National Hip Fracture Data Base
|
|
|
- Esmond Owens
- 5 years ago
- Views:
Transcription
1 National Hip Fracture Data Base National Hip Fracture Data Base Spring Meeting Chester 3 February 2010
2 Hip Fracture Best Practice: Multidisciplinary Approach (Evidence Based Medicine) Atef Michael Consultant Orthogeriatrician Russells Hall Hospital Honorary Senior Lecturer of Medicine
3 Epidemiology The Profile of Patients with Hip Fracture Preoperative & Postoperative Issues The surgeon & Anaesthetist Orthogeriatric Ward Hip Fracture Nurse Multidisciplinary Rehabilitation NHFDB

4 Projected numbers of people aged 60 years and over Khaw K T. BMJ 1999;319:
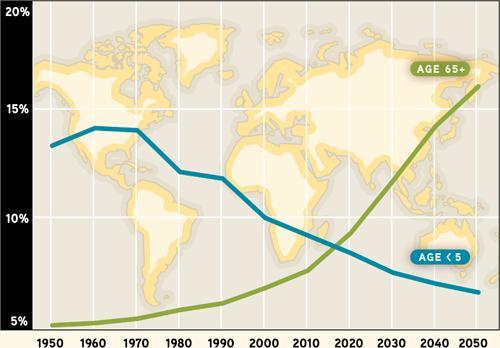
5

6 Estimated numbers of hip fractures in people aged over 60 in UK Khaw K T. BMJ 1999;319:
7
8 Epidemiology By extreme old age 1/3 of all women 1/6 of all men will sustain a hip fracture
9 The Profile of Patients with Hip Fracture The mean age is 82 y Roche JJ, Wenn RT et al. BMJ 2005; 331(7529) : % are women 90 % result from a fall Baker SP, Harvey AH. Clin Geriat Med 1985;1: % have one major co morbidity
10 Hip Fractures The median LOS 12 days on a trauma ward + 6 days on a rehabilitation ward Roche JJ, Wenn RT et al. BMJ 2005; 331(7529) : 1374 >20% of all orthopaedic bed occupancy in the UK Kanis JA, et al. Osteoporos Int 1997;7:

11 = Bad News
12 Hip fracture results in a 10% - 15% decrease in life expectancy
13 Following Hip Fracture 20% die within a year 30% require long-term nursing home care 50% lose the ability to live independently NICE Scope Osteoporosis 2004
14 80 % of older women prefer death to a bad hip fracture that would result in nursing home admission Salkeld G et al. BMJ 2000
15 What do patients die from? Trauma Major surgery Concurrent medical problems Postoperative complications: Pneumonia (Aspiration & HAP) Thromboembolic disease Coronary events Bandolier.Outcome after Hip Fracture. 1998; 48(2)
16 How to improve hip fracture care? Coordinated multi-disciplinary teams delivering High quality : Preoperative care Operative care Postoperative care Rehabilitation Secondary prevention of fragility fractures Osteoporosis risk assessment & treatment Falls risk assessment Audit & feedback


17
18
19 6 Standards for hip fracture care Admission to the ward within 4 hours Surgery within 48 hours of admission Minimising the risk of pressure ulcers Access to acute orthogeriatric medical support Assessment for antiresorptive therapy Multidisciplinary assessment and intervention to prevent future falls
20 Preoperative Issues
21 The mean age of patients sustaining a hip fracture is 82 Roche JJ, Wenn RT et al. BMJ 2005; 331(7529) : 1374

22 Michael A, Doos L. Osteoporos Int. 2009; 20 (supplement 4): S289.
23 Ageing = Lack of Physiologic Reserve Left ventricular filling declines 50% The lung function is about 50% Renal function declines by 50% Liver weight declines by 1/3 The brain shrinks by 5-10%
24 Consequences of Lack of the Physiologic Reserve At risk of LVF Stress of trauma & surgery Volume overload Acute Kidney Injury Dehydration (on admission) NSAIDs Metabolism of the medications may be impaired Delirium
25 Co morbid conditions & Polypharmcy Most patients have co morbid conditions CCF (10% prevalence after age 80 years) AF (18 % prevalence in people older than 85) COPD CKD CVD PVD Dementia (prevalence among persons aged 85 years and older may approach 50%) PD Polypharmcy: > 40 % of people aged 77 years are exposed to polypharmacy, defined as the use of 5 drugs (Swedish study) Haider S.I et al. Clinical Therapeutics, 2008 Feb;30(2):419-27
26
27 long lie Syndrome Hypothermia Acute (on chronic) renal impairment Rhabdomyolysis Hypo / hyperglycaemia Delirium
28 3 Mortality at 30 days & Preoperative Co morbidity Preoperative Respiratory Disease Preoperative Renal Disease Patients with 3 Co morbidities
29 Venous Thromboembolism (VTE) PE is the most common preventable cause of hospital death

30 Arch Intern Med 151[5]: , 1991
31 High Risk Venous Thromboembolism Without prophylaxis the incidence of hospitalacquired DVT is 40 to 60% Geerts WH, Pineo GF, Heit JA, et al. Chest 2004; 126:338S
32 Venous Thromboembolism 1/4 to 1/3 involve the proximal deep veins much more likely to be symptomatic and to result in PE Geerts WH, Pineo GF, Heit JA, et al. Chest 2004; 126:338S The majority of symptomatic VTE occur after hospital discharge Geerts WH, Pineo GF, Heit JA, et al. Chest 2004; 126:338S
33 Duration of Thromboprophylaxis Should be extended beyond 10 days and up to 35 days after surgery Options include: LMWH Or Warfarin ACCP Evidence-Based Clinical Practice Guidelines (8th Edition)
34 The Timing of Surgery To operate or to wait?
35

36 Odds ratios of death within hospital by operative delay Bottle, A. et al. BMJ 2006;332:
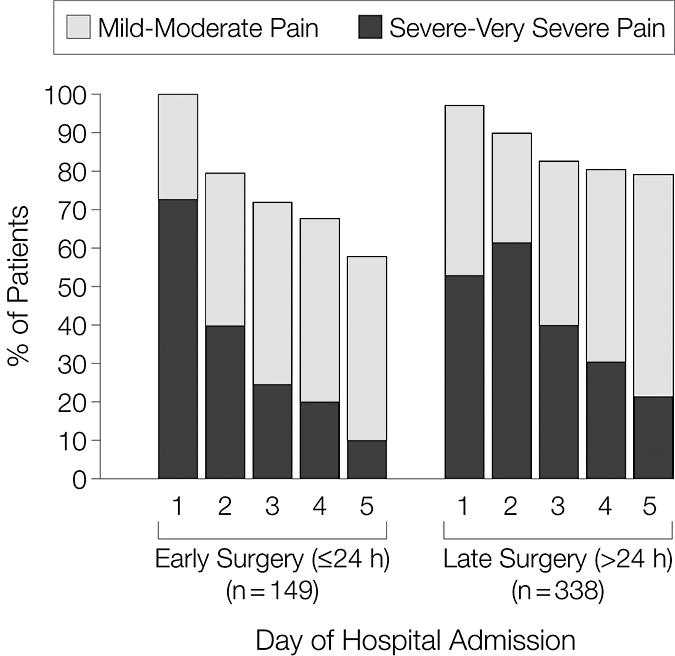
37 The Timing of Surgery As soon as possible Early surgery is associated with reduced pain and decreased length of stay Orosz, GM, Magaziner, J, Hannan, EL, et al. JAMA 2004; 291:1738 Surgery within hours reduces mortality Bottle A, Aylin P. BMJ 2006; 332:947
38 Why do juniors delay surgery? Medical assessment Cardiac murmurs Echocardiography Chest infection Anaemia Hyponatraemia & Hypokalaemia
39 Flow Murmurs 25% of older individuals have flow murmurs Minimal functional significance
40 Major Abnormalities Likely to require correction prior to surgery McLaughlin et al. Journal of General Internal Medicine 2006;21(3);
41 Major Abnormalities Likely to require correction prior to surgery Blood Pressure Systolic < 90 mm HG Heart Rate and Rhythm AF or SVT > 121 VT 3rd degree block HR < 45 Infection/Pneumonia Temperature < 35 C or > 38.5 C, with clinical diagnosis of pneumonia or infiltrate on CXR
42 Major Abnormalities Likely to require correction prior to surgery Chest Pain New MI on ECG Chest pain with abnormal ECG CCF Pulmonary oedema on CXR, CCF on CXR with dyspnea +/or abnormal exam Respiratory Failure Pulse oximetry <90%, po2 < 8 KPa, or pco2 > 7.3 kpa
43 Major Abnormalities Likely to require correction prior to surgery INR 1.6 Electrolytes Na < 125 or >155 mmol/l K < 2.5 or > 6.1 mmol/l HCO3 < 18 or >36 mmol/l Journal of General Internal Medicine. 2006;21(3);
44 Major Abnormalities Likely to require correction prior to surgery Renal Function Urea > 18 mmol/litre Creatinine > 230 µmol/litre Glucose > 33 mmol/litre Anaemia Hb < 7.5 gm/dl without history of ESRD
45 Postoperative Issues Nutrition Hip fracture patients achieve only 1/2 their recommended daily energy and nutritional requirements Duncan D et al. Age & Ageing 2001;30:Suppl2:22 Pressure sores 1/3 of hip fracture patients will develop pressure sores Versluysen M. JBJS (Br) 1985;67:1:10-13

46
47 Pressure Ulcers Occur in 10 to 40 % of patients Beaupre, LA, Jones, CA, Saunders, LD, et al. J Gen Intern Med 2005; 20:1019 Use of alternating pressure mattresses reduce the incidence of pressure ulcers Beaupre, LA, Jones, CA, Saunders, LD, et al. J Gen Intern Med 2005; 20:1019
48 Postoperative Medical Complications The most common complications are Chest infection 9 % Acute heart failure 5 % Mortality rate of 15 20% Roche J, Moran C. Ger Med, 2006 Oct (36):67-74
49 Delirium Occurs in 15 to 74% of postoperative patients The associated hospital mortality rates for delirium are 25 to 33% (= acute MI or sepsis)
50 Hip Fracture Outcomes: Does the Surgeon Really Matter?
51 Experience of the surgeon & Long term outcome Significant difference in long term out come of cemented hemi replacement based on the surgeon s experience Malal J G, Pillai A, Nimon GA. J B J S British Volume 2009, 91 B, Supp I, 134.
52 Hip Fracture Outcomes: Does Surgeon Really Matter? Low-volume surgeons have Higher in-hospital mortality rate (p = 0.005) Higher incidence of transfusion, pneumonia, and decubitus ulcer (p = <0.05) Longer lengths of stay (p = <0.05) Browne J A, Pietrobon R, Olson S A. The Journal of Trauma: Injury, Infection, and Critical Care: March 2009 (66) 3- pp
53 Weekends & Weekdays
54 Weekends & Weekdays Patients are more likely to die in the hospital if they are admitted on a weekend than if they are admitted on a weekday. Bell CM and Redelmeier DA.N Engl J Med 2001; 345:663 8
55 Weekends & Weekdays Patients admitted on weekends experienced slightly higher risk-adjusted mortality than did patients admitted on weekdays. Cram P, Hillis SL et al. Am J Med 2004; 117:151 7
56 Weekends and Holidays Patients with a hip fracture had an independently increased risk of early postoperative mortality when admitted during longer holiday periods Foss NB, Kehlet H. BJA 2006; 96:450-4
57 Orthogeriatric Ward
58 Orthogeriatric Ward The NSF for Older People states that:..at least one general ward in an acute hospital should be developed as a centre of excellence for orthogeriatric practice.
59 Six standards for hip fracture care Standard 4 All patients presenting with a fragility fracture should be managed on an orthopaedic ward with routine access to acute orthogeriatric medical support from the time of admission The Blue Book
60 Hip Fracture Nurse Hip Fracture Practioner To coordinate and supervise Initial assessment Pre-operative work-up Post-operative care Rehabilitation Discharge planning Secondary prevention Follow-up
61 Multidisciplinary Rehabilitation

62 Early Mobilisation Early mobilisation of patients after hip fracture repair is safe, although the benefits of this approach have not been conclusively demonstrated Handoll, HH, Parker, MJ, Sherrington, C. Cochrane Database Syst Rev 2003
63 Physiotherapy More frequent physical therapy (at least 2 sessions/d) was associated with better outcomes Penrod, JD, Boockvar, KS, Litke, A, et al. J Am Geriatr Soc 2004; 52:1114
64 Rehabilitation Intensive geriatric rehabilitation may reduce length of stay Huusko, TM, Karppi, P, Avikainen, V, et al. Acta Orthop Scand 2002; 73:425
65 Multidisciplinary Rehabilitation Vs Usual Orthopaedic Care Multidisciplinary rehabilitation was associated with a modest but important reduction in poor outcome Halbert J, CrottyM et al. Journal of Rehabilitation Medicine 2007;39(7):
66 Dietetic Assistants Showed a trend for a reduction in mortality Avenell A, Handoll HHG. Cochrane Database of Systematic Reviews 2006
67 Never Forget Osteoporosis treatment & Falls assessment
68
69 Osteoporotic Fractures Sustaining a fragility fracture is the strongest predictor of a future osteoporotic fracture at least doubles the risk of future fractures The risk of further fracture can be halved by anti-resorptive therapy Start treatment; it is never too late
70 Falls 90 % of hip fractures in the elderly result from a fall Prognosis of Falls 20% die within one year 30% are admitted to 24 h care
71 Secondary prevention (bone protection and falls assessment) is of proven value
72 NHFD: Why? Focus attention Benchmark care A drive for sustained improvements Cost effectiveness
73
74 In conclusion Enthusiastic team Regular orthogeriatrician input Experienced surgeon Senior anaesthetist Hip fracture nurse Multidisciplinary input (PT, OT, Dietatien, Discharge coordinator, social service ) Orthogeriatric Ward (Unit) NHFDB
75 Thank you
Audit of perioperative management of patients with fracture neck of femur
 Audit of perioperative management of patients with fracture neck of femur *M Dissanayake 1, N Wijesuriya 2 Registrar in Anaesthesia 1, Consultant Anaesthetist 2, North Colombo Teaching Hospital, Ragama,
Audit of perioperative management of patients with fracture neck of femur *M Dissanayake 1, N Wijesuriya 2 Registrar in Anaesthesia 1, Consultant Anaesthetist 2, North Colombo Teaching Hospital, Ragama,
Rehabilitation - Reducing costs and hospital stay. Dr Elizabeth Aitken Consultant Physician
 Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
Dr Ben Edwards Consultant Anaesthetist Sheffield Teaching Hospitals
 Dr Ben Edwards Consultant Anaesthetist Sheffield Teaching Hospitals 70-75,000 #NOF per annum (costs 2 billion) 10% die within 1 month 33% die within 1 year Operative delays >48hs more than doubles risk
Dr Ben Edwards Consultant Anaesthetist Sheffield Teaching Hospitals 70-75,000 #NOF per annum (costs 2 billion) 10% die within 1 month 33% die within 1 year Operative delays >48hs more than doubles risk
AN AUDIT: THROMBOPROPHYLAXIS FOR TOTAL HIP REPLACEMENT PATIENTS AT NORTHWICK PARK AND CENTRAL MIDDLESEX HOSPITALS
 The West London Medical Journal 2010 Vol 2 No 4 pp 19-24 AN AUDIT: THROMBOPROPHYLAXIS FOR TOTAL HIP REPLACEMENT PATIENTS AT NORTHWICK PARK AND CENTRAL MIDDLESEX HOSPITALS Soneji ND Agni NR Acharya MN Anjari
The West London Medical Journal 2010 Vol 2 No 4 pp 19-24 AN AUDIT: THROMBOPROPHYLAXIS FOR TOTAL HIP REPLACEMENT PATIENTS AT NORTHWICK PARK AND CENTRAL MIDDLESEX HOSPITALS Soneji ND Agni NR Acharya MN Anjari
SAFE HIP FRACTURES. Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust
 SAFE HIP FRACTURES Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust Why hip fracture? Common in older adult (~84 years) UK current incidence : 70000 (Stockport
SAFE HIP FRACTURES Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust Why hip fracture? Common in older adult (~84 years) UK current incidence : 70000 (Stockport
Hip Fracture (HFR) Measures Document
 Measures Document") Hip Fracture (HFR) Measures Document HFR Version: 2 - covering patients discharged between 01/10/2017 and present. Programme Lead: Sam Doddridge Clinical Leads: Ms Phil Thorpe Dr John Tsang Number of Measures
Hip Fracture (HFR) Measures Document HFR Version: 2 - covering patients discharged between 01/10/2017 and present. Programme Lead: Sam Doddridge Clinical Leads: Ms Phil Thorpe Dr John Tsang Number of Measures
The Peterborough experience over the years with hip fractures. Martyn Parker Peterborough UK
 The Peterborough experience over the years with hip fractures Martyn Parker Peterborough UK PETERBOROUGH HIP FRACTURE PROJECT Avoid delays to surgery Minimally invasive surgery by experienced staff Unrestricted
The Peterborough experience over the years with hip fractures Martyn Parker Peterborough UK PETERBOROUGH HIP FRACTURE PROJECT Avoid delays to surgery Minimally invasive surgery by experienced staff Unrestricted
Guidelines to standards. Orthogeriatrics How The UK Care For Fragility Fractures
 Guidelines to standards Orthogeriatrics How The UK Care For Fragility Fractures Karen Hertz-SOTN Advanced Nurse Practitioner The NHFD Project - jointly led by BOA and BGS with the involvement of the RCN
Guidelines to standards Orthogeriatrics How The UK Care For Fragility Fractures Karen Hertz-SOTN Advanced Nurse Practitioner The NHFD Project - jointly led by BOA and BGS with the involvement of the RCN
Role and impact of orthogeriatric service in the hip fracture care pathway: 15-year experience
 Role and impact of orthogeriatric service in the hip fracture care pathway: 15-year experience AA Fisher, MW Davis Department of Geriatric Medicine, The Canberra Hospital, and Australian National University
Role and impact of orthogeriatric service in the hip fracture care pathway: 15-year experience AA Fisher, MW Davis Department of Geriatric Medicine, The Canberra Hospital, and Australian National University
Effect of Ortho-Geriatric Co-Management on Hip Fractures
 Effect of Ortho-Geriatric Co-Management on Hip Fractures Kenji Shigemoto Takeshi Sawaguchi Daigo Sakagoshi Kenichi Goshima Yu Hatsuchi Dept. Orthop. Surg. Toyama Municipal Hospital, Toyama, Japan Purpose
Effect of Ortho-Geriatric Co-Management on Hip Fractures Kenji Shigemoto Takeshi Sawaguchi Daigo Sakagoshi Kenichi Goshima Yu Hatsuchi Dept. Orthop. Surg. Toyama Municipal Hospital, Toyama, Japan Purpose
Implementing a new Orthogeriatric model to improve patient care and outcomes Aiming for Excellence!
 Implementing a new Orthogeriatric model to improve patient care and outcomes Aiming for Excellence! Introduction Hip fractures effect 70,000 people in UK Central challenge for UK Trauma services- 560 in
Implementing a new Orthogeriatric model to improve patient care and outcomes Aiming for Excellence! Introduction Hip fractures effect 70,000 people in UK Central challenge for UK Trauma services- 560 in
Dr Micheal Looney Consultant Anaesthetist Connolly Hospital Blanchardstown. To Delay or Not to Delay Hip Fracture Surgery
 Dr Micheal Looney Consultant Anaesthetist Connolly Hospital Blanchardstown To Delay or Not to Delay Hip Fracture Surgery "You may delay, but time will not, and lost time is never found again." Benjamin
Dr Micheal Looney Consultant Anaesthetist Connolly Hospital Blanchardstown To Delay or Not to Delay Hip Fracture Surgery "You may delay, but time will not, and lost time is never found again." Benjamin
IAEM Clinical Guideline 11 Management of Patients with Suspected Hip Fracture in the Emergency Department
 IAEM Clinical Guideline 11 Management of Patients with Suspected Hip Fracture in the Emergency Department Version 1 September 2018 Authors: Dr Mary Moore, Ms Marianne Walsh, Dr Termizi Hassan Guideline
IAEM Clinical Guideline 11 Management of Patients with Suspected Hip Fracture in the Emergency Department Version 1 September 2018 Authors: Dr Mary Moore, Ms Marianne Walsh, Dr Termizi Hassan Guideline
The Experience in Exeter with. hip fracture care. Data For Change
 The Experience in Exeter with hip fracture care Data For Change John Charity Associate Specialist in T&O, Lead NHFD Clinician, Royal Devon and Exeter NHS Foundation Trust Respond Deliver & Enable People
The Experience in Exeter with hip fracture care Data For Change John Charity Associate Specialist in T&O, Lead NHFD Clinician, Royal Devon and Exeter NHS Foundation Trust Respond Deliver & Enable People
My hip fracture care: 12 questions to ask A guide for patients, their families and carers
 My hip fracture care: 12 questions to ask A guide for patients, their families and carers About this guide This guide is aimed at patients who have a hip fracture, and their families and carers. It explains
My hip fracture care: 12 questions to ask A guide for patients, their families and carers About this guide This guide is aimed at patients who have a hip fracture, and their families and carers. It explains
Scottish Standards of Care for Hip Fracture Patients
 Scottish Standards of Care for Hip Fracture Patients This document has been prepared in collaboration with Healthcare Improvement Scotland to align with the forthcoming updated Older People in Hospitals
Scottish Standards of Care for Hip Fracture Patients This document has been prepared in collaboration with Healthcare Improvement Scotland to align with the forthcoming updated Older People in Hospitals
Effect of age, sex, co morbidities, delay in surgery and complications on outcome in elderly with proximal femur fractures
 2018; 4(3): 498-506 ISSN: 2395-1958 IJOS 2018; 4(3): 498-506 2018 IJOS www.orthopaper.com Received: 27-05-2018 Accepted: 28-06-2018 P Venu Gopala Reddy Assistant Professor, Department of Orthopaedic Surgery,
2018; 4(3): 498-506 ISSN: 2395-1958 IJOS 2018; 4(3): 498-506 2018 IJOS www.orthopaper.com Received: 27-05-2018 Accepted: 28-06-2018 P Venu Gopala Reddy Assistant Professor, Department of Orthopaedic Surgery,
The in-hospital management of COPD-exacerbation includes three core processes:
 Appendix 1A. Process flow for in-hospital management of COPDexacerbation The in-hospital management of COPD-exacerbation includes three core processes: 1. Diagnostic assessment 2. Pharmacological management
Appendix 1A. Process flow for in-hospital management of COPDexacerbation The in-hospital management of COPD-exacerbation includes three core processes: 1. Diagnostic assessment 2. Pharmacological management
Anticoagulation for prevention of venous thromboembolism
 Anticoagulation for prevention of venous thromboembolism Original article by: Michael Tam Note: updated in June 2009 with the eighth edition (from the seventh) evidence-based clinical practice guidelines
Anticoagulation for prevention of venous thromboembolism Original article by: Michael Tam Note: updated in June 2009 with the eighth edition (from the seventh) evidence-based clinical practice guidelines
Clinical Care Team approach to management of key conditions
 Clinical Care Team approach to management of key conditions BJD Ho Chi Minh City Nov 30, 2012 Kristina Åkesson, MD, PhD Dept of Orthopedics Malmö University Hospital Lund University Malmö, Sweden Multidisciplinary
Clinical Care Team approach to management of key conditions BJD Ho Chi Minh City Nov 30, 2012 Kristina Åkesson, MD, PhD Dept of Orthopedics Malmö University Hospital Lund University Malmö, Sweden Multidisciplinary
Misunderstandings of Venous thromboembolism prophylaxis
 Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
The Geriatrician in the Trauma Service. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013
 Annual Scientific Meeting and Training 2013") The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
Title. Lau, TW; Fang, CX; Leung, FKL. Geriatric Orthopaedic Surgery and Rehabilitation, 2013, v. 4 n. 1, p Citation.
 Title The Effectiveness of a Geriatric Hip Fracture Clinical Pathway in Reducing Hospital and Rehabilitation Length of Stay and Improving Short-Term Mortality Rates Author(s) Lau, TW; Fang, CX; Leung,
Title The Effectiveness of a Geriatric Hip Fracture Clinical Pathway in Reducing Hospital and Rehabilitation Length of Stay and Improving Short-Term Mortality Rates Author(s) Lau, TW; Fang, CX; Leung,
Management of Hip Fractures
 Management of Hip Fractures in the Elderly Patient David A. Brown MD COL U.S. Army Ret. The Center for Orthopedics and Neurosurgery Optimizing Management of Hip Fractures in the Elderly Patient Optimizing
Management of Hip Fractures in the Elderly Patient David A. Brown MD COL U.S. Army Ret. The Center for Orthopedics and Neurosurgery Optimizing Management of Hip Fractures in the Elderly Patient Optimizing
1. SCOPE of GUIDELINE:
 Page 1 of 35 CLINICAL PRACTICE GUIDELINE: Venous Thromboembolism (VTE) Prevention Guideline: Thromboprophylaxis AUTHORIZATION: VP, Medicine Date Approved: May 17, 2012 Date Revised: Vancouver Coastal Health
Page 1 of 35 CLINICAL PRACTICE GUIDELINE: Venous Thromboembolism (VTE) Prevention Guideline: Thromboprophylaxis AUTHORIZATION: VP, Medicine Date Approved: May 17, 2012 Date Revised: Vancouver Coastal Health
Peterborough Community Rehabilitation Schemes. Martyn Parker
 Peterborough Community Rehabilitation Schemes Martyn Parker Peterborough Hospital at Home Established 1987 Provided home care for patients Initially used by for hip fracture patients and after hysterectomy
Peterborough Community Rehabilitation Schemes Martyn Parker Peterborough Hospital at Home Established 1987 Provided home care for patients Initially used by for hip fracture patients and after hysterectomy
Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement. Marilyn Szekendi, PhD, RN
 Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement Marilyn Szekendi, PhD, RN ANA 7 th Annual Nursing Quality Conference, February 2013 Research Team Banafsheh Sadeghi,
Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement Marilyn Szekendi, PhD, RN ANA 7 th Annual Nursing Quality Conference, February 2013 Research Team Banafsheh Sadeghi,
Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley
 Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley British Journal of Surgery 2013; 100: 1045 1049 The risk of 30 day mortality
Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley British Journal of Surgery 2013; 100: 1045 1049 The risk of 30 day mortality
Geriatric Hip Fracture Co-Management. Pannida Wattanapanom, M.D., FACP.
 Geriatric Hip Fracture Co-Management Pannida Wattanapanom, M.D., FACP. An 80 year old man with a hip fracture The General Medicine approach: Medical clearance for surgery Role of Geriatrician Assess caused
Geriatric Hip Fracture Co-Management Pannida Wattanapanom, M.D., FACP. An 80 year old man with a hip fracture The General Medicine approach: Medical clearance for surgery Role of Geriatrician Assess caused
Falls and Fragility Fracture Audit Programme
 Falls and Fragility Fracture Audit Programme Update for Healthcare Conference 5 th November 2014 Dr Helen Wilson Member of FFFAP Executive Board Content The Falls and Fragility Fracture Audit Programme
Falls and Fragility Fracture Audit Programme Update for Healthcare Conference 5 th November 2014 Dr Helen Wilson Member of FFFAP Executive Board Content The Falls and Fragility Fracture Audit Programme
Komorbiditet og ortopædkirugi - erfaringer og viden. Benn Rønnow Duus, Ledende overlæge, Ortopædkirurgisk afdeling Bispebjerg Hospital
 Komorbiditet og ortopædkirugi - erfaringer og viden Benn Rønnow Duus, Ledende overlæge, Ortopædkirurgisk afdeling Bispebjerg Hospital Kræft og komorbiditet alle skal have del i de gode resultater 1 Kræftens
Komorbiditet og ortopædkirugi - erfaringer og viden Benn Rønnow Duus, Ledende overlæge, Ortopædkirurgisk afdeling Bispebjerg Hospital Kræft og komorbiditet alle skal have del i de gode resultater 1 Kræftens
Anaesthesia & The Hip Fracture Patient
 Anaesthesia & The Hip Fracture Patient Richard Griffiths MD FRCA Peterborough & Stamford Hospitals Thursday, 25 July 13 Declarations of Interest Honorary Secretary of the Association of Anaesthetists of
Anaesthesia & The Hip Fracture Patient Richard Griffiths MD FRCA Peterborough & Stamford Hospitals Thursday, 25 July 13 Declarations of Interest Honorary Secretary of the Association of Anaesthetists of
Care of older people in surgery (COPS)
") Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
*Corresponding Author:
 Audit of venous thromboembolism prophylaxis administered to general surgical patients undergoing elective and emergency operations at National Hospital, Sri Lanka *Migara Seneviratne 1, Asanka Hemachandra
Audit of venous thromboembolism prophylaxis administered to general surgical patients undergoing elective and emergency operations at National Hospital, Sri Lanka *Migara Seneviratne 1, Asanka Hemachandra
Risk factors affecting inhospital mortality after hip fracture: retrospective analysis using the Japanese Diagnosis Procedure Combination Database
 Open Access To cite: Shoda N, Yasunaga H, Horiguchi H, et al. Risk factors affecting inhospital mortality after hip fracture: retrospective analysis using the Japanese Diagnosis Procedure Combination Database.
Open Access To cite: Shoda N, Yasunaga H, Horiguchi H, et al. Risk factors affecting inhospital mortality after hip fracture: retrospective analysis using the Japanese Diagnosis Procedure Combination Database.
Appendix E : Evidence table 9 Rehabilitation: Other Key Documents
 Appendix E : Evidence table 9 Rehabilitation: Other Key Documents 1. Cameron et al. Geriatric rehabilitation following following fractures in older people: a systematic review. Health Technology Assessment
Appendix E : Evidence table 9 Rehabilitation: Other Key Documents 1. Cameron et al. Geriatric rehabilitation following following fractures in older people: a systematic review. Health Technology Assessment
Death by Bedrest: The Perils of The Hospital
 Death by Bedrest: The Perils of The Hospital Mindy Fain, MD Professor of Clinical Medicine Director, Arizona Reynolds Program of Applied Geriatrics Section Head, Geriatrics & Gerontology University of
Death by Bedrest: The Perils of The Hospital Mindy Fain, MD Professor of Clinical Medicine Director, Arizona Reynolds Program of Applied Geriatrics Section Head, Geriatrics & Gerontology University of
Striving to improve hip fracture care
 Striving to improve hip fracture care The UHL experience 2008-2015 Mr F. Condon, Consultant Orthopaedic Surgeon Ms Jude Ryan, Consultant Ortho-Geriatrician (Mat Leave) & A. Butler Orthopaedic CNS (Mat
Striving to improve hip fracture care The UHL experience 2008-2015 Mr F. Condon, Consultant Orthopaedic Surgeon Ms Jude Ryan, Consultant Ortho-Geriatrician (Mat Leave) & A. Butler Orthopaedic CNS (Mat
What is the shared care model for the Hip fracture patient The Ortho-geriatric Model of Care at St Vincent s Public Hospital Our team and how we make
 What is the shared care model for the Hip fracture patient The Ortho-geriatric Model of Care at St Vincent s Public Hospital Our team and how we make it work! Benefits of a Shared Care Model The Shared
What is the shared care model for the Hip fracture patient The Ortho-geriatric Model of Care at St Vincent s Public Hospital Our team and how we make it work! Benefits of a Shared Care Model The Shared
Fragility Fracture Network - FFN
 Fragility Fracture Network - FFN A Global Multidisciplinary Network to Improve Fragility Fracture Management and Prevention Ami Hommel RN, CNS, PhD, Associate Professor Lund University & Skane university
Fragility Fracture Network - FFN A Global Multidisciplinary Network to Improve Fragility Fracture Management and Prevention Ami Hommel RN, CNS, PhD, Associate Professor Lund University & Skane university
A new future for hip fracture care orthogeriatrician lead in an Acute Hip Unit
 Clinical Medicine 2014 Vol 14, No 6: 591 6 CLINICAL PRACTICE A new future for hip fracture care orthogeriatrician lead in an Acute Hip Unit Authors: Abhaya Gupta A and William Havelock B ABSTRACT Although
Clinical Medicine 2014 Vol 14, No 6: 591 6 CLINICAL PRACTICE A new future for hip fracture care orthogeriatrician lead in an Acute Hip Unit Authors: Abhaya Gupta A and William Havelock B ABSTRACT Although
A Best Practice Clinical Care Pathway for Major Amputation Surgery
 A Best Practice Clinical Care Pathway for Major Amputation Surgery April 2016 Introduction The perioperative mortality rate after major lower limb amputation in the UK is unacceptably high in modern medical
A Best Practice Clinical Care Pathway for Major Amputation Surgery April 2016 Introduction The perioperative mortality rate after major lower limb amputation in the UK is unacceptably high in modern medical
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies
 VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
Admit date (YYYY/MM/DD): Cardiologist On-Call: Diagnosis: Lab Tests. CBC, Electrolytes, Urea, Creatinine, Glucose, INR, PTT, Urinalysis
: Cardiologist On-Call: Diagnosis: Lab Tests. CBC, Electrolytes, Urea, Creatinine, Glucose, INR, PTT, Urinalysis") of nurse 1. Admit under ward Attending Physician: Dr. Admit date (YYYY/MM/DD): Cardiologist On-Call: Diagnosis: Lab Tests 2. On admission (if not already performed in Emergency Department or in Coronary
of nurse 1. Admit under ward Attending Physician: Dr. Admit date (YYYY/MM/DD): Cardiologist On-Call: Diagnosis: Lab Tests 2. On admission (if not already performed in Emergency Department or in Coronary
SIGN. Management of hip fracture in older people. June A national clinical guideline. Scottish Intercollegiate Guidelines Network
 SIGN Scottish Intercollegiate Guidelines Network Part of NHS Quality Improvement Scotland 111 Management of hip fracture in older people A national clinical guideline June 2009 KEY TO EVIDENCE STATEMENTS
SIGN Scottish Intercollegiate Guidelines Network Part of NHS Quality Improvement Scotland 111 Management of hip fracture in older people A national clinical guideline June 2009 KEY TO EVIDENCE STATEMENTS
Acute Care of Older Surgical Patients. Dr Shane O Hanlon Consultant Geriatrician St Vincent s University Hospital IHFM 8 th Nov 2017
 Acute Care of Older Surgical Patients Dr Shane O Hanlon Consultant Geriatrician St Vincent s University Hospital IHFM 8 th Nov 2017 NCEPOD 2010 overall care % 50 45 40 35 30 25 20 15 10 5 0 Good practice
Acute Care of Older Surgical Patients Dr Shane O Hanlon Consultant Geriatrician St Vincent s University Hospital IHFM 8 th Nov 2017 NCEPOD 2010 overall care % 50 45 40 35 30 25 20 15 10 5 0 Good practice
TITLE: Acetylsalicylic Acid for Venous Thromboembolism Prophylaxis: A Review of Clinical Evidence, Benefits and Harms
 TITLE: Acetylsalicylic Acid for Venous Thromboembolism Prophylaxis: A Review of Clinical Evidence, Benefits and Harms DATE: 23 August 2011 CONTEXT AND POLICY ISSUES: Thromboembolism occurs when a blood
TITLE: Acetylsalicylic Acid for Venous Thromboembolism Prophylaxis: A Review of Clinical Evidence, Benefits and Harms DATE: 23 August 2011 CONTEXT AND POLICY ISSUES: Thromboembolism occurs when a blood
Anaesthesia. Clinical overview articles. Update in. Neck of femur fracture: perioperative management. Ronald Cheung
 Neck of femur fracture: perioperative management Ronald Cheung Correspondence: roncheung39@gmail.com Originally published as Anaesthesia Tutorial of the Week 296, 21 October 2013 INTRODUCTION Several large
Neck of femur fracture: perioperative management Ronald Cheung Correspondence: roncheung39@gmail.com Originally published as Anaesthesia Tutorial of the Week 296, 21 October 2013 INTRODUCTION Several large
Hospital at Home. Frailty and Hospital at Home. 17 th March Pam Livingstone and Gwyneth Thom
 Hospital at Home Frailty and Hospital at Home 17 th March 2016 Pam Livingstone and Gwyneth Thom National Definition of Hospital at Home December 2013 An episode of specialist care delivered at home as
Hospital at Home Frailty and Hospital at Home 17 th March 2016 Pam Livingstone and Gwyneth Thom National Definition of Hospital at Home December 2013 An episode of specialist care delivered at home as
HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD
 HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting honorariums or other payments
HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting honorariums or other payments
Introduction. Peripheral arterial disease. Hospital inpatient data - 5,498 FCE (2009/10), & 530 deaths in England alone
, & 530 deaths in England alone") 1 Introduction 2 Introduction Peripheral arterial disease Affects 20% adults in Europe and North America In the UK 500-1000/million PAD, 1-2% require amputation LLA 8-15% in people with diabetes with up
1 Introduction 2 Introduction Peripheral arterial disease Affects 20% adults in Europe and North America In the UK 500-1000/million PAD, 1-2% require amputation LLA 8-15% in people with diabetes with up
Hip Fracture Orthopaedic Department Patient Information Leaflet
 riginator: Anne Flavall Professional Development Lead, Mr Marsh and Mr Quraishi Orthopaedic Consultant Surgeons Date: March 2012 Version: 2 Date for Review: March 2015 DGOH Ref No: DGOH/PIL/00611 Hip Fracture
riginator: Anne Flavall Professional Development Lead, Mr Marsh and Mr Quraishi Orthopaedic Consultant Surgeons Date: March 2012 Version: 2 Date for Review: March 2015 DGOH Ref No: DGOH/PIL/00611 Hip Fracture
Dynamic hip screw (sliding hip screw)
") Dynamic hip screw (sliding hip screw) Trauma and Orthopaedics Patient Information Leaflet Introduction This leaflet is about an operation called a dynamic hip screw, sometimes also known as a sliding hip
Dynamic hip screw (sliding hip screw) Trauma and Orthopaedics Patient Information Leaflet Introduction This leaflet is about an operation called a dynamic hip screw, sometimes also known as a sliding hip
NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE. Measure Information Form
 Last Updated: Version 4.3 NQF-ENORSE VOLUNTARY CONSENSUS STANARS FOR HOSPITAL CARE Measure Information Form Measure Set: Venous Thromboembolism (VTE) Set Measure Set I #: Performance Measure Name: Intensive
Last Updated: Version 4.3 NQF-ENORSE VOLUNTARY CONSENSUS STANARS FOR HOSPITAL CARE Measure Information Form Measure Set: Venous Thromboembolism (VTE) Set Measure Set I #: Performance Measure Name: Intensive
Accompanied to walk Yes No Accompanied to walk Yes No Side of Fracture
 Fracture Neck Of Femur / Fast Track Criteria: Admission where femoral neck fracture is the primary diagnosis Accident & Emergency Assessment (To be completed by A/E Nurse and/or A/E doctor) Patient label
Fracture Neck Of Femur / Fast Track Criteria: Admission where femoral neck fracture is the primary diagnosis Accident & Emergency Assessment (To be completed by A/E Nurse and/or A/E doctor) Patient label
Cumulated Ambulation Score to evaluate mobility is feasible in geriatric patients and in patients with hip fracture
 Cumulated Ambulation Score to evaluate mobility is feasible in geriatric patients and in patients with hip fracture Morten Tange Kristensen 1, 2,Thomas Linding Jakobsen 3, 4, Jesper Westphal Nielsen 1,
Cumulated Ambulation Score to evaluate mobility is feasible in geriatric patients and in patients with hip fracture Morten Tange Kristensen 1, 2,Thomas Linding Jakobsen 3, 4, Jesper Westphal Nielsen 1,
Hemiarthroplasty (half hip replacement)
") Hemiarthroplasty (half hip replacement) Trauma and Orthopaedics Patient Information Leaflet Introduction This leaflet is about an operation called a half hip replacement. It gives information about the
Hemiarthroplasty (half hip replacement) Trauma and Orthopaedics Patient Information Leaflet Introduction This leaflet is about an operation called a half hip replacement. It gives information about the
Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami
 Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami James Holstine, DO Medical Director for the Joint Replacement Center, Geriatric Fracture Center, Orthopedic Surgeon PeaceHealth Whatcom
Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami James Holstine, DO Medical Director for the Joint Replacement Center, Geriatric Fracture Center, Orthopedic Surgeon PeaceHealth Whatcom
THE NEW ZEALAND MEDICAL JOURNAL Vol 118 No 1214 ISSN
 THE NEW ZEALAND MEDICAL JOURNAL Vol 118 No 1214 ISSN 1175 8716 Shared care between geriatricians and orthopaedic surgeons as a model of care for older patients with hip fractures John Thwaites, Fazal Mann,
THE NEW ZEALAND MEDICAL JOURNAL Vol 118 No 1214 ISSN 1175 8716 Shared care between geriatricians and orthopaedic surgeons as a model of care for older patients with hip fractures John Thwaites, Fazal Mann,
National Hip Fracture Database North West Regional Meeting 13th March 2013 Planning patient care and achieving Best Practice Tariff
 National Hip Fracture Database North West Regional Meeting 13th March 2013 Planning patient care and achieving Best Practice Tariff Dr John Tsang MB ChB, FRCP Consultant Orthogeriatrician Lead clinician
National Hip Fracture Database North West Regional Meeting 13th March 2013 Planning patient care and achieving Best Practice Tariff Dr John Tsang MB ChB, FRCP Consultant Orthogeriatrician Lead clinician
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care
 Accelero Health Partners, 2015 WHITE PAPER Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Jason Pry, Senior Director ABSTRACT Every year more than a quarter of a million
Accelero Health Partners, 2015 WHITE PAPER Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Jason Pry, Senior Director ABSTRACT Every year more than a quarter of a million
Fractured Neck of Femur Proforma Orthopaedic Unit. First name: Registration no: Date of birth: Age:
 Fractured Neck of Femur Proforma Orthopaedic Unit Date: Surname : ED doctor s name: Time seen: Orthopaedic admitting doctor s name: Time seen: Presenting complaint and history of fall: First name: Registration
Fractured Neck of Femur Proforma Orthopaedic Unit Date: Surname : ED doctor s name: Time seen: Orthopaedic admitting doctor s name: Time seen: Presenting complaint and history of fall: First name: Registration
DOAC and NOAC are terms for a novel class of directly acting oral anticoagulant drugs including Rivaroxaban, Apixaban, Edoxaban, and Dabigatran.
 Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
How to limit avoidable disability
 How to limit avoidable disability Associate professor Susanne S Hernes Sept.22. 2017 Add the logo of your institution here CONFLICT OF INTEREST DISCLOSURE I have no potential conflicts of interest to report
How to limit avoidable disability Associate professor Susanne S Hernes Sept.22. 2017 Add the logo of your institution here CONFLICT OF INTEREST DISCLOSURE I have no potential conflicts of interest to report
FRAGILITY FRACTURE REGISTRY IN HONG KONG. Dr. WK NGAI COC (O&T), Hospital Authority
, Hospital Authority") FRAGILITY FRACTURE REGISTRY IN HONG KONG Dr. WK NGAI COC (O&T), Hospital Authority Osteoporosis - Silent Epidemic Every year, 2 million fractures occur in USA that no accident, but signs of osteoporosis
FRAGILITY FRACTURE REGISTRY IN HONG KONG Dr. WK NGAI COC (O&T), Hospital Authority Osteoporosis - Silent Epidemic Every year, 2 million fractures occur in USA that no accident, but signs of osteoporosis
Optimising Perioperative Pain Management And Surgical Outcomes
 Optimising Perioperative Pain Management And Surgical Outcomes Dr Chew Ghee Kheng MBBS FRCOG MD FAMS Senior Consultant Gynaecologist Subspecialist in Gynaecology Oncology Surgery Singapore General Hospital
Optimising Perioperative Pain Management And Surgical Outcomes Dr Chew Ghee Kheng MBBS FRCOG MD FAMS Senior Consultant Gynaecologist Subspecialist in Gynaecology Oncology Surgery Singapore General Hospital
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture
 Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Our Experience as Mortality Outliers. Calderdale and Huddersfield NHS Foundation Trust Chris Ramsdale Sudhi Ankarath
 Our Experience as Mortality Outliers Calderdale and Huddersfield NHS Foundation Trust Chris Ramsdale Sudhi Ankarath Where were we? 2 orthopaedic wards 61 beds Patients admitted wherever the empty bed was
Our Experience as Mortality Outliers Calderdale and Huddersfield NHS Foundation Trust Chris Ramsdale Sudhi Ankarath Where were we? 2 orthopaedic wards 61 beds Patients admitted wherever the empty bed was
Multidisciplinary Geriatric Trauma Care Guideline
 Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care
 Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Every year more than a quarter of a million people over the age of 65 are admitted to a hospital with a hip fracture. Mortality
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Every year more than a quarter of a million people over the age of 65 are admitted to a hospital with a hip fracture. Mortality
Prevention and Management of Hip Fracture in Older People
 Scottish Intercollegiate Guidelines Network 56 Prevention and Management of Hip Fracture in Older People A national clinical guideline 1 Introduction 1 2 Prevention of hip fracture 4 3 Pre-hospital management
Scottish Intercollegiate Guidelines Network 56 Prevention and Management of Hip Fracture in Older People A national clinical guideline 1 Introduction 1 2 Prevention of hip fracture 4 3 Pre-hospital management
Please inform the Diabetes Nurse Specialist that this patient has been admitted within 24hrs of admission.
 Adult Diabetic Ketoacidosis Care Bundle (V1. Issued October 2014 Review October 2015) Improving patient care This pack includes: DKA Management Guideline Name: (Patient Addressograph) DOB: Hospital No:
Adult Diabetic Ketoacidosis Care Bundle (V1. Issued October 2014 Review October 2015) Improving patient care This pack includes: DKA Management Guideline Name: (Patient Addressograph) DOB: Hospital No:
Quality improvement for patients with hip fracture: experience from a multi-site audit
 QUALITY IMPROVEMENT REPORT Quality improvement for patients with hip fracture: experience from a multi-site audit C Freeman, C Todd, C Camilleri-Ferrante, C Laxton, P Murrell, C R Palmer, M Parker, B Payne,
QUALITY IMPROVEMENT REPORT Quality improvement for patients with hip fracture: experience from a multi-site audit C Freeman, C Todd, C Camilleri-Ferrante, C Laxton, P Murrell, C R Palmer, M Parker, B Payne,
Venous Thromboembolism (VTE) Prevention and Treatment of VTE in Patients Admitted to Hospital
 Prevention and Treatment of VTE in Patients Admitted to Hospital") Please Note: This policy is currently under review and is still fit for purpose. Venous Thromboembolism (VTE) Prevention and Treatment of VTE in Patients Admitted to Hospital This procedural document supersedes
Please Note: This policy is currently under review and is still fit for purpose. Venous Thromboembolism (VTE) Prevention and Treatment of VTE in Patients Admitted to Hospital This procedural document supersedes
Venous Thromboembolism. Prevention
 Venous Thromboembolism Prevention August 2010 Venous Thromboembloism Prevention 1 1 Expected Practice Assess all patients upon admission to the ICU for risk factors of venous thromboembolism (VTE) and
Venous Thromboembolism Prevention August 2010 Venous Thromboembloism Prevention 1 1 Expected Practice Assess all patients upon admission to the ICU for risk factors of venous thromboembolism (VTE) and
Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders
 SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
Objectives. Venous Thromboembolism (VTE) Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?
 Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?") Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Connecticut Joint Replacement Institute (CJRI) Outcomes Report
 Outcomes Report") Connecticut Joint Replacement Institute () Outcomes Report Our Highlights: Nationally recognized Over 27,000 surgeries performed Devoted to excellence in patient care Proven superior outcomes that matter.
Connecticut Joint Replacement Institute () Outcomes Report Our Highlights: Nationally recognized Over 27,000 surgeries performed Devoted to excellence in patient care Proven superior outcomes that matter.
SUBJECT: LIMB PNEUMATIC COMPRESSION EFFECTIVE DATE: 06/27/13 DEVICES FOR VENOUS REVISED DATE: 06/26/14 THROMBOEMBOLISM PROPHYLAXIS
 MEDICAL POLICY SUBJECT: LIMB PNEUMATIC COMPRESSION PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical
MEDICAL POLICY SUBJECT: LIMB PNEUMATIC COMPRESSION PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical
Shared Care Protocol for the Prescription and Supply of Low Molecular Weight Heparins
 Tameside Hospital NHS Foundation Trust and NHS Tameside and Glossop Shared Care Protocol for the Prescription and Supply of Low Molecular Weight Heparins Version 5.2 Version: 5.2 Authorised by: Joint Medicines
Tameside Hospital NHS Foundation Trust and NHS Tameside and Glossop Shared Care Protocol for the Prescription and Supply of Low Molecular Weight Heparins Version 5.2 Version: 5.2 Authorised by: Joint Medicines
Fatal P.E. Historic 1-2% Current %
 Dr. (Prof.) Anil Arora MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London, UK) Senior
Dr. (Prof.) Anil Arora MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London, UK) Senior
MAINTAINING GOOD HEALTH FOR OLDER PEOPLE WITH DEMENTIA WHO EXPERIENCE FRACTURED NECK OF FEMUR: REPORT FOR PHASE 2
 MAINTAINING GOOD HEALTH FOR OLDER PEOPLE WITH DEMENTIA WHO EXPERIENCE FRACTURED NECK OF FEMUR: REPORT FOR PHASE 2 Catherine Henderson, Juliette Malley and Martin Knapp 1 Personal Social Services Research
MAINTAINING GOOD HEALTH FOR OLDER PEOPLE WITH DEMENTIA WHO EXPERIENCE FRACTURED NECK OF FEMUR: REPORT FOR PHASE 2 Catherine Henderson, Juliette Malley and Martin Knapp 1 Personal Social Services Research
Title: Low Molecular Weight Heparins (LMWH), fondaparinux (Arixtra)
, fondaparinux (Arixtra)") Origination: 03/29/05 Revised: 09/01/10 Annual Review: 11/20/13 Purpose: To provide guidelines and criteria for the review and decision determination of requests for medications that requires prior authorization.
Origination: 03/29/05 Revised: 09/01/10 Annual Review: 11/20/13 Purpose: To provide guidelines and criteria for the review and decision determination of requests for medications that requires prior authorization.
of the Bone and Joint Decade The Global Challenge of Fragility Fractures and the Role of Fragility fracture Network
 of the Bone and Joint Decade The Global Challenge of Fragility Fractures and the Role of Fragility fracture Network The Fragility Fracture Network of the Bone and Joint Decade Mission: To promote globally
of the Bone and Joint Decade The Global Challenge of Fragility Fractures and the Role of Fragility fracture Network The Fragility Fracture Network of the Bone and Joint Decade Mission: To promote globally
Anaemia impedes functional mobility after hip fracture surgery
 Age and Ageing 2008; 37: 173 178 doi:10.1093/ageing/afm161 The Author 2008. Published by Oxford University Press on behalf of the British Geriatrics Society. All rights reserved. For Permissions, please
Age and Ageing 2008; 37: 173 178 doi:10.1093/ageing/afm161 The Author 2008. Published by Oxford University Press on behalf of the British Geriatrics Society. All rights reserved. For Permissions, please
Prevention of Venous Thromboembolism
 Prevention of Venous Thromboembolism Surgical Care Improvement Project Dale W. Bratzler, DO, MPH President and CEO Dale W. Bratzler, DO, MPH Oklahoma Foundation for Medical Quality QIOSC Medical Director
Prevention of Venous Thromboembolism Surgical Care Improvement Project Dale W. Bratzler, DO, MPH President and CEO Dale W. Bratzler, DO, MPH Oklahoma Foundation for Medical Quality QIOSC Medical Director
NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE. Measure Information Form. Performance Measure Name: Venous Thromboembolism Prophylaxis
 Last Updated: Version 4.3 NQF-ENORSE VOLUNTARY CONSENSUS STANARS FOR HOSPITAL CARE Measure Information Form Measure Set: Venous Thromboembolism (VTE) Set Measure Set I #: Performance Measure Name: Venous
Last Updated: Version 4.3 NQF-ENORSE VOLUNTARY CONSENSUS STANARS FOR HOSPITAL CARE Measure Information Form Measure Set: Venous Thromboembolism (VTE) Set Measure Set I #: Performance Measure Name: Venous
Development and Utilization of Standardized Hip Fracture Guidelines
 Development and Utilization of Standardized Hip Fracture Guidelines Sally Knight RN Clinical Quality Nurse Lori Smith RN Clinical Quality Nurse Deborah Newall RN Orthopedic Program Coordinator Wallace
Development and Utilization of Standardized Hip Fracture Guidelines Sally Knight RN Clinical Quality Nurse Lori Smith RN Clinical Quality Nurse Deborah Newall RN Orthopedic Program Coordinator Wallace
Improving Healthcare Utilization in Injured Older Adults
 Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Venous Thromboembolism (VTE): Prophylaxis and the Incidence of Hospital Acquired VTE(HAQ VTE) Olaide Akande, MBChB Mentor: John Hall, MD, FACP
: Prophylaxis and the Incidence of Hospital Acquired VTE(HAQ VTE) Olaide Akande, MBChB Mentor: John Hall, MD, FACP") Venous Thromboembolism (VTE): Prophylaxis and the Incidence of Hospital Acquired VTE(HAQ VTE) Olaide Akande, MBChB Mentor: John Hall, MD, FACP Outline Rationale Background Objective Methods Results Conclusion
Venous Thromboembolism (VTE): Prophylaxis and the Incidence of Hospital Acquired VTE(HAQ VTE) Olaide Akande, MBChB Mentor: John Hall, MD, FACP Outline Rationale Background Objective Methods Results Conclusion
AMI Talking Points. Provide appropriate treatment to Acute MI patients with these core measures:
 AMI Provide appropriate treatment to Acute MI patients with these core measures: Aspirin received within 24 hours of arrival or contraindication documented Primary PCI Received Within 90 Minutes of Hospital
AMI Provide appropriate treatment to Acute MI patients with these core measures: Aspirin received within 24 hours of arrival or contraindication documented Primary PCI Received Within 90 Minutes of Hospital
Ortho-geriatric Management of the #NOF Patient
 Ortho-geriatric Management of the #NOF Patient Dr Glenise Berry, MBBS,FRACP Geriatrician to the Ortho-geriatric Service PAH 8 th September 2017 For The Qld. Orthopaedic Physiotherapy Network 10.Own the
Ortho-geriatric Management of the #NOF Patient Dr Glenise Berry, MBBS,FRACP Geriatrician to the Ortho-geriatric Service PAH 8 th September 2017 For The Qld. Orthopaedic Physiotherapy Network 10.Own the
Registry Highlights. Dale Daniel Symposium Hip Fracture Registry. Overall Volume by Year and Region 3/7/2014
 Dale Daniel Symposium 2014 Registry Highlights Overview: Updated Volume NCAL/SCAL Snapshot Hip Fracture Registry Update Gary Zohman, MD SCAL Regional Lead Anaheim, CA Quarterly Quality Report Review Future
Dale Daniel Symposium 2014 Registry Highlights Overview: Updated Volume NCAL/SCAL Snapshot Hip Fracture Registry Update Gary Zohman, MD SCAL Regional Lead Anaheim, CA Quarterly Quality Report Review Future
Venous Thromboembolism Prophylaxis: Checked!
 Venous Thromboembolism Prophylaxis: Checked! William Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University of Toronto National Lead, VTE Prevention, Safer
Venous Thromboembolism Prophylaxis: Checked! William Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University of Toronto National Lead, VTE Prevention, Safer
VTE in Children: Practical Issues
 VTE in Children: Practical Issues Wasil Jastaniah MBBS,FAAP,FRCPC Consultant Pediatric Hem/Onc/BMT May 2012 Top 10 Reasons Why Pediatric VTE is Different 1. Social, ethical, and legal implications. 2.
VTE in Children: Practical Issues Wasil Jastaniah MBBS,FAAP,FRCPC Consultant Pediatric Hem/Onc/BMT May 2012 Top 10 Reasons Why Pediatric VTE is Different 1. Social, ethical, and legal implications. 2.
Venous thromboembolism - reducing the risk
 Venous thromboembolism - reducing the risk Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital NICE guideline Draft for consultation,
Venous thromboembolism - reducing the risk Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital NICE guideline Draft for consultation,
Chairs: John Lainchbury & Andrew Aitken. Elderly/Frailty
 Frailty Elderly/Frailty Ralph Stewart Chairs: John Lainchbury & Andrew Aitken Elderly/Frailty Ralph Stewart Green Lane Cardiovascular Service and Cardiovascular Research Unit Auckland City Hospital 1 What
Frailty Elderly/Frailty Ralph Stewart Chairs: John Lainchbury & Andrew Aitken Elderly/Frailty Ralph Stewart Green Lane Cardiovascular Service and Cardiovascular Research Unit Auckland City Hospital 1 What
NICE Guidance: Venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital 1
 in patients admitted to hospital 1") The College of Emergency Medicine Patron: HRH The Princess Royal Churchill House Tel +44 (0)207 404 1999 35 Red Lion Square Fax +44 (0)207 067 1267 London WC1R 4SG www.collemergencymed.ac.uk CLINICAL EFFECTIVENESS
The College of Emergency Medicine Patron: HRH The Princess Royal Churchill House Tel +44 (0)207 404 1999 35 Red Lion Square Fax +44 (0)207 067 1267 London WC1R 4SG www.collemergencymed.ac.uk CLINICAL EFFECTIVENESS