas Healthcare System; o-director, Esophageal Diseases enter, Professor of
3/22/217 arrett s Esophagus: re We Making any Progress? Stuart Jon Spechler, M.D. hief, Division of Gastroenterology, V North Texas Healthcare System; o-director, Esophageal Diseases enter, Professor of
GI Histology Lab 1. Prepared by: Zeina Kalaji
 GI Histology Lab 1 Prepared by: Zeina Kalaji Lip ORAL MUCOSA -Arrow shows labial salivary glands in the submucosa. VERMILLION transitional zone. SKIN Stratified Squamous epithelium, keratinized -Arrow
GI Histology Lab 1 Prepared by: Zeina Kalaji Lip ORAL MUCOSA -Arrow shows labial salivary glands in the submucosa. VERMILLION transitional zone. SKIN Stratified Squamous epithelium, keratinized -Arrow
Frozen Section Analysis of Esophageal Endoscopic Mucosal Resection Specimens in the Real-Time Management of Barrett s Esophagus
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:173 178 Frozen Section Analysis of Esophageal Endoscopic Mucosal Resection Specimens in the Real-Time Management of Barrett s Esophagus GANAPATHY A. PRASAD,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:173 178 Frozen Section Analysis of Esophageal Endoscopic Mucosal Resection Specimens in the Real-Time Management of Barrett s Esophagus GANAPATHY A. PRASAD,*
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Sixteen-year follow-up of Barrett s esophagus, endoscopically treated with argon plasma coagulation
 Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Patterns of recurrent and persistent intestinal metaplasia after successful radiofrequency ablation of Barrett s esophagus
 Patterns of recurrent and persistent intestinal metaplasia after successful radiofrequency ablation of Barrett s esophagus Robert J. Korst, MD, a,b Sobeida Santana-Joseph, MSN, a,b John R. Rutledge, MAS,
Patterns of recurrent and persistent intestinal metaplasia after successful radiofrequency ablation of Barrett s esophagus Robert J. Korst, MD, a,b Sobeida Santana-Joseph, MSN, a,b John R. Rutledge, MAS,
04/09/2018. Squamous Cell Neoplasia and Precursor Lesions. Agenda. Squamous Dysplasia. Squamo-proliferative lesions. Architectural features
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Upper GIT IV Gastric cancer
 Upper GIT IV Gastric cancer Luigi Tornillo PathoBasic 23.10.2014 Pathology Introduction Classification Morphogenesis Problems Intraepithelial neoplasia Surveillance EGJ Predictive factors Gastric cancer
Upper GIT IV Gastric cancer Luigi Tornillo PathoBasic 23.10.2014 Pathology Introduction Classification Morphogenesis Problems Intraepithelial neoplasia Surveillance EGJ Predictive factors Gastric cancer
Characteristics of intramural metastasis in gastric cancer. Tatsuya Hashimoto Kuniyoshi Arai Yuichi Yamashita Yoshiaki Iwasaki Tsunekazu
 ORIGINAL ARTICLE Characteristics of intramural metastasis in gastric cancer Tatsuya Hashimoto Kuniyoshi Arai Yuichi Yamashita Yoshiaki Iwasaki Tsunekazu Hishima Author for correspondence: T. Hashimoto
ORIGINAL ARTICLE Characteristics of intramural metastasis in gastric cancer Tatsuya Hashimoto Kuniyoshi Arai Yuichi Yamashita Yoshiaki Iwasaki Tsunekazu Hishima Author for correspondence: T. Hashimoto
7/20/2017. Esophageal Cancer: A Less Common But Deadly Cancer. Objectives. Disclosure Statement NYNPA Conference October Saratoga New York
 Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Histopathology: gastritis and peptic ulceration
 Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Disclosures. Gastroesophageal Reflux Disease. Gastroesophageal Reflux Disease
 Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
This medical position statement considers a series of
 GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
ATLAS OF HEAD AND NECK PATHOLOGY METAPLASIA
 Metaplasia is the conversion of one adult differentiated cell type to another. Generally it is the result of persistent cellular trauma and serves as a protective mechanism. Thus anteriorly along the nasal
Metaplasia is the conversion of one adult differentiated cell type to another. Generally it is the result of persistent cellular trauma and serves as a protective mechanism. Thus anteriorly along the nasal
Squamous Cell Neoplasia and Precursor Lesions
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Relative risk of dysplasia for patients with intestinal metaplasia in the distal oesophagus and in the gastric cardia
 Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
The Digestive System Laboratory
 The Digestive System Laboratory 1 The Digestive Tract The alimentary canal is a continuous tube stretching from the mouth to the anus. Liver Gallbladder Small intestine Anus Parotid, sublingual, and submaxillary
The Digestive System Laboratory 1 The Digestive Tract The alimentary canal is a continuous tube stretching from the mouth to the anus. Liver Gallbladder Small intestine Anus Parotid, sublingual, and submaxillary
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
The esophageal submucosal glands are considered to be a continuation
 248 Significance of Involvement by Squamous Cell Carcinoma of the Ducts of Esophageal Submucosal Glands Analysis of 201 Surgically Resected Superficial Squamous Cell Carcinomas Yusuke Tajima, M.D. 1,2
248 Significance of Involvement by Squamous Cell Carcinoma of the Ducts of Esophageal Submucosal Glands Analysis of 201 Surgically Resected Superficial Squamous Cell Carcinomas Yusuke Tajima, M.D. 1,2
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
ESMO Preceptorship Gastrointestinal Tumours Valencia October 2017
 www.esmo.org ESMO Preceptorship Valencia 06-07 October 2017 Gastrointestinal Tumours I have no conflicts of interest to declare Fátima Carneiro Gastrointestinal tumours Multidisciplinary management, standards
www.esmo.org ESMO Preceptorship Valencia 06-07 October 2017 Gastrointestinal Tumours I have no conflicts of interest to declare Fátima Carneiro Gastrointestinal tumours Multidisciplinary management, standards