Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants
|
|
|
- Alberta Perkins
- 5 years ago
- Views:
Transcription



1 Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011
2 Disclosure I have no actual or potential conflict of interest in relation to this program
3 Objectives 1. Describe the primary pathogens/pathology in the febrile neonate and infant 2. Interpret the evaluation of the febrile infant using evidence-based guidelines 3. Distinguish special circumstances regarding the evaluation of febrile infants (RSV, influenza)
4 Outline Febrile Infant CPG Febrile Neonates Bacteria HSV Febrile Infants Low-Risk Criteria Special Circumstances RSV Influenza
 Axillary/tympanic/ pacifier temperatures are unreliable in young children -Baraff.")
5 Terminology: Fever Core temperature (rectal) 38.0 o C (100.4 o F) Axillary/tympanic/ pacifier temperatures are unreliable in young children -Baraff. Ann Emerg Med 2000; 36:
 Skin temperature 2.")

6 Bundling Elevates skin temperature not rectal temperature (N=64) Skin temperature 2.67 o C/hr Rectal temperature 0.06 o C/hr - Grover. Pediatrics 1994; 94: Fever > 38.0 o C should not be attributed to bundling
 Enterovirus (EV)")
7 Febrile Neonates 0-28 Days: Pathogens Bacterial Listeria monocytogenes Group B streptococcus Escherichia coli Viral Herpes simplex (HSV) Enterovirus (EV)
8

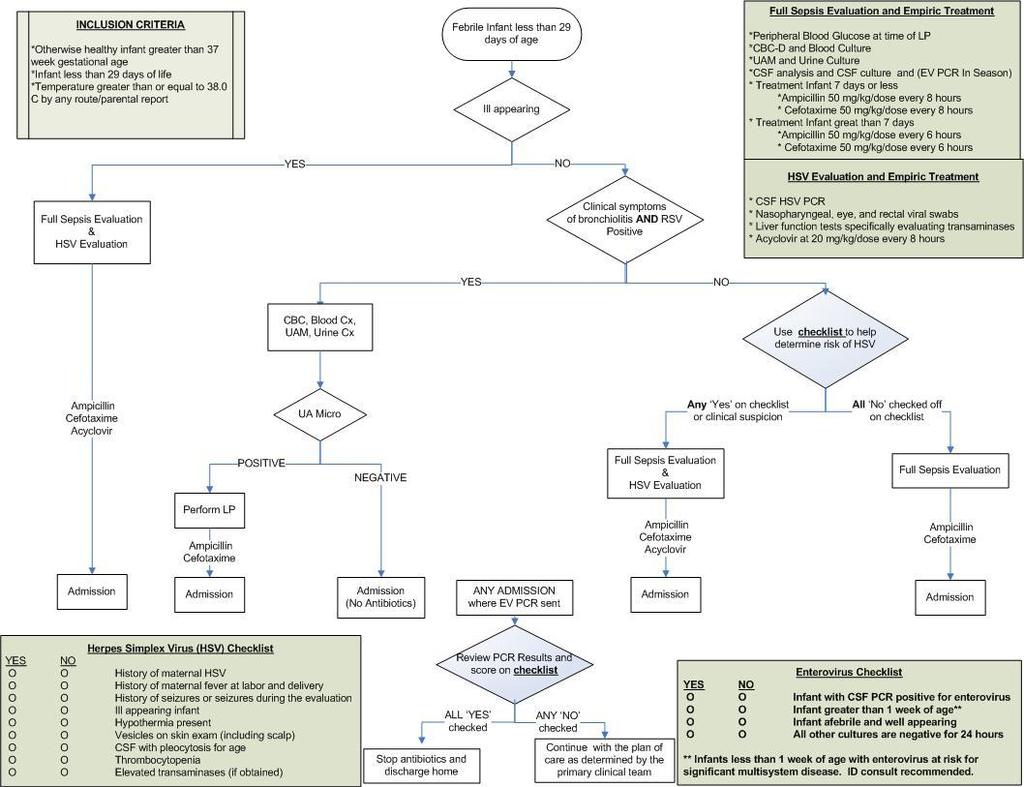
9 Febrile Neonates No criteria exist to safely identify febrile neonates as low-risk for serious bacterial infections (SBI) All febrile neonates require full sepsis evaluation with inpatient antibiotics regardless of clinical appearance Perhaps 1 exception (RSV)
 Kimberlin et al.")
10 Herpes Simplex (HSV) Must be considered in infants 28 days who have any of the following: Are ill-appearing Have mucocutaneous vesicles Have neurologic symptoms (seizures) Have CSF pleocytosis with a negative Gram stain Lethargy correlates with CNS infection Elevated liver enzymes correlate with disseminated HSV infection (N=186) Kimberlin et al. Pediatrics 2001; 108:
11
12 Herpes Simplex Virus and SBI in Febrile Infants Herpes Simplex Virus (HSV) Checklist YES NO O O History of maternal HSV O O History of maternal fever at labor and delivery O O History of seizures or seizures during the evaluation O O Ill appearing infant O O Hypothermia present O O Vesicles on skin exam (including scalp) O O CSF with pleocytosis for age O O Thrombocytopenia O O Elevated transaminases (if obtained)
13 Herpes Simplex Virus and SBI in Febrile Infants: Conclusion If any item of the HSV checklist is present: RECOMMEND A thorough HSV evaluation be completed Empiric treatment with acyclovir (20 mg/kg) tid HSV Evaluation and Empiric Treatment * CSF HSV PCR * Nasopharyngeal, eye, and rectal viral swabs * Liver function tests specifically evaluating transaminases * Acyclovir at 20 mg/kg/dose every 8 hours
14

15
 days of life Similar pathogens to previous group Limited Listeria infection risk Late onset")
16 What is a Febrile Infant? Ages (?90) days of life Similar pathogens to previous group Limited Listeria infection risk Late onset GBS Limited number of herpes infections after 4 weeks of age

17 Background: Febrile Young Infants Evaluation of febrile infants studied for decades 1% of all pediatric ED visits CMH ~650/year; national ~1% all visits Significant burden to hospital resources & society
18 Bachur 2001
19 SBI in low risk patients (%) Febrile Infant Protocols: Reported Statistics Sensitivity 92% Rochester Philadelphia Boston 1.1% 0.4% 5.4% (83-97) Specificity 50% (47-53) PPV 12.3% (10-16) NPV 98.9% (97-100) - Bachur. Pediatrics. 2001; 108; % (92-100) 42% (38-46) 14% (11-17) 99.7% (98-100) N/A 94.6% N/A N/A
20 Febrile Infant Protocols: Reported Statistics Rochester Philadelphia Boston SBI in low risk patients (%) 1.1% 0.4% 5.4% Sensitivity 92% (83-97) Specificity 50% (47-53) PPV 12.3% (10-16) NPV 98.9% (97-100) - Bachur. Pediatrics. 2001; 108; % (92-100) 42% (38-46) 14% (11-17) 99.7% (98-100) N/A 94.6% N/A N/A
 NPV 94.")
 NPV 99.7% (95% CI 98,100) -Pediatrics.")
21 Presumptive Failure Rates of Low-Risk FYI Protocols Boston 54/1000 (5.4%) NPV 94.6% (95% CI 92,96) Philadelphia 3.5/1000 (0.4%) NPV 99.7% (95% CI 98,100) -Pediatrics. 1999; 103;
22
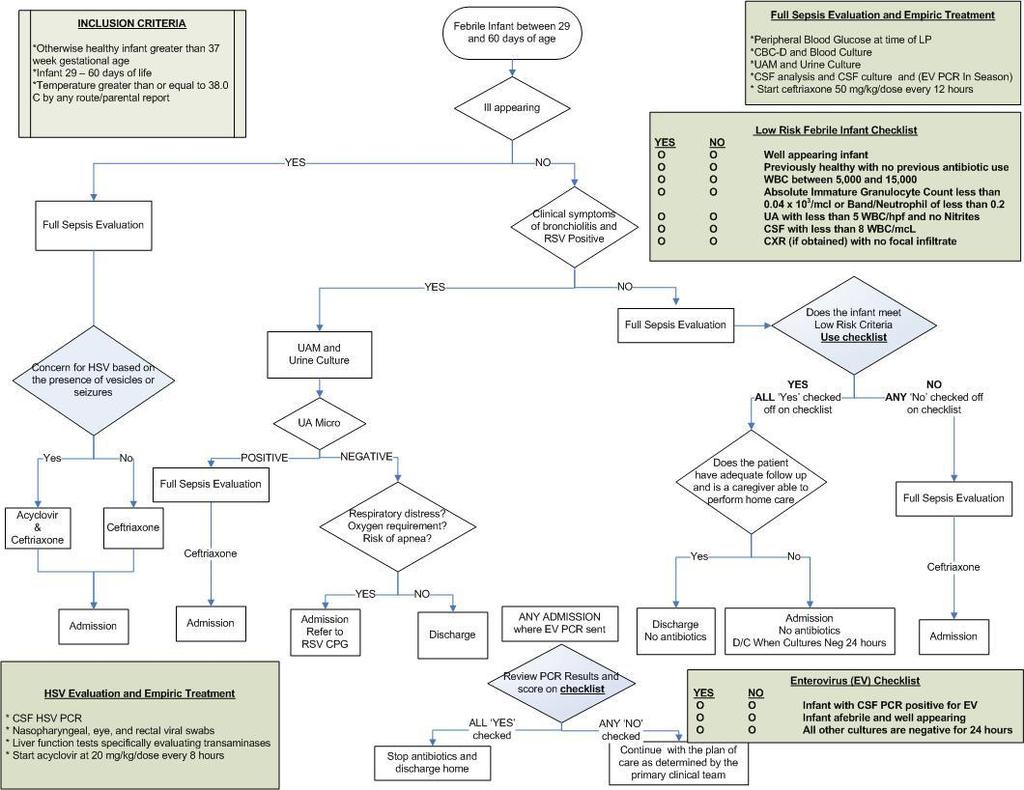
23 Low Risk Febrile Infant Checklist Low Risk Febrile Infant Checklist YES NO O O Well appearing infant O O Previously healthy with no previous antibiotic use O O WBC between 5,000 and 15,000 O O Absolute Immature Granulocyte Count less than 0.04 x 10 3 / mcl or Band to Neutrophil ratio of less than 0.2 O O UA with less than 5 WBC/hpf and no Nitrites O O CSF with less than 8 WBC/hpf O O Chest x-ray (if obtained) with no focal infiltrate
24
25 CMH Febrile Infant CPG Requires full sepsis evaluation RSV exception Disposition up to evaluating MD and primary physician if patient is determined to be low-risk
26
 RSV+/SBI+ 2/174 (1.2%) Both UTI RSV-/SBI+ 22/174 (12.")
27 RSV+ and Risk of SBI Does RSV positive status lower the risk of SBI? Retrospective cohort FYI (N=174) RSV+/SBI+ 2/174 (1.2%) Both UTI RSV-/SBI+ 22/174 (12.6%) UTI 17/22 Titus et al Pediatrics. 2003; 112:
 RSV+ (n= 269)")
 All 3 < 29 days Bacterial Meningitis: 0 (0%) RSV- (n=")
 Bacterial Meningitis: 8 (~0.")
28 Respiratory Syncytial Virus and SBI in Febrile Infants Prospective, cross-sectional study (N=1248) RSV+ (n= 269) 17 (~7.0%) UTI: 14 (~5.4%) Bacteremia: 3 (~1.1%) All 3 < 29 days Bacterial Meningitis: 0 (0%) RSV- (n= 979) 116 (~12.5%) UTI: 98 (~10.1%) Bacteremia: 8 (~2.3%) Bacterial Meningitis: 8 (~0.9%) Levine et al Pediatrics. 2004;
 5 UTI s, 3 Bacteremia RSV-/SBI+: 47/329 (14.2%) Levine et al Pediatrics.")
29 RSV + and Risk of SBI: Limitations Only 411 (33%) 28 DOL RSV+/SBI+: 8/82 (10.1%) 5 UTI s, 3 Bacteremia RSV-/SBI+: 47/329 (14.2%) Levine et al Pediatrics. 2004;
30 Respiratory Syncytial Virus and SBI in Febrile Infants Statistically lower (but still clinically important) rates of UTI 3 bacteremia all in < 29 DOL 0 cases of meningitis Not powered to detect a difference in bacteremia or meningitis
31 Recommendations Full sepsis evaluation if the patient is ill appearing Blood culture and urine culture/ua with microscopy in all febrile infants less than 29 days Admit Hold antibiotics unless UAM positive UA with microscopy and urine culture in all febrile infants days Hold antibiotics Disposition based on RSV CPG
32
33 Influenza and Risk of SBI Retrospective, cross-sectional study (N=705; 0-36 months old) Influenza positive (N=163) SBI rate 3/163 (1.8%) 2 UTI, 1 bacteremia, 0 meningitis Odds ratio of SBI and Influenza 0.14 Influenza negative (N=542) SBI rate 65/542 (12.0%) 38 UTI, 23 bacteremia, 4 meningitis Limitations Insufficient number of <29 DOL (13 +, 49 -) Smitherman et al Pediatrics 2005; 115:
34 Influenza and Risk of SBI Multicenter, prospective, cross-sectional study N=1091; 0 to 60 DOL Influenza positive (N=123/844) [14.3%] SBI rate 3/119 (2.5%) 3 UTI, 0 bacteremia, 0 meningitis Influenza negative (N=721/844) [85.7%] SBI rate 92/690 (13.3%) 77 UTI, 16 bacteremia, 6 meningitis Relative Risk of SBI and Influenza 0.19 [ ] Limitations Number of febrile neonates (268 <29 DOL, DOL) Not powered for bacteremia/meningitis detection Krief et al Pediatrics 2009; 124(1): 30-9

35 Current Data on FYI with Documented Influenza Influenza positive febrile young infants (29-60 days of life) have a significantly lower risk of SBI than influenza negative FYI. Limited data on febrile neonates Currently, all influenza+ infants at least need UA and urinary cultures (+/- blood culture)
36 Conclusions Important to perform a full diagnostic evaluation in all febrile young infants No component of the screening assessment can be omitted Management without antibiotics of febrile illnesses can be safely accomplished in selected infants
Fever in neonates (age 0 to 28 days)
") Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in the Newborn Period
 Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
The Febrile Infant. SJRH ED Rounds Dec By: Robin Clouston
 1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
Fevers and Seizures in Infants and Young Children
 Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Rational Evaluation of the Febrile Infant
 Disclosures Rational Evaluation of the Febrile Infant Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending
Disclosures Rational Evaluation of the Febrile Infant Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending
Faculty Disclosure. Stephen I. Pelton, MD. Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Evidence-based Management of Fever in Infants and Young Children
 Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Fever Without a Source Age: 0-28 Day Pathway - Emergency Department Evidence Based Outcome Center
 Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Disclosures. Background. Definitions. Why Worry about these Infants? Goals. Bacterial infection in the neonate and young infant: a review
 Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Fever in Young Infants 7 90 days of age
 Fever in Young Infants 7 90 days of age Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation.
Fever in Young Infants 7 90 days of age Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation.
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014
 Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
+ Objectives. n Define who is at risk for SBI. n Clarify risk stratification. n Provide treatment guidelines. n Bust some myths
 Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Hot Hot Tot:! The Hot Tot. Fever in KIds <90 Days 5/26/10
 Hot Hot Tot:! Fever in KIds
Hot Hot Tot:! Fever in KIds
1. Introduction Algorithm: Infant with Fever 0-28 Days Algorithm: Infant with Fever Days...3
 These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
4/14/2010. Theoretical purpose of fever? Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010
 Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
 1 Use the Yale Observation Scale to assess whether the patient is ill or well appearing. A score greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
1 Use the Yale Observation Scale to assess whether the patient is ill or well appearing. A score greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
Evaluating Fever in Infants. Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist
 Evaluating Fever in Infants Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation. I will
Evaluating Fever in Infants Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation. I will
Neonatal HSV SARA SAPORTA-KEATING 3/1/17
 Neonatal HSV SARA SAPORTA-KEATING 3/1/17 Pt Sx onset Presentation Clinical Presentation HSV risk factor(s) HSV results CSF WBC 1 DOL 7 DOL 8 Vesicular rash FOC with active cold sore (DOL2), C/S 2 DOL 7
Neonatal HSV SARA SAPORTA-KEATING 3/1/17 Pt Sx onset Presentation Clinical Presentation HSV risk factor(s) HSV results CSF WBC 1 DOL 7 DOL 8 Vesicular rash FOC with active cold sore (DOL2), C/S 2 DOL 7
PEDIATRIC INFECTIOUS DISEASES UPDATE. Neonatal HSV. Recognition, Diagnosis, and Management Coleen Cunningham MD
 Neonatal HSV Recognition, Diagnosis, and Management Coleen Cunningham MD Important questions Who is at risk? When do you test? What tests do you perform? When do you treat? What is appropriate therapy?
Neonatal HSV Recognition, Diagnosis, and Management Coleen Cunningham MD Important questions Who is at risk? When do you test? What tests do you perform? When do you treat? What is appropriate therapy?
Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE
 Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE Objectives A short history of the kiddie fever business Vaccinations Rapid viral testing Biomarkers Month-by-month approach to fevers in these
Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE Objectives A short history of the kiddie fever business Vaccinations Rapid viral testing Biomarkers Month-by-month approach to fevers in these
 Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Your first patient of the day
 Your first patient of the day 1 month old male with 2 days of fussiness Decreased stool output for 3 days Poor latch during breastfeeding noted at 3AM on day of arrival to the ED Started spitting up later
Your first patient of the day 1 month old male with 2 days of fussiness Decreased stool output for 3 days Poor latch during breastfeeding noted at 3AM on day of arrival to the ED Started spitting up later
Fever in Infants: Pediatric Dilemmas in Antibiotherapy
 Fever in Infants: Pediatric Dilemmas in Antibiotherapy Jahzel M. Gonzalez Pagan, MD, FAAP Pediatric Emergency Medicine Associate Professor, UPH Medical Advisor, SJCH June 9 th, 2017 S Objectives S Review
Fever in Infants: Pediatric Dilemmas in Antibiotherapy Jahzel M. Gonzalez Pagan, MD, FAAP Pediatric Emergency Medicine Associate Professor, UPH Medical Advisor, SJCH June 9 th, 2017 S Objectives S Review
NEONATAL SEPSIS. Dalima Ari Wahono Astrawinata Departemen Patologi Klinik, FKUI-RSCM
 NEONATAL SEPSIS Dalima Ari Wahono Astrawinata Departemen Patologi Klinik, FKUI- Background Neonatal sepsis : Early-onset Late-onset Early-onset : mostly premature neonates Within 24 hours 85% 24-48 hours
NEONATAL SEPSIS Dalima Ari Wahono Astrawinata Departemen Patologi Klinik, FKUI- Background Neonatal sepsis : Early-onset Late-onset Early-onset : mostly premature neonates Within 24 hours 85% 24-48 hours
EPG Clinical Guidelines
 Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Sample Selection- Vignettes
 Sample Selection- Vignettes Rangaraj Selvarangan, BVSc, PhD, D(ABMM) Professor, UMKC School of Medicine Director, Microbiology, Virology and Molecular Infectious Diseases Laboratory Director, Laboratory
Sample Selection- Vignettes Rangaraj Selvarangan, BVSc, PhD, D(ABMM) Professor, UMKC School of Medicine Director, Microbiology, Virology and Molecular Infectious Diseases Laboratory Director, Laboratory
Fever in Babies. Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases
 Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
CHAPTER 167 Pediatric Fever
 CHAPTER 167 Pediatric Fever Nathan W. Mick Fever is the most common chief complaint of pediatric patients presenting to the emergency department (ED), accounting for up to 20% of ED visits. Most cases
CHAPTER 167 Pediatric Fever Nathan W. Mick Fever is the most common chief complaint of pediatric patients presenting to the emergency department (ED), accounting for up to 20% of ED visits. Most cases
MICROBIOLOGICAL TESTING IN PICU
 MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
5/5/2010. Phil Bernard, MD. 2 week old presents to your office with fever to F HR 150 RR 40
 2 week old presents to your office with fever to 101.5 F HR 150 RR 40 BP not obtained obtained Sats 95% Phil Bernard, MD Baraff LJ, Bass JW, Fleisher GR, Klein JO, McCracken GH, Powell KR, et al. Practice
2 week old presents to your office with fever to 101.5 F HR 150 RR 40 BP not obtained obtained Sats 95% Phil Bernard, MD Baraff LJ, Bass JW, Fleisher GR, Klein JO, McCracken GH, Powell KR, et al. Practice
Facing the ongoing challenge of the febrile young infant
 DePorre et al. Critical Care (2017) 21:68 DOI 10.1186/s13054-017-1646-9 REVIEW Facing the ongoing challenge of the febrile young infant Adrienne G. DePorre 1,2*, Paul L. Aronson 3 and Russell J. McCulloh
DePorre et al. Critical Care (2017) 21:68 DOI 10.1186/s13054-017-1646-9 REVIEW Facing the ongoing challenge of the febrile young infant Adrienne G. DePorre 1,2*, Paul L. Aronson 3 and Russell J. McCulloh
Neonatal Herpes Infection: Case Report and Discussion
 BRIEF REPORT Neonatal Herpes Infection: Case Report and Discussion Jordan C. White, MD, and Susanna R. Magee, MD, MPH Neonatal herpes simplex virus (HSV) infections are often life-threatening. Although
BRIEF REPORT Neonatal Herpes Infection: Case Report and Discussion Jordan C. White, MD, and Susanna R. Magee, MD, MPH Neonatal herpes simplex virus (HSV) infections are often life-threatening. Although
CNS Infections. Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London. Hammersmith Acute Medicine 2011
 CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
FEVER. What is fever?
 FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
Critical Review Form Clinical Prediction or Decision Rule
 Critical Review Form Clinical Prediction or Decision Rule Development and Validation of a Multivariable Predictive Model to Distinguish Bacterial from Aseptic Meningitis in Children, Pediatrics 2002; 110:
Critical Review Form Clinical Prediction or Decision Rule Development and Validation of a Multivariable Predictive Model to Distinguish Bacterial from Aseptic Meningitis in Children, Pediatrics 2002; 110:
J of Evolution of Med and Dent Sci/ eissn , pissn / Vol. 4/ Issue 66/ Aug 17, 2015 Page 11432
 BLOOD CULTURE AND BACTEREMIA PREDICTORS IN INFANTS LESS THAN ONE YEAR OF AGE WITH FEVER WITHOUT SOURCE (FWS) Y. G. Sathish Kumar 1, A. Udayamaliny 2, S. Ankitha 3 HOW TO CITE THIS ARTICLE: Y. G. Sathish
BLOOD CULTURE AND BACTEREMIA PREDICTORS IN INFANTS LESS THAN ONE YEAR OF AGE WITH FEVER WITHOUT SOURCE (FWS) Y. G. Sathish Kumar 1, A. Udayamaliny 2, S. Ankitha 3 HOW TO CITE THIS ARTICLE: Y. G. Sathish
Dr. Bob Wilson Golden BC
 Fever in Infants Under 3 Mon. Dr. Bob Wilson Golden BC What is the risk of serious bacterial infection in a febrile 2 A. 5% B. 10% C. 25% D. 50% E. 100% month old infant? What is the most common congenital
Fever in Infants Under 3 Mon. Dr. Bob Wilson Golden BC What is the risk of serious bacterial infection in a febrile 2 A. 5% B. 10% C. 25% D. 50% E. 100% month old infant? What is the most common congenital
MANAGEMENT OF SUSPECTED VIRAL ENCEPHALITIS IN CHILDREN
 MANAGEMENT OF SUSPECTED VIRAL ENCEPHALITIS IN CHILDREN OVERVIEW 1980s: dramatically improved by aciclovir HSV encephalitis in adults Delays treatment(> 48h after hospital admission): associated with a
MANAGEMENT OF SUSPECTED VIRAL ENCEPHALITIS IN CHILDREN OVERVIEW 1980s: dramatically improved by aciclovir HSV encephalitis in adults Delays treatment(> 48h after hospital admission): associated with a
Emergency Neurological Life Support Meningitis and Encephalitis
 Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
ENCEPHALITIS. Diana Montoya Melo
 ENCEPHALITIS Diana Montoya Melo 4 yo female patient, brought to the ED after having a GTC seizure 30 mins ago, which lasted up to a min. Mom reports that he has a ho 3 days of fever and runny nose, associated
ENCEPHALITIS Diana Montoya Melo 4 yo female patient, brought to the ED after having a GTC seizure 30 mins ago, which lasted up to a min. Mom reports that he has a ho 3 days of fever and runny nose, associated
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS
 ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
Fever in Children. Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital
 Fever in Children Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital Update on Children s services @ GCUH Dedicated Children s Pod in the Emergency
Fever in Children Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital Update on Children s services @ GCUH Dedicated Children s Pod in the Emergency
Time to Detection of Bacterial Cultures in Infants Aged 0 to 90 Days
 RESEARCH ARTICLE Time to Detection of Bacterial Cultures in Infants Aged 0 to 90 Days AUTHORS Rianna C. Evans, MD, Bryan R. Fine, MD, MPH Division of Pediatric Hospital Medicine, Department of Pediatrics,
RESEARCH ARTICLE Time to Detection of Bacterial Cultures in Infants Aged 0 to 90 Days AUTHORS Rianna C. Evans, MD, Bryan R. Fine, MD, MPH Division of Pediatric Hospital Medicine, Department of Pediatrics,
Neonatal sepsis INCIDENCE RISK FACTORS RISK FACTORS 5/18/2015
 Angelica Floren MD.FAAP. Caring for Little Miracles 6 Th Annual Care Of the Sick Newborn Conference Neonatal sepsis Neonatal sepsis is a disease that may start with minimal or nonspecific symptoms and
Angelica Floren MD.FAAP. Caring for Little Miracles 6 Th Annual Care Of the Sick Newborn Conference Neonatal sepsis Neonatal sepsis is a disease that may start with minimal or nonspecific symptoms and
Rebecca T Slagle, MN, APRN, NNP-BC. Speak up!!
 Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Disclosures. Objectives. Epidemiology. Enterovirus 68. Enterovirus species 9/24/2015. Enterovirus D68: Lessons Learned from the Frontline
 Enterovirus D68: Lessons Learned from the Frontline Disclosures Jennifer Schuster, MD MSCI Children s Mercy Hospital Pediatric Infectious Diseases September 16, 2015 I have nothing to disclose I do not
Enterovirus D68: Lessons Learned from the Frontline Disclosures Jennifer Schuster, MD MSCI Children s Mercy Hospital Pediatric Infectious Diseases September 16, 2015 I have nothing to disclose I do not
Laboratory Diagnosis of Central Nervous System Infections in Children
 Laboratory Diagnosis of Central Nervous System Infections in Children R. Selvarangan. BVSc, PhD, D(ABMM). Professor, UMKC-SOM Director, Microbiology Laboratory Children's Mercy Hospital Kansas City, MO
Laboratory Diagnosis of Central Nervous System Infections in Children R. Selvarangan. BVSc, PhD, D(ABMM). Professor, UMKC-SOM Director, Microbiology Laboratory Children's Mercy Hospital Kansas City, MO
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS. All children with suspected or confirmed meningitis
 GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
RESEARCH ARTICLE ABSTRACT
 RESEARCH ARTICLE Evaluating the Impact of Implementing a Clinical Practice Guideline for Febrile Infants With Positive Respiratory Syncytial Virus or Enterovirus Testing Adrienne DePorre, MD, a David D.
RESEARCH ARTICLE Evaluating the Impact of Implementing a Clinical Practice Guideline for Febrile Infants With Positive Respiratory Syncytial Virus or Enterovirus Testing Adrienne DePorre, MD, a David D.
FILMARRAY: CAN IT MAKE A DIFFERENCE FOR CSF TESTING L O U I S E O S U L L I V A N, M M U H O S U L L I V A N M A T E R. I E
 FILMARRAY: CAN IT MAKE A DIFFERENCE FOR CSF TESTING L O U I S E O S U L L I V A N, M M U H O S U L L I V A N L @ M A T E R. I E Level 4 teaching hospital based in Dublin s north inner city Over 600 in-patient
FILMARRAY: CAN IT MAKE A DIFFERENCE FOR CSF TESTING L O U I S E O S U L L I V A N, M M U H O S U L L I V A N L @ M A T E R. I E Level 4 teaching hospital based in Dublin s north inner city Over 600 in-patient
Should blood cultures be obtained in all infants 3 to 36 months presenting with significant fever? abstract CLINICAL QUESTION REVIEW
 CLINICAL QUESTION REVIEW CQR is a recurring section in Hospital Pediatrics where authors start with a relevant clinical question, find and synthesize the recent literature and provide their best answer
CLINICAL QUESTION REVIEW CQR is a recurring section in Hospital Pediatrics where authors start with a relevant clinical question, find and synthesize the recent literature and provide their best answer
Neonatal Sepsis. Neonatal sepsis ehandbook
 Neonatal Sepsis Neonatal sepsis ehandbook Sepsis Any baby who is unwell must be considered at risk of sepsis 1 in 8 per 1000 lives births The consequences of untreated sepsis are devastating - 10-30% risk
Neonatal Sepsis Neonatal sepsis ehandbook Sepsis Any baby who is unwell must be considered at risk of sepsis 1 in 8 per 1000 lives births The consequences of untreated sepsis are devastating - 10-30% risk
Outline. The Scarlet H : Neonatal herpes simplex virus infection in the 21 st century. Ancient History. Ancient History. History.
 The Scarlet H : Neonatal herpes simplex virus infection in the 21 st century J.B. Cantey, MD Pediatric Grand Rounds University of Texas Health San Antonio September 15, 2017 Outline Historical perspectives
The Scarlet H : Neonatal herpes simplex virus infection in the 21 st century J.B. Cantey, MD Pediatric Grand Rounds University of Texas Health San Antonio September 15, 2017 Outline Historical perspectives
Kidz Medical Services Infant Exposed to Genital Herpes Simplex Virus
 Kidz Medical Services Infant Exposed to Genital Herpes Simplex Virus Guideline: HSV Guideline: I. Herpes Simplex Virus (HSV): A. HSV is an enveloped, double-stranded DNA virus that enters the body via
Kidz Medical Services Infant Exposed to Genital Herpes Simplex Virus Guideline: HSV Guideline: I. Herpes Simplex Virus (HSV): A. HSV is an enveloped, double-stranded DNA virus that enters the body via
Neonatal infections. Joanna Seliga-Siwecka
 Neonatal infections Joanna Seliga-Siwecka Neonatal infections Early onset sepsis Late onset sepsis TORCH Early onset sepsis (EOS) Blood or cerebral fluid culture-proven infection at fewer than 7 days
Neonatal infections Joanna Seliga-Siwecka Neonatal infections Early onset sepsis Late onset sepsis TORCH Early onset sepsis (EOS) Blood or cerebral fluid culture-proven infection at fewer than 7 days
Fever and Infections in Pediatrics
 Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
PDFlib PLOP: PDF Linearization, Optimization, Protection. Page inserted by evaluation version
 PDFlib PLOP: PDF Linearization, Optimization, Protection Page inserted by evaluation version www.pdflib.com sales@pdflib.com ACAD EMERG MED d December 2004, Vol. 11, No. 12 d www.aemj.org 1297 A Low Peripheral
PDFlib PLOP: PDF Linearization, Optimization, Protection Page inserted by evaluation version www.pdflib.com sales@pdflib.com ACAD EMERG MED d December 2004, Vol. 11, No. 12 d www.aemj.org 1297 A Low Peripheral
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital
 Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Community Acquired Pneumonia
 April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
CNS Infections. GBS Streptococcus agalactiae. Meningitis - Neonate
 CNS Infections GBS Streptococcus agalactiae Bacterial meningitis - Pathophysiology - general Specific organisms - Age Hosts Treatment/Prevention Distinguish from viral disease Common commensal flora childbearing
CNS Infections GBS Streptococcus agalactiae Bacterial meningitis - Pathophysiology - general Specific organisms - Age Hosts Treatment/Prevention Distinguish from viral disease Common commensal flora childbearing
NIH Public Access Author Manuscript Pediatrics. Author manuscript; available in PMC 2007 November 14.
 NIH Public Access Author Manuscript Published in final edited form as: Pediatrics. 2006 July ; 118(1): 34 40. Prospective Evaluation of the Risk of Serious Bacterial Infection in Children Who Present to
NIH Public Access Author Manuscript Published in final edited form as: Pediatrics. 2006 July ; 118(1): 34 40. Prospective Evaluation of the Risk of Serious Bacterial Infection in Children Who Present to
Infant Fever, What s Old What s New Brian R. Moore, M.D., F.A.A.P.
 Infant Fever, What s Old What s New Brian R. Moore, M.D., F.A.A.P. PEM Fellowship Director Assistant Professor, Departments of Emergency Medicine and Pediatrics University of New Mexico Health Science
Infant Fever, What s Old What s New Brian R. Moore, M.D., F.A.A.P. PEM Fellowship Director Assistant Professor, Departments of Emergency Medicine and Pediatrics University of New Mexico Health Science
IDPH ESF-8 Plan: Pediatric and Neonatal Surge Annex Sample Pediatric Admission Orders 2015
 Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
enter the room. Persons immune from previous varicella infection may enter the room without a mask. Those immune by adenoviruses, influenza viruses.
 All clients admitted to the hospital automatically are considered to be on standard precautions. The diseases listed below require standard precautions plus additional precautions that are noted in the
All clients admitted to the hospital automatically are considered to be on standard precautions. The diseases listed below require standard precautions plus additional precautions that are noted in the
Viral Diseases. T Bamdad, PhD, Tarbiat Modares University
 Viral Diseases 1 Categorizing viral infections by the organ system most commonly affected (eg, lungs, GI tract, skin, liver, CNS, mucous membranes) can be clinically useful, although certain viral disorders
Viral Diseases 1 Categorizing viral infections by the organ system most commonly affected (eg, lungs, GI tract, skin, liver, CNS, mucous membranes) can be clinically useful, although certain viral disorders
HSV Screening: Are Wesley Obstetricians Following the Guidelines? Dawn Boender, PGY4 Taylor Bertschy, PGY3
 HSV Screening: Are Wesley Obstetricians Following the Guidelines? Dawn Boender, PGY4 Taylor Bertschy, PGY3 Goals To increase obstetrician knowledge regarding HSV screening Institute clinical changes at
HSV Screening: Are Wesley Obstetricians Following the Guidelines? Dawn Boender, PGY4 Taylor Bertschy, PGY3 Goals To increase obstetrician knowledge regarding HSV screening Institute clinical changes at
Dilemmas in the Management of Meningitis & Encephalitis HEADACHE AND FEVER. What is the best initial approach for fever, headache, meningisums?
 Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Oh SCH It s a neonatal emergency
 trekk.ca 1 1 Oh SCH It s a neonatal emergency Emma Burns, MD, FRCPC IWK Health Centre 2 1 Objectives Critically ill neonate approach and tips Stay on time! Thanks to: Shannon MacPhee, Mike Young, Jon Cherry,
trekk.ca 1 1 Oh SCH It s a neonatal emergency Emma Burns, MD, FRCPC IWK Health Centre 2 1 Objectives Critically ill neonate approach and tips Stay on time! Thanks to: Shannon MacPhee, Mike Young, Jon Cherry,
Herpesvirus infections in pregnancy
 Herpesvirus infections in pregnancy Dr. med. Daniela Huzly Institute of Virology University Medical Center Freiburg, Germany Herpes simplex virus 1+2 Risk in pregnancy and at birth Primary infection in
Herpesvirus infections in pregnancy Dr. med. Daniela Huzly Institute of Virology University Medical Center Freiburg, Germany Herpes simplex virus 1+2 Risk in pregnancy and at birth Primary infection in
Febrile Seizures. Preface. Definition, Evaluation, Assessment, and Prognosis. Definition
 Febrile Seizures Guideline significantly revised by Rebecca Latch, MD, in collaboration with the ANGELS team. Last reviewed by Rebecca Latch, MD, July 22, 2016. Guideline replaced Evaluation and Treatment
Febrile Seizures Guideline significantly revised by Rebecca Latch, MD, in collaboration with the ANGELS team. Last reviewed by Rebecca Latch, MD, July 22, 2016. Guideline replaced Evaluation and Treatment
Management of Complex Febrile Seizures
 Management of Complex Febrile Seizures An 13 month old girl presents to the ED after having a shaking episode at home. Mom describes shaking of both arms and legs, lasting 20 minutes. The child has no
Management of Complex Febrile Seizures An 13 month old girl presents to the ED after having a shaking episode at home. Mom describes shaking of both arms and legs, lasting 20 minutes. The child has no
Upper...and Lower Respiratory Tract Infections
 Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Syndromic Testing for Infectious Diseases
 Syndromic Testing for Infectious Diseases Part 3: Central Nervous System Infections HOT TOPIC / 2017 Presenter: Elitza S. Theel, Ph.D., D(ABMM) Director of Infectious Diseases Serology Department of Laboratory
Syndromic Testing for Infectious Diseases Part 3: Central Nervous System Infections HOT TOPIC / 2017 Presenter: Elitza S. Theel, Ph.D., D(ABMM) Director of Infectious Diseases Serology Department of Laboratory
11/9/2012. Group B Streptococcal Infections: Consensus and Controversies. Prevention of Early-Onset GBS Disease in the USA.
 Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Paediatrica Indonesiana. Urine dipstick test for diagnosing urinary tract infection
 Paediatrica Indonesiana VOLUME 53 November NUMBER 6 Original Article Urine dipstick test for diagnosing urinary tract infection Syarifah Julinawati, Oke Rina, Rosmayanti, Rafita Ramayati, Rusdidjas Abstract
Paediatrica Indonesiana VOLUME 53 November NUMBER 6 Original Article Urine dipstick test for diagnosing urinary tract infection Syarifah Julinawati, Oke Rina, Rosmayanti, Rafita Ramayati, Rusdidjas Abstract
Fever Interval before Diagnosis, Prior Antibiotic Treatment, and Clinical Outcome for Young Children with Bacterial Meningitis
 MAJOR ARTICLE Fever Interval before Diagnosis, Prior Antibiotic Treatment, and Clinical Outcome for Young Children with Bacterial Meningitis Bema K. Bonsu 1 and Marvin B. Harper 2 1 Department of Medicine,
MAJOR ARTICLE Fever Interval before Diagnosis, Prior Antibiotic Treatment, and Clinical Outcome for Young Children with Bacterial Meningitis Bema K. Bonsu 1 and Marvin B. Harper 2 1 Department of Medicine,
UTI Update: Have We Been Led Astray? Disclosure. Objectives
 UTI Update: Have We Been Led Astray? KAAP Sept 28, 2012 Robert Wittler, MD 1 Disclosure Neither I nor any member of my immediate family has a financial relationship or interest with any entity related
UTI Update: Have We Been Led Astray? KAAP Sept 28, 2012 Robert Wittler, MD 1 Disclosure Neither I nor any member of my immediate family has a financial relationship or interest with any entity related
CRACKCast E167 Pediatric Fever. Key Concepts. CrackCast Show Notes Pediatric Fever April 2018
 CRACKCast E167 Pediatric Fever Key Concepts Fever is the #1 kids are brought to the ED! Vaccination (for Haemophilus influenzae type b and Streptococcus pneumoniae) has dropped the rates of serious bacterial
CRACKCast E167 Pediatric Fever Key Concepts Fever is the #1 kids are brought to the ED! Vaccination (for Haemophilus influenzae type b and Streptococcus pneumoniae) has dropped the rates of serious bacterial
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
Fever is one of the most frequent reasons for consultation in
 ORIGINAL STUDIES Impact of Rapid Viral Testing for Influenza A and B Viruses on Management of Febrile Infants Without Signs of Focal Infection Javier Benito-Fernández, MD, Miguel A. Vázquez-Ronco, MD,
ORIGINAL STUDIES Impact of Rapid Viral Testing for Influenza A and B Viruses on Management of Febrile Infants Without Signs of Focal Infection Javier Benito-Fernández, MD, Miguel A. Vázquez-Ronco, MD,
Isolation Precautions in Clinics
 Purpose Audience General principles Possible Exposures To define isolation precautions in a clinic setting. Clinics Isolation status should be determined primarily by the suspected disease and/or pathogen.
Purpose Audience General principles Possible Exposures To define isolation precautions in a clinic setting. Clinics Isolation status should be determined primarily by the suspected disease and/or pathogen.
Sara Lawson Chadwick. B.S. Microbiology, Marshall University, B.S. Biochemistry, Marshall University, Submitted to the Graduate Faculty of
 A RETROSPECTIVE CHART REVIEW OF CEREBROSPINAL FLUID CHARACTERISTICS OF INFANTS WHO PRESENT TO THE EMERGENCY DEPARTMENT WITH FEVER: ESTABLISHING NORMAL VALUES by Sara Lawson Chadwick B.S. Microbiology,
A RETROSPECTIVE CHART REVIEW OF CEREBROSPINAL FLUID CHARACTERISTICS OF INFANTS WHO PRESENT TO THE EMERGENCY DEPARTMENT WITH FEVER: ESTABLISHING NORMAL VALUES by Sara Lawson Chadwick B.S. Microbiology,
Central Nervous System Infection
 Central Nervous System Infection Lingyun Shao Department of Infectious Diseases Huashan Hospital, Fudan University Definition Meningitis: an inflammation of the arachnoid membrane, the pia mater, and the
Central Nervous System Infection Lingyun Shao Department of Infectious Diseases Huashan Hospital, Fudan University Definition Meningitis: an inflammation of the arachnoid membrane, the pia mater, and the
The Child with HIV and a Fever 1
 The Child with HIV and a Fever 1 Author: Andrew Riordan Amanda Williams Date of preparation: August 2003 Date reviewed: February 2012 Next review date: February 2014 Contents 1. Introduction 2. HIV disease
The Child with HIV and a Fever 1 Author: Andrew Riordan Amanda Williams Date of preparation: August 2003 Date reviewed: February 2012 Next review date: February 2014 Contents 1. Introduction 2. HIV disease
4/11/2017 COMMUNITY ACQUIRED PNEUMONIA. Disclaimer. A Review of How to Treat Common Infections in a Pediatric Patient. Objectives for Technicians
 Disclaimer A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland reports that she has no actual or potential conflict of interest in relation to this presentation. Off label use
Disclaimer A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland reports that she has no actual or potential conflict of interest in relation to this presentation. Off label use
ID Emergencies. BUMC-P Internal Medicine Edwin Yu
 ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
Surveillance for encephalitis in Bangladesh: preliminary results
 Surveillance for encephalitis in Bangladesh: preliminary results In Asia, the epidemiology and aetiology of encephalitis remain largely unknown, particularly in Bangladesh. A prospective, hospital-based
Surveillance for encephalitis in Bangladesh: preliminary results In Asia, the epidemiology and aetiology of encephalitis remain largely unknown, particularly in Bangladesh. A prospective, hospital-based
Controversies in Diagnosis and Therapy of Neonatal Sepsis
 Controversies in Diagnosis and Therapy of Neonatal Sepsis Sarah S. Long, M.D. Professor of Pediatrics Drexel University College of Medicine Chief, Section of Infectious Diseases St. Christopher s Hospital
Controversies in Diagnosis and Therapy of Neonatal Sepsis Sarah S. Long, M.D. Professor of Pediatrics Drexel University College of Medicine Chief, Section of Infectious Diseases St. Christopher s Hospital
A Practical Approach to Leukopenia/Neutropenia in Children. Vandy Black, M.D., M.Sc., FAAP OLOL Children s Hospital August 24, 2014
 A Practical Approach to Leukopenia/Neutropenia in Children Vandy Black, M.D., M.Sc., FAAP OLOL Children s Hospital August 24, 2014 Disclosures EPIC trial MAST Therapeutics SUSTAIN trial Selexys Pharmaceuticals
A Practical Approach to Leukopenia/Neutropenia in Children Vandy Black, M.D., M.Sc., FAAP OLOL Children s Hospital August 24, 2014 Disclosures EPIC trial MAST Therapeutics SUSTAIN trial Selexys Pharmaceuticals
CNS Infections in the Pediatric Age Group
 CNS Infections in the Pediatric Age Group Introduction CNS infections are frequently life-threatening In the Philippines, bacterial meningitis is one of the top leading causes of mortality in children
CNS Infections in the Pediatric Age Group Introduction CNS infections are frequently life-threatening In the Philippines, bacterial meningitis is one of the top leading causes of mortality in children
Pediatric and Adolescent Infectious Disease Concerns
 Pediatric and Adolescent Infectious Disease Concerns Sean P. Elliott, MD Professor of Pediatrics Associate Chair of Education, Department of Pediatrics University of Arizona College of Medicine Tucson,
Pediatric and Adolescent Infectious Disease Concerns Sean P. Elliott, MD Professor of Pediatrics Associate Chair of Education, Department of Pediatrics University of Arizona College of Medicine Tucson,
ID Emergencies. BGSMC Internal Medicine Edwin Yu
 ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
Estimating RSV Disease Burden in the United States
 Estimating RSV Disease Burden in the United States Brian Rha, MD, MSPH Medical Epidemiologist, Division of Viral Diseases Centers for Disease Control and Prevention Severe Acute Respiratory Infection Surveillance
Estimating RSV Disease Burden in the United States Brian Rha, MD, MSPH Medical Epidemiologist, Division of Viral Diseases Centers for Disease Control and Prevention Severe Acute Respiratory Infection Surveillance
MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
 MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSP There are no translations available. MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSP There are no translations available. MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
4/11/2017. A Review of How to Treat Common Infections in a Pediatric Patient. Disclaimer. Objectives for Pharmacists
 A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland, Pharm D. PGY2 Pediatric Pharmacy Resident Tara-bergland@uiowa.edu Disclaimer Tara Bergland reports that she has no actual
A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland, Pharm D. PGY2 Pediatric Pharmacy Resident Tara-bergland@uiowa.edu Disclaimer Tara Bergland reports that she has no actual
Pediatric Infectious Disease Concerns in Primary Care
 Pediatric Infectious Disease Concerns in Primary Care Sean P. Elliott, MD Professor of Pediatrics Associate Chair of Education, Department of Pediatrics University of Arizona College of Medicine Tucson,
Pediatric Infectious Disease Concerns in Primary Care Sean P. Elliott, MD Professor of Pediatrics Associate Chair of Education, Department of Pediatrics University of Arizona College of Medicine Tucson,
National Survey on the Impact of Viral Testing for the ED and Inpatient Management of Febrile Young Infants
 RESEARCH ARTICLE National Survey on the Impact of Viral Testing for the ED and Inpatient Management of Febrile Young Infants Brett Burstein, MD CM, PhD, a Alexander Sasha Dubrovsky, MD CM, MSc, a Andrew
RESEARCH ARTICLE National Survey on the Impact of Viral Testing for the ED and Inpatient Management of Febrile Young Infants Brett Burstein, MD CM, PhD, a Alexander Sasha Dubrovsky, MD CM, MSc, a Andrew