Antifungal therapies differences in agents
|
|
|
- Arron Curtis Bridges
- 5 years ago
- Views:
Transcription
1 Antifungal therapies differences in agents

2 The basic Fungi are eukaryotes Eukaryote = an organism whose cells contain complex structures enclosed within membrane.
3 Most Common Fungal Pathogens Dermatophytes Sporothrix schenckii Candida Penicillium Histoplasma Cryptococcus Aspergillus Rhizopus
4 Fungal Nomenclature YEASTS Moist & creamy MOULDS Filamentous fungi Candida Cryptococcus Trichosporon Curvularia Bipolaris Cladosporium Aseptate Hyphae Zygomycetes Rhizopus Mucor Dematiaceous Septate Hyphae Hyaline Histoplasma P marneffei Sporothrix Dimorphics Opportunists Dermatophytes 2 forms in 2 different temp yeast in body temp & moulds in room temp Koneman, Roberts GD, Practical laboratory mycology 1985 Aspergillus Scedosporium Fusarium Microsporum Trichophyton Epidermophyton
5 The basic Fungal cells = human cells designing antifungal without harm to human cells difficult! Major different btw fungi & human cells = sterol type for plasma membrane Fungal cell wall = ergosterols Human cell wall = cholesterol

6 The (small) world of antifungals Membrane function: Amphotericin B Cellwall synthesis: Echinocandins Ergosterol synthesis: Azoles
7 Antıfungal Drugs - Mode Of Action 1. Membrane disrupting agents - Amphotericin B, nystatin 2. Ergosterol synthesis inhibitors - Azoles, allylamines, morpholine 3. Glucan synthesis inhibitors -Echinocandins 5. Nucleic acid inhibitor - Flucytosine 6. Chitin synthesis inhibitor - Nikkomycin 7. Protein synthesis inhibitors - Sordarins, azasordarins 8. Anti-mitotic (spindle disruption) - Griseofulvin
8 Antıfungal Drugs 1. POLYENES - Amphotericin B, nystatin 2. AZOLES Ketoconazole, Fluconazole, itraconazole, voriconazole, posaconazole, 3. ECHINOCANDINS - Caspofungin, anidulafungin, micafungin 4. FLUORINATED PYRIMIDINE - Flucytosine 5. MORPHOLINE - Amorolfine 6. PEPTIDE-NUCLEOSIDE - Nikkomycin Z 7. TETRAHYDROFURAN DERIVATIVES - Sordarins, azasordarins 8. OTHER - Griseofulvin
9 superficial Mycoses Dermatophytosis (Tinea = Ringworm) & Pityriasis versicolor Fungal infections in human Sub-cutaneous Mycoses Sporotrichosis Systemic Mycoses Candidiasis Penicilliosis Histoplasmosis Cryptococcosis Aspergillosis Zygomycosis


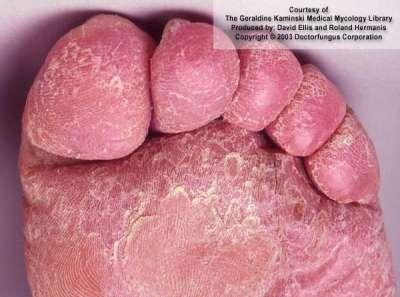

10 Tinea Capitis Tinea Corporis Tinea Pedis Pityriasis Vesicolor
11 Dermatophytosis-Transmission Close human contact Sharing clothes, combs, brushes, towels, bedsheets... (Indirect) Animal-to-human contact (Zoophilic)
12 Dermatophytosis-Treatment 1. Topical - Miconazole, clotrimazole, econazole, terbinafine 2. Oral Griseofulvin, Ketaconazole Itraconazole, Terbinafine
13 superficial Mycoses Dermatophytosis (Tinea = Ringworm) & Pityriasis versicolor Fungal infections in human Sub-cutaneous Mycoses Sporotrichosis Systemic Mycoses Candidiasis Penicilliosis Histoplasmosis Cryptococcosis Aspergillosis Zygomycosis
14 Sporotrichosis - Pathogenesis Chronic infection involving cutaneous, subcutaneous and lymphatic tissue Skin: Follows minor trauma Nodule ulcer necrosis Skin/subcutaneous tissue lymphatic channels lymph nodes Systemic dissemination: bones, joints, meninges Primary pulmonary: chronic alcoholics


15 Lymphocutaneous sporotrichosis showing more advanced, ulcerating lesions developing along the lymph system of the forearm
16 Sporotrichosis-Treatment Cutaneous : Potassium iodide, local heat therapy Disseminated : Amphotericin B, Itraconazole *Spontaneous healing is possible *Treatment should be continued for 2-4 weeks after all lesions have resolved, usually for a total of 3-6 months

17 superficial Mycoses Dermatophytosis (Tinea = Ringworm) & Pityriasis versicolor Fungal infections in human Sub-cutaneous Mycoses Sporotrichosis Systemic Mycoses Candidiasis Penicilliosis Histoplasmosis Cryptococcosis Aspergillosis Zygomycosis
18 Candida sp Normal flora in the GIT & GUT of humans > invade & cause disease when flora imbalances occur The host immune response = important determinant of Candida infection manifestation Manifestation vary from minimal fever fullblown sepsis syndrome Candida in a blood culture should always prompt a search for the source & it is not a contaminant

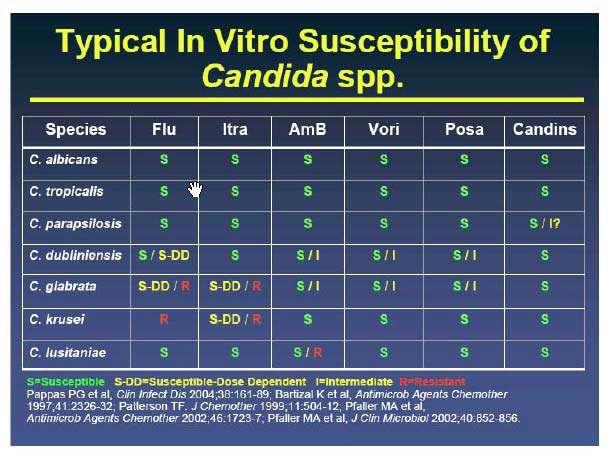
19 Albican vs non-albicans *All C. krusei are fluconazole-resistant *A variable proportion of C. glabrata are fluconazole-resistant C. albicans *C. krusei C. tropicalis Most commonly isolated Candida sp *C. glabrata C. parapsilosis
,")
 C.")
20 C. albicans (green colonies), C. tropicalis (bluish-purple colonies), C. krusei (filamentous, large pink colonies) C. glabrata (pink yeast colonies)
21 C. krusei 1. Intrinsically resistant to fluconazole 2. Resistance cannot be overcome with use of higher drug doses 3. Decreased susceptibility to ampho B requires higher doses (1 mg/kg/day)
22 C. glabrata 1. Many isolates are resistant to the azoles & cross-resistance among the azoles is common 2. MICs for voriconazole are highest with C. glabrata. 3. Resistance may be overcome by higher doses of fluconazole 4. Isolates that are resistant to fluconazole are generally resistant to voriconazole, as well 5. The echinocandins have generally retained excellent activity 6. Higher doses of ampho B are recommended (1 mg/kg/day)
23 C. parapsilosis 1. Highly susceptible to most antifungal agents 2. MIC for all the echinocandins are higher than for other Candida species 3. The clinical implications of these in vitro data are unclear
24 C. parapsilosis Five trials of caspofungin use in patients with invasive candidiasis, the overall (clinical and microbiologic) success rate among patients with C. parapsilosis (74% ) was similar to patients with invasive candidiasis caused by other Candida species
25 Weird Candida s C. lusitaniae often resistant to or quickly becomes resistant to amp B; however, it is usually susceptible to the azoles and echinocandins C. guilliermondii more often in hematologic malignancies. Some isolates have reduced susceptibility to fluconazole and many have reduced susceptibility to echinocandins However, C. guilliermondii is usually susceptible to amp B.
26 Candidemia is a broad topic Candidemia Organ involvement Some trial data Mostly anecdotal Catheterrelated candidemia Acute disseminated candidiasis Chronic disseminated candidiasis Deep organ candidiasis
27 Risk Factors For Candidemia Immunosupressed pt hematologic malignancies solid organ or stem cell transplants recipients Pt on chemotherapeutic agents, especially if associated with extensive GIT mucosal damage In ICU CVC TPN Broad-spectrum antibiotics High APACHE scores Acute renal failure, particularly if requiring HD Abdominal surgery GIT perforations and anastomotic leaks
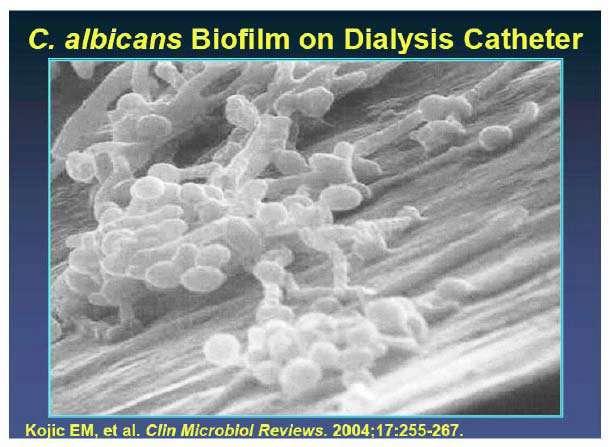
28 Through the GIT mucosal barrier Pathogenesis of Candidemia Via intravascular catheter From a localized focus of infection *Colonization with Candida sp is an independent predictor of candidemia



29 Oral Thrush Tiny pustular lesions Endogenous Candida endophthalmitis Splenic microabscesses
30
31

32 Why Echinocandins over Azoles as Primary Therapy?
33 ECHINOCANDIN EFFECT 1. Excellent broad spectrum antifungal activity Cidal for majority of Candida spp.) 2. Safe & Easy to use (low AEs) 3. Low drug-drug interactions
34 Candidemia in immunocompetent patients The echinocandins appear to be as effective as and better tolerated than amphotericin B Comparison of caspofungin and amphotericin B for invasive candidiasis. N Engl J Med 2002; 347:2020.
35 Candidemia in immunocompetent patients 1. The echinocandins appear to be as effective as and better tolerated than amphotericin B 2. Several randomized trials have shown that fluconazole & voriconazole is as effective as amphotericin B 3. Nephrotoxicity was significantly less with fluconazole
36 Combination therapy 1. Has not been established & not generally given 2. A controlled trial randomly assigned 219 nonneutropenic patients with candidemia to fluconazole (800 mg/day) alone for two weeks or fluconazole (800 mg/day) plus amp B (0.7 mg/kg per day) for the first four to seven days followed by fluconazole alone to finish the two week course more rapid clearing of fungemia with initial combination therapy, but success rates were similar in the two groups
37 Persistent Fungemia Median time to negative BC after start drug 2.6 d with catheter exchange, 5.6 d without Fungemia that persists longer: Dirty line, endocarditis, septic phlebitis Dirty lines: breakthru infections of susceptible bugs! Persistent neutropenia
38 To remove lines or not? A) This ID pandai pandai ask to remove lines, not easy to put new one, very hard to find lines ok! Ask him to insert a new one then only he knows. B)What s the big deal anyway? Just leave the lines alone. He is on antifungal therapy anyway! C) Insert a new one at same site - can or not? D) I put Daktarin cream at insertion site, sure ok one!
39 Higher mortality if catheters remain The removal of all compromised vascular lines is independently correlated with decreased early and late mortality
40 No benefit if catheters removed Early removal of central venous catheter in patients with candidemia does not improve outcome: analysis of 842 patients from 2 randomized clinical trials. Clin Infect Dis. 2010;51(3):295.
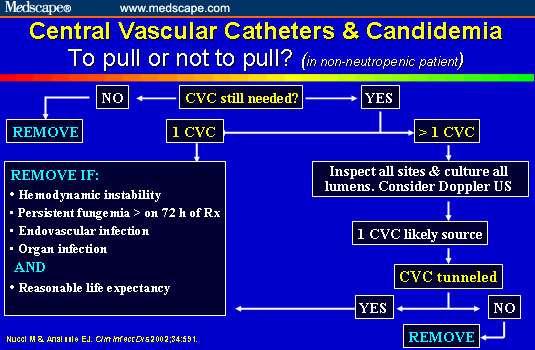
41 No benefit if catheters removed Some authorities have suggested that catheter removal may not be necessary in neutropenic patients with candidemia in whom the source is often the gastrointestinal tract rather than the central venous catheter Should vascular catheters be removed from all patients with candidemia? An evidence-based review. Clin Infect Dis 2002; 34:591. Early removal of central venous catheter in patients with candidemia does not improve outcome: analysis of 842 patients from 2 randomized clinical trials. Clin Infect Dis 2010; 51:295.
42 % Candidemic Catheters & Candidemia Non-neutropenic #1 source! All new by day 0 No change by d0 Cancer patients Tunneled lines are less often sources The gut is probably a frequent source in neutropenic patients with mucositis Day of Last +BC Start Rx
43 Catheter removal Despite the controversy, the current consensus, including IDSA guidelines, remains that in most patients with candidemia, intravascular catheters should be removed, realizing that in some patients this may not be feasible
44
45 Now you want me to remove the line or
46 Suggested indications for removal of tunnelled catheters Severe hypotension, shock, absence of clinical improvement after 72 h of therapy, endocarditis, septic thrombophlebitis or cellulitis
47
48 Ophthalmology Referral: Why? A)If eye involved, that need intravitreous treatment B)She is already on antifungal treatment. No Need!It wont change management!!! C) Refer cause maybe change type of antifungal D) Cause I don t like the ophthalmology MO s attitude give him some work!! E) Refer cause maybe prolong duration of treatment
49 Ophthalmology Referral? The frequency of endophthalmitis is relatively low (3 5% of all candidemic patients)
50 The reason is It requires prolonged antifungal therapy. Failure to perform this examination can result in disseminated disease and subsequent relapse. Retinal lesions as clues to disseminated bacterial and candidal infections: frequency, natural history, and etiology. Medicine (Baltimore) 2003; 82:
51 When should I suspect Candida Endophthalmitis? The onset of symptoms may occur subacutely, days to several weeks after fungemia.
52 Candida Endophthalmitis The eye infection is often clinically silent at first Initially, may be associated with minimal eye pain, and vision decrease may be subtle until the infection is advanced Treatment outcomes in a 10-year study of endogenous fungal endophthalmitis. Ophthalmic Surg Lasers 1997; 28:185.

53 Multiple chorioretinal lesions
54 Candida Endophthalmitis Endophthalmitis: 0% to 6% ; Chorioretinitis: 2% to 26%, Characteristic findings: "cotton ball" or "string of pearls" opacities High risk for blindness Perform at a time when the candidemia appears to be controlled Neutropnia patients risk highest when neutropenia improve
55 Candida Endophthalmitis Favorable outcome if treatment is administered before the onset of retinal complications Recommended treatment vitrectomy, intravitreal and systemic antifungal therapy. Recommended systemic therapy: AmB-d + flucytosine for advanced lesions/macula fluconazole can be used for less severe infections Recommended duration of tx: 4 to 6 weeks.
56 Candida Endophthalmitis Echinocandins and Amp B have limited vitreal penetration Best drug : Fluconazole,Voriconazole,Flucytosine in terms of penetration

57 *All C. krusei are fluconazole-resistant *A variable proportion of C. glabrata are fluconazole-resistant
58 Dose and duration of therapy - not too much, not too little Data from trials on duration Generally for 14 days after last culture negative Relapse/complication rate ~1% Doses Fluco: at least 6 mg/kg. 12 mg/kg being studied and may be better for C. glabrata Ampho: at least 0.5 mg/kg. More for glabrata? Lipid ampho: ~3 mg/kg seems comparable to mg/kg for Candida Walsh et al. AAC 41:1944, 1997; Linden et al. Pharmacotherapy 19:1261, 1999
59 Candidiemia treatment (IDSA) 1. All intravenous catheters should be removed and replaced 2. Daily or EOD cultures after starting treatment 3. Duration of therapy Minimum 2 weeks after blood c&s becomes negative
60 Oral step-down therapy Susceptible to fluconazole who are clinically stable can be switched from an echinocandin to fluconazole Voriconazole is recommended as oral stepdown therapy only for patients with C. krusei or voriconazole-susceptible C. glabrata.
61 When to consider empirical antifungal? Not debated in cancer, fever, & neutropenia. BUT, what about ICU, fever, and leukocytosis?
62 Empirical antifungal.. In the febrile non-neutropenic patient? Early treatment is theoretically attractive IDSA Guidelines Appropriate use has not been defined My approach & suggestions: Antibiotics, lines, no other source, and Colonized somewhere with Candida - I don t distinguish sites: anywhere works for me More sites/fungus = more risk (Pittet, Ann Surg 220:751, 1994)



63 Candidemia empiric choice Prior Azole prophylaxis Prior colonisation with glabrata/krusei Hemodynamically unstable Amphotericin B Caspofungin For others: Fluconazole 800mg loading dose followed by 400mg od
64 Candiduria So, tell me, just exactly why did you order this urine culture?
65 Thinking About Candiduria.. In the symptomatic or febrile patient Treat symptomatic UTI (of course!) View as a risk factor for dissemination in the febrile and critically-ill patient In the asymptomatic patient Approach as you would for bacteruria Correct anatomic factors remove CBD Treatment is probably irrelevant This is idea is now supported by data...
66 A very instructive study! Sobel et al., CID 30:19-24, 2000 Asymptomatic candiduria (no fever, no sx) Fluco (200/d, N = 159) vs. placebo (N = 157) x 14d Fluco cleared urine in 50%, placebo in 29% Continuous cath reduced efficacy: 63% vs. 39% 50% C. albicans, mix of others. C. tropicalis was most difficult to clear. Funguria two weeks later: Same cure rate in both groups! (60% with cath, 70% without cath)

67
ANTIMYCOTIC DRUGS Modes of Action
 ANTIMYCOTIC DRUGS Modes of Action Prapasarakul Nuvee, D.V.M., Ph.D. Department of Veterinary Microbiology, Faculty of Veterinary Science, Chulalongkorn University 1 What drugs act as antifungal agents?
ANTIMYCOTIC DRUGS Modes of Action Prapasarakul Nuvee, D.V.M., Ph.D. Department of Veterinary Microbiology, Faculty of Veterinary Science, Chulalongkorn University 1 What drugs act as antifungal agents?
Antifungal drugs Dr. Raz Muhammed
 Antifungal drugs 13. 12. 2018 Dr. Raz Muhammed 2. Flucytosine (5-FC) Is fungistatic Is a synthetic pyrimidine antimetabolite Is often used in combination with amphotericin B in the treatment of systemic
Antifungal drugs 13. 12. 2018 Dr. Raz Muhammed 2. Flucytosine (5-FC) Is fungistatic Is a synthetic pyrimidine antimetabolite Is often used in combination with amphotericin B in the treatment of systemic
Management of fungal infection
 Management of fungal infection HKDU symposium 17 th May 2015 Speaker: Dr. Thomas Chan MBBS (Hons), MRCP, FHKCP, FHKAM Synopsis Infection caused by fungus mycoses Skin infection by fungus is common in general
Management of fungal infection HKDU symposium 17 th May 2015 Speaker: Dr. Thomas Chan MBBS (Hons), MRCP, FHKCP, FHKAM Synopsis Infection caused by fungus mycoses Skin infection by fungus is common in general
An Update in the Management of Candidiasis
 An Update in the Management of Candidiasis Daniel B. Chastain, Pharm.D., AAHIVP Infectious Diseases Pharmacy Specialist Phoebe Putney Memorial Hospital Adjunct Clinical Assistant Professor UGA College
An Update in the Management of Candidiasis Daniel B. Chastain, Pharm.D., AAHIVP Infectious Diseases Pharmacy Specialist Phoebe Putney Memorial Hospital Adjunct Clinical Assistant Professor UGA College
Common Fungi. Catherine Diamond MD MPH
 Common Fungi Catherine Diamond MD MPH Birth Month and Day & Last Four Digits of Your Cell Phone # BEFORE: http://tinyurl.com/kvfy3ts AFTER: http://tinyurl.com/lc4dzwr Clinically Common Fungi Yeast Mold
Common Fungi Catherine Diamond MD MPH Birth Month and Day & Last Four Digits of Your Cell Phone # BEFORE: http://tinyurl.com/kvfy3ts AFTER: http://tinyurl.com/lc4dzwr Clinically Common Fungi Yeast Mold
Antifungal Update. Candida: In Vitro Antifungal Susceptibility Testing
 Antifungal Update B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy School of Pharmacy University of California San Francisco The patient spikes a new fever and 3/3 blood
Antifungal Update B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy School of Pharmacy University of California San Francisco The patient spikes a new fever and 3/3 blood
Antifungal Update 2/22/12. Which is the most appropriate initial empirical therapy in a candidemic patient?
 Antifungal Update B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy School of Pharmacy University of California San Francisco 3/3 blood cultures are positive for an unidentified
Antifungal Update B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy School of Pharmacy University of California San Francisco 3/3 blood cultures are positive for an unidentified
About the Editor Gerri S. Hall, Ph.D.
 About the Editor Gerri S. Hall, Ph.D. Dr. Hall s professional career has been focused on clinical microbiology: direct clinical activities of various areas such as bacteriology, mycobacteria, STD testing,
About the Editor Gerri S. Hall, Ph.D. Dr. Hall s professional career has been focused on clinical microbiology: direct clinical activities of various areas such as bacteriology, mycobacteria, STD testing,
Fungi are eukaryotic With rigid cell walls composed largely of chitin rather than peptidoglycan (a characteristic component of most bacterial cell
 Antifungal Drugs Fungal infections (Mycoses) Often chronic in nature. Mycotic infections may be superficial and involve only the skin (cutaneous mycoses extending into the epidermis) Others may penetrate
Antifungal Drugs Fungal infections (Mycoses) Often chronic in nature. Mycotic infections may be superficial and involve only the skin (cutaneous mycoses extending into the epidermis) Others may penetrate
Fungal infections in ICU. Tang Swee Fong Department of Paediatrics Universiti Kebangsaan Malaysia
 Fungal infections in ICU Tang Swee Fong Department of Paediatrics Universiti Kebangsaan Malaysia Epidemiology of invasive fungal infections - US +300% Martin GS, et al. N Engl J Med 2003;348:1546-1554
Fungal infections in ICU Tang Swee Fong Department of Paediatrics Universiti Kebangsaan Malaysia Epidemiology of invasive fungal infections - US +300% Martin GS, et al. N Engl J Med 2003;348:1546-1554
Antifungal Stewardship. Önder Ergönül, MD, MPH Koç University, School of Medicine, Istanbul 6 October 2017, ESGAP course, Istanbul
 Antifungal Stewardship Önder Ergönül, MD, MPH Koç University, School of Medicine, Istanbul 6 October 2017, ESGAP course, Istanbul 1 2 Objectives What do we know? Invasive Candida and Aspergillosis Impact
Antifungal Stewardship Önder Ergönül, MD, MPH Koç University, School of Medicine, Istanbul 6 October 2017, ESGAP course, Istanbul 1 2 Objectives What do we know? Invasive Candida and Aspergillosis Impact
Antifungals and current treatment guidelines in pediatrics and neonatology
 Dragana Janic Antifungals and current treatment guidelines in pediatrics and neonatology Dragana Janic. University Children`s Hospital, Belgrade, Serbia 10/10/17 Hotel Crowne Plaza, Belgrade, Serbia; www.dtfd.org
Dragana Janic Antifungals and current treatment guidelines in pediatrics and neonatology Dragana Janic. University Children`s Hospital, Belgrade, Serbia 10/10/17 Hotel Crowne Plaza, Belgrade, Serbia; www.dtfd.org
Fungal Infection in the ICU: Current Controversies
 Fungal Infection in the ICU: Current Controversies Andrew F. Shorr, MD, MPH, FCCP, FACP Washington Hospital Center Georgetown University, Washington, DC Disclosures I have served as a consultant to, researcher/investigator
Fungal Infection in the ICU: Current Controversies Andrew F. Shorr, MD, MPH, FCCP, FACP Washington Hospital Center Georgetown University, Washington, DC Disclosures I have served as a consultant to, researcher/investigator
ADEQUATE ANTIFUNGAL USE FOR BLOODSTREAM INFECTIONS
 ADEQUATE ANTIFUNGAL USE FOR BLOODSTREAM INFECTIONS COMMERCIAL RELATIONS DISCLOSURE 2500 9000 15000 Astellas Gilead Sciences Pfizer Inc Expert advice Speaker s bureau Speaker s bureau OUTLINE OF THE PRESENTATION
ADEQUATE ANTIFUNGAL USE FOR BLOODSTREAM INFECTIONS COMMERCIAL RELATIONS DISCLOSURE 2500 9000 15000 Astellas Gilead Sciences Pfizer Inc Expert advice Speaker s bureau Speaker s bureau OUTLINE OF THE PRESENTATION
Antifungal Update 2/24/11. Which is the most appropriate initial empirical therapy in a candidemic patient?
 Antifungal Update B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy School of Pharmacy University of California San Francisco The patient spikes a new fever and 3/3 blood
Antifungal Update B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy School of Pharmacy University of California San Francisco The patient spikes a new fever and 3/3 blood
Current options of antifungal therapy in invasive candidiasis
 Current options of antifungal therapy in invasive candidiasis Saloua Ladeb Bone Marrow Transplant Center Tunis HAMMAMET 24 th April 2012 DEFINITION One or more positive results on blood culture for Candida
Current options of antifungal therapy in invasive candidiasis Saloua Ladeb Bone Marrow Transplant Center Tunis HAMMAMET 24 th April 2012 DEFINITION One or more positive results on blood culture for Candida
Antifungals in Invasive Fungal Infections: Antifungals in neutropenic patients
 BVIKM-SBIMC La Hulpe, 6 November 2008 Antifungals in Invasive Fungal Infections: Antifungals in neutropenic patients Johan Maertens, MD Acute Leukemia and SCT Unit University Hospital Gasthuisberg Catholic
BVIKM-SBIMC La Hulpe, 6 November 2008 Antifungals in Invasive Fungal Infections: Antifungals in neutropenic patients Johan Maertens, MD Acute Leukemia and SCT Unit University Hospital Gasthuisberg Catholic
Antifungal Agents. Polyenes Azoles Allyl and Benzyl Amines Other antifungals
 OPTO 6434 General Pharmacology Antifungal Agents Dr. Alison McDermott Room 254 HBSB, Phone 713-743 1974 Email amcdermott@optometry.uh.edu Fall 2015 Reading: Chapter 50 Brody s Human Pharmacology by Wecker
OPTO 6434 General Pharmacology Antifungal Agents Dr. Alison McDermott Room 254 HBSB, Phone 713-743 1974 Email amcdermott@optometry.uh.edu Fall 2015 Reading: Chapter 50 Brody s Human Pharmacology by Wecker
MANAGEMENT OF HOSPITAL-ACQUIRED FUNGAL INFECTIONS
 MANAGEMENT OF HOSPITAL-ACQUIRED FUNGAL INFECTIONS Paul D. Holtom, MD Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine Numbers of Cases of Sepsis in the United States, According
MANAGEMENT OF HOSPITAL-ACQUIRED FUNGAL INFECTIONS Paul D. Holtom, MD Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine Numbers of Cases of Sepsis in the United States, According
Use of Antifungal Drugs in the Year 2006"
 Use of Antifungal Drugs in the Year 2006" Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine
Use of Antifungal Drugs in the Year 2006" Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine
Condition First line Alternative Comments Candidemia Nonneutropenic adults
 Recommendations for the treatment of candidiasis. Clinical Practice Guidelines for the Management of Candidiasis: 2009 Update by the Infectious Diseases Society of America. Condition First line Alternative
Recommendations for the treatment of candidiasis. Clinical Practice Guidelines for the Management of Candidiasis: 2009 Update by the Infectious Diseases Society of America. Condition First line Alternative
Case Studies in Fungal Infections and Antifungal Therapy
 Case Studies in Fungal Infections and Antifungal Therapy Wayne L. Gold MD, FRCPC Annual Meeting of the Canadian Society of Internal Medicine November 4, 2017 Disclosures No financial disclosures or industry
Case Studies in Fungal Infections and Antifungal Therapy Wayne L. Gold MD, FRCPC Annual Meeting of the Canadian Society of Internal Medicine November 4, 2017 Disclosures No financial disclosures or industry
Antifungal resistance mechanisms in pathogenic fungi
 Antifungal resistance mechanisms in pathogenic fungi Shivaprakash M Rudramurthy Additional Professor, Mycology Division Center of Advanced Research in Medical Mycology, National Culture Collection of Pathogenic
Antifungal resistance mechanisms in pathogenic fungi Shivaprakash M Rudramurthy Additional Professor, Mycology Division Center of Advanced Research in Medical Mycology, National Culture Collection of Pathogenic
Improving Clinical Outcomes in Fungal Infection Control and Management
 Improving Clinical Outcomes in Fungal Infection Control and Management DISCLAIMER The information within this CME/CE activity is for continuing education purposes only, and is not intended to substitute
Improving Clinical Outcomes in Fungal Infection Control and Management DISCLAIMER The information within this CME/CE activity is for continuing education purposes only, and is not intended to substitute
Current Options in Antifungal Pharmacotherapy
 Current Options in Antifungal Pharmacotherapy John Mohr, Pharm.D., Melissa Johnson, Pharm.D., Travis Cooper, Pharm.D., James S. Lewis, II, Pharm.D., and Luis Ostrosky-Zeichner, M.D. Infections caused by
Current Options in Antifungal Pharmacotherapy John Mohr, Pharm.D., Melissa Johnson, Pharm.D., Travis Cooper, Pharm.D., James S. Lewis, II, Pharm.D., and Luis Ostrosky-Zeichner, M.D. Infections caused by
CURRENT AND NEWER ANTI-FUNGAL THERAPIES- MECHANISMS, INDICATIONS, LIMITATIONS AND PROBLEMS. Dr AMIT RAODEO DM SEMINAR
 CURRENT AND NEWER ANTI-FUNGAL THERAPIES- MECHANISMS, INDICATIONS, LIMITATIONS AND PROBLEMS Dr AMIT RAODEO DM SEMINAR Introduction The incidence of invasive fungal infections in critically ill intensive
CURRENT AND NEWER ANTI-FUNGAL THERAPIES- MECHANISMS, INDICATIONS, LIMITATIONS AND PROBLEMS Dr AMIT RAODEO DM SEMINAR Introduction The incidence of invasive fungal infections in critically ill intensive
Cigna Drug and Biologic Coverage Policy
 Cigna Drug and Biologic Coverage Policy Subject Voriconazole Effective Date... 3/15/2018 Next Review Date... 3/15/2019 Coverage Policy Number... 4004 Table of Contents Coverage Policy... 1 General Background...
Cigna Drug and Biologic Coverage Policy Subject Voriconazole Effective Date... 3/15/2018 Next Review Date... 3/15/2019 Coverage Policy Number... 4004 Table of Contents Coverage Policy... 1 General Background...
Objec&ves. Clinical Presenta&on
 Michelle A. Barron, MD Associate Professor of Medicine Division of Infectious Diseases University of Colorado Denver Objec&ves Determine who is at risk for invasive candidiasis. Understand whether prophylaxis
Michelle A. Barron, MD Associate Professor of Medicine Division of Infectious Diseases University of Colorado Denver Objec&ves Determine who is at risk for invasive candidiasis. Understand whether prophylaxis
Medical Mycology. Dr. Hala Al Daghistani
 Medical Mycology Dr. Hala Al Daghistani Mycotic Infections GENERAL CONCEPTS A. The fungi represent a diverse, heterogeneous group of eukaryotic B. Most of these organisms are plant pathogens and relatively
Medical Mycology Dr. Hala Al Daghistani Mycotic Infections GENERAL CONCEPTS A. The fungi represent a diverse, heterogeneous group of eukaryotic B. Most of these organisms are plant pathogens and relatively
Treatment of rare and emerging fungal infections. EFISG Educational Workshop 15 th ECCMID April 2, 2005, Copenhagen
 Treatment of rare and emerging fungal infections EFISG Educational Workshop 15 th ECCMID April 2, 2005, Copenhagen Helen Sambatakou Lecturer in Medicine and Infectious Diseases, University of Athens, Greece
Treatment of rare and emerging fungal infections EFISG Educational Workshop 15 th ECCMID April 2, 2005, Copenhagen Helen Sambatakou Lecturer in Medicine and Infectious Diseases, University of Athens, Greece
Antimycotics. November 14, Jan Strojil. Ústav farmakologie LF UP
 Ústav farmakologie LF UP November 14, 2005 Introduction Polyens Azoles Alylamines Other Outline Introduction Polyens Azoles Alylamines and morfolines Other Introduction Polyens Azoles Alylamines Other
Ústav farmakologie LF UP November 14, 2005 Introduction Polyens Azoles Alylamines Other Outline Introduction Polyens Azoles Alylamines and morfolines Other Introduction Polyens Azoles Alylamines Other
Antifungal Resistance in Asia: Mechanisms, Epidemiology, and Consequences
 5th MMTN Conference 5-6 November 2016 Bangkok, Thailand 10:20-10:45, 6 Nov, 2016 Antifungal Resistance in Asia: Mechanisms, Epidemiology, and Consequences Yee-Chun Chen, M.D., PhD. Department of Medicine,
5th MMTN Conference 5-6 November 2016 Bangkok, Thailand 10:20-10:45, 6 Nov, 2016 Antifungal Resistance in Asia: Mechanisms, Epidemiology, and Consequences Yee-Chun Chen, M.D., PhD. Department of Medicine,
Current and Emerging Azole Antifungal Agents
 CLINICAL MICROBIOLOGY REVIEWS, Jan. 1999, p. 40 79 Vol. 12, No. 1 0893-8512/99/$04.00 0 Copyright 1999, American Society for Microbiology. All Rights Reserved. Current and Emerging Azole Antifungal Agents
CLINICAL MICROBIOLOGY REVIEWS, Jan. 1999, p. 40 79 Vol. 12, No. 1 0893-8512/99/$04.00 0 Copyright 1999, American Society for Microbiology. All Rights Reserved. Current and Emerging Azole Antifungal Agents
Title: Author: Speciality / Division: Directorate:
 Antifungal guidelines for CANDIDIASIS INFECTIONS (Adults) Proven infection: Targeted antifungal therapy should be prescribed for: o Positive cultures from a sterile site with clinical or radiological abnormality
Antifungal guidelines for CANDIDIASIS INFECTIONS (Adults) Proven infection: Targeted antifungal therapy should be prescribed for: o Positive cultures from a sterile site with clinical or radiological abnormality
Rheem Totah, Office H172M, Ph Office hours MWF 11:30 12:20 or by arrangement
 Rheem Totah, Office H172M, Ph 206-543-9481 rtotah@uw.edu Office hours MWF 11:30 12:20 or by arrangement Date/Time Topic Readings Mon March 26 Antifungal agents Foye s Chapter 40 Wed March 28 Antifungal
Rheem Totah, Office H172M, Ph 206-543-9481 rtotah@uw.edu Office hours MWF 11:30 12:20 or by arrangement Date/Time Topic Readings Mon March 26 Antifungal agents Foye s Chapter 40 Wed March 28 Antifungal
TOWARDS PRE-EMPTIVE? TRADITIONAL DIAGNOSIS. GALACTOMANNAN Sensitivity 61% Specificity 93% Neg Predict Value >95% β-d-glucan Neg Predict Value 100% PCR
 TOWARDS PRE-EMPTIVE? GALACTOMANNAN Sensitivity 61% Specificity 93% Neg Predict Value >95% TRADITIONAL DIAGNOSIS β-d-glucan Neg Predict Value 100% PCR diagnostics FUNGAL BURDEN FIRST TEST POSITIVE FOR ASPERGILLOSIS
TOWARDS PRE-EMPTIVE? GALACTOMANNAN Sensitivity 61% Specificity 93% Neg Predict Value >95% TRADITIONAL DIAGNOSIS β-d-glucan Neg Predict Value 100% PCR diagnostics FUNGAL BURDEN FIRST TEST POSITIVE FOR ASPERGILLOSIS
Course content. Chemotherapeutic agents
 Course content 1 Chemotherapeutic agents Mechanism of actions Indications Contraindications/Cautions Drug interactions Side-effects/Adverse reactions Dosage regimen (occasionally) Reference Books 2 Pharmacology
Course content 1 Chemotherapeutic agents Mechanism of actions Indications Contraindications/Cautions Drug interactions Side-effects/Adverse reactions Dosage regimen (occasionally) Reference Books 2 Pharmacology
Med Chem 401: Mycology (www.doctorfungus.org) Mycology
 Mycology") Med Chem 401: Mycology (www.doctorfungus.org) Mycology is the Study of Fungi (Monera, Protoctista, Fungi, Plantae, Animalia). Fungi are eukaryotic cells and as such contain nuclei, mitochondria, ER, golgi,
Med Chem 401: Mycology (www.doctorfungus.org) Mycology is the Study of Fungi (Monera, Protoctista, Fungi, Plantae, Animalia). Fungi are eukaryotic cells and as such contain nuclei, mitochondria, ER, golgi,
Introduction. Study of fungi called mycology.
 Fungi Introduction Study of fungi called mycology. Some fungi are beneficial: ex a) Important in production of some foods, ex: cheeses, bread. b) Important in production of some antibiotics, ex: penicillin
Fungi Introduction Study of fungi called mycology. Some fungi are beneficial: ex a) Important in production of some foods, ex: cheeses, bread. b) Important in production of some antibiotics, ex: penicillin
Case. Fungal infections for the community provider. Case. Case. April 25, 2014 Peter V. Chin-Hong M.D. Infectious Diseases UCSF UCSF
 Case Fungal infections for the community provider April 25, 2014 Peter V. Chin-Hong M.D. Infectious Diseases UCSF peter.chin-hong@ucsf.edu UCSF A 38-year-old African-American female financial analyst is
Case Fungal infections for the community provider April 25, 2014 Peter V. Chin-Hong M.D. Infectious Diseases UCSF peter.chin-hong@ucsf.edu UCSF A 38-year-old African-American female financial analyst is
Dr Kaniz Fatema. FCPS (Medicine), MD (Critical Care Medicine) Associate Professor Dept of Critical Care Medicine BIRDEM General Hospital
, MD (Critical Care Medicine) Associate Professor Dept of Critical Care Medicine BIRDEM General Hospital") Dr Kaniz Fatema FCPS (Medicine), MD (Critical Care Medicine) Associate Professor Dept of Critical Care Medicine BIRDEM General Hospital 65-years old lady HTN (15 yrs) Adult Still s Disease (2 mon)
Dr Kaniz Fatema FCPS (Medicine), MD (Critical Care Medicine) Associate Professor Dept of Critical Care Medicine BIRDEM General Hospital 65-years old lady HTN (15 yrs) Adult Still s Disease (2 mon)
Fungal infection in the immunocompromised patient. Dr Kirsty Dodgson
 Fungal infection in the immunocompromised patient Dr Kirsty Dodgson Aims Discuss different types of fungi Overview of types of clinical infections Clinical Manifestations Fungus Includes Moulds Aspergillus
Fungal infection in the immunocompromised patient Dr Kirsty Dodgson Aims Discuss different types of fungi Overview of types of clinical infections Clinical Manifestations Fungus Includes Moulds Aspergillus
Fungal update. Liise-anne Pirofski, M.D. Albert Einstein College of Medicine
 Liise-anne Pirofski, M.D. Albert Einstein College of Medicine Fungal update http://clicks.robertgenn.com/miss-potter.php http://letterfromhere.blogspot.com/2007/06/beatrix-potters-jog-trot-through.html
Liise-anne Pirofski, M.D. Albert Einstein College of Medicine Fungal update http://clicks.robertgenn.com/miss-potter.php http://letterfromhere.blogspot.com/2007/06/beatrix-potters-jog-trot-through.html
Fungi GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER NUMBER 53: Author Moi Lin Ling, MBBS, FRCPA, CPHQ, MBA
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER NUMBER 53: Fungi Author Moi Lin Ling, MBBS, FRCPA, CPHQ, MBA Chapter Editor Ziad A. Memish, MD, FRCPC, FACP Cover heading - Topic Outline Topic outline
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER NUMBER 53: Fungi Author Moi Lin Ling, MBBS, FRCPA, CPHQ, MBA Chapter Editor Ziad A. Memish, MD, FRCPC, FACP Cover heading - Topic Outline Topic outline
Use of Antifungals in the Year 2008
 Use of Antifungals in the Year 2008 Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine Diagnosis
Use of Antifungals in the Year 2008 Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine Diagnosis
Micafungin, a new Echinocandin: Pediatric Development
 Micafungin, a new Echinocandin: Pediatric Development Andreas H. Groll, M.D. Infectious Disease Research Program Center for Bone Marrow Transplantation and Department of Pediatric Hematology/Oncology University
Micafungin, a new Echinocandin: Pediatric Development Andreas H. Groll, M.D. Infectious Disease Research Program Center for Bone Marrow Transplantation and Department of Pediatric Hematology/Oncology University
Ali Alabbadi. Sarah Jaar ... Nader
 24 Ali Alabbadi Sarah Jaar... Nader Intro to Mycology *underlined text was explained in the lecture but is not found in the slides -mycology: the study of the mycoses of man (fungal infections) -less than
24 Ali Alabbadi Sarah Jaar... Nader Intro to Mycology *underlined text was explained in the lecture but is not found in the slides -mycology: the study of the mycoses of man (fungal infections) -less than
Medical Mycology. Dr. Hala Al Daghistani
 Medical Mycology Dr. Hala Al Daghistani FAre eukaryotes that grow in two basic forms, a yeasts and molds (or moulds). Growth in the mold form occurs by production of multicellular filamentous colonies.
Medical Mycology Dr. Hala Al Daghistani FAre eukaryotes that grow in two basic forms, a yeasts and molds (or moulds). Growth in the mold form occurs by production of multicellular filamentous colonies.
Updated Guidelines for Management of Candidiasis. Vidya Sankar, DMD, MHS April 6, 2017
 Updated Guidelines for Management of Candidiasis Vidya Sankar, DMD, MHS April 6, 2017 Statement of Disclosure I have no actual or potential conflict of interest in relation to this presentation Outline
Updated Guidelines for Management of Candidiasis Vidya Sankar, DMD, MHS April 6, 2017 Statement of Disclosure I have no actual or potential conflict of interest in relation to this presentation Outline
SUSCEPTIBILITY PROFILE OF EMERGING FUNGAL PATHOGENS
 SUSCEPTIBILITY PROFILE OF EMERGING FUNGAL PATHOGENS Professor Lia Monica JUNIE, Department of Microbiology, University of Medicine and Pharmacy, Cluj Napoca, Romania The most common fungal pathogens are:
SUSCEPTIBILITY PROFILE OF EMERGING FUNGAL PATHOGENS Professor Lia Monica JUNIE, Department of Microbiology, University of Medicine and Pharmacy, Cluj Napoca, Romania The most common fungal pathogens are:
Pathogens with Intermediate Virulence Dermatophytes opportunistic Pathogens
 Pathogens with Intermediate Virulence Dermatophytes opportunistic Pathogens Cryptococcus neoformans Candida albicans Aspergillus species Pneumocystis carinii 1 Dermatophytes Named for derma skin Cause
Pathogens with Intermediate Virulence Dermatophytes opportunistic Pathogens Cryptococcus neoformans Candida albicans Aspergillus species Pneumocystis carinii 1 Dermatophytes Named for derma skin Cause
NEW ANTI-INFECTIVE AGENTS IN 2003 : SPECTRUM AND INDICATIONS. 20th Symposium (spring 2003) Thursday May 22nd 2003
 Thursday May 22nd 2003") NEW ANTI-INFECTIVE AGENTS IN 2003 : SPECTRUM AND INDICATINS 20th Symposium (spring 2003) Thursday May 22nd 2003 The slides presented at this meeting are available on this site as "Web slide shows" and
NEW ANTI-INFECTIVE AGENTS IN 2003 : SPECTRUM AND INDICATINS 20th Symposium (spring 2003) Thursday May 22nd 2003 The slides presented at this meeting are available on this site as "Web slide shows" and
Voriconazole October 2015 Risk Management Plan. Voriconazole
 Voriconazole October 2015 VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Invasive aspergillosis (IA) is the most devastating of Aspergillus related diseases, targeting severely
Voriconazole October 2015 VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Invasive aspergillosis (IA) is the most devastating of Aspergillus related diseases, targeting severely
How Can We Prevent Invasive Fungal Disease?
 How Can We Prevent Invasive Fungal Disease? Chris Kibbler Professor of Medical Microbiology University College London And Royal Free Hospital, London, UK Invasive Aspergillosis 2 - Acquisition Preventive
How Can We Prevent Invasive Fungal Disease? Chris Kibbler Professor of Medical Microbiology University College London And Royal Free Hospital, London, UK Invasive Aspergillosis 2 - Acquisition Preventive
WHAT IS THE ROLE OF EMPIRIC TREATMENT FOR SUSPECTED INVASIVE CANDIDIASIS IN NONNEUTROPENIC PATIENTS IN THE ICU?
 WHAT IS THE ROLE OF EMPIRIC TREATMENT FOR SUSPECTED INVASIVE CANDIDIASIS IN NONNEUTROPENIC PATIENTS IN THE ICU? Empiric antifungal therapy should be considered in critically ill patients with risk factors
WHAT IS THE ROLE OF EMPIRIC TREATMENT FOR SUSPECTED INVASIVE CANDIDIASIS IN NONNEUTROPENIC PATIENTS IN THE ICU? Empiric antifungal therapy should be considered in critically ill patients with risk factors
1. Pre-emptive therapy. colonization, colonization, pre-emptive therapy. , ICU colonization. colonization. 2, C. albicans
 Jpn. J. Med. Mycol. Vol. 45, 217 221, 2004 ISSN 0916 4804,.,, colonization, pre-emptive therapy. 2, non-albicans Candida., fluconazole.,. Key words: postoperative infection, non-albicans Candida, pre-emptive
Jpn. J. Med. Mycol. Vol. 45, 217 221, 2004 ISSN 0916 4804,.,, colonization, pre-emptive therapy. 2, non-albicans Candida., fluconazole.,. Key words: postoperative infection, non-albicans Candida, pre-emptive
Fungi. Eucaryotic Rigid cell wall(chitin, glucan) Cell membrane ergosterol Unicellular, multicellular Classic fungus taxonomy:
 Cell membrane ergosterol Unicellular, multicellular Classic fungus taxonomy:") MYCOLOGY Mycology I Fungi Eucaryotic Rigid cell wall(chitin, glucan) Cell membrane ergosterol Unicellular, multicellular Classic fungus taxonomy: Morphology Spore formation FFungi Yeast Mold Yeastlike
MYCOLOGY Mycology I Fungi Eucaryotic Rigid cell wall(chitin, glucan) Cell membrane ergosterol Unicellular, multicellular Classic fungus taxonomy: Morphology Spore formation FFungi Yeast Mold Yeastlike
C. albicans C. tropicalis C. parapsilosis C. kefyr C. glabrata C. krusei C. guillermondii C. lusitaniae THERAPY USING ANTIFUNGALS AND ANTIVIRALS
 THERAPY USING ANTIFUNGALS AND ANTIVIRALS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu CLASSIFICATION OF FUNGI Yeasts Candida Cryptococcus
THERAPY USING ANTIFUNGALS AND ANTIVIRALS Douglas Black, Pharm.D. Associate Professor School of Pharmacy University of Washington dblack@u.washington.edu CLASSIFICATION OF FUNGI Yeasts Candida Cryptococcus
WHICH ANTIFUNGAL AGENT IS THE CHOICE FOR SUSPECTED FUNGAL INFECTIONS?
 WHICH ANTIFUNGAL AGENT IS THE CHOICE FOR SUSPECTED FUNGAL INFECTIONS? Assoc. Prof. Dr. Serkan SENER Acibadem University Medical School Department of Emergency Medicine, Istanbul Acibadem Ankara Hospital,
WHICH ANTIFUNGAL AGENT IS THE CHOICE FOR SUSPECTED FUNGAL INFECTIONS? Assoc. Prof. Dr. Serkan SENER Acibadem University Medical School Department of Emergency Medicine, Istanbul Acibadem Ankara Hospital,
Epidemiology and ecology of fungal diseases
 Epidemiology and ecology of fungal diseases Healthcare Focus on: - individual - diagnosis - treatment Public Health Focus on: - population - prevention The nature of fungi Kingdom Fungi (lat. fungus, -i)
Epidemiology and ecology of fungal diseases Healthcare Focus on: - individual - diagnosis - treatment Public Health Focus on: - population - prevention The nature of fungi Kingdom Fungi (lat. fungus, -i)
Pharmaceutical Chemistry II. Antifungal Agents. = Antimycotics. Tutorial 1
 Pharmaceutical Chemistry II Antifungal Agents = Antimycotics Tutorial 1 1) Give examples of some common fungal infections indicating whether they are rather superficial or systemic. Fungal infections Tinea
Pharmaceutical Chemistry II Antifungal Agents = Antimycotics Tutorial 1 1) Give examples of some common fungal infections indicating whether they are rather superficial or systemic. Fungal infections Tinea
Prophylaxis versus Diagnostics-driven approaches to treatment of Invasive fungal diseases. Y.L. Kwong Department of Medicine University of Hong Kong
 Prophylaxis versus Diagnostics-driven approaches to treatment of Invasive fungal diseases Y.L. Kwong Department of Medicine University of Hong Kong Pathogenic yeast Candida Cryptococcus Trichosporon Pathogenic
Prophylaxis versus Diagnostics-driven approaches to treatment of Invasive fungal diseases Y.L. Kwong Department of Medicine University of Hong Kong Pathogenic yeast Candida Cryptococcus Trichosporon Pathogenic
When is failure failure?
 When is failure failure? Bart-Jan Kullberg, M.D. Radboud University Nijmegen The Netherlands The ICU patient with candidemia!! Female, 39 years old!! Multiple abdominal surgeries for Crohn's disease!!
When is failure failure? Bart-Jan Kullberg, M.D. Radboud University Nijmegen The Netherlands The ICU patient with candidemia!! Female, 39 years old!! Multiple abdominal surgeries for Crohn's disease!!
Micafungin and Candida spp. Rationale for the EUCAST clinical breakpoints. Version February 2013
 Micafungin and Candida spp. Rationale for the EUCAST clinical breakpoints. Version 1.0 5 February 2013 Foreword EUCAST The European Committee on Antimicrobial Susceptibility Testing (EUCAST) is organised
Micafungin and Candida spp. Rationale for the EUCAST clinical breakpoints. Version 1.0 5 February 2013 Foreword EUCAST The European Committee on Antimicrobial Susceptibility Testing (EUCAST) is organised
Antifungal Pharmacotherapy
 Interpreting Antifungal Susceptibility Testing: Science or Smoke and Mirrors A. W. F O T H E R G I L L, M A, M B A U N I V E R S I T Y O F T E X A S H E A L T H S C I E N C E C E N T E R S A N A N T O
Interpreting Antifungal Susceptibility Testing: Science or Smoke and Mirrors A. W. F O T H E R G I L L, M A, M B A U N I V E R S I T Y O F T E X A S H E A L T H S C I E N C E C E N T E R S A N A N T O
PROGRESSI NELLA TERAPIA ANTIFUNGINA. A tribute to Piero Martino
 PROGRESSI NELLA TERAPIA ANTIFUNGINA A tribute to Piero Martino 1946-2007 ITALIAN ICONS IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI 1961 CAUSES OF DEATH IN PATIENTS WITH MALIGNANCIES
PROGRESSI NELLA TERAPIA ANTIFUNGINA A tribute to Piero Martino 1946-2007 ITALIAN ICONS IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI 1961 CAUSES OF DEATH IN PATIENTS WITH MALIGNANCIES
Candida auris: an Emerging Hospital Infection
 National Center for Emerging and Zoonotic Infectious Diseases Candida auris: an Emerging Hospital Infection Paige Armstrong MD MHS Epidemic Intelligence Service Officer Mycotic Diseases Branch Association
National Center for Emerging and Zoonotic Infectious Diseases Candida auris: an Emerging Hospital Infection Paige Armstrong MD MHS Epidemic Intelligence Service Officer Mycotic Diseases Branch Association
Introduction Medical Mycology. Prof. Dr. Asem Shehabi Faculty of Medicine University of Jordan
 Introduction Medical Mycology Prof. Dr. Asem Shehabi Faculty of Medicine University of Jordan General Fungi-1 Medical Mycology deals with fungi cause human diseases directly (mycoses, allergies) or indirectly
Introduction Medical Mycology Prof. Dr. Asem Shehabi Faculty of Medicine University of Jordan General Fungi-1 Medical Mycology deals with fungi cause human diseases directly (mycoses, allergies) or indirectly
Systemic Candidiasis for the clinicians: between guidelines and daily clinical practice
 Systemic Candidiasis for the clinicians: between guidelines and daily clinical practice Anastasia Antoniadou Assoc. Professor Internal Medicine and Infectious Diseases National and Kapodistrian University
Systemic Candidiasis for the clinicians: between guidelines and daily clinical practice Anastasia Antoniadou Assoc. Professor Internal Medicine and Infectious Diseases National and Kapodistrian University
Clinical Considerations in the Management of Systemic Fungal Infections. Conducted during the 41 st ASHP Midyear Clinical Meeting Anaheim, California
 Clinical Considerations in the Management of Systemic Fungal Infections Conducted during the 41 st ASHP Midyear Clinical Meeting Anaheim, California CONTINUING EDUCATION ACCREDITATION The American Society
Clinical Considerations in the Management of Systemic Fungal Infections Conducted during the 41 st ASHP Midyear Clinical Meeting Anaheim, California CONTINUING EDUCATION ACCREDITATION The American Society
Antifungal Pharmacodynamics A Strategy to Optimize Efficacy
 Antifungal Pharmacodynamics A Strategy to Optimize Efficacy David Andes, MD Associate Professor, Department of Medicine Division of Infectious Diseases Medical Microbiology and Immunology University of
Antifungal Pharmacodynamics A Strategy to Optimize Efficacy David Andes, MD Associate Professor, Department of Medicine Division of Infectious Diseases Medical Microbiology and Immunology University of
Biochemical Targets for Antifungal Chemotherapy
 Biochemical Targets for Antifungal Chemotherapy Fungal cells are complex organisms that share many biochemical targets with other eukaryotic cells. Therefore, agents that interact with fungal targets not
Biochemical Targets for Antifungal Chemotherapy Fungal cells are complex organisms that share many biochemical targets with other eukaryotic cells. Therefore, agents that interact with fungal targets not
Nursing college, Second stage Microbiology Dr.Nada Khazal K. Hendi Medical Microbiology
 1 Nursing college, Second stage Microbiology Medical Microbiology Lecture-1- Fungi (Mycosis) They are a diverse group of saprophytic and parasitic eukaryotic organisms. Human fungal diseases (mycoses)
1 Nursing college, Second stage Microbiology Medical Microbiology Lecture-1- Fungi (Mycosis) They are a diverse group of saprophytic and parasitic eukaryotic organisms. Human fungal diseases (mycoses)
ESCMID Online Lecture Library. by author
 What is the best antifungal strategy for severe intra-abdominal infections? Philippe Montravers MD, PhD Anaesthesia and Surgical ICU Bichat Claude Bernard Hospital Assistance Publique Hopitaux de Paris
What is the best antifungal strategy for severe intra-abdominal infections? Philippe Montravers MD, PhD Anaesthesia and Surgical ICU Bichat Claude Bernard Hospital Assistance Publique Hopitaux de Paris
(Notes on Anti-TB agents are included in the TB syllabus)
") (Notes on Anti-TB agents are included in the TB syllabus) Antifungal Agents A. Zuger MD General background: 1. Fungi are eukaryotes, with more cellular similarities to human cells than to bacterial cells.
(Notes on Anti-TB agents are included in the TB syllabus) Antifungal Agents A. Zuger MD General background: 1. Fungi are eukaryotes, with more cellular similarities to human cells than to bacterial cells.
Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America
 Clinical Infectious Diseases IDSA GUIDELINE Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America Peter G. Pappas, 1 Carol A. Kauffman,
Clinical Infectious Diseases IDSA GUIDELINE Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America Peter G. Pappas, 1 Carol A. Kauffman,
Nationwide survey of treatment for pediatric patients with invasive fungal infections in Japan
 J Infect Chemother (2013) 19:946 950 DOI 10.1007/s10156-013-0624-7 ORIGINAL ARTICLE Nationwide survey of treatment for pediatric patients with invasive fungal infections in Japan Masaaki Mori Received:
J Infect Chemother (2013) 19:946 950 DOI 10.1007/s10156-013-0624-7 ORIGINAL ARTICLE Nationwide survey of treatment for pediatric patients with invasive fungal infections in Japan Masaaki Mori Received:
ESCMID Online Lecture Library. by author
 How To Best Use Antifungal Agents Cornelia Lass-Flörl Division of Hygiene and Medical Microbiology Innsbruck Medical University ESCMID SUMMER SCHOOL 2012 Epidemiology Diagnosis Roadmap Antifungal drugs
How To Best Use Antifungal Agents Cornelia Lass-Flörl Division of Hygiene and Medical Microbiology Innsbruck Medical University ESCMID SUMMER SCHOOL 2012 Epidemiology Diagnosis Roadmap Antifungal drugs
Early Diagnosis and Therapy for Fungal Infections
 Early Diagnosis and Therapy for Fungal Infections Debra Goff PharmD, FCCP Clinical Associate Professor Infectious Disease Specialist The Ohio State University Medical Center Columbus Ohio, USA The Ohio
Early Diagnosis and Therapy for Fungal Infections Debra Goff PharmD, FCCP Clinical Associate Professor Infectious Disease Specialist The Ohio State University Medical Center Columbus Ohio, USA The Ohio
Invasive Fungal Infections in Critically Ill Patients. Dr Ravinder Kaur Director Professor&HOD Department of Microbiology,LHMC
 Invasive Fungal Infections in Critically Ill Patients Dr Ravinder Kaur Director Professor&HOD Department of Microbiology,LHMC Invasive fungal infections(ifis) Major causes of morbidity and mortality in
Invasive Fungal Infections in Critically Ill Patients Dr Ravinder Kaur Director Professor&HOD Department of Microbiology,LHMC Invasive fungal infections(ifis) Major causes of morbidity and mortality in
Fungal biology. Fungal Infections. Fungal cell structure. Pathogenesis
 Fungal Infections Once exotic and rare; now increasingly common Fungi are not virulent But they are good at taking advantage Opportunistic in many senses Fungal biology Eukaryotic (organized nucleus and
Fungal Infections Once exotic and rare; now increasingly common Fungi are not virulent But they are good at taking advantage Opportunistic in many senses Fungal biology Eukaryotic (organized nucleus and
Fungal Infections. Alessandro Diana November 22th 2007
 Fungal Infections Alessandro Diana November 22th 2007 alessandro.diana@ne.ch Topics Aspergillosis Candidiasis Cryptococcosis Histoplasmosis Coccidioidomycosis Blastomyocosis Sporotrichosis Pneumocystis
Fungal Infections Alessandro Diana November 22th 2007 alessandro.diana@ne.ch Topics Aspergillosis Candidiasis Cryptococcosis Histoplasmosis Coccidioidomycosis Blastomyocosis Sporotrichosis Pneumocystis
Fungal biology. Pathogenesis. Fungal cell structure. Fungal Infections MID 25 & 26. Eukaryotic (organized nucleus and cell structure) Non-motile
 Non-motile") Fungal Infections Once exotic and rare; now increasingly common Fungi are not virulent But they are good at taking advantage Opportunistic in many senses Fungal biology Eukaryotic (organized nucleus and
Fungal Infections Once exotic and rare; now increasingly common Fungi are not virulent But they are good at taking advantage Opportunistic in many senses Fungal biology Eukaryotic (organized nucleus and
Mycology. BioV 400. Clinical classification. Clinical classification. Fungi as Infectious Agents. Thermal dimorphism. Handout 6
 BioV 400 Mycology Handout 6 Fungi as Infectious Agents True or primary fungal pathogens invades and grows in a healthy, noncompromise d host Most striking adaptation to survival and growth in the human
BioV 400 Mycology Handout 6 Fungi as Infectious Agents True or primary fungal pathogens invades and grows in a healthy, noncompromise d host Most striking adaptation to survival and growth in the human
Antifungal Agents. Prof. Suheil Zmeili Faculty of Medicine Department of Pharmacology University of Jordan
 Antifungal Agents Prof. Suheil Zmeili Faculty of Medicine Department of Pharmacology University of Jordan Antifungal Agents Objectives: - Know Available antifungal drugs - Know their MOA - Know their Pharmacokinetic
Antifungal Agents Prof. Suheil Zmeili Faculty of Medicine Department of Pharmacology University of Jordan Antifungal Agents Objectives: - Know Available antifungal drugs - Know their MOA - Know their Pharmacokinetic
number Done by Corrected by Doctor د.حامد الزعبي
 number Fungi#1 Done by نرجس الس ماك Corrected by مهدي الشعراوي Doctor د.حامد الزعبي Introduction to Mycology -Terms: -Medical Mycology: The study of mycosis and their etiological agents -Mycosis: Disease
number Fungi#1 Done by نرجس الس ماك Corrected by مهدي الشعراوي Doctor د.حامد الزعبي Introduction to Mycology -Terms: -Medical Mycology: The study of mycosis and their etiological agents -Mycosis: Disease
Voriconazole. Voriconazole VRCZ ITCZ
 7 7 8 7 8 fluconazole itraconazole in vitro in vivo Candida spp. C. glabrata C. krusei Cryptococcus neoformans in vitro Aspergillus spp. in vitro in vivo Aspergillus fumigatus Candida albicans C. krusei
7 7 8 7 8 fluconazole itraconazole in vitro in vivo Candida spp. C. glabrata C. krusei Cryptococcus neoformans in vitro Aspergillus spp. in vitro in vivo Aspergillus fumigatus Candida albicans C. krusei
Primary Antifungal Prophylaxis in Adult Hematopoietic Stem Cell Transplant Recipients: Current Therapeutic Concepts
 Primary Antifungal Prophylaxis in Adult Hematopoietic Stem Cell Transplant Recipients: Current Therapeutic Concepts Dorothy McCoy, Pharm.D., Daryl D. DePestel, Pharm.D., and Peggy L. Carver, Pharm.D. In
Primary Antifungal Prophylaxis in Adult Hematopoietic Stem Cell Transplant Recipients: Current Therapeutic Concepts Dorothy McCoy, Pharm.D., Daryl D. DePestel, Pharm.D., and Peggy L. Carver, Pharm.D. In
The incidence of invasive fungal infections
 AN EPIDEMIOLOGIC UPDATE ON INVASIVE FUNGAL INFECTIONS * Michael A. Pfaller, MD ABSTRACT *Based on a presentation given by Dr Pfaller at a symposium held in conjunction with the 43rd Interscience Conference
AN EPIDEMIOLOGIC UPDATE ON INVASIVE FUNGAL INFECTIONS * Michael A. Pfaller, MD ABSTRACT *Based on a presentation given by Dr Pfaller at a symposium held in conjunction with the 43rd Interscience Conference
Clinical, Cellular, and Molecular Factors That Contribute to Antifungal Drug Resistance
 CLINICAL MICROBIOLOGY REVIEWS, Apr. 1998, p. 382 402 Vol. 11, No. 2 0893-8512/98/$04.00 0 Copyright 1998, American Society for Microbiology Clinical, Cellular, and Molecular Factors That Contribute to
CLINICAL MICROBIOLOGY REVIEWS, Apr. 1998, p. 382 402 Vol. 11, No. 2 0893-8512/98/$04.00 0 Copyright 1998, American Society for Microbiology Clinical, Cellular, and Molecular Factors That Contribute to
Antibiotics 301: Antifungal Agents
 Antibiotics 301: Antifungal Agents B. Joseph Guglielmo, Pharm.D. Professor and Dean School of Pharmacy University of California San Francisco Disclosures No potential conflicts of interest. 1 3/3 blood
Antibiotics 301: Antifungal Agents B. Joseph Guglielmo, Pharm.D. Professor and Dean School of Pharmacy University of California San Francisco Disclosures No potential conflicts of interest. 1 3/3 blood
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
Malaria prevention: source = The Sanford Guide to Antimicrobial Therapy. Gilbert et al.
 Malaria prevention: Agent Adult dose a Contraindications Application Notes Atovaquoneproguanil 250/100mg x1/day Insufficient data in pregnancy Prophylaxis for areas with CQ resistance, 2 expensive with
Malaria prevention: Agent Adult dose a Contraindications Application Notes Atovaquoneproguanil 250/100mg x1/day Insufficient data in pregnancy Prophylaxis for areas with CQ resistance, 2 expensive with
Correlation of culture with histopathology in fungal burn wound colonization and infection
 burns 33 (2007) 341 346 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/burns Correlation of culture with histopathology in fungal burn wound colonization and infection Christina
burns 33 (2007) 341 346 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/burns Correlation of culture with histopathology in fungal burn wound colonization and infection Christina
Update on Candida Infection Nov. 2010
 Update on Candida Infection Nov. 2010 Gary Wong Pharmacy Clinical site leader University Health Network Course coordinator University of Toronto Goals What is an yeast infection Risk factors for yeast
Update on Candida Infection Nov. 2010 Gary Wong Pharmacy Clinical site leader University Health Network Course coordinator University of Toronto Goals What is an yeast infection Risk factors for yeast
All three dermatophytes contain virulence factors that allow them to invade the skin, hair, and nails. Keratinases. Elastase.
 DERMATOPHYTOSIS (=Tinea = Ringworm) Infection of the skin, hair or nails caused by a group of keratinophilic fungi, called dermatophytes Microsporum Epidermophyton Hair, skin Skin, nail Tih Trichophyton
DERMATOPHYTOSIS (=Tinea = Ringworm) Infection of the skin, hair or nails caused by a group of keratinophilic fungi, called dermatophytes Microsporum Epidermophyton Hair, skin Skin, nail Tih Trichophyton
New triazoles and echinocandins: mode of action, in vitro activity and mechanisms of resistance
 For reprint orders, please contact reprints@expert-reviews.com New triazoles and echinocandins: mode of action, in vitro activity and mechanisms of resistance Expert Rev. Anti Infect. Ther. 7(8), 981 998
For reprint orders, please contact reprints@expert-reviews.com New triazoles and echinocandins: mode of action, in vitro activity and mechanisms of resistance Expert Rev. Anti Infect. Ther. 7(8), 981 998
Resistance epidemiology
 ECMM/EFISG symposium: Multidrug resistance in fungi? A formidable foe Resistance epidemiology Ana Alastruey Izquierdo Mycology Reference Lab Spain Instituto de Salud Carlos III Disclousure I have received
ECMM/EFISG symposium: Multidrug resistance in fungi? A formidable foe Resistance epidemiology Ana Alastruey Izquierdo Mycology Reference Lab Spain Instituto de Salud Carlos III Disclousure I have received
ESCMID Online Lecture Library. by author
 The antibacterial experience: indications for clinical use of antimicrobial combinations To prevent the emergence of resistant organisms (tuberculosis) To treat polymicrobial infections (abdominal complicated
The antibacterial experience: indications for clinical use of antimicrobial combinations To prevent the emergence of resistant organisms (tuberculosis) To treat polymicrobial infections (abdominal complicated
Dr Hamed Alzoubi. Fungal infections
 Dr Hamed Alzoubi Fungal infections Skin & subcutaneous Mycoses 1-Superficial mycoses such as 2-Cutaneous mycoses such as 3-Subcutaneous mycoses Tinea versicolor or Pityriasis versicolor Ring worm or Tinea
Dr Hamed Alzoubi Fungal infections Skin & subcutaneous Mycoses 1-Superficial mycoses such as 2-Cutaneous mycoses such as 3-Subcutaneous mycoses Tinea versicolor or Pityriasis versicolor Ring worm or Tinea