Henry Moon was one of the giants in academic pathology during my early years.
|
|
|
- Roger Lee
- 5 years ago
- Views:
Transcription

1 Henry Moon was one of the giants in academic pathology during my early years.
2 Controversial stuff that occurs slightly above, within or slightly below the gastroesophageal junction, including Barrett s mucosa: What role do we pathologists play?
3 We fuss a lot over goblet cells & cancer in and around the GE junction, but do they deserve all the fuss?
4 Pretty small This is it! considering the size of everything around it!
5 Sometimes the lower esophagus and the GEJ are connected by the same changes, almost as if they are a single entity
6
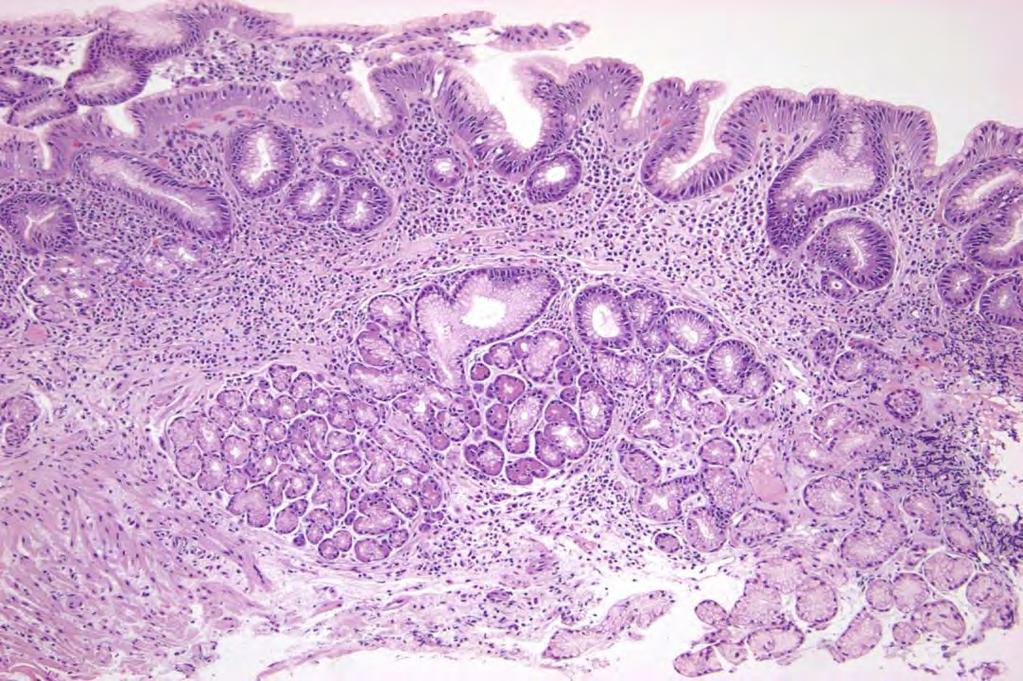
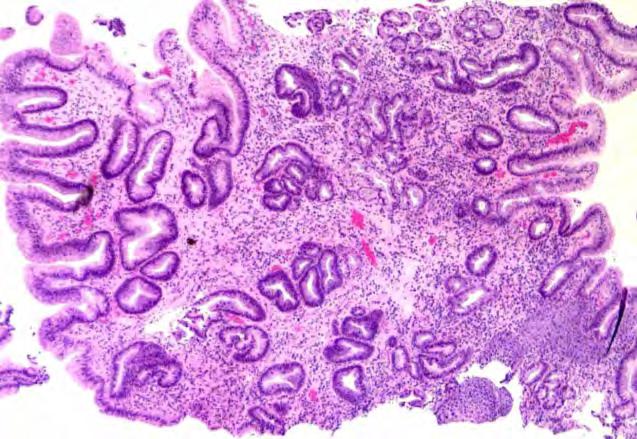
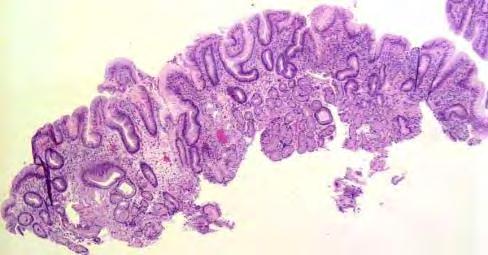
7 #1: Dyspeptic adult woman not responding to medication (PPIs) has upper endoscopy. The endoscopist saw erythema at the gastroesophageal junction. Nothing else. The erythema was biopsied
8 Biopsies of erythema are among But we the won t least informative discourage of all biopsies. the GI people from biopsying erythema We need the business!! Biopsies of erythema account for about 7% of my income

9 columnar columnar squamous squamous #1 #2 squamous columnar columnar columnar squamous
10 3 #1 1 2
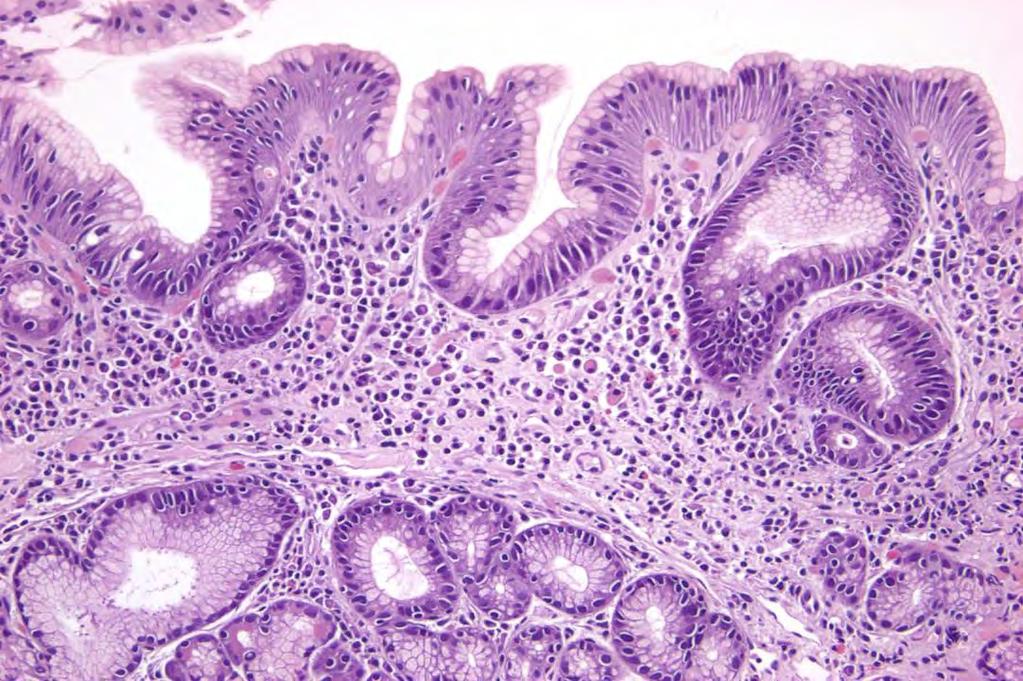
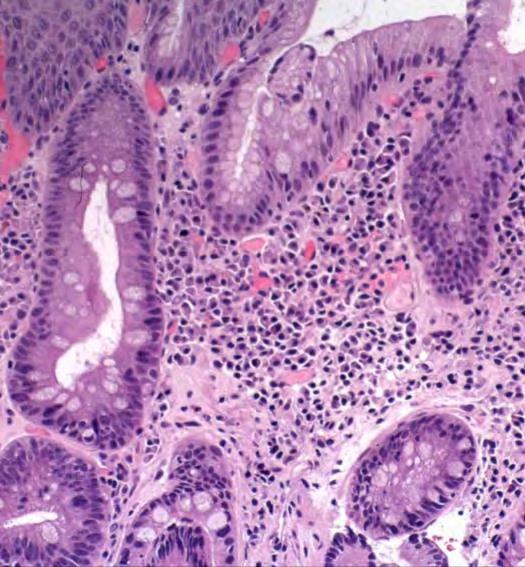
11 1 Chronic inflammation!

12 Plasma cells

 2")


13 Pancreatic acinar metaplasia (PAM) 2 Pancreatic acinar cells mixed with cardiac gland mucus cells




14 3 Huge pit cells: pseudogoblet cells


15 Don t confuse these with real goblet cells

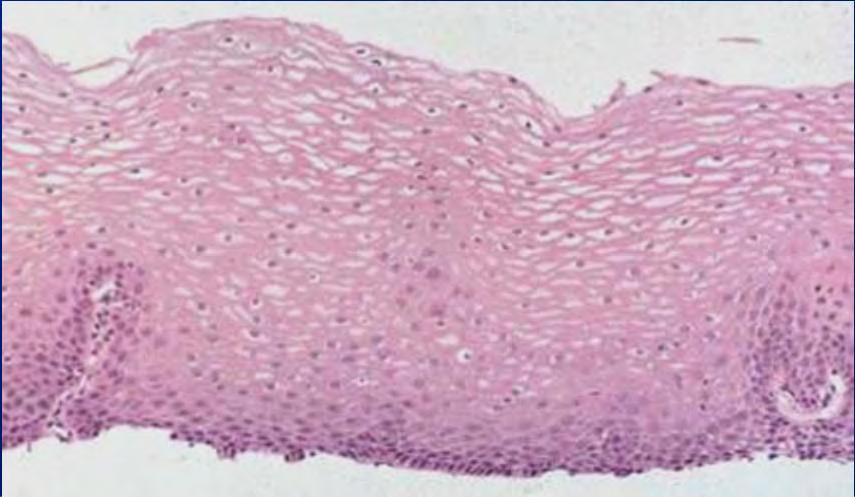
16 #2 Squamo-columnar junction No goblet cells!



17 Finally, way off at the edge of the biopsy The evil, dreaded goblet cells!!

18 Summary Endoscopic erythema at the GE Junction. No endoscopic Barrett s mucosa Squamous and columnar mucosae The columnar mucosa has Inflammation: plasma cells SO? Goblet cells.and mimics Pancreatic acinar cells in the cardiac glands
19 This is a common biopsy. It is annoying, because it does not have a standard name has a lot of features, but what do they all mean? I will deal with this. does not answer the clinical question: what caused dyspepsia?
20 #2: Obese adult white male (the Barrett model) Heartburn for 20 years, recently worse Not responding to PPIs endoscopy GEJ tongues: cannot tell if this is an exaggerated Z-line or short segment Barrett s Bx taken of the tongues Pathologist told (not asked) to R/O Barrett s (The true request was to R/I Barrett s)


21 Inflammation like the first bx Goblet cells Pseudogoblet cells
22 Summary Endoscopic: changes that may be either an exaggerated Z-line (squamocolumnar junction) or short segment Barrett s mucosa Histologic: Columnar mucosa Inflammation Goblet cells..and mimics

23 These 2 sets of biopsies around the gastroesophageal junction have Columnar mucosa Impressive chronic SO? inflammation Goblet cells

24
25 There are 2 compelling reasons


26 First: Because it includes Barrett s mucosa and the gastric cardia, both of which have cancer associations
27 Everything interesting and contentious about the cardia and Barrett s is driven by cancer risk because cancers in and around the GEJ are said to have been increasing at a great rate in western societies. Otherwise, we wouldn t care!
 we cannot tell where the cancer is arising!")
28 Adenocarcinomas at and around the Gastroesophageal Junction Distal Esophagus (Barrett s) Junctional NOS Sometimes (often?) we cannot tell where the cancer is arising! Fundus Cardia Upper Body
29 Second: The GE junction affects my standard of living much more than its size suggests it should!

30 Disclaimer: This is it! About 10% of my income is derived from specimens taken from the GEJ and nearby.
31 Our clients, the gastroenterologists actually have to deal with 2 junctions.
 visible line Spechler SJ.")
32 Junction #1 The Squamocolumnar Junction (Z-line) an endoscopic (gross) visible line Spechler SJ. Gastroenterol 117:218, 1999
33 Junction #2 The Gastroesophageal Junction: an endoscopic less obvious line.. Defined somewhat arbitrarily, as the level of the most proximal extent of the gastric folds Spechler SJ. Gastroenterol 117:218, 1999
34 Top of the proximal fold Thus, the GE Junction Also, the squamocolumnar junction (Z-line)
 Another definition of the GEJ is the point where the lumen")
35 Top of the proximal fold Thus, the GE Junction Also, the squamocolumnar junction (Z-line) Another definition of the GEJ is the point where the lumen flares
 (top of folds & point of")
36 Columnar epithelium lined lower esophagus SCJ GEJ (Z-line) (top of folds & point of flare)
37 Normal Cardiac Mucosa Pits and glands equal thickness Clustered mucus glands
38 The Cardia There are 2 cardias 1. The gross anatomic structure 2. The microscopic mucosa Of these, the important one is the microscopic mucosa
39 If we want to study the cardia, where should we find it?

40 The Gross Cardia Where in the hell is it?
41 The Gross Cardia Where in the hell is it? The AJCC gave it a site code: C16.0 which includes cardia and EG jct. Their definition of the cardia in 2010: The proximal 5 cm of stomach

42 Published Definitions of the Cardia: seem to mix gross and microscopic 1. No size. 2. About 1 cm long cm long 4. Several cm long to 4 cm long
43 Published Definitions of the Cardia 6. Within 5 cm of EGJ 7. 1 cm proximal to 2 cm distal to the EGJ 8. Narrow zone between esophagus and stomach 9. A small ill-defined area, extending 1-3 cm from the GEJ (Owens, Hist for Pathol, 2012)
44 Where is the cardia? Somewhere around here

45 Cardiac mucosa may be minute. The only way to study it is to biopsy the SCJ Cardiac mucosa Squamous mucosa Body mucosa
46 If you want to study the cardia, where do you take biopsies? Across the normal Hiatal hernia squamo-columnar junction 5 cm AJCC cardia
47 Is cardiac mucosa normal? Studies from U Southern California conclude that cardiac mucosa is abnormal and due to reflux, and that it is the precursor of Barrett s mucosa (Chandrasoma, et al, AJSP, 2000 to present) Other studies indicate cardiac mucosa occurs in infants and children, suggesting that it is normal (Zhou, et al, Mod Pathol, 1999, Kilgore,et al, AJG, 2000) Suggestions that it may be normal in some and abnormal in others
48 It doesn t matter if cardiac mucosa is normal or abnormal. It exists, so we have to deal with it!

49 Cardiac mucosa is usually inflamed

50 Carditis Chronic: Plasma cells Activity: PMNs

51 Cardiac intense inflammation Oxyntic very mild inflammation
52 Carditis Definition: microscopic inflammation in cardiac mucosa Almost every cardiac mucosa has some Causes: Currently an enigma H pylori? The intense active/chronic forms Acid Reflux? Data inconsistent Bile Reflux? one study from Leeds Unknown? Many?most mild cases Multifactorial? Possibly
53 Carditis: 2 types in Boston Definitions Type GERD active H pylori sx esophagitis gastritis Reflux yes yes no H pylori no no yes Looks like overlap to me! Results of analysis Type Overall PMNs Plasma multilayered M:F inflam cells epithelium Reflux less fewer fewer yes 7:3 H pylori more more more no 3:5+ Wieczorek, Wang, Antonioli, Glickman, Odze (BI-Deaconess & Brig-Woman's), Am J Surg Pathol, 27:960, 2003

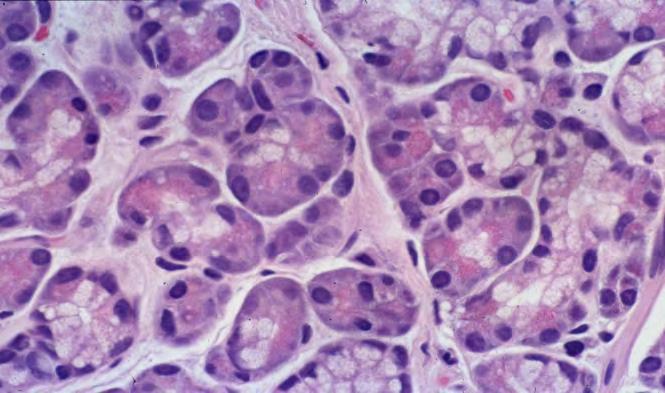
54 PAM Pancreatic Acinar Metaplasia
55 Pancreatic Acinar Metaplasia Is it a metaplasia, or is it congenital? 16% peds cardiac bx Is it a disease, or is it normal? Common in the cardia 24% of 155 adult junction bxs So far: no significance

56 Goblet cells
57 Goblet Cells in Cardiac Mucosa Numerous studies Sites of biopsies vary from lower 2-3 cm of esophagus This is utter nonsense! (as long as the SCJ is normal) to 2-3 cm below the GEJ Prevalence of goblet cells: 3% to 36% The M:F = 0.4:1 to 9:1
58 How common is cardiac IM 4 US centers, 940 adults 40 yrs and older who came for colonoscopy and agreed to have upper endoscopy. 122 (12.9%) cardiac goblet cells associated with advancing age and +H pylori test Rex, et al, Gastroenterol. 125:1670, 2003


59 Goblet Cells in Cardiac Mucosa 195 patients, elective upper endoscopy no endoscopic Barrett s magnification endoscopy with acetic acid spraying single targeted biopsy of specific mucosal types 86 (44%) had intestinal metaplasia (goblet cells) villiform pattern: 60% Cerebriform pattern: 96% conclusion: with this technique, cardiac goblet cells are very common Guelrud, et, Am J Gastroenterol 97:584-9, 2002
60 Goblet Cells in Cardiac Mucosa Causes acid reflux bile reflux H pylori at least 2 of the above something else
61 Goblet Cells in Cardiac Mucosa Significance: We worry that they are markers of high cancer risk. There is no data that they are.
62 Cardiac IM called histologic Barrett s mucosa in a German study 128 patients with 5 yr follow-up 33 (26%) developed endoscopic Barrett s Known length in 26 of the pts: <1cm short 11 pts: 1 to <3cm segment 3 pts: 3cm (long segment) No idea what this means for neoplastic risk Leodolter, et al: Scand J Gastoenterol 2012;47:1429
63 So whenever cardiac mucosa is biopsied, you get various combinations of
64 Inflammation Goblet cells PAM
65 Histologic features of cardia biopsies in volunteers 226 adults, mean age 45, 61% F, 49% Afr-Am 2 jumbo bx at or within 5mm of the SCJ (some may be too distal) Cardia, defined simply as presence of mucus glands, found in 191 (85%) Chronic carditis in 70% Active carditis in 30%, all definitely or probably H pylori Goblet cells in 15%; PAM in 13% El-Serag, et al, Scand J Gastroenterol, 42: , 2007
66 #1: Dyspeptic adult woman not responding to medication (PPIs) has upper endoscopy. The endoscopist saw erythema at the GE junction. Nothing else. The erythema was biopsied Look what we got:

67 Pancreatic acinar cells Inflammation Goblet cells
68 Possible Diagnoses chronic carditis ± PAM ± IM of unknown etiology or chronic carditis ± PAM ± IM due to ( if you really believe you know) or no significant abnormality (since everyone has some, who cares?)
69 What do I do every day? Before deciding, I polled my gastroenterologist colleagues to see what they wanted. I asked them if they wanted to know if there was carditis, PAM and/or IM, and if so, which item would change their management of the patient.
70 They said they did not care about any of these items except for IM, which might affect management in certain circumstances.
71 My diagnosis (they want this): Minute focus of IM at the GEJ What should be the diagnosis in other institutions or practices? This depends on what the GI colleagues want to know. The best way to find out is to ask them. Then tell them what they want.
72 Summary Cardias are small Cardias are often biopsied, so we see stuff Inflammation is almost universal The cause is unknown Goblet cells are common The cause is unknown Significance is minimal if that much Pancreatic acinar cells are common The cause is unknown
73 Other than for cancer and dysplasia, almost everything else that we say about a cardia in our reports is meaningless!
74 Now that I have killed cardiac mucosa, what about the other part of this discussion, Barrett s mucosa?
75 Am J Gastroenterol. 2008;103: This summarizes our approach to Barrett s mucosa, including the definition we use.
76 Barrett s Esophagus: Definition A change in the distal esophageal epithelium of any length that can be recognized as columnar type mucosa at endoscopy and is confirmed to have intestinal metaplasia by biopsy of the tubular esophagus Wang, Sampliner and the ACG Practice Parameters Committee, Am J Gastro, 103:788, 2008

77 Barrett s definition A change in the distal esophageal epithelium of any length.. it is an esophageal disease, not a GE junction disease!)

78 Barrett s definition..that can be recognized as columnar type mucosa at endoscopy (it is grossly, i e, endoscopically abnormal.) Tongues of pink mucosa
79 Barrett s Esophagus: Definition..and is confirmed to have intestinal metaplasia by biopsy of the tubular esophagus. (IM means goblet cells.)

80 Goblet cells in columnar mucosa Typical Barrett s Mucosa A few basal mucous glands
81 Goblet cells are irrefutable evidence of metaplasia. This definition also avoids dealing with cardiac mucosa in the distal esophagus.
82 The cancer rationale: Gastric mucosa with one type of intestinal metaplasia has an increased cancer risk Mucosa without IM has no increased cancer risk.
83 The cancer supposition: Esophageal mucosa with that same type of intestinal metaplasia has an increased cancer risk Mucosa without IM has no increased cancer risk.
84 2014 Diagnosis of mucosal biopsies at or slightly above the GEJ Histologic findings No goblet cells Goblet cells Diagnosis No Barrett s!!!!! Endoscopic Tongues above the GEJ Barrett s Z-line, no tongues Cardiac goblet cells Not certain if tongues Not certain if Barrett s No information Not certain if Barrett s
85 #2: Obese adult male Heartburn for 20 years, recently worse Not responding to PPIs endoscopy GEJ tongues: cannot tell if this is an exaggerated Z-line or short segment Barrett s Bx taken of the tongues Pathologist told (not asked) to R/O Barrett s (The true request was to R/I Barrett s)
86 Chronic inflammation Goblet cells
87 Diagnosis: Cardio-esophageal junction, biopsy: Columnar mucosa with goblet cells either in the cardia or in short segment Barrett s mucosa. Comment for the endoscopist: If you can t tell it is Barrett s, neither can I! (with a reference to Wang and Sampliner or to anyone else, if that seems necessary)
88 Barrett s mucosa has a bunch of metaplastic cells




89 Barrett s Goblet cells H & E Alcian blue




90 Columnar Blues H & E Alcian Blue


91 Columnar Blues Alcian Blue These columnar cells with acid mucin are metaplastic cells, but they are not considered to be equal to goblet cells for diagnosis.


92 Barrett s: other cell types Endocrine cells Paneth cells


93 Barrett s mucosa is also commonly inflamed. No one seems to care! Probably they just blame reflux.
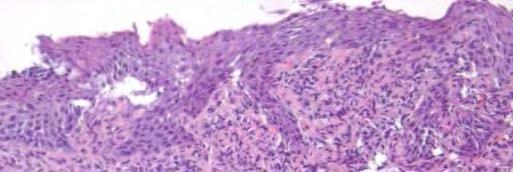
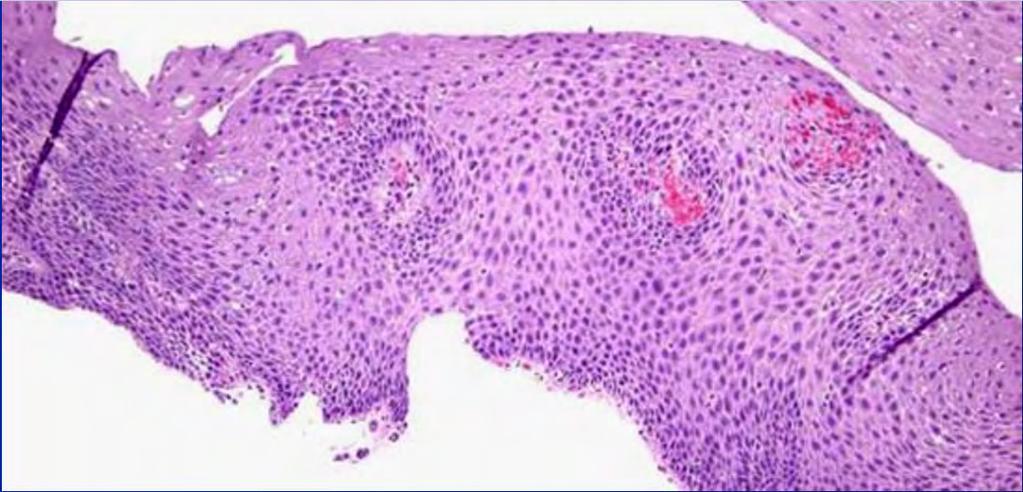
94 How does the mucosa turn from squamous to columnar? Squamous (normal) Columnar (Barrett s)
95 Barrett s mucosa: theoretical progression Injury We assume that this is refluxate Inflammation Mediators > cellular Metaplasia (Barrett s) Why metaplasia? Squamous epithelium heals perfectly well. Dysplasia Carcinoma We know a lot about the molecular and genetic changes here

96 How does the mucosa turn from squamous to columnar? gene gene gene factor factor Barrett s

97 Studies using cultures of esophageal squames or mucosa found that acid and/or bile salts up-regulate intestinal differentiation factors like CDX2 and CDX1, and/or up-regulate HB-EGF in lamina propria fibroblasts that promotes CDX2, and/or stimulate BMP4 in stromal cells that promotes columnar cell keratins

98 CK7+ columnar cell keratin in squamous cells above Barrett s
99 In the laboratory, reflux type substances induce changes in esophageal squamous cells that might precede intestinal metaplasia. We need to prove that these (or other) factors actually cause this metaplasia in vivo.
100 Why do we need columnar mucosa? Columnar metaplasia may be an adaptation by the host to better withstand the chemical (acid and bile) injury. El-Omar and Jankowski, Am J Gastroenterol. 107:1342, 2012


101 Barrett s esophagus: putative precursors Submucosal gland duct Cardiac mucosa Stem cells at squamous base


102 Barrett s Mucosa Multilayered epithelium the proposed origin in Boston
103 Barrett s mucosa has been separated into two types, based on segment length: Long segment (LSBE): 3 cm or more Short segment (SSBE): less than 3 cm A less well recognized segment length has been called ultrashort segment (USSBE). The definitions are not uniform. One definition uses less than 1 cm.
104 Unfortunately, goblet cells at the GEJ is also sometimes referred to as ultrashort segment Barrett s mucosa
105 Short segment Barrett s Definition: < 3 cm of columnar mucosa above the proximal gastric folds Over-diagnosed endoscopically: 3/4 in one study, but 3/8 in another May not be found on subsequent endoscopy
106 Looks like short segment Barrett s mucosa with typical red tongues The biopsy was not Barrett s The red is probably due to increase in superficial blood vessels

107 Endoscopic pseudobarretts 1. Papillomatosis in squamous 2. Healing ulcer in squamous 3. Cardiac mucosa 4. Normal squamous mucosa
108 Barrett s: squamous metaplasia (Pseudoregression) Squamous Broad stretch island May be stimulated by PPIs: lead to decreased endoscopic length and hidden stuff




109 What is hiding below the squamous metaplasia? The Barrett s only Dysplasia Carcinoma
110 Barrett s mucosa is a high-risk cancer precursor, right? So all this fuss is worthwhile, right?
111 We need to know 2 things 1. How common is Barretts? 2. What really is the cancer risk?
112 3 US studies: Prevalence of Barrett s in Males Stratified by Age Author # Age %Barr Ward Gerson Rex
113 How common is Barrett s in Sweden? 1000 randomly selected people in 2 Swedish places underwent upper endoscopy. Mean age 53.5 yrs, 51% women 16 (only 1.6%) had Barrett s, 5 long segment 400 had reflux sx: 2.3% had Barrett s 600 had no reflux sx: 1.2% had Barrett s 103 had endoscopic esophagitis: 2.6% had Barrett s 897 had no endoscopic esophagitis: 1.4% had Barrett s Alcohol and smoking were independent risk factors Ronkainen J, et al. Gastroenterol 129:1825, 2005
114 There seems to be a lot of Barrett s mucosa in the USA in older men. The Swedes have very little, but we don t live there!
115 What really is the cancer risk? Author Date Location #pts Cancer incidence Spechler 2011 USA N/A 0.5%/yr estimate Wani 2011 USA %/yr Bhat 2011 No Ire %/yr**** Hvid-Jen 2012 Denmark %/yr ***included both IM and non-im, CA esoph and cardia
116 Summary Barrett s mucosa is common Carcinomas developing after negative initial biopsies are rare Surveillance is expensive. Time to personalize surveillance.
117

118 Normal Cardiac Mucosa pits and glands equal thickness Clustered mucus glands
119 Cardiac Mucosa with a twist Esophageal submucosal gland duct Proof of tubular esophageal location
120 Cardiac Mucosa in the tubular esophagus Columnar lined lower esophagus
121 Gastric oxyntic mucosa Submucosal glands, also proof of esophageal location
122 What shall we do when gastric mucosa without goblet cells lines the lower esophagus?
123 2006 British Society of Gastroenterology guidelines for the diagnosis and management of Barrett s oesophagus (BO) BO is defined as an endoscopically apparent area above the OGJ that is suggestive of Barrett s which is supported by the finding of columnar lined oesophagus on histology...im is not a requirement for diagnosis. (because sampling may miss IM) Playford. Gut 55:442-3, 2006
124 .They suggest that IM not be required for the definition of BO..

125 Then these would be Barrett s in the UK If these came from mucosae that looked like endoscopic Barrett s
 to R/O Barrett s (The true request was to R/I Barrett s)")
126 #2: Obese adult male Heartburn for 20 years, recently worse Not responding to PPIs endoscopy GEJ tongues: cannot tell if this is an exaggerated Z-line or short segment Barrett s Bx taken of the tongues Pathologist told (not asked) to R/O Barrett s (The true request was to R/I Barrett s)

127 Chronic inflammation Goblet cells
128 Diagnosis: Cardio-esophageal junction, biopsy: Columnar mucosa with goblet cells Maybe add: either in the cardia or in short segment Barrett s mucosa. Comment: If you can t tell it is Barrett s, neither can I! (with a reference to Wang and Sampliner or Spechler or Fitzgerald, if that seems necessary) Even in the UK this is not Barrett s because of the endoscopic uncertainty
129 Some people in the US and in a few other places want us to adopt the British definition for Barrett s that doesn t require goblet cells.
130 They have some data to support this
131 3 studies: cardiac mucosa without IM in the distal esophagus had CDX2, an intestinal differentiation marker, in some, but not all cases. Phillips, et al, Am J Surg Pathol, 27:1442, 2003 Groisman, et al, Mod Pathol, 17:1282, 2004 Shi, et al, Am J Clin Pathol, 129:571, 2008
 had similar DNA content changes. Stomach No IM IM Liu, et al. Am J Gastroenterol 104:816, 2009")
132 A study of endoscopically confirmed columnar epithelium in the distal esophagus by image analysis: mucosa with IM and without (cardiac type) had similar DNA content changes. Stomach No IM IM Liu, et al. Am J Gastroenterol 104:816, 2009
133 One study from Germany: 70% of 141 small (>2 cm) distal esophageal cancers treated by EMR were surrounded by cardiac mucosa, not mucosa with goblet cells. No IM anywhere in over half of the EMR specimens Conclusion: no support for the view that Barrett adenocarcinoma is nearly always accompanied and preceded by IM. Takubo, et al. Hum Pathol. 40:65, 2009
134 In contrast, Another study from U of Southern California of esophageal, EGJ and cardiac carcinomas: residual IM was found next to 52% of 33 tumors >4cm 76% of 36 tumors <4cm 100% of 8 tumors 1cm 92% of 26 tumors confined to the wall Residual IM was related to tumor size. Chandrasoma, et al. Dis of the Esophagus. 20:36, 2007
135 Problems with these data: they are all retrospective We want to know if non-im mucosa needs surveillance. Specifically, does it have the same cancer risk as does IM mucosa


136 The latest word from the US folks AGA Institute Medical Position Panel Spechler, et al. Gastroenterol 140:1084, 2011
137 Definition of Barrett s Esophagus the condition in which any extent of metaplastic columnar epithelium that predisposes to cancer development replaces the stratified squamous epithelium..
138 Definition of Barrett s Esophagus Presently, intestinal metaplasia is required for the diagnosis.. because intestinal metaplasia is the only type of esophageal columnar epithelium that clearly predisposes to malignancy
139 Although cardia-type epithelium might be a risk factor for malignancy, the magnitude of that risk remains unclear. Based on this lack of data, it is justified not to perform endoscopic surveillance for patients solely with cardia-type epithelium
140 Then these would be Barrett s in the UK as of 2006 If these came from mucosae that looked like endoscopic Barrett s

141 The new BSG Barrett s guidelines Gut, 2014;63:7-42
142 British Society of Gastroenterology guidelines 2014 BO: any portion of the normal distal squamous epithelial lining that has been replaced by metaplastic columnar epithelium, which is clearly visible endoscopically ( 1 cm). and is confirmed microscopically from biopsies.. Old: Has both endo and histo requirements New: A minimum length is now defined. Fitzgerald, et al. Gut :7-42



143 then these would be still Barrett s in the UK as of 2014 If these came from mucosae that looked like endoscopic Barrett s, 1 cm
144 .The BSG suggests that IM not be required for the definition of BO, but it (the lack of IM) should be taken into account when deciding on the clinical management
145 ..even though the insistence of the identification of IM to define or confirm a diagnosis of Barrett s oesophagus is problematic, it is recognised that the inclusion of gastric-type mucosa in short tongues of columnar-lined oesophagus is of less clinical importance in terms of the likelihood of malignant transformation and has the potential to greatly influence the frequency of diagnosis of Barrett s oesophagus at index endoscopy and the number of patients entering into follow-up and surveillance programmes. Long discussion by the BSG summarized in the next slide
146 ..non-im columnar mucosa has little cancer risk, and inclusion of it in the BO diagnosis will greatly increase the number of people on surveillance who don t need it.
147 U of Chicago study 2012: Westerhoff, et al. Clin Gastroenterol Hepatol 2012;10: Decreasing the requirement for goblet cells would increase the diagnosis of BE by 147%. Among patients with short columnar segments, 12% had goblet cells on subsequent endoscopy, so most of the columnar mucosa might represent proximal stomach. No patient without goblet cells developed carcinoma. Decreasing the requirement for goblet cells would cause many patients to be inaccurately labeled as BE.
148 U of Chicago study 2012: Westerhoff, et al. Clin Gastroenterol Hepatol 2012;10: Sounds like a Decreasing the requirement for goblet cells would increase the diagnosis of BE by 147%. waste of time, resouces and Among patients with short columnar segments, 12% had goblet cells on subsequent endoscopy, so most of the columnar mucosa money might represent to proximal stomach. include these No patient without goblet cells developed carcinoma. Decreasing the requirement for goblet cells would cause many patients to be inaccurately labeled as BE. people!
149 What happens to people with non-im columnar lined lower esophagus (CLE) over time? There is limited longterm follow-up data
150 U of Chicago study: 12% of CLE patients without IM developed goblet cells on F-U exam within 5.8 years. Westerhoff, et al. Clin Gastroenterol Hepatol 2012;10: Houston VA study: 29% of CLE patients without IM developed goblet cells on F-U exam within 2 years Khandwalla, et al. Am J Gastroenterol 2014;109:
151 Does non-im CLE have a cancer risk? There is very little data. U of Chicago study, 2012: No patient without IM developed carcinoma, over a mean F-U of 5.8 years. This is a small series, and 5.8 years is not long enough.
152 Northern Ireland study, ,522 Barrett's pts, mean 7 years FU Incidence/yr of esoph/cardia AdCA With IM 0.38% Without IM 0.07%. Bhat, et al. JNCI, 2011;103:
153 I have not mentioned surveillance and diagnosing dysplasias. That requires a 2 hour lecture accompanied by teeth nashing and screaming!
154 Summary Cardiac mucosa has lots of stuff that seems to be clinically unimportant. Barrett s mucosa is so common and its cancers are so rare that most screening may be pointless. If these facts become widely accepted, the 10% of my income that comes from the GEJ will be cut substantially
155 Are we fussing too much about goblet cells and cancer in and around the GE Junction?
156 Goblet cells in the esophagus are required for the diagnosis of Barrett s mucosa. Barrett s mucosa is common. The diagnosis of Barrett s mucosa leads to unpleasant surveillance endocopy and biopsy Barrett s carcinomas are uncommon
157 Goblet cells in the cardia are common Their link to carcinoma is pretty puny Surveillance for cardiac IM is not recommended
158 Are we fussing too much about goblet cells and cancer in and around the GE Junction?
159 What role do pathologists play in all this? We still have to find the damned goblet cells regardless of whether they are important We still have to diagnose dysplasias for which there are no great criteria
160 Sorry. There is nothing I can do about this FINAL CLEVER SLIDE:


161 It takes To be a GI pathologist
Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful in characterizing esophageal location
 Diseases of the Esophagus (2005) 18, 87 92 2005 ISDE Blackwell Publishing, Ltd. Original article Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful
Diseases of the Esophagus (2005) 18, 87 92 2005 ISDE Blackwell Publishing, Ltd. Original article Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of the distal esophagus, gastroesophageal junction and gastric cardia?
 Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
In 1998, the American College of Gastroenterology issued ALIMENTARY TRACT
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions
 Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
 Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST QUESTIONS. Ver. #
 SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
Gastrooesophageal reflux disease. Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia
 Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Relative risk of dysplasia for patients with intestinal metaplasia in the distal oesophagus and in the gastric cardia
 Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
The increasing incidence of esophageal adenocarcinoma
 GASTROENTEROLOGY 2004;127:310 330 A Critical Review of the Diagnosis and Management of Barrett s Esophagus: The AGA Chicago Workshop PRATEEK SHARMA,* KENNETH MCQUAID, JOHN DENT, M. BRIAN FENNERTY, RICHARD
GASTROENTEROLOGY 2004;127:310 330 A Critical Review of the Diagnosis and Management of Barrett s Esophagus: The AGA Chicago Workshop PRATEEK SHARMA,* KENNETH MCQUAID, JOHN DENT, M. BRIAN FENNERTY, RICHARD
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Barrett esophagus. Bible class Inselspital
 Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Adenocarcinoma of the distal esophagus is a recognized
 ORIGINAL ARTICLE Adenocarcinomas of the Distal Esophagus and Gastric Cardia Are Predominantly Esophageal Carcinomas Parakrama Chandrasoma, MD, Kumari Wickramasinghe, MD, PhD, Yanling Ma, MD, and Tom DeMeester,
ORIGINAL ARTICLE Adenocarcinomas of the Distal Esophagus and Gastric Cardia Are Predominantly Esophageal Carcinomas Parakrama Chandrasoma, MD, Kumari Wickramasinghe, MD, PhD, Yanling Ma, MD, and Tom DeMeester,
Barrett s Esophagus and Intestinal Metaplasia of Gastric Cardia: Prevalence, Clinical, Endoscopic and Histological Features
 ORIGINAL PAPER Barrett s Esophagus and Intestinal Metaplasia of Gastric Cardia: Prevalence, Clinical, Endoscopic and Histological Features Ofelia Daniela Pascarenco¹, Alina Boeriu¹, Simona Mocan², Ghenadie
ORIGINAL PAPER Barrett s Esophagus and Intestinal Metaplasia of Gastric Cardia: Prevalence, Clinical, Endoscopic and Histological Features Ofelia Daniela Pascarenco¹, Alina Boeriu¹, Simona Mocan², Ghenadie
From reflux to esophageal cancer. Josh Boys, MD TCV 2 nd year indentured servant
 From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
SAM PROVIDER TOOLKIT
 THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
Gastroesophageal Junction Pathology: Diagnostic and Controversial Issues
 Gastroesophageal Junction Pathology: Diagnostic and Controversial Issues Robert D. Odze, MD, FRCPC BULLET POINTS The gastric cardia is the area of mucosa located distal to the GEJ (proximal aspect of gastric
Gastroesophageal Junction Pathology: Diagnostic and Controversial Issues Robert D. Odze, MD, FRCPC BULLET POINTS The gastric cardia is the area of mucosa located distal to the GEJ (proximal aspect of gastric
Esophageal submucosal mass icd 10
 Esophageal submucosal mass icd 10 Search 6-6-2011 ICD-10; Risk Adjustment / HCC; Evaluation & Management (E/M). I'm hoping someone can help me with this DX, "soft tissue mass in. Upper gastrointestinal
Esophageal submucosal mass icd 10 Search 6-6-2011 ICD-10; Risk Adjustment / HCC; Evaluation & Management (E/M). I'm hoping someone can help me with this DX, "soft tissue mass in. Upper gastrointestinal
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD?
 Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL
 THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL PATHOLOGY SOCIETY Amitabh Srivastava 1, Henry Appelman
THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL PATHOLOGY SOCIETY Amitabh Srivastava 1, Henry Appelman
Histological Features of Gastric Cardia in Adults: an Autopsy
 original PAPERs Histological Features of Gastric Cardia in Adults: an Autopsy Study Zorica M. Stojsic 1, Radmila M. Stevanovic 1, Martina M. Stojanovic 1, Aleksandar D. Stanojevic 2, Dragoljub T. Bacetic
original PAPERs Histological Features of Gastric Cardia in Adults: an Autopsy Study Zorica M. Stojsic 1, Radmila M. Stevanovic 1, Martina M. Stojanovic 1, Aleksandar D. Stanojevic 2, Dragoljub T. Bacetic
Division of Anatomic Pathology & Molecular Oncology, University of Utah and ARUP Laboratories, Huntsman Cancer Institute, Salt Lake City, UT, USA
 REVIEW ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2014.14.3.131 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2014;14(3):131-162 Barrett s Esophagus Mary P. Bronner Division
REVIEW ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2014.14.3.131 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2014;14(3):131-162 Barrett s Esophagus Mary P. Bronner Division
Vital staining and Barrett s esophagus
 Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
The esophagogastric junction (EGJ), the region between
, the region between") Review Article Definition of the Esophagogastric Junction A Critical Mini Review Qin Huang, MD, PhD N Context. Accurate diagnosis of diseases involving the esophagogastric junction (EGJ) is challenging
Review Article Definition of the Esophagogastric Junction A Critical Mini Review Qin Huang, MD, PhD N Context. Accurate diagnosis of diseases involving the esophagogastric junction (EGJ) is challenging
The presence of intestinal-type goblet cells (ITGCs) in
 in") Goblet Cell Mimickers in Esophageal Biopsies Are Not Associated With an Increased Risk for Dysplasia Mamoun Younes, MD; Atilla Ertan, MD; Gulchin Ergun, MD; Ray Verm, MD; Margaret Bridges, MD; Karen Woods,
Goblet Cell Mimickers in Esophageal Biopsies Are Not Associated With an Increased Risk for Dysplasia Mamoun Younes, MD; Atilla Ertan, MD; Gulchin Ergun, MD; Ray Verm, MD; Margaret Bridges, MD; Karen Woods,
Burning Issues in the Esophagus
 Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Barrett esophagus is a premalignant condition resulting
 Diagnostic Challenges in the Pathologic Evaluation of Barrett Esophagus Rhonda K. Yantiss, MD N Context. Barrett esophagus represents an unstable epithelium resulting from chronic gastroesophageal reflux
Diagnostic Challenges in the Pathologic Evaluation of Barrett Esophagus Rhonda K. Yantiss, MD N Context. Barrett esophagus represents an unstable epithelium resulting from chronic gastroesophageal reflux
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you)
") What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
Gastrointestinal pathology 2018 lecture 2. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Barrett s esophagus. Barrett s neoplasia treatment trends
 Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
Barrett's Esophagus: Sorting Out the Controversy
 Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
58 year old male complaining of 3-week history of increasing epigastric pain
 Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
American Journal of Gastroenterology. Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma
 Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Frequency of Barrett Esophagus in Patients with Symptoms of Gastroesophageal Reflux Disease
 Original Article Frequency of Barrett Esophagus in Patients with Symptoms of Gastroesophageal Reflux Disease From Military Hospital, Rawalpindi Obaid Ullah Khan, Abdul Rasheed Correspondence: Dr. Abdul
Original Article Frequency of Barrett Esophagus in Patients with Symptoms of Gastroesophageal Reflux Disease From Military Hospital, Rawalpindi Obaid Ullah Khan, Abdul Rasheed Correspondence: Dr. Abdul
Management of Barrett s Esophagus. Case Presentation
 Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Changes to the diagnosis and management of Barrett s Oesophagus
 Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
32 Adenocarcinoma of the oesophagogastric junction
 Adenocarcinoma of the oesophagogastric junction S.J. Spechler P. Hainaut M.F. Dixon R. Lambert R. Genta R. Siewert Definition Adenocarcinomas that straddle the junction of the oesophagus and stomach are
Adenocarcinoma of the oesophagogastric junction S.J. Spechler P. Hainaut M.F. Dixon R. Lambert R. Genta R. Siewert Definition Adenocarcinomas that straddle the junction of the oesophagus and stomach are
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
This medical position statement considers a series of
 GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Ablation for Barrett s Esophagus: Burn or Freeze
 Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Hiatal Hernias and Barrett s esophagus. Dr Sajida Ahad Mercy General Surgery
 Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Chapter 2 Complications of Gastroesophageal Reflux Disease
 Chapter 2 Complications of Gastroesophageal Reflux Disease Patrick Yachimski Acute esophageal exposure to gastric and/or duodenal refluxate can result in pyrosis and symptomatic gastroesophageal reflux
Chapter 2 Complications of Gastroesophageal Reflux Disease Patrick Yachimski Acute esophageal exposure to gastric and/or duodenal refluxate can result in pyrosis and symptomatic gastroesophageal reflux
Current Management: Role of Radiofrequency Ablation
 Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Disclosures. Heartburn and Barrett s Esophagus. Heartburn and Barrett s Esophagus. GERD is common in the U.S. None
 Heartburn and Barrett s Esophagus None Disclosures Christian Mathy, MD University of California, San Francisco 2015 Heartburn and Barrett s Esophagus Heartburn and GERD GERD therapy Extraesophageal GERD
Heartburn and Barrett s Esophagus None Disclosures Christian Mathy, MD University of California, San Francisco 2015 Heartburn and Barrett s Esophagus Heartburn and GERD GERD therapy Extraesophageal GERD
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations
 Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert
Present Day Management of Barrett s Esophagus
 Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
594 Lewin, Weinstein, and Riddell s Gastrointestinal Pathology and Its Clinical Implications
 594 Lewin, Weinstein, and Riddell s Gastrointestinal Pathology and Its Clinical Implications Figure 13-20. Stages in the natural history of H. pylori. Biopsies from the antrum are on the left and the oxyntic
594 Lewin, Weinstein, and Riddell s Gastrointestinal Pathology and Its Clinical Implications Figure 13-20. Stages in the natural history of H. pylori. Biopsies from the antrum are on the left and the oxyntic
Barrett s Esophagus: State of the Art Management
 In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH
In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH
Earlyoesophagealcancer. dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia
 Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Screening of Barrett: Is it cost-effective? Is there a high-risk population? T Ponchon Ed. Herriot Hospital Lyon, France
 Screening of Barrett: Is it cost-effective? Is there a high-risk population? T Ponchon Ed. Herriot Hospital Lyon, France Barrett s esophagus (BE) is an acquired condition in which the normal squamous epithelium
Screening of Barrett: Is it cost-effective? Is there a high-risk population? T Ponchon Ed. Herriot Hospital Lyon, France Barrett s esophagus (BE) is an acquired condition in which the normal squamous epithelium
Barrett s Oesophagus Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
Inflammation and Specialized Intestinal Metaplasia of Cardiac Mucosa Is a Manifestation of
 ANNALS OF SURGERY Vol. 226, No. 4, 522-532 1997 Lippincott-Raven Publishers Inflammation and Specialized Intestinal Metaplasia of Cardiac Mucosa Is a Manifestation of Gastroesophageal Ref ux Disease Stefan
ANNALS OF SURGERY Vol. 226, No. 4, 522-532 1997 Lippincott-Raven Publishers Inflammation and Specialized Intestinal Metaplasia of Cardiac Mucosa Is a Manifestation of Gastroesophageal Ref ux Disease Stefan
ATLAS OF HEAD AND NECK PATHOLOGY METAPLASIA
 Metaplasia is the conversion of one adult differentiated cell type to another. Generally it is the result of persistent cellular trauma and serves as a protective mechanism. Thus anteriorly along the nasal
Metaplasia is the conversion of one adult differentiated cell type to another. Generally it is the result of persistent cellular trauma and serves as a protective mechanism. Thus anteriorly along the nasal
Histopathology: gastritis and peptic ulceration
 Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Sixteen-year follow-up of Barrett s esophagus, endoscopically treated with argon plasma coagulation
 Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Current issues in Barrett s oesophagus and the oesophago-gastric junction
 Current issues in Barrett s oesophagus and the oesophago-gastric junction Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May 11 2016 The changing role of
Current issues in Barrett s oesophagus and the oesophago-gastric junction Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May 11 2016 The changing role of
Identifying Intestinal Metaplasia at the Squamocolumnar Junction by Using Optical Coherence Tomography
 Identifying Intestinal Metaplasia at the Squamocolumnar Junction by Using Optical Coherence Tomography The Harvard community has made this article openly available. Please share how this access benefits
Identifying Intestinal Metaplasia at the Squamocolumnar Junction by Using Optical Coherence Tomography The Harvard community has made this article openly available. Please share how this access benefits
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Barrett s Esophagus: Are We Making any Progress?
 3/22/217 arrett s Esophagus: re We Making any Progress? Stuart Jon Spechler, M.D. hief, Division of Gastroenterology, V North Texas Healthcare System; o-director, Esophageal Diseases enter, Professor of
3/22/217 arrett s Esophagus: re We Making any Progress? Stuart Jon Spechler, M.D. hief, Division of Gastroenterology, V North Texas Healthcare System; o-director, Esophageal Diseases enter, Professor of
Table 2.9. Case control studies of helicobacter pylori infection and oesophageal adenocarcinoma
 Characteristics of Characteristics of controls Detection Chow et al (1998) 1993-1995 129 of newly diagnosed oesophageal/gastric cardia (OGC) adenocarcinoma. 224 population controls selected by random digit
Characteristics of Characteristics of controls Detection Chow et al (1998) 1993-1995 129 of newly diagnosed oesophageal/gastric cardia (OGC) adenocarcinoma. 224 population controls selected by random digit
Oesophageal Disorders
 Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Extraesophageal GERD: Fact or Fiction?
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/gi-insights/extraesophageal-gerd-fact-or-fiction/4157/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/gi-insights/extraesophageal-gerd-fact-or-fiction/4157/
Patterns of recurrent and persistent intestinal metaplasia after successful radiofrequency ablation of Barrett s esophagus
 Patterns of recurrent and persistent intestinal metaplasia after successful radiofrequency ablation of Barrett s esophagus Robert J. Korst, MD, a,b Sobeida Santana-Joseph, MSN, a,b John R. Rutledge, MAS,
Patterns of recurrent and persistent intestinal metaplasia after successful radiofrequency ablation of Barrett s esophagus Robert J. Korst, MD, a,b Sobeida Santana-Joseph, MSN, a,b John R. Rutledge, MAS,
Alimentary Canal (I)
") Alimentary Canal (I) Esophagus and Stomach (Objectives) By the end of this lecture, the student should be able to discuss the microscopic structure in correlation with the function of the following organs:
Alimentary Canal (I) Esophagus and Stomach (Objectives) By the end of this lecture, the student should be able to discuss the microscopic structure in correlation with the function of the following organs:
Current Management of Low-Grade Dysplasia in Barrett Esophagus
 Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Intestinal metaplasia at the gastro-oesophageal junction: Helicobacter pylori gastritis or gastro-oesophageal reflux disease?
 Gut 1998;43:17 21 17 Gastroenterology, Hepatology, and Infectious Diseases A Hackelsberger V Schultze G Manes J-E Dominguez-Muñoz P Malfertheiner Pathology, Otto-von-Guericke University, Magdeburg, Germany
Gut 1998;43:17 21 17 Gastroenterology, Hepatology, and Infectious Diseases A Hackelsberger V Schultze G Manes J-E Dominguez-Muñoz P Malfertheiner Pathology, Otto-von-Guericke University, Magdeburg, Germany
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process
 MEASURE TYPE: Process") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Transfer of Health Information and Interoperability 2019 COLLECTION TYPE:
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Transfer of Health Information and Interoperability 2019 COLLECTION TYPE:
Intestinal Metaplasia of the Esophagus or Esophagogastric Junction Evidence of Distinct Clinical, Pathologic, and Histochemical Staining Features
 Anatomic Pathology / ESOPHAGEAL AND JUNCTIONAL INTESTINAL METAPLASIA Intestinal Metaplasia of the Esophagus or Esophagogastric Junction Evidence of Distinct Clinical, Pathologic, and Histochemical Staining
Anatomic Pathology / ESOPHAGEAL AND JUNCTIONAL INTESTINAL METAPLASIA Intestinal Metaplasia of the Esophagus or Esophagogastric Junction Evidence of Distinct Clinical, Pathologic, and Histochemical Staining
Digestive system L 2. Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section
 Digestive system L 2 Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section objectives 1-Describe the general structure of digestive tract: a-mucosa. b-submucosa. c-muscularis externa d-adventitia
Digestive system L 2 Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section objectives 1-Describe the general structure of digestive tract: a-mucosa. b-submucosa. c-muscularis externa d-adventitia
Accepted Manuscript. CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D
 Accepted Manuscript CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D PII: S1542-3565(18)31093-0 DOI: 10.1016/j.cgh.2018.10.010 Reference: YJCGH 56132
Accepted Manuscript CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D PII: S1542-3565(18)31093-0 DOI: 10.1016/j.cgh.2018.10.010 Reference: YJCGH 56132
THE CONNECTIVE TISSUE AND EPITHELIUM
 THE CONNECTIVE TISSUE AND EPITHELIUM The focus of this week s lab will be pathology of connective tissue and epithelium. The lab will introduce you to the four basic tissue types: epithelium, connective
THE CONNECTIVE TISSUE AND EPITHELIUM The focus of this week s lab will be pathology of connective tissue and epithelium. The lab will introduce you to the four basic tissue types: epithelium, connective
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
One of the more common specimens encountered by
 Controversies in the Diagnosis of Barrett Esophagus and Barrett-Related Dysplasia One Pathologist s Perspective John R. Goldblum, MD N Context. Pathologists frequently assess esophageal biopsy specimens
Controversies in the Diagnosis of Barrett Esophagus and Barrett-Related Dysplasia One Pathologist s Perspective John R. Goldblum, MD N Context. Pathologists frequently assess esophageal biopsy specimens
What Is Barrett s Esophagus?
 What Is Barrett s Esophagus? Having Barrett s esophagus means the cells lining the esophagus (the tube that links the mouth and the stomach) have changed into types of intestinal cells that are not normal
What Is Barrett s Esophagus? Having Barrett s esophagus means the cells lining the esophagus (the tube that links the mouth and the stomach) have changed into types of intestinal cells that are not normal
The normal esophagus is lined with squamous epithelium.
 .. ALAN J. CAMERON, M.D. In Barrett's esophagus, the squamous lining of the lower esophagus is replaced by columnar epithelium. Barrett's esophagus is associated with gastroesophageal reflux and an increased
.. ALAN J. CAMERON, M.D. In Barrett's esophagus, the squamous lining of the lower esophagus is replaced by columnar epithelium. Barrett's esophagus is associated with gastroesophageal reflux and an increased
B. Cystic Teratoma: Refer to virtual microscope slide p_223 ovary, teratoma and compare to normal virtual microscope slide 086 ovary.
 LAB 2: THE CONNECTIVE TISSUE AND EPITHELIUM The focus of this week s lab will be pathology of connective tissue and epithelium. The lab will introduce you to the four basic tissue types: epithelium, connective
LAB 2: THE CONNECTIVE TISSUE AND EPITHELIUM The focus of this week s lab will be pathology of connective tissue and epithelium. The lab will introduce you to the four basic tissue types: epithelium, connective
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
College of American Pathologists. Pathology Performance Measures included in CMS 2012 PQRS
 College of American Pathologists Pathology Performance Measures included in CMS 2012 PQRS Breast Cancer Resection Pathology Reporting Measure #99 pt category (primary tumor) and pn category (regional lymph
College of American Pathologists Pathology Performance Measures included in CMS 2012 PQRS Breast Cancer Resection Pathology Reporting Measure #99 pt category (primary tumor) and pn category (regional lymph
Gastric atrophy: use of OLGA staging system in practice
 Gastroenterology and Hepatology From Bed to Bench. 2016 RIGLD, Research Institute for Gastroenterology and Liver Diseases ORIGINAL ARTICLE Gastric atrophy: use of OLGA staging system in practice Mahsa
Gastroenterology and Hepatology From Bed to Bench. 2016 RIGLD, Research Institute for Gastroenterology and Liver Diseases ORIGINAL ARTICLE Gastric atrophy: use of OLGA staging system in practice Mahsa
Speaker disclosure. Objectives. GERD: Who and When to Treat 7/21/2015
 GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
Kids Like to Break the Rules: Gastrointestinal Pathology in Children
 Kids Like to Break the Rules: Gastrointestinal Pathology in Children Jeffrey Goldsmith MD Director of Surgical Pathology, Beth Israel Deaconess Medical Center; Consultant in Gastrointestinal Pathology,
Kids Like to Break the Rules: Gastrointestinal Pathology in Children Jeffrey Goldsmith MD Director of Surgical Pathology, Beth Israel Deaconess Medical Center; Consultant in Gastrointestinal Pathology,
CLINICAL EFFECTIVENESS
 Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Module 2 Heartburn Glossary
 Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
1. Esophageal diverticulum located above the upper esophageal sphincter is called
 Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ
 - Project manual + FAQ") Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable