Foamy Urine and Sickled Cells. Margaret Prat Huntwork, MD, MSEd Tulane / Ochsner Residency Program New Orleans, LA
|
|
|
- Dwayne Barrett
- 5 years ago
- Views:
Transcription
1 Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane / Ochsner Residency Program New Orleans, LA

2
3
4
5


6
7 Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane University Health Sciences Center New Orleans, LA
8 History of Present Illness A 19 year-old girl with known sickle cell disease (Hgb SS) presented with one day of lower back and bilateral thigh pain. Symptoms were typical of her usual pain crisis.
9 Review of Systems Foamy urine. Facial swelling. Decreased appetite. One episode of vomiting. Feels dizzy when standing up rapidly. No shortness of breath, no cough, no fever, no chest pain, no focal weakness.
10 Past Medical History Hemoglobin SS Disease, with history of vaso-occlusive crises, but no acute chest, stroke, avascular necrosis, or any other known complications. Crigler-Najjar Type 2 Two recent ER visits for vaso-occulsive crises, and one recent hospitalization for pneumonia.
11 Additional History No surgeries. Family history significant for sickle cell trait. Lives with her mother, is studying to be a respiratory therapist. Denies alcohol, drug use, tobacco use.
12 Folic acid Amoxicillin Medications Tylenol with codeine Phenobarbital Chart review: she had received ten doses of ketorolac over the past month, at ER visits, clinic visits, and from her last hospital admission.
13 Physical Exam T: 97.5 HR: 108 RR: 12 BP: 116/74 O2: 100% +Orthostatic hypotension HEENT: Mild scleral icterus CV: tachycardic, regular rhythm Pulm: clear to auscultation Abd: nontender, no organomegaly Ext: Anasarca present, including periorbital and facial edema, edema of hands and feet. Full ROM of extremities, no tenderness to palpation.
14 Laboratory Studies Complete blood count demonstrated a white blood cell count of 18,000 per mm3, hemoglobin of 5.7 mg/dl (baseline is ~7), and a reticulocyte count of 10%. Chemistry was significant for a blood urea nitrogen of 43 mg/dl, a creatinine of 3.6 mg/dl (baseline is 0.5 mg/dl). Bicarbonate level was 17 mmol/l. Liver function tests revealed an albumin of 1.3 g/dl and a total bilirubin of 3 mg/dl (baseline is ~2). Urinalysis showed a protein greater than 500 mg/dl. Spot urine protein-to-creatinine ratio was 27. (Nephrotic range proteinuria is greater than 5.)
15 Diagnosis Given the patient s elevated creatinine, high urine protein-to-creatinine ratio, hypoalbuminemia, and generalized edema, she was diagnosed with acute kidney injury due to nephrotic syndrome. What is the etiology of the patient s nephrotic syndrome: is it secondary to sickle cell disease or another cause? Or is it a primary nephrotic syndrome?
16 Nephrotic Syndrome: A Differential diagnosis Primary Glomerular Disease FSGS Membranous Nephropathy Minimal Change Disease Membranoproliferative GN Secondary to a systemic disease DM Hepatitis Sickle Cell SLE Amyloidosis Cryoglobulinemia
17 Miscellaneous Labs Complement levels were normal, making immune complex disease causing membranoproliferative nephropathy less likely. ANA was negative, making SLE causing membranous nephropathy less likely. Hepatitis and syphilis serologies were negative, ruling out infection causing a membranous nephropathy.
18
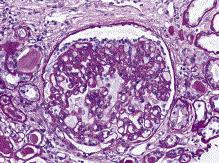
19 Renal Biopsy Light microscopy demonstrated focal segmental glomerulosclerosis. Electron microscopy revealed widespread areas of complete podocyte effacement. There was not enough tissue to perform immune staining.
20
21 She was ultimately diagnosed with focal segmental glomerulosclerosis with notable podocyte effacement. FSGS is a known complication of sickle cell disease. So, it doesn t matter that the patient got 10 doses of ketorolac over the past month?
22 Discussion
23 Discussion Outline 1. Why this patient is a set-up for renal injury. 2. Sickle cell disease and nephrotic syndrome. 3. NSAIDs and nephrotic syndrome.
24 1. A Set-Up for Renal Injury? Our patient had multiple risk factors for development of acute kidney injury: presence of sickle cell disease recent pneumonia state of volume depletion history of multiple vaso-occlusive crises in a short time span too many doses of ketorolac in the last month
25 2. Sickle Cell Disease and Nephrotic Syndrome Vaso-occlusive Crisis Sickle cell crisis is associated with a decrease in creatinine clearance with return to baseline demonstrated around four weeks after the episode, suggesting a mechanism of transient glomerular dysfunction during acute episodes.
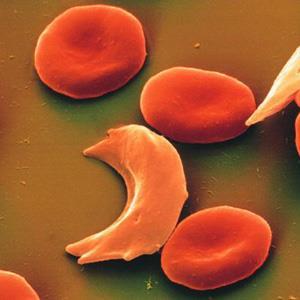
26 2. Sickle Cell Disease and Nephrotic Syndrome Sickle cell disease can cause a nephrotic picture entirely on its own. Altered regulation of vasoconstrictive and vasodilatory cytokines cause decreased systemic resistance and increased renal blood flow. Increased renal blood flow causes hyperfiltration at the glomerular level. Hyperfiltration results in an increased GFR and lower serum creatinine. Chronic glomerular hyperperfusion can lead to glomerular injury or glomerulosclerosis thus leading to development of proteinuria. While the renal cortex is hyperperfused, the medulla is hypoperfused. A hypertonic, hypoxic, acidotic environment sickles RBCs, slows flow in the vasa recta, and can cause infarcts resulting in painless hematuria.
27 3. NSAIDs and Renal Injury Acute kidney injury resulting from NSAID use is well documented in the adult literature. In children, NSAID-induced acute kidney injury often occurs in conjunction with other comorbid conditions (i.e. sickle cell disease, volume depletion) which likely increase a patient s susceptibility to the nephrotoxic effects.
28 3. NSAIDs and Renal Injury NSAIDs inhibit cyclooxygenase and decrease prostaglandin production. Prostaglandins mediate vasodilation of the afferent arteriole. Decreased prostaglandin production causes decreased renal blood flow, decreased GFR, and this can cause ischemic injury and acute tubular necrosis. In the case of glomerular disease, NSAIDs cause acute kidney injury and minimal change disease as a direct toxic effect of therapy.
29 3. NSAIDs and Renal Injury Acute kidney injury (hemodynamically-mediated or acute tubular necrosis) Acute interstitial nephritis Nephrotic syndrome (minimal change disease or membranous nephropathy) Hyponatremia Hyperkalemia/type 4 renal tubular acidosis Hypertension/edema Acute papillary necrosis Chronic tubulointerstitial nephritis/analgesic nephropathy Uroepithelial malignancy

30
31 NSAIDs and Sickle Cell NSAID use is a common practice in acute episodes of vasoocclusive crisis associated with sickle cell disease. They are on many pre-printed order sheets for sickle cell pain crises. Ketorolac has an opiate-like efficacy and the additional benefit of being parenterally administered. Use of NSAIDs has decreased risk of respiratory depression and other central nervous system adverse effects. There is also a lower addictive potential. NHLBI states that, due to the need for more safety data, the current recommendation is that ketorolac should not be used by any route or combination of routes for longer than 5 days in a given month because of the increased risk of toxicity.
32 NSAIDs causing AKI and nephrotic syndrome Our Patient Glomerular injury due to sickle cell nephropathy Multiple consecutive vaso-occlusive crisis Volume depletion
33 What to do now? In a patient with frequent vasoocclusive pain crises, clinicians should carefully monitor frequency and dosing of NSAIDs because there is risk for developing nephrotic syndrome and acute renal failure in the sickle cell population.
34 Special Thanks Dr. Yosypiv Dr. El-Dahr Dr. Singleton Dr. Chavan Dr. DeBord Dr. Meghan Howell and Dr. Jessica May
35
36 References The Management of Sickle Cell Disease. NHLBI. NIH Publication No Fourth Edition. June Accessed online Aug Ender, et al. Use of a clinical pathway to improve the acute management of vaso-occlusive crisis in pediatric sickle cell disease. Pediatric Blood & Cancer Apr; 61(4): Management of Acute Pain in Pediatric Patient s with Sickle Cell Disease. New England Pediatric Sickle Cell Consortium. March Accessed online Aug Hardwick WE et al. Effect of ketorolac in pediatric sickle cell vaso-occlusive pain crisis. Pediatr Emerg Care 1999 Jun; 15(3): Wright SW, et al. Ketorolac for sickle cell vaso-occlusive crisis pain in the emergency department: lack of a narcotic-sparing effect. Ann Emerg Med Aug; 21(8):
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Nephrotic Syndrome. Sara Alsharhan PharmD candidate, KSU 2014
 Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Diabetes, Obesity and Heavy Proteinuria
 Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Evaluation and Management of Proteinuria. Negiin Pourafshar, MD University of Virginia Division of Nephrology
 Evaluation and Management of Proteinuria Negiin Pourafshar, MD University of Virginia Division of Nephrology Case A 30-year-old man, is turned down for life insurance because of the presence of an unspecified
Evaluation and Management of Proteinuria Negiin Pourafshar, MD University of Virginia Division of Nephrology Case A 30-year-old man, is turned down for life insurance because of the presence of an unspecified
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS. Myriam Farah, MD, FRCPC
 ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
Acute Kidney Injury. I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS
 Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
GOOD MORNING. Welcome Applicants! Friday, October 31, (Happy Halloween!)
") GOOD MORNING Welcome Applicants! Friday, October 31, 2014 (Happy Halloween!) PREP QUESTION A 14-year-old girl has had 3 days of new, unremitting headache associated with vomiting and awakening from sleep
GOOD MORNING Welcome Applicants! Friday, October 31, 2014 (Happy Halloween!) PREP QUESTION A 14-year-old girl has had 3 days of new, unremitting headache associated with vomiting and awakening from sleep
Nephritic vs. Nephrotic Syndrome
 Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Clinical Case Presentation. Dana Assis, MD
 Clinical Case Presentation Dana Assis, MD 4.12.2016 Clinical Presentation 63 year old male with medical history AIDS (CD4 11, VL 62K), Hep C cirrhosis (never treated), DM II c/b diabetic retinopathy, HTN,
Clinical Case Presentation Dana Assis, MD 4.12.2016 Clinical Presentation 63 year old male with medical history AIDS (CD4 11, VL 62K), Hep C cirrhosis (never treated), DM II c/b diabetic retinopathy, HTN,
Proteinuria DR. SANJAY PANDEYA MD. FRCPC.
 Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
Special Challenges and Co-Morbidities
 Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
MHD I SESSION X. Renal Disease
 MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
CASE OF THE WEEK 1
 www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
Nephrotic syndrome in children. Bashir Admani KPA Nephrology Precongress 24/4/2018
 Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management
 Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management") AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
Documentation Dissection
 History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
C-Star Case Studies: Block D AKI-CKD - Prerenal/Intra-Renal/Post-renal. Setting: ER ID: 61-year-old female of African American Origin
 C-Star Case Studies: Block D AKI-CKD - Prerenal/Intra-Renal/Post-renal Setting: ER ID: 61-year-old female of African American Origin Reasons for visit: Feeling tired, with an itch all over the body HPI:
C-Star Case Studies: Block D AKI-CKD - Prerenal/Intra-Renal/Post-renal Setting: ER ID: 61-year-old female of African American Origin Reasons for visit: Feeling tired, with an itch all over the body HPI:
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Mr. I.K 58 years old
 Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
11/9/2015. Childhood Nephrotic Syndrome: The Clinical Pathway. Learning Objectives. Nephrotic Syndrome - Definition. Proteinuria.
 Childhood Nephrotic Syndrome: The Clinical Pathway Cherry Mammen, MD, FRCPC, MHSc Douglas G. Matsell, MDCM, FRCPC Division of Nephrology, BC Children s Hospital Grand Rounds Nov 13th, 2015 Learning Objectives
Childhood Nephrotic Syndrome: The Clinical Pathway Cherry Mammen, MD, FRCPC, MHSc Douglas G. Matsell, MDCM, FRCPC Division of Nephrology, BC Children s Hospital Grand Rounds Nov 13th, 2015 Learning Objectives
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
Case Studies: Renal and Urologic Impairments Workshop
 Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
CKD FOR INTERNISTS. Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College
 CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
Acute kidney injury definition, causes and pathophysiology. Financial Disclosure. Some History Trivia. Key Points. What is AKI
 Acute kidney injury definition, causes and pathophysiology Financial Disclosure Current support: Center for Sepsis and Critical Illness Award P50 GM-111152 from the National Institute of General Medical
Acute kidney injury definition, causes and pathophysiology Financial Disclosure Current support: Center for Sepsis and Critical Illness Award P50 GM-111152 from the National Institute of General Medical
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
PRE-RENAL AKI: DOES IT LEAD TO ATN. Sushma Bhusal
 PRE-RENAL AKI: DOES IT LEAD TO ATN Sushma Bhusal 9.9.14 CASE PRESENTATION CC : 31 AAM presented with Fatigue, malaise and body aches x 10 days HPI: STD testing done 2 weeks prior, all results negative
PRE-RENAL AKI: DOES IT LEAD TO ATN Sushma Bhusal 9.9.14 CASE PRESENTATION CC : 31 AAM presented with Fatigue, malaise and body aches x 10 days HPI: STD testing done 2 weeks prior, all results negative
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s. Part 1: Clinical
 Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
** Accordingly GFR can be estimated by using one urine sample and do creatinine testing.
 This sheet includes the lecture and last year s exam. When a patient goes to a clinic, we order 2 tests: 1) kidney function test: in which we measure UREA and CREATININE levels, and electrolytes (Na+,
This sheet includes the lecture and last year s exam. When a patient goes to a clinic, we order 2 tests: 1) kidney function test: in which we measure UREA and CREATININE levels, and electrolytes (Na+,
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University
 RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)
Nephrotic Syndrome NS
 Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
DIABETES MELLITUS. Kidney in systemic diseases. Slower the progression: Pathology: Patients with diabetes mellitus are prone to other renal diseases:
 Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
II.Tubulointerstitial diseases
 II.Tubulointerstitial diseases two major groups of processes (1) ischemic or toxic tubular injury, leading to acute kidney injury (AKI) and acute renal failure, and (2) inflammatory reactions of the tubules
II.Tubulointerstitial diseases two major groups of processes (1) ischemic or toxic tubular injury, leading to acute kidney injury (AKI) and acute renal failure, and (2) inflammatory reactions of the tubules
ENAL VEIN ROMBOSIS WHAT WAS IT? DR.JANANI SANKAR UNIT DR. KEDARI NAGARJUNA, DNB P KKCTH
 ENAL VEIN ROMBOSIS WHAT WAS IT? DR.JANANI SANKAR UNIT DR. KEDARI NAGARJUNA, DNB P KKCTH RESENTING COMPLAINTS: u 9 ¾ yrs, boy u Fever, Loose stools 10 days back u Right sided Abdominal pain+ NVESTIGATIONS
ENAL VEIN ROMBOSIS WHAT WAS IT? DR.JANANI SANKAR UNIT DR. KEDARI NAGARJUNA, DNB P KKCTH RESENTING COMPLAINTS: u 9 ¾ yrs, boy u Fever, Loose stools 10 days back u Right sided Abdominal pain+ NVESTIGATIONS
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications.
 Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
Management of Nephrotic Syndrome
 Management of Nephrotic Syndrome 1. Introduction Incidence 2-4/100,000. Boys > girls 3:2; age of onset 2-6 years 80% of cases in children is due to minimal change (MCD) of which 80% will respond to steroid
Management of Nephrotic Syndrome 1. Introduction Incidence 2-4/100,000. Boys > girls 3:2; age of onset 2-6 years 80% of cases in children is due to minimal change (MCD) of which 80% will respond to steroid
Biomarkers of renal diseases. By Dr. Gouse Mohiddin Shaik
 By Dr. Gouse Mohiddin Shaik Introduction Renal system performs several functions Excretory Waste products like urea, creatinine, drug, toxins clearance Regulatory Water, electrolyte and acid base balance
By Dr. Gouse Mohiddin Shaik Introduction Renal system performs several functions Excretory Waste products like urea, creatinine, drug, toxins clearance Regulatory Water, electrolyte and acid base balance
Steroid Resistant Nephrotic Syndrome. Sanjeev Gulati, Debashish Sengupta, Raj K. Sharma, Ajay Sharma, Ramesh K. Gupta*, Uttam Singh** and Amit Gupta
 Steroid Resistant Nephrotic Syndrome Sanjeev Gulati, Debashish Sengupta, Raj K. Sharma, Ajay Sharma, Ramesh K. Gupta*, Uttam Singh** and Amit Gupta From the Departments of Nephrology, Pathology* and Biostatistics**,
Steroid Resistant Nephrotic Syndrome Sanjeev Gulati, Debashish Sengupta, Raj K. Sharma, Ajay Sharma, Ramesh K. Gupta*, Uttam Singh** and Amit Gupta From the Departments of Nephrology, Pathology* and Biostatistics**,
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Renal Transporters- pathophysiology of drug - induced renal disorders. Lisa Harris, Pharmacist, John Hunter Hospital, Newcastle, 2015 November
 Renal Transporters- pathophysiology of drug - induced renal disorders Lisa Harris, Pharmacist, John Hunter Hospital, Newcastle, 2015 November Renal Failure Up to 25% of acute renal failure is drug induced
Renal Transporters- pathophysiology of drug - induced renal disorders Lisa Harris, Pharmacist, John Hunter Hospital, Newcastle, 2015 November Renal Failure Up to 25% of acute renal failure is drug induced
Paediatrics Dr. Bakr Lecture 3 Nephrotic Syndrome
 P a g e 1 DEFINITION Paediatrics Dr. Bakr Lecture 3 Nephrotic Syndrome Definition: nephrotic syndrome is a disorder characterized by heavy proteinuria with hypoprpteinimia,hyper lipidemia and edema. It
P a g e 1 DEFINITION Paediatrics Dr. Bakr Lecture 3 Nephrotic Syndrome Definition: nephrotic syndrome is a disorder characterized by heavy proteinuria with hypoprpteinimia,hyper lipidemia and edema. It
CHAPTER 4. Paediatric Renal Biopsies
 2nd Report of the Malaysian Registry of Renal Biopsy 2008 PAEDIATRIC RENAL BIOPSIES CHAPTER 4 Paediatric Renal Biopsies Lee Ming Lee Lim Yam Ngo Lynster Liaw Susan Pee Wan Jazilah Wan Ismail Yap Yok Chin
2nd Report of the Malaysian Registry of Renal Biopsy 2008 PAEDIATRIC RENAL BIOPSIES CHAPTER 4 Paediatric Renal Biopsies Lee Ming Lee Lim Yam Ngo Lynster Liaw Susan Pee Wan Jazilah Wan Ismail Yap Yok Chin
Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome. Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium
 Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium Objectives Discuss the pathophysiology of thrombosis in nephrotic
Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium Objectives Discuss the pathophysiology of thrombosis in nephrotic
Introduction to Clinical Diagnosis Nephrology
 Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER
: 30 YEARS LATER") HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER Gaston Zilleruelo M.D. Professor of Pediatrics Director of Pediatric Nephrology University of Miami/Holtz Children s Hospital Worldwide 33.2 million
HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER Gaston Zilleruelo M.D. Professor of Pediatrics Director of Pediatric Nephrology University of Miami/Holtz Children s Hospital Worldwide 33.2 million
Hepatorenal Syndrome
 Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
Clinical Significance of ARF. Hospital Acquired Renal Insufficiency. Case - Acute Renal Failure. Hospital Acquired Renal Insufficiency
 Case - Acute Renal Failure 73 yo diabetic F w hx of mild HBP but normal renal function develops infection of R foot. Over 1 week fever, chills, inflammation swelling of her R foot and leg. She takes Motrin
Case - Acute Renal Failure 73 yo diabetic F w hx of mild HBP but normal renal function develops infection of R foot. Over 1 week fever, chills, inflammation swelling of her R foot and leg. She takes Motrin
Glomerular Diseases. Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology
 Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
Diabetic Nephropathy
 Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Nephrotic Syndrome. Department of pediatrics The first affiliated hospital Sun Yat Sen University. Yue Zhihui ( 岳智慧 )
") Nephrotic Syndrome Department of pediatrics The first affiliated hospital Sun Yat Sen University Yue Zhihui ( 岳智慧 ) yuezhihui810@yahoo.com.cn Contents Definition Pathophysiology Clinical manifestation
Nephrotic Syndrome Department of pediatrics The first affiliated hospital Sun Yat Sen University Yue Zhihui ( 岳智慧 ) yuezhihui810@yahoo.com.cn Contents Definition Pathophysiology Clinical manifestation
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to
 Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
PATTERNS OF RENAL INJURY
 PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
Sickle cell disease, nephrotic syndrome, and renal failure
 the renal consult http://www.kidney-international.org & 2006 International Society of Nephrology Sickle cell disease, nephrotic syndrome, and renal failure SH Nasr 1, GS Markowitz 1, RL Sentman 2 and VD
the renal consult http://www.kidney-international.org & 2006 International Society of Nephrology Sickle cell disease, nephrotic syndrome, and renal failure SH Nasr 1, GS Markowitz 1, RL Sentman 2 and VD
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Dialyzing challenging patients: Patients with hepato-renal conditions
 Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Dr P Sigwadi 30 May 2012
 Dr P Sigwadi 30 May 2012 Introduction Haematuria Positive blood on urine dipstick 5 red blood cells/ microliter of urine Prevalence Gross haematuria ( macroscopic) 0.13 % Microscopic- 1.5% Haematuria +
Dr P Sigwadi 30 May 2012 Introduction Haematuria Positive blood on urine dipstick 5 red blood cells/ microliter of urine Prevalence Gross haematuria ( macroscopic) 0.13 % Microscopic- 1.5% Haematuria +
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Update on HIV-Related Kidney Diseases. Agenda
 Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Education Visit #1 *** All Sickle Cell Patients*** from A Parent s Handbook for Sickle Cell Disease Booklet.
 Education Visit #1 *** All Sickle Cell Patients*** Step 1: Administer Pretest A. Step 2: Education Watch DVD: Education Visit #1 For All Patients Handout So You Have Sickle Cell Disorder Handout Infection
Education Visit #1 *** All Sickle Cell Patients*** Step 1: Administer Pretest A. Step 2: Education Watch DVD: Education Visit #1 For All Patients Handout So You Have Sickle Cell Disorder Handout Infection
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009
 Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
changes that occur in kidney with aging is THE MOST DRAMATIC ANY ORGAN SYSTEM.
 The Kidney in Aging The the OF OF changes that occur in kidney with aging is THE MOST DRAMATIC ANY ORGAN SYSTEM. Age related charges in kidney structure and function At age 2 GFR at adult level. Reamins
The Kidney in Aging The the OF OF changes that occur in kidney with aging is THE MOST DRAMATIC ANY ORGAN SYSTEM. Age related charges in kidney structure and function At age 2 GFR at adult level. Reamins
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
High Impact Rheumatology
 High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
The kidneys of patients with SCD are susceptible to structural and functional abnormalities affecting many parts of the nephron.
 9. RENAL COMPLICATIONS Principles To institute methods of primary prevention for renal complications. To monitor for and identify renal complications in a timely manner. To effectively prevent progression
9. RENAL COMPLICATIONS Principles To institute methods of primary prevention for renal complications. To monitor for and identify renal complications in a timely manner. To effectively prevent progression
5/10/2014. Observation, control of blood pressure. Observation, control of blood pressure and risk factors.
 Overview The Kidneys Nicola Barlow Clinical Biochemistry Department City Hospital Renal physiology Renal pathophysiology Acute kidney injury Chronic kidney disease Assessing renal function GFR Proteinuria
Overview The Kidneys Nicola Barlow Clinical Biochemistry Department City Hospital Renal physiology Renal pathophysiology Acute kidney injury Chronic kidney disease Assessing renal function GFR Proteinuria
Proteinuria Nephrotic syndrome
 Proteinuria Nephrotic syndrome Pathophysiology & management Miriam Davidovits, MD Institute of Nephrology Schneider Children s Medical Center of Israel 1 Abnormal excretion of protein into the urine is
Proteinuria Nephrotic syndrome Pathophysiology & management Miriam Davidovits, MD Institute of Nephrology Schneider Children s Medical Center of Israel 1 Abnormal excretion of protein into the urine is
CASE-BASED SMALL GROUP DISCUSSION
 MHD I, Session 13, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION SESSION 13 MHD I Autoimmunity November 10, 2016 STUDENT COPY MHD I, Session 13, STUDENT Copy Page 2 Case 1 CHIEF COMPLAINT: I am
MHD I, Session 13, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION SESSION 13 MHD I Autoimmunity November 10, 2016 STUDENT COPY MHD I, Session 13, STUDENT Copy Page 2 Case 1 CHIEF COMPLAINT: I am
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Diabetes Case Study: Co-morbidity of Nonadherence
 Diabetes Case Study: Co-morbidity of Nonadherence Maureen Dever, MSN, CRNP, PPCNP.BC, CDE PENS 5/18 Comorbidity of Diabetes Case Study Objective: the learner will discuss an underreported comorbidity of
Diabetes Case Study: Co-morbidity of Nonadherence Maureen Dever, MSN, CRNP, PPCNP.BC, CDE PENS 5/18 Comorbidity of Diabetes Case Study Objective: the learner will discuss an underreported comorbidity of
Glomerular Disease. January 16, Katharine Dahl, MD
 Glomerular Disease January 16, 2018 Katharine Dahl, MD kdahl@akdhc.com Glomerular Disease Nomenclature Diffuse >50% glomeruli ---- Focal
Glomerular Disease January 16, 2018 Katharine Dahl, MD kdahl@akdhc.com Glomerular Disease Nomenclature Diffuse >50% glomeruli ---- Focal
Clinical pathological correlations in AKI
 Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Faculty/Presenter Disclosure
 CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
Tenth Visit posttest
 Test Code 10C Patient s name: Tenth Visit posttest Patient s birth date: Your name and relationship to patient: Today s date: 1. Which one of the medications listed below should every child with a sickle
Test Code 10C Patient s name: Tenth Visit posttest Patient s birth date: Your name and relationship to patient: Today s date: 1. Which one of the medications listed below should every child with a sickle
Chronic Kidney Disease for the Primary Care Physician in What do the Kidneys do? CKD in the US
 1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
Diabetes Case Study: Co-morbidity of Nonadherence Maureen Dever, MSN, CRNP, PPCNP.BC, CDE PENS 5/18
 Diabetes Case Study: Co-morbidity of Nonadherence Maureen Dever, MSN, CRNP, PPCNP.BC, CDE PENS 5/18 Comorbidity of Diabetes Case Study Objective: the learner will discuss an underreported comorbidity of
Diabetes Case Study: Co-morbidity of Nonadherence Maureen Dever, MSN, CRNP, PPCNP.BC, CDE PENS 5/18 Comorbidity of Diabetes Case Study Objective: the learner will discuss an underreported comorbidity of
Proteinuria Nephrotic syndrome
 Proteinuria Nephrotic syndrome Pathophysiology & management Miriam Davidovits, MD Institute of Nephrology Schneider Children s Medical Center of Israel 1 Abnormal excretion of protein into the urine is
Proteinuria Nephrotic syndrome Pathophysiology & management Miriam Davidovits, MD Institute of Nephrology Schneider Children s Medical Center of Israel 1 Abnormal excretion of protein into the urine is
Agenda. Management of Accelerated Hypertension (Updated in 2017) Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 2/27/2017
 Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 2/27/2017") Management of Accelerated Hypertension (Updated in 2017) By Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 Agenda Definition of Accelerated HTN Pathophysiology & Etiology Prognosis
Management of Accelerated Hypertension (Updated in 2017) By Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 Agenda Definition of Accelerated HTN Pathophysiology & Etiology Prognosis