Hepatitis C Introduction and Overview
|
|
|
- Darleen White
- 5 years ago
- Views:
Transcription
1 Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama Financial Relationships with Commercial Entities Dr Saag has received research grants and support awarded to his institution from and served as scientific advisor to Merck, Proteus, ViiV Healthcare, and Gilead Sciences, Inc. (Updated 09/18/18) Slide 2 of 54 Learning Objectives After attending this presentation, learners will be able to: List the genotypes of HCV and how they relate to treatment effects Stage HCV infection and describe why it is important to accurately stage Recall the clinical presentation of advanced liver disease (cirrhosis) Describe emerging treatments of HCV and how the changing landscape will impact treatment decisions in the near future List the new changes to the HCV Guidelines (Sept 2018) Slide 3 of 54
2 ARS Question #1: Which test most accurately stage liver fibrosis? 1. Fibroscan 2. Fibrosure 3. APRI 4. Liver biopsy 5. Liver percussion Slide 4 of 54 ARS Question #2: What percent of persons with chronic HCV infection develop cirrhosis over 30 years? % 2. 5% 20% 3. 20% 50% 4. 50% 75% 5. >75% Slide 5 of 54 ARS Question #3: What is the most common genotype of HCV in the United States? 1. Genotype 1 2. Genotype 2 3. Genotype 3 4. Genotype 4 5. Genotype 5 6 Slide 6 of 54

3 Objectives Epidemiology Natural History Staging Genome and Drug Targets Viral Kinetics With Therapy Current Treatments What Does SVR Really Mean? Slide 7 of 54 Objectives Epidemiology Natural History Staging Genome and Drug Targets Viral Kinetics With Therapy Current Treatments What Does SVR Really Mean? Slide 8 of 54 HCV Research Timeline AIDS 1982 HIV 1984 AZT 1987 Moradpour Nature Reviews 2007; 5: Slide 9 of 54

; genotypes 2, 4, and 6 (22.8%); genotype 5 <1%.")

4 HCV Worldwide million infected Highest Asia & Africa Egypt > 15% USA 1.6% 3-4 million infected Slide 10 of 54 Worldwide prevalence of each HCV genotype by GBD HCV genotype 1 (83.4 million cases: 46.2%)- one-third of which are in East Asia. Genotype 3 (54.3 million: 30.1%); genotypes 2, 4, and 6 (22.8%); genotype 5 <1%. While genotypes 1 and 3 dominate in most countries irrespective of economic Status: largest proportions of genotypes 4 and 5 are in lower-income countries. Slide 11 of 54 The Treatment Cascade of HCV infection in the US: ~3 4 million persons infected 100% 100% 75% 50% 50% 38% 23% 25% 11% 6% 0% Slide 12 of 54 Adapted from Holmberg et al. NEJM 2013
5 Future Burden of Hepatitis C Related Morbidity and Mortality in the US Markov model of health outcomes Of 2.7 M HCV infected persons in primary care 1.47 M will develop cirrhosis 350,000 will develop liver cancer 897,000 will die from HCV-related complications Number Deaths DCC HCC Rein D, et al. Dig Liver Dis Slide 13 of 54 Objectives Epidemiology Natural History Staging Genome and Drug Targets Viral Kinetics With Therapy Current Treatments What Does SVR Really Mean? Slide 14 of 54 Slide 15 of 70 Natural History of HCV Infection Time (yrs) ~15% ~85% Resolved Exposure (Acute Phase) ~80% Stable 5-year survival in patients with HCC is <5%* Chronic ~75% Slowly Progressive ~ 20-year progression rate may be accelerated with HIV, HBV, alcohol, and steatosis 1,2 ~20% Cirrhosis ~6%/yr ESLD ESLD: end-stage liver disease ~3%-4%/yr HCC Transplant/Death ~4%/yr Slide 15 of 54 *NIH Consens Statement. June 10-12, 2002;19(3):1-46. NIH Consens Statement. March 24-26, 1997;15(3): Di Bisceglie AM. Hepatology. 2000;31(4): Bialek SR, Terrault NA. Clin Liver Dis. 2006;10(4):



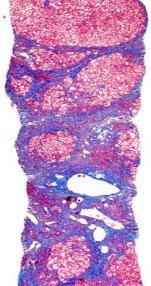
6 Objectives Epidemiology Natural History Staging Genome and Drug Targets Viral Kinetics With Therapy Current Treatments What Does SVR Really Mean? Slide 16 of 54 Fibrosis/Cirrhosis Slide 17 of 54 Objectives Epidemiology Natural History Staging Genome and Drug Targets Viral Kinetics With Therapy Current Treatments What Does SVR Really Mean? Slide 22 of 54

7 Potential Therapeutic Targets in the HCV Replication Cycle Transport and release Translation Fusion and uncoating HCV RNA RNA replication Viral assembly NS5A inhibitors NS5B polymerase inhibitors Polyprotein processing NS3/4A protease inhibitors NS2 NS4B CypA NS3 NS5B NS5A NS4B NS2 NS3 NS5A NS5B HCV NS proteins NS5A inhibitors Adapted from slide courtesy Ray Chung Slide 23 of 54 PROTEASE INHIBITORS NS5A INHIBITORS NUCLEOSIDE INHIBITORS Non-NUCLEOSIDE INHIBITORS Slide 24 of 54 Suffixes Matter! PREVIR (Protease / NS3-4a) ASVIR (NS5a) BUVIR (NS5b) Slide 25 of 54

8 Agents and Regimens: Fall 2017 NS3 NS5A Antiviral Non-Nuc NS5B Nuc NS5B Ledipasvir/sofosbuvir FDC Paritaprevir/r/ombitasvir FDC + dasabuvir Simeprevir + sofosbuvir Glecaprevir / pibrentasvir FDC Sofosbuvir + daclatasvir Elbasvir/grazoprevir FDC Velpatasvir/sofosbuvir FDC Velpat/ Sof / voxilaprevir FDC Slide 26 of 54 Objectives Epidemiology Natural History Staging Genome and Drug Targets Viral Kinetics With Therapy Current Treatments What Does SVR Really Mean? Slide 27 of 54 On Treatment Viral Kinetics 2 log decline LOD Slide 28 of 54

9 Objectives Epidemiology Natural History Staging Genome and Drug Targets Viral Kinetics With Therapy Current Treatments What Does SVR Really Mean? Slide 29 of 54 Chronic HCV prior SOC SVR, % Slide 30 of 54 Pegylated IFN + RBV weeks Significant AEs Response > GT 2/3 Fried MW, NEJM 2002 Manns MP, Lancet 2001 Antiviral HCV treatments (FDA-approved as of September, 2017) Monotherapies IFN-2a IFN-2b PEG-IFN 2a PEG-IFN 2b IFN-2a + Ribavirin IFN-2b + Ribavirin PEG-IFN 2a + Ribavirin* PEG-IFN 2b + Ribavirin PEG-IFN + ribavirin plus either: Boceprevir (GT1) Telaprevir (GT1) Simeprevir (GT1) In combination with other agents: Sofosbuvir Combination Therapies Elbasvir + Grazoprevir (GT 1, 4) Ledipasvir + Sofosbuvir (FDC, GT1,4,5,6) Daclatasvir + Sofosbuvir (GT1,3)* Simeprevir + Sofosbuvir (GT1) Paritaprevir / ritonavir / ombitasvir (FDC) + dasabuvir (GT1) Paritaprevir / ritonavir/ ombitasvir (FDC) (GT4) Pangenotypic Regimens (GT 1 6 ) Velpatasvir / Sofosbuvir FDC Voxilaprevir / Velpatasvir / Sofosbuvir FDC Glecaprevir / Pibrentasvir FDC Slide 31 of 54




10 Slide 32 of 70 Sofosbuvir plus Daclatasvir for GT1 n= No documented virologic failures. All failures due to missing sample/lost to follow-up or re-infection. Slide 32 of 54 Slide 33 of 70 Slide 33 of 54 Predictors of relapse to sofosbuvir-based regimens RB SO V F 12 week FISSION POSITRON FUSION VALENCE n=285 RBV SOF 24 week VALENCE n=247 GT4 GT3 4% 10% GT2 9% PE RB G SO V 12 week F ATOMIC NEUTRINO n=339 Who will do poorly with currentlyavailable SOF-based regimens? GT1 77% Slide 34 of 54 Foster et al. EASL 2014 Abstract 66



11 Predictors of relapse to sofosbuvir-based regimens RB SO V F 12 week FISSION POSITRON FUSION VALENCE n=285 PE RB G SO V F 12 week ATOMIC NEUTRINO n=339 RBV SOF 24 week VALENCE n=247 Who will do poorly with currentlyavailable SOF-based regimens? Slide 35 of 54 Foster et al. EASL 2014 Abstract 66 Predictors of relapse to sofosbuvir-based regimens RB SO V 12 Fweek FISSION POSITRON FUSION VALENCE n=285 RBV SOF 24 week VALENCE n=247 PE RB G SO V F 12 week ATOMIC NEUTRINO n=339 Who will do poorly with currentlyavailable SOF-based regimens? Six factors associated with relapse: Treatment-experienced IL28B non-cc Male sex Weight > 75 kg Cirrhosis High viral load >800,000 IU/mL Slide 36 of 54 Foster et al. EASL 2014 Abstract 66 Updated Guidelines Slide 37 of 54
12 Slide 38 of 70 ARS Question #4: Which of the following statements is true of FDA approval of glecaprevir/pibrentasvir? 1. It is an 8 week regimen only in patients without cirrhosis 2. It is a 12 week regimen regardless of presence of cirrhosis 3. It is an 8 week regimen only in treatment naïve patients 4. It is a 16 week regimen in patients with prior treatment experience to DAA 5. It is a single daily dosed pill Slide 38 of 54 Glecaprevir (NS3)/pibrentasvir (NS5A) Slide 39 of 70 Co-formulated 3 pills once daily Pangenotypic Next generation Active vs NS3 RAS at 80, 155, 168 and NS5A RAS at 28, Q30, 31, 93 A30K associated with failure in GT3 infection Negligible renal excretion Contains a protease inhibitor Has interaction with acid suppressing meds Slide 39 of 54 Glecaprevir/pibrentasvir: no cirrhosis 8 (N=828) vs 12 (N=1076) weeks TN and TE PEG, RBV, SOF No DAA otherwise Relapse <1% Tx emergent RAS TN GT3 may need 12W TE GT3 may need 16 weeks weeks 12 weeks All GT 1 GT 2 GT 3 GT 4 GT 5 GT 6 Slide 40 of 54 Puoti et al. EASL 2017

13 ARS Question #5: Which of the following statements is true of FDA approval of sofosbuvir/velpatasvir/voxilaprevir? 1. It is an 8 week regimen only in patients without cirrhosis 2. It is a 12 week regimen regardless of presence of cirrhosis 3. It is an 8 week regimen regardless of prior treatment experience to DAA 4. It is approved for all genotypes across all DAA failures Slide 41 of 54 Sofosbuvir/velpatasvir/voxilaprevir: 8 vs 12 weeks of SOF/VEL POLARIS 2 GT 1-6 w/ and w/o cirrhosis POLARIS 3 GT 3 with cirrhosis 2 relapses Pooled analysis N=611 8 weeks of therapy failed non-inferiority in POLARIS-2 3.8% relapse 14 GT1a (regardless of cirrhosis) Slide 42 of GT 1a GT 1b GT 2 GT 3 GT 4 GT 5 GT 6 Roberts et al. EASL 2017; Jacobson et al. Gastro 2017 Sofosbuvir/velpatasvir/voxilaprevir NS5A Inhibitor DAA -Experienced POLARIS 1 GT 1-6 (30% GT3) 12 weeks of therapy vs placebo Including compensated cirrhosis (46%) 2.2% relapse 4 GT 3 relapse all 3a and ¾ had BL NS5A RAS No treatment emergent RAS all VF had cirrhosis (6 R, 1 VBT) Slide 43 of 54 Bourliere et al. NEJM 2017
14 Does Failure = Resistance? Slide 44 of 54 Key HCV Resistance Concepts HCV resistance associated substitutions (RASs) can be present without drug exposure HCV RASs impacts treatment responses in specific situation HCV is resistance is NOT absolute Patient characteristics are just (if not more) important than RASs Future regimens appear to obviate the need for most resistance testing Slide 45 of 54 Resistance Characteristics of HCV Antiviral Classes Class NS3 Protease Inhibitors Antiviral Potency +++ to ++++ Genotype Activity 1, 4 (± 2, 3, 6) Resistance Barrier Low to High FDA Approvals Simeprevir (2013) Paritaprevir (2014) Grazoprevir (2016) Voxilaprevir (2017) Glecaprevir (2017) NS5B Nucleotide Very High Sofosbuvir (2013) NS5B Nonnucleoside NS5A Inhibitors ++++ *anticipated US FDA approvals ++ 1 Low Dasabuvir (2014) 1, 4, 6 (± 2, 3) Low To High Ledipasvir (2014) Daclatasvir (2015) Ombitasvir (2014) Elbasvir (2016) Velpatasvir (2016) Pibrentasvir (2017) Slide 46 of 54

15 Broad Cross-Resistance With Early Generation NS5As Fold Change Genotype 1a Genotype 1b M28T Q30R L31M/V Y93H/N L31V Y93H/N Ledipasvir 20x > 100x Ombitasvir > 1000x > 100x Daclatasvir > 100x > 1000x Elbasvir 20x > 100x > 100x/ > 100x > 1000x/ > 10,000 < 3x > 10,000x/ > 100x > 10,000x > 100x/ > 1000x Velpatasvir < 10x < 3x 20x/50x > 1000x/ > 10,000x > 10x > 1000x/ > 100x > 1000x > 100x/ > 1000x > 100x/-- < 10x 20x/50x < 10x 20x/50x < 10x > 100x/-- < 3x < 3x/-- Pibrentasvir < 3x < 3x < 3x < 10x/< 10x < 3x < 3x/< 3x Ruzasvir < 10x < 10x < 10x < 10x < 10x < 10x Slide 47 of 54 Objectives Epidemiology Natural History Staging Genome and Drug Targets Viral Kinetics With Therapy Current Treatments What Does SVR Really Mean? Slide 48 of 54 Long-Term Follow-Up of SOF Phase 3 Studies 78/78 52/52 88/88 37/37 84/84 185/185 1/1 Median time to follow-up: 170 days (~ 24 weeks) after SVR24 Of 480 patients with SVR24 from phase 3 trials, 435 (91%) and 90 (19%) had post-treatment week 48 and 72 data, respectively Slide 49 of 54 Cheng W, et al. EASL P1112.
:370-378. doi:10.1001/jama.2012.")
 achieved SVR Slide 51 of 54 van der Meer AJ, et al. 308(24):2584 2593.")
16 JAMA. 2012;308(4): doi: /jama Slide 50 of 54 Clinical Benefits of SVR: Liver Failure, HCC Hepatocellular Carcinoma Liver Failure Hepatocellular Carcinoma (%) Liver Failure (%) Time, y Time, y 530 Europeans followed for a median 8.4 years after HCV treatment 192 (36%) achieved SVR Slide 51 of 54 van der Meer AJ, et al. JAMA. 2012;308(24): Effects of SVR on the risk of liver transplant, hepatocellular carcinoma, death and re-infection: meta analysis, 129 studies, 34,563 patients 5-year risk of death (all-cause) by SVR 5-year risk of hepatocellular carcinoma by SVR Gen 18 stud n=29,269 Avg. FU=4.6 years Cirr 9 stud n=2,734 Avg. FU=6.6 years HIV/HCV: 5 stud n=2,560 Avg. FU=5.1 years General: 21 stud n=12,496 Avg. FU=6.1 years Cirrhotic: 18 stud HIV/HCV: 3 studies n=4,987 n=2,085 Avg. FU=6.6 years Avg. FU=4.7 years Slide 52 of 54 Hill AASLD 2014

17 Slide 53 of 70 Slide 53 of 54 Question-and-Answer Remember to raise your hand and wait until you have the microphone before you ask your question we are recording! Slide 54 of 54 Slide 54 of 54
Hepatitis C Resistance Associated Variants (RAVs)
") Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV?
 Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Management of HCV in Prior Treatment Failure
 Management of HCV in Prior Treatment Failure Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending this presentation, learners
Management of HCV in Prior Treatment Failure Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending this presentation, learners
Treating Hepatitis C Virus (HCV) Infection
 Infection") Slide 1 of 42 Treating Hepatitis C Virus (HCV) Infection Susanna Naggie, MD, MHS Associate Professor of Medicine Duke Clinical Research Institute Durham, North Carolina Slide 3 of 42 Learning Objectives
Slide 1 of 42 Treating Hepatitis C Virus (HCV) Infection Susanna Naggie, MD, MHS Associate Professor of Medicine Duke Clinical Research Institute Durham, North Carolina Slide 3 of 42 Learning Objectives
Hepatitis C Update: What s New in 2017
 Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
HEPATITIS C: UPDATE AND MANAGEMENT
 HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
Viva La Revolución: Options to Combat Hepatitis C
 Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York
 Newly Approved Hepatitis C Virus Drugs: Approach to Initial Therapy Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York Learning Objectives After attending this presentation,
Newly Approved Hepatitis C Virus Drugs: Approach to Initial Therapy Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York Learning Objectives After attending this presentation,
Updates on the AASLD/IDSA HCV Guidance
 Updates on the AASLD/IDSA HCV Guidance Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University School of Medicine Durham, North Carolina Learning Objectives After attending this presentation,
Updates on the AASLD/IDSA HCV Guidance Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University School of Medicine Durham, North Carolina Learning Objectives After attending this presentation,
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD
 Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD") Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
HCV Resistance Clinical Aspects. Sanjay Bhagani Royal Free Hospital/UCL London
 HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
Hepatitis C in 2018: From Evolution to Revolution
 Hepatitis C in 218: From Evolution to Revolution Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Director, Viral Hepatitis Clinic Massachusetts General Hospital Boston, Massachusetts
Hepatitis C in 218: From Evolution to Revolution Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Director, Viral Hepatitis Clinic Massachusetts General Hospital Boston, Massachusetts
Hepatitis C in Disclosures
 Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
Current trends in CHC 1st genotype treatment
 Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
HCV therapy : Clinical case
 HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
Disclosures. Advanced HCV management. Overview. Renal failure 1/10/2018. Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH
 Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
Universal HCV treatment: Strategies for simplification
 Universal HCV treatment: Strategies for simplification PARIS HEPATOLOGY CONFERENCE 3 January 217 Tarik Asselah (MD, PhD) Hepatology & Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures
Universal HCV treatment: Strategies for simplification PARIS HEPATOLOGY CONFERENCE 3 January 217 Tarik Asselah (MD, PhD) Hepatology & Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures
Case. 63 year old woman now with:
 Case 63 year old woman now with: HCV GT 1b, HCV RNA 6.2 x 10 6 IU/mL Asymptomatic except for fatigue Normal exam ALT 72 IU/mL, Bili 0.9 mg/dl, INR 1.1, Albumin 3.9 g/dl, Creatinine 0.7 mg/dl Normal EGD
Case 63 year old woman now with: HCV GT 1b, HCV RNA 6.2 x 10 6 IU/mL Asymptomatic except for fatigue Normal exam ALT 72 IU/mL, Bili 0.9 mg/dl, INR 1.1, Albumin 3.9 g/dl, Creatinine 0.7 mg/dl Normal EGD
Current HCV Treatment by Genotype
 Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
HCV in 2017: New Therapies and New Opportunities. Presentation prepared by: Date prepared: OBJECTIVES
 Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Selecting HCV Treatment
 Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
A treatment revolution: current management for chronic HCV
 A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
Hepatitis C Genotypes
 9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London
 HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
The Dawn of a New Era: Hepatitis C
 The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
Cases: Management of Hepatitis C in Prior Treatment Failure
 Cases: Management of Hepatitis C in Prior Treatment Failure David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After
Cases: Management of Hepatitis C in Prior Treatment Failure David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After
Current HCV Treatment by Genotype Ira M. Jacobson, MD
 Current HCV Treatment by Genotype Ira M. Jacobson, MD Director of Hepatology NYU School of Medicine Objectives To understand the prevalence of HCV and distribution of HCV genotypes Describe the HCV lifecycle
Current HCV Treatment by Genotype Ira M. Jacobson, MD Director of Hepatology NYU School of Medicine Objectives To understand the prevalence of HCV and distribution of HCV genotypes Describe the HCV lifecycle
Meet the Professor: HIV/HCV Coinfection
 Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Virological tools for hepatitis C: re-treatment and resistance. Joop Arends Will Irving. by author
 Virological tools for hepatitis C: re-treatment and resistance Joop Arends Will Irving Disclosures Joop Arends Advisory board: Gilead, Abbvie, Janssen, MSD, BMS (research) grants: Abbvie, BMS, MSD and
Virological tools for hepatitis C: re-treatment and resistance Joop Arends Will Irving Disclosures Joop Arends Advisory board: Gilead, Abbvie, Janssen, MSD, BMS (research) grants: Abbvie, BMS, MSD and
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret
 New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
Special developments in the management of Hepatitis C. Disclosures
 Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
AASLD/IDSA HCV treatment guidelines. Arthur Y. Kim, MD Massachusetts General Hospital Harvard Medical School
 AASLD/IDSA HCV treatment guidelines Arthur Y. Kim, MD Massachusetts General Hospital Harvard Medical School Disclosure Statement for Arthur Kim Grant/research support to institution, last 12 months: Gilead
AASLD/IDSA HCV treatment guidelines Arthur Y. Kim, MD Massachusetts General Hospital Harvard Medical School Disclosure Statement for Arthur Kim Grant/research support to institution, last 12 months: Gilead
Update on Hepatitis C. Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017
 Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Debate: Do We Need More HCV Drugs Con Standpoint
 Debate: Do We Need More HCV Drugs Con Standpoint 18 th Antivirals PK Workshop, Friday 16 th June 2017, Chicago Jürgen Rockstroh Department of Medicine I University Hospital Bonn, Bonn, Germany Conflict
Debate: Do We Need More HCV Drugs Con Standpoint 18 th Antivirals PK Workshop, Friday 16 th June 2017, Chicago Jürgen Rockstroh Department of Medicine I University Hospital Bonn, Bonn, Germany Conflict
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity. Cody A. Chastain, MD
 Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Management of Chronic HCV 2017 and Beyond
 Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano. Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future
 Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future DAA classes and subclasses Drug Class Subclass Potency
Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future DAA classes and subclasses Drug Class Subclass Potency
What is the Optimized Treatment Duration? To Overtreat versus Undertreat. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
HTA: Models, Costs & Benefits.
 HTA: Models, Costs & Benefits John.Cairns@lshtm.ac.uk Explicit evaluation of costs and benefits Advantages Potential for more consistent decision making Potential for more transparent decision making Facilitates
HTA: Models, Costs & Benefits John.Cairns@lshtm.ac.uk Explicit evaluation of costs and benefits Advantages Potential for more consistent decision making Potential for more transparent decision making Facilitates
Eliminating Hepatitis C from New Zealand
 Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
HCV Infection: EASL Clinical Practice Guidelines Francesco Negro University Hospital Geneva Switzerland
 HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE
 THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE MARIA SCHINA CONSULTANT PHYSICIAN INTERNAL MEDICINE AND HEPATOLOGY ATHENS EUROCLINIC 10 th INTERNATIONAL CONGRESS OF
THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE MARIA SCHINA CONSULTANT PHYSICIAN INTERNAL MEDICINE AND HEPATOLOGY ATHENS EUROCLINIC 10 th INTERNATIONAL CONGRESS OF
Cases: Initial Treatment of Hepatitis C
 Cases: Initial Treatment of Hepatitis C Kristen Marks, MD Assistant Professor of Medicine Weill Cornell Medical College New York, New York Off-Label Warning I will discuss the following off-label use in
Cases: Initial Treatment of Hepatitis C Kristen Marks, MD Assistant Professor of Medicine Weill Cornell Medical College New York, New York Off-Label Warning I will discuss the following off-label use in
HIV/HCV Coinfection: Why It Matters and What To Do About It. Cody A. Chastain, MD 10/26/16
 HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
Management of HIV/HCV Coinfection. Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY
 Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
10/21/2016. Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina. Learning Objectives
 A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College
 Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Treatments of Genotype 2, 3,and 4: Now and in the future
 Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy
 Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
Drug Class Prior Authorization Criteria Hepatitis C
 Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: November 14, 2018 Effective Date: January 1, 2019 This drug class prior authorization criteria have been
Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: November 14, 2018 Effective Date: January 1, 2019 This drug class prior authorization criteria have been
TREATMENT OF GENOTYPE 2
 Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
Hepatitis C Update: Screening, Diagnosis, and Treatment
 Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical
Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical
Hepatitis C Elimination: Screening, Linkage and Treatment. Eric Lawitz, MD The Texas Liver Institute San Antonio, Texas
 Hepatitis C Elimination: Screening, Linkage and Treatment Eric Lawitz, MD The Texas Liver Institute San Antonio, Texas Hepatitis C: Worldwide Presence Worldwide prevalence: 130-150 million Viral hepatitis
Hepatitis C Elimination: Screening, Linkage and Treatment Eric Lawitz, MD The Texas Liver Institute San Antonio, Texas Hepatitis C: Worldwide Presence Worldwide prevalence: 130-150 million Viral hepatitis
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
Disclosures. I have given sponsored lectures for the following pharmaceutical companies: Gilead, Abbvie and MSD. I own shares of Gilead Sciences.
 Disclosures I have given sponsored lectures for the following pharmaceutical companies: Gilead, Abbvie and MSD. I own shares of Gilead Sciences. Chronic Hepatitis C Prof CL Lai University Department of
Disclosures I have given sponsored lectures for the following pharmaceutical companies: Gilead, Abbvie and MSD. I own shares of Gilead Sciences. Chronic Hepatitis C Prof CL Lai University Department of
Update on the Treatment of HCV
 Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Hepatitis C Prior Authorization Policy
 Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
New York State HCV Provider Webinar Series. Treatment of HCV/HIV Co-Infection
 New York State HCV Provider Webinar Series Treatment of HCV/HIV Co-Infection Objectives Review the epidemiology of HCV and HIV/HCV co-infection Discuss the burden of HIV/HCV co-infection Discuss the treatment
New York State HCV Provider Webinar Series Treatment of HCV/HIV Co-Infection Objectives Review the epidemiology of HCV and HIV/HCV co-infection Discuss the burden of HIV/HCV co-infection Discuss the treatment
HCV Treatment in 2016: Genotypes 1, 2, and 3. Cody A. Chastain, MD October 12, 2016
 HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado
 FORMATTED: 1/3/16 Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? Atlanta, Georgia: October 2, 216 David L. Wyles, MD Chief, Division of Infectious Disease Denver Health
FORMATTED: 1/3/16 Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? Atlanta, Georgia: October 2, 216 David L. Wyles, MD Chief, Division of Infectious Disease Denver Health
Hepatitis C: a treatment revolution
 Sunday, 10th July 2016 Michaelmas Cay 2 Room Concurrent 11 Health Innovation Hepatitis C: a treatment revolution Dr. Heather McNamee Hepatitis C a treatment revolution Dr Heather McNamee Medical Director
Sunday, 10th July 2016 Michaelmas Cay 2 Room Concurrent 11 Health Innovation Hepatitis C: a treatment revolution Dr. Heather McNamee Hepatitis C a treatment revolution Dr Heather McNamee Medical Director
Associate Professor of Medicine University of Chicago
 Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Sofosbuvir-Velpatasvir-Voxilaprevir in DAA-Experienced GT 1-6 POLARIS-4
 Phase 3 Treatment Experienced Sofosbuvir-Velpatasvir-Voxilaprevir in DAA-Experienced GT 1-6 POLARIS-4 Bourlière M, et al. N Engl J Med. 217;376:2134-46. POLARIS-4: Study Features POLARIS-4 Trial Design:
Phase 3 Treatment Experienced Sofosbuvir-Velpatasvir-Voxilaprevir in DAA-Experienced GT 1-6 POLARIS-4 Bourlière M, et al. N Engl J Med. 217;376:2134-46. POLARIS-4: Study Features POLARIS-4 Trial Design:
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline
 PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
Dr. Siddharth Srivastava
 Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Glecaprevir-Pibrentasvir in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2)
") Phase 3 Treatment-Experienced in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2) in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2): Study Features MAGELLAN-1 (Part 2) Trial Design: Randomized,
Phase 3 Treatment-Experienced in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2) in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2): Study Features MAGELLAN-1 (Part 2) Trial Design: Randomized,
Hepatitis C Treatment 2014
 Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
10/21/2016. David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado
 Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado FORMATTED: 1/3/16
Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado FORMATTED: 1/3/16
Drug Class Prior Authorization Criteria Hepatitis C
 Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim (pending P&T approval) Effective Date: July 1, 2018 This policy has been developed through review
Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim (pending P&T approval) Effective Date: July 1, 2018 This policy has been developed through review
Updates in the Treatment of HCV
 Updates in the Treatment of HCV Misty Miller, Pharm.D., BCPS, AAHIVP Associate Professor University of Oklahoma College of Pharmacy September 21 st, 2018 Overview HCV Review and Definitions HCV Genotypes
Updates in the Treatment of HCV Misty Miller, Pharm.D., BCPS, AAHIVP Associate Professor University of Oklahoma College of Pharmacy September 21 st, 2018 Overview HCV Review and Definitions HCV Genotypes
Genotype 1 Treatment Naïve No Cirrhosis Options
 Genotype 1 Treatment Naïve No Cirrhosis Options Elbasvir/Grazoprevir (Zepatier ) x 12 weeks 1 Glecaprevir/Pibrentasvir (Mavyret ) x 8 weeks Ledipasvir/Sofosbuvir (Harvoni ) x 8-12 weeks 2 1 If genotype
Genotype 1 Treatment Naïve No Cirrhosis Options Elbasvir/Grazoprevir (Zepatier ) x 12 weeks 1 Glecaprevir/Pibrentasvir (Mavyret ) x 8 weeks Ledipasvir/Sofosbuvir (Harvoni ) x 8-12 weeks 2 1 If genotype
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
HIV-HCV Co-Infection in Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School
 HIV-HCV Co-Infection in 2018 Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School AASLD/IDSA and DHHS Guidance: HIV/HCV Coinfection All pts with HIV should be screened
HIV-HCV Co-Infection in 2018 Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School AASLD/IDSA and DHHS Guidance: HIV/HCV Coinfection All pts with HIV should be screened
The Changing World of Hepatitis C
 The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C Second Generation Antivirals Page 1 of 32 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Hepatitis C Second Generation Antivirals Page 1 of 32 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Drug Class Monograph
 Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira Pak), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira Pak), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Treating Hepatitis C in Patients with Advanced Renal Disease
 Treating Hepatitis C in Patients with Advanced Renal Disease Seyed Moayed Alavian M.D. Professor of Medicine, Hepatologist alavian@thc.ir Hemodialysis Patients hemodialysis Preventive Strategies Strict
Treating Hepatitis C in Patients with Advanced Renal Disease Seyed Moayed Alavian M.D. Professor of Medicine, Hepatologist alavian@thc.ir Hemodialysis Patients hemodialysis Preventive Strategies Strict
IFN-free therapy in naïve HCV GT1 patients
 IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C Second Generation Antivirals Page 1 of 30 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Hepatitis C Second Generation Antivirals Page 1 of 30 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
1/16/2019. Goals of HCV Therapy. Objectives. Treating Hepatitis C and HIV Co Infection. Cure Defined as sustained virologic response (SVR)
") HCV ECHO WESTERN STATES HCV ECHO WESTERN STATES Treating Hepatitis C and HIV Co Infection Paulina Deming, Pharm D Associate Professor, College of Pharmacy Assistant Director, Viral Hepatitis Programs,
HCV ECHO WESTERN STATES HCV ECHO WESTERN STATES Treating Hepatitis C and HIV Co Infection Paulina Deming, Pharm D Associate Professor, College of Pharmacy Assistant Director, Viral Hepatitis Programs,
HCV Treatment of Genotype 1: Now and in the Future
 HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
Initial Treatment of the Hepatitis C Virus-Infected Patient
 IDSA/AASLD www.hcvguidelines.org http://www.easl.eu/research/our-contributions/clinical-practice-guidelines/detail/easl-recommendations-ontreatment-of-hepatitis-c-216 Initial Treatment of the Hepatitis
IDSA/AASLD www.hcvguidelines.org http://www.easl.eu/research/our-contributions/clinical-practice-guidelines/detail/easl-recommendations-ontreatment-of-hepatitis-c-216 Initial Treatment of the Hepatitis
Drug Class Prior Authorization Criteria Hepatitis C
 Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim Criteria Pending P&T Approval Effective Date: August 16, 2018 This drug class prior authorization
Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim Criteria Pending P&T Approval Effective Date: August 16, 2018 This drug class prior authorization
Hepatitis B and Hepatitis C Virus in non-liver Transplant Recipients. Karim Qumosani MD, FRCPC, ABIM, MdMEd Multi-organ Transplant Unit, London
 Hepatitis B and Hepatitis C Virus in non-liver Transplant Recipients Karim Qumosani MD, FRCPC, ABIM, MdMEd Multi-organ Transplant Unit, London Financial Disclosures Research Grants Merck, Gilead, Abbvie,
Hepatitis B and Hepatitis C Virus in non-liver Transplant Recipients Karim Qumosani MD, FRCPC, ABIM, MdMEd Multi-organ Transplant Unit, London Financial Disclosures Research Grants Merck, Gilead, Abbvie,
New York State HCV Provider Webinar Series. Side Effects of Therapy
 New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related
New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related
3/28/2016. The Top 5 Things to Remember about Treating HCV
 The Top 5 Things to Remember about Treating HCV Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University School of Medicine Durham, North Carolina FORMATTED: MM/DD/YY New York, New York:
The Top 5 Things to Remember about Treating HCV Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University School of Medicine Durham, North Carolina FORMATTED: MM/DD/YY New York, New York:
Shorter Durations and Pan-genotypic Regimens The Final Frontier. Professor Greg Dore
 Shorter Durations and Pan-genotypic Regimens The Final Frontier Professor Greg Dore Disclosures Funding and speaker fees from AbbVie, Bristol-Myers Squibb, Gilead Sciences and Merck Efficacy Evolution
Shorter Durations and Pan-genotypic Regimens The Final Frontier Professor Greg Dore Disclosures Funding and speaker fees from AbbVie, Bristol-Myers Squibb, Gilead Sciences and Merck Efficacy Evolution
What do we need to know about RAVs clinically?
 14 th European HIV & Hepatitis Workshop Rome, 25-27 May, 2016 What do we need to know about RAVs clinically? Stefan Zeuzem, MD University of Frankfurt Germany Background Resistance associated variants
14 th European HIV & Hepatitis Workshop Rome, 25-27 May, 2016 What do we need to know about RAVs clinically? Stefan Zeuzem, MD University of Frankfurt Germany Background Resistance associated variants
Treatment of Hepatitis C with sofosbuvir/ledipasvir (Harvoni )
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline
 Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir) PHARMACY PRI AUTHIZATION Hepatitis C Clinical Guideline Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir) Harvoni
Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir) PHARMACY PRI AUTHIZATION Hepatitis C Clinical Guideline Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir) Harvoni
Hepatitis C: the 2015 Perspective for the Family Medicine Practitioner
 Hepatitis C: the 2015 Perspective for the Family Medicine Practitioner Annie Luetkemeyer, MD Division of HIV,ID & Global Medicine San Francisco General Hospital Disclosures I have received research grant
Hepatitis C: the 2015 Perspective for the Family Medicine Practitioner Annie Luetkemeyer, MD Division of HIV,ID & Global Medicine San Francisco General Hospital Disclosures I have received research grant
Tough Cases in HIV/HCV Coinfection
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014