Quality Improvement Updates Foley Discontinuation Protocol Surgical Care Improvement Project
|
|
|
- Jade Jordan
- 5 years ago
- Views:
Transcription

1 Quality Improvement Updates Foley Discontinuation Protocol Surgical Care Improvement Project Barbara J Martin, RN, MBA Quality Consultant, Center for Clinical Improvement
2 Indwelling Urinary Catheters Insertion, Care and Maintenance, and Discontinuation Urinary Tract Infection Reduction Task Force Roger Dmochowski, MD Chair
3 Insertion Policy Key Points Urinary Catheters require an order Clinical Indications for indwelling catheter: Urinary retention not relieved with intermittent catheterization Current regional / epidural anesthesia Terminal illness receiving comfort care or withdrawal of care Stage 3 or greater pressure ulcers Critical illness AND a need for accurate monitoring of urinary output
4 Care and Management Key Points Assess patient especially for continued need q 12 hr; w/ caregiver change; or per unit standard Perform perineal meatal care with soap & least q 12 hr; after BM; & PRN Anchor foley & maintain unobstructed urine flow Use strict aseptic technique when opening or accessing (for specimen) drainage system Maintain drainage system above floor and below patient bladder at all times including transport.
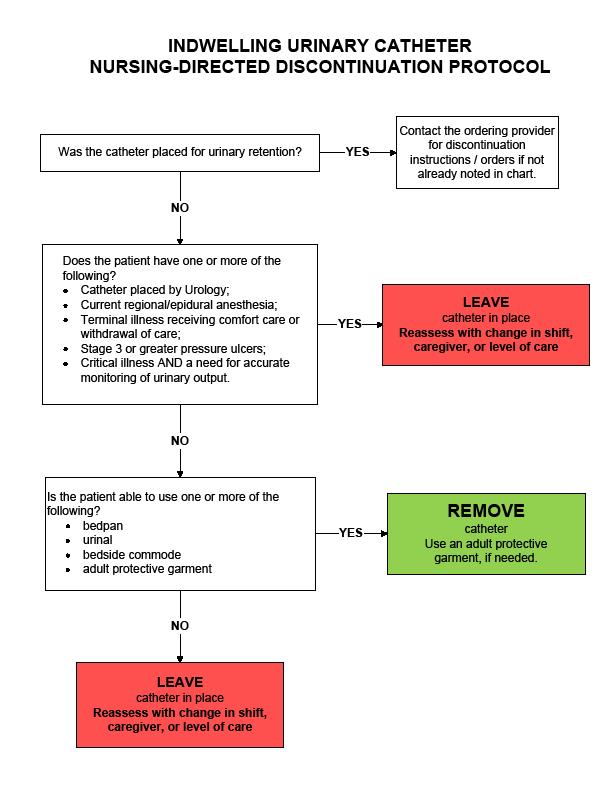
5 Discontinuation Protocol Purpose and Policy Implementation Date September 15 Reduction in catheter-associated associated complications, including infections from indwelling urinary catheters Patients with indwelling urinary catheters are assessed for continued need and catheters are discontinued when clinical indications are no longer present
6 Discontinuation Protocol An order is required for indwelling urinary catheterization When an indwelling urinary catheter is ordered, the provider may order the discontinuation protocol. If the discontinuation protocol is not used, a specific order is required for to remove the catheter.

7 FOLEY-REMOVE DATE/TIME: FOLEY-REMOVE PER PROTOCOL FOLEY-REMOVE BY PROVIDER ORDER New foley orderables Typing foley, urinary, catheter, & similar search words will bring up list of indwelling urinary catheter options in the upper right window foley
8
9 Discontinuation Protocol Patients are assessed by an RN for clinical indications for continued use of the indwelling urinary catheter: Upon admission Every shift or with change in caregiver Change in level of care
10 Discontinuation Protocol After the catheter is d/c d, d, the patient is assessed at intervals to determine ability to void, to empty the bladder, and to maintain continence If the patient is unable to void within six hours after the catheter is removed, the nurse may obtain an order for straight catheterization If the patient is incontinent, the nurse takes measures to assist with strategies to improve urinary control.
11 Discontinuation Key Points Consider whether catheter is necessary prior to insertion Default order is by provider order Ordering the protocol allows nursing staff to assess need for catheter, and remove when need is no longer present May order discontinuation at a specific point in time (e.g., 0600)


12
13 Objectives Review measures included in SCIP data submission. Identify mechanisms for process review and improvement relative to perioperative care. Describe internal monitoring for maintaining and improving compliance with surgical care metrics.
14 Core Measures: SCIP Core measures are required by the Joint Commission and based on CMS regulatory requirements SIP (Surgical Infection Prevention) measures began in 2004 with antibiotic administration metrics Changed to SCIP in 2006 with addition VTE and cardiac measures
15 SCIP Procedures ICD-9 9 Principal Procedure Code Coronary Artery Bypass Other Cardiac Surgery Colorectal Surgery Hysterectomy Total Hip Arthroplasty Total Knee Arthroplasty Vascular Surgery Major Surgery
16 Inclusion / Exclusion Case / metric exclusion based on clinical and administrative factors Infection prior to induction of anesthesia Chronic anticoagulation Procedure specific metrics Cardiac surgery: postop glycemic control Colectomies: Postoperative normothermia
17 SCIP Metrics SCIP 1: Prophylactic antibiotic administered within 1 hour prior to incision (2 hours for vancomycin or fluoroquinolone antibiotics) SCIP 2: Appropriate prophylactic antibiotic selection SCIP 3: Discontinuation of prophylactic antibiotics within 24 / 48 hours after surgery end time SCIP 4: Cardiac surgery patients with controlled 6 A.M. postoperative serum glucose
18 SCIP Metrics SCIP-6: Appropriate hair removal SCIP-7: Colorectal surgery patients with immediate postoperative normothermia SCIP-VTE VTE-1 1 and 2: Patients with recommended venous thromboembolism prophylaxis ordered and received SCIP-CARD CARD-2: Patients on beta blocker therapy prior to admission who receive a beta blocker during the perioperative period
19 Abstraction Methodology Weekly case sampling by discharge date (80 cases per month) Abstraction from electronic and paper medical record Monthly reports sent to administrators, chairs, and chiefs for review Patient data reviewed by clinicians before submission to CMS Charts selected by CMS quarterly for validation
20 A Note about Abstraction Abstraction is validated internally as well as externally Information must be part of the patient s permanent medical record Conflicting documentation is abstracted as unable to determine Must abstract based on most reasonable interpretation No appeal process for individual cases
21 SCIP Inf-1 1 and 2 Antibiotic Administration Patients with documented infection are excluded Must be started within 60 minutes of incision (120 for vancomycin, fluoroquinolones) Administered in OR by anesthesia ( vanc /quinolones which are given in holding) Verify infusion is started prior to incision Vancomycin usually requires justification MRSA colonization Beta-lactam allergy x
22 Other Considerations: Preop ABX Patients on antibiotic therapy Appropriate coverage provided? Redosing indicated? Is indication documented prior to surgery? Appropriate weight-based dosing Redosing prior to incision when prophylaxis is given in the ED
23 Specifications Manual for National Hospital Quality Measures Discharges (3Q09) through (2Q10) SCIP Inf SCIP Inf-2 Antibiotic Selection Antibiotic Selection
24 SCIP Inf-3 3 Antibiotic Discontinuation Cardiac Surgery Patients: Five doses for antibiotics given every 8 hours; OR Three doses for antibiotics given every 12 hours; OR Seven doses for antibiotics given every 6 hours. All Other Surgery Patients: Two doses for antibiotics given every 8 hours; OR One dose for antibiotics given every 12 hours; OR Three doses for antibiotics given every 6 hours.
25 Antibiotic Discontinuation No indication for prophylaxis beyond 24 hours Therapeutic antibiosis must be justified Document known or suspected infection Signs, symptoms and interventions will not meet CMS requirements If consulting service extends antibiotics, reason must be documented
26 Hair removal If hair removal required, clippers or depilatory must be used All cases evaluated Compliance for FY 2008: 100% All razors removed from OR Abstracted from OR Nursing Record

27 Postoperative Normothermia Currently colorectal surgery only Within 15 minutes of leaving the OR 36 C Route not specified If no temp documented within 15 minutes, measure fails
28 VTE Prophylaxis Mechanical and Pharmacologic Procedure-specific Cardiac and vascular excluded Procedure dictates required prophylaxis Heparin / enoxaparin/ warfarin (requires order to be abstracted) SCDs / TEDs Order within 48 hours, start within 24 hours Preop administration meets criteria
29 Perioperative Beta Blockade All cases evaluated Patients on beta blockers prior to surgery must have administration of a beta blocker documented within 24 hours before surgery through discharge from PACU, or within six hours after surgery if not in PACU postoperatively
30 Beta Blocker Documentation Patients admitted day of surgery Document BB taken at home on the day of surgery. If taken the night before, requires time taken Contraindications must be specifically documented Bradycardia (HR < 50) is a contrainidcation
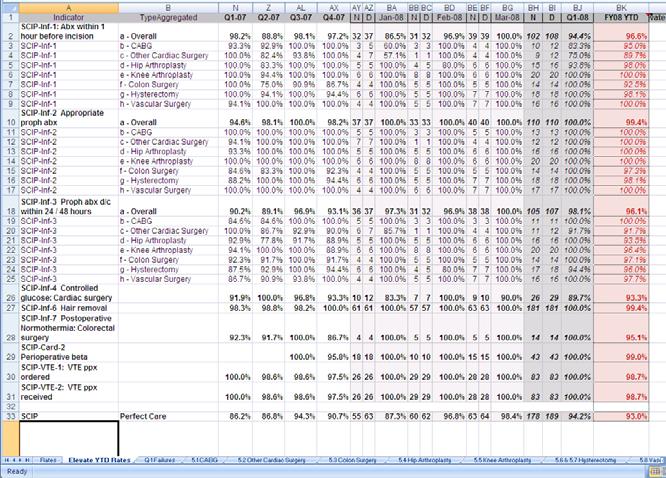
31 SCIP Performance FY 2009 Indicator FY O9 SCIP Inf 1: Abx within 1 hour before incision 96.9% SCIP Inf 2 Appropriate proph abx 98.5% SCIP Inf 3 Proph abx d/c within 24 / 48 hours 96.1 % SCIP Inf 4 Controlled glucose: Cardiac surgery 90.2% SCIP Inf 6 Hair removal 100% SCIP Inf 7 Postop Normothermia: Colorectal surgery 75.4% SCIP Card 2 Perioperative beta blockade 81.5% SCIP VTE 1: VTE ppx ordered 99.0% SCIP VTE 2: VTE ppx received 98.0% SCIP Perfect Care 88.4%
32 New SCIP Measures: Oct 2009 SCIP Inf 9: Urinary Catheter Removed on POD 1 or POD 2 Exclusions Urologic, gynecologic, and perineal procedures Infection prior to surgery ICU and on diuretics Documentation of continued need for catheter
33 New SCIP Measures: Oct 2009 SCIP Inf 10: Surgery Patients with Perioperative Temperature Measurement Documentation of active warming intraoperatively, or documentation of at least one temperature > 36 C within the last 30 minutes prior to or the 15 minutes immediately after Anesthesia End Time.

34 Public Reporting
35 Outpatient Surgery Measures OP 6 Antibiotic Timing OP 7 Antibiotic Selection Included Procedures Cardiac (PPM / AICDs) Orthopedic/Podiatry Genitourinary Gastric / Biliary Head and neck Neurological Gynecological Vascular


36 External Metrics: Internal Review
37 Maintaining Compliance Reminders Electronic forcing functions Redose reminders Concurrent reporting VPIMS SCIP reports M & M Review of failures Service chief follow-up of successes / failures Surgical services Anesthesiology
38 Opportunities Antibiotic administration Inpatient antibiotic redosing / timing / selection Emergency Department > OR antibiotic timing Holding room to incision timing for administration Glucose control Evaluate protocol compliance Monitor patient variables affecting hyperglycemia timing Beta blockade Preoperative instruction Documentation mechanisms in VPIMS Normothermia Evaluate system and process issues r/t equipment and documentation
39 Future SCIP Measures? Expanded beta blockade requirement Intraoperative antibiotic redosing Surgical site infection rate Postoperative VTE Rate
40 Beyond SCIP Wash your hands Control the environment Monitor and enforce infection prevention practices Address breaches yourself, or have them addressed Be constantly vigilant Every Patient, Every Time
41 SCIP Improvement Initiatives R. Daniel Beauchamp, MD, FACS Chair, Section of Surgical Sciences Michael S. Higgins, MD, MPH Chair, Department of Anesthesiology Nancye Feistritzer, MSN, RN Associate Hospital Director Stephanie Randa, RN, MHA Administrative Director, Operative Services Susie Leming-Lee, Lee, MSN, RN, CPHQ Director, Perioperative Quality Management Thomas R. Talbot, III, MD, MPH Chief Hospital Epidemiologist
AMI Talking Points. Provide appropriate treatment to Acute MI patients with these core measures:
 AMI Provide appropriate treatment to Acute MI patients with these core measures: Aspirin received within 24 hours of arrival or contraindication documented Primary PCI Received Within 90 Minutes of Hospital
AMI Provide appropriate treatment to Acute MI patients with these core measures: Aspirin received within 24 hours of arrival or contraindication documented Primary PCI Received Within 90 Minutes of Hospital
Surgical Care, Pneumonia, Immunizations and Emergency Department Core Measures
 Surgical Care, Pneumonia, Immunizations and Emergency Department Core Measures Audrey Paulman, MD, MMM Principal Clinical Coordinator & Jackie Trojan, RN, BSN Quality Improvement Advisor This material
Surgical Care, Pneumonia, Immunizations and Emergency Department Core Measures Audrey Paulman, MD, MMM Principal Clinical Coordinator & Jackie Trojan, RN, BSN Quality Improvement Advisor This material
Quality Committee Core Measures Report AMI. Acute Myocardial Infarction
 AMI 2011 Acute Myocardial Infarction ASPIRIN AT ARRIVAL: A higher number is better. This measure shows the percentage of heart attack patients who receive aspirin within 24 hrs of arrival at hospital.
AMI 2011 Acute Myocardial Infarction ASPIRIN AT ARRIVAL: A higher number is better. This measure shows the percentage of heart attack patients who receive aspirin within 24 hrs of arrival at hospital.
UCLA Health System Apr - Jun 2013 (Q2)
") Denom Observed VBP Standard VBP Benchmark Denom Observed VBP Standard VBP Benchmark N Percent x/n N Percent x/n Value Based Purchasing-Clinical Process of Care Measures (%) SCIP-Inf-9 Urinary catheter
Denom Observed VBP Standard VBP Benchmark Denom Observed VBP Standard VBP Benchmark N Percent x/n N Percent x/n Value Based Purchasing-Clinical Process of Care Measures (%) SCIP-Inf-9 Urinary catheter
SUNY Downstate Medical Center/University Hospital Oct - Dec 2013 (Q4)
") Value Based Purchasing-Clinical Process of Care Measures Denom Observed VBP VBP Benchmark Standard Denom Observed VBP VBP Benchmark Standard N Percent x/n N Percent x/n SCIP-Inf-9 Urinary catheter removed
Value Based Purchasing-Clinical Process of Care Measures Denom Observed VBP VBP Benchmark Standard Denom Observed VBP VBP Benchmark Standard N Percent x/n N Percent x/n SCIP-Inf-9 Urinary catheter removed
2012 Core Measures. Acute Myocardial Infarction (AMI)
") 2012 Core Measures Acute Myocardial Infarction (AMI) Aspirin at Arrival Aspirin Prescribed at Discharge Angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) for left ventricular
2012 Core Measures Acute Myocardial Infarction (AMI) Aspirin at Arrival Aspirin Prescribed at Discharge Angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) for left ventricular
Physician's Core Measure Pocket Guide AMI
 Physician's Core Measure Pocket Guide Core Measure Hotline: Ext. 4448 http://centegramedsource.com Indicator: AMI AMI VER. 9/2018 MUST document WHY no ASA unless there is documentation of contraindication
Physician's Core Measure Pocket Guide Core Measure Hotline: Ext. 4448 http://centegramedsource.com Indicator: AMI AMI VER. 9/2018 MUST document WHY no ASA unless there is documentation of contraindication
This Core Measure Report shows performance to date. CAVEAT: Data collection is still in progress for the current and immediate past quarter!
 This Core Measure Report shows performance to date. CAVEAT: Data collection is still in progress for the current and immediate past quarter! AMI-1 -- Aspirin at Arrival 9 8 7 6 5 4 3 2 1 AMI-2 -- Aspirin
This Core Measure Report shows performance to date. CAVEAT: Data collection is still in progress for the current and immediate past quarter! AMI-1 -- Aspirin at Arrival 9 8 7 6 5 4 3 2 1 AMI-2 -- Aspirin
EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES
 EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES Clifford Ko, MD, MS, MSHS, FACS, FASCRS Professor of Surgery UCLA Director, ACS NSQIP, American College of Surgeons EVIDENCE Ban
EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES Clifford Ko, MD, MS, MSHS, FACS, FASCRS Professor of Surgery UCLA Director, ACS NSQIP, American College of Surgeons EVIDENCE Ban
SCORES FOR 4 TH QUARTER, RD QUARTER, 2014
 SCORES FOR 4 TH QUARTER, 2013 3 RD QUARTER, 2014 PATIENT SATISFACTION SCORES (HCAHPS): 4 STARS OUT OF 5 (ONLY 4 AREA ACUTE CARE HOSPITALS RECEIVED A 4-STAR RATING. NONE ACHIEVED 5-STARS). STRUCTURAL MEASURES:
SCORES FOR 4 TH QUARTER, 2013 3 RD QUARTER, 2014 PATIENT SATISFACTION SCORES (HCAHPS): 4 STARS OUT OF 5 (ONLY 4 AREA ACUTE CARE HOSPITALS RECEIVED A 4-STAR RATING. NONE ACHIEVED 5-STARS). STRUCTURAL MEASURES:
NEW JERSEY 2012 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY 2012 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment June 2013 NEW JERSEY
NEW JERSEY 2012 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment June 2013 NEW JERSEY
NYSPFP CAUTI Educational Session: No Harm Across the Board and CAUTI Reduction
 NYS PARTNERSHIP FOR PATIENTS NYSPFP CAUTI Educational Session: No Harm Across the Board and CAUTI Reduction Tuesday, September 30, 2014 NYS PARTNERSHIP FOR PATIENTS Today s Agenda Welcome and Introductions
NYS PARTNERSHIP FOR PATIENTS NYSPFP CAUTI Educational Session: No Harm Across the Board and CAUTI Reduction Tuesday, September 30, 2014 NYS PARTNERSHIP FOR PATIENTS Today s Agenda Welcome and Introductions
Performance Measure. Inpatient Clinical Process of Care Measures
 Acute Myocardial Infarction (AMI) 's Maryland Hospital Performance Evaluation System: Inpatient s Quality Based Reimbursement () Measures Highlighted in Green (02/27/2014) Inpatient Clinical Process of
Acute Myocardial Infarction (AMI) 's Maryland Hospital Performance Evaluation System: Inpatient s Quality Based Reimbursement () Measures Highlighted in Green (02/27/2014) Inpatient Clinical Process of
SURGICAL CARE IMPROVEMENT PROJECT QUALITY MEASURES
 SURGICAL CARE IMPROVEMENT PROJECT QUALITY MEASURES Hospitals can reduce the risk of infection after surgery by making sure they provide the standard of care that is known to get the best results for most
SURGICAL CARE IMPROVEMENT PROJECT QUALITY MEASURES Hospitals can reduce the risk of infection after surgery by making sure they provide the standard of care that is known to get the best results for most
CMS National Patient Safety Initiative for Surgical Care
 CMS National Patient Safety Initiative for Surgical Care Ongoing Opportunities for Improvement Dale W. Bratzler, DO, MPH President and CEO Oklahoma Foundation for Medical Quality An update where are we
CMS National Patient Safety Initiative for Surgical Care Ongoing Opportunities for Improvement Dale W. Bratzler, DO, MPH President and CEO Oklahoma Foundation for Medical Quality An update where are we
Measure Information Form
 Last Updated: Version 3.2 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Information Form Measure Set: Surgical Care Improvement Project (SCIP) Set Measure ID#: SCIP- Performance
Last Updated: Version 3.2 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Information Form Measure Set: Surgical Care Improvement Project (SCIP) Set Measure ID#: SCIP- Performance
SCIP Cardiac Measure. Lee A. Fleisher, M.D.
 SCIP Cardiac Measure Lee A. Fleisher, M.D. fleishel@uphs.upenn.edu Medicare Surgical Infection Prevention (SIP) Project Objective To decrease the morbidity and mortality associated with postoperative infection
SCIP Cardiac Measure Lee A. Fleisher, M.D. fleishel@uphs.upenn.edu Medicare Surgical Infection Prevention (SIP) Project Objective To decrease the morbidity and mortality associated with postoperative infection
Presentation at ACS NSQIP National Conference in July Surgical Site Infection Reduction Strategies
 Presentation at ACS NSQIP National Conference in July 2015 Surgical Site Infection Reduction Strategies PeaceHealth Sacred Heart Medical Center at RiverBend Level II Trauma Center 379 Beds 15,060 cases
Presentation at ACS NSQIP National Conference in July 2015 Surgical Site Infection Reduction Strategies PeaceHealth Sacred Heart Medical Center at RiverBend Level II Trauma Center 379 Beds 15,060 cases
Preventing Surgical Site Infections: The SSI Bundle
 Preventing Surgical Site Infections: The SSI Bundle 1 Why SSI? New York State 30,000 hospital discharges 1984 3.7% of patients experience serious adverse events related to medical management The top three
Preventing Surgical Site Infections: The SSI Bundle 1 Why SSI? New York State 30,000 hospital discharges 1984 3.7% of patients experience serious adverse events related to medical management The top three
Developed by Kathy Wonderly RN, BSPA, CPHQ Performance Improvement Coordinator Developed : October 2009 Most recently updated: September 2011
 Developed by Kathy Wonderly RN, BSPA, CPHQ Performance Improvement Coordinator Developed : October 2009 Most recently updated: September 2011 To identify the patients who should receive a beta blocker
Developed by Kathy Wonderly RN, BSPA, CPHQ Performance Improvement Coordinator Developed : October 2009 Most recently updated: September 2011 To identify the patients who should receive a beta blocker
NEW JERSEY 2011 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY 2011 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health and Senior Services Health Care Quality Assessment
NEW JERSEY 2011 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health and Senior Services Health Care Quality Assessment
CMS Hospital IQR Program Measure Comparison Tables FY 2018 (CY 2016) Measures Required to Meet Hospital IQR APU Requirements NHSN Submission
 Measures Required to Meet Hospital IQR APU Requirements NHSN Submission") CMS IQR Program Measure Comparison Tables (CY 2016) NHSN Submission CLABSI Central Line-Associated Bloodstream Infection (CLABSI) Required NHSN CAUTI Catheter-Associated Urinary Tract Infection (CAUTI)
CMS IQR Program Measure Comparison Tables (CY 2016) NHSN Submission CLABSI Central Line-Associated Bloodstream Infection (CLABSI) Required NHSN CAUTI Catheter-Associated Urinary Tract Infection (CAUTI)
LINKS OF INTEREST DISCLOSURE
 LINKS OF INTEREST DISCLOSURE Name of the speaker: Sarah L. Krein I have no link of interest. www.sf2h.net 7, 8 et 9 juin 2017 And what about getting rid of catheter-associated urinary tract infections?
LINKS OF INTEREST DISCLOSURE Name of the speaker: Sarah L. Krein I have no link of interest. www.sf2h.net 7, 8 et 9 juin 2017 And what about getting rid of catheter-associated urinary tract infections?
Contributions To Safer Surgery At Valley Medical center
 Contributions To Safer Surgery At Valley Medical center Safe Surgery Initiatives The Joint Commission World Health Organization Institute for Healthcare Improvement WSHA Qualis Safe Surgery Initiatives
Contributions To Safer Surgery At Valley Medical center Safe Surgery Initiatives The Joint Commission World Health Organization Institute for Healthcare Improvement WSHA Qualis Safe Surgery Initiatives
Urinary Catheters. Prevalence of Infections
 Urinary Catheterisation Urinary catheterisation is defined as an intervention to enable the emptying of the bladder by insertion of a catheter. Catheters can be short term less than 28 days or long term
Urinary Catheterisation Urinary catheterisation is defined as an intervention to enable the emptying of the bladder by insertion of a catheter. Catheters can be short term less than 28 days or long term
including prevention, healthy lifestyle behaviors, populations at risk & disparities (age, race/ ethnicity, gender, geographic & socioeconomic)
") Endorsement Maintenance 2010 Identification of Gap Areas for which Evidence-based Surgery-related Measures are Needed Cardiac, General, Other Surgical Subspecialties The table below is a tool that identifies
Endorsement Maintenance 2010 Identification of Gap Areas for which Evidence-based Surgery-related Measures are Needed Cardiac, General, Other Surgical Subspecialties The table below is a tool that identifies
Catheter Associated Urinary Tract Infection
 Catheter Associated Urinary Tract Infection Facts about CAUTI 12% to 16% of adult patients will receive a urinary catheter during hospitalization. 4 th most common HAI Accounts for more than 12% of acute
Catheter Associated Urinary Tract Infection Facts about CAUTI 12% to 16% of adult patients will receive a urinary catheter during hospitalization. 4 th most common HAI Accounts for more than 12% of acute
Prescribe appropriate immunizations for. Prescribe childhood immunization as per. Prescribe influenza vaccinations in high-risk
 Supplemental Digital Appendix 1 46 Health Care Problems and the Corresponding 59 Practice Indicators Expected of All Physicians Entering or in Practice Infectious and parasitic diseases Avoidable complications/death
Supplemental Digital Appendix 1 46 Health Care Problems and the Corresponding 59 Practice Indicators Expected of All Physicians Entering or in Practice Infectious and parasitic diseases Avoidable complications/death
SCIP and NSQIP the Alphabet Soup of Surgical Quality
 SCIP and NSQIP the Alphabet Soup of Surgical Quality NSQIP National Conference Christopher C Johnson M.D. Caryn Foster RN, SCR Nicholas Hellenthal M.D., F.A.C.S. 7/26/15 Disclosure None Introduction The
SCIP and NSQIP the Alphabet Soup of Surgical Quality NSQIP National Conference Christopher C Johnson M.D. Caryn Foster RN, SCR Nicholas Hellenthal M.D., F.A.C.S. 7/26/15 Disclosure None Introduction The
50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations
 50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations mstockstill on DSKH9S0YB1PROD with RULES2 VerDate Mar2010 17:02 Aug 13, 2010 Jkt 220001 PO 00000 Frm 00158
50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations mstockstill on DSKH9S0YB1PROD with RULES2 VerDate Mar2010 17:02 Aug 13, 2010 Jkt 220001 PO 00000 Frm 00158
ST. DOMINIC-JACKSON MEMORIAL HOSPITAL JACKSON, MISSISSIPPI
 Date & Time Post-Op Inpatient General Orthopedic Page 1 of 5 Pharmacy Mnemonic: POIGOP1 1. Admit as inpatient to Dr. 2.Diagnosis: 3.Admit to PACU and then to floor ICU 4.Radiology: AP Pelvis in PACU AP
Date & Time Post-Op Inpatient General Orthopedic Page 1 of 5 Pharmacy Mnemonic: POIGOP1 1. Admit as inpatient to Dr. 2.Diagnosis: 3.Admit to PACU and then to floor ICU 4.Radiology: AP Pelvis in PACU AP
Using PDSA Cycles to Implement CAUTI Bundles and Transfer Communication between Settings
 Using PDSA Cycles to Implement CAUTI Bundles and Transfer Communication between Settings Katherine Abraham Evans, DNP, FNP-C, GNP-BC, ACHPN Clinical Assistant Professor DNP Program Coordinator Georgia
Using PDSA Cycles to Implement CAUTI Bundles and Transfer Communication between Settings Katherine Abraham Evans, DNP, FNP-C, GNP-BC, ACHPN Clinical Assistant Professor DNP Program Coordinator Georgia
convey the clinical quality measure's title, number, owner/developer and contact
 CMS-0033-P 153 convey the clinical quality measure's title, number, owner/developer and contact information, and a link to existing electronic specifications where applicable. TABLE 20: Proposed Clinical
CMS-0033-P 153 convey the clinical quality measure's title, number, owner/developer and contact information, and a link to existing electronic specifications where applicable. TABLE 20: Proposed Clinical
Why focus on surgical quality?
 The Surgical Infection Prevention and Surgical Care Improvement Projects Where we started and where we re going Dale W. Bratzler, DO, MPH QIOSC Medical Director Why focus on surgical quality? ~30 million
The Surgical Infection Prevention and Surgical Care Improvement Projects Where we started and where we re going Dale W. Bratzler, DO, MPH QIOSC Medical Director Why focus on surgical quality? ~30 million
(Page 1 of 5) Diagnosis: Procedure: Right Total Knee Replacement Unicompartmental Knee Left Total Hip Revision Total Shoulder
 Diagnosis: Procedure: Right Total Knee Replacement Unicompartmental Knee Left Total Hip Revision Total Shoulder") (Page 1 of 5) Allergies/Sensitivities/Reactions: Height: Inches cm Weight: Kg Pounds = Automatic = Physician s option, Check off to Order Diagnosis: Procedure: Right Total Knee Replacement Unicompartmental
(Page 1 of 5) Allergies/Sensitivities/Reactions: Height: Inches cm Weight: Kg Pounds = Automatic = Physician s option, Check off to Order Diagnosis: Procedure: Right Total Knee Replacement Unicompartmental
QI Successes & Failures Learning from Both
 QI Successes & Failures Learning from Both E. Patchen Dellinger, MD, FACS, FIDSA, FSHEA Professor of Surgery University of Washington Medical Center (UWMC), Seattle, Washington Conflict of Interest Over
QI Successes & Failures Learning from Both E. Patchen Dellinger, MD, FACS, FIDSA, FSHEA Professor of Surgery University of Washington Medical Center (UWMC), Seattle, Washington Conflict of Interest Over
Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients)
: Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients)") Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) 2013 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage
Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) 2013 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage
Appendix G Explanation/Clarification Summary
 Appendix G Explanation/Clarification Summary Summary of Changes for Recommendations Alignment of measures with VBP by fiscal year Measures and service dates were adjusted to be consistent with the FY2016
Appendix G Explanation/Clarification Summary Summary of Changes for Recommendations Alignment of measures with VBP by fiscal year Measures and service dates were adjusted to be consistent with the FY2016
Prevention of Important HAIs: Principle & Case Scenario in VAP/CAUTI. CPT. Pasri Maharom MD, MPH Dec 15, 2015
 Prevention of Important HAIs: Principle & Case Scenario in VAP/CAUTI CPT. Pasri Maharom MD, MPH Dec 15, 2015 Catheter Associated Urinary Tract Infection CAUTI CAUTI Epidemiology Key Principles of Preventing
Prevention of Important HAIs: Principle & Case Scenario in VAP/CAUTI CPT. Pasri Maharom MD, MPH Dec 15, 2015 Catheter Associated Urinary Tract Infection CAUTI CAUTI Epidemiology Key Principles of Preventing
2016 Hospital Measures
 2016 Hospital Measures Vicki Tang Olson, Stratis Health Statewide Quality Reporting and Measurement System (SQRMS) Annual Forum June 22, 2015 Objectives Share the process used for 2016 hospital measures
2016 Hospital Measures Vicki Tang Olson, Stratis Health Statewide Quality Reporting and Measurement System (SQRMS) Annual Forum June 22, 2015 Objectives Share the process used for 2016 hospital measures
State of the State: Hospital Performance in Pennsylvania September 2012
 State of the State: Hospital Performance in Pennsylvania September 2012 Measuring Progress in PA Hospital Performance: Process Measures 1 PA Hospital Performance: Process Measures We examined the latest
State of the State: Hospital Performance in Pennsylvania September 2012 Measuring Progress in PA Hospital Performance: Process Measures 1 PA Hospital Performance: Process Measures We examined the latest
FY X Time (48 hrs for cardiac surgery) SCIP-Inf-4 Cardiac Surgery Patients With Controlled 6 A.M. Postoperative Blood
 SCIP-Inf-4 Cardiac Surgery Patients With Controlled 6 A.M. Postoperative Blood") Valuebased 2013 Hospital Measure Summary Data Collection for Inpatient Quality Reporting FY2015 and Outpatient Reporting CY2014 January 2013 Key: = Required by both CMS and State of Minnesota = Required
Valuebased 2013 Hospital Measure Summary Data Collection for Inpatient Quality Reporting FY2015 and Outpatient Reporting CY2014 January 2013 Key: = Required by both CMS and State of Minnesota = Required
Choosing Wisely (Outpatient Edition)
") Choosing Wisely (Outpatient Edition) Michael Johansen, MD, MS Assistant Professor - Clinical Department of Family Medicine The Ohio State University Wexner Medical Center Prostate Cancer Screening (and
Choosing Wisely (Outpatient Edition) Michael Johansen, MD, MS Assistant Professor - Clinical Department of Family Medicine The Ohio State University Wexner Medical Center Prostate Cancer Screening (and
Choosing Wisely (Outpatient Edition)
") Choosing Wisely (Outpatient Edition) Michael Johansen, MD, MS Assistant Professor - Clinical Department of Family Medicine The Ohio State University Wexner Medical Center Prostate Cancer Screening (and
Choosing Wisely (Outpatient Edition) Michael Johansen, MD, MS Assistant Professor - Clinical Department of Family Medicine The Ohio State University Wexner Medical Center Prostate Cancer Screening (and
Urinary Catheters Do Not Have to Be Removed if They Were Never Placed
 Urinary Catheters Do Not Have to Be Removed if They Were Never Placed A formal performance improvement project to decrease utilization of urinary catheters in surgical patients A. D. Yang 1,2,3, M. W.
Urinary Catheters Do Not Have to Be Removed if They Were Never Placed A formal performance improvement project to decrease utilization of urinary catheters in surgical patients A. D. Yang 1,2,3, M. W.
GENERAL SURGICAL ADULT POST-OPERATIVE ORDERS 1 of 4
 down ADULT POST-OPERATIVE 1 of 4 9 Actual 9 Estimated Patient ID Area Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART Admit to: Post Anesthesia Care Unit (PACU),
down ADULT POST-OPERATIVE 1 of 4 9 Actual 9 Estimated Patient ID Area Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART Admit to: Post Anesthesia Care Unit (PACU),
CARD THORACOTOMY PRE-OP PLAN
 CARD THORACOTOMY PRE-OP PLAN PHYSICIAN S Diagnosis Weight Allergies Patient Care Perform Oral Care Perform night before surgery. Brush teeth with toothpaste, then swish and spit 15 ml chlorhexidine mouth
CARD THORACOTOMY PRE-OP PLAN PHYSICIAN S Diagnosis Weight Allergies Patient Care Perform Oral Care Perform night before surgery. Brush teeth with toothpaste, then swish and spit 15 ml chlorhexidine mouth
r*po1004*r PHYSICIAN S ORDERS Page 1 of 7 HOUR THORACOTOMY POSTOPERATIVE ORDERS General x Admit to Inpatient Status x Admitting Physician: Admit to:
 PHYSICIAN S ORDERS Page 1 of 7 General x Admit to Inpatient Status x Admitting Physician: Admit to: SICU Telemetry Med/Surg room x Resuscitation status: see Resuscitation Status Order Activity x Bed rest
PHYSICIAN S ORDERS Page 1 of 7 General x Admit to Inpatient Status x Admitting Physician: Admit to: SICU Telemetry Med/Surg room x Resuscitation status: see Resuscitation Status Order Activity x Bed rest
NHSN and Public Reporting. Linda R. Greene, RN,MPS,CIC Manager Infection Prevention Highland Hospital Rochester, NY linda_
 1 NHSN and Public Reporting Linda R. Greene, RN,MPS,CIC Manager Infection Prevention Highland Hospital Rochester, NY linda_ greene@urmc.rochester.edu 2 Objectives Describe challenges and opportunities
1 NHSN and Public Reporting Linda R. Greene, RN,MPS,CIC Manager Infection Prevention Highland Hospital Rochester, NY linda_ greene@urmc.rochester.edu 2 Objectives Describe challenges and opportunities
National Patient Safety Goal Preventing Catheter-Associated Urinary Tract Infections (CAUTI) 9/19/2016 1
 9/19/2016 1") Catheter-Associated Urinary Tract Infection (CAUTI) National Patient Safety Goal 07.06.01 Preventing Catheter-Associated Urinary Tract Infections (CAUTI) 9/19/2016 1 OBJECTIVES Describe appropriate screening
Catheter-Associated Urinary Tract Infection (CAUTI) National Patient Safety Goal 07.06.01 Preventing Catheter-Associated Urinary Tract Infections (CAUTI) 9/19/2016 1 OBJECTIVES Describe appropriate screening
IF YOU RECEIVED THIS FACSIMILE IN ERROR, PLEASE CALL IMMEDIATELY. ADMISSION INSTRUCTIONS: Admitted to Dr.
 ADMISSION INSTRUCTIONS: Admitted to Dr. Procedure: Right Hip Left Hip CODE STATUS: Full DNR level of intervention DIET: Dysphagia screen consult SLP High protein, high energy Regular Nutrient dense Boost
ADMISSION INSTRUCTIONS: Admitted to Dr. Procedure: Right Hip Left Hip CODE STATUS: Full DNR level of intervention DIET: Dysphagia screen consult SLP High protein, high energy Regular Nutrient dense Boost
Venous Thromboembolism Prophylaxis: Checked!
 Venous Thromboembolism Prophylaxis: Checked! William Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University of Toronto National Lead, VTE Prevention, Safer
Venous Thromboembolism Prophylaxis: Checked! William Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University of Toronto National Lead, VTE Prevention, Safer
ADULT TRANSCATHETER AORTIC VALVE REPLACEMENT (TAVR) TELEMETRY BED TRANSFER ORDERS 1 of 4
 TELEMETRY BED TRANSFER ORDERS 1 of 4") TELEMETRY BED TRANSFER 1 of 4 9 Actual 9 Estimated Patient ID Area Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART Transfer to: 10 South Attending Physician: Diagnosis:
TELEMETRY BED TRANSFER 1 of 4 9 Actual 9 Estimated Patient ID Area Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART Transfer to: 10 South Attending Physician: Diagnosis:
Gastrointestinal and urinary complications in the postoperative period
 The 13 th Annual Perioperative Medicine Summit Fort Lauderdale, Florida Gastrointestinal and urinary complications in the postoperative period Dan Hunt, MD Professor of Medicine Director, Division of Hospital
The 13 th Annual Perioperative Medicine Summit Fort Lauderdale, Florida Gastrointestinal and urinary complications in the postoperative period Dan Hunt, MD Professor of Medicine Director, Division of Hospital
America s Hospitals: Improving Quality and Safety
 America s Hospitals: Improving Quality and Safety The Joint Commission s Annual Report 2014 Top Performer on Key Quality Measures America s Hospitals: Improving Quality and Safety The Joint Commission
America s Hospitals: Improving Quality and Safety The Joint Commission s Annual Report 2014 Top Performer on Key Quality Measures America s Hospitals: Improving Quality and Safety The Joint Commission
Chapter 18. Assisting With Urinary Elimination. Elsevier items and derived items 2014, 2010 by Mosby, an imprint of Elsevier Inc. All rights reserved.
 Chapter 18 Assisting With Urinary Elimination The urinary system: The Urinary System Removes waste products from the blood Maintains the body s water balance 2 Normal Urination The healthy adult produces
Chapter 18 Assisting With Urinary Elimination The urinary system: The Urinary System Removes waste products from the blood Maintains the body s water balance 2 Normal Urination The healthy adult produces
The Centers for Medicare & Medicaid Services (CMS) Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures
 Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures") ID M easure Name NQF # H os pital M easurement Period H os pital H os pital Value-Bas ed Purchas ing M easurement Period H os pital H ealth Record (EH R) Incentive M easurement Period H os pital H os pital-
ID M easure Name NQF # H os pital M easurement Period H os pital H os pital Value-Bas ed Purchas ing M easurement Period H os pital H ealth Record (EH R) Incentive M easurement Period H os pital H os pital-
Alberta Surgical Fractured Hip Care Pathway Version 3: Last Updated February 9, 2018
 Alberta Surgical Fractured Hip Care Pathway Assessment / Pain Mngmt EMS Transport Neurovascular assessment Vital signs Pain assessment Splint only (no traction) Position of comfort Start IV and use appropriate
Alberta Surgical Fractured Hip Care Pathway Assessment / Pain Mngmt EMS Transport Neurovascular assessment Vital signs Pain assessment Splint only (no traction) Position of comfort Start IV and use appropriate
O3_A2_A_Scientific Evidence
 O3_A2_A_Scientific Evidence PERFORMING URETHROVESICAL CATHETERIZATION (FOLEY PROBE) IN FEMALE PATIENTS Q1 Outcome When is urinary catheterization necessary in patients hospitalized in a palliative settings/facility?
O3_A2_A_Scientific Evidence PERFORMING URETHROVESICAL CATHETERIZATION (FOLEY PROBE) IN FEMALE PATIENTS Q1 Outcome When is urinary catheterization necessary in patients hospitalized in a palliative settings/facility?
Nancy Hailpern, Director, Regulatory Affairs K Street, NW, Suite 1000 Washington, DC 20005
 Summary of Infection Prevention Issues in the Centers for Medicare & Medicaid Services (CMS) FY 2014 Inpatient Prospective Payment System (IPPS) Final Rule Hospital Readmissions Reduction Program-Fiscal
Summary of Infection Prevention Issues in the Centers for Medicare & Medicaid Services (CMS) FY 2014 Inpatient Prospective Payment System (IPPS) Final Rule Hospital Readmissions Reduction Program-Fiscal
ADULT CARDIAC SURGERY TELEMETRY BED TRANSFER ORDERS 1 of 4
 ADULT CARDIAC SURGERY TELEMETRY BED TRANSFER 1 of 4 9 Actual 9 Estimated Attending Surgeon: Medical Record Number Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART
ADULT CARDIAC SURGERY TELEMETRY BED TRANSFER 1 of 4 9 Actual 9 Estimated Attending Surgeon: Medical Record Number Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART
CAUTI CONFERENCE CAUTI Prevention and Appropriate Use of Indwelling Urinary Catheters in the Hospital Setting
 CAUTI CONFERENCE CAUTI Prevention and Appropriate Use of Indwelling Urinary Catheters in the Hospital Setting James T. Fields, MD Carolinas Center for Medical Excellence Columbia, South Carolina February
CAUTI CONFERENCE CAUTI Prevention and Appropriate Use of Indwelling Urinary Catheters in the Hospital Setting James T. Fields, MD Carolinas Center for Medical Excellence Columbia, South Carolina February
URINARY TRACT INFECTIONS: Focus on CA UTIs
 URINARY TRACT INFECTIONS: Focus on CA UTIs William A. Rutala, Ph.D., M.P.H. Director, Statewide Program for Infection Control and Epidemiology and Research Professor of Medicine, University of North Carolina
URINARY TRACT INFECTIONS: Focus on CA UTIs William A. Rutala, Ph.D., M.P.H. Director, Statewide Program for Infection Control and Epidemiology and Research Professor of Medicine, University of North Carolina
Post operative voiding dysfunction and the Value of Urodynamics. Dr Salwan Al-Salihi Urogynaecologist Obstetrician and Gynaecologist
 Post operative voiding dysfunction and the Value of Urodynamics Dr Salwan Al-Salihi Urogynaecologist Obstetrician and Gynaecologist Learning objectives: v Pathophysiology of post op voiding dysfunction.
Post operative voiding dysfunction and the Value of Urodynamics Dr Salwan Al-Salihi Urogynaecologist Obstetrician and Gynaecologist Learning objectives: v Pathophysiology of post op voiding dysfunction.
Surgical Site Infections: the international guidelines for best practices and effective actions
 Surgical Site Infections: the international guidelines for best practices and effective actions SSIs are the second most common type of adverse event occurring in hospitalised patients. SSIs have been
Surgical Site Infections: the international guidelines for best practices and effective actions SSIs are the second most common type of adverse event occurring in hospitalised patients. SSIs have been
AHRQ Safety Program for Long-term Care: HAIs/CAUTI. Training LTC Facility Staff on Catheter Insertion & Maintenance to Prevent CAUTIs
 AHRQ Safety Program for Long-term Care: HAIs/CAUTI Training LTC Facility Staff on Catheter Insertion & Maintenance to Prevent CAUTIs National Content Series for Facility Team Leads and Core Team Members
AHRQ Safety Program for Long-term Care: HAIs/CAUTI Training LTC Facility Staff on Catheter Insertion & Maintenance to Prevent CAUTIs National Content Series for Facility Team Leads and Core Team Members
Advances in Joint Replacement
 Advances in Joint Replacement Seth Greenky, MD Chairman, Musculoskeletal Services, St. Joseph s Hospital Partner, Syracuse Orthopedic Specialists Associate Clinical Professor, Upstate Medical Center CoMedical
Advances in Joint Replacement Seth Greenky, MD Chairman, Musculoskeletal Services, St. Joseph s Hospital Partner, Syracuse Orthopedic Specialists Associate Clinical Professor, Upstate Medical Center CoMedical
Measure Applications Partnership. Hospital Workgroup In-Person Meeting Follow- Up Call
 Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
The Impact of Clinical Decision Support (CDS) Tools on Catheter Associated Urinary Tract Infections (CAUTI) January 22, 2010.
 Tools on Catheter Associated Urinary Tract Infections (CAUTI) January 22, 2010.") 4 th Annual NDNQI Conference The Impact of Clinical Decision Support (CDS) Tools on Catheter Associated Urinary Tract Infections (CAUTI) January 22, 2010 UPMC St Margaret Bonnie B. Anton, MN RN antonbb@upmc.edu
4 th Annual NDNQI Conference The Impact of Clinical Decision Support (CDS) Tools on Catheter Associated Urinary Tract Infections (CAUTI) January 22, 2010 UPMC St Margaret Bonnie B. Anton, MN RN antonbb@upmc.edu
Slide 1. Slide 2. Slide 3. Bladder Management and Preventing CAUTI. Bladder management CAUTI prevention standards
 Slide 1 Bladder Management and Preventing CAUTI Diana Weinel, MS RN James A. Haley Veterans Hospital & Clinics Tampa, FL Florida State Association of Rehabilitation Nurses Conference May, 2018 Slide 2
Slide 1 Bladder Management and Preventing CAUTI Diana Weinel, MS RN James A. Haley Veterans Hospital & Clinics Tampa, FL Florida State Association of Rehabilitation Nurses Conference May, 2018 Slide 2
Our Commitment to Quality and Patient Safety Core Measures
 Calvert Memorial Hospital is committed to our community, with a focus on patient-centered care. High quality and safe patient care is not our goal, it is our priority. That means delivering the best possible
Calvert Memorial Hospital is committed to our community, with a focus on patient-centered care. High quality and safe patient care is not our goal, it is our priority. That means delivering the best possible
Possible Denominator Codes Applicable to OMS * Le Fort Fractures 21346, 21347, 21348, 21422, 21423, 21432, 21433, 21435, 21436
 2015 Individual PQRS s Eligible OMS #22: Perioperative Care: Discontinuation of Prophylactic Antibiotics (Non- Cardiac Procedures) Percentage of noncardiac surgical patients aged 18 years and older undergoing
2015 Individual PQRS s Eligible OMS #22: Perioperative Care: Discontinuation of Prophylactic Antibiotics (Non- Cardiac Procedures) Percentage of noncardiac surgical patients aged 18 years and older undergoing
CPT only copyright 2014 American Medical Association. All rights reserved. 12/23/2014 Page 66 of 593
 Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2015 PQRS OPTIONS FOR INDIVIDUAL MEASURES:
Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2015 PQRS OPTIONS FOR INDIVIDUAL MEASURES:
Sample. Fractured Hip Post-Operative Orders. Legend < Mandatory fields o Optional fields. Height Allergies: List or o Up to date in electronic system
 Legend Mandatory fields o Optional fields Height Allergies: List or o Up to date in electronic system cm Weight Diagnosis kg Date (yyyy-mon-dd) Time (hh:mm) Anticipated Date Of Discharge (ADOD) o Greater
Legend Mandatory fields o Optional fields Height Allergies: List or o Up to date in electronic system cm Weight Diagnosis kg Date (yyyy-mon-dd) Time (hh:mm) Anticipated Date Of Discharge (ADOD) o Greater
2017 Eligible Measure Applicability (EMA) for Registry Data Submission of Individual Quality Measures
 for Registry Data Submission of Individual Quality Measures") 2017 Eligible Measure Applicability (EMA) for Registry Data Submission of Individual Quality Measures 07/17/2017 Page 1 of 10 QPP Clinically Related Measure Analysis Used in EMA Clinical Relation including
2017 Eligible Measure Applicability (EMA) for Registry Data Submission of Individual Quality Measures 07/17/2017 Page 1 of 10 QPP Clinically Related Measure Analysis Used in EMA Clinical Relation including
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Surgical Consensus Standards Endorsement Maintenance NQF-Endorsed Surgical Maintenance Standards (Phase I) Table of Contents
 Table of Contents") Table of Contents #0113: Participation in a Systematic Database for Cardiac Surgery... 2 #0114: Post-operative Renal Failure... 2 #0115: Surgical Re-exploration... 3 #0116: Anti-Platelet Medication at
Table of Contents #0113: Participation in a Systematic Database for Cardiac Surgery... 2 #0114: Post-operative Renal Failure... 2 #0115: Surgical Re-exploration... 3 #0116: Anti-Platelet Medication at
IR Central Venous Access [ ] Pre Procedure
![IR Central Venous Access [ ] Pre Procedure](/thumbs/90/104119758.jpg "IR Central Venous Access [ ] Pre Procedure") IR Central Venous Access [1050200001] Pre Procedure Case Request/Scheduling Procedure Enter IR Case Request if not already completed (All hospitals except Grant Medical Center) [ ] Case Request IR Lab
IR Central Venous Access [1050200001] Pre Procedure Case Request/Scheduling Procedure Enter IR Case Request if not already completed (All hospitals except Grant Medical Center) [ ] Case Request IR Lab
Surgical Consensus Standards Endorsement Maintenance NQF-Endorsed Surgical Maintenance Standards (Phase II) Table of Contents
 Table of Contents") Table of Contents #0200: Death among surgical inpatients with treatable serious complications (failure to rescue)... 2 #0217: Surgery Patients with Recommended Venous Thromboembolism (VTE) Prophylaxis
Table of Contents #0200: Death among surgical inpatients with treatable serious complications (failure to rescue)... 2 #0217: Surgery Patients with Recommended Venous Thromboembolism (VTE) Prophylaxis
State of the State: Hospital Performance in Pennsylvania August 2010
 State of the State: Hospital Performance in Pennsylvania August 2010 Measuring Progress in PA Hospital Performance: Process Measures Quality Measures Analysis We reviewed the latest year-over-year changes
State of the State: Hospital Performance in Pennsylvania August 2010 Measuring Progress in PA Hospital Performance: Process Measures Quality Measures Analysis We reviewed the latest year-over-year changes
Assessment. Consults & Referrals
 University of Virginia Health System Clinical Pathway: Whipple Enhanced Recovery After () LOS: 4-5 days Date of Origin/Revision: June 29, 2016/September 6, 2017/January 31, 2018 : SAS : : : D1 D2 D 3/
University of Virginia Health System Clinical Pathway: Whipple Enhanced Recovery After () LOS: 4-5 days Date of Origin/Revision: June 29, 2016/September 6, 2017/January 31, 2018 : SAS : : : D1 D2 D 3/
CAUTI Timeline. SEPT: *Implementation Phase 1 OCT: *Foley insertion competency for 4 th RNs and FP. Awarded CAUTI Grant to purchase catheter hooks
 CAUTI Timeline Created CAUTI Computer Based Learning Module and Meditech Catheter care Intervention FEB: *Decision on which unit we would pilot *Created CAUTI Charter APRIL-MAY: *Began process for Foley
CAUTI Timeline Created CAUTI Computer Based Learning Module and Meditech Catheter care Intervention FEB: *Decision on which unit we would pilot *Created CAUTI Charter APRIL-MAY: *Began process for Foley
AMI 100% 80% 60% 40% 20% AMI: Aspirin at Arrival Targets AMI: Aspirin at D/C 2 - Aspirin at Discharge: Targets 100% 80% 60% 40% 20%
 AMI AMI: 1 - Aspirin at Arrival AMI: 2 - Aspirin at Discharge AMI: Aspirin at Arrival Targets AMI: Aspirin at D/C 2 - Aspirin at Discharge: Targets AMI: 3 - ACEI or ARB for LVSD AMI: 4 - Adult Smoking
AMI AMI: 1 - Aspirin at Arrival AMI: 2 - Aspirin at Discharge AMI: Aspirin at Arrival Targets AMI: Aspirin at D/C 2 - Aspirin at Discharge: Targets AMI: 3 - ACEI or ARB for LVSD AMI: 4 - Adult Smoking
Preventing CLABSI & CAUTI Preventive Measures for Central Line Associated Bloodstream Infection & Catheter Associated UTI
 Preventing CLABSI & CAUTI Preventive Measures for Central Line Associated Bloodstream Infection & Catheter Associated UTI Kaiser Permanente For Internal use only Objectives By the end of this lesson, you
Preventing CLABSI & CAUTI Preventive Measures for Central Line Associated Bloodstream Infection & Catheter Associated UTI Kaiser Permanente For Internal use only Objectives By the end of this lesson, you
1 of 5. Integrated Order Set Inpatient, Adult. Gynecological Surgery Enhanced Recovery Orders apply to patients 18 years and older.
 Orders apply to patients 18 years and older. All preprinted doses are based on normal renal and hepatic function and must be assessed for adjustment against the individual patient s renal and hepatic function
Orders apply to patients 18 years and older. All preprinted doses are based on normal renal and hepatic function and must be assessed for adjustment against the individual patient s renal and hepatic function
ST. DOMINIC-JACKSON MEMORIAL HOSPITAL JACKSON, MISSISSIPPI
 Date & Time TAVR Pre-Op Admission Clinical Pathway Page 1 of 3 1. Admit as INPATIENT to Dr.. For Surgery Today or Tomorrow 3. Diagnosis: 4. Allergies: Pharmacy Mnemonic: PRETAVR 5. Vital signs on arrival.
Date & Time TAVR Pre-Op Admission Clinical Pathway Page 1 of 3 1. Admit as INPATIENT to Dr.. For Surgery Today or Tomorrow 3. Diagnosis: 4. Allergies: Pharmacy Mnemonic: PRETAVR 5. Vital signs on arrival.
Keeping Up with the Regulatory Requirements and Other Hocus Pocus. Vicky A. Mahn-DiNicola RN, MS, CPHQ Vice President and Product Manager ACS MIDAS+
 Keeping Up with the Regulatory Requirements and Other Hocus Pocus Vicky A. Mahn-DiNicola RN, MS, CPHQ Vice President and Product Manager ACS MIDAS+ Session Objectives Review Medicare s proposed strategies
Keeping Up with the Regulatory Requirements and Other Hocus Pocus Vicky A. Mahn-DiNicola RN, MS, CPHQ Vice President and Product Manager ACS MIDAS+ Session Objectives Review Medicare s proposed strategies
2016 Physician Quality Reporting System Data Collection Form: Coronary Artery Bypass Graft (CABG) (for patients aged 18 years and older)
 (for patients aged 18 years and older)") 2016 Physician Quality Reporting System Data Collection Form: Coronary Artery Bypass Graft (CABG) (for patients aged 18 years and older) IMPORTANT: Any measure with a 0% performance rate (100% for inverse
2016 Physician Quality Reporting System Data Collection Form: Coronary Artery Bypass Graft (CABG) (for patients aged 18 years and older) IMPORTANT: Any measure with a 0% performance rate (100% for inverse
Hospital Compare Quality Measures: 2011 National and Tennessee Results for Critical Access Hospitals
 March 2013 Hospital Compare Quality Measures: 2011 National and Results for Critical Access Michelle Casey, MS, Peiyin Hung, MSPH, Maeve McClellan, BS, Ira Moscovice, PhD, University of Minnesota Rural
March 2013 Hospital Compare Quality Measures: 2011 National and Results for Critical Access Michelle Casey, MS, Peiyin Hung, MSPH, Maeve McClellan, BS, Ira Moscovice, PhD, University of Minnesota Rural
Enhanced Recovery Thoracic Surgery. Esophagus Pathway
 Enhanced Recovery Thoracic Surgery Esophagus Pathway Preoperative Patient Education/Expectations for Hospital and Home Medical Risk Consultation: Cardiac Clearance and PFTs for All Patients Surgery Wellness
Enhanced Recovery Thoracic Surgery Esophagus Pathway Preoperative Patient Education/Expectations for Hospital and Home Medical Risk Consultation: Cardiac Clearance and PFTs for All Patients Surgery Wellness
DENOMINATOR: All surgical patients aged 18 years and older undergoing procedures for which VTE prophylaxis is indicated in all patients
 Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES:
Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES:
Tied with pneumonia as the second most common type of healthcareassociated
 Tied with pneumonia as the second most common type of healthcareassociated infection. > 15% of HAIs reported to NHSN Estimated > 560,000 nosocomial UTIs annually Increased morbidity & mortality Estimated
Tied with pneumonia as the second most common type of healthcareassociated infection. > 15% of HAIs reported to NHSN Estimated > 560,000 nosocomial UTIs annually Increased morbidity & mortality Estimated
Proof 2. CLINICAL PATHWAY PLAN CLINIQUE GENERAL SURGERY CHIRURGIE GÉNÉRAL Enhanced Recovery After Surgery (ERAS) Bowel Surgery /
 Bowel Surgery /") CLINICAL PATHWAY PLAN CLINIQUE GENERAL SURGERY CHIRURGIE GÉNÉRAL Enhanced Recovery After Surgery (ERAS) Bowel Surgery / Proof 2 Addressograph/Plaque Cancer Assessment Clinic (CAC) Date: yyaa mm dj Day
CLINICAL PATHWAY PLAN CLINIQUE GENERAL SURGERY CHIRURGIE GÉNÉRAL Enhanced Recovery After Surgery (ERAS) Bowel Surgery / Proof 2 Addressograph/Plaque Cancer Assessment Clinic (CAC) Date: yyaa mm dj Day
Admit date (YYYY/MM/DD): Cardiologist On-Call: Diagnosis: Lab Tests. CBC, Electrolytes, Urea, Creatinine, Glucose, INR, PTT, Urinalysis
: Cardiologist On-Call: Diagnosis: Lab Tests. CBC, Electrolytes, Urea, Creatinine, Glucose, INR, PTT, Urinalysis") of nurse 1. Admit under ward Attending Physician: Dr. Admit date (YYYY/MM/DD): Cardiologist On-Call: Diagnosis: Lab Tests 2. On admission (if not already performed in Emergency Department or in Coronary
of nurse 1. Admit under ward Attending Physician: Dr. Admit date (YYYY/MM/DD): Cardiologist On-Call: Diagnosis: Lab Tests 2. On admission (if not already performed in Emergency Department or in Coronary
Nurse-Initiated Removal of Unnecessary Urinary Catheters in the Non-Intensive Care Units
 Nurse-Initiated Removal of Unnecessary Urinary Catheters in the Non-Intensive Care Units (Based on a study performed at St. John Hospital and Medical Center in Detroit, Michigan) November 2010 This toolkit
Nurse-Initiated Removal of Unnecessary Urinary Catheters in the Non-Intensive Care Units (Based on a study performed at St. John Hospital and Medical Center in Detroit, Michigan) November 2010 This toolkit
Core = Core required measures for all CAH nationally r = Required by State of Minnesota X = Additional for MBQIP
 Key: 2016 Hospital Measure Summary Minnesota Statewide Quality eporting and Measurement System (SQMS) and FY2018 for Center for Medicare and Medicaid Services () January 2016 = equired by Core = Core required
Key: 2016 Hospital Measure Summary Minnesota Statewide Quality eporting and Measurement System (SQMS) and FY2018 for Center for Medicare and Medicaid Services () January 2016 = equired by Core = Core required
LONG TERM CARE FACILITY ADMIT ORDERS
 Page 1 of 7 LONG TERM CARE FACILITY ADMIT ORDERS ADMISSION: Admit patient to Skilled Nursing Facility: Admit patient to Acute Rehabilitation Facility: Admit patient to Subacute Rehabilitation Facility:
Page 1 of 7 LONG TERM CARE FACILITY ADMIT ORDERS ADMISSION: Admit patient to Skilled Nursing Facility: Admit patient to Acute Rehabilitation Facility: Admit patient to Subacute Rehabilitation Facility:
Initials * Page 1 of 6. (place patient label here) Patient Name: Diagnosis: Allergies with reaction type:
 Patient Name: Diagnosis: Allergies with reaction type:") Patient Name: Diagnosis: Allergies with reaction type: Orthopedic Upper Ext Post Op Version 3 4/20/17 Patient Placement General Diagnosis/Procedure: Preferred Location/Unit Ortho/Neuro General Medical
Patient Name: Diagnosis: Allergies with reaction type: Orthopedic Upper Ext Post Op Version 3 4/20/17 Patient Placement General Diagnosis/Procedure: Preferred Location/Unit Ortho/Neuro General Medical
Bariatric Surgery Post Op Plan PACU Phase
 Bariatric Surgery Post Op Plan PACU Phase PHYSICIAN S Weight Allergies Admit/Discharge/Transfer Patient Status Pt Status: Inpatient (LOS > 2 midnights) Pt Status: Observation (LOS < 2 midnights) Code Status
Bariatric Surgery Post Op Plan PACU Phase PHYSICIAN S Weight Allergies Admit/Discharge/Transfer Patient Status Pt Status: Inpatient (LOS > 2 midnights) Pt Status: Observation (LOS < 2 midnights) Code Status
Hip Hemiarthroplasty Post Op Version 2 4/20/17
 Patient Name: Diagnosis: Allergies with reaction type: Hip Hemiarthroplasty Post Op Version 2 4/20/17 Patient Placement General Diagnosis/Procedure: Preferred Location/Unit Ortho/Neuro PCU ICU General
Patient Name: Diagnosis: Allergies with reaction type: Hip Hemiarthroplasty Post Op Version 2 4/20/17 Patient Placement General Diagnosis/Procedure: Preferred Location/Unit Ortho/Neuro PCU ICU General