Controversies in Diagnosis and Therapy of Neonatal Sepsis
|
|
|
- Hector Turner
- 5 years ago
- Views:
Transcription

1 Controversies in Diagnosis and Therapy of Neonatal Sepsis Sarah S. Long, M.D. Professor of Pediatrics Drexel University College of Medicine Chief, Section of Infectious Diseases St. Christopher s Hospital for Children Philadelphia, Pennsylvania Dr. Long has no conflict of interest to disclose


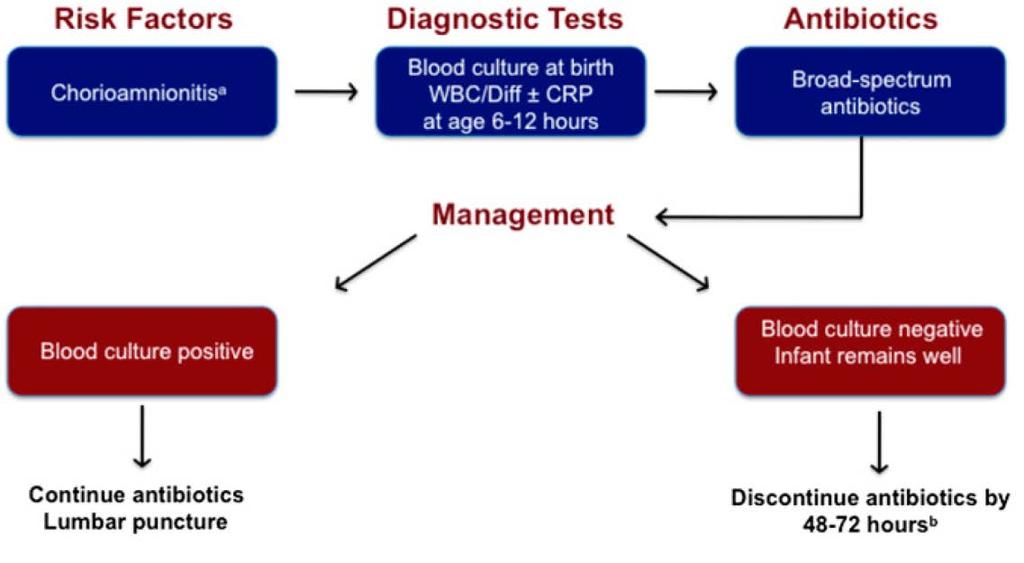
2 Evaluation of a newborn infant shows a normal examination. He was born at 38 weeks gestation by vaginal delivery after 8 hours of rupture of membranes. Mother had fever on presentation in labor and was begun on antibiotics for presumed chorioamnionitis. The most appropriate management of the newborn is: A. Observation B. CBC at 6-12 hrs with further management pending results C. Blood culture, CBC at 6-12 hrs with further management pending results D. Blood culture, CBC at 6-12 hrs, empiric antibiotics, further decision regarding management at 48 hrs

3 Perinatal GBS Guidelines and Resource Utilization Pediatrics 2014;133:196 Guidelines for intrapartum antibiotic prophylaxis 1996, 2002 and 2010 Management well neonate after inadequate IAP: 2002 Guideline Evaluation 15% well-appearing > 35 weeks gestation Empiric antibiotics for 50% evaluated 2010 Guideline Change to evaluate only if additional risk factor present Retrospective cohort study Brigham and Women s of >15000 infants born >36 wks 1 year before and after the 2010 guideline change Results EOS evaluations because of inadequate IAP 31 to <1/1000 neonates Overall evaluations of well appearing neonates 25% No negative consequences/outcomes
 We would not")
4 Chorioamnionitis (CAM) complicates 1-10% of pregnancies Risk early onset neonatal sepsis Maternal Abx risk early onset sepsis Maternal Abx sensitivity neonatal blood cultures AAP CoFN 2012 recs: BC at birth + Empiric Antibiotics If infant remains well appearing Perform CBC + CRP at 6-12 hrs D/C Abx 48 hrs if normal labs & culture Meant to emphasize when to D/C Abx (well, BC, CBC) We would not treat a well appearing >48-72 hrs even if labs abnormal
 24% given prolonged Abx (Most only because of labs) (Most")

5 Study: Phila Retro 554 neonates > 35 wks CAM exposed 28% WBC had IT >.2 or CRP >1 (<1% BC+) 24% given prolonged Abx (Most only because of labs) (Most had LP) Pediatrics 2014;133:1122 Can see how the combination of statements is confusing. CoFN modified its recs in Authors Reply to Ltr to the Editor in 2012 But no new box..


6 2012 Recommendations Commentary 2014 Conundrums New Box
7 J Peds : 1070r Reappraisal of Guidelines Management Suspected EOS Benitz WE, Wynn JL, Polin RA. Commentary J Pediatr (In Press) Generations of CDC/AAP recs prevent/manage EOS since 1992 Inconsistent Clarifications are necessary Local adaptations are common Compliance rates are low Reasons for lack of consensus management re EOS 1) OB prevention strategies incidence EOS Strategy based on risk factors has validity All-cause 34 wks gest >2 in s <<1 in 2000s 2) New data relationships among risk factors and clinical signs Risk predictors may have different utilities in different groups
8 J Peds 2015 Benitz New Data Newborn with Clinical Signs of Illness Many with mild illness (esp. respiratory) become asymptomatic by 6 hrs manage with observation Most (80-100%) with positive blood culture have clinical signs illness <48 hrs Few (2%-5%) with clinical signs illness have EOS NNT with clinical signs to benefit 1 with EOS = Bottom line: Until new tests NPV EOS, evaluate and Rx ill Use serial normal lab test results to discontinue Rx early
9 J Peds 2015 Benitz New Data Newborn with Maternal Chorioamnionitis Guidelines recommend Rx neonate when Dx made Early studies linking Chorio & EOS used strict criteria (maternal fever clinical) Chorio found in 90% cases failure intrapartum abx to prevent EOS Strict criteria Chorio difficult in current practice Dx often based on maternal fever alone Maternal Dx Chorio = crux of reliability as predictor Currently Chorio present in <50% EOS after failed intrapartum abx Currently Chorio risk EOS is strongly dependent on gest age Rates EOS >35 wks if Chorio = <1% (NNT ) <35 wks if Chorio = 5%-17% (NNT 6-21) (Not stratified by clinical signs) Bottom lines: Rx of Chorio-exposed preterm infants is justified. Rx chorio-exp well-appearing >34 wks should be abandoned
10 New Data EOS Stratification Late Preterm/Term by Mat & Infant Risks Peds : ,000 infants >34 weeks gestation Model risk prediction EOS on mult maternal, IP & neonate s exam findings Findings: Optimal utilization of information fails accept strategy Acceptably low NNT ~100 captures only 50% EOS Hashavya PIDJ :840 F-Rimon ActaPaed :e540 Cantoni J Peds :568 G-Munoz PedNeo :381 Need an alternative strategy Multinational studies U.S., Israel, Italy since 2010s Eval incidence EOS >100,000 infants >35 weeks gestation & well-appearing Risk factors maternal +neonatal lab screening tests Findings: Risk EOS extremely low (1/100,000) Lab screening tests add little/no diagnostic info Bottom line: Rely on serial clinical examinations rather than risk factors and lab screening tests
11 Bottom of the Bottom Lines of Benitz, Wynn & Polin Obstetrical interventions to prevent EOS are effective Infant w persistent progressive mod severe signs = Empiric Rx Infant w mild-mod respiratory signs immed birth = Observe for resolution (~6h?) w/o Rx A rapid diagnostic test with sensitivity + NPV = Great but doesn t exist Preterm (<34 wks or <1500g) have risk EOS = Consider Until more data on value risk factors, use them (maternal, clinical & laboratory test in the neonate) Most with infection will have clin signs = Rx Preterm well and no risks = Consider serial monitoring/serial tests
12 Bottom of the Bottom Lines of Benitz, Wynn & Polin Well-appearing late-preterm and term w or w/o risk factors = Close clinical observation (because poor sensitivity risk factors for EOS) Most infants treated for EOS, even with selective strategy, are not infected. Serial normal lab test results = early stop Abx (<48h) In well-appearing with negative culture, Isolated abnormal result(s) should not prolong Abx > 48 hrs Implementation of novel strategies for ascertainment and Rx EOS in late preterm/term should be cautious




13 32 cases perinatally acquired HSV 2011;30:556 50% had only nonspecific S/S at presentation, which was fever in 75% 75% had CNS HSV (40% HSV presenting with mucocutaneous only, 83% HSV with seizures, 94% HSV with nonspecific S/S only) Age 21 days at onset S/S captured 90% of all cases and 94% with nonspecific S/S only Shah. Pediatr 2011;128:1153 Delay acyclovir Rx perinatal HSV from Hosp Day 1 to Day 2/3 was assoc with OR death 2.63




14 Don t forget to look 2012;161:134 J Peds 2015;1 66:827 Plasma and CSF herpes simplex virus levels at diagnosis and outcome of neonatal infection. Melvin AJ, Mohan KM, Schiffer JT et al 63 Seattle infants with HSV and quant. plasma PCR at diagnosis Dissem disease 100% DNAemia CNS disease 64% DNAemia Overall 83% DNAemia SEM disease 78% DNAemia
15 Kimberlin and NIAID CASG 2011;365:1284 Patients: CASG 103 CNS Rx acyclovir IV x3 wks CASG 104 SEM Rx acyclovir IV x 2 wks (Culture/PCR dx, <28d, >800g) Intervent: Acyclovir 300mg/m 2 /dose vs placebo tid x 6 mo or until 2 nd cutaneous recurrence Outcomes: 1 o = Bayley Scales of Infant 2 o = <2 cutaneous recurrences to 12 mo CSF PCR + during/post suppr to 12 mo 3 o = Toxic effects > grade 2 (WHO) Assess: 2 & 4 wks; then q mo on study drug; 12 mo
16 TIME TO DISCONTINUATION OF STUDY DRUG PER PROTOCOL DUE TO 2 RECURRENCES * Median time infants rec d study drug was 2.5 mos longer in acyclovir vs placebo groups (P=0.009) (4.1 mos longer if CNS; 1.7 mos longer if SEM)
17 NEURODEVELOPMENTAL OUTCOMES CASG 103 (CNS) 45 Acyclovir Placebo m 12 m Score = Score = P =.046* Bayley M-D scores ; 100 mean *Adjusted HC & Wt
18 NEURODEVELOPMENTAL OUTCOMES CASG Neurologic impairment CASG 103 Normal Mild Mod Severe Acyclovir 69% 6% 6% 19% Placebo 33% 8% 25% 33% Bayley scores incrementally higher w dur suppr Rx none =58, <6 mos = 70, 6 mos = 90 No significant differences in CASG 104 (SEM) in Bayley 12 months (8/15 acyclovir and 7/14 placebo recips studied) Neurologic outcome not different by HSV type
 Suppressive therapy is indicated 6 mos age (Acyclovir 300 mg/m 2 /dose tid PO) Follow up needed re neutropenia, recurrences and")
19 Bottom Lines Perinatal HSV, 2015 Can manifest nonspecifically as sepsis or less <21 days Plasma PCR should be included in diagnostic testing Treatment is acyclovir 20 mg/kg/dose q8h IV (SEM 2 weeks, CNS or Dissem 3 weeks) Suppressive therapy is indicated 6 mos age (Acyclovir 300 mg/m 2 /dose tid PO) Follow up needed re neutropenia, recurrences and outcome





20
 *CASG II Valganciclovir PO drug expose ganciclovir IV NEJM 2015;372:933 Study: *CASG III RDPCT Valganciclovir PO 6 wks vs 6 mos for sympt CMV 1")
21 Congenital CMV and Long Term Suppression Journal of Pediatrics 2003 JID 2011 *CASG I RDPCT of 6-wk ganciclovir IV for symptom CMV Showed benefit re best-ear 6 mos Waning 2 yrs? Probable improved neurodevelopmental outcome (poor F/U) *CASG II Valganciclovir PO drug expose ganciclovir IV NEJM 2015;372:933 Study: *CASG III RDPCT Valganciclovir PO 6 wks vs 6 mos for sympt CMV 1 o Outcome = Change best-ear hearing baseline 6 mos 2 o Outcomes = Change hearing baseline 12 & 24 mos Neurodevelopmental 12 & 24 mos
22 Findings 6 Weeks vs 6 Months Valganciclovir for ccmv 6-wk Therapy 6-mo Therapy 6 wks Hearing 24 mos Bayley 24 mos Best-ear 6 mos NS NS Total 12 mos* 57% 73% Total 24 mos 64% 77% Bayley 24 mos Superior ǂ Bayley 24 mos Superior ǂ Bayley cognitive & 24 mos Superior Grade 3-4 Neutropenia < 6 wks 19% 19% Grade 3-4 Neutropenia > 6 wk 6 mos 21% 27% Improved or still normal (one or both ears) P ǂ P
23
24 TREATMENT FOR SYMPTOMATIC CCMV Questions WHO INITIAL DRUG HOW LONG Comments and Suggestions Symptomatic ccmv infections Start treatment within first 4 weeks of life IV ganciclovir (6mg/kg/dose q 12hr Or PO valganciclovir (16mg/kg/dose q12hr Initial therapy 6 weeks Then consider PO valganciclovir (same dose, adj) to age 6 months? 1yr
25 CONGENITAL CMV TREATMENT DECISIONS Severe ccmv infections CNS ccmv infections Symptomatic ccmv infections YES YES YES Asymptomatic ccmv infections NO Treatment = until 6 months of age
26 MANAGEMENT CONSIDERATIONS Follow-up Infectious Diseases Ophthalmology Audiology Neurodevelopmental Evaluation Neurology Physical, Occupational, Speech Therapies Support for parents/caregivers Support for infant/child At least monthly while on treatment At least yearly until age 5 yrs Every 3-6 months until age 2-3 yrs Then yearly until age 7 yrs PMD at each visit Formal evaluation at 12 mos As needed depending on CNS involvement As appropriate, case-by-case Ongoing Ongoing community services Kadambari S, Williams EJ, Luck s, Griffiths PD, Sharland M. Evidence based management guidelines for the detection and treatment of congenital CMV. Early Human Develop. 2011;87:
27 Bottom Lines Congenital and Postnatal CMV, 2015 Definition of symptomatic ccmv for Rx is expanding Begin treatment of symptomatic ccmv early (<4 wks of age) Initial Rx ganciclovir IV vs valganciclovir PO should be discussed Suppressive Rx valganciclovir PO is indicated 6 mos of age Multispecialty follow up is required re Rx issues and outcomes We need to learn more about peri/postnatal CMV in preterm


 Odds ratio mortality @ 7 days, 30 days and discharge if delayed = 1.1 1.")
28 Nationwide Children s-associated Neo Services, CLABSI rate per 1000 catheter days for >5 years Each of 8 nurseries logged >1 year CLABSI free J Pediatr 2015;167:41 Yale-New Haven NICU, Of 410 episodes sepsis, 90% late onset Cases late-onset sepsis in latter years CoNS responsible 31% cases , none after 2011 J Pediatrr2015;166:1193 Duke University Ped Med Group 348 NICUs, CoNS BSI if >2 blood cultures positive <4 days cases in ~1 million infants 35% had delayed vancomycin (85% 1-2 day delay) Odds ratio 7 days, 30 days and discharge if delayed = (All 95% Cis <1 to <2) PIDJ 2015;34:371
PEDIATRIC INFECTIOUS DISEASES UPDATE. Neonatal HSV. Recognition, Diagnosis, and Management Coleen Cunningham MD
 Neonatal HSV Recognition, Diagnosis, and Management Coleen Cunningham MD Important questions Who is at risk? When do you test? What tests do you perform? When do you treat? What is appropriate therapy?
Neonatal HSV Recognition, Diagnosis, and Management Coleen Cunningham MD Important questions Who is at risk? When do you test? What tests do you perform? When do you treat? What is appropriate therapy?
CONGENITAL CMV INFECTION
 CONGENITAL CMV INFECTION Pablo J. Sánchez, MD 20 th International Symposium on Neonatology.... São Paolo, Brazil 9/10-12/15 HUMAN CYTOMEGALOVIRUS DNA virus; herpesvirus family; 1881 (Ribbert) Infected
CONGENITAL CMV INFECTION Pablo J. Sánchez, MD 20 th International Symposium on Neonatology.... São Paolo, Brazil 9/10-12/15 HUMAN CYTOMEGALOVIRUS DNA virus; herpesvirus family; 1881 (Ribbert) Infected
CMV: perinatal management of infected neonates
 CMV: perinatal management of infected neonates ccmv Epidemiology The prevalence of ccmv in developed countries is 04 0 0.4 0.8% In the UK, symptomatic congenital infection was estimated to be 3/1000 in
CMV: perinatal management of infected neonates ccmv Epidemiology The prevalence of ccmv in developed countries is 04 0 0.4 0.8% In the UK, symptomatic congenital infection was estimated to be 3/1000 in
Long-Term Hearing Outcomes of Symptomatic Congenital CMV Infected Children Treated with Valganciclovir
 Long-Term Hearing Outcomes of Symptomatic Congenital CMV Infected Children Treated with Valganciclovir Hilary McCrary MD MPH, Xiaoming Sheng PhD, Tom Greene PhD, Albert Park MD University of Utah Disclosures:
Long-Term Hearing Outcomes of Symptomatic Congenital CMV Infected Children Treated with Valganciclovir Hilary McCrary MD MPH, Xiaoming Sheng PhD, Tom Greene PhD, Albert Park MD University of Utah Disclosures:
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants
 Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
Neonatal HSV SARA SAPORTA-KEATING 3/1/17
 Neonatal HSV SARA SAPORTA-KEATING 3/1/17 Pt Sx onset Presentation Clinical Presentation HSV risk factor(s) HSV results CSF WBC 1 DOL 7 DOL 8 Vesicular rash FOC with active cold sore (DOL2), C/S 2 DOL 7
Neonatal HSV SARA SAPORTA-KEATING 3/1/17 Pt Sx onset Presentation Clinical Presentation HSV risk factor(s) HSV results CSF WBC 1 DOL 7 DOL 8 Vesicular rash FOC with active cold sore (DOL2), C/S 2 DOL 7
Kidz Medical Services Infant Exposed to Genital Herpes Simplex Virus
 Kidz Medical Services Infant Exposed to Genital Herpes Simplex Virus Guideline: HSV Guideline: I. Herpes Simplex Virus (HSV): A. HSV is an enveloped, double-stranded DNA virus that enters the body via
Kidz Medical Services Infant Exposed to Genital Herpes Simplex Virus Guideline: HSV Guideline: I. Herpes Simplex Virus (HSV): A. HSV is an enveloped, double-stranded DNA virus that enters the body via
Wales Neonatal Network Guideline
 Guideline for the Management of Neonatal Herpes Infection Introduction: Herpes simplex virus type 1 and 2 are DNA viruses that belong to Alphaherpesviridae, a subfamily of the Herpesviridae family. Both
Guideline for the Management of Neonatal Herpes Infection Introduction: Herpes simplex virus type 1 and 2 are DNA viruses that belong to Alphaherpesviridae, a subfamily of the Herpesviridae family. Both
Congenital/Neonatal Herpes Simplex Infections
 Congenital/Neonatal Herpes Simplex Infections Infectious and Tropical Pediatric Division Department of Child Health Medical Faculty University of Sumatera Utara Herpes Infections Herpes from the Greek
Congenital/Neonatal Herpes Simplex Infections Infectious and Tropical Pediatric Division Department of Child Health Medical Faculty University of Sumatera Utara Herpes Infections Herpes from the Greek
11/9/2012. Group B Streptococcal Infections: Consensus and Controversies. Prevention of Early-Onset GBS Disease in the USA.
 Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Fever in neonates (age 0 to 28 days)
") Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
ESCMID Postgraduate Education Course Infectious Diseases in Pregnant Women, Fetuses and Newborns Bertinoro, Italy 3 7 October 2010
 ESCMID Postgraduate Education Course Infectious Diseases in Pregnant Women, Fetuses and Newborns Bertinoro, Italy 3 7 October 2010 Robert Pass University of Alabama at Birmingham School of Medicine Disclosures:
ESCMID Postgraduate Education Course Infectious Diseases in Pregnant Women, Fetuses and Newborns Bertinoro, Italy 3 7 October 2010 Robert Pass University of Alabama at Birmingham School of Medicine Disclosures:
Diagnosis and Treatment of Neurological Disease from Herpesvirus infection in Neonates and Children Cheryl Jones The Children s s Hospital at
 Diagnosis and Treatment of Neurological Disease from Herpesvirus infection in Neonates and Children Cheryl Jones The Children s s Hospital at Westmead, NSW University of Sydney Overview Members of herpesvirus
Diagnosis and Treatment of Neurological Disease from Herpesvirus infection in Neonates and Children Cheryl Jones The Children s s Hospital at Westmead, NSW University of Sydney Overview Members of herpesvirus
Outline. The Scarlet H : Neonatal herpes simplex virus infection in the 21 st century. Ancient History. Ancient History. History.
 The Scarlet H : Neonatal herpes simplex virus infection in the 21 st century J.B. Cantey, MD Pediatric Grand Rounds University of Texas Health San Antonio September 15, 2017 Outline Historical perspectives
The Scarlet H : Neonatal herpes simplex virus infection in the 21 st century J.B. Cantey, MD Pediatric Grand Rounds University of Texas Health San Antonio September 15, 2017 Outline Historical perspectives
Congenital CMV infection. Infectious and Tropical Pediatric Division Department of Child Health Medical Faculty, University of Sumatera Utara
 Congenital CMV infection Infectious and Tropical Pediatric Division Department of Child Health Medical Faculty, University of Sumatera Utara Congenital CMV infection Approximately 0.15 2% of live births
Congenital CMV infection Infectious and Tropical Pediatric Division Department of Child Health Medical Faculty, University of Sumatera Utara Congenital CMV infection Approximately 0.15 2% of live births
Sample Selection- Vignettes
 Sample Selection- Vignettes Rangaraj Selvarangan, BVSc, PhD, D(ABMM) Professor, UMKC School of Medicine Director, Microbiology, Virology and Molecular Infectious Diseases Laboratory Director, Laboratory
Sample Selection- Vignettes Rangaraj Selvarangan, BVSc, PhD, D(ABMM) Professor, UMKC School of Medicine Director, Microbiology, Virology and Molecular Infectious Diseases Laboratory Director, Laboratory
1. Introduction Algorithm: Infant with Fever 0-28 Days Algorithm: Infant with Fever Days...3
 These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
HSV Screening: Are Wesley Obstetricians Following the Guidelines? Dawn Boender, PGY4 Taylor Bertschy, PGY3
 HSV Screening: Are Wesley Obstetricians Following the Guidelines? Dawn Boender, PGY4 Taylor Bertschy, PGY3 Goals To increase obstetrician knowledge regarding HSV screening Institute clinical changes at
HSV Screening: Are Wesley Obstetricians Following the Guidelines? Dawn Boender, PGY4 Taylor Bertschy, PGY3 Goals To increase obstetrician knowledge regarding HSV screening Institute clinical changes at
Rebecca T Slagle, MN, APRN, NNP-BC. Speak up!!
 Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Rational Evaluation of the Febrile Infant
 Disclosures Rational Evaluation of the Febrile Infant Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending
Disclosures Rational Evaluation of the Febrile Infant Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending
C M V a n d t h e N e o n a t e D r M e g P r a d o N e o n a t o l o g i s t D i r e c t o r, N I C U, S t F r a n c i s M e d i c a l C e n t e r
 C M V a n d t h e N e o n a t e D r M e g P r a d o N e o n a t o l o g i s t D i r e c t o r, N I C U, S t F r a n c i s M e d i c a l C e n t e r C M V S e r o - P r e v a l e n c e ( I g G p o s i t
C M V a n d t h e N e o n a t e D r M e g P r a d o N e o n a t o l o g i s t D i r e c t o r, N I C U, S t F r a n c i s M e d i c a l C e n t e r C M V S e r o - P r e v a l e n c e ( I g G p o s i t
Herpesvirus infections in pregnancy
 Herpesvirus infections in pregnancy Dr. med. Daniela Huzly Institute of Virology University Medical Center Freiburg, Germany Herpes simplex virus 1+2 Risk in pregnancy and at birth Primary infection in
Herpesvirus infections in pregnancy Dr. med. Daniela Huzly Institute of Virology University Medical Center Freiburg, Germany Herpes simplex virus 1+2 Risk in pregnancy and at birth Primary infection in
Learning Objectives. At the conclusion of this module, participants should be better able to:
 Learning Objectives At the conclusion of this module, participants should be better able to: Treat asymptomatic neonatal hypoglycemia with buccal dextrose gel Develop patient-specific approaches to intravenous
Learning Objectives At the conclusion of this module, participants should be better able to: Treat asymptomatic neonatal hypoglycemia with buccal dextrose gel Develop patient-specific approaches to intravenous
Herpes Simplex Viruses: Disease Burden. Richard Whitley The University of Alabama at Birmingham Herpes Virus Infection and Immunity June 18-20, 2012
 Herpes Simplex Viruses: Disease Burden Richard Whitley The University of Alabama at Birmingham Herpes Virus Infection and Immunity June 18-20, 2012 Mucocutaneous HSV Infections Life-Threatening HSV Diseases
Herpes Simplex Viruses: Disease Burden Richard Whitley The University of Alabama at Birmingham Herpes Virus Infection and Immunity June 18-20, 2012 Mucocutaneous HSV Infections Life-Threatening HSV Diseases
One View of STEROIDS Who is this? EBV/Mono. Infections With Possible Steroid Rx STEROID USE IN PEDIATRIC INFECTION. EBV TB Meningitis Septic Arthritis
 One View of STEROIDS Who is this? STEROID USE IN PEDIATRIC INFECTION Peggy Weintrub Infections With Possible Steroid Rx EBV/Mono EBV TB Meningitis Septic Arthritis Who painted this young woman with mono?
One View of STEROIDS Who is this? STEROID USE IN PEDIATRIC INFECTION Peggy Weintrub Infections With Possible Steroid Rx EBV/Mono EBV TB Meningitis Septic Arthritis Who painted this young woman with mono?
Neonatal sepsis INCIDENCE RISK FACTORS RISK FACTORS 5/18/2015
 Angelica Floren MD.FAAP. Caring for Little Miracles 6 Th Annual Care Of the Sick Newborn Conference Neonatal sepsis Neonatal sepsis is a disease that may start with minimal or nonspecific symptoms and
Angelica Floren MD.FAAP. Caring for Little Miracles 6 Th Annual Care Of the Sick Newborn Conference Neonatal sepsis Neonatal sepsis is a disease that may start with minimal or nonspecific symptoms and
Neurodevelopmental Risk?
 Normal Newborn During transitional hypoglycemia normal newborns have an enhanced ketogenic response to fasting. Newborn brains have enhanced capability to use ketone bodies for fuel Allows newborns to
Normal Newborn During transitional hypoglycemia normal newborns have an enhanced ketogenic response to fasting. Newborn brains have enhanced capability to use ketone bodies for fuel Allows newborns to
What is symptomatic? Neonatal hypoglycemia: how low can you go? Hypoglycemia and MRI. Conflicts. What s the problem? Hypoglycemia and MRI
 Neonatal hypoglycemia: how low can you go? Kristi Watterberg, MD Professor of Pediatrics, UNM What is symptomatic? Jitteriness Cyanosis Poor feeding Weak, high-pitched cry Seizures Apnea Lethargy, low
Neonatal hypoglycemia: how low can you go? Kristi Watterberg, MD Professor of Pediatrics, UNM What is symptomatic? Jitteriness Cyanosis Poor feeding Weak, high-pitched cry Seizures Apnea Lethargy, low
Optimization of Antibiotics Practices by Applying Antibiotic Stewardship Principles. Joel Weiner, MD September 12, 2014
 Optimization of Antibiotics Practices by Applying Antibiotic Stewardship Principles Joel Weiner, MD September 12, 2014 O Nothing to disclose Disclosure Reducing Initial Antibiotic Exposure in Selected
Optimization of Antibiotics Practices by Applying Antibiotic Stewardship Principles Joel Weiner, MD September 12, 2014 O Nothing to disclose Disclosure Reducing Initial Antibiotic Exposure in Selected
GENITAL HERPES. 81.1% of HSV-2 infections are asymptomatic or unrecognized. Figure 14 HSV-2 seroprevalence among persons aged years by sex.
 GENITAL HERPES Genital herpes is a chronic, lifelong, sexually transmitted disease caused by herpes simplex virus type 1 (HSV-1) and type 2 (HSV-2). HSV-1 typically causes small, painful, fluid-filled,
GENITAL HERPES Genital herpes is a chronic, lifelong, sexually transmitted disease caused by herpes simplex virus type 1 (HSV-1) and type 2 (HSV-2). HSV-1 typically causes small, painful, fluid-filled,
The Role of Cytomegalovirus Evaluation in Pediatric Hearing Loss. Albert Park, MD Dept. Surgery and Pediatrics University of Utah
 The Role of Cytomegalovirus Evaluation in Pediatric Hearing Loss Albert Park, MD Dept. Surgery and Pediatrics University of Utah Nondisclosure: Triological Career Development Awardmurine model of CMV induced
The Role of Cytomegalovirus Evaluation in Pediatric Hearing Loss Albert Park, MD Dept. Surgery and Pediatrics University of Utah Nondisclosure: Triological Career Development Awardmurine model of CMV induced
Evidence-based Management of Fever in Infants and Young Children
 Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Use of a Multidisciplinary Care Model for Pregnant Women Living with HIV & Their Infants Sarah McBeth, MD MPH
 Use of a Multidisciplinary Care Model for Pregnant Women Living with HIV & Their Infants Sarah McBeth, MD MPH University of Pittsburgh Medical Center Disclosures Presenter has no financial interests to
Use of a Multidisciplinary Care Model for Pregnant Women Living with HIV & Their Infants Sarah McBeth, MD MPH University of Pittsburgh Medical Center Disclosures Presenter has no financial interests to
Fevers and Seizures in Infants and Young Children
 Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Screening for Congenital CMV Infection
 London s Global University Screening for Congenital CMV Infection Venice April 25 2016 Paul D Griffiths MD DSc FRCPath Professor of Virology UCL Institute of Immunity and Transplantation Overview Definition
London s Global University Screening for Congenital CMV Infection Venice April 25 2016 Paul D Griffiths MD DSc FRCPath Professor of Virology UCL Institute of Immunity and Transplantation Overview Definition
Best Practices for Infection Prevention and Control in Perinatology In All Health Care Settings that Provide Obstetrical and Newborn Care, PIDAC 2012
 Best Practices for Infection Prevention and Control in Perinatology In All Health Care Settings that Provide Obstetrical and Newborn Care, PIDAC 2012 Perinatal Infections Mary Vearncombe, MD, FRCPC Chair,
Best Practices for Infection Prevention and Control in Perinatology In All Health Care Settings that Provide Obstetrical and Newborn Care, PIDAC 2012 Perinatal Infections Mary Vearncombe, MD, FRCPC Chair,
+ Objectives. n Define who is at risk for SBI. n Clarify risk stratification. n Provide treatment guidelines. n Bust some myths
 Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Expert opinion on clinical symptoms, management and treatment of infants with congenital cytomegalovirus infection
 Expert opinion on clinical symptoms, management and treatment of infants with congenital cytomegalovirus infection J. Gunkel, J. Nijman, M.A. Maciolek-Verboon, T.F.W. Wolfs, L.S. de Vries Financial disclosure
Expert opinion on clinical symptoms, management and treatment of infants with congenital cytomegalovirus infection J. Gunkel, J. Nijman, M.A. Maciolek-Verboon, T.F.W. Wolfs, L.S. de Vries Financial disclosure
Pertussis: Trends, Prevention and Challenges Flor M. Munoz, MD Associate Professor Pediatric Infectious Diseases
 Pertussis: Trends, Prevention and Challenges Flor M. Munoz, MD Associate Professor Pediatric Infectious Diseases Disclosure I do not have any relevant conflicts of interest to disclose. Page 1 xxx00.#####.ppt
Pertussis: Trends, Prevention and Challenges Flor M. Munoz, MD Associate Professor Pediatric Infectious Diseases Disclosure I do not have any relevant conflicts of interest to disclose. Page 1 xxx00.#####.ppt
Zika Virus. Robert Wittler, MD
 Zika Virus Robert Wittler, MD Disclosure I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this CME
Zika Virus Robert Wittler, MD Disclosure I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this CME
Zika Virus. Disclosure. Zika Virus 8/26/2016
 Zika Virus Robert Wittler, MD Disclosure I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this CME
Zika Virus Robert Wittler, MD Disclosure I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this CME
The Febrile Infant. SJRH ED Rounds Dec By: Robin Clouston
 1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
Neonatal Sepsis. Neonatal sepsis ehandbook
 Neonatal Sepsis Neonatal sepsis ehandbook Sepsis Any baby who is unwell must be considered at risk of sepsis 1 in 8 per 1000 lives births The consequences of untreated sepsis are devastating - 10-30% risk
Neonatal Sepsis Neonatal sepsis ehandbook Sepsis Any baby who is unwell must be considered at risk of sepsis 1 in 8 per 1000 lives births The consequences of untreated sepsis are devastating - 10-30% risk
Intrapartum and Postpartum Management of the Diabetic Mother and Infant
 Intrapartum and Postpartum Management of the Diabetic Mother and Infant Intrapartum Management Women with gestational diabetes who maintain normal glucose levels during pregnancy on diet and exercise therapy
Intrapartum and Postpartum Management of the Diabetic Mother and Infant Intrapartum Management Women with gestational diabetes who maintain normal glucose levels during pregnancy on diet and exercise therapy
PEDIATRIC NEWBORN MEDICINE CLINICAL PRACTICE GUIDELINES. Cytomegalovirus (CMV) Screening Protocol
 Screening Protocol") Clinical Guideline Name Cytomegalovirus (CMV) Screening Protocol Effective Date January 2017 Approved By Department of Pediatric Newborn Medicine Clinical Practice Council_12/8/16_ CWN PPG 12/14/16 BWH
Clinical Guideline Name Cytomegalovirus (CMV) Screening Protocol Effective Date January 2017 Approved By Department of Pediatric Newborn Medicine Clinical Practice Council_12/8/16_ CWN PPG 12/14/16 BWH
CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA. Date
 CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA 350 300 250 Number 200 150 100 50 0 1/01/1997 1/01/1998 1/01/1999 1/01/2000 31/12/2000 31/12/2001 31/12/2002 Date July 2004 Reported number of perinatally exposed
CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA 350 300 250 Number 200 150 100 50 0 1/01/1997 1/01/1998 1/01/1999 1/01/2000 31/12/2000 31/12/2001 31/12/2002 Date July 2004 Reported number of perinatally exposed
Group B Streptococcus
 Group B Streptococcus (Invasive Disease) Infants Younger than 90 Days Old DISEASE REPORTABLE WITHIN 24 HOURS OF DIAGNOSIS Per N.J.A.C. 8:57, healthcare providers and administrators shall report by mail
Group B Streptococcus (Invasive Disease) Infants Younger than 90 Days Old DISEASE REPORTABLE WITHIN 24 HOURS OF DIAGNOSIS Per N.J.A.C. 8:57, healthcare providers and administrators shall report by mail
ZIKA Jordan H. Perlow MD Banner University Medical Center Division of Maternal Fetal Medicine Phoenix Perinatal Asoociates
 ZIKA Jordan H. Perlow MD Banner University Medical Center Division of Maternal Fetal Medicine Phoenix Perinatal Asoociates Disclosures I have no relevant financial relationships to disclose or conflicts
ZIKA Jordan H. Perlow MD Banner University Medical Center Division of Maternal Fetal Medicine Phoenix Perinatal Asoociates Disclosures I have no relevant financial relationships to disclose or conflicts
Fever in the Newborn Period
 Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Diagnostic Value of C - Reactive Protein and Other Hematological Parameters in Neonatal Sepsis
 Diagnostic Value of C - Reactive Protein and Other Hematological Parameters in Neonatal Sepsis Hafadh Jaleel Hussein*, Yusra Fayyadh Alwan** ABSTRACT: BACKGROUND: There have been many attempts to develop
Diagnostic Value of C - Reactive Protein and Other Hematological Parameters in Neonatal Sepsis Hafadh Jaleel Hussein*, Yusra Fayyadh Alwan** ABSTRACT: BACKGROUND: There have been many attempts to develop
Congenital Zika Virus. Rebecca E. Levorson, MD Pediatric Infectious Diseases Pediatric Specialists of Virginia November 4, 2017
 Congenital Zika Virus Rebecca E. Levorson, MD Pediatric Infectious Diseases Pediatric Specialists of Virginia November 4, 2017 Objectives 1. Understand Congenital Zika Virus and why evaluating for congenital
Congenital Zika Virus Rebecca E. Levorson, MD Pediatric Infectious Diseases Pediatric Specialists of Virginia November 4, 2017 Objectives 1. Understand Congenital Zika Virus and why evaluating for congenital
MCARTOR SYMPOSIUM SUMMARY By Maria-Cristina Javier, MD Medical Director of Education
 MCARTOR SYMPOSIUM SUMMARY By Maria-Cristina Javier, MD Medical Director of Education LAURA E. RILEY, MD MATERNAL INFECTIONS AND THEIR LIFELONG CONSEQUENCES TO THE FETUS FEVER IN LABOR: WHAT DOES THAT MEAN
MCARTOR SYMPOSIUM SUMMARY By Maria-Cristina Javier, MD Medical Director of Education LAURA E. RILEY, MD MATERNAL INFECTIONS AND THEIR LIFELONG CONSEQUENCES TO THE FETUS FEVER IN LABOR: WHAT DOES THAT MEAN
Standard of Newborn Care in the Age of Birth Plans. Stephanie Deal, MD Tiffany McKee-Garrett, MD
 Standard of Newborn Care in the Age of Birth Plans Stephanie Deal, MD Tiffany McKee-Garrett, MD Disclosure We have no relevant financial relationships with the manufacturers(s) of any commercial products(s)
Standard of Newborn Care in the Age of Birth Plans Stephanie Deal, MD Tiffany McKee-Garrett, MD Disclosure We have no relevant financial relationships with the manufacturers(s) of any commercial products(s)
Neonatal infections. Joanna Seliga-Siwecka
 Neonatal infections Joanna Seliga-Siwecka Neonatal infections Early onset sepsis Late onset sepsis TORCH Early onset sepsis (EOS) Blood or cerebral fluid culture-proven infection at fewer than 7 days
Neonatal infections Joanna Seliga-Siwecka Neonatal infections Early onset sepsis Late onset sepsis TORCH Early onset sepsis (EOS) Blood or cerebral fluid culture-proven infection at fewer than 7 days
Summary of Changes: References/content updated to reflect most current standards of practice.
 Alaska Native Medical Center: Mother Baby Unit Guideline: Neonatal Hypoglycemia Subject: Neonatal Hypoglycemia REVISION DATE: Jan 2015,12/2011, 02/2009, 11, 2007, 07/2007,04/2001, 04/1999 REPLACES: NSY:
Alaska Native Medical Center: Mother Baby Unit Guideline: Neonatal Hypoglycemia Subject: Neonatal Hypoglycemia REVISION DATE: Jan 2015,12/2011, 02/2009, 11, 2007, 07/2007,04/2001, 04/1999 REPLACES: NSY:
The Ever-Changing Approaches to Diabetes in Pregnancy
 The Ever-Changing Approaches to Diabetes in Pregnancy Kirsten E. Salmeen, MD Assistant Professor Obstetrics, Gynecology & Reproductive Sciences Maternal-Fetal Medicine I have nothing to disclose. Approaches
The Ever-Changing Approaches to Diabetes in Pregnancy Kirsten E. Salmeen, MD Assistant Professor Obstetrics, Gynecology & Reproductive Sciences Maternal-Fetal Medicine I have nothing to disclose. Approaches
Acyclovir dose for meningitis
 P ford residence southampton, ny Acyclovir dose for meningitis Aciclovir (ACV), also known as acyclovir, is an antiviral medication. It is primarily used for the treatment of herpes simplex virus infections,
P ford residence southampton, ny Acyclovir dose for meningitis Aciclovir (ACV), also known as acyclovir, is an antiviral medication. It is primarily used for the treatment of herpes simplex virus infections,
Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants
 Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants Ajou University School of Medicine Department of Pediatrics Moon Sung Park M.D. Hee Cheol Jo, M.D., Jang Hoon Lee,
Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants Ajou University School of Medicine Department of Pediatrics Moon Sung Park M.D. Hee Cheol Jo, M.D., Jang Hoon Lee,
Acyclovir suppression to prevent clinical recurrences at delivery after first episode genital herpes in pregnancy: an open-label trial
 Infect Dis Obstet Gynecol 2001;9:75 80 Acyclovir suppression to prevent clinical recurrences at delivery after first episode genital herpes in pregnancy: an open-label trial L. Laurie Scott 1, Lisa M.
Infect Dis Obstet Gynecol 2001;9:75 80 Acyclovir suppression to prevent clinical recurrences at delivery after first episode genital herpes in pregnancy: an open-label trial L. Laurie Scott 1, Lisa M.
Disclosures. Background. Definitions. Why Worry about these Infants? Goals. Bacterial infection in the neonate and young infant: a review
 Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
CCC ARV Dosing Recommendations for HIV-exposed infants Updated
 USERS NOTE: Please note this document does not provide guidance on overall decisionmaking regarding what medication(s) to use for HIV-exposed infants. This document is meant to facilitate ARV dosing for
USERS NOTE: Please note this document does not provide guidance on overall decisionmaking regarding what medication(s) to use for HIV-exposed infants. This document is meant to facilitate ARV dosing for
Prematurity as a Risk Factor for ASD. Disclaimer
 Prematurity as a Risk Factor for ASD Angela M. Montgomery, MD, MSEd Assistant Professor of Pediatrics (Neonatology) Director, Yale NICU GRAD Program Suzanne L. Macari, PhD Research Scientist, Child Study
Prematurity as a Risk Factor for ASD Angela M. Montgomery, MD, MSEd Assistant Professor of Pediatrics (Neonatology) Director, Yale NICU GRAD Program Suzanne L. Macari, PhD Research Scientist, Child Study
Faculty Disclosure. Stephen I. Pelton, MD. Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/22368 holds various files of this Leiden University dissertation Author: Lugt, Neeltje Margaretha van der Title: Neonatal pearls : safety and efficacy of
Cover Page The handle http://hdl.handle.net/1887/22368 holds various files of this Leiden University dissertation Author: Lugt, Neeltje Margaretha van der Title: Neonatal pearls : safety and efficacy of
Pediatric Potpourri: What do we now?
 Pediatric Potpourri: What do we now? April 19, 2013 Robert Wittler, MD 1 Disclosure I have no relevant financial relationships with the manufacturer(s) of any commercial products(s) and/or provider of
Pediatric Potpourri: What do we now? April 19, 2013 Robert Wittler, MD 1 Disclosure I have no relevant financial relationships with the manufacturer(s) of any commercial products(s) and/or provider of
Mrs Kate Johnston, Mr Phil Lindsey, Mrs Charlotte Wilson Dr Marieke Emonts, Mrs Ailsa Pickering. Newcastle upon Tyne Hospitals NHS Foundation Trust
 'Testing for congenital cytomegalovirus (CMV) in babies identified with permanent childhood hearing impairment (PCHI) through the newborn hearing screening programme (NHSP) Mrs Kate Johnston, Mr Phil Lindsey,
'Testing for congenital cytomegalovirus (CMV) in babies identified with permanent childhood hearing impairment (PCHI) through the newborn hearing screening programme (NHSP) Mrs Kate Johnston, Mr Phil Lindsey,
Wales Neonatal Network Guideline
 Congenital infection: Diagnosis and management Overview: Infections transmitted and acquired in utero. Most as a result of primary infection of mother during pregnancy, some organisms such as Cytomegalovirus
Congenital infection: Diagnosis and management Overview: Infections transmitted and acquired in utero. Most as a result of primary infection of mother during pregnancy, some organisms such as Cytomegalovirus
Acyclovir prophylaxis for pregnant women with a known history of herpes simplex virus: a cost-effectiveness analysis Little S E, Caughey A B
 Acyclovir prophylaxis for pregnant women with a known history of herpes simplex virus: a cost-effectiveness analysis Little S E, Caughey A B Record Status This is a critical abstract of an economic evaluation
Acyclovir prophylaxis for pregnant women with a known history of herpes simplex virus: a cost-effectiveness analysis Little S E, Caughey A B Record Status This is a critical abstract of an economic evaluation
Christine Yoshinaga-Itano, Ph.D. Professor University of Colorado, Boulder Department of Speech, Language & Hearing Sciences Allison Sedey, Ph.D.
 Christine Yoshinaga-Itano, Ph.D. Professor University of Colorado, Boulder Department of Speech, Language & Hearing Sciences Allison Sedey, Ph.D. Rosalinda Baca, Ph.D. Molly Dalpes, AuD Kristin Uhler,
Christine Yoshinaga-Itano, Ph.D. Professor University of Colorado, Boulder Department of Speech, Language & Hearing Sciences Allison Sedey, Ph.D. Rosalinda Baca, Ph.D. Molly Dalpes, AuD Kristin Uhler,
Congenital Cytomegalovirus (CMV)
") August 2011 Congenital Cytomegalovirus (CMV) Revision Dates Case Definition Reporting Requirements Remainder of the Guideline (i.e., Etiology to References sections inclusive) August 2011 August 2011 June
August 2011 Congenital Cytomegalovirus (CMV) Revision Dates Case Definition Reporting Requirements Remainder of the Guideline (i.e., Etiology to References sections inclusive) August 2011 August 2011 June
MATERNAL VACCINATION. Dr Sushena Krishnaswamy
 MATERNAL VACCINATION Dr Sushena Krishnaswamy CVU November 2017 Outline 1. Principles 2. Flu- infant benefit 3. Pertussis- optimal timing, cocooning 4. How we re faring 5. Strategies to improve uptake 6.
MATERNAL VACCINATION Dr Sushena Krishnaswamy CVU November 2017 Outline 1. Principles 2. Flu- infant benefit 3. Pertussis- optimal timing, cocooning 4. How we re faring 5. Strategies to improve uptake 6.
greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
 1 Use the Yale Observation Scale to assess whether the patient is ill or well appearing. A score greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
1 Use the Yale Observation Scale to assess whether the patient is ill or well appearing. A score greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
Insults to the Developing Brain & Effect on Neurodevelopmental Outcomes
 Insults to the Developing Brain & Effect on Neurodevelopmental Outcomes Ira Adams-Chapman, MD Assistant Professor of Pediatrics Director, Developmental Progress Clinic Emory University School of Medicine
Insults to the Developing Brain & Effect on Neurodevelopmental Outcomes Ira Adams-Chapman, MD Assistant Professor of Pediatrics Director, Developmental Progress Clinic Emory University School of Medicine
Acyclovir suppression to prevent recurrent genital herpes at delivery
 Infect Dis Obstet Gynecol 2002;10:71 77 Acyclovir suppression to prevent recurrent genital herpes at delivery L. L. Scott 1, L. M. Hollier 1, D. McIntire 1, P. J. Sanchez 2, G. L. Jackson 2 and G. D. Wendel,
Infect Dis Obstet Gynecol 2002;10:71 77 Acyclovir suppression to prevent recurrent genital herpes at delivery L. L. Scott 1, L. M. Hollier 1, D. McIntire 1, P. J. Sanchez 2, G. L. Jackson 2 and G. D. Wendel,
EPG Clinical Guidelines
 Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Congenital Cytomegalovirus: A Pilot Study
 Congenital Cytomegalovirus: A Pilot Study Maggie Dreon Mark Schleiss, Sheila Dollard, Tatiana Lanzieri, Nelmary Hernandez-Alvarado, Carrie Wolf, Kirsten Coverstone, Ruth Lynfield, Mark McCann Special Thanks
Congenital Cytomegalovirus: A Pilot Study Maggie Dreon Mark Schleiss, Sheila Dollard, Tatiana Lanzieri, Nelmary Hernandez-Alvarado, Carrie Wolf, Kirsten Coverstone, Ruth Lynfield, Mark McCann Special Thanks
The Healthcare Cost of Symptomatic Congenital CMV Disease in Privately Insured US Children: Estimates from Administrative Claims Data
 National Center on Birth Defects and Developmental Disabilities The Healthcare Cost of Symptomatic Congenital CMV Disease in Privately Insured US Children: Estimates from Administrative Claims Data Scott
National Center on Birth Defects and Developmental Disabilities The Healthcare Cost of Symptomatic Congenital CMV Disease in Privately Insured US Children: Estimates from Administrative Claims Data Scott
Extensive cystic periventricular leukomalacia following early-onset group B streptococcal sepsis in a very low birth weight infant
 SWISS SOCIETY OF NEONATOLOGY Extensive cystic periventricular leukomalacia following early-onset group B streptococcal sepsis in a very low birth weight infant July 2012 2 Berger TM, Caduff JC, Neonatal
SWISS SOCIETY OF NEONATOLOGY Extensive cystic periventricular leukomalacia following early-onset group B streptococcal sepsis in a very low birth weight infant July 2012 2 Berger TM, Caduff JC, Neonatal
Maternal-fetal Opiate Medical Home (MOMH) Jocelyn Davis DNP,CNM, RN, CEFMM Karen Frantz BSN, RNC
 Jocelyn Davis DNP,CNM, RN, CEFMM Karen Frantz BSN, RNC") Maternal-fetal Opiate Medical Home (MOMH) Jocelyn Davis DNP,CNM, RN, CEFMM Karen Frantz BSN, RNC Objectives 1. Discuss the effects of opiate addiction on mothers and infants. 2. Discuss a Medical Home
Maternal-fetal Opiate Medical Home (MOMH) Jocelyn Davis DNP,CNM, RN, CEFMM Karen Frantz BSN, RNC Objectives 1. Discuss the effects of opiate addiction on mothers and infants. 2. Discuss a Medical Home
HYPERIMMUNOGLOBULIN and CMV- DNAemia IN PREGNANT WOMEN WITH PRIMARY CYTOMEGALOVIRUS INFECTION
 HYPERIMMUNOGLOBULIN and CMV- DNAemia IN PREGNANT WOMEN WITH PRIMARY CYTOMEGALOVIRUS INFECTION Giovanni Nigro, Rome, Italy Stuart P Adler, Richmond, VA, USA To avoid fetal rejection (50% allograft) an estrogeninduced
HYPERIMMUNOGLOBULIN and CMV- DNAemia IN PREGNANT WOMEN WITH PRIMARY CYTOMEGALOVIRUS INFECTION Giovanni Nigro, Rome, Italy Stuart P Adler, Richmond, VA, USA To avoid fetal rejection (50% allograft) an estrogeninduced
Objectives. Apnea Definition and Pitfalls. Pathophysiology of Apnea. Apnea of Prematurity and hypoxemia episodes 5/18/2015
 Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Language Abilities of Infants Born Preterm to Mothers With Diabetes
 Language Abilities of Infants Born Preterm to Mothers With Diabetes Diane Frome Loeb a, Caitlin Imgrund a, & Steven M. Barlow b a The University of Kansas b The University of Nebraska-Lincoln Disclosure:
Language Abilities of Infants Born Preterm to Mothers With Diabetes Diane Frome Loeb a, Caitlin Imgrund a, & Steven M. Barlow b a The University of Kansas b The University of Nebraska-Lincoln Disclosure:
Disclosures. CMV and EBV Infection in Pediatric Transplantation. Goals. Common Aspects CMV (Cytomegalovirus) and EBV (Epstein-Barr virus)
 and EBV (Epstein-Barr virus)") Disclosures I have financial relationships with the following companies: CMV and EBV Infection in Pediatric Transplantation Elekta Inc Lucence Diagnostics Spouse employed Spouse employed I will not discuss
Disclosures I have financial relationships with the following companies: CMV and EBV Infection in Pediatric Transplantation Elekta Inc Lucence Diagnostics Spouse employed Spouse employed I will not discuss
Objectives. Birth Depression Management. Birth Depression Terms
 Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Controversies in Neonatal Hypoglycemia PAC / LAC CONFERENCE, JUNE 1 ST 2017
 Controversies in Neonatal Hypoglycemia PRIYA JEGATHEESAN, MD PAC / LAC CONFERENCE, JUNE 1 ST 2017 Disclosure I have no conflicts of interest to disclose Objectives Review Recommendations from different
Controversies in Neonatal Hypoglycemia PRIYA JEGATHEESAN, MD PAC / LAC CONFERENCE, JUNE 1 ST 2017 Disclosure I have no conflicts of interest to disclose Objectives Review Recommendations from different
Hot Hot Tot:! The Hot Tot. Fever in KIds <90 Days 5/26/10
 Hot Hot Tot:! Fever in KIds
Hot Hot Tot:! Fever in KIds
No conflict of interest to report
 Ultrasound Findings in Fetal Infection No conflict of interest to report Kim A. Boggess MD Ob Gyn UNC at Chapel Hill Learning Objectives At conclusion, participants will Identify maternal infections that
Ultrasound Findings in Fetal Infection No conflict of interest to report Kim A. Boggess MD Ob Gyn UNC at Chapel Hill Learning Objectives At conclusion, participants will Identify maternal infections that
Rango de saturacion de oxigeno: Cual es la evidencia?
 Rango de saturacion de oxigeno: Cual es la evidencia? Wally Carlo, M.D. University of Alabama at Birmingham Department of Pediatrics Division of Neonatology wcarlo@peds.uab.edu 1 2 Stevie Wonder 4 Objectives
Rango de saturacion de oxigeno: Cual es la evidencia? Wally Carlo, M.D. University of Alabama at Birmingham Department of Pediatrics Division of Neonatology wcarlo@peds.uab.edu 1 2 Stevie Wonder 4 Objectives
Neonatal HSV. Version: 1. Governance Group. Date of Approval: Date of Ratification Signature of ratifying Group Chair
 Paediatric Neonatal HSV Version: 1 Approval Committee: Date of Approval: 25-04-2018 Ratification Group (eg Clinical network): Date of Ratification Signature of ratifying Group Chair Author s and job titles
Paediatric Neonatal HSV Version: 1 Approval Committee: Date of Approval: 25-04-2018 Ratification Group (eg Clinical network): Date of Ratification Signature of ratifying Group Chair Author s and job titles
Red Stick ID Visual Diagnosis Questions August 22, 2014
 Red Stick ID Visual Diagnosis Questions August 22, 2014 James H. Brien, DO Case #1 The setting is a Pediatric Clinic in San Antonio, Texas on a Saturday in 1989. However, it could have been yesterday in
Red Stick ID Visual Diagnosis Questions August 22, 2014 James H. Brien, DO Case #1 The setting is a Pediatric Clinic in San Antonio, Texas on a Saturday in 1989. However, it could have been yesterday in
1. Introduction. Correspondence should be addressed to Richard J. Drew; Received 23 July 2015; Accepted 15 November 2015
 Infectious Diseases in Obstetrics and Gynecology Volume 2015, Article ID 218080, 5 pages http://dx.doi.org/10.1155/2015/218080 Research Article Pregnancy Outcomes of Mothers with Detectable CMV-Specific
Infectious Diseases in Obstetrics and Gynecology Volume 2015, Article ID 218080, 5 pages http://dx.doi.org/10.1155/2015/218080 Research Article Pregnancy Outcomes of Mothers with Detectable CMV-Specific
MFMU - Background. MFMU - Background MFMU GOALS
 MFMU - Background Highlights From The MFM Units Network Ronald Wapner, MD Modern OB management (especially high risk pregnancies) has adopted principles of care, employed pharmaceuticals, applied methodologies
MFMU - Background Highlights From The MFM Units Network Ronald Wapner, MD Modern OB management (especially high risk pregnancies) has adopted principles of care, employed pharmaceuticals, applied methodologies
Neonatal infections and neonatal seizures. Mohamed Waheed Elsharief Dept. of paediatrics Faculty of medicine Jazan University KSA
 Neonatal infections and neonatal seizures Mohamed Waheed Elsharief Dept. of paediatrics Faculty of medicine Jazan University KSA objectives By the end of this lecture the student should Define neonatal
Neonatal infections and neonatal seizures Mohamed Waheed Elsharief Dept. of paediatrics Faculty of medicine Jazan University KSA objectives By the end of this lecture the student should Define neonatal
Neonatal Herpes Infection: Case Report and Discussion
 BRIEF REPORT Neonatal Herpes Infection: Case Report and Discussion Jordan C. White, MD, and Susanna R. Magee, MD, MPH Neonatal herpes simplex virus (HSV) infections are often life-threatening. Although
BRIEF REPORT Neonatal Herpes Infection: Case Report and Discussion Jordan C. White, MD, and Susanna R. Magee, MD, MPH Neonatal herpes simplex virus (HSV) infections are often life-threatening. Although
 Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever Without a Source Age: 0-28 Day Pathway - Emergency Department Evidence Based Outcome Center
 Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Newborn screening for cytomegalovirus
 Newborn screening for cytomegalovirus External review against programme appraisal criteria for the UK National Screening Committee (UK NSC) Version: Final Bazian Ltd. October 2017 This analysis has been
Newborn screening for cytomegalovirus External review against programme appraisal criteria for the UK National Screening Committee (UK NSC) Version: Final Bazian Ltd. October 2017 This analysis has been
ENCEPHALITIS. Diana Montoya Melo
 ENCEPHALITIS Diana Montoya Melo 4 yo female patient, brought to the ED after having a GTC seizure 30 mins ago, which lasted up to a min. Mom reports that he has a ho 3 days of fever and runny nose, associated
ENCEPHALITIS Diana Montoya Melo 4 yo female patient, brought to the ED after having a GTC seizure 30 mins ago, which lasted up to a min. Mom reports that he has a ho 3 days of fever and runny nose, associated
NEWBORN FEMALE WITH GOITER PAYAL PATEL, M.D. PEDIATRIC ENDOCRINOLOGY FELLOW FEBRUARY 12, 2015
 NEWBORN FEMALE WITH GOITER PAYAL PATEL, M.D. PEDIATRIC ENDOCRINOLOGY FELLOW FEBRUARY 12, 2015 CHIEF COMPLAINT 35 6/7 week F with goiter, born to a mother with Graves disease (GD) HPI 35 6/7 week F born
NEWBORN FEMALE WITH GOITER PAYAL PATEL, M.D. PEDIATRIC ENDOCRINOLOGY FELLOW FEBRUARY 12, 2015 CHIEF COMPLAINT 35 6/7 week F with goiter, born to a mother with Graves disease (GD) HPI 35 6/7 week F born