What s new in Hepatology AASLD 2016
|
|
|
- Louise Gaines
- 5 years ago
- Views:
Transcription

1 What s new in Hepatology AASLD 2016 CWN Spearman C Kassianides
2 What s new in Hepatology? AASLD 2016 CWN SPEARMAN Hepatitis C Alcoholic liver disease Cholestatic Liver Disease Primary biliary Cholangitis Primary Sclerosing cholangitis Cirrhosis C KASSIANIDES Hepatitis B NASH
3 HEPATITIS C
4 Hepatitis C : ERA of DAAs CURE is now possible for : SVR >90% o o o Treatment naïve, experienced and cirrhotic patients HIV/HCV co-infection Liver transplant patients SVR improves prognosis of non-cirrhotic and cirrhotic HCV pts o o Concerns re HCC and Hepatitis B reactivation on DAA therapy Re-infection risks must be addressed: harm reduction programmes SVR improves both all-cause and liver-related mortality All patients with chronic hepatitis C are candidates for Rx Prioritise patients with : o o o o Advanced fibrosis or cirrhosis HIV/HBV co-infection Extrahepatic manifestations Transplant patients
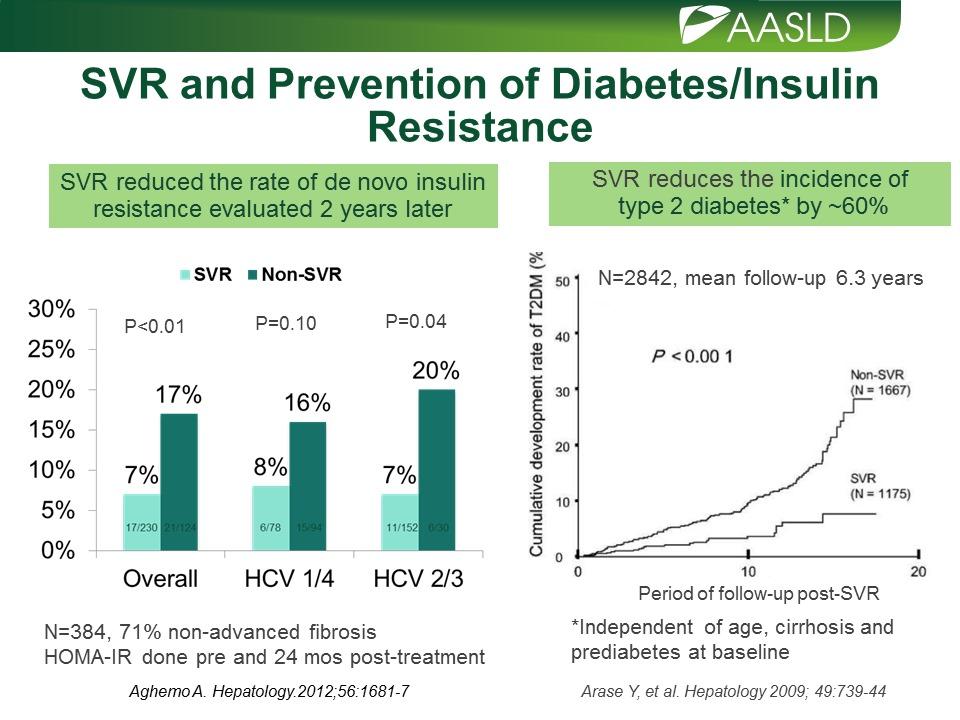
5

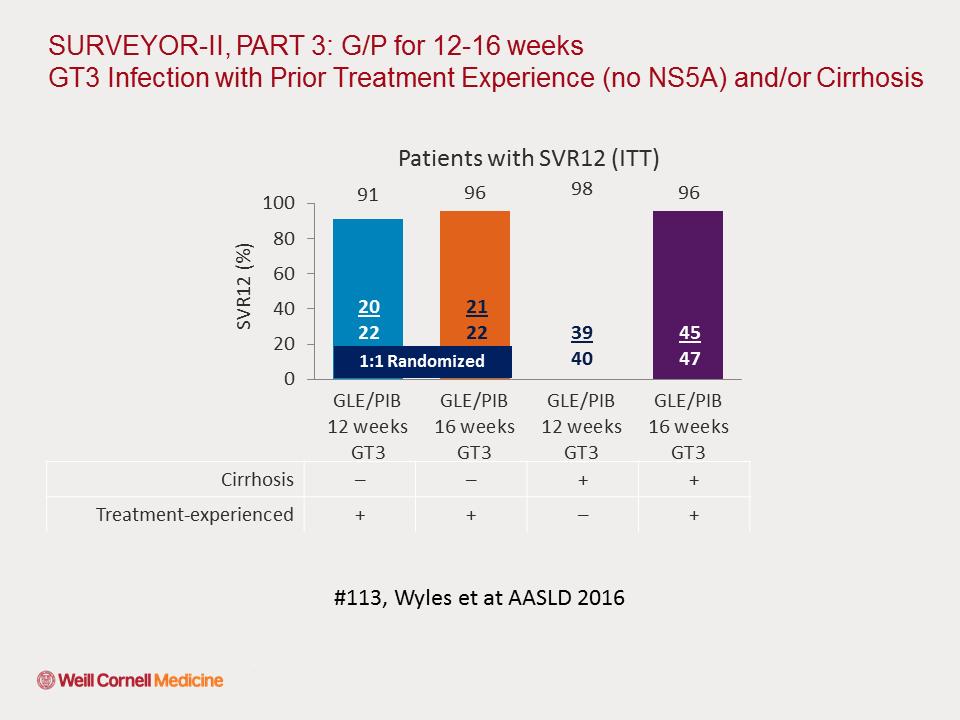
6

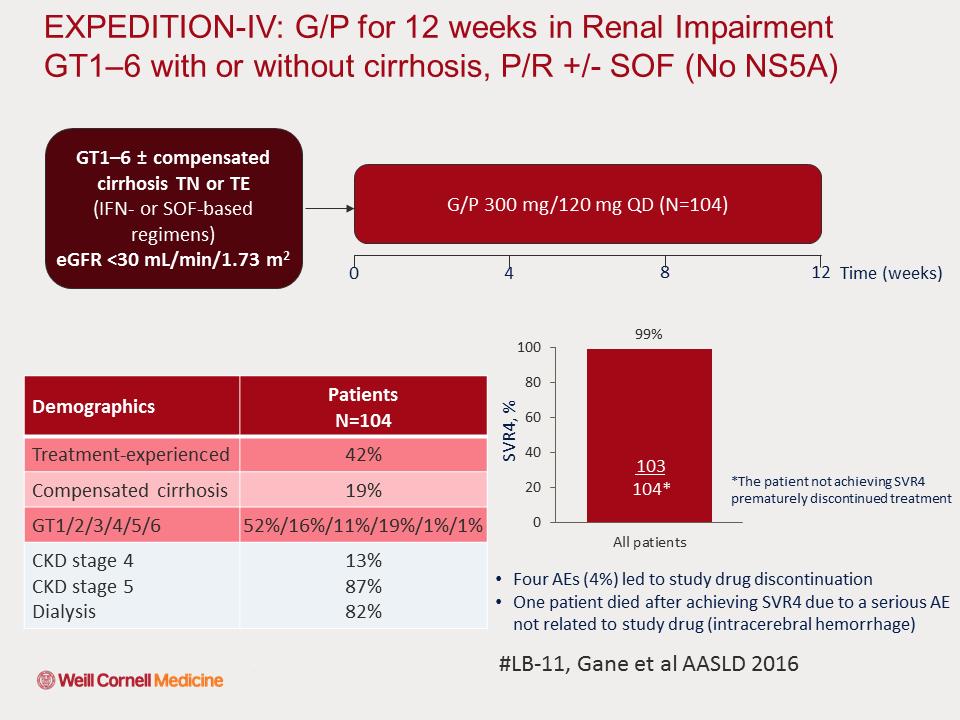
7

8
9 HCV Treatment : The Future? Pan-genotypic DAA Shorter duration with minimal monitoring: 8, 12 & 16 wks Aim for Test and treat: Are we ready? Better DAA Options in 2016 for: o Genotype 3 o o Stage 4 kidney disease/dialysis Decompensated cirrhosis In 2016: What our new therapeutic options?
10 GILEAD S PROGRAMME EPCLUSA Sofosbuvir (NS5B)/Velpastasvir (NS5A) o o Pangenotypic FDC ASTRAL1-4 Studies: >90% SVR - GT 1-6; Rx naïve and experienced; cirrhosis & decompensated dis o FDA approved in June 2016 Sofosbuvir/Velpatasvir/Voxilaprevir (NS3/4A) o Pangenotypic FDC o POLARIS 1-4 Studies
11 Sofosbuvir (NS5B) / Velpatasvir (NS5A ) / Voxilaprevir (NS3/4A)

12

13

14

15

16
17 MERCK 2016 PROGRAMME Grazoprevir (NS3A/4A) + Elbasvir (NS5A) + SOF MK-3682/Grazoprevir (NS3A/4A)/Ruzasvir (NS5A)
 + SOF ±")
18 Grazoprevir (NS3A/4A) + Elbasvir (NS5A) + SOF ± RIBA
 + Elbasvir (NS5A) + SOF ±")
19 Genotype 3 Cirrhotics: Grazoprevir (NS3A/4A) + Elbasvir (NS5A) + SOF ± RIBA

20

21 MK-3682/Grazoprevir/Ruzasvir

22
23 Abbvie s DAA 2016 Programme Glecaprevir (NS3A/4A) / Pibrentasvir (NS5A)

24

25 Glecapravir/Pribrentasvir

26 Glecapravir/Pribrentasvir

27
28

29

30

31

32
33 Chronic HCV, DAA s and HCC Italian Study: 3075 pts with chronic hepatitis C infection: Follow-up for mean of days after the start of DAA therapy Cumulative incidence rates of HCC not significantly different: o o o F3 advanced fibrosis (0.23% per person per year) Child-Pugh A cirrhotics (1.64% per person per year) Child-Pugh B cirrhotics (2.92% per person per year) Incidence rates no different from historic control cohorts with similar patients from the same geographic region (Northern Italy) who did not receive antiviral therapy Fibrosis and cirrhosis stage is the driving factor, not oral directacting antiviral agents Severity of HCC did appear to correlate with antiviral therapy over a 540-day follow-up period o 5 (12.2%) pts had portal vein thromboses & 4 (9.7%) had extra-hepatic metastases
 HCC diagnosed at wk 4 in 3 patients, at wk 8 in 3 patients, at wk 12 in 6 patients, from wk 12-23 in 13 patients, and after EOT in 16 pts Multivariate Analysis: SVR12 significant predictor of")
34 Disease Severity in the 41 Patients Who Developed HCC At 12 weeks, HCC more aggressive in pts who did not achieve SVR12 vs pts with SVR vs undetermined response (53.8% vs 33.3% vs 28.6%) HCC diagnosed at wk 4 in 3 patients, at wk 8 in 3 patients, at wk 12 in 6 patients, from wk in 13 patients, and after EOT in 16 pts Multivariate Analysis: SVR12 significant predictor of HCC: HR 0.20; P =.001 Changes in immunologic and molecular microenvironment in liver and in tumor suppression mechanisms, which could allow or even promote the growth of previously undiagnosed microscopic hepatocellular carcinoma foci Romano et al; Abstract 19; November 13, 2016

35

36

37
38 HCV : Late Relapse or Reinfection Systematic review & meta-analysis: 59 studies (>9000 pts) Mono-HCV infected "low-risk" patients; Mono-HCV infected "high-risk" patients : PWUD or prisoners HIV/HCV co-infected patient Overall 5 year recurrence rates Low-risk patients : 0.95% High-risk patients : 10.67% HCV/HIV co-infected patients : 15.02% Increase in reinfection rather than late relapse Prevention campaigns for individuals at high-risk of HCV re-exposure Simmons et al; Clin Infect Dis 2016, Jan 19

39 Grazoprevir/Elbasvir

40
41 Hepatitis B Reactivation : DAA therapy US FDA received 24 unique reports of HBV-R associated with DAA Rx Boxed warning 2 fatal outcomes and 1 liver transplantation HBV-R: Pts were heterogeneous: HCV genotype, DAA received, and baseline HBV viral parameters At baseline: 7 patients had detectable HBV VL, 4 patients had a positive HBsAg and undetectable HBV VL, & 3 patients had negative HBsAg and undetectable HBV VL The remaining cases either did not report these data points, or data were interpretable Despite provider knowledge of baseline HBV status, delay in diagnosis and treatment of HBV-R was noted in 5 cases, with possible delay in 3 others Limitations: Spontaneous reporting system subject to variable data quality and underreporting Unable to estimate incidence of DAA associated HBV-R, and ability to make causal inference is limited Patients with history of HBV require clinical monitoring while on DAA s o Need full HBV serology Bersoff-Matcha et al, LB Abstract 17, AASLD 2016
42 Hepatitis B Reactivation : DAA therapy Meta-analysis 35 studies involving 1121 CHC patients 30 studies were using interferon All studies reported SVR rates, 26 studies reported HBV reactivation, 22 studies reported occurrence of hepatitis due to HBV reactivation Overall SVR rate was 47% in HBV/HCV co-infected patients SVR rate: Interferon (43%) and DAAs (100%); p<0.001 Overall HBV reactivation rate 12.3%: IFN (12.4%) & DAAs (12.2%, p=0.90) Overall incidence of hepatitis due to HBV reactivation 0.3% (0-1.1% in IFN treated) vs % with DAAs, p=0.02 Most cases HBV reactivation occurred during follow-up of IFN treatment (3 wks to 72 months post-treatment) All cases were observed during DAAs treatment (4 to 11 wks during Rx) Wang et al; Abstract 918, AASLD 2016
43 Liver Tx: DAA Therapy and Purgatory MELD: Fact or Fiction? UNOS database: 20,411 HCV waitlist LT candidates: 10,606 candidates 18 months pre-daa: May 2012 to October ,805 candidates in post-daa period: January 2014 to June 2015 Compared to pre-daa period HCV waitlist LT candidates during post-daa : significantly lower rate o Removal due to death (7.4 % to 11.5%, p < 0.01) o Too sick to transplant (7.9% to 11.3%, p < 0.01) Post-DAA HCV waitlist LT candidates had a significantly lower rate of liver transplantation (29.9% to 38.7%, p < 0.01) This should be taken into account in setting of poor donor access Cholankeril et al, Abstract 859, AASLD 2016
44 Alcoholic Liver Disease Alcoholic Cirrhosis Acute alcoholic hepatitis Cirrhosis HCC Fibrosis Steatohepatitis Fatty liver ALD Years
45 STOPAH Trial : Prednisolone or Pentoxifylline for AH Multicenter, double-blind, randomized trial: 1103 pts Prednisolone reduction : 28-day mortality 14% (Pred) vs 19% (PTX) vs 17% (placebo) No outcome improvement : 90 days or 1 yr Prednisone: serious infections 13% vs 7% 37% completely abstinent at 1yr NEJM 2015;372 (17):1619

46

47
48 Liver Transplantation in Acute Alcoholic Hepatitis Multicentre Franco-Belgian Study: 26 pts failed to respond to prednisone (Lille score >0.45. Received LTx, mean of 13 days after stopping steroids Highly selected patients : 8.3% patients with AH, 1 st episode 2.9% of LTx performed Criteria for acceptance for LTx: Needed to be approved by Patient and patient s family 4 groups of physicians caring for patient o Residents/fellows o Addiction specialist o o Hepatologist Liver Tx anaesthetist and surgeon Recidivism: 3 pts (720, 740 and 1140 days post LTx) NEJM 2011;365(19): 1790

49

50 Alcoholic Cirrhosis and Statins Propensity score matched cohort: 2275 pts compensated cirrhosis and 1435 pts with decompensated cirrhosis 25% patients on statins in each group Primary end point: Incidence of death at 15 years Mortality Rates Halved Improved survival in patients with Child-Pugh class A or B cirrhosis, but not in patients with class C Gastroenterology. 2016;150: e3)
51 Alcoholic Cirrhosis and Statins Mortality rates lower in statin users Compensated cirrhosis (86 vs 199 per 1000 person-years) o Adjusted HR 0.45; P <.0001 Decompensated cirrhosis (132 vs 290 per 1000 person-years); o Adjusted HR, 0.55; P <.0001 Risk for decompensation: Secondary end point Lower in statin users (10% vs 25%; adjusted HR 0.31; P <.0001) Statins are thought to have an anti-inflammatory effect on the liver Reduces portal hypertension, a prognostic marker for death Propensity score matching was used to rule out as many confounders Gastroenterology. 2016;150: e3
52 CHOLESTATIC LIVER DISEASE
53 PBC Chronic immune-mediated lymphocytic cholangitis Early diagnosis and initiation of UDCA (13-15 mg/kg/day) o o 66% patients have expected survival equivalent to general population Only a minority will develop cirrhosis Proposed Name change: Primary Biliary Cholangitis Proposed by Dame Sheila Sherlock in 1959! Accepted in 2015 by AASLD, EASL and AGA Can we stratify risk of progression to cirrhosis? On treatment (UDCA) biochemical response at 1 year most robust endpoint to stratify risk of progression and potential need for 2 nd line Rx GLOBE score: UK-PBC risk score:
) 2.266708 * Alb x LLN at 1 year 0.002581 * PLT at 1 year) + 1.")
54 GLOBE score : ( * age at start of UDCA therapy * NL(Bili x ULN) at 1 year)) + ( * NL(ALP x ULN at 1year)) * Alb x LLN at 1 year * PLT at 1 year)

55


56
57

58

59
60 PSC MRCP preferred diagnostic imaging Liver biopsy: Small duct PSC or AIH overlap Test IgG4 at least once UDCA doses 28 mg/kg/day should not be used Better Px: Normalisation of liver biochemistry spontaneously or UDCA o 20 mg/kg/day frequently used in clinical practice Routine stenting after dilatation of dominant stricture not recommended Dominant strictures should be evaluated: Biopsies, brushings & FISH Refer for Liver Transplant when MELD>14 o Increased risk of ischaemic cholangiopathy with DCD organs Annual colonoscopy, preferably chromoendoscopy: PSC + colitis PSC without IBD: colonoscopy every 3-5 years Screening for CCA with cross-sectional imaging and serial CA19-9 every 6-12 months Am J Gastro 2015;110:646

61 Significant dose-dependent reduction of s-alp values during 12 weeks of norudca compared to placebo with the highest effect at 1500mg/day Biochemical response to norudca was independent of UDCA pre-rx & response
62 CIRRHOSIS

63

64

65

66

67 Health Disparities: sub-saharan Africa Burden of liver disease in sub-saharan Africa is substantial Challenges Lack of data to accurately establish disease prevalence Lack of access to health facilities - diagnostic and interventional Access and cost of medications Apply similar programmes to HIV/AIDS to combat liver Disease in ssa - PEPFAR - Global Fund to Fight AIDS, TB and Malaria brought medication at affordable prices to ssa
Special developments in the management of Hepatitis C. Disclosures
 Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany
 Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
RATIONALE FOR INCLUSION IN PA PROGRAM
 RATIONALE FOR INCLUSION IN PA PROGRAM Background Hepatitis C is a viral disease that causes inflammation of the liver that can lead to diminished liver function or liver failure. Most people infected with
RATIONALE FOR INCLUSION IN PA PROGRAM Background Hepatitis C is a viral disease that causes inflammation of the liver that can lead to diminished liver function or liver failure. Most people infected with
Management of Chronic HCV 2017 and Beyond
 Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
Hepatitis C Update: What s New in 2017
 Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
HCV care after cure. This program is supported by educational grants from
 HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
Dr. Siddharth Srivastava
 Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
HCV Infection: EASL Clinical Practice Guidelines Francesco Negro University Hospital Geneva Switzerland
 HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Update on Hepatitis C. Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017
 Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
Hepatitis B and Hepatitis C Virus in non-liver Transplant Recipients. Karim Qumosani MD, FRCPC, ABIM, MdMEd Multi-organ Transplant Unit, London
 Hepatitis B and Hepatitis C Virus in non-liver Transplant Recipients Karim Qumosani MD, FRCPC, ABIM, MdMEd Multi-organ Transplant Unit, London Financial Disclosures Research Grants Merck, Gilead, Abbvie,
Hepatitis B and Hepatitis C Virus in non-liver Transplant Recipients Karim Qumosani MD, FRCPC, ABIM, MdMEd Multi-organ Transplant Unit, London Financial Disclosures Research Grants Merck, Gilead, Abbvie,
Hepatitis C Introduction and Overview
 Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
HEPATITIS C: UPDATE AND MANAGEMENT
 HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
AASLD, Boston, USA, 10 th November 2014 [oral presentation]
![AASLD, Boston, USA, 10 th November 2014 [oral presentation]](/thumbs/89/98795522.jpg "AASLD, Boston, USA, 10 th November 2014 [oral presentation]") Effects of Sustained Virological Response on the of liver transplant, hepatocellular carcinoma, death and re-infection: meta-analysis of 129 studies in 34,563 patients with Hepatitis C infection. Andrew
Effects of Sustained Virological Response on the of liver transplant, hepatocellular carcinoma, death and re-infection: meta-analysis of 129 studies in 34,563 patients with Hepatitis C infection. Andrew
Hepatitis C Policy Discussion
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR
 Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR This program is supported by educational grants from AbbVie, Gilead Sciences, and Merck About These Slides Please feel free to use,
Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR This program is supported by educational grants from AbbVie, Gilead Sciences, and Merck About These Slides Please feel free to use,
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
HCV Therapies: The Last challenges 12th Paris Hepatology Conference 14th January Stefan Zeuzem, MD University Hospital, Frankfurt, Germany
 HCV Therapies: The Last challenges 2th Paris Hepatology Conference 4th January 209 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany Disclosures Advisory boards: AbbVie, Gilead Sciences, Intercept,
HCV Therapies: The Last challenges 2th Paris Hepatology Conference 4th January 209 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany Disclosures Advisory boards: AbbVie, Gilead Sciences, Intercept,
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Treatment of Unique Populations Raymond T. Chung, MD
 Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
Case 1 AND. Treatment of HCV: Pre- vs Post- Transplant. 58 yo male, ESRD/diabetic nephropathy, HD for 3 weeks
 Treatment of HCV: Pre- vs Post- Transplant Roy D. Bloom MD Professor of Medicine University of Pennsylvania Roy D. Bloom MD Professor of Medicine Medical Director, Kidney Transplant Program University
Treatment of HCV: Pre- vs Post- Transplant Roy D. Bloom MD Professor of Medicine University of Pennsylvania Roy D. Bloom MD Professor of Medicine Medical Director, Kidney Transplant Program University
TREATMENT OF GENOTYPE 2
 Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
47 th Annual Meeting AISF
 47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
Staging liver disease
 Staging liver disease A hepatologist, ID doc, primary care provider, and insurance executive go to a bar Slide 1 of 44 Staging liver disease A hepatologist, ID doc, primary care provider, and insurance
Staging liver disease A hepatologist, ID doc, primary care provider, and insurance executive go to a bar Slide 1 of 44 Staging liver disease A hepatologist, ID doc, primary care provider, and insurance
ACG Clinical Guideline: Primary Sclerosing Cholangitis
 ACG Clinical Guideline: Primary Sclerosing Cholangitis Keith D. Lindor, MD, FACG 1, Kris V. Kowdley, MD, FACG 2, and M. Edwyn Harrison, MD 3 1 College of Health Solutions, Arizona State University, Phoenix,
ACG Clinical Guideline: Primary Sclerosing Cholangitis Keith D. Lindor, MD, FACG 1, Kris V. Kowdley, MD, FACG 2, and M. Edwyn Harrison, MD 3 1 College of Health Solutions, Arizona State University, Phoenix,
HCV Resistance Clinical Aspects. Sanjay Bhagani Royal Free Hospital/UCL London
 HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
Current trends in CHC 1st genotype treatment
 Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
Hepatitis C in Special Populations
 Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano. Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future
 Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future DAA classes and subclasses Drug Class Subclass Potency
Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future DAA classes and subclasses Drug Class Subclass Potency
VIRAL LIVER DISEASE. OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015
 VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France
 How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE
 THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE MARIA SCHINA CONSULTANT PHYSICIAN INTERNAL MEDICINE AND HEPATOLOGY ATHENS EUROCLINIC 10 th INTERNATIONAL CONGRESS OF
THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE MARIA SCHINA CONSULTANT PHYSICIAN INTERNAL MEDICINE AND HEPATOLOGY ATHENS EUROCLINIC 10 th INTERNATIONAL CONGRESS OF
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Current HCV Treatment by Genotype
 Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Antiviral treatment in HCV cirrhotic patients on waiting list
 Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Universal HCV treatment: Strategies for simplification
 Universal HCV treatment: Strategies for simplification PARIS HEPATOLOGY CONFERENCE 3 January 217 Tarik Asselah (MD, PhD) Hepatology & Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures
Universal HCV treatment: Strategies for simplification PARIS HEPATOLOGY CONFERENCE 3 January 217 Tarik Asselah (MD, PhD) Hepatology & Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy
 Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran
 A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran Teheran, 22 July 2016 Massimo Colombo Treatment of HCV genotype 1 & 4 with DAAs
A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran Teheran, 22 July 2016 Massimo Colombo Treatment of HCV genotype 1 & 4 with DAAs
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA. Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona
 Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
New York State HCV Provider Webinar Series. Side Effects of Therapy
 New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related
New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE?
 IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity. Cody A. Chastain, MD
 Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Hepatitis C in Disclosures
 Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Impatto della clearance virale e rischio di carcinoma epatocellulare
 EPATITE CRONICA DA HCV: Impatto della clearance virale e rischio di carcinoma epatocellulare Rodolfo Sacco, M.D., PhD Direttore U.O.C. Gastroenterologia ed Endoscopia Digestiva A.O.U. Ospedali Riuniti"
EPATITE CRONICA DA HCV: Impatto della clearance virale e rischio di carcinoma epatocellulare Rodolfo Sacco, M.D., PhD Direttore U.O.C. Gastroenterologia ed Endoscopia Digestiva A.O.U. Ospedali Riuniti"
Hepatitis C - results in real life
 Hepatitis C - results in real life Robert Flisiak Department of Infectious Diseases and Hepatology Medical University of Białystok, Poland 10th PHC Paris, 30-31 January 2017 Disclosures Advisor and/or
Hepatitis C - results in real life Robert Flisiak Department of Infectious Diseases and Hepatology Medical University of Białystok, Poland 10th PHC Paris, 30-31 January 2017 Disclosures Advisor and/or
3 Workshop on HCV THERAPY ADVANCES New Antivirals in Clinical Practice
 3 Workshop on HCV THERAPY ADVANCES New Antivirals in Clinical Practice Rome, 13 December 2013 Management and monitoring of HCC in the future era of DAA s Prof. Massimo Colombo Chairman Department of Liver,
3 Workshop on HCV THERAPY ADVANCES New Antivirals in Clinical Practice Rome, 13 December 2013 Management and monitoring of HCC in the future era of DAA s Prof. Massimo Colombo Chairman Department of Liver,
Rome, February nd Riunione Annuale AISF th AISF ANNUAL MEETING
 Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline
 PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
Future strategies with new DAAs
 Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
New York State HCV Provider Webinar Series. Side Effects of Therapy and Drug-Drug Interactions
 New York State HCV Provider Webinar Series Side Effects of Therapy and Drug-Drug Interactions Case Presentation Case 56 year-old lady with Genotype 1A Hepatitis C, Treatment-naive Noninvasive fibrosis
New York State HCV Provider Webinar Series Side Effects of Therapy and Drug-Drug Interactions Case Presentation Case 56 year-old lady with Genotype 1A Hepatitis C, Treatment-naive Noninvasive fibrosis
What Should We Do With Difficult to Treat HCV Populations?
 What Should We Do With Difficult to Treat HCV Populations? Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah
What Should We Do With Difficult to Treat HCV Populations? Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah
Description of Antivirals for Hepatitis C. LCDR Dwayne David, PharmD, BCPS, NCPS Cherokee Nation Infectious Diseases
 Description of Antivirals for Hepatitis C LCDR Dwayne David, PharmD, BCPS, NCPS Cherokee Nation Infectious Diseases Dwayne-David@cherokee.org Objectives Compare the different classes of direct-acting antiviral
Description of Antivirals for Hepatitis C LCDR Dwayne David, PharmD, BCPS, NCPS Cherokee Nation Infectious Diseases Dwayne-David@cherokee.org Objectives Compare the different classes of direct-acting antiviral
Hepatitis C Difficult to Treat. Population. Disclosures
 Hepatitis C Difficult to Treat Populations Paul Y Kwo MD Professor of Medicine Director of Hepatology Stanford University School of Medicine 75 Welch Road #21 Palo Alto, CA 9434 Disclosures Advisory Board
Hepatitis C Difficult to Treat Populations Paul Y Kwo MD Professor of Medicine Director of Hepatology Stanford University School of Medicine 75 Welch Road #21 Palo Alto, CA 9434 Disclosures Advisory Board
Liver transplant: what is left after the viruses
 Riunione Monotematica A.I.S.F. 2016 The Future of Liver Disease: Beyond HCV is there a Role for Hepatologist? Milan 15 th 2016 Liver transplant: what is left after the viruses Stefano Ginanni Corradini
Riunione Monotematica A.I.S.F. 2016 The Future of Liver Disease: Beyond HCV is there a Role for Hepatologist? Milan 15 th 2016 Liver transplant: what is left after the viruses Stefano Ginanni Corradini
HIV and Hepatitis C Have we finally slayed the beast?
 HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
Liver Pathology and the Clinician in 2015: At the Crossroads. Thomas D. Schiano, M.D. Mount Sinai Medical Center New York, New York
 Liver Pathology and the Clinician in 2015: At the Crossroads Thomas D. Schiano, M.D. Mount Sinai Medical Center New York, New York DISCLOSURES Consultant for: Salix Merck Gilead BMS Synageva Research funding:
Liver Pathology and the Clinician in 2015: At the Crossroads Thomas D. Schiano, M.D. Mount Sinai Medical Center New York, New York DISCLOSURES Consultant for: Salix Merck Gilead BMS Synageva Research funding:
Is Treatment cost effective HCV and Organ Transplantation
 Is Treatment cost effective HCV and Organ Transplantation Dr Kosh Agarwal Institute of Liver Studies King s College Hospital Barcelona 2016 Disclosures: BoJo Pharma support: AbbVie/Achillion/ Astellas/
Is Treatment cost effective HCV and Organ Transplantation Dr Kosh Agarwal Institute of Liver Studies King s College Hospital Barcelona 2016 Disclosures: BoJo Pharma support: AbbVie/Achillion/ Astellas/
Viva La Revolución: Options to Combat Hepatitis C
 Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Treating now vs. post transplant
 Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Hepatitis C ew Medications, New Hope and New. V. Opportunities for Primary Care. Outline. HCV Disease Outcomes in the US 9/21/2016
 Hepatitis C ew Medications, New Hope and New Opportunities for Primary Care Primary Care Principles and Practice October 14, 2016 Disclosures: Grant support Gilead Sciences, Inc Quality improvement Systematized
Hepatitis C ew Medications, New Hope and New Opportunities for Primary Care Primary Care Principles and Practice October 14, 2016 Disclosures: Grant support Gilead Sciences, Inc Quality improvement Systematized
New York State HCV Provider Webinar Series. Side Effects of Therapy and Drug-Drug Interactions
 New York State HCV Provider Webinar Series Side Effects of Therapy and Drug-Drug Interactions Case Presentation Case 56 year-old lady with Genotype 1A Hepatitis C, Treatment-naive Noninvasive fibrosis
New York State HCV Provider Webinar Series Side Effects of Therapy and Drug-Drug Interactions Case Presentation Case 56 year-old lady with Genotype 1A Hepatitis C, Treatment-naive Noninvasive fibrosis
Treating Hepatitis C Virus (HCV) Infection
 Infection") Slide 1 of 42 Treating Hepatitis C Virus (HCV) Infection Susanna Naggie, MD, MHS Associate Professor of Medicine Duke Clinical Research Institute Durham, North Carolina Slide 3 of 42 Learning Objectives
Slide 1 of 42 Treating Hepatitis C Virus (HCV) Infection Susanna Naggie, MD, MHS Associate Professor of Medicine Duke Clinical Research Institute Durham, North Carolina Slide 3 of 42 Learning Objectives
National Clinical Guidelines for the treatment of HCV in adults. Version 3
 National Clinical Guidelines for the treatment of HCV in adults Version 3 January 2017 Sponsors and Authorship The guidelines have been authored on behalf of the viral hepatitis clinical leads and MCN
National Clinical Guidelines for the treatment of HCV in adults Version 3 January 2017 Sponsors and Authorship The guidelines have been authored on behalf of the viral hepatitis clinical leads and MCN
Update in hepatitis C virus infection
 Update in hepatitis C virus infection Eoin Feeney Consultant in Infectious Diseases St. Vincent s University Hospital Overview Natural history Diagnosis, screening, staging Management Barriers going forward
Update in hepatitis C virus infection Eoin Feeney Consultant in Infectious Diseases St. Vincent s University Hospital Overview Natural history Diagnosis, screening, staging Management Barriers going forward
HCV in 2017: New Therapies and New Opportunities. Presentation prepared by: Date prepared: OBJECTIVES
 Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
HCV Screening, Management, and Treatment Guidelines
 HCV ECHO WESTERN STATES HCV Screening, Management, and Treatment Guidelines Paulina Deming, PharmD, PhC Associate Professor of Pharmacy-College of Pharmacy Project ECHO University of New Mexico Health
HCV ECHO WESTERN STATES HCV Screening, Management, and Treatment Guidelines Paulina Deming, PharmD, PhC Associate Professor of Pharmacy-College of Pharmacy Project ECHO University of New Mexico Health
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Disclosures. Advanced HCV management. Overview. Renal failure 1/10/2018. Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH
 Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
ANTIVIRAL THERAPY FOR HCV. Alfredo Alberti
 CLINICAL IMPACT OF SVR AFTER ANTIVIRAL THERAPY FOR HCV Alfredo Alberti Department of Histology,Microbiology and Medical Biotechnologies Molecular Hepatology Unit Venetian Institute of Molecular Medicine
CLINICAL IMPACT OF SVR AFTER ANTIVIRAL THERAPY FOR HCV Alfredo Alberti Department of Histology,Microbiology and Medical Biotechnologies Molecular Hepatology Unit Venetian Institute of Molecular Medicine
The future of liver transplantation for viral hepatitis
 The future of liver transplantation for viral hepatitis François Durand Hepatology & Liver Intensive Care Hospital Beaujon, Clichy University Paris Diderot France Liver transplantation in France 2013:
The future of liver transplantation for viral hepatitis François Durand Hepatology & Liver Intensive Care Hospital Beaujon, Clichy University Paris Diderot France Liver transplantation in France 2013:
Treatment of Patients with HCV and HIV
 Treatment of Patients with HCV and HIV BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY Four Questions Is HIV/HCV
Treatment of Patients with HCV and HIV BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY Four Questions Is HIV/HCV
Hepatitis C Genotypes
 9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
HCV Treatment in 2016
 HCV Treatment in 2016 Hugo E. Vargas, MD Professor of Medicine Mayo College of Medicine Medical Director, Clinical Trials Office Vice Chair, Department of Research Educational Goals Caveats: Cannot cover
HCV Treatment in 2016 Hugo E. Vargas, MD Professor of Medicine Mayo College of Medicine Medical Director, Clinical Trials Office Vice Chair, Department of Research Educational Goals Caveats: Cannot cover
Hepatitis C Policy Discussion
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Outline. HCV Disease Outcomes in the US. Hepatitis C: The New Landscape 5/24/16. Advances in Internal Medicine May 24, I have no disclosures
 5/24/16 Hepatitis C: The New Landscape Advances in Internal Medicine May 24, 2016 I have no disclosures Rena K. Fo, MD Professor of Clinical Medicine, UCSF Outline I. Current HCV outcomes in the US II.
5/24/16 Hepatitis C: The New Landscape Advances in Internal Medicine May 24, 2016 I have no disclosures Rena K. Fo, MD Professor of Clinical Medicine, UCSF Outline I. Current HCV outcomes in the US II.
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C Second Generation Antivirals Page 1 of 32 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Hepatitis C Second Generation Antivirals Page 1 of 32 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Prior Authorization Guideline
 Prior Authorization Guideline Guideline Name Sovaldi (sofosbuvir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/8/2014 1. Indications Drug Name: Sovaldi
Prior Authorization Guideline Guideline Name Sovaldi (sofosbuvir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/8/2014 1. Indications Drug Name: Sovaldi
Management of HCV in Decompensated Liver Disease
 Management of HCV in Decompensated Liver Disease Michael P. Manns Hannover Medical School (MHH) Department of Gastroenterology, Hepatology and Endocrinology Helmholtz Center for Infection Research (HZI),
Management of HCV in Decompensated Liver Disease Michael P. Manns Hannover Medical School (MHH) Department of Gastroenterology, Hepatology and Endocrinology Helmholtz Center for Infection Research (HZI),
HCV Management in Decompensated Cirrhosis: Current Therapies
 Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Management of HIV/HCV Coinfection. Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY
 Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College
 Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Meet the Professor: HIV/HCV Coinfection
 Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Worldwide Causes of HCC
 Approach to HCV Treatment in Patients with HCC Mark W. Russo, MD, MPH, FACG Carolinas HealthCare System Charlotte Worldwide Causes of HCC 60% 50% 40% 30% 20% 10% 0% 54% 31% 15% Hepatitis B Hepatitis C
Approach to HCV Treatment in Patients with HCC Mark W. Russo, MD, MPH, FACG Carolinas HealthCare System Charlotte Worldwide Causes of HCC 60% 50% 40% 30% 20% 10% 0% 54% 31% 15% Hepatitis B Hepatitis C
Current HCV Treatment by Genotype Ira M. Jacobson, MD
 Current HCV Treatment by Genotype Ira M. Jacobson, MD Director of Hepatology NYU School of Medicine Objectives To understand the prevalence of HCV and distribution of HCV genotypes Describe the HCV lifecycle
Current HCV Treatment by Genotype Ira M. Jacobson, MD Director of Hepatology NYU School of Medicine Objectives To understand the prevalence of HCV and distribution of HCV genotypes Describe the HCV lifecycle
What is the Optimized Treatment Duration? To Overtreat versus Undertreat. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
A treatment revolution: current management for chronic HCV
 A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
HCV elimination : lessons from Scotland
 HCV elimination : lessons from Scotland Sharon Hutchinson Glasgow Caledonian University / Health Protection Scotland BHIVA Hepatology Highlights, Edinburgh, 17 th April 2018 Disclosures Honoraria from
HCV elimination : lessons from Scotland Sharon Hutchinson Glasgow Caledonian University / Health Protection Scotland BHIVA Hepatology Highlights, Edinburgh, 17 th April 2018 Disclosures Honoraria from
Hepatitis C Resistance Associated Variants (RAVs)
") Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C: New Antivirals in the Liver Transplant Setting. Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona
 Hepatitis C: New Antivirals in the Liver Transplant Setting Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Patient survival Hepatitis C and Liver Transplantation Years after transplantation
Hepatitis C: New Antivirals in the Liver Transplant Setting Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Patient survival Hepatitis C and Liver Transplantation Years after transplantation
Sovaldi (sofosbuvir)
") Market DC Sovaldi (sofosbuvir) Override(s) Prior Authorization Quantity Limit Approval Duration Based on Genotype, Treatment status, Cirrhosis status, or Ribavirin Eligibility status **IN, SC, WA Medicaid
Market DC Sovaldi (sofosbuvir) Override(s) Prior Authorization Quantity Limit Approval Duration Based on Genotype, Treatment status, Cirrhosis status, or Ribavirin Eligibility status **IN, SC, WA Medicaid
Pediatric PSC A children s tale
 Pediatric PSC A children s tale September 8 th PSC Partners seeking a cure Tamir Miloh Assistant Professor Pediatric Hepatology Mount Sinai Hospital, NY Incidence Primary Sclerosing Cholangitis (PSC) ;
Pediatric PSC A children s tale September 8 th PSC Partners seeking a cure Tamir Miloh Assistant Professor Pediatric Hepatology Mount Sinai Hospital, NY Incidence Primary Sclerosing Cholangitis (PSC) ;
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C Second Generation Antivirals Page 1 of 30 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Hepatitis C Second Generation Antivirals Page 1 of 30 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Treatment of Hepatitis C Recurrence after Liver Transplantation. Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona
 Treatment of Hepatitis C Recurrence after Liver Transplantation Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Agenda 1. Introduction 2. Treatment options for hepatitis C recurrence after transplantation
Treatment of Hepatitis C Recurrence after Liver Transplantation Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Agenda 1. Introduction 2. Treatment options for hepatitis C recurrence after transplantation
Updates in the Treatment of HCV
 Updates in the Treatment of HCV Misty Miller, Pharm.D., BCPS, AAHIVP Associate Professor University of Oklahoma College of Pharmacy September 21 st, 2018 Overview HCV Review and Definitions HCV Genotypes
Updates in the Treatment of HCV Misty Miller, Pharm.D., BCPS, AAHIVP Associate Professor University of Oklahoma College of Pharmacy September 21 st, 2018 Overview HCV Review and Definitions HCV Genotypes