ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
|
|
|
- Darren Gibson
- 5 years ago
- Views:
Transcription
1 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc

2 Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive during acute respira-
3 In which patient should you worry? Tidal volume consistently > 6-8 ml/kg IBW in relation to ventilated lung volume Severe lung injury Obvious excessive inspiratory efforts - use of accessory muscles Transpulmonary pressure > 2-22 cm H2O, PTP > 2 P.1 > 3-4 cm H2O Low threshold for EAdi and Ppl measurement
4 P.1 Marker for respiratory drive and WOB (normal cm H2O)
5 Therapeutic measures Lower the level of spontaneous effort Optimize patient-ventilator interaction Control the patient s respiratory drive Treat acidosis and hypoxemia + fever/pain Provide sufficient sedation and analgesia Use (partial) neuromuscular blockade Extracorporeal CO2 removal Apply sufficient PEEP to maximize fluid-like lung behavior
6 Explain what you see! (A) ( ) P aw (cmh 2 O) ( ) Flow (L/s) 4 1 ( ) P es (cmh 2 O) ( ) P L (cmh 2 O) Peak Plateau ( ) Regional Lung Stretch ( Z) Nondependent ( ) Regional Lung Stretch ( Z) Dependent Time (S) (B) ( ) P aw (cmh 2 O) ( ) Flow (L/s) 3 2 ( ) P es (cmh 2 O) ( ) P L (cmh 2 O) Peak Plateau ( ) Regional Lung Stretch ( Z) Nondependent ( ) Regional Lung Stretch ( Z) Dependent Time (S)
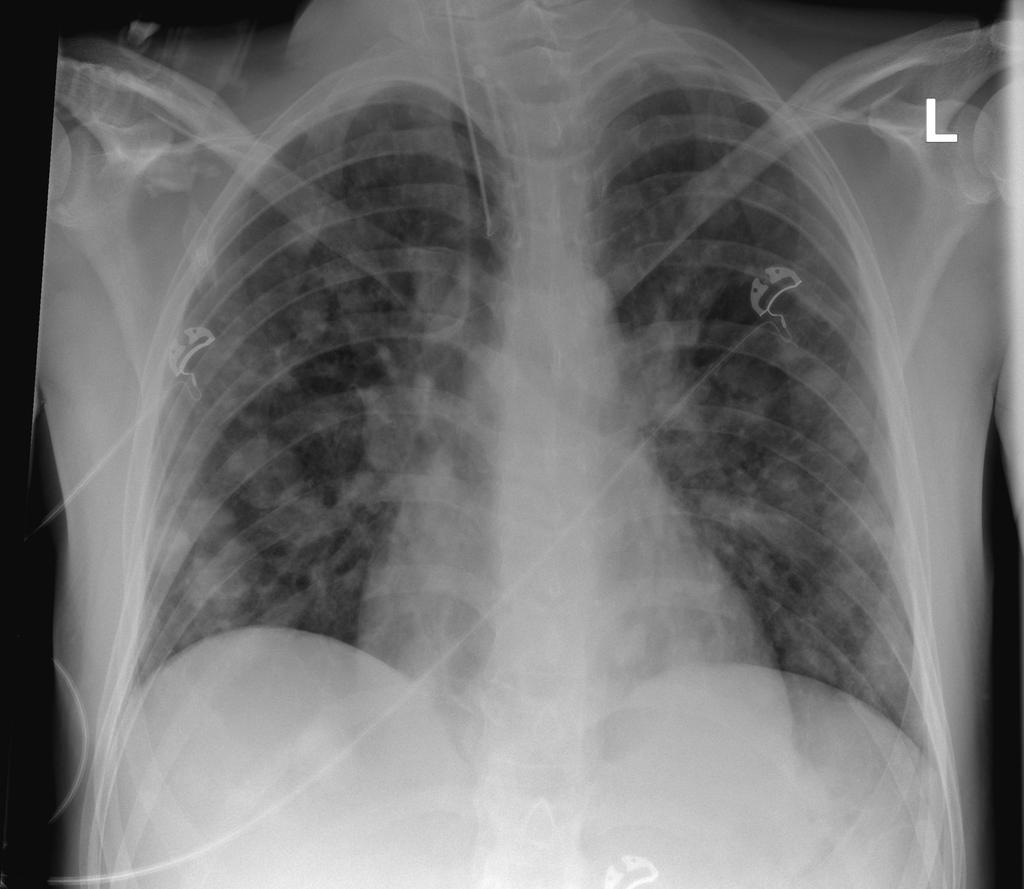
7 A recent case Male, 3 PMH: negative 22/9: admission with progressive dyspnea Diagnosis: metastasized nonseminoma testicular cancer


8 A recent case Chest X-ray admission CT scan 3/1
9 Patient 2/1 PSV: 6/6, Tv 65-7 ml RR: 2 P.1: 5 cmh2o Dynamic compliance 9-1 ml/cmh2o
10 PSV 6/6 Flow Pairway Pes TPP TDP EDi
11 Spontaneous breathing Flow Pes TPP TDP EDi
12 Work of breathing PSV 6/6 Spontaneous breathing WOB J/L (N.35) WOB J/min (N 2.4)
13 22/1
14 A recent case 23/1: Passes SBT Extubation - transfer to intermediate care unit
15 Conclusion High respiratory drive in spontaneously breathing patients or on assisted ventilation may induce lung injury However, it is unclear exactly when P-SILI starts and has an impact on outcome Rethink your strategy when danger signs are present especially in inhomogeneous lungs with solid like behavior
16 Ventilator Induced Lung Injury Vigor spontaneous efforts Mechanical heterogeneity ph and vascular pressures Reduced lung capacity Stress / Strain Mechanical power Disease stage and VILI predisposition Mechanical heterogeneity
17 Rescue therapies Prone position NO or prostacyclin inhalation High frequency oscillation Extra corporeal life support






18 Difficulties with Oxygenation Adequate CO ino Prone Higher PEEP Recruitment Maneuvers Prone Position HFO When above strategies are ineffective consider VV-ECMO
19 Beneficial effects of prone position 2 P/F increase 27-39% 3 N = 29 Supine higher Prone higher 1 Day 1 Day 2 Day 3 Patients (%) Meta-analysis N = 929 In total 7-8% of patients responded < > 24 P/F response (mmhg) Sus S. Intensive Care Med 21;36: Gattinoni L. Crit care Med 23;31:
20 Mechanical effects of proning Supine Prone 4 P <.5 NS P <.5 P < Median Ecw (cmh2/l) El (cmh2o/l) Pplat (cmh2o) Rl (cmh2o/l/s) Riad Z. Am J Respir Crit Care Med 218
21 Prone position in patients with ARDS All evidence points to the fact that in the prone position blood flow is greatest in the dorsal (non-dependent) parts demonstrating the importance of the arterial tree Total ventilation may increase by a more homogenous pleural pressure and by eliminating the weight of the heart and liver
22 Reduction in pleural gradient with proning

23 The position of the heart
24 Prone position in severe ARDS MC (27) RCT Severe ARDS and MV < 36 hrs with PF < 15 mmhg, FiO2.6 and PEEP 5 Tv 6 ml/kg PBW After inclusion stabilization period of hrs Guérin C. N Engl J Med 213
25 Prone position in severe ARDS Prone for at least 16 consecutive hrs PEEP and FiO2 from table: Pplat < 3 and ph Clear criteria for stopping prone position (P/F 15 + PEEP 1 + FiO2.6 in supine position Strategy followed for up to 28 days Proning as rescue in the supine group strictly controlled Guérin C. N Engl J Med 213
26 Prone position in severe ARDS Supine (N = 229) Prone (N = 237) 1 P <.1 P <.1 P < , , ,6 16 Mortality D28 Mortality D9 Extubation D9 Better oxygenation and less rescue therapy in prone group Main cause pneumonia - 4 ± 4 prone sessions Guérin C. N Engl J Med 213
27 Prone position - metaanalysis Sus S. CMAJ 214;186:E381
28 Prone position - metaanalysis Homogenous distribution of lung stress along the vertical gradient Beitler JR. Intensive Care Med 214;4:
29
30 Prone position and RV failure Before PP After 18 h of PP P-value SAP (mm Hg) 115 ± ± 14 NS HR (bpm) 17 ± 15 1 ± 13,19 CI (l/min/m 2 ) 2.9 ± ±.8,13 RVEDA/LVEDA.91 ± ±.21 <,1 Septal eccentricity 1.5 ± ±.1 <,1 TR (n) 2 7 LVEDV (ml) 45 ± ± 21 <,1 LVEF (%) 58 ± 11 6 ± 9 NS N = 21 Severe ARDS PF < 1 Veillard-Baron A. Chest 27;132:
31 Adverse effects? Pressure ulcers (RR 1.29 [1.16,1.44]) ET obstruction (RR 1.58 [1.24,2.1]) Thoracostomy tube dislodgement (RR 3.14 [1.2,9.69]) Sus S. Intensive Care Med 21;36:
32 Prone position and ICP N = kpa Supine Prone 1 min Prone 1 h Prone 3 h Supine 1 min Supine 1 h PaO2 PaCO2 Thelandersson A. Acta Anaesthesiol Scand 26;5:
33 Prone position and ICP N = 11 mm Hg Supine Prone 1 min Prone 1 h Prone 3 h Supine 1 min Supine 1 h ICP CPP Thelandersson A. Acta Anaesthesiol Scand 26;5:
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Effects of mechanical ventilation on organ function. Masterclass ICU nurses
 Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Year in Review Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
MECHANICAL VENTILATION PROTOCOLS
 GENERAL or SURGICAL Initial Ventilator Parameters Ventilator Management (see appendix I) Assess Patient Data (see appendix II) Data Collection Mode: Tidal Volume: FIO2: PEEP: Rate: I:E Ratio: ACUTE PHASE
GENERAL or SURGICAL Initial Ventilator Parameters Ventilator Management (see appendix I) Assess Patient Data (see appendix II) Data Collection Mode: Tidal Volume: FIO2: PEEP: Rate: I:E Ratio: ACUTE PHASE
A simple case of.. Acute severe asthma. MasterclassIC Schiermonnikoog 2017
 A simple case of.. Acute severe asthma MasterclassIC Schiermonnikoog 2017 Case (1) Female, 27 - G1P0 (26 weeks) PMH - several admissions for severe acute asthma (no MV) Progressive dyspnea for 1 week Admitted
A simple case of.. Acute severe asthma MasterclassIC Schiermonnikoog 2017 Case (1) Female, 27 - G1P0 (26 weeks) PMH - several admissions for severe acute asthma (no MV) Progressive dyspnea for 1 week Admitted
Protective ventilation for ALL patients
 Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Ventilator ECMO Interactions
 Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
How ARDS should be treated in 2017
 How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
What s New About Proning?
 1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal
 Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
Right Ventricle. Interaction with the pulmonary circulation. Fellowship Intensive Care Nijmegen
 Right Ventricle Interaction with the pulmonary circulation Fellowship Intensive Care Nijmegen Normal right ventricle PAP 25/10 EF 62 ± 8% Constant low pressure perfusion of the lung Maintain low RA pressure
Right Ventricle Interaction with the pulmonary circulation Fellowship Intensive Care Nijmegen Normal right ventricle PAP 25/10 EF 62 ± 8% Constant low pressure perfusion of the lung Maintain low RA pressure
Management of Severe ARDS: Current Canadian Practice
 Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Part 2 of park s Ventilator and ARDS slides for syllabus
 Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
ARDS & TBI - Trading Off Ventilation Targets
 ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ECMO: a breakthrough in care for respiratory failure. PD Dr. Thomas Müller Regensburg no conflict of interest
 ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Does proning patients with refractory hypoxaemia improve mortality?
 Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
OSCAR & OSCILLATE. & the Future of High Frequency Oscillatory Ventilation (HFOV)
") & & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
& & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
Neuromuscular Blockade in ARDS
 Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Noninvasive respiratory support:why is it working?
 Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Outline. Basic principles of lung protective ventilation. The challenging areas. Small tidal volumes Recruitment
 ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Proportional Assist Ventilation (PAV) (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure
 (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure") Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Patient-Ventilator Synchrony and Impact on Outcome
 Variables Controlled during Mechanical Ventilation Patient-Ventilator Synchrony and Impact on Outcome 9-30-17 Cox Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts
Variables Controlled during Mechanical Ventilation Patient-Ventilator Synchrony and Impact on Outcome 9-30-17 Cox Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts
Inhaled nitric oxide: clinical evidence for use in adults
 Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
Patient Asynchrony and Its Impact on Patient Outcome
 Patient Asynchrony and Its Impact on Patient Outcome 5-14-18 CSRC Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts Conflict of Interest Disclosure Robert
Patient Asynchrony and Its Impact on Patient Outcome 5-14-18 CSRC Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts Conflict of Interest Disclosure Robert
Adjunct Therapies for Pediatric ARDS: Where are the Data?
 Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
ECMO/ECCO 2 R in Acute Respiratory Failure
 ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
11 th Annual Congress Turkish Thoracic Society. Mechanical Ventilation in Acute Hypoxemic Respiratory Failure
 11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
Mechanical ventilation induced or exacerbated right ventricular failure
 Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
Acute Lung Injury/ARDS. Disclosures. Overview. Acute Respiratory Failure 5/30/2014. Research funding: NIH, UCSF CTSI, Glaxo Smith Kline
 Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS
 with surfactant in pediatric ARDS") Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Pro: Early use of VV ECMO for ARDS
 Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Dr. Yasser Fathi M.B.B.S, M.Sc, M.D. Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah
 BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
Ventilation de l obèse: les 10 points clés
 Ventilation de l obèse: les 10 points clés Samir JABER Department of Critical Care Medicine and Anesthesiology (DAR B) Saint Eloi University Hospital and Montpellier School of Medicine; INSERM U1046 University
Ventilation de l obèse: les 10 points clés Samir JABER Department of Critical Care Medicine and Anesthesiology (DAR B) Saint Eloi University Hospital and Montpellier School of Medicine; INSERM U1046 University
Seminar. Current Concepts
 Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME
 FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
Recognizing and Correcting Patient-Ventilator Dysynchrony
 2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
Instellen van beademingsparameters bij de obese pa3ent. MDO Nynke Postma
 Instellen van beademingsparameters bij de obese pa3ent MDO 19-1- 2015 Nynke Postma 1. Altered respiratory mechanics in obese pa@ents 2. Transpulmonary pressure 3. Titra@ng PEEP 4. Titra@ng @dal volume
Instellen van beademingsparameters bij de obese pa3ent MDO 19-1- 2015 Nynke Postma 1. Altered respiratory mechanics in obese pa@ents 2. Transpulmonary pressure 3. Titra@ng PEEP 4. Titra@ng @dal volume
How the Knowledge Proceeds in Intensive Care: the ARDS Example
 How the Knowledge Proceeds in Intensive Care: the ARDS Example 2016, Antalya Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany INDUCTION: From particular (application) to general (law/theory)
How the Knowledge Proceeds in Intensive Care: the ARDS Example 2016, Antalya Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany INDUCTION: From particular (application) to general (law/theory)
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
NIV in hypoxemic patients
 NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
Tracking lung recruitment and regional tidal volume at the bedside. Antonio Pesenti
 Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Concerns and Controversial Issues in NPPV. Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation
 : Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
: Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
OLB (Open Lung Biopsy) in ARDS
 in ARDS") OLB (Open Lung Biopsy) in ARDS Claude GUERIN MD PhD Réanimation Médicale Hôpital de la Croix-Rousse Université de Lyon Lyon, France CCF Toronto October 28 th 2012 CCF 2012 1 Disclosure No conflict of interest
OLB (Open Lung Biopsy) in ARDS Claude GUERIN MD PhD Réanimation Médicale Hôpital de la Croix-Rousse Université de Lyon Lyon, France CCF Toronto October 28 th 2012 CCF 2012 1 Disclosure No conflict of interest
LAS VEGAS Case Report Form 1 Intra-Operative
 LAS VEGAS Case Report Form 1 Intra-Operative Patient Informed Consent 1. Informed consent applicable: yes no (choose no if waived by local EC) 1.1 If applicable; was consent obtained? yes no 1.2 If yes,
LAS VEGAS Case Report Form 1 Intra-Operative Patient Informed Consent 1. Informed consent applicable: yes no (choose no if waived by local EC) 1.1 If applicable; was consent obtained? yes no 1.2 If yes,
Mechanical Ventilation in COPD patients
 Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Ventilation update Anaesthesia departmental PGME. Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care
 Ventilation update Anaesthesia departmental PGME Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care What s fashionable in ICU ventilation? Acute respiratory distress syndrome
Ventilation update Anaesthesia departmental PGME Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care What s fashionable in ICU ventilation? Acute respiratory distress syndrome
Mechanical Ventilation in COPD patients
 Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
RESCUE VENTILATION SUMMARY
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Supplementary Online Content 2
 Supplementary Online Content 2 van Meenen DMP, van der Hoeven SM, Binnekade JM, et al. Effect of on demand vs routine nebulization of acetylcysteine with salbutamol on ventilator-free days in intensive
Supplementary Online Content 2 van Meenen DMP, van der Hoeven SM, Binnekade JM, et al. Effect of on demand vs routine nebulization of acetylcysteine with salbutamol on ventilator-free days in intensive
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
You are caring for a patient who is intubated and. pressure control ventilation. The ventilator. up to see these scalars
 Test yourself Test yourself #1 You are caring for a patient who is intubated and ventilated on pressure control ventilation. The ventilator alarms and you look up to see these scalars What is the most
Test yourself Test yourself #1 You are caring for a patient who is intubated and ventilated on pressure control ventilation. The ventilator alarms and you look up to see these scalars What is the most
Spontaneous Breathing Trial and Mechanical Ventilation Weaning Process
 Page 1 of 5 ASSESSMENT INTERVENTION Patient receiving mechanical ventilation Baseline ventilatory mode/ settings RT and RN to assess criteria 1 for SBT Does patient meet criteria? RT to initiate SBT Does
Page 1 of 5 ASSESSMENT INTERVENTION Patient receiving mechanical ventilation Baseline ventilatory mode/ settings RT and RN to assess criteria 1 for SBT Does patient meet criteria? RT to initiate SBT Does
Literature List Electrical Impedance Tomography
 Literature List Electrical Impedance Tomography 2017 Electrical Impedance Tomography (EIT) Literature List 2017 INDEX Writer Subject Publication Page Piraino T, Fan E Acute life-threatening hypoxemia during
Literature List Electrical Impedance Tomography 2017 Electrical Impedance Tomography (EIT) Literature List 2017 INDEX Writer Subject Publication Page Piraino T, Fan E Acute life-threatening hypoxemia during
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
INTELLiVENT -ASV insight. Alexandra Geiger CAS, Dr. Marc Wysocki, Head of Medical Research Hamilton Medical
 INTELLiVENT -ASV insight Alexandra Geiger CAS, Dr. Marc Wysocki, Head of Medical Research Hamilton Medical First Automation of HAMILTON MEDICAL 1998 Adaptive Support Ventilation (ASV) ASV optimize VT and
INTELLiVENT -ASV insight Alexandra Geiger CAS, Dr. Marc Wysocki, Head of Medical Research Hamilton Medical First Automation of HAMILTON MEDICAL 1998 Adaptive Support Ventilation (ASV) ASV optimize VT and
Weaning: Neuro Ventilatory Efficiency
 Weaning: Neuro Ventilatory Efficiency Christer Sinderby Department of Critical Care Keenan Research Center at the Li Ka Shing Knowledge Institute of St. Michael's Hospital Faculty of Medicine, University
Weaning: Neuro Ventilatory Efficiency Christer Sinderby Department of Critical Care Keenan Research Center at the Li Ka Shing Knowledge Institute of St. Michael's Hospital Faculty of Medicine, University
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
Respiratory Mechanics
 Respiratory Mechanics Critical Care Medicine Specialty Board Tutorial Dr Arthur Chun-Wing LAU Associate Consultant Intensive Care Unit, Pamela Youde Nethersole Eastern Hospital, Hong Kong 17 th June 2014
Respiratory Mechanics Critical Care Medicine Specialty Board Tutorial Dr Arthur Chun-Wing LAU Associate Consultant Intensive Care Unit, Pamela Youde Nethersole Eastern Hospital, Hong Kong 17 th June 2014
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
New Modes to Enhance Synchrony & Dietrich Henzler MD, PhD, FRCPC Division of Critical Care
 New Modes to Enhance Synchrony & Dietrich Henzler MD, PhD, FRCPC Division of Critical Care Disclosure Conflicts of Interest 2001-2011 Research Grants & Payments (cost reimbursements, speaker fees) Draeger
New Modes to Enhance Synchrony & Dietrich Henzler MD, PhD, FRCPC Division of Critical Care Disclosure Conflicts of Interest 2001-2011 Research Grants & Payments (cost reimbursements, speaker fees) Draeger
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION