Dr Ben Edwards Consultant Anaesthetist Sheffield Teaching Hospitals
|
|
|
- Angela Snow
- 5 years ago
- Views:
Transcription

1 Dr Ben Edwards Consultant Anaesthetist Sheffield Teaching Hospitals
2 70-75,000 #NOF per annum (costs 2 billion) 10% die within 1 month 33% die within 1 year Operative delays >48hs more than doubles risk of post op complications DVT, pneumonia, UTI Surgery is the best analgesia NICE & AAGBI guidelines (Oct 2013 )
3
4 NICE recommend the following should happen: Pain is assessed and treated Obtain imaging X-ray MRI/CT if clinical suspicion but x-ray negative All patients receive formal acute Orthogeriatric / Orthopaedic ward-based Hip Fracture Programme
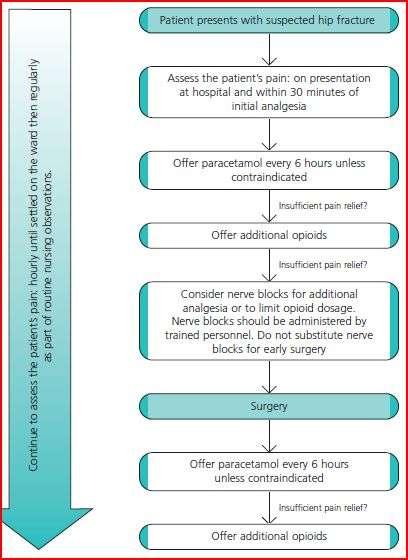
5 Assess the patient s pain: immediately upon presentation at hospital And within 30 mins of administering initial analgesia And hourly until settled on the ward And regularly as part of routine nursing observations throughout admission. Ensure sufficient analgesia to allow movements necessary for investigations, nursing care & rehabilitation. NSAIDs are not recommended. Paracetamol until U&E s ok then opiods Fascia Iliaca blocks commonly sited in ED
6
7 70% of patients are ASA % have one co-morbidity 17% have 2 7% have >3 The most common co-morbidities: Cardiovascular 35% Respiratory 14% Cerebrovascular 13%, diabetes 9% Malignancy 8% Renal disease 3%
8 FBC, group & save: anaemia is present in 40% higher blood transfusion trigger in the elderly i.e. Hb < 90 g/l (< 100 g/l with ischaemic heart disease) Leukocytosis and neutrophilia are common may represent a reaction to trauma rather than infection. Clotting A platelet count of < 80 is a relative contraindication to neuraxial anaesthesia. Platelet count < 50 will usually need a platelet transfusion.

9 U&E Hyper and hypokalemia, and hyponatraemia are common. ECG required in all patients with a NOF. CXR not necessary for all patients but useful in those with pneumonia or heart failure.
10 Perform surgery on the day of, or the day after admission Identify and treat correctable co-morbidities immediately to avoid delaying surgery
11 Chest infection prompt antibiotics AAGBI recommend proceeding to surgery under regional anaesthesia Diabetes do not delay surgery if hyperglycaemic unless the patient is ketotic and/or dehydrated Heart murmur There is debate regarding delaying surgery pending echo in light of unrecognised aortic stenosis. The majority of clinicians favour proceeding to surgery with modification of their techniques toward general anaesthesia with invasive blood pressure monitoring.
12 Indicated in order to: Establish left ventricular function if the patient is breathless at rest or on low level exertion To investigate severity of an ejection systolic murmur heart in the aortic area, particularly if >2 of the following are present: Unexplained syncope or pre-syncope Slow rising pulse Absent second heart sound LVH on ECG without hypertension
13 Aspirin should be withheld (unless indicated for unstable angina or stroke) Clopidogrel AAGBI: should not delay surgery or have prophylactic platelets. Do not stop on admission (especially in those with drug eluting stents) BUT this need balancing against individual risk. Warfarin INR < 2 for surgery and < 1.5 for neuraxial anaesthesia. vitamin K or prothrombinex to reverse if necessary. recommence 24 hours after surgery. If unsure about the management of anticoagulation, haematologist advice should be sought promptly.
14 Inappropriate reasons Lack of facilities or theatre space Awaiting echocardiography Unavailable surgical expertise Minor electrolyte abnormalities Appropriate reasons Hb < 80 Na < 120 or > 150 K+ < 2.8 or > 6.0 Uncontrolled diabetes Correctable cardiac arrhythmias (ventricular rate > 120) Chest infection with sepsis Reversible coagulopathy
15 Offer patients a choice of spinal or general anaesthesia after discussing the risks and benefits But not both in combination! Use nerve blocks Morphine sparing action intra and postoperatively
16
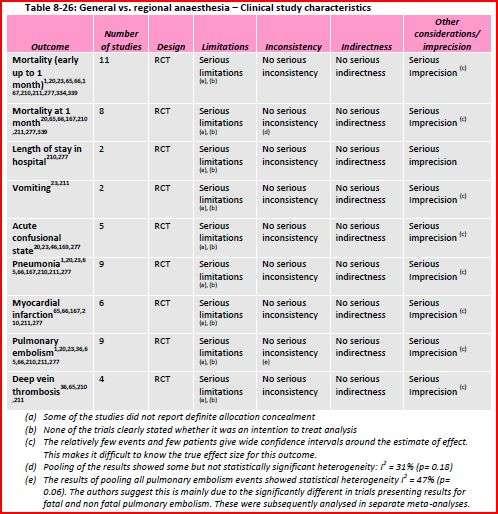
17 Statistically & clinically significant reduction in early mortality (up to 1 month) in patients having regional anaesthesia compared to general anaesthesia (LOW QUALITY) Statistically significant but not clinically significant improvement in postoperative confusion and reduction in incidence of DVT in patients receiving regional compared to general anaesthesia (LOW QUALITY)
18 There were no statistically significant differences in length of stay in hospital, vomiting, pneumonia, myocardial infarction and pulmonary embolism (LOW QUALITY) Economic : One study found general anaesthesia to be more costly than spinal anaesthesia. This evidence has very serious limitations; it did not evaluate effectiveness and may not have included all important cost differences
19 Aim to block femoral, obturator and lateral cutaneous nerves Lumbar plexus and fascia iliaca most effective Femoral less effective Aim is to reduce post-op morphine requirements
20 Careful titration induction agents Inhalation induction is well tolerated May facilitate haemodynamically stable induction Debate as to if spontaneous ventilation is preferable to mechanical ventilation
21 Regular paracetamol Avoid codeine Variable pharmacokinetics and efficacy Tramadol instead? Caution NSAIDs and opiates
22 High risk patient group Need early analgesia and surgery Dedicated care pathways Aims Spinal + nerve block Hb >10 POSU/extended recovery Early mobilisation
Anaesthesia. Clinical overview articles. Update in. Neck of femur fracture: perioperative management. Ronald Cheung
 Neck of femur fracture: perioperative management Ronald Cheung Correspondence: roncheung39@gmail.com Originally published as Anaesthesia Tutorial of the Week 296, 21 October 2013 INTRODUCTION Several large
Neck of femur fracture: perioperative management Ronald Cheung Correspondence: roncheung39@gmail.com Originally published as Anaesthesia Tutorial of the Week 296, 21 October 2013 INTRODUCTION Several large
Dr Micheal Looney Consultant Anaesthetist Connolly Hospital Blanchardstown. To Delay or Not to Delay Hip Fracture Surgery
 Dr Micheal Looney Consultant Anaesthetist Connolly Hospital Blanchardstown To Delay or Not to Delay Hip Fracture Surgery "You may delay, but time will not, and lost time is never found again." Benjamin
Dr Micheal Looney Consultant Anaesthetist Connolly Hospital Blanchardstown To Delay or Not to Delay Hip Fracture Surgery "You may delay, but time will not, and lost time is never found again." Benjamin
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture
 Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Audit of perioperative management of patients with fracture neck of femur
 Audit of perioperative management of patients with fracture neck of femur *M Dissanayake 1, N Wijesuriya 2 Registrar in Anaesthesia 1, Consultant Anaesthetist 2, North Colombo Teaching Hospital, Ragama,
Audit of perioperative management of patients with fracture neck of femur *M Dissanayake 1, N Wijesuriya 2 Registrar in Anaesthesia 1, Consultant Anaesthetist 2, North Colombo Teaching Hospital, Ragama,
IAEM Clinical Guideline 11 Management of Patients with Suspected Hip Fracture in the Emergency Department
 IAEM Clinical Guideline 11 Management of Patients with Suspected Hip Fracture in the Emergency Department Version 1 September 2018 Authors: Dr Mary Moore, Ms Marianne Walsh, Dr Termizi Hassan Guideline
IAEM Clinical Guideline 11 Management of Patients with Suspected Hip Fracture in the Emergency Department Version 1 September 2018 Authors: Dr Mary Moore, Ms Marianne Walsh, Dr Termizi Hassan Guideline
PREOPERATIVE PATIENT PREPARATION PROTOCOL
 PREOPERATIVE PATIENT PREPARATION PROTOCOL Each surgical discipline should have a standard set of published guidelines for the preparation of its patients for theatre procedures. These should be readily
PREOPERATIVE PATIENT PREPARATION PROTOCOL Each surgical discipline should have a standard set of published guidelines for the preparation of its patients for theatre procedures. These should be readily
Fascia Iliaca Compartment Block. Angela Stewart ANP 10/11/17
 Fascia Iliaca Compartment Block Angela Stewart ANP 10/11/17 1 Driving force Dr J. Mitchell from acute pain service Ayr hospital produced a comprehensive guideline to authorise Non-medical prescribers (NMP)
Fascia Iliaca Compartment Block Angela Stewart ANP 10/11/17 1 Driving force Dr J. Mitchell from acute pain service Ayr hospital produced a comprehensive guideline to authorise Non-medical prescribers (NMP)
Accompanied to walk Yes No Accompanied to walk Yes No Side of Fracture
 Fracture Neck Of Femur / Fast Track Criteria: Admission where femoral neck fracture is the primary diagnosis Accident & Emergency Assessment (To be completed by A/E Nurse and/or A/E doctor) Patient label
Fracture Neck Of Femur / Fast Track Criteria: Admission where femoral neck fracture is the primary diagnosis Accident & Emergency Assessment (To be completed by A/E Nurse and/or A/E doctor) Patient label
SAFE HIP FRACTURES. Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust
 SAFE HIP FRACTURES Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust Why hip fracture? Common in older adult (~84 years) UK current incidence : 70000 (Stockport
SAFE HIP FRACTURES Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust Why hip fracture? Common in older adult (~84 years) UK current incidence : 70000 (Stockport
Role and impact of orthogeriatric service in the hip fracture care pathway: 15-year experience
 Role and impact of orthogeriatric service in the hip fracture care pathway: 15-year experience AA Fisher, MW Davis Department of Geriatric Medicine, The Canberra Hospital, and Australian National University
Role and impact of orthogeriatric service in the hip fracture care pathway: 15-year experience AA Fisher, MW Davis Department of Geriatric Medicine, The Canberra Hospital, and Australian National University
The in-hospital management of COPD-exacerbation includes three core processes:
 Appendix 1A. Process flow for in-hospital management of COPDexacerbation The in-hospital management of COPD-exacerbation includes three core processes: 1. Diagnostic assessment 2. Pharmacological management
Appendix 1A. Process flow for in-hospital management of COPDexacerbation The in-hospital management of COPD-exacerbation includes three core processes: 1. Diagnostic assessment 2. Pharmacological management
Guidelines for the Perioperative Care of Elderly Hip Fracture Patients
 Guidelines for the Perioperative Care of Elderly Hip Fracture Patients This protocol has been agreed by colleagues from the departments of Anaesthesia, Haematology, Cardiology, Emergency Medicine, Orthogeriatrics
Guidelines for the Perioperative Care of Elderly Hip Fracture Patients This protocol has been agreed by colleagues from the departments of Anaesthesia, Haematology, Cardiology, Emergency Medicine, Orthogeriatrics
Heart Valves: Before and after surgery
 Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Fall-related hip fracture in NSW Epidemiology, evidence, practice and the future
 Fall-related hip fracture in NSW Epidemiology, evidence, practice and the future Jacqueline CT Close Orthogeriatrician, Prince of Wales Hospital Director - Falls and Injury Prevention Group Neuroscience
Fall-related hip fracture in NSW Epidemiology, evidence, practice and the future Jacqueline CT Close Orthogeriatrician, Prince of Wales Hospital Director - Falls and Injury Prevention Group Neuroscience
Fascia Iliaca Compartment Block. Angela Stewart ANP 22/08/17
 Fascia Iliaca Compartment Block Angela Stewart ANP 22/08/17 Motivation Anaesthetist Dr Joellene Mitchell from acute pain service Ayr hospital produced a guideline to allow Non-medical prescribers (NMP)
Fascia Iliaca Compartment Block Angela Stewart ANP 22/08/17 Motivation Anaesthetist Dr Joellene Mitchell from acute pain service Ayr hospital produced a guideline to allow Non-medical prescribers (NMP)
GALA GENERAL ANAESTHESIA vs LOCAL ANAESTHESIA FOR CAROTID SURGERY HOSPITAL DISCHARGE OR 7 DAY POST-SURGERY FOLLOW-UP FORM
 GALA GENERAL ANAESTHESIA vs LOCAL ANAESTHESIA FOR CAROTID SURGERY HOSPITAL DISCHARGE OR 7 DAY POST-SURGERY FOLLOW-UP FORM To the surgeon and anesthetist: Please complete questions 1-29 (pages 1, 2 & 3)
GALA GENERAL ANAESTHESIA vs LOCAL ANAESTHESIA FOR CAROTID SURGERY HOSPITAL DISCHARGE OR 7 DAY POST-SURGERY FOLLOW-UP FORM To the surgeon and anesthetist: Please complete questions 1-29 (pages 1, 2 & 3)
ANTICOAGULANTS AND HIP FRACTURE SURGERY. Jon Antrobus Anaesthetist Borders General Hospital
 ANTICOAGULANTS AND HIP FRACTURE SURGERY Jon Antrobus Anaesthetist Borders General Hospital Anticoagulation is common amongst the hip fracture patient population (6-10%) Anticoagulation signifies co-morbidity
ANTICOAGULANTS AND HIP FRACTURE SURGERY Jon Antrobus Anaesthetist Borders General Hospital Anticoagulation is common amongst the hip fracture patient population (6-10%) Anticoagulation signifies co-morbidity
Fractured Neck of Femur Proforma Orthopaedic Unit. First name: Registration no: Date of birth: Age:
 Fractured Neck of Femur Proforma Orthopaedic Unit Date: Surname : ED doctor s name: Time seen: Orthopaedic admitting doctor s name: Time seen: Presenting complaint and history of fall: First name: Registration
Fractured Neck of Femur Proforma Orthopaedic Unit Date: Surname : ED doctor s name: Time seen: Orthopaedic admitting doctor s name: Time seen: Presenting complaint and history of fall: First name: Registration
DOCUMENT CONTROL PAGE
 DOCUMENT CONTROL PAGE Title Title: UNDERGOING SPINAL DEFORMITY SURGERY Version: 2 Reference Number: Supersedes Supersedes: all other versions Description of Amendment(s): Revision of analgesia requirements
DOCUMENT CONTROL PAGE Title Title: UNDERGOING SPINAL DEFORMITY SURGERY Version: 2 Reference Number: Supersedes Supersedes: all other versions Description of Amendment(s): Revision of analgesia requirements
Atrial Fibrillation. A guide for Southwark General Practice. Key Messages. Always work within your knowledge and competency
 Atrial Fibrillation A guide for Southwark General Practice Key Messages 1. Routinely offer pulse checks to patients at high risk of AF 2. Use the CHA 2 DS 2 VASc score to identify patients for anticoagulation
Atrial Fibrillation A guide for Southwark General Practice Key Messages 1. Routinely offer pulse checks to patients at high risk of AF 2. Use the CHA 2 DS 2 VASc score to identify patients for anticoagulation
Rehabilitation - Reducing costs and hospital stay. Dr Elizabeth Aitken Consultant Physician
 Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY
 INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
Anaesthesia for ECT. Session 1. Dr Richard Cree Consultant in Anaesthesia & ICU. Roseberry Park Hospital and The James Cook Hospital, Middlesbrough
 Anaesthesia for ECT Session 1 Dr Richard Cree Consultant in Anaesthesia & ICU Roseberry Park Hospital and The James Cook Hospital, Middlesbrough Anaesthesia for ECT CHAPTERS 1. The principles of anaesthesia
Anaesthesia for ECT Session 1 Dr Richard Cree Consultant in Anaesthesia & ICU Roseberry Park Hospital and The James Cook Hospital, Middlesbrough Anaesthesia for ECT CHAPTERS 1. The principles of anaesthesia
Atrial Fibrillation Implementation challenges. Lesley Edgar Ross Maconachie
 Atrial Fibrillation Implementation challenges Lesley Edgar Ross Maconachie Atrial Fibrillation Most common heart rhythm disturbance Rapid and irregular electrical signals Reduced efficiency of blood flow
Atrial Fibrillation Implementation challenges Lesley Edgar Ross Maconachie Atrial Fibrillation Most common heart rhythm disturbance Rapid and irregular electrical signals Reduced efficiency of blood flow
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital
 What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
DOAC and NOAC are terms for a novel class of directly acting oral anticoagulant drugs including Rivaroxaban, Apixaban, Edoxaban, and Dabigatran.
 Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR
 MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR 1.1 Time to lower INR Prothrombinex-VF - 15 minutes Fresh Frozen Plasma
MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR 1.1 Time to lower INR Prothrombinex-VF - 15 minutes Fresh Frozen Plasma
Pulmonary Embolism Pathway
 Pulmonary Embolism Pathway Ambulatory Care Pathway Dr. A. Zafar, Dr. A. Rehman, Dr. T. Malik September, 2011. Patient Identification Label Pulmonary Embolism Pathway Clinical History Comments Hospital
Pulmonary Embolism Pathway Ambulatory Care Pathway Dr. A. Zafar, Dr. A. Rehman, Dr. T. Malik September, 2011. Patient Identification Label Pulmonary Embolism Pathway Clinical History Comments Hospital
AIMS: CHEST PAIN. Causes of chest pain. Causes of chest pain: Cardiac causes: Acute coronary syndromes pericarditis thoracic aortic dissection
 CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
Multidisciplinary Geriatric Trauma Care Guideline
 Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Pre-operative Assessment
 Pre-operative Assessment Dr Craig Taylor Andrea Harris On behalf of the WM RTC Audit Group A good example of an audit cycle...... or is it!!?? Identify Better Blood Transfusion 2002 2007 West Midlands
Pre-operative Assessment Dr Craig Taylor Andrea Harris On behalf of the WM RTC Audit Group A good example of an audit cycle...... or is it!!?? Identify Better Blood Transfusion 2002 2007 West Midlands
Top tips for surviving your first on call Dr Maleeha Rizvi
 Top tips for surviving your first on call Dr Maleeha Rizvi Specialist Registrar in Cardiology University Hospital Lewisham Overview Practical points The Bleep and prioritising on call Cardiac arrests Prescribing
Top tips for surviving your first on call Dr Maleeha Rizvi Specialist Registrar in Cardiology University Hospital Lewisham Overview Practical points The Bleep and prioritising on call Cardiac arrests Prescribing
The following content was supplied by the author as supporting material and has not been copy-edited or verified by JBJS.
 Page 1 The following content was supplied by the author as supporting material and has not been copy-edited or verified by JBJS. Appendix TABLE E-1 Care-Module Trigger Events That May Indicate an Adverse
Page 1 The following content was supplied by the author as supporting material and has not been copy-edited or verified by JBJS. Appendix TABLE E-1 Care-Module Trigger Events That May Indicate an Adverse
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
HEART CONDITIONS IN SPORT
 HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
Yes No Unknown. Major Infection Information
 Rehospitalization Intervention Check any that occurred during this hospitalization. Pacemaker without ICD ICD Atrial arrhythmia ablation Ventricular arrhythmia ablation Cardioversion CABG (coronary artery
Rehospitalization Intervention Check any that occurred during this hospitalization. Pacemaker without ICD ICD Atrial arrhythmia ablation Ventricular arrhythmia ablation Cardioversion CABG (coronary artery
More acute cardiology
 Case 1 RC 86, Male More acute cardiology Dr John Chambers Consultant Cardiologist A&E: SOB at rest. No chest pain. Exertional SOB for 6/12. PMHx: HT Rx: Ramipril 5mg od Examination: Afebrile, HR = 105,
Case 1 RC 86, Male More acute cardiology Dr John Chambers Consultant Cardiologist A&E: SOB at rest. No chest pain. Exertional SOB for 6/12. PMHx: HT Rx: Ramipril 5mg od Examination: Afebrile, HR = 105,
PRE Operative Care of the High Risk Surgical Patient. Dr A T Dewhurst Consultant Anaesthetist St George s Hospital London
 PRE Operative Care of the High Risk Surgical Patient Dr A T Dewhurst Consultant Anaesthetist St George s Hospital London Perioperative Optimization Shoemaker oxygen delivery goal directed therapy ITS NOT
PRE Operative Care of the High Risk Surgical Patient Dr A T Dewhurst Consultant Anaesthetist St George s Hospital London Perioperative Optimization Shoemaker oxygen delivery goal directed therapy ITS NOT
National Hip Fracture Data Base
 National Hip Fracture Data Base National Hip Fracture Data Base Spring Meeting Chester 3 February 2010 Hip Fracture Best Practice: Multidisciplinary Approach (Evidence Based Medicine) Atef Michael Consultant
National Hip Fracture Data Base National Hip Fracture Data Base Spring Meeting Chester 3 February 2010 Hip Fracture Best Practice: Multidisciplinary Approach (Evidence Based Medicine) Atef Michael Consultant
Introduction. Peripheral arterial disease. Hospital inpatient data - 5,498 FCE (2009/10), & 530 deaths in England alone
, & 530 deaths in England alone") 1 Introduction 2 Introduction Peripheral arterial disease Affects 20% adults in Europe and North America In the UK 500-1000/million PAD, 1-2% require amputation LLA 8-15% in people with diabetes with up
1 Introduction 2 Introduction Peripheral arterial disease Affects 20% adults in Europe and North America In the UK 500-1000/million PAD, 1-2% require amputation LLA 8-15% in people with diabetes with up
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근
 Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
Heart failure for syndicate
 Heart failure for syndicate By M.Wafaie Aboleineen,MD,FACC ESC Guidelines for the diagnosis and treatment of heart failure Part I 1 4 2 Common ECG abnormalities in HF 3 Common CXR abnormalities in HF Common
Heart failure for syndicate By M.Wafaie Aboleineen,MD,FACC ESC Guidelines for the diagnosis and treatment of heart failure Part I 1 4 2 Common ECG abnormalities in HF 3 Common CXR abnormalities in HF Common
Blunt Chest Trauma (Rib Fracture) Management Guideline
 Management Guideline") Blunt Chest Trauma (Rib Fracture) Management Guideline Midlands Critical Care, Trauma and Burns Networks Network: Midlands Trauma Networks Publication: Document purpose: Trauma Guidelines Document name:
Blunt Chest Trauma (Rib Fracture) Management Guideline Midlands Critical Care, Trauma and Burns Networks Network: Midlands Trauma Networks Publication: Document purpose: Trauma Guidelines Document name:
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006
 TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
Ischaemic Heart Disease
 Ischaemic Heart Disease Katherine Rothwell Case 1 65 yr old female PMHx : Eczema, is a smoker 20/day Comes to see you complaining of central chest pain Present past few months. Comes on when gardening
Ischaemic Heart Disease Katherine Rothwell Case 1 65 yr old female PMHx : Eczema, is a smoker 20/day Comes to see you complaining of central chest pain Present past few months. Comes on when gardening
Development of an RANP role, Acute Medicine. Emily Bury RANP, Acute Medicine
 Development of an RANP role, Acute Medicine Emily Bury RANP, Acute Medicine Background 2010 National Acute Medicine Programme NAMP recommends established the in development of ANP Ireland. posts with emphasis
Development of an RANP role, Acute Medicine Emily Bury RANP, Acute Medicine Background 2010 National Acute Medicine Programme NAMP recommends established the in development of ANP Ireland. posts with emphasis
NICE Guidance: Venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital 1
 in patients admitted to hospital 1") The College of Emergency Medicine Patron: HRH The Princess Royal Churchill House Tel +44 (0)207 404 1999 35 Red Lion Square Fax +44 (0)207 067 1267 London WC1R 4SG www.collemergencymed.ac.uk CLINICAL EFFECTIVENESS
The College of Emergency Medicine Patron: HRH The Princess Royal Churchill House Tel +44 (0)207 404 1999 35 Red Lion Square Fax +44 (0)207 067 1267 London WC1R 4SG www.collemergencymed.ac.uk CLINICAL EFFECTIVENESS
National Vascular Registry
 National Vascular Registry AAA Repair Patient Details Patient Consent* 0 No 1 Yes 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s)
National Vascular Registry AAA Repair Patient Details Patient Consent* 0 No 1 Yes 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s)
National Vascular Registry
 National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
2 Summary of NICE TA 249: Atrial fibrillation - Dabigatran Etexilate
 Service Notification in response to DHSSPS endorsed NICE Technology Appraisals NICE TA 249: Atrial fibrillation - Dabigatran Etexilate 1 Name of Commissioning Team Long Term Conditions Commissioning Team
Service Notification in response to DHSSPS endorsed NICE Technology Appraisals NICE TA 249: Atrial fibrillation - Dabigatran Etexilate 1 Name of Commissioning Team Long Term Conditions Commissioning Team
Pre-operative Anaemia Colorectal and Orthopaedic Surgery
 Pre-operative Anaemia Colorectal and Orthopaedic Surgery Dr Simon Rang Consultant Anaesthetist East Kent Hospitals NHS Trust Dreamland Pre-operative Anaemia Anaemia is a perioperative risk factor Perioperative
Pre-operative Anaemia Colorectal and Orthopaedic Surgery Dr Simon Rang Consultant Anaesthetist East Kent Hospitals NHS Trust Dreamland Pre-operative Anaemia Anaemia is a perioperative risk factor Perioperative
References: Murtagh J. Murtagh s General Practice. 5 th edn. Sydney: McGraw Hill; 2010.
 This presentation is designed to be delivered to people who work in a health care setting; such as nurses, carers and other nursing home staff. If you are an accredited pharmacist, you can use this presentation
This presentation is designed to be delivered to people who work in a health care setting; such as nurses, carers and other nursing home staff. If you are an accredited pharmacist, you can use this presentation
Preliminary Programme
 Preliminary Programme The scientific programme comprises various styles of presentations and sessions, each offering a unique opportunity to amass new and important scientific information. Optimal management
Preliminary Programme The scientific programme comprises various styles of presentations and sessions, each offering a unique opportunity to amass new and important scientific information. Optimal management
Reducing the risk of venous thrombo-embolism (VTE) in hospital and after discharge
 in hospital and after discharge") Reducing the risk of venous thrombo-embolism (VTE) in hospital and after discharge What is a venous thromboembolism (VTE)? This is a medical term that describes a blood clot that develops in a deep vein
Reducing the risk of venous thrombo-embolism (VTE) in hospital and after discharge What is a venous thromboembolism (VTE)? This is a medical term that describes a blood clot that develops in a deep vein
Emergency Department Guidelines COLLAPSE? CAUSE / SYNCOPE. Version x (x 201x) Review date: x 2014 Page 1 of 5
 Review date: x 2014 Page 1 of 5") COLLAPSE? CAUSE / SYNCOPE Review date: x 2014 Page 1 of 5 KEY POINTS: Do not use this guideline for mechanical falls Definition: Syncope is a transient loss of consciousness with an inability to maintain
COLLAPSE? CAUSE / SYNCOPE Review date: x 2014 Page 1 of 5 KEY POINTS: Do not use this guideline for mechanical falls Definition: Syncope is a transient loss of consciousness with an inability to maintain
PE Pathway. The charts are listed as follows:
 PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
Guideline for the Management of Acute Chest Syndrome in Children with Sickle Cell Disease
 Guideline for the Management of Acute Chest Syndrome in Children with Sickle Cell Disease Definition Acute chest syndrome (ACS) is defined as an acute illness characterized by fever and/or respiratory
Guideline for the Management of Acute Chest Syndrome in Children with Sickle Cell Disease Definition Acute chest syndrome (ACS) is defined as an acute illness characterized by fever and/or respiratory
These are guidelines only and can be deviated from if it is thought to be in the patient s best interest.
 Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics Venous thromboembolism (VTE) is a recognised complication associated with inactivity and surgical procedures. Therefore, all
Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics Venous thromboembolism (VTE) is a recognised complication associated with inactivity and surgical procedures. Therefore, all
Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Warfarin in Adults : Guidelines for the use of. These guidelines apply to all patients commenced or continuing on warfarin
 Warfarin in Adults : Guidelines for the use of Document Type: Clinical Guideline Clinical Lead: Ian Neilly Author/s: Ian Neilly/Paul Barbieri Directorate: Haematology Approved by Haematology Specialty
Warfarin in Adults : Guidelines for the use of Document Type: Clinical Guideline Clinical Lead: Ian Neilly Author/s: Ian Neilly/Paul Barbieri Directorate: Haematology Approved by Haematology Specialty
convey the clinical quality measure's title, number, owner/developer and contact
 CMS-0033-P 153 convey the clinical quality measure's title, number, owner/developer and contact information, and a link to existing electronic specifications where applicable. TABLE 20: Proposed Clinical
CMS-0033-P 153 convey the clinical quality measure's title, number, owner/developer and contact information, and a link to existing electronic specifications where applicable. TABLE 20: Proposed Clinical
Aneurin Bevan University Health Board Sickle Cell Anaemia and Haemoglobinopathy Screening and Management in Pregnancy Guidelines
 Sickle Cell Anaemia and Haemoglobinopathy Screening and Management in Pregnancy Guidelines N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed
Sickle Cell Anaemia and Haemoglobinopathy Screening and Management in Pregnancy Guidelines N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed
Appendix 2H - SECONDARY CARE CONVERSION GUIDELINES ORAL ANTICOAGULANTS
 Appendix 2H - SECONDARY CARE CONVERSION GUIDELINES ORAL ANTICOAGULANTS Please note that newer oral anticoagulants e.g. rivaroxaban, dabigatran and apixiban should be only be considered in patients with
Appendix 2H - SECONDARY CARE CONVERSION GUIDELINES ORAL ANTICOAGULANTS Please note that newer oral anticoagulants e.g. rivaroxaban, dabigatran and apixiban should be only be considered in patients with
Venothromboembolism prophylaxis: Trauma and Orthopaedics Clinical guideline, V2
 Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics 11/11/11 TEMPORARY GUIDANCE There is no prophylactic tinzaparin available in the Trust currently. Please substitute enoxaparin
Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics 11/11/11 TEMPORARY GUIDANCE There is no prophylactic tinzaparin available in the Trust currently. Please substitute enoxaparin
The Perioperative Care Chain is Only as Strong as its weakest link
 The Perioperative Care Chain is Only as Strong as its weakest link Associate Professor Kerin Fielding The University of Notre Dame, Australia School of Medicine, Sydney Outline The perioperative chain
The Perioperative Care Chain is Only as Strong as its weakest link Associate Professor Kerin Fielding The University of Notre Dame, Australia School of Medicine, Sydney Outline The perioperative chain
FRACTURED NECK OF FEMUR CLINICAL PATHWAY
 FRACTURED NECK OF FEMUR CLINICAL PATHWAY Patient s... Hospital No. Date... Information Taken By. Designation History of Injury Date and of Event Clinical Assessment of Injury Affected Limb Right Left Reason:
FRACTURED NECK OF FEMUR CLINICAL PATHWAY Patient s... Hospital No. Date... Information Taken By. Designation History of Injury Date and of Event Clinical Assessment of Injury Affected Limb Right Left Reason:
URN: Family name: Given name(s): Address: Initial Signature Print Name Role
: Address: Initial Signature Print Name Role") Do Not Write in this binding margin v5.00-02/2012 Mat. No.: 10206019 SW030b The State of Queensland (Queensland Health) 2012 Contact CIM@health.qld.gov.au ÌSW030bIÎ Facility: s Never Replace Clinical Judgement
Do Not Write in this binding margin v5.00-02/2012 Mat. No.: 10206019 SW030b The State of Queensland (Queensland Health) 2012 Contact CIM@health.qld.gov.au ÌSW030bIÎ Facility: s Never Replace Clinical Judgement
The following pages are extracted from the system help pages and provides a little background to each dataset item.
 1.00 Dataset Item Summary Notes FFN Hip Fracture Audit database Minimum Common Dataset (MCD MCD) Version 1.5 June 2014 The following pages are extracted from the system help pages and provides a little
1.00 Dataset Item Summary Notes FFN Hip Fracture Audit database Minimum Common Dataset (MCD MCD) Version 1.5 June 2014 The following pages are extracted from the system help pages and provides a little
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Sickle cell acute episode: management of an acute painful sickle cell episode in hospital 1.1 Short title Sickle cell acute
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Sickle cell acute episode: management of an acute painful sickle cell episode in hospital 1.1 Short title Sickle cell acute
Hip Fracture (HFR) Measures Document
 Measures Document") Hip Fracture (HFR) Measures Document HFR Version: 2 - covering patients discharged between 01/10/2017 and present. Programme Lead: Sam Doddridge Clinical Leads: Ms Phil Thorpe Dr John Tsang Number of Measures
Hip Fracture (HFR) Measures Document HFR Version: 2 - covering patients discharged between 01/10/2017 and present. Programme Lead: Sam Doddridge Clinical Leads: Ms Phil Thorpe Dr John Tsang Number of Measures
Striving to improve hip fracture care
 Striving to improve hip fracture care The UHL experience 2008-2015 Mr F. Condon, Consultant Orthopaedic Surgeon Ms Jude Ryan, Consultant Ortho-Geriatrician (Mat Leave) & A. Butler Orthopaedic CNS (Mat
Striving to improve hip fracture care The UHL experience 2008-2015 Mr F. Condon, Consultant Orthopaedic Surgeon Ms Jude Ryan, Consultant Ortho-Geriatrician (Mat Leave) & A. Butler Orthopaedic CNS (Mat
Transcatheter Aortic Valve Implantation Procedure (TAVI)
") Page 1 of 5 Procedure (TAVI) Introduction Aortic stenosis (AS) is a common heart valve problem associated with heart failure and death. Surgical valve repair or replacement is recommended if AS patients
Page 1 of 5 Procedure (TAVI) Introduction Aortic stenosis (AS) is a common heart valve problem associated with heart failure and death. Surgical valve repair or replacement is recommended if AS patients
National Vascular Registry
 National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
Trust Guideline for the Management of Patient Controlled Analgesia (PCA) in Adults
 in Adults") Patient Controlled Analgesia (PCA) in Adults A clinical guideline recommended for use For Use in: In all Clinical Areas By: Anaesthetists, Ward Nurses, Recovery Staff Acute Pain Service Staff For: Adult
Patient Controlled Analgesia (PCA) in Adults A clinical guideline recommended for use For Use in: In all Clinical Areas By: Anaesthetists, Ward Nurses, Recovery Staff Acute Pain Service Staff For: Adult
Preoperative tests (update)
") National Institute for Health and Care Excellence. Preoperative tests (update) Routine preoperative tests for elective surgery NICE guideline NG45 Appendix C: April 2016 Developed by the National Guideline
National Institute for Health and Care Excellence. Preoperative tests (update) Routine preoperative tests for elective surgery NICE guideline NG45 Appendix C: April 2016 Developed by the National Guideline
IFT1 Interfacility Transfer of STEMI Patients. IFT2 Interfacility Transfer of Intubated Patients. IFT3 Interfacility Transfer of Stroke Patients
 IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
Assessing perioperative risk
 Assessing perioperative risk Chronic Obstructive Pulmonary Disease Dr. Michelle Caldecott Respiratory & Sleep Physician Epworth Healthcare Austin Health Impact of COPD on Postoperative Outcomes: Results
Assessing perioperative risk Chronic Obstructive Pulmonary Disease Dr. Michelle Caldecott Respiratory & Sleep Physician Epworth Healthcare Austin Health Impact of COPD on Postoperative Outcomes: Results
PAEDIATRIC NERVE BLOCK / WOUND INFILTRATION
 PAEDIATRIC NERVE BLOCK / WOUND INFILTRATION Addendum to the MULTIDISCIPLINARY GUIDELINES FOR ACUTE PAIN MANAGEMENT IN CHILDREN AND YOUNG PEOPLE Policy Owner: Approved by: Ratified by: ABMU HB Pain Management
PAEDIATRIC NERVE BLOCK / WOUND INFILTRATION Addendum to the MULTIDISCIPLINARY GUIDELINES FOR ACUTE PAIN MANAGEMENT IN CHILDREN AND YOUNG PEOPLE Policy Owner: Approved by: Ratified by: ABMU HB Pain Management
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
Breathlessness in advanced disease. February 2017
 Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
Preoperative Management of Patients Receiving Antithrombotics
 Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
PATIENT SELECTION PUSHING THE FRONTIERS OF DAY SURGERY. Dr Theresa Hinde Anaesthetic ST7 Council Member British Association of Day Surgery
 PATIENT SELECTION PUSHING THE FRONTIERS OF DAY SURGERY Dr Theresa Hinde Anaesthetic ST7 Council Member British Association of Day Surgery HOW A DAY SURGERY MINDSET CAN TRANSFORM THE OUTCOMES FOR BOTH YOUR
PATIENT SELECTION PUSHING THE FRONTIERS OF DAY SURGERY Dr Theresa Hinde Anaesthetic ST7 Council Member British Association of Day Surgery HOW A DAY SURGERY MINDSET CAN TRANSFORM THE OUTCOMES FOR BOTH YOUR
Evaluation of a diagnostic pathway in heart failure in primary care, using electrocardiography and brain natriuretic peptide guided echocardiography
 Evaluation of a diagnostic pathway in heart failure in primary care, using electrocardiography and brain natriuretic peptide guided echocardiography Rebecka Karlsson Pardeep Jhund 1 Material and methods
Evaluation of a diagnostic pathway in heart failure in primary care, using electrocardiography and brain natriuretic peptide guided echocardiography Rebecka Karlsson Pardeep Jhund 1 Material and methods
National Vascular Registry
 National Vascular Registry AAA Repair Patient Details Patient Consent* 0 No 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s)
National Vascular Registry AAA Repair Patient Details Patient Consent* 0 No 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s)
Acute coronary syndromes
 Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
TAVR : Caring for your patients before and after TAVR
 TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
Chest pain and troponins on the acute take. J N Townend Queen Elizabeth Hospital Birmingham
 Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
SIGN. Management of hip fracture in older people. June A national clinical guideline. Scottish Intercollegiate Guidelines Network
 SIGN Scottish Intercollegiate Guidelines Network Part of NHS Quality Improvement Scotland 111 Management of hip fracture in older people A national clinical guideline June 2009 KEY TO EVIDENCE STATEMENTS
SIGN Scottish Intercollegiate Guidelines Network Part of NHS Quality Improvement Scotland 111 Management of hip fracture in older people A national clinical guideline June 2009 KEY TO EVIDENCE STATEMENTS
Blood Transfusions in Children with Haemoglobinopathies
 Blood Transfusions in Children with Haemoglobinopathies Version: 2 Date: 22 nd April 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/ committees involved in
Blood Transfusions in Children with Haemoglobinopathies Version: 2 Date: 22 nd April 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/ committees involved in
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS
 GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
Perioperative TTE an under-utilised modality?
 Perioperative TTE an under-utilised modality? David Canty Senior Lecturer Department of Surgery, University of Melbourne Cardiothoracic Anaesthetist Disclosures Employed University of Melbourne POC workshops,
Perioperative TTE an under-utilised modality? David Canty Senior Lecturer Department of Surgery, University of Melbourne Cardiothoracic Anaesthetist Disclosures Employed University of Melbourne POC workshops,
Følgende dias er fremlagt ved DCS / DTS Fællesmøde 13. januar 2011 og alle rettigheder tilhører foredragsholderen. Gengivelse må kun foretages ved
 . Følgende dias er fremlagt ved DCS / DTS Fællesmøde 13. januar 2011 og alle rettigheder tilhører foredragsholderen. Gengivelse må kun foretages ved tilladelse Antithrombotic therapy in Atrial Fibrillation
. Følgende dias er fremlagt ved DCS / DTS Fællesmøde 13. januar 2011 og alle rettigheder tilhører foredragsholderen. Gengivelse må kun foretages ved tilladelse Antithrombotic therapy in Atrial Fibrillation
Rituximab (weekly) for Primary Cutaneous B cell Lymphoma
 for Primary Cutaneous B cell Lymphoma") Rituximab (weekly) for Primary Cutaneous B cell Lymphoma Indication: Palliative therapy for Low grade Primary Cutaneous B cell Lymphoma (Primary cutaneous Follicle centre cell Lymphoma and Primary cutaneous
Rituximab (weekly) for Primary Cutaneous B cell Lymphoma Indication: Palliative therapy for Low grade Primary Cutaneous B cell Lymphoma (Primary cutaneous Follicle centre cell Lymphoma and Primary cutaneous
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Discharge Letter Example 1
 Discharge Letter Example 1 Admission: Specialty -.; Ward xx Diagnosis: Musculoskeletal chest pain Ischaemic heart disease Type II diabetes mellitus Hypertension Previous CVA Obesity This [..] year old
Discharge Letter Example 1 Admission: Specialty -.; Ward xx Diagnosis: Musculoskeletal chest pain Ischaemic heart disease Type II diabetes mellitus Hypertension Previous CVA Obesity This [..] year old
Scottish Standards of Care for Hip Fracture Patients
 Scottish Standards of Care for Hip Fracture Patients This document has been prepared in collaboration with Healthcare Improvement Scotland to align with the forthcoming updated Older People in Hospitals
Scottish Standards of Care for Hip Fracture Patients This document has been prepared in collaboration with Healthcare Improvement Scotland to align with the forthcoming updated Older People in Hospitals
Question 1: Between 1 July 2014 and 30 June 2015, in the area covered by your CCG:
 Atrial Fibrillation in Your Area Question 1: Between 1 July 2014 and 30 June 2015, in the area covered by your CCG: a) What was the prevalence of atrial fibrillation (AF)? 6636 (as of 22/10/2015) 2.1%
Atrial Fibrillation in Your Area Question 1: Between 1 July 2014 and 30 June 2015, in the area covered by your CCG: a) What was the prevalence of atrial fibrillation (AF)? 6636 (as of 22/10/2015) 2.1%
Intro Who should read this document 2 Key practice points 2 What is new in this version 3 Background 3 Guideline Subsection headings
 Enhanced Recovery for Major Urology and Gynaecological Classification: Clinical Guideline Lead Author: Dr Dominic O Connor Additional author(s): Jane Kingham Authors Division: Anaesthesia Unique ID: DDCAna3(12)
Enhanced Recovery for Major Urology and Gynaecological Classification: Clinical Guideline Lead Author: Dr Dominic O Connor Additional author(s): Jane Kingham Authors Division: Anaesthesia Unique ID: DDCAna3(12)