Cases AMC HIV/HCV Conference 2015
|
|
|
- Osborn Skinner
- 5 years ago
- Views:
Transcription
1 Cases AMC HIV/HCV Conference 2015 CYNTHIA MILLER, MD SHELLEY GILROY, MD DIVISION OF H IV MEDICI N E A LBANY MEDICAL COLLEG E JUNE 3, 2015 Pre-Exposure Prophylaxis A 32 y.o. male comes to your office for HIV testing. On review, you learn that he is sexually active with several men, usually without condoms. At completion of the appointment, you: A. Refer him for STD testing B. Refer him for STD testing and recommend he consider PrEP C. Test him for HIV with no further discussion D. Tell him what he s doing is immoral 91% 3% 6% 0% Refer him for STD testing Refer him for STD testing... Test him for HIV with no... Tell him what he s doing i... 1
2 You refer him for STD testing (or do it yourself if that is an option) and recommend consideration of PrEP. PrEP has been found to be: 88% A. 25% effective at HIV prevention when the patient takes all doses of medication B. 46% effective C. 71% effective D. 92% effective 0% 0% 12% 25% effective at HIV prev... 46% effective 71% effective 92% effective What is the recommended medication for PrEP? A. Tenofovir alone B. Tenofovir and emtricitabine C. Lamivudine and abacavir D. Both B and C 53% 23% 23% 0% Tenofovir alone Tenofovir and emtricitabine Lamivudine and abacavir Both B and C 2
3 What laboratories should be monitored regularly? A. Serum Cr B. RPR C. Urine, throat, and rectal chlamydia and gonorrhea D. All of the above 36% 51% 7% 7% Serum Cr RPR Urine, throat, and rectal... All of the above Success or Failure? A 54 y.o. male is new to your office. He is known to be HCV positive and has failed therapy in the past with pegylated interferon (PEG) and ribavirin (RBV). Further details are not known and are unavailable. Additional past medical history includes coronary artery disease, s/p CABG, and moderate but stable renal failure. He is HIV negative. 3
4 Baseline laboratories include normal CBC and chemistries as follows: Na- 139 K- 4.2 Cl- 115 Bicarb- 25 BUN- 10 Cr- 1.9 Glucose- 102 AST- 30 (12-30) ALT- 45 (15-60) Evaluation of the liver should include: A. Liver biopsy, the gold standard 91% B. HCV genotype; no further evaluation needed if he has genotype 4 because disease will not advance C. No evaluation is necessary because his transaminases are normal D. FibroSURE or FibroSPECT, HCV genotype 5% 3% 0% Liver biopsy, the gold st... HCV genotype; no furthe... No evaluation is necessa.. FibroSURE or FibroSPECT... 4
5 Do you need a viral load in order to decide whether to treat? A. Yes B. No 77% 23% Yes No The patient s results return with Fibrosis level 3, Activity level (inflammation) 1. This patient should A. Be treated, as he has significant disease B. Not be treated, as he does not have significant disease C. He cannot be treated due to his renal disease 96% 2% 2% Be treated, as he has sign... Not be treated, as he do.. He cannot be treated du... 5
6 The patient has genotype 1a virus. What is the best choice for treatment among those listed? A. Sofosbuvir/ledipasvir for 12 weeks B. Sofosbuvir/simeprevir for 24 weeks C. Sofosbuvir/ribavirin for 24 weeks 62% 29% 9% Sofosbuvir/ledipasvir for... Sofosbuvir/simeprevir fo... Sofosbuvir/ribavirin for... At 12 weeks, this pt s HCV viral load is detectable but <12. Has this patient failed therapy? A. Yes B. No 65% 35% Yes No 6
7 Drug-Drug Interactions A 36 y.o. male with a history of IV drug use has both HIV and HCV infections. He is not co-infected with HBV. He is known to have compensated cirrhosis with a history of small nonbleeding varices. He has a history of a psychotic break while taking PEG/ RBV. After treatment with respiradone, he was shepherded carefully through re-treatment with triple therapy including PEG, RBV, and telaprevir, but failed at 24 weeks, after initial success. You would like to try again to treat. He is genotype 1a. Medications: Tenofovir-emtricitabine, nelfinavir, and risperadone You can go ahead with treatment: 50% 50% A. True B. False 7
8 Change nelfinavir to: A. Darunavir/ritonavir B. Raltegravir C. Rilpivirine D. Elvitegravir/cobicistat 30% 48% 15% 7% Darunavir/ritonavir Raltegravir Rilpivirine Elvitegravir/cobicistat The patient is now on Tenofovir-emtricitabine and raltegravir. Now you can treat? A. True B. False 84% 16% True False 8
9 Change tenofovir to: A. Abacavir, after checking HLA B5701 B. Lamivudine C. Maraviroc 67% 17% 17% Abacavir, after checking... Lamivudine Maraviroc Now you can treat: A. True B. False 0% 0% True False 9
10 Our patient is more than halfway through his 24 week therapy, currently with viral load undetectable. Acute Hepatitis A 54 y.o. male relocated to Albany was seen in the office to resume medication. He had previously been on a darunavir/ritonavir combination but had not tolerated it well. He is HIV positive, CDC class C3, with recent diarrhea due to giardiasis, now resolving after treatment. He is sexually active with his long- term partner, without consistent use of condoms. He has no known HIV resistance mutations. His baseline CD4 cell count is
11 He is begun on tenofovir-emtricitabine and raltegravir in the summer of When seen 1, 3, and 6 months later, He is tolerating this regimen well. Diarrhea has resolved. He is asymptomatic. Past labs include HCV Ab negative and HBV sab positive. 3 months ago transaminases were normal. Routine labs return with CD4 cell count 67, HIV VL<40, AST 271 and ALT 340. What has happened? A. Acute Hepatitis due to antiretrovirals B. Acute hepatitis due to hepatitis B C. Acute hepatitis due to hepatitis C D. Acute hepatitis due to hepatitis D 33% 15% 52% 0% Acute Hepatitis due to an... Acute hepatitis due to h... Acute hepatitis due to h... Acute hepatitis due to h... 11
12 On questioning he admits unsafe sex outside his partnership. What tests should you order now? A. Hepatitis C Ab 54% B. Hepatitis C viral load C. Both A and B D. Hepatitis C genotype E. And don t forget to test for other STDs! 10% 10% 5% 22% Hepatitis C Ab Hepatitis C viral load Both A and B Hepatitis C genotype And don t forget to test... Hepatitis C Ab is negative and viral load is positive at IU/ml, consistent with acute hepatitis C. What should you do next? A. Treat for hepatitis C B. Hold treatment for hepatitis C 55% 45% Treat for hepatitis C Hold treatment for hepati... 12


13 Transaminases As time passes it becomes clear that he has developed chronic hepatitis C. His transaminases have returned to normal but HCV viral load remains positive. The CD4 cell count is 106. What should you do now? A. Treat for hepatitis C B. Hold treatment for hepatitis C 67% 33% Treat for hepatitis C Hold treatment for hepati... 13
14 Six months later his CD4 cell count is over 200 and you decide to treat HCV. He is genotype 3. What is the recommended therapy? 49% A. Sofosbuvir/ledisasvir B. Sofosbuvir /declatasvir C. Ombitasvir/paritaprevir/ritonavir and dasabuvir D. Sofosbuvir and RBV 10% 15% 26% Sofosbuvir/ledisasvir Sofosbuvir /declatasvir Ombitasvir/paritaprevir/... Sofosbuvir and RBV Does he have significant drug-drug interactions? He is now on tenofovir- emtricitabine-elvitegravir-cobicistat, having changed due to wishing to be on a simpler regimen: A. Yes B. No 54% 46% Yes No 14
15 The patient begins therapy with sofosbuvir/ribavirin for 24 weeks. He is currently undetectable at 12 weeks. HIV remains in control. HIV Treatment Failure A 54 y.o. male with HIV CDC class C3 returns to Albany after 10 years in another community. In the past he had been treated with serial mono- and duotherapy: AZT (zidovudine) alone, ddi (didanosine) alone, AZT plus 3TC (lamivudine), indinavir plus AZT and 3TC, nelfinavir plus AZT and 3TC. He cannot recall everything he took while he was away. For a while, he took a drug holiday (off therapy for 2 years). At present he is on tipranavir, ritonavir, tenofovir, and raltegravir. 15
16 He is HCV negative. He is HBV negative, vaccinated but with no response. He is 100% adherent to medication and has not been sexually active in many years. His only symptom is chronic diarrhea, for many years, both on and off medication. Workup for GI pathology including colonoscopy is negative. He uses imodium regularly. Current CD4 cell count is over 500. On routine follow up in late 2014 (1.5 years later), HIV viral load is 123. What should you do now? A. Repeat VL in one month. He may have had a blip. B. Repeat VL at the next office visit 80% 20% Repeat VL in one month... Repeat VL at the next offi.. 16
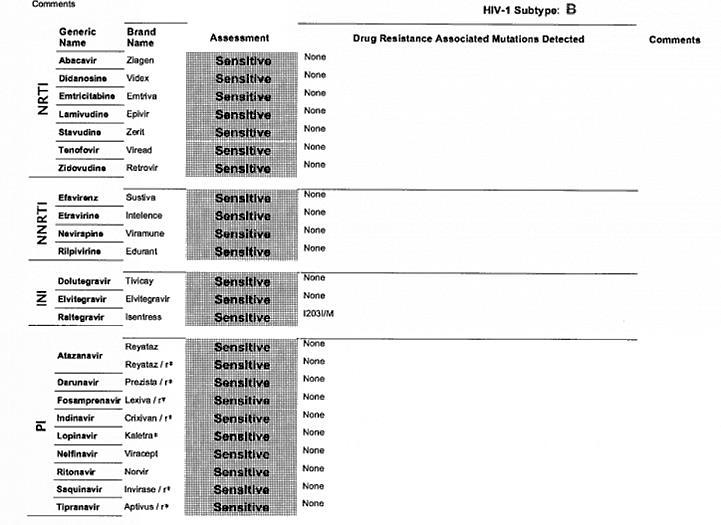
17 Repeat VL done now is 320. What should you do now? A. Obtain a genotype B. Obtain a phenotype C. Review old genos/phenos 31% 22% 47% Obtain a genotype Obtain a phenotype Review old genos/phenos Review of old genos/phenos reveals: 67N, 70R, 184V, 211K, 98G, 1791, 198A and multiple PI mutations. (9) He has never had resistance testing for integrase inhibitors. However, his most recent genotype, done at his previous doctor s, is pansensitive. What should you do now? 17


18 March 2, 2006 July 13,

19 January 15, 2015 A genotype Archive is obtained. At present the patient remains stable with an excellent CD4 cell count and low but positive VL. 19

20 February 2,
Hepatitis C Medications Prior Authorization Criteria
 Hepatitis C Medications Authorization Criteria Epclusa (/velpatasvir), Harvoni (ledipasvir/), Sovaldi (), Daklinza (daclatasvir), Zepatier (elbasvir/grazoprevir), Olysio (simeprevir), Viekira Pak (ombitasvir/paritaprevir/ritonavir;
Hepatitis C Medications Authorization Criteria Epclusa (/velpatasvir), Harvoni (ledipasvir/), Sovaldi (), Daklinza (daclatasvir), Zepatier (elbasvir/grazoprevir), Olysio (simeprevir), Viekira Pak (ombitasvir/paritaprevir/ritonavir;
HIV Update Objectives. Epidemiology. Epidemiology, Transmission and Natural History. Transmission Risk by Exposure. Transmission 9/29/2014
 Objectives HIV Update 2014 Jay Sizemore, MD, MPH Medical Director Chattanooga CARES Assistant Professor UTCOM Chattanooga 2October 2014 Review HIV epidemiology and screening/testing guidelines Discuss
Objectives HIV Update 2014 Jay Sizemore, MD, MPH Medical Director Chattanooga CARES Assistant Professor UTCOM Chattanooga 2October 2014 Review HIV epidemiology and screening/testing guidelines Discuss
SEVERE LIVER DISEASES & HIV INFECTION
 SEVERE LIVER DISEASES & HIV INFECTION SEVERE LIVER DISEASES AND HIV INFECTION Liver diseases ranks as a serious cause of morbidity and mortality in HIV infected persons, whose HIV disease is effectively
SEVERE LIVER DISEASES & HIV INFECTION SEVERE LIVER DISEASES AND HIV INFECTION Liver diseases ranks as a serious cause of morbidity and mortality in HIV infected persons, whose HIV disease is effectively
Section 6: Treatment of Hepatitis C virus (HCV)
") Section 6: Treatment of Hepatitis C virus (HCV) Dr. Niklas Luhmann (Médecins du Monde) Training Hepatitis C and HR for PWUD, 9 th -13 th May 2016, Hanoi, Vietnam Learning objective of the session: understanding
Section 6: Treatment of Hepatitis C virus (HCV) Dr. Niklas Luhmann (Médecins du Monde) Training Hepatitis C and HR for PWUD, 9 th -13 th May 2016, Hanoi, Vietnam Learning objective of the session: understanding
British HIV Association Guidelines for the Management of Hepatitis Viruses in Adults Infected with HIV 2013 Appendix 2
 British HIV Association Guidelines for the Management of Hepatitis Viruses in Adults Infected with HIV 2013 Appendix 2 Systematic literature search 2.1 Questions and PICO criteria Data bases: Medline,
British HIV Association Guidelines for the Management of Hepatitis Viruses in Adults Infected with HIV 2013 Appendix 2 Systematic literature search 2.1 Questions and PICO criteria Data bases: Medline,
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV
 POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines
 The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
HIV basics. Katya Calvo Medical Director of Antimicrobial Stewardship
 HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
Case-Based Scenarios in Hepatitis C
 Case-Based Scenarios in Hepatitis C Alicia Stivala, NP HIV/HCV Co-infection Clinic, Mount Sinai Medical Center New York, NY Final Achieving an SVR is Associated With Improved Outcomes Sustained viral response
Case-Based Scenarios in Hepatitis C Alicia Stivala, NP HIV/HCV Co-infection Clinic, Mount Sinai Medical Center New York, NY Final Achieving an SVR is Associated With Improved Outcomes Sustained viral response
Global Prevalence of HBV, HCV, HIV
 Treatment of Patients with HCV and HIV Paul Y. Kwo, MD, FACG Professor of Medicine Stanford University email: pkwo@stanford.edu Global Prevalence of HBV, HCV, HIV 24 m Journal of Clinical Virology Page
Treatment of Patients with HCV and HIV Paul Y. Kwo, MD, FACG Professor of Medicine Stanford University email: pkwo@stanford.edu Global Prevalence of HBV, HCV, HIV 24 m Journal of Clinical Virology Page
Separate clinical trials for HIV- HCV coinfected patients are NOT a necessity. Patrick Ingiliz, Berlin
 Separate clinical trials for HIV- HCV coinfected patients are NOT a necessity Patrick Ingiliz, Berlin Back in the days when HCV genotype 1 was the problem SVR (%) 100 90 80 70 60 50 40 30 20 10 0 35% PRESCO
Separate clinical trials for HIV- HCV coinfected patients are NOT a necessity Patrick Ingiliz, Berlin Back in the days when HCV genotype 1 was the problem SVR (%) 100 90 80 70 60 50 40 30 20 10 0 35% PRESCO
Nothing to disclose.
 Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital HIV UPDATE FOR THE PRIMARY CARE PROVIDER Nothing to disclose. 1 Outline Epidemiology Screening / testing for HIV
Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital HIV UPDATE FOR THE PRIMARY CARE PROVIDER Nothing to disclose. 1 Outline Epidemiology Screening / testing for HIV
HCV Case Studies (and Special Populations)
") HCV Case Studies (and Special Populations) Case 1: Alfred 58 y/o man presents to clinic for primary care f/u. PMH: Hypertension, diabetes Medications: lisinopril, glipizide Allergies: NKDA Family History:
HCV Case Studies (and Special Populations) Case 1: Alfred 58 y/o man presents to clinic for primary care f/u. PMH: Hypertension, diabetes Medications: lisinopril, glipizide Allergies: NKDA Family History:
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Considerations for the management of Hepatitis C in patients with HIV co-infection
 Considerations for the management of Hepatitis C in patients with HIV co-infection Marcella Honkonen, PharmD, BCPS Sunday, February 22, 2012 at 10:15 AM AzPA Southwest Clinical Conference JW Marriott,
Considerations for the management of Hepatitis C in patients with HIV co-infection Marcella Honkonen, PharmD, BCPS Sunday, February 22, 2012 at 10:15 AM AzPA Southwest Clinical Conference JW Marriott,
THE HIV LIFE CYCLE. Understanding How Antiretroviral Medications Work
 THE HIV LIFE CYCLE Understanding How Antiretroviral Medications Work DEFINITIONS Host: The animal or cell that another organism lives in. In HIV human CD4 T-cells are the host for HIV. Nucleus: The core
THE HIV LIFE CYCLE Understanding How Antiretroviral Medications Work DEFINITIONS Host: The animal or cell that another organism lives in. In HIV human CD4 T-cells are the host for HIV. Nucleus: The core
HIV/HCV Coinfection: Why It Matters and What To Do About It. Cody A. Chastain, MD 10/26/16
 HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
ART and Prevention: What do we know?
 ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
Review: How to work up your patient with Hepatitis C
 Review: How to work up your patient with Hepatitis C You screened your patient, and now the HCV antibody test is positive. What do you do next? The antibody test only means they have been exposed to HCV.
Review: How to work up your patient with Hepatitis C You screened your patient, and now the HCV antibody test is positive. What do you do next? The antibody test only means they have been exposed to HCV.
TORONTO GENERAL HOSPITAL HIV AMBULATORY CARE ROTATION
 TGH - ambulatory rotation page 1 of 5 TORONTO GENERAL HOSPITAL HIV AMBULATORY CARE ROTATION SITE: Immunodeficiency Clinic, Toronto General Hospital, University Health Network Location: 13 th floor, Norman
TGH - ambulatory rotation page 1 of 5 TORONTO GENERAL HOSPITAL HIV AMBULATORY CARE ROTATION SITE: Immunodeficiency Clinic, Toronto General Hospital, University Health Network Location: 13 th floor, Norman
Developments in the Treatment of Hepatitis C: A New Era
 Developments in the Treatment of Hepatitis C: A New Era Nancy Love, PharmD, BCPS Memorial Medical Center, Johnstown, PA October 17, 2014 Pharmacist Objectives Summarize the results of clinical trials for
Developments in the Treatment of Hepatitis C: A New Era Nancy Love, PharmD, BCPS Memorial Medical Center, Johnstown, PA October 17, 2014 Pharmacist Objectives Summarize the results of clinical trials for
PHARMACOKINETICS OF ANTIRETROVIRAL AND ANTI-HCV AGENTS
 8. PHARMACOKINETICS OF ANTIRETROVIRAL AND ANTI-HCV AGENTS David Burger José Moltó Table 8.1a: INFLUENCE OF FOOD ON ABSORPTION (AREA UNDER THE CURVE) OF ANTIRETROVIRAL AGENTS NUCLEOSIDE ANALOGUES NtRTI
8. PHARMACOKINETICS OF ANTIRETROVIRAL AND ANTI-HCV AGENTS David Burger José Moltó Table 8.1a: INFLUENCE OF FOOD ON ABSORPTION (AREA UNDER THE CURVE) OF ANTIRETROVIRAL AGENTS NUCLEOSIDE ANALOGUES NtRTI
Case # 1. Case #1 (cont d)
") Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C First Generation Agents Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Hepatitis C First Generation Agents Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret
 New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
Woman with HIV/HBV/HCV
 Case Woman with HIV/HBV/HCV 50 year woman with past IDU and high risk sexual intercourse with HIV and HBV HIV is well controlled on Darunavir/ritonavir + Tenfovir/Emtricitabine (first regimen) HBV HBeAg
Case Woman with HIV/HBV/HCV 50 year woman with past IDU and high risk sexual intercourse with HIV and HBV HIV is well controlled on Darunavir/ritonavir + Tenfovir/Emtricitabine (first regimen) HBV HBeAg
Transmission of HCV in the United States (CDC estimate)
") Transmission of HCV in the United States (CDC estimate) Past and Future US Incidence and Prevalence of HCV Infection Decline among IDUs Overall incidence Overall prevalence Infected 20+ years Armstrong
Transmission of HCV in the United States (CDC estimate) Past and Future US Incidence and Prevalence of HCV Infection Decline among IDUs Overall incidence Overall prevalence Infected 20+ years Armstrong
Bruce A. Luxon, MD, Ph.D. Anton and Margaret Fuisz Chair in Medicine Professor and Chair Department of Medicine Georgetown University
 Bruce A. Luxon, MD, PhD, FACG Bruce A. Luxon, MD, Ph.D. Anton and Margaret Fuisz Chair in Medicine Professor and Chair Department of Medicine Georgetown University Dr. Luxon is on the speakers p bureau
Bruce A. Luxon, MD, PhD, FACG Bruce A. Luxon, MD, Ph.D. Anton and Margaret Fuisz Chair in Medicine Professor and Chair Department of Medicine Georgetown University Dr. Luxon is on the speakers p bureau
NON-OCCUPATIONAL POST EXPOSURE PROPHYLAXIS IN HIV PREVENTION. Jason E. Vercher, PA-C, AAHIVM
 NON-OCCUPATIONAL POST EXPOSURE PROPHYLAXIS IN HIV PREVENTION Jason E. Vercher, PA-C, AAHIVM Disclosures No disclosures to report Learning Objectives q Identify Individuals who would benefit from non-occupational
NON-OCCUPATIONAL POST EXPOSURE PROPHYLAXIS IN HIV PREVENTION Jason E. Vercher, PA-C, AAHIVM Disclosures No disclosures to report Learning Objectives q Identify Individuals who would benefit from non-occupational
HIV Basics: Clinical Tests and Guidelines
 HIV Basics: Clinical Tests and Guidelines ACTHIV 2010 Zelalem Temesgen MD Mayo Clinic Topics Baseline laboratory evaluation Laboratory monitoring through the continuum of care Patients not on antiretroviral
HIV Basics: Clinical Tests and Guidelines ACTHIV 2010 Zelalem Temesgen MD Mayo Clinic Topics Baseline laboratory evaluation Laboratory monitoring through the continuum of care Patients not on antiretroviral
HIV-HCV coinfection. Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Baltimore, Maryland
 HIV-HCV coinfection Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Baltimore, Maryland Disclosures Principal investigator for research grants Funds paid to Johns Hopkins
HIV-HCV coinfection Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Baltimore, Maryland Disclosures Principal investigator for research grants Funds paid to Johns Hopkins
Length of Authorization: 8-12 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
What we will cover. HIV in Case 1. HIV drugs frequently cause drug reactions. What is the most likely diagnosis
 HIV in 2009 Susan Hopkins Consultant in Infectious Diseases & Microbiology Royal Free Hampstead NHS Trust What we will cover Not Opportunistic Infections Important adverse events Important points to consider
HIV in 2009 Susan Hopkins Consultant in Infectious Diseases & Microbiology Royal Free Hampstead NHS Trust What we will cover Not Opportunistic Infections Important adverse events Important points to consider
Treatment of respiratory virus infection Influenza A & B Respiratory Syncytial Virus (RSV)
") Treatment of respiratory virus infection Influenza A & B Respiratory Syncytial Virus (RSV) Amantadine and Rimantadine Use is limited to Influenza A infection. Very effective in preventing infection if
Treatment of respiratory virus infection Influenza A & B Respiratory Syncytial Virus (RSV) Amantadine and Rimantadine Use is limited to Influenza A infection. Very effective in preventing infection if
HIV medications HIV medication and schedule plan
 Living with HIV (human immunodeficiency virus) It may be scary to find out that you re HIV-positive or have AIDS. Coping with this news may be difficult. Although HIV is a serious infection, people with
Living with HIV (human immunodeficiency virus) It may be scary to find out that you re HIV-positive or have AIDS. Coping with this news may be difficult. Although HIV is a serious infection, people with
Pegylated Interferons and Ribavirins
 Pegylated Interferons and Ribavirins Goal(s): Cover drugs only for those clients where there is evidence of effectiveness and safety Length of Authorization: 16 weeks plus 12-36 additional weeks or 12
Pegylated Interferons and Ribavirins Goal(s): Cover drugs only for those clients where there is evidence of effectiveness and safety Length of Authorization: 16 weeks plus 12-36 additional weeks or 12
Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update
 Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
The Future of HIV: Advances in Drugs and Research. Shauna Gunaratne December 17, 2018
 The Future of HIV: Advances in Drugs and Research Shauna Gunaratne December 17, 2018 Overview Epidemiology Science of HIV How HIV treatment and management have changed over the years New medicines and
The Future of HIV: Advances in Drugs and Research Shauna Gunaratne December 17, 2018 Overview Epidemiology Science of HIV How HIV treatment and management have changed over the years New medicines and
HIV Drugs and the HIV Lifecycle
 HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV and Hepatitis C Have we finally slayed the beast?
 HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
Simplifying HIV Treatment Now and in the Future
 Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
HIV 101. Applications of Antiretroviral Therapy
 HIV 101. Applications of Antiretroviral Therapy Michael S. Saag, MD Professor of Medicine Associate Dean for Global Health Jim Straley Chair in AIDS Research University of Alabama at Birmingham Birmingham,
HIV 101. Applications of Antiretroviral Therapy Michael S. Saag, MD Professor of Medicine Associate Dean for Global Health Jim Straley Chair in AIDS Research University of Alabama at Birmingham Birmingham,
Meet the Professor: HIV/HCV Coinfection
 Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Clinical Criteria for Hepatitis C (HCV) Therapy
 Therapy") Diagnosis Clinical Criteria for Hepatitis C (HCV) Therapy Must have chronic hepatitis C (HCV infection > 6 months), genotype and sub-genotype specified to determine the length of therapy; Liver biopsy
Diagnosis Clinical Criteria for Hepatitis C (HCV) Therapy Must have chronic hepatitis C (HCV infection > 6 months), genotype and sub-genotype specified to determine the length of therapy; Liver biopsy
KEEP LOVING. Because HIV doesn t change who you are.
 KEEP LOVING. Because HIV doesn t change who you are. BIKTARVY is a complete, 1-pill, once-a-day prescription medicine used to treat HIV-1 in certain adults. BIKTARVY does not cure HIV-1 or AIDS. Please
KEEP LOVING. Because HIV doesn t change who you are. BIKTARVY is a complete, 1-pill, once-a-day prescription medicine used to treat HIV-1 in certain adults. BIKTARVY does not cure HIV-1 or AIDS. Please
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C First Generation Agents Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Hepatitis C First Generation Agents Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
BVHG/BASL/BSG/BHIVA/BIA/CVN Guidelines for management of chronic HCV infection
 BVHG/BASL/BSG/BHIVA/BIA/CVN Guidelines for management of chronic HCV infection Headline Recommendations 1. We recommend that NHSE considers commissioning pan-genotypic regimens for use in the community
BVHG/BASL/BSG/BHIVA/BIA/CVN Guidelines for management of chronic HCV infection Headline Recommendations 1. We recommend that NHSE considers commissioning pan-genotypic regimens for use in the community
HIV Management Update 2015
 9/30/15 HIV Management Update 2015 Larry Pineda, PharmD, PhC, BCPS Visiting Assistant Professor Pharmacy Practice and Administrative Science ljpineda@salud.unm.edu Pharmacist Learning Objectives Describe
9/30/15 HIV Management Update 2015 Larry Pineda, PharmD, PhC, BCPS Visiting Assistant Professor Pharmacy Practice and Administrative Science ljpineda@salud.unm.edu Pharmacist Learning Objectives Describe
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES?
 WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
1/16/2019. Goals of HCV Therapy. Objectives. Treating Hepatitis C and HIV Co Infection. Cure Defined as sustained virologic response (SVR)
") HCV ECHO WESTERN STATES HCV ECHO WESTERN STATES Treating Hepatitis C and HIV Co Infection Paulina Deming, Pharm D Associate Professor, College of Pharmacy Assistant Director, Viral Hepatitis Programs,
HCV ECHO WESTERN STATES HCV ECHO WESTERN STATES Treating Hepatitis C and HIV Co Infection Paulina Deming, Pharm D Associate Professor, College of Pharmacy Assistant Director, Viral Hepatitis Programs,
Didactic Series. Archive Genotype Resistance Testing in the Setting of Regimen Switching
 Didactic Series Archive Genotype Resistance Testing in the Setting of Regimen Switching Craig Ballard, Pharm.D., AAHIVP UCSD Medical Center Owen Clinic June 11, 2015 ACCREDITATION STATEMENT: University
Didactic Series Archive Genotype Resistance Testing in the Setting of Regimen Switching Craig Ballard, Pharm.D., AAHIVP UCSD Medical Center Owen Clinic June 11, 2015 ACCREDITATION STATEMENT: University
PEARL-I. Ombitasvir + Paritaprevir + Ritonavir +/- Ribavirin in HCV GT4. Treatment Naïve and Treatment Experienced
 Phase 2b Treatment Naïve and Treatment Experienced Ombitasvir + Paritaprevir + Ritonavir +/- Ribavirin in HCV GT4 PEARL-I Hézode C, et al. Lancet. 2015 March 30. [Epub ahead of print] PEARL-I: Study Design
Phase 2b Treatment Naïve and Treatment Experienced Ombitasvir + Paritaprevir + Ritonavir +/- Ribavirin in HCV GT4 PEARL-I Hézode C, et al. Lancet. 2015 March 30. [Epub ahead of print] PEARL-I: Study Design
Brief Review of HIV and Hepatitis C Virus (HCV) Infection (with focus on HCV)
 Infection (with focus on HCV)") Brief Review of HIV and Hepatitis C Virus (HCV) Infection (with focus on HCV) James Morrill, MD, PhD MGH Charlestown HealthCare Center Massachusetts General Hospital www.mghcme.org Disclosures Neither
Brief Review of HIV and Hepatitis C Virus (HCV) Infection (with focus on HCV) James Morrill, MD, PhD MGH Charlestown HealthCare Center Massachusetts General Hospital www.mghcme.org Disclosures Neither
Blood-Borne Pathogens and Post-Exposure Prophylaxis
 Blood-Borne Pathogens and Post-Exposure Prophylaxis Christopher Behrens MD Northwest Association of Occupational and Environmental Medicine October 2017 with thanks to Shireesha Dhanireddy MD Disclosures
Blood-Borne Pathogens and Post-Exposure Prophylaxis Christopher Behrens MD Northwest Association of Occupational and Environmental Medicine October 2017 with thanks to Shireesha Dhanireddy MD Disclosures
Hepatitis and HIV Co-Infection: Situation in Ukraine.
 2nd Central and Eastern European Meeting on Viral Hepatitis and Co-Infection with HIV Hepatitis and HIV Co-Infection: Situation in Ukraine. Pavlo Skala Associate Director: Policy & Partnership Ukraine
2nd Central and Eastern European Meeting on Viral Hepatitis and Co-Infection with HIV Hepatitis and HIV Co-Infection: Situation in Ukraine. Pavlo Skala Associate Director: Policy & Partnership Ukraine
WOMEN'S INTERAGENCY HIV STUDY METABOLIC STUDY: MS01 SPECIMEN COLLECTION FORM
 WOMEN'S INTERAGENCY HIV STUDY METABOLIC STUDY: MS01 SPECIMEN COLLECTION FORM ID LABEL HERE ---> VERSION DATE 10/01/07 - - - VISIT #: FORM COMPLETED BY: A1. DATE OF BLOOD DRAW: / / M D Y A2. Do you take
WOMEN'S INTERAGENCY HIV STUDY METABOLIC STUDY: MS01 SPECIMEN COLLECTION FORM ID LABEL HERE ---> VERSION DATE 10/01/07 - - - VISIT #: FORM COMPLETED BY: A1. DATE OF BLOOD DRAW: / / M D Y A2. Do you take
I M ENDING HIV PATIENT INFORMATION. endinghiv.org.au/prep
 I M ENDING HIV PrEP PATIENT INFORMATION endinghiv.org.au/prep THIS BOOKLET PROVIDES YOU WITH INFORMATION ABOUT Pre-Exposure Prophylaxis (PrEP) for HIV. CONTENTS 06 Who will benefit from PrEP? 04 What is
I M ENDING HIV PrEP PATIENT INFORMATION endinghiv.org.au/prep THIS BOOKLET PROVIDES YOU WITH INFORMATION ABOUT Pre-Exposure Prophylaxis (PrEP) for HIV. CONTENTS 06 Who will benefit from PrEP? 04 What is
Management of HIV Infected Children and Adolescents: Public Sector Approach in Kenya
 Management of HIV Infected Children and Adolescents: Public Sector Approach in Kenya KPA 2018 24-04-2018 Dr. Margaret Wainaina- Wafula Outline Introduction Evaluation of a child living with HIV. Standard
Management of HIV Infected Children and Adolescents: Public Sector Approach in Kenya KPA 2018 24-04-2018 Dr. Margaret Wainaina- Wafula Outline Introduction Evaluation of a child living with HIV. Standard
What is Hepatitis C Virus (HCV)?
?") HEPATITIS C VIRUS (HCV) What is Hepatitis C Virus (HCV)? Hepatitis is an inflammation (swelling or tenderness) of the liver. Hepatitis C virus (HCV) is the most common form of viral hepatitis and usually
HEPATITIS C VIRUS (HCV) What is Hepatitis C Virus (HCV)? Hepatitis is an inflammation (swelling or tenderness) of the liver. Hepatitis C virus (HCV) is the most common form of viral hepatitis and usually
Principles of Antiretroviral Therapy
 Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Hepatitis C Direct-Acting Antivirals
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
HIV, Hepatitis C, and Treatment 3/26/13. What Do HIV Medications Do? George Beatty, MD, MPH
 HIV, Hepatitis C, and Treatment 3/26/13 What Do HIV Medications Do? George Beatty, MD, MPH BIOGRAPHY: Dr Beatty is a clinician educator and has been on the faculty since 1998. He served as Director of
HIV, Hepatitis C, and Treatment 3/26/13 What Do HIV Medications Do? George Beatty, MD, MPH BIOGRAPHY: Dr Beatty is a clinician educator and has been on the faculty since 1998. He served as Director of
2015 OPSC Annual Convention. syllabus. February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California
 2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California SUNDAY, FEBRUARY 8, 2015: 10:00am - 11:00am Primary Care of the HIV Patient Presented by Jim Lee,
2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California SUNDAY, FEBRUARY 8, 2015: 10:00am - 11:00am Primary Care of the HIV Patient Presented by Jim Lee,
HIV and Hepatitis C: Advances in Treatment
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and Hepatitis C: Advances in Treatment John Scott, MD, MSc Asst Professor University of Washington Presentation prepared & presented by: John Scott, MD,
NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and Hepatitis C: Advances in Treatment John Scott, MD, MSc Asst Professor University of Washington Presentation prepared & presented by: John Scott, MD,
HCV Treatment in 2016: Genotypes 1, 2, and 3. Cody A. Chastain, MD October 12, 2016
 HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
Objectives. HIV in the Trenches HIV Update for the Primary Care Provider, An Overview The HIV Continuum of Care.
 1:30 2:30pm HIV Update SPEAKER Gordon Dickinson, MD Presenter Disclosure Information The following relationships exist related to this presentation: Gordon Dickinson, MD, has no financial relationships
1:30 2:30pm HIV Update SPEAKER Gordon Dickinson, MD Presenter Disclosure Information The following relationships exist related to this presentation: Gordon Dickinson, MD, has no financial relationships
Antiretroviral Dosing in Renal Impairment
 Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
Hepatitis C Management and Treatment
 Hepatitis C Management and Treatment Kaya Süer Near East University Faculty of Medicine Infectious Diseases and Clinical Microbiology 1 Discovery of Hepatitis C Key facts Hepatitis C: the virus can cause
Hepatitis C Management and Treatment Kaya Süer Near East University Faculty of Medicine Infectious Diseases and Clinical Microbiology 1 Discovery of Hepatitis C Key facts Hepatitis C: the virus can cause
HEPATITIS C TREATMENT UPDATE
 HEPATITIS C TREATMENT UPDATE Hepatitis C: Burden of Disease in USA HCV is generally asymptomatic until advanced liver disease 4.1 million persons ever infected; 3.2 million chronic infections Up to 75%
HEPATITIS C TREATMENT UPDATE Hepatitis C: Burden of Disease in USA HCV is generally asymptomatic until advanced liver disease 4.1 million persons ever infected; 3.2 million chronic infections Up to 75%
Starting Immediate Treatment for HIV-1
 Starting Immediate Treatment for HIV-1 Ronald P. Hattis, MD, MPH Email: ronhattis@foundation.beyondaids.org Associate Prof. of Preventive Medicine, Loma Linda University Secretary, Beyond AIDS Foundation
Starting Immediate Treatment for HIV-1 Ronald P. Hattis, MD, MPH Email: ronhattis@foundation.beyondaids.org Associate Prof. of Preventive Medicine, Loma Linda University Secretary, Beyond AIDS Foundation
Dr Andrew Ustianowski
 BHIVA AUTUMN CONFERENCE 2014 Including CHIVA Parallel Sessions Dr Andrew Ustianowski North Manchester General Hospital 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
BHIVA AUTUMN CONFERENCE 2014 Including CHIVA Parallel Sessions Dr Andrew Ustianowski North Manchester General Hospital 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
LET S TALK about Sticking with your treatment plan
 LET S TALK about Sticking with your treatment plan HOW ONGOING HIV CARE HELPS YOU LIVE A LONGER AND HEALTHIER LIFE Your treatment plan is vital to your overall health (and to reducing HIV transmission)
LET S TALK about Sticking with your treatment plan HOW ONGOING HIV CARE HELPS YOU LIVE A LONGER AND HEALTHIER LIFE Your treatment plan is vital to your overall health (and to reducing HIV transmission)
HIV MEDICATIONS AT A GLANCE. Atripla 600/200/300 mg tablet tablet daily. Complera 200/25/300 mg tablet tablet daily
 HIV MEDICATIONS AT A GLANCE Generic Name Trade Name Strength DIN Usual Dosage Single Tablet Regimen (STR) Products Efavirenz/ Emtricitabine/ rilpivirine/ elvitegravir/ cobicistat/ alafenamide Emtricitabine/
HIV MEDICATIONS AT A GLANCE Generic Name Trade Name Strength DIN Usual Dosage Single Tablet Regimen (STR) Products Efavirenz/ Emtricitabine/ rilpivirine/ elvitegravir/ cobicistat/ alafenamide Emtricitabine/
Hepatitis C Virus (HCV) & Infectious Disease 101 for Hubs & Spokes April 24, :00 pm 1:00 pm
 & Infectious Disease 101 for Hubs & Spokes April 24, :00 pm 1:00 pm") Hepatitis C Virus (HCV) & Infectious Disease 101 for Hubs & Spokes April 24, 2018 12:00 pm 1:00 pm Presenters: Thomas E. Freese, PhD, Larissa Mooney, MD, & Rachel McLean, MPH, Chief, Office of Viral Hepatitis
Hepatitis C Virus (HCV) & Infectious Disease 101 for Hubs & Spokes April 24, 2018 12:00 pm 1:00 pm Presenters: Thomas E. Freese, PhD, Larissa Mooney, MD, & Rachel McLean, MPH, Chief, Office of Viral Hepatitis
Updates in the Treatment of Hepatitis C
 Disclosures Updates in the Treatment of Hepatitis C Arslan Kahloon M.D Assistant Professor of Medicine University of Tennessee, Chattanooga I have no conflicts of interest or financial sponsorship to disclose
Disclosures Updates in the Treatment of Hepatitis C Arslan Kahloon M.D Assistant Professor of Medicine University of Tennessee, Chattanooga I have no conflicts of interest or financial sponsorship to disclose
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
HIV in in Women Women
 HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
Antiviral treatment in Unique Populations
 Antiviral treatment in Unique Populations Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Unique HCV Populations HIV/HCV co-infected
Antiviral treatment in Unique Populations Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Unique HCV Populations HIV/HCV co-infected
HEPATITIS C UPDATES. Sanaa S. Said 10 th April, 2014
 HEPATITIS C UPDATES Sanaa S. Said 10 th April, 2014 CONTENTS Introduction Epidemiology Transmission and Natural history Kenyan guidelines What is new? References INTRODUCTION Hepacivirus genus, Flaviviridae
HEPATITIS C UPDATES Sanaa S. Said 10 th April, 2014 CONTENTS Introduction Epidemiology Transmission and Natural history Kenyan guidelines What is new? References INTRODUCTION Hepacivirus genus, Flaviviridae
Second-Line Therapy NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
SFAF CLINICAL PROTOCOLS
 SFAF CLINICAL PROTOCOLS Page 1 of Supersedes Date: December 31, 2016 Original Date: August 20, 2014 Version: 03 Policy Section: Patient Care Non-Occupational Post Exposure Prophylaxis Program Back ground:
SFAF CLINICAL PROTOCOLS Page 1 of Supersedes Date: December 31, 2016 Original Date: August 20, 2014 Version: 03 Policy Section: Patient Care Non-Occupational Post Exposure Prophylaxis Program Back ground:
HIV-HCV Co-Infection. George Mason University Falls Church, Virginia. Overview. Prevalence of HCV co-infection Incidence and Recent Trends
 HIV-HCV Co-Infection Zobair Younossi MD, MPH, FACG, AGAF, FAASLD Chairman, Department of Medicine, Inova Fairfax Hospital Vice President for Research, Inova Health System Professor of Medicine, VCU-Inova
HIV-HCV Co-Infection Zobair Younossi MD, MPH, FACG, AGAF, FAASLD Chairman, Department of Medicine, Inova Fairfax Hospital Vice President for Research, Inova Health System Professor of Medicine, VCU-Inova
If you are a man that ONLY has sex with women this may not be the brochure for you.
 If you are a man that ONLY has sex with women this may not be the brochure for you. To find resources that best meet your needs check out the following website: http://www.cdc.gov/men Whether you are gay,
If you are a man that ONLY has sex with women this may not be the brochure for you. To find resources that best meet your needs check out the following website: http://www.cdc.gov/men Whether you are gay,
PREP CASES BREAKOUT CASE 1: COPING WITH PILL FATIGUE PE/LABS
 PREP CASES BREAKOUT CASE 1: COPING WITH PILL FATIGUE 28 year-old HIV-negative MSM CC: Rectal Mass and Diarrhea x 2 weeks PMH: No chronic medical issues - Diagnosed with secondary syphilis 9 months ago
PREP CASES BREAKOUT CASE 1: COPING WITH PILL FATIGUE 28 year-old HIV-negative MSM CC: Rectal Mass and Diarrhea x 2 weeks PMH: No chronic medical issues - Diagnosed with secondary syphilis 9 months ago
Guidelines for Implementing Pre-Exposure Prophylaxis For The Prevention of HIV in Youth Peter Havens, MD MS Draft:
 Guidelines for Implementing Pre-Exposure Prophylaxis For The Prevention of HIV in Youth Peter Havens, MD MS Draft: 10-2-2015 Clinical studies demonstrate that when a person without HIV infection takes
Guidelines for Implementing Pre-Exposure Prophylaxis For The Prevention of HIV in Youth Peter Havens, MD MS Draft: 10-2-2015 Clinical studies demonstrate that when a person without HIV infection takes
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Woman with Cervicitis
 1 Infectious Diseases Update David Spach, MD Last Updated: January 30, 2015 Infectious Diseases 2015 Update STDs Hepatitis C Virus HIV Chikungunya Virus Ebola Virus Sexually Transmitted Diseases 2 Woman
1 Infectious Diseases Update David Spach, MD Last Updated: January 30, 2015 Infectious Diseases 2015 Update STDs Hepatitis C Virus HIV Chikungunya Virus Ebola Virus Sexually Transmitted Diseases 2 Woman
Important Safety Information for Adolescents Who Don t Have HIV
 Important Safety Information for Adolescents Who Don t Have HIV This booklet tells you about: HIV The medicine emtricitabine/tenofovir disoproxil fumarate for HIV-1 PrEP What you need to do while taking
Important Safety Information for Adolescents Who Don t Have HIV This booklet tells you about: HIV The medicine emtricitabine/tenofovir disoproxil fumarate for HIV-1 PrEP What you need to do while taking
The Future is Here Now!
 HCV Treatment: Assessing the Patient Prior to Treatment. How Will This Change in the Future? JORGE L. HERRERA M.D., FACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE, MOBILE, AL The Future is Here Now!
HCV Treatment: Assessing the Patient Prior to Treatment. How Will This Change in the Future? JORGE L. HERRERA M.D., FACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE, MOBILE, AL The Future is Here Now!
Management of patients with antiretroviral treatment failure: guidelines comparison
 The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
Hepatitis C: Let s Talk About It. Causes of Hepatitis
 Hepatitis C: Let s Talk About It Susan Thompson, RN, MPH Technical Assistance and Training Program NC Communicable Disease Branch July 2012 Causes of Hepatitis any swelling, inflammation, or irritation
Hepatitis C: Let s Talk About It Susan Thompson, RN, MPH Technical Assistance and Training Program NC Communicable Disease Branch July 2012 Causes of Hepatitis any swelling, inflammation, or irritation
HCV/HIV Coinfection ANTON AND MARGARET FUISZ CHAIR IN MEDICINE. HIV and HCV Share Risk Factors PREVALENCE OF CO-INFECTION BY RISK FACTOR 60%
 HCV/HIV Coinfection BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY HIV and HCV Share Risk Factors PREVALENCE
HCV/HIV Coinfection BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY HIV and HCV Share Risk Factors PREVALENCE
Selecting HCV Treatment
 Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
PrEP in the Real World: Clinical Case Studies
 PrEP in the Real World: Clinical Case Studies Kevin L. Ard, MD, MPH April 30, 2015 Massachusetts General Hospital, National LGBT Health Education Center Continuing Medical Education Disclosure Program
PrEP in the Real World: Clinical Case Studies Kevin L. Ard, MD, MPH April 30, 2015 Massachusetts General Hospital, National LGBT Health Education Center Continuing Medical Education Disclosure Program
HCV TREATMENT OPTIONS
 HCV TREATMENT OPTIONS Trea2ng HCV is never an emergency, but early treatment prevents further liver damage. DAAs are easier to take, and be0er tolerated than PEG- IFN and RBV. Treatment is recommended
HCV TREATMENT OPTIONS Trea2ng HCV is never an emergency, but early treatment prevents further liver damage. DAAs are easier to take, and be0er tolerated than PEG- IFN and RBV. Treatment is recommended
HIV Prevention Pearls
 HIV Prevention Pearls Meghan Rothenberger, MD Assistant Professor Division of Infectious Diseases University of Minnesota Director, Youth and AIDS Projects October 27, 2017 Disclosure Information I have
HIV Prevention Pearls Meghan Rothenberger, MD Assistant Professor Division of Infectious Diseases University of Minnesota Director, Youth and AIDS Projects October 27, 2017 Disclosure Information I have
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Cost impact of an HIV MDT for managing anti-retroviral switch
 Cost impact of an HIV MDT for managing anti-retroviral switch 2016 ST4 Farnaz Dave Infectious Diseases & General Internal Medicine Mr Ian Sayers Specialist Infectious Diseases Pharmacist Dr Fahar Niazi
Cost impact of an HIV MDT for managing anti-retroviral switch 2016 ST4 Farnaz Dave Infectious Diseases & General Internal Medicine Mr Ian Sayers Specialist Infectious Diseases Pharmacist Dr Fahar Niazi