Landmark articles on ventilation
|
|
|
- Preston Walton
- 5 years ago
- Views:
Transcription
1 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
2 ARDS
3 AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP 18mm Hg or absence of clinical e/o LA hypertension PaO2 : FiO2 ratio 300 ARDS PaO2 : FiO2 ratio 200 And all the above Independent of PEEP Bernard et al, Am J Respir CCM; 1994;149:818-24
4 Shortcomings of AECC Defination Confusion relating to ALI No explicit criteria for defining acute leading to ambiguity regarding cases of acute-on-chronic hypoxemia. High interobserver variability in interpreting chest X-rays. Difficulties identifying / ruling out cardiogenic or hydrostatic pulmonary edema, especially in an era of plummeting pulmonary artery catheter use. PaO2 / FiO2 ratio is sensitive to changes in ventilator settings

5
6 Berlin definition of acute respiratory distress syndrome Timing Chest imagining a Origin of oedema Oxygenation b Mild Within 1 week of a known clinical insult or new/worsening respiratory symptoms Bilateral opacities not fully explained by effusion, lobar/lung collapse, or nodules Respiratory failure not fully explained by cardiac failure or fluid overload; need objective assessment (for example, echocardiography) to exclude hydrostatic oedema if no risk factor present 200 <PaO 2 /FiO 2 < 300, with PEEP or CAP > 25 cmh 2 O c CPAP, continuous positive airway pressure;fio 2, fraction of inspired oxygen; PaO 2, partial pressure of arterial oxygen; PEEP, positive end-expiratory pressure. a Chest X-ray or computed tomography scan. b If altitude higher > 100 m, correction factors should be made as follows: PaO 2 /FiO 2 X (barometric pressure / 760). C this may be delivered non-invasively in the mild acute respiratory distress syndrome group. Adapted with permission from[9]. Moderate 100 <PaO 2 /FiO 2 < 200, with PEEP > 5 CmH 2 ) Severe PaO 2 /FiO 2 < 100, with PEEP > 5 cmh 2 O ARDS Definition task force: Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307:
7 Salient Differences Acute lung injury no longer exists.pao2/fio = mild ARDS. Acute onset of ARDS : within 7 days of some defined event, which may be sepsis, pneumonia, or simply a patient s recognition of worsening respiratory symptoms. Bilateral opacities consistent with pulmonary edema must be present ; may be detected on CT or chest X-ray. No need to exclude heart failure in the new ARDS definition; patients LV failure can coexist with ARDS. An objective assessment meaning an echocardiogram in most cases if there is no clear risk factor present
8 Is it any better? Compared with the AECC definition, the final Berlin Definition had better predictive validity for mortality, with an area under the ROC of (95% CI, ) vs (95% CI, ;P<.001) Gordon D. Rubenfeld, MD,JAMA. 2012;307(23):doi: /jama

9 CONCLUSIONS: The present study did not validate the Berlin definition of ARDS. Neither the stratification by severity nor the PaO2/FiO2 at study entry was independently associated with mortality Intensive care Med (2013) 39;
10 Low Tidal Volume Ventilation
11
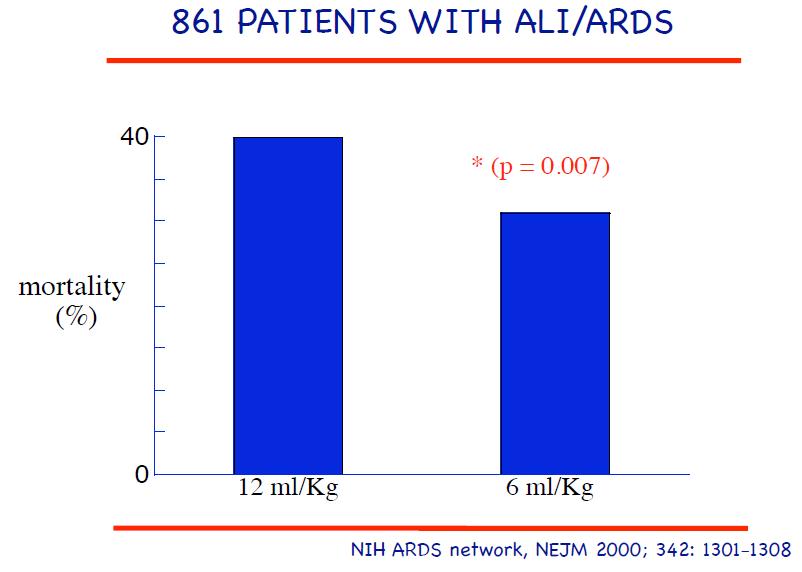
12 Summary Study design: Enrolled 861 patients and compared traditional ventilation treatment (initial tidal volume of 12 ml/kg PBW) and a Pplat of 50 cm of H2O, with ventilation with a lower tidal volume (initial tidal volume of 6 ml/kg PBW and a Pplat 30 cm of H2O. Primary outcome: death before a patient was discharged home and was breathing without assistance. Second primary outcome: ventilator-free days from day 1 to day 28.
13
14
15 Summary Results The trial was stopped after the enrollment of 861 patients because mortality was lower in the group treated with lower tidal volumes than in the group treated with traditional tidal volumes (31.0 percent vs percent, P=0.007) Low TV ventilation reduces absolute mortality by about 7-9%, number needed to treat of between The number of days without ventilator use during the first 28 days after randomization was greater in this group (12±11 vs. 10±11; P=0.007).
16 Summary Conclusions In patients with acute lung injury and the acute respiratory distress syndrome, mechanical ventilation with a lower tidal volume than is traditionally used results in decreased mortality and increases the number of days without ventilator use.

17
18
19 High PEEP or Low PEEP

20
21 Summary Objectives To evaluate the association of higher vs lower PEEP with patient-important outcomes in adults with acute lung injury or ARDS who are receiving ventilation with low tidal volumes and to investigate whether these associations differ across prespecified subgroups. Involved analysis of 3 trials: ALVEOLI, LOVS and EXPRESS

22
23 From: Higher vs Lower Positive End-Expiratory Pressure in Patients With Acute Lung Injury and Acute Respiratory Distress Syndrome: Systematic Review and Meta-analysis JAMA. 2010;303(9): doi: /jama For patients with ARDS at baseline: higher PEEP group had lesser mortality (34.1% vs 39.1%; P =.049) and more likely to achieve unassisted breathing earlier (64.3% vs 57.8%); For patients without ARDS at baseline: the RR for death in hospital with higher vs lower PEEP was higher (27.2% vs 19.4%) and the time to unassisted breathing proportions at 28 days was more, 70.1% vs 80.9%) Date of download: 6/17/2015
24 Summary Conclusions Treatment with higher vs lower levels of PEEP was not associated with improved hospital survival. However, higher levels were associated with improved survival among the subgroup of patients with ARDS. High PEEP is unlikely to benefit in patients with less severe lung injury; indeed, a strategy of treating these patients using high PEEP levels may be harmful.
25
26 Summary Objective To compare an established low-tidal-volume ventilation strategy (target TV of 6 ml/kg of PBW, Pplat 30 cm H 2 O, and conventional levels of PEEP (n = 508) with an experimental strategy based on the original openlung approach, combining low tidal volume, lung recruitment maneuvers, and high positive-end expiratory pressure (target TV of 6 ml/kg PBW + Pplat 40 cm H 2 O + recruitment maneuvers, and higher PEEP)(n = 475)
27 From: Ventilation Strategy Using Low Tidal Volumes, Recruitment Maneuvers, and High Positive End-Expiratory Pressure for Acute Lung Injury and Acute Respiratory Distress Syndrome: A Randomized Controlled Trial JAMA. 2008;299(6): doi: /jama Figure Legend: Patients were censored at hospital discharge and at death in the 2 analyses, respectively. Date of download: 6/17/2015 Copyright 2015 American Medical Association. All rights reserved.
28 Summary Main Outcome Measure All-cause hospital mortality. Conclusion: Higher PEEP provided no benefit in 28-day mortality (28 vs 32%, p = 0.2). This open-lung strategy did appear to improve secondary end points related to hypoxemia (reduced refractory hypoxia (~5% vs. 10%, p = 0.01) and use of rescue therapies This results, in combination with the 2 other major trials could justify use of higher PEEP levels as an alternative to the established low-peep, low-tidal-volume strategy
29 PRONING


30
31 Summary Multicenter, randomized trial in France and Spain, 466 patients Included patients with early, severe ARDS Early = within 36 hours of meeting ARDS criteria Severe = PaO 2 :FiO 2 ratio < 150 mm Hg (with FiO 2 of at least 60%, PEEP 5 cm H 2 0, and tidal volume of 6 ml/kg ideal weight) All patients underwent a hour stabilization period to verify inclusion criteria prior to randomization Prone positioning was conducted for at least 16 consecutive hours per day in standard ICU beds. Primary outcome: All cause mortality within 28 days after inclusion
32
33 Summary Proning was stopped once the patient met oxygenation requirements while supine for at least four hours (PaO 2 :FiO mm Hg with PEEP 10 and FiO2 60 Results Prone positioning significantly reduced 28-day all-cause mortality compared to supine positioning (16% vs 32.8%,NNT 6, p<0.001). 17% Absolute risk reduction Proning also reduced 90-day mortality (23.6% vs. 41%, NNT 6, p<0.001) No increase in adverse events
34 Summary Conclusion This trial showed that patients with ARDS and severe hypoxemia (as confirmed by a Pao2:Fio2 ratio of <150 mm Hg, with an Fio2 of 0.6 and a PEEP of 5 cm of water) can benefit from prone treatment when it is used early and in relatively long sessions
35 Current Role of HFOV

36
37 Summary Methods In a multicenter, RCT conducted at 39 intensive care units in five countries, we randomly assigned adults with new-onset, moderate-to-severe ARDS to HFOV targeting lung recruitment or to a control ventilation strategy targeting lung recruitment with the use of low tidal volumes and high PEEP Primary outcome was the rate of in-hospital death from any cause.
38 Summary Result: Trial stopped after 548 of a planned 1200 patients had undergone randomization in view of consistent trend towards harm. In-hospital mortality was 47% in the HFOV group, as compared with 35% in the control group (relative risk of death with HFOV, 1.33; 95% CI, 1.09 to 1.64; P = 0.005) More and longer need for sedation and vasoactive drugs in HFOV group

39
40 Summary Conclusions In adults with moderate-to-severe ARDS, early application of HFOV, as compared with a ventilation strategy of low tidal volume and high positive endexpiratory pressure, does not reduce, and may increase, in-hospital mortality

41
42 Role of ECMO

43
44 Summary Objective: RCT To evaluate the safety, clinical efficacy, and cost-effectiveness of extracorporeal membrane oxygenation (ECMO) compared with conventional ventilation support. Subjects: 180 adults aged years with severe (Murray score >3.0 or ph <7.20) but potentially reversible respiratory failure
45 Summary Primary outcome was death or severe disability at 6 months after randomization or before discharge from hospital. Primary analysis was by intention to treat Results 766 patients were screened; 180 were enrolled and randomly allocated to consideration for treatment by ECMO (n=90 patients) or to receive conventional management (n=90) 68 (75%) patients actually received ECMO 63% (57/90) of patients allocated to consideration for treatment by ECMO survived to 6 months without disability compared with 47% (41/87) of those allocated to conventional management (relative risk 0.69, p=0.03).
46 The absolute risk reduction for the primary outcome was 16%, which translates into a number-needed-to-treat of 6.2 patients
47 Summary Conclusions We recommend transferring of adult patients with severe but potentially reversible respiratory failure, whose Murray score exceeds 3.0 or who have a ph of less than 7.20 on optimum conventional management, to a centre with an ECMO-based management protocol to significantly improve survival without severe disability. This strategy is also likely to be cost-effective in settings with similar services to those in the UK
48 Areas of Uncertainty It is not clear which patients with ARDS are the best candidates for this treatment or which is the most favourable timing for the initiation of ECMO? The intervention in CESAR was referral to an ECMO centre not treatment with ECMO. In fact, only 75% of ECMO-referred patients actually received ECMO Lack of a management protocol for patients randomized to conventional treatment Would the results be replicable in smaller or less experienced centres Should we exclude patients who have required more than 7 days of high-pressure or high-fio2 ventilation from receiving ECMO.
49
50 Summary Methods Multicenter, double-blind trial enrolled 340 patients, with an onset of severe ARDS within the previous 48 hours were randomly assigned to receive, for 48 hours, either cisatracurium besylate (178 patients) or placebo (162 patients). Severe ARDS was defined as a ratio of the PaO2/FiO2) <150, with a PEEP of 5 cm H2O and a tidal volume of 6 to 8 ml/kg PBW. Primary outcome : 90-day in-hospital mortality rate
51
52 Summary Results The crude 90-day mortality was 31.6% in the cisatracurium group and 40.7% in the placebo group (P = 0.08). Mortality at 28 days was 23.7% with cisatracurium and 33.3% with placebo (P = 0.05). The rate of ICU-acquired paresis did not differ significantly between the two groups
53 Summary Conclusions In patients with severe ARDS, early administration of a neuromuscular blocking agent improved the adjusted 90-day survival and increased the time off the ventilator without increasing muscle weakness

54
55 Summary Study design Multicenter, double-blind, parallel-group trial Randomized 400 adults at intermediate to high risk of pulmonary complications after major abdominal surgery to either nonprotective mechanical ventilation or a strategy of lung-protective ventilation. Low tidal volume mechanical ventilation (LTV) ml/kg IBW; PEEP 6-8 cm H2O; recruitment maneuvers every 30 minutes Ordinary mechanical ventilation -- tidal volume ml/kg PEEP and recruitment maneuvers were not protocolized but could be provided at the anesthesiologist's discretion Primary outcome: a composite of major pulmonary and extrapulmonary complications occurring within the first 7 days after surgery.

56
57 Summary Results: Major postop complications (within 1 week after abdominal surgery): 27.5% of the patients receiving larger tidal volumes, but only in 10.5% of LTV. Postop acute respiratory failure: 5% of patients in the LTV group required invasive or NIV in the week after surgery, compared to 17% in the conventional ventilation group -- a 69% relative risk reduction. Pulmonary complications (pneumonia, atelectasis, ARDS, respiratory failure): 17.5% of patients receiving LTV had of any type, compared to 36% in the conventional ventilation group. 30-day mortality was similar in both groups (~3%), but hospital stays were slightly shorter in LTV. There was no apparent harm from low tidal volume mechanical ventilation.
58 Summary CONCLUSIONS As compared with a practice of nonprotective mechanical ventilation, the use of a lungprotective ventilation strategy in intermediate-risk and high-risk patients undergoing major abdominal surgery was associated with improved clinical outcomes and reduced health care utilization

59
60

61 Sherpa Neto et al, Curr Opin Crit Care 2015, 21:65 73

62

63

64

65
66 Early or Late Tracheotomy
67
68 Summary Objective To test whether early vs late tracheostomy would be associated with lower mortality in adult patients requiring mechanical ventilation in ICU. Study Design Multicentered RCT enrolled 909 adult patients on mechanical ventilation for less than 4 days and identified by the treating physician as likely to require at least 7 more days of mechanical ventilation. Patients were randomized 1:1 to early tracheostomy (within 4 days) or late tracheostomy (after 10 days if still indicated). Primary outcome measure was 30-day mortality.
69 Summary Results Early tracheostomy group: 91.9% received a tracheostomy late tracheostomy group: 44.9% received a tracheostomy. All-cause 30 days mortality was 30.8% in the early and 31.5% in the late group (absolute risk reduction for early vs late, 0.7%). Two-year mortality was 51.0% in the early and 53.7% in the late group (P =.74). Median critical care unit length of stay in survivors was 13.0 days in the early and 13.1 days in the late group (P =.74). Tracheostomy-related complications were reported for 6.3% of patients (5.5% in the early group, 7.8% in the late group).
70 Summary Conclusions Early tracheostomy within 4 days of critical care admission was not associated with an improvement in 30-day mortality or other important secondary outcomes. The ability of clinicians to predict which patients required extended ventilatory support was limited.
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Acute Lung Injury/ARDS. Disclosures. Overview. Acute Respiratory Failure 5/30/2014. Research funding: NIH, UCSF CTSI, Glaxo Smith Kline
 Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
How ARDS should be treated in 2017
 How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
Management of Severe ARDS: Current Canadian Practice
 Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Part 2 of park s Ventilator and ARDS slides for syllabus
 Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
ARDS: MANAGEMENT UPDATE
 ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
OSCAR & OSCILLATE. & the Future of High Frequency Oscillatory Ventilation (HFOV)
") & & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
& & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE (LUNG-SAFE)
") Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE (LUNG-SAFE) John Laffey, Giacomo Bellani, Tai Pham, Eddy Fan, Antonio Pesenti on behalf of the LUNG SAFE Investigators
Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE (LUNG-SAFE) John Laffey, Giacomo Bellani, Tai Pham, Eddy Fan, Antonio Pesenti on behalf of the LUNG SAFE Investigators
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Ventilation update Anaesthesia departmental PGME. Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care
 Ventilation update Anaesthesia departmental PGME Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care What s fashionable in ICU ventilation? Acute respiratory distress syndrome
Ventilation update Anaesthesia departmental PGME Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care What s fashionable in ICU ventilation? Acute respiratory distress syndrome
The GOLD Study. Goal of Open Lung Ventilation in Donors. Michael A. Matthay M.D. and Lorraine B. Ware, MD. Disclosures
 The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
Does proning patients with refractory hypoxaemia improve mortality?
 Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Protective ventilation for ALL patients
 Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
What s New About Proning?
 1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
Year in Review Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
Seminar. Current Concepts
 Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
Biomarkers for ARDS not so simple. John Laffey. Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA
 Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Acute respiratory distress syndrome
 20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
How the Knowledge Proceeds in Intensive Care: the ARDS Example
 How the Knowledge Proceeds in Intensive Care: the ARDS Example 2016, Antalya Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany INDUCTION: From particular (application) to general (law/theory)
How the Knowledge Proceeds in Intensive Care: the ARDS Example 2016, Antalya Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany INDUCTION: From particular (application) to general (law/theory)
NIV in hypoxemic patients
 NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
Outline. Basic principles of lung protective ventilation. The challenging areas. Small tidal volumes Recruitment
 ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
Prone Positioning in Severe Acute Respiratory Distress Syndrome
 Prone Positioning in Severe Acute Respiratory Distress Syndrome Claude Guérin, M.D., Ph.D., Jean Reignier, M.D., Ph.D., Jean-Christophe Richard, M.D., Ph.D., Pascal Beuret, M.D., Arnaud Gacouin, M.D.,
Prone Positioning in Severe Acute Respiratory Distress Syndrome Claude Guérin, M.D., Ph.D., Jean Reignier, M.D., Ph.D., Jean-Christophe Richard, M.D., Ph.D., Pascal Beuret, M.D., Arnaud Gacouin, M.D.,
ARDS and treatment strategies
 ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Phenotyping of ARDS and non ARDS Patients
 Critical Care Canada Forum 2018 Sheraton Toronto, Toronto, Canada November 8, 2018; 11:05h 11:25h Phenotyping of and non Patients Berlin & Kigali, RALE score, Reclassification, Driving Pressure and Mechanical
Critical Care Canada Forum 2018 Sheraton Toronto, Toronto, Canada November 8, 2018; 11:05h 11:25h Phenotyping of and non Patients Berlin & Kigali, RALE score, Reclassification, Driving Pressure and Mechanical
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
The Berlin Definition: Does it fix anything?
 The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE
 ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE Acute respiratory distress syndrome: challenges for translational research and opportunities
ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE Acute respiratory distress syndrome: challenges for translational research and opportunities
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME
 FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
Year in Review: Critical Care Medicine
 Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Oregon Health and Science University Portland, Oregon USA
 Classifying ARDS The Role of EVLW Ch l Philli MD Charles Phillips MD Oregon Health and Science University Portland, Oregon USA Incidence High ARDS 2013 150,000 200,000 per year in US alone. Mortality persists
Classifying ARDS The Role of EVLW Ch l Philli MD Charles Phillips MD Oregon Health and Science University Portland, Oregon USA Incidence High ARDS 2013 150,000 200,000 per year in US alone. Mortality persists
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
ARDS AND ECLS DEPARTMENT OF CRITICAL CARE JOSHUA HUELSTER, MD ABBOTT NORTHWESTERN HOSPITAL
 ARDS AND ECLS JOSHUA HUELSTER, MD DEPARTMENT OF CRITICAL CARE ABBOTT NORTHWESTERN HOSPITAL DISCLOSURES I have no financial disclosures I have no conflicts of interest I have my own biases (we all do) OBJECTIVES
ARDS AND ECLS JOSHUA HUELSTER, MD DEPARTMENT OF CRITICAL CARE ABBOTT NORTHWESTERN HOSPITAL DISCLOSURES I have no financial disclosures I have no conflicts of interest I have my own biases (we all do) OBJECTIVES
Trial protocol - NIVAS Study
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 Trial protocol - NIVAS Study METHODS Study oversight The Non-Invasive Ventilation after Abdominal Surgery
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 Trial protocol - NIVAS Study METHODS Study oversight The Non-Invasive Ventilation after Abdominal Surgery
Section: Therapy Effective Date: October 15, 2016 Subsection: Original Policy Date: June 19, 2015 Subject:
 Last Review Status/Date: September 2016 Page: 1 of 30 Summary Extracorporeal membrane oxygenation (ECMO) provides extracorporeal circulation and physiologic gas exchange for temporary cardiorespiratory
Last Review Status/Date: September 2016 Page: 1 of 30 Summary Extracorporeal membrane oxygenation (ECMO) provides extracorporeal circulation and physiologic gas exchange for temporary cardiorespiratory
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
ECMO/ECCO 2 R in Acute Respiratory Failure
 ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal
 Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
ARDS Survival: Building A Roadmap to Achieve Successful Short and Long Term Outcomes
 ARDS Survival: Building A Roadmap to Achieve Successful Short and Long Term Outcomes Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant LLC Director/Ambassador WFCCN
ARDS Survival: Building A Roadmap to Achieve Successful Short and Long Term Outcomes Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant LLC Director/Ambassador WFCCN
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
PAEDIATRIC RESPIRATORY FAILURE. Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre
 PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Neuromuscular Blockade in ARDS
 Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
NIV in acute hypoxic respiratory failure
 All course materials, including the original lecture, are available as webcasts/podcasts at www.ers-education. org/niv2009.htm NIV in acute hypoxic respiratory failure Educational aims This presentation
All course materials, including the original lecture, are available as webcasts/podcasts at www.ers-education. org/niv2009.htm NIV in acute hypoxic respiratory failure Educational aims This presentation
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015
: Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015") Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Agenda. Mechanical Ventilation in Morbidly Obese Patients. Paolo Pelosi. ESPCOP, Ostend, Belgium Saturday, November 14, 2009.
 Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
15 Years Of Clinical Trials In ARDS: What Progress Have We Made?
 15 Years Of Clinical Trials In ARDS: What Progress Have We Made? Niall D. Ferguson, MD, FRCPC, MSc Head of Critical Care Medicine University Health Network & Mount Sinai Hospital Senior Scientist, Toronto
15 Years Of Clinical Trials In ARDS: What Progress Have We Made? Niall D. Ferguson, MD, FRCPC, MSc Head of Critical Care Medicine University Health Network & Mount Sinai Hospital Senior Scientist, Toronto
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
ECMO and refractory Hypoxemia
 ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Kansas City, MO 2 University of Missouri-Kansas City, MO 3 University of Kansas School of Pharmacy,
 in Acute Respiratory Distress Syndrome Joshua R. Howitt, Pharm.D. 1,2,3, John D. Hill, Pharm.D. Candidate 2, Trenton D. Nauser, M.D. 1,4 1 Department of Veterans Affairs, Kansas City, MO 2 University of
in Acute Respiratory Distress Syndrome Joshua R. Howitt, Pharm.D. 1,2,3, John D. Hill, Pharm.D. Candidate 2, Trenton D. Nauser, M.D. 1,4 1 Department of Veterans Affairs, Kansas City, MO 2 University of
Noninvasive Ventilation: Non-COPD Applications
 Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Data Collection Tool. Standard Study Questions: Admission Date: Admission Time: Age: Gender:
 Data Collection Tool Standard Study Questions: Admission Date: Admission Time: Age: Gender: Specifics of Injury: Time of Injury: Mechanism of Injury Blunt vs Penetrating? Injury Severity Score? Injuries:
Data Collection Tool Standard Study Questions: Admission Date: Admission Time: Age: Gender: Specifics of Injury: Time of Injury: Mechanism of Injury Blunt vs Penetrating? Injury Severity Score? Injuries:
Adjunct Therapies for Pediatric ARDS: Where are the Data?
 Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Lung-protective ventilation in intensive care unit and operation room Serpa Neto, A.
 UvA-DARE (Digital Academic Repository) Lung-protective ventilation in intensive care unit and operation room Serpa Neto, A. Link to publication Citation for published version (APA): Serpa Neto, A. (2017).
UvA-DARE (Digital Academic Repository) Lung-protective ventilation in intensive care unit and operation room Serpa Neto, A. Link to publication Citation for published version (APA): Serpa Neto, A. (2017).
ARDS A Brief Overview. Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine
 ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Acute Respiratory Distress Syndrome
 Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Noninvasive respiratory support:why is it working?
 Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1).
.") PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
Ventilator ECMO Interactions
 Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none