THE USE OF TRIPLE THERAPY IN SPECIAL POPULATIONS (HIV, OLT)
|
|
|
- Godwin Reynard Daniels
- 5 years ago
- Views:
Transcription



1 Massimo Puoti Dept. of Infectious Diseases AO Ospedale Niguarda Cà Granda Milan, Italy THE USE OF TRIPLE THERAPY IN SPECIAL POPULATIONS (HIV, OLT) 14 TH AISF Pre-meeting course: HCV treatment: the new scenario in the era of Direct-acting Antiviral Agents (DAAs) Rome February 22 nd 2012 Aula Magna Università di Roma Sapienza. P.le A. Moro 5 Course Directors: R. Bruno, Pavia and P. Caraceni, Bologna
2 Massimo Puoti SC MALATTIE INFETTIVE AO OSPEDALE NIGUARDA, Ca GRANDA MILANO Il sottoscritto dichiara di aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione per collaborazioni occasionali come: advisor o relatore in own events o docente in corsi per personale interno o percettore di grants di ricerca o investigator in RCT con: MSD, JANSSEN CILAG, ROCHE, GILEAD SCIENCES, BMS, BOEHRINGER INGELHEIM, e che la presentazione contiene discussione di farmaci in studio o ad uso off-label Boceprevir, Telaprevir, Daclatasvir, TMC-435, BI ,ITX 5061
3 The use of triple therapy in special populations: HIV and OLT Challenges: Two unmet medical needs: High HCV prevalence Accelerated progression of chronic Hep C significant cause of reduced survival Disappointing results with SOC Life sparing concurrent treatment with consistent DDI
4 The use of triple therapy in HIV+ Rationale DDI Studies Provisional clinical guidelines
5 The use of triple therapy in HIV+ Rationale DDI Studies Provisional clinical guidelines


6 Causes of death in the Swiss HIV Cohort study Ruppik M. et al. Changing patterns of causes of death in the SHCS CROI Poster # 789. Available at:
 Overall Mortality 3.12 (2.16,4.37) 0.23 (0.01,1.27) 1.65 (0.98,2.16) Liver-Related Mortality 4.33 (3.16,5.8) 0.23 (0.01,1.27) 0 (0,0.84) Liver Decompensation 0.83 (0.38,1.")
7 Achieving Sustained Virologic Response: Impact on Long-Term Outcomes in HIV/HCV-Coinfection GESIDA 3603 Cohort: 711 pts treated for HCV Long-Term Outcome Rate (per 100 person/years) 0.46* (0.06,1.65) Overall Mortality 3.12 (2.16,4.37) 0.23 (0.01,1.27) 1.65 (0.98,2.16) Liver-Related Mortality 4.33 (3.16,5.8) 0.23 (0.01,1.27) 0 (0,0.84) Liver Decompensation 0.83 (0.38,1.58) Hepatocarcinoma 0 (0,0.84) 1.02 (0.50,1.82) Liver Transplantation Achieved SVR Did not achieve SVR 0.23 (0.01,1.27) 0.93 (0.44,1.70) New AIDS Conditions *P=0.003, P=0.028, P<0.001, and P=0.034 versus not attaining a sustained virologic response. n=711 HIV/HCV-coinfected patients receiving interferon (peg or conventional) + ribavirin. Berenguer J. et al. Hepatology 2009.
 HCV-RNA+ 2257 out of 3177 tested: 71%")


8 Prevalence of HCV genotypes in patients from the MASTER COHORT (stratified by the date of 1st HIV Ab+) HCV-RNA out of 3177 tested: 71% Prevalence (%) Distribution of HCV G1 subtypes HCV Genotype 1a: 59% HCV Genotype 1b: 27% HCV G1 not subtyped or mixed: 13% G: genotype Year Presented by G. Carosi at the 7th International Workshop on HIV & Hepatitis Co-infection, June
9 Summary of Results From Coinfection Trials Study N Treatment SVR (%) All GT 1 GT non-1 RIBAVIC 412 PEG IFN α-2b + RBV * 44 IFN α-2b + RBV ACTG 133 PEG IFN α 2a + RBV IFN α -2a + RBV APRICOT 860 PEG IFN α 2a + RBV IFN α -2a + RBV LAGUNO 93 PEG IFN α-2b + W/B RBV IFN α-2b + W/B RBV PRESCO 389 PEG IFN α-2a + W/B RBV G1 48 w 31 72w 52 G2 24 w 67 48w 82
10 The use of triple therapy in HIV+ Rationale Liver diseases are the 1 st cause of death in HIV+ SVR is associated with reduced mortality HCV G1 is the most prevalent in Italy SVR after SOC in HIV/HCV is disappointing ( 14-39%)
11 The use of triple therapy in HIV+ Rationale DDI Studies Provisional clinical guidelines
12 Characteristics of New anti HCV drugs potential for DDI with antiretrovirals Directly Acting Antivirals (DAA) Host proteins Targeted Antivirals (HTA) Class 1 st Gen NS3 inhib. 2 nd Gen NS3 inhib. 3 rd Gen NS3 Inhib. Nuc NS 5B inhib 1 st gen. Nuc NS5B inhib. 2 nd gen No Nuc NS5B inhib. NS5A inhib. Cycl ophi llin Inhi bi. Intefe ron lambd a NRTI DDI with Antiretrovirals NNRTI PI RAL
13 Pharmacokinetic Interactions Between Telaprevir and Antiretrovirals TVR dose ARV TVR AUC TVR C min ARV AUC ARV C min TVR 750mg tid ATV/r 0.80 ( ) 0.85 ( ) 1.17 ( ) 1.85 ( ) DRV/r 0.65 ( ) 0.68 ( ) 0.60 ( ) 0.58 ( ) FPV/r 0.68 ( ) 0.70 ( ) 0.53 ( ) 0.44 ( ) LPV/r 0.46 ( ) 0.48 ( ) 1.06 ( ) 1.14 ( ) RAL ( ) 1.78 ( ) TVR 1125mg tid EFV TDF 0.82 ( ) 0.75 ( ) 0.82 ( ) 1.10 ( ) 0.90 ( ) 1.17 ( ) TVR 1500mg bid EFV TDF 0.80 ( ) 0.52 ( ) 0.85 ( ) 1.10 ( ) 0.89 ( ) 1.06 ( ) ARV: antiretroviral; ATV: atazanavir; DRV: darunavir; EFV: efavienz FPV: fosamprenavir; LPV: lopinavir; r: ritonavir; TDF: tenofovir van Heeswijk R, et al. 51st ICAAC Abstract A1-1738a van Heeswijk R, et al. CROI Abstract 119
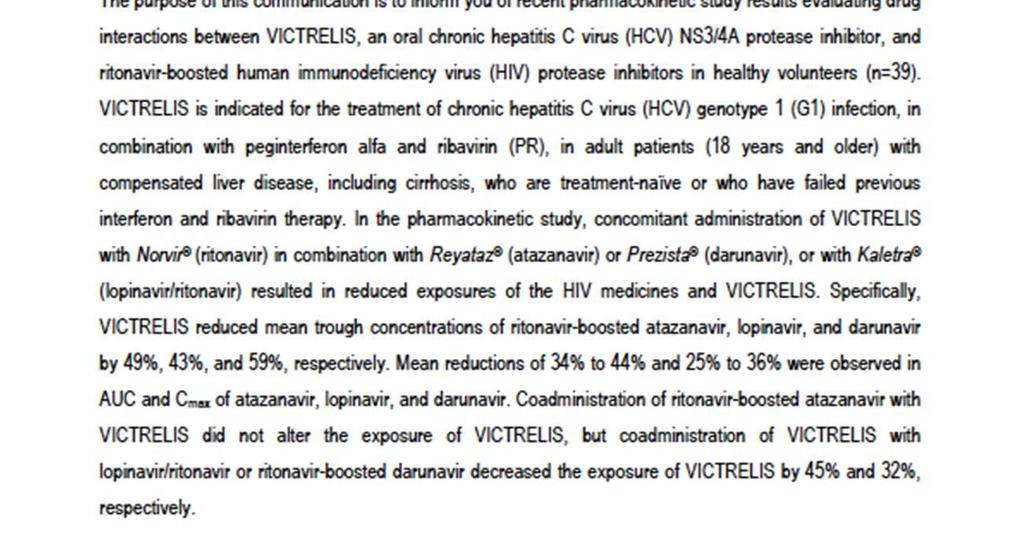
14 Pharmacokinetic Interactions Between Boceprevir 800 mg tid and Antiretrovirals ARV BOC AUC BOC C max BOC C min ARV AUC ARV C max ARV C min ATV/r Unchanged Not reported Unchanged - 49% DRV/r - 32% Not reported Not reported % % - 59% LPV/r - 45% Not reported Not reported - 43% EFV (90% CI) - 19% (11-25) -8% ( ) - 44% (26-58) + 20% (15-26) +11% (2-20) Not reported TDF +8% (2-14%) +5% (- 2+12) Not reported +5% (1-9)* +32% (19-45%) Not reported RAL Unchanged? ARV: antiretroviral; ATV: atazanavir; DRV: darunavir; EFV: efavienz FPV: fosamprenavir; LPV: lopinavir; r: ritonavir; TDF: tenofovir Modified from Kassera C, et al. CROI Abstract 118 and MSD Dear Doctor letter February 6th 2012
15
16 The use of triple therapy in HIV+ Rationale DDI Liver diseases are the 1 st cause of death in HIV+ SVR is associated with reduced mortality HCV G1 is the most prevalent in Italy SVR after SOC in HIV/HCV is disappointing ( 14-39%) There are major DDI with antiretrovirals: Treatment with BOC is not indicated in HIV+ ARV drugs use is restricted in candidates for Telaprevir; Telaprevir dose adjustment is required with EFV
17 The use of triple therapy in HIV+ Rationale DDI Studies Provisional clinical guidelines



18 Phase 2 studies with HCV PI in HIV/HCV Naggie S et al. Submitted 2011
19 Studies with DAA in HIV+ Efficacy
20 Virologic Breakthroughs Boceprevir 1 Telaprevir 2 HIVRNA breakthrough 2 on placebo 2 on ATZ/RTV None HCVRNA breakthrough None 7 patients EFV 4 out of 16 at weeks 4 (n=1), 8 (1), 12 (2) ATZ /RTV 3 out of 15 at weeks 4 (1), 8 (1), 12 (1) 1. Sulkowski M et al. IDSA Sherman KE et al. AASLD 2011
 n/n= 3/34 3/64 5/34 24/64 8/32 35/62 11/32")

21 Boceprevir in HCV/HIV co-infection: undetectable HCV RNA over time PR BOC/PR Patients with undetectable HCV RNA (%) n/n= 3/34 3/64 5/34 24/64 8/32 35/62 11/32 43/61 At TW12, there were no marked differences in CD4 count or % of subjects with HIV RNA <50 copies/ml in the treatment groups Sulkowski M, et al. IDSA 2011: Abstract LB-37
 T/PR PR T/PR PR n/n= 5/7 12/16 9/15 0/6 0/8 0/8 4/7 12/16 7/15 0/6 0/8 0/8")

22 Telaprevir in HCV/HIV co-infection: RVR and ervr by ART regimen No ART EFV+TDF+FTC ATV/r+TDF+FTC 68 RVR 61 ervr Patients (%) T/PR PR T/PR PR n/n= 5/7 12/16 9/15 0/6 0/8 0/8 4/7 12/16 7/15 0/6 0/8 0/8 RVR: rapid virologic response=undetectable HCV RNA at Week 4 ervr: extended rapid virologic response=undetectable HCV RNA at Weeks 4 and 12 Sherman KE, et al. Hepatology 2011;54(Suppl. S1): Abstract LB-8


23 Telaprevir + PR vs PR in HIV+: interim analysis at 4 and 12 weeks vs data from phase III Illuminate trial in HIV Sulkowski M et al. CROI 2011 abs 146LB
 55 (12/22) P=0.")

24 Telaprevir in HCV/HIV co-infection: undetectable HCV RNA at Week 24 by ART regimen No ART EFV+TDF+FTC ATV/r+TDF+FTC 71 (27/38) 55 (12/22) P=0.5 Patients with undetectable HCV RNA (%) T/PR PR n/n= 6/7 11/16 10/15 2/6 4/8 6/8 Roche COBAS TaqMan HCV test v2.0, LLOQ=25 IU/mL, LOD=10 IU/mL Sherman KE, et al. Hepatology 2011;54(Suppl. S1): Abstract LB-8
25 Studies with DAA in HIV+ Safety
26 Boceprevir in HCV/HIV co-infection: patient disposition n (%) PR BOC/PR Treated 34 (100) 64 (100) Discontinued during treatment phase Due to AE Due to treatment failure 14 (41) 3 (9) 11 (32) 16 (25)* 9 (14) 3 (5) Completed treatment phase 1 (3) 2 (3) Ongoing 19 (56) 46 (72) *Four subjects in the BOC/PR group discontinued treatment for reasons unrelated to AE or treatment failure; AE: adverse event Sulkowski M, et al. IDSA 2011: Abstract LB-37
27 Boceprevir in HCV/HIV co-infection: most common AEs with a difference of 10% between groups* % PR (n=34) BOC/PR (n=64) Neutropenia 3 13 Dysgeusia Vomiting Pyrexia Headache Decreased appetite *A difference of 10% for patients in the BOC/PR group when compared with PR Sulkowski M, et al. IDSA 2011: Abstract LB-37
28 Boceprevir in HCV/HIV co-infection: summary of hematologic AEs n (%) PR (n=34) BOC/PR (n=64) Anemia AEs Serious AEs AEs leading to discontinuation Grade 2 (8.0 to <9.5 g/dl) Grade 3 (6.5 to <8.0 g/dl) Erythropoietin use Transfusions Neutropenia AEs Grade 3 (<0.75 x 10 9 /L) Grade 4 (<0.5 x 10 9 /L) 9 (26) 2 (6) 1 (3) 7 (21) 1 (3) 7 (21) 2 (6) 1 (3) 3 (9) * 19 (30) 1 (2) 1 (2) 10 (16) 3 (5) 17 (27) 4 (6) 8 (13) 10 (16) * *To maintain blinding in this continuing study, the table only shows data where events occurred in 1 patient in each treatment group Sulkowski M, et al. IDSA 2011: Abstract LB-37
29 Telaprevir in HCV/HIV co-infection: SAEs and premature discontinuations Part A Part B No ART EFV+TDF+FTC ATV/r+TDF+FTC n PR (n=6) T/PR (n=7) PR (n=8) T/PR (n=16) PR (n=8) T/PR (n=15) SAEs* Reason for discontinuation Discontinuation due to HCV futility rule, n Discontinuation of TVR only due to AE, n (due to jaundice) Discontinuation of all study drugs due to AE (overall treatment phase), n Due to cholelithiasis Due to hemolytic anemia *One additional patient had an SAE of pneumococcal pneumonia reported after the Week 4 safety follow-up visit Reported as severe AE, occurred at Week 3; Patient had Grade 3 hemoglobin, also experienced Grade 4 hemoglobin (SAE of hemolytic anemia); AE: adverse event; SAE: serious AE Sherman KE, et al. Hepatology 2011;54(Suppl. S1): Abstract LB-8
30 Telaprevir in HCV/HIV co-infection: most common AEs PR (n=22) T/PR (n=38) Any AE, % Most common AEs,* % Fatigue Pruritus 9 39 Headache Nausea Rash Diarrhea Dizziness Pyrexia 9 21 Depression 9 21 Neutropenia Anemia Vomiting 9 18 Myalgia Chills Insomnia Decreased appetite Weight decreased *Regardless of severity and reported in 15% of patients in total T/PR or PR groups during overall treatment phase Grouped term for related dermatologic AEs, no severe rashes were reported Grouped term for related anemia AEs, 4 patients (1 Part A, 3 Part B) received an erythropoietin-stimulating agent Pruritus, headache, nausea, rash, pyrexia, depression, insomnia, decreased weight and abdominal pain occurred with >10% higher frequency in T/PR vs PR group Bilirubin AEs with ATV/r more frequent in T/PR vs PR groups (27% vs 0%, respectively) Hyper-bilirubinemia was primarily unconjugated Sherman KE, et al. Hepatology 2011;54(Suppl. S1): Abstract LB-8
31 Telaprevir in HCV/HIV co-infection: pharmacokinetics Telaprevir pharmacokinetics were comparable across ART regimens Pharmacokinetics of ARVs showed modest changes when co-administered with T/PR Ratio to reference (%) TVR pharmacokinetics* EFV-based ART ATV/r-based ART C min C avg C max ART pharmacokinetics (C min ) PR T/PR ATV EFV Tenofovir (given with EFV) Tenofovir (not given with EFV) *Ratio of mean concentration with ART (test) versus no ART (reference) Ratio of median C min after (test) versus before (reference) anti-hcv treatment ARV: antiretrovrial; C min : minimum plasma concentration; C avg : average plasma concentration C max : maximum plasma concentration Sherman KE, et al. Hepatology 2011;54(Suppl. S1): Abstract LB-8
32 Summary: studies with boceprevir or telaprevir in HCV/HIV co-infection HCV-HIV co-infected naïve patients had higher rates of HCV response with BOC/PR and TPV/PR compared to PR alone Preliminary safety data in co-infected patients showed a profile consistent with that observed in mono-infected patients No unexpected trends in CD4 counts or HIV RNA level Sulkowski M, et al. IDSA 2011: Abstract LB-37 Sherman KE, et al. Hepatology 2011;54(Suppl. S1): Abstract LB-8
33 The use of triple therapy in HIV+ Rationale DDI Studies Provisional clinical guidelines

34 Antiretroviral therapy in candidates for PEG IFN + RBV + TPV. BOCEPREVIR IS NOT INDICATED FOR USE IN PATIENTS WHO ARE INFECTED WITH BOTH HIV-1 AND CHRONIC HCV. CLASS Antiretrovirals TELAPREVIR NRTI AZT, ddi, d4t Avoid coadministration ABC: No data Potential interaction with UDP-glucuronyl tranferase TDF FTC, LAM. No Data but no potential interactions Combine with caution Can be combined Can be combined PI LPV/R, DRV/R, FPV/R, Avoid coadministration ATZ/R Can be combined NNRTI EFV 1125 mg tid NVP RPV ETV: Data expected soon on ETV and RPV Avoid coadministration II RAL Can be combined
35 Telaprevir: Treatment schedule in HIV+ 750 mg (two 375-mg tablets) q8hr with food (not low fat; standard fat meal is 21 g) If on Efavirenz based ART :1125 (three 375-mg tablets) q 8 hr with food ( not low fat; standard fat meal is 21g) TVR + PR PR ervr: HCVRNA undetectable at 4 & 12 weeks: useful to reinforce patients adherence but not for Response Guided Therapy Time Point Criterion Stopping Rule Wk 4 or 12 HCV RNA > 1000 IU/mL Discontinue all therapy Wk 24 Detectable HCV RNA Discontinue PR Any Discontinuation of PR for any reason Discontinue TVR Telaprevir [package insert]. May EMA. Telaprevir [package insert] 2011.
36 Il 28 b SNP and RVR as predictors of SVR in 64 HIV/HCV G1 pts (54 with RVR) IL28 b Rs RVR NO/all (% 95% CI) All 48/54 (89%; 85-93%) AA 4/14 (29%; 16-40%) AG & GG 2/34 (6%;2-10%) All 6/48 (12%; 8-17%) Rate of SVR RVR YES/all ( % ; 95% CI) 6/54 (11%; 7-15%) 3/3 (100%) 2/3 (67%; 39-94%) 5/6 (83% 68-99%) ALL (%; 95% CI) 8/20 (40%; 29-51%) 4/44 (9%; 5-13%) 12/64 (19%; 14-24%) Puoti M et al. 45 th AISF annual meeting Poster n. 45 February 24 th 2012
37 Management of HIV-HCV coinfected genotype-1 patients according to fibrosis stage and prior treatment outcome: a proposal * Lead in phase Fbrosis stage IL28 & RVR Naïve Experienced Relapsers Partial responders Null responders Undefined F0-F1 At least one predictor P+R Consider P+R+T Defer Defer Defer No Predictors Defer F2-F3 RVR* P+ R P+R+T No RVR F4 Lead in HCVRNA decrease >1 Log Lead in HCVRNA decrease <1 Log P+R+T P+R+T* Defer
38 HIV/HCV studies with Boceprevir on clinical.trial.gov Drug ID Sponsor Design Target population N of subjects (status on Feb ) Boceprevir NCT NIAID Open uncontrolle d Boceprevir NCT NIAID Controlled vs HIV- Boceprevir NCT ARNS Open uncontrolle d Naives + Experienced Naives HIV+ vs Naives HIV- 310 (not yet recruiting) 200 (recruiting) Experienced 80 (recruiting)
39 HIV/HCV studies with Telaprevir in HIV on clinical.trial.gov Drug ID Sponsor Design Target population N of subjects (status on Feb ) Telaprevir NCT VX Vertex Open uncontrolle d (1125 mg bid or tid with EFV) Naïve Experienced 160 (recruiting) Telaprevir NCT VX- 950HPC3008 Tibotec Open uncontrolle d Naïve Experienced 150 (recruiting) Telaprevir NCT VX- 950HPC3005 Janssen Cilag Open uncontrolle d Naïve Experienced F3 F4 500 (recruiting)
40 HIV/HCV studies with other DAA on clinical.trial.gov Drug ID Sponsor Design Target population N of subjects (status on Feb ) TMC435 NCT TMC435- TiDP16-C212 Tibotec Open uncontroled? 100 BI NCT Boehringer Randomized( 12 vs 24 w) Daclatasvir (BMS ) NCT AI BMS Open Uncontrolled Naïve Relapsers 316 Naive 300
41 Rationale DDI Triple therapy in HIV+ Liver diseases are the 1 st cause of death in HIV+ SVR is associated with reduced mortality HCV G1 is the most prevalent in Italy SVR after SOC in HIV/HCV is disappointing ( 14-39%) There are major DDI with antiretrovirals: Treatment with BOC is not indicated in HIV+ ARV drugs use is restricted in candidates for Telaprevir and TPV dose should be increased with EFV Preliminary data HCV-HIV co-infected patients who were previously untreated had higher rates of HCV response with BOC/PR and TPV/PR compared to PR alone Preliminary safety data in co-infected patients showed a profile consistent with that observed in mono-infected patients No unexpected trends in CD4 counts or HIV RNA level Provisional guidelines for use Usage of TPV in selected HIV coinfected patients with adjusted ART possibly in clinical studies
42 The use of triple therapy in OLT Rationale DDI Study
43 The use of triple therapy in OLT Rationale DDI Study




44 N. of adults with 1 st LT: 1204; Non viral indications : 436

45 Outcome of HCV post-transplant Gane E LT 2008;14:S36-44.
46 Natural History of Recurrent HCV Decompensation in Recurrent Cirrhosis Rate of Decompensation 100% 75% 50% 25% 0% *Once cirrhosis present in allograft 3 y survival < 10% 42% 4% 62% 9% Years Recurrent HCV-cirrhosis Berenguer, 2000 Non-transplant HCV-cirrhosis Fattovich, 1997
47 Rationale for DAAs treatment of recurrent chronic hep C in liver transplant recipients HCV infection remains the most common indication for orthotopic Liver Transplantation in Italy Most patients are viremic at time of liver transplantation Hepatitis C recurrence after OLTx is universal and results in accelerated progression of fibrosis to cirrhosis in 20% at 5 years and 50% at 10 years Allograft HCV recurrence with subsequent liver failure is the one of the most common reason for decreased allograft survival in HCV infected patients HCV genotype 1 is the most common genotype in Italy 47
48 The use of triple therapy in OLT Rationale DDI Study



49 49
50 Pharmacokinetic Interactions Between Telaprevir and Immunosuppressants Telaprevir is expected to have a significant effect on both cylcosporine and tacrolimus as they are substrates of CYP3A and P-gp 1 Calcineurin Inhbitor Cyclosporine Tacrolimus C max AUC t 1/2 1.3-fold increase 9.4-fold increase 4.6-fold increase 70-fold increase From hours From hours Single doses of cyclosporine or tacrolimus had no major effect on telaprevir pharmacokinetics According to Drug metabolism interaction with sirolimus and everolimus could be expected C max : maximum plasma concentration Garg et al Hepatology 2011; 54: 20-7
51 The use of triple therapy in OLT Rationale DDI Study
52 Preliminary data from a pilot study on efficacy and safety of TPV based triple therapy of Hep C recurrence in Liver transplant recipients Study population 7 LT recipients with HCV recurrence 3mo - 6 yrs post Tx aged yrs; 1/7 F4 6/7 F0-2 Immunosuppressive therapy: TAC ½ of pre Tx dose once weekly with TDM every other day in first 2 weeks. TAC dose resumed 5 days after Telaprevir withdrawal with gradual escalation Schedule of Anti HCV Tx 6/7 triple therapy; 1/7 TPV add on PEG (6: 2a; 1: 2b) + RBV mg/d 52Mantry PS et al Global Antiviral Journal, Volume 7, Suppl. 1 (HEPDART 2011) : 90
53 Preliminary data from a pilot study on efficacy and safety of TPV based triple therapy of Hep C recurrence in Liver transplant recipients Efficacy: 1 NR + 4/7 ervr + 2/7 cevr Safety: 1 deceased ( Pneumonia + ARDS) with 3 hospitalization and 4 transfusion 3 at least 1 hospitalization ( 2 infections: 2 UTI 1 with sepsis) 5/7 blood transfusions ( 2 or more) Conclusions: TAC dose adjustment with intensive monitoring no toxicity or rejection Rapid HCV suppression Substantial side effects should be discussed with pts. 53Mantry PS et al Global Antiviral Journal, Volume 7, Suppl. 1 (HEPDART 2011) : 90
54 HIV/HCV studies with DAA in Liver Transplant Recipients Drug ID Sponsor Design Target population N of subjects (status on Feb ) ITX 5061 (HCV entry inhibitor) NCT University of Birmingham Phase I Open Label Liver transplant recipients 20 Telaprevir NCT VX Vertex Phase II Open Label 1125 bid Stable LT recipients assuming Sirolimus + PDN 75 Boceprevir ANRS HC 29 BOCEPRETRAN SPLANT ANRS Phase II Open Label Cirrhosis LT candidates MELD < 18 64
55 Triple therapy in OLT Rationale DDI HCV infection most common indication for OLT in Italy Universal Hepatitis C recurrence with accelerated progression to cirrhosis and significantly deceased allograft survival HCV genotype 1 is the most common genotype in Italy Significant DDI with calcineurin and mtor inhibitors: calcineurin dose adjustments as in HIV+ OLT taking Pi based ART Study No data to define any provisional guideline Studies with careful surveillance for safety are urgently needed
Treatment of chronic hepatitis C in HIV co-infected patients
 Treatment of chronic hepatitis C in HIV co-infected patients Vicente Soriano Department of Infectious Diseases Hospital Carlos III, Madrid, Spain The most prevalent chronic viral infections in humans HBV
Treatment of chronic hepatitis C in HIV co-infected patients Vicente Soriano Department of Infectious Diseases Hospital Carlos III, Madrid, Spain The most prevalent chronic viral infections in humans HBV
Treatment of chronic hepatitis C in drug-naïve patients
 Treatment of chronic hepatitis C in drug-naïve patients 8th International Workshop on HIV & Hepatitis Co-infection Madrid, 31. May 2012 Christoph Sarrazin J. W. Goethe-University Hospital Medizinische
Treatment of chronic hepatitis C in drug-naïve patients 8th International Workshop on HIV & Hepatitis Co-infection Madrid, 31. May 2012 Christoph Sarrazin J. W. Goethe-University Hospital Medizinische
47 th Annual Meeting AISF
 47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
Massimo Puoti Dept. of Infectious Diseases AO Ospedale Niguarda Cà Granda Milan, Italy. Treatment with DDA in special populations
 Massimo Puoti Dept. of Infectious Diseases AO Ospedale Niguarda Cà Granda Milan, Italy Treatment with DDA in special populations Massimo Puoti. SC Malattie Infettive AO Ospedale Niguarda Ca Grnada Il sottoscritto
Massimo Puoti Dept. of Infectious Diseases AO Ospedale Niguarda Cà Granda Milan, Italy Treatment with DDA in special populations Massimo Puoti. SC Malattie Infettive AO Ospedale Niguarda Ca Grnada Il sottoscritto
Antiviral agents in HCV
 Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Rome, February nd Riunione Annuale AISF th AISF ANNUAL MEETING
 Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Provisional Guidance on the Use of Hepatitis C Virus Protease Inhibitors for Treatment of Hepatitis C in HIV-Infected Persons
 INVITED ARTICLE HIV/AIDS Kenneth H. Mayer, Section Editor Provisional Guidance on the Use of Hepatitis C Virus Protease Inhibitors for Treatment of Hepatitis C in HIV-Infected Persons David L. Thomas,
INVITED ARTICLE HIV/AIDS Kenneth H. Mayer, Section Editor Provisional Guidance on the Use of Hepatitis C Virus Protease Inhibitors for Treatment of Hepatitis C in HIV-Infected Persons David L. Thomas,
Treatment of Chronic Hepatitis C in HIV infection
 Treatment of Chronic Hepatitis C in HIV infection June 25, 211 Andrew Talal, MD, MPH Associate Professor of Medicine Associate Medical Director Center for the Study of Hepatitis C Weill Cornell Medical
Treatment of Chronic Hepatitis C in HIV infection June 25, 211 Andrew Talal, MD, MPH Associate Professor of Medicine Associate Medical Director Center for the Study of Hepatitis C Weill Cornell Medical
Protease inhibitor based triple therapy in treatment experienced patients
 Protease inhibitor based triple therapy in treatment experienced patients Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
Protease inhibitor based triple therapy in treatment experienced patients Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
HIV and Hepatitis C: Advances in Treatment
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and Hepatitis C: Advances in Treatment John Scott, MD, MSc Asst Professor University of Washington Presentation prepared & presented by: John Scott, MD,
NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and Hepatitis C: Advances in Treatment John Scott, MD, MSc Asst Professor University of Washington Presentation prepared & presented by: John Scott, MD,
Telaprevir in Combination with Peginterferon Alfa-2a/Ribavirin in HCV/HIV Co-infected Patients: A 24-Week Treatment Interim Analysis
 Poster LB-8 Telaprevir in Combination with Peginterferon Alfa-2a/Ribavirin in HCV/HIV Co-infected Patients: A 24-Week Treatment Interim Analysis KE Sherman 1, JK Rockstroh 2, DT Dieterich 3, V Soriano
Poster LB-8 Telaprevir in Combination with Peginterferon Alfa-2a/Ribavirin in HCV/HIV Co-infected Patients: A 24-Week Treatment Interim Analysis KE Sherman 1, JK Rockstroh 2, DT Dieterich 3, V Soriano
Bristol-Myers Squibb. HCV Full Development Portfolio Overview. Richard Bertz Int Workshop CP HIV Meeting Amsterdam, Netherlands 24 April 2013
 Bristol-Myers Squibb HCV Full Development Portfolio Overview Richard Bertz Int Workshop CP HIV Meeting Amsterdam, Netherlands 24 April 2013 1 BMS Agents in Clinical Development: DAAs and INF Lambda Lambda
Bristol-Myers Squibb HCV Full Development Portfolio Overview Richard Bertz Int Workshop CP HIV Meeting Amsterdam, Netherlands 24 April 2013 1 BMS Agents in Clinical Development: DAAs and INF Lambda Lambda
Pierluigi Toniutto Clinica di Medicina Interna Azienda Ospedaliero Universitaria Udine
 Pierluigi Toniutto Clinica di Medicina Interna Azienda Ospedaliero Universitaria Udine Il sottoscritto dichiara di non aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Pierluigi Toniutto Clinica di Medicina Interna Azienda Ospedaliero Universitaria Udine Il sottoscritto dichiara di non aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Treatment of Hepatitis C in HIV-Coinfected Patients. Vincent Soriano Department of Infectious Diseases Hospital Carlos III Madrid, Spain
 Treatment of Hepatitis C in HIV-Coinfected Patients Vincent Soriano Department of Infectious Diseases Hospital Carlos III Madrid, Spain Estimated no. of persons infected with HIV and hepatitis viruses
Treatment of Hepatitis C in HIV-Coinfected Patients Vincent Soriano Department of Infectious Diseases Hospital Carlos III Madrid, Spain Estimated no. of persons infected with HIV and hepatitis viruses
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
Evolution of Therapy in HCV
 Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Clinical Pharmacology of DAA s for HCV: What s New & What s In Pipeline
 Clinical Pharmacology of DAA s for HCV: What s New & What s In Pipeline Kirk Bertelsen, PhD Clinical Pharmacology Janssen Pharmaceuticals, Research & Development 4/24/2013 1 Incivo Simeprevir 2 Janssen
Clinical Pharmacology of DAA s for HCV: What s New & What s In Pipeline Kirk Bertelsen, PhD Clinical Pharmacology Janssen Pharmaceuticals, Research & Development 4/24/2013 1 Incivo Simeprevir 2 Janssen
Treatment with the New Direct Acting Antivirals for Hepatitis C
 Treatment with the New Direct Acting Antivirals for Hepatitis C Mary Olson, DNP, ANP-BC Clinical Trials Program Director Weill Cornell Medical College The Center for the Study of Hepatitis C Objectives
Treatment with the New Direct Acting Antivirals for Hepatitis C Mary Olson, DNP, ANP-BC Clinical Trials Program Director Weill Cornell Medical College The Center for the Study of Hepatitis C Objectives
CURRENT TREATMENTS. Mitchell L Shiffman, MD Director Liver Institute of Virginia. Richmond and Newport News, VA, USA
 CURRENT TREATMENTS FOR HCV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA Liver Institute of Virginia Education, Research and
CURRENT TREATMENTS FOR HCV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA Liver Institute of Virginia Education, Research and
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA. Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona
 Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
BOCEPREVIR (BOC): EVIDENCE FROM TRIALS
: EVIDENCE FROM TRIALS") BOCEPREVIR (BOC): EVIDENCE FROM TRIALS ROME, FEBRUARY 22 nd -25 th, 212 Savino Bruno, MD Department of Internal Medicine A.O. Fatebenefratelli e Oftalmico Milan, Italy Savino Bruno, MD Director of InternalMedicine,
BOCEPREVIR (BOC): EVIDENCE FROM TRIALS ROME, FEBRUARY 22 nd -25 th, 212 Savino Bruno, MD Department of Internal Medicine A.O. Fatebenefratelli e Oftalmico Milan, Italy Savino Bruno, MD Director of InternalMedicine,
Hepatitis C Treatment 2014
 Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
ICVH 2016 Oral Presentation: 28
 Ledipasvir/Sofosbuvir Is Safe and Effective for the Treatment of Patients with Genotype 1 Chronic HCV Infection in Both HCV Mono- and HIV/HCV Coinfected Patients A Luetkemeyer 1, C Cooper 2, P Kwo 3, K
Ledipasvir/Sofosbuvir Is Safe and Effective for the Treatment of Patients with Genotype 1 Chronic HCV Infection in Both HCV Mono- and HIV/HCV Coinfected Patients A Luetkemeyer 1, C Cooper 2, P Kwo 3, K
Professor Massimo Puoti
 THIRD JOINT CONFERENCE OF BHIVA AND BASHH 2014 Professor Massimo Puoti Niguarda Ca Granda Hospital, Milan, Italy 1-4 April 2014, Arena and Convention Centre Liverpool THIRD JOINT CONFERENCE OF BHIVA AND
THIRD JOINT CONFERENCE OF BHIVA AND BASHH 2014 Professor Massimo Puoti Niguarda Ca Granda Hospital, Milan, Italy 1-4 April 2014, Arena and Convention Centre Liverpool THIRD JOINT CONFERENCE OF BHIVA AND
Hepatitis C: Management of Treatment Naïve Patients with First Line Protease Inhibitors
 Hepatitis C: Management of Treatment Naïve Patients with First Line Protease Inhibitors Eric Lawitz, MD, AGAF, CPI The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science
Hepatitis C: Management of Treatment Naïve Patients with First Line Protease Inhibitors Eric Lawitz, MD, AGAF, CPI The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science
Case #1. Case #1. Case #1: Audience vote VS. The Great Debate: When to Treat HCV in our HIV coinfected patients
 Case #1 The Great Debate: When to Treat HCV in our HIV coinfected patients Medical Management of AIDS December, 2012 Moderated by George Beatty,MD 35 year old African American man, CD4 + 450, HIV RNA
Case #1 The Great Debate: When to Treat HCV in our HIV coinfected patients Medical Management of AIDS December, 2012 Moderated by George Beatty,MD 35 year old African American man, CD4 + 450, HIV RNA
VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES
 VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES REGIMENES TERAPÊUTICOS DE LA HEPATITIS C, INTERFERÓN FREE A Coruña 2 Febrero 2013 Rui Sarmento e Castro Centro Hospitalar do Porto HJU ECS Universidade
VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES REGIMENES TERAPÊUTICOS DE LA HEPATITIS C, INTERFERÓN FREE A Coruña 2 Febrero 2013 Rui Sarmento e Castro Centro Hospitalar do Porto HJU ECS Universidade
ABCs of Hepatitis C: What s New. The Long-Awaited New Era: Protease Inhibitors for HCV Genotype 1
 ABCs of Hepatitis C: What s New ACG Postgraduate Course Washington, DC October 30, 2011 Ira M. Jacobson, M.D. Vincent Astor Professor of Medicine Chief, Division of Gastronterology and Hepatology Medical
ABCs of Hepatitis C: What s New ACG Postgraduate Course Washington, DC October 30, 2011 Ira M. Jacobson, M.D. Vincent Astor Professor of Medicine Chief, Division of Gastronterology and Hepatology Medical
How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy
 How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber- und Studienzentrum
How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber- und Studienzentrum
Introduction. The ELECTRON Trial
 63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
Understudied treatment populations: manage with care. Massimo Puoti Infectious Diseases Dept. AO Ospedale Niguarda Ca Granda Milan, Italy
 Understudied treatment populations: manage with care Massimo Puoti Infectious Diseases Dept. AO Ospedale Niguarda Ca Granda Milan, Italy Understudied treatment populations Cirrhotics Data from registrative
Understudied treatment populations: manage with care Massimo Puoti Infectious Diseases Dept. AO Ospedale Niguarda Ca Granda Milan, Italy Understudied treatment populations Cirrhotics Data from registrative
Current State of Treatment for HCV. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 Activity Code FA376 Current State of Treatment for HCV Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives Upon completion of this presentation, learners should be
Activity Code FA376 Current State of Treatment for HCV Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives Upon completion of this presentation, learners should be
HCV Case Study. Treat Now or Wait for New Therapies
 HCV Case Study Treat Now or Wait for New Therapies This program is supported by educational grants from Kadmon and Merck Pharmaceuticals. Program Disclosure This activity has been planned and implemented
HCV Case Study Treat Now or Wait for New Therapies This program is supported by educational grants from Kadmon and Merck Pharmaceuticals. Program Disclosure This activity has been planned and implemented
Treatment Targets HCV Genotype 1 & PIs Treating HCV G2&3 Future Therapies. Advances in treatment of HCV Dr John F Dillon
 Treatment Targets HCV Genotype 1 & PIs Treating HCV G2&3 Future Therapies Advances in treatment of HCV Dr John F Dillon Disclosure slide I have received consulting fees and Honoraria from MSD, Abbott,
Treatment Targets HCV Genotype 1 & PIs Treating HCV G2&3 Future Therapies Advances in treatment of HCV Dr John F Dillon Disclosure slide I have received consulting fees and Honoraria from MSD, Abbott,
Antiviral treatment in Unique Populations
 Antiviral treatment in Unique Populations Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Unique HCV Populations HIV/HCV co-infected
Antiviral treatment in Unique Populations Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Unique HCV Populations HIV/HCV co-infected
HIV Infection with HCV Future Directions
 HIV Infection with HCV Future Directions Dr Ranjababu (Babu) Kulasegaram Consultant Physician in HIV/GU Medicine Guy s and St Thomas NHS Foundation Trust London, UK Presenter disclosure information Dr
HIV Infection with HCV Future Directions Dr Ranjababu (Babu) Kulasegaram Consultant Physician in HIV/GU Medicine Guy s and St Thomas NHS Foundation Trust London, UK Presenter disclosure information Dr
Pazienti con Genotipo 1 e Cirrosi Scompensata, pre-/post-olt
 Monotematica AISF 2013 Pazienti con Genotipo 1 e Cirrosi Scompensata, pre-/post-olt Pietro Andreone Dipartimento di Scienze Mediche e Chirurgiche Alma Mater Studiorum, Università di Bologna Pisa, 17-19
Monotematica AISF 2013 Pazienti con Genotipo 1 e Cirrosi Scompensata, pre-/post-olt Pietro Andreone Dipartimento di Scienze Mediche e Chirurgiche Alma Mater Studiorum, Università di Bologna Pisa, 17-19
Latest Treatment Updates for GT 2 and GT 3 Patients
 Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Hepatitis C: Management of Previous Non-responders with First Line Protease Inhibitors
 Hepatitis C: Management of Previous Non-responders with First Line Protease Inhibitors Fred Poordad, MD The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science Center
Hepatitis C: Management of Previous Non-responders with First Line Protease Inhibitors Fred Poordad, MD The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science Center
HEPATITIS WEB STUDY. Treatment of Hepatitis C following Liver Transplantation
 HEPATITIS WEB STUDY Treatment of Hepatitis C following Liver Transplantation Terry D. Box, MD Associate Professor of Medicine Division of Gastroenterology/Hepatology University of Utah Health Sciences
HEPATITIS WEB STUDY Treatment of Hepatitis C following Liver Transplantation Terry D. Box, MD Associate Professor of Medicine Division of Gastroenterology/Hepatology University of Utah Health Sciences
Future strategies with new DAAs
 Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV?
 Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Highlights of AASLD 2012 CCO Official Conference Coverage of the 2012 Annual Meeting of the American Association for the Study of Liver Diseases
 Highlights of AASLD 12 CCO Official Conference Coverage of the 12 Annual Meeting of the American Association for the Study of Liver Diseases November 9-13, 12 Boston, Massachusetts In partnership with
Highlights of AASLD 12 CCO Official Conference Coverage of the 12 Annual Meeting of the American Association for the Study of Liver Diseases November 9-13, 12 Boston, Massachusetts In partnership with
Interferon Side Effects and The Future of Interferon Sparing Regimens. Todd Wills, MD ETAC Infectious Disease Specialist
 Interferon Side Effects and The Future of Interferon Sparing Regimens Todd Wills, MD ETAC Infectious Disease Specialist HEPATITIS C TREATMENT EXPANSION INITIATIVE MULTISITE CONFERENCE CALL FEBRUARY 15,
Interferon Side Effects and The Future of Interferon Sparing Regimens Todd Wills, MD ETAC Infectious Disease Specialist HEPATITIS C TREATMENT EXPANSION INITIATIVE MULTISITE CONFERENCE CALL FEBRUARY 15,
Efficacy and safety of protease inhibitors for sever hepatitis C recurrence after liver transplantation: a first multicentric experience
 Efficacy and safety of protease inhibitors for sever hepatitis C recurrence after liver transplantation: a first multicentric experience A. Coilly, B. Roche, J. Dumortier, D. Botta-Fridlund, V. Leroy,
Efficacy and safety of protease inhibitors for sever hepatitis C recurrence after liver transplantation: a first multicentric experience A. Coilly, B. Roche, J. Dumortier, D. Botta-Fridlund, V. Leroy,
Slide Presentation. Management of HCV Coinfection Susanna Naggie, MD, MHS
 Slide Presentation Management of HCV Coinfection Assistant Professor of Medicine Duke University School of Medicine & Durham VA Medical Center Director of Infectious Diseases Duke Clinical Research Institute
Slide Presentation Management of HCV Coinfection Assistant Professor of Medicine Duke University School of Medicine & Durham VA Medical Center Director of Infectious Diseases Duke Clinical Research Institute
Azienda ULSS12 Veneziana
 Azienda ULSS12 Veneziana Risultati del trattamento dei monoinfetti con Sofosbuvir, Simeprevir nella coorte veneziana. Confronto di esito con la coorte del trattamento con Boceprevir e Telaprevir Dr.ssa
Azienda ULSS12 Veneziana Risultati del trattamento dei monoinfetti con Sofosbuvir, Simeprevir nella coorte veneziana. Confronto di esito con la coorte del trattamento con Boceprevir e Telaprevir Dr.ssa
HCV: Beyond the current generation of protease inhibitors
 HCV: Beyond the current generation of protease inhibitors Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S. University of Palermo, Italy antonio.craxi@unipa.it Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S. University
HCV: Beyond the current generation of protease inhibitors Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S. University of Palermo, Italy antonio.craxi@unipa.it Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S. University
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
The HCV pipeline: Will IFN-free treatment be possible? Heiner Wedemeyer. Hannover Medical School Germany
 : Will IFN-free treatment be possible? Heiner Wedemeyer Hannover Medical School Germany Interferon-free regimens to treat hepatitis C What should be the goal of interferon-free treatment regimens: Sustained
: Will IFN-free treatment be possible? Heiner Wedemeyer Hannover Medical School Germany Interferon-free regimens to treat hepatitis C What should be the goal of interferon-free treatment regimens: Sustained
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE?
 IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
Bruce A. Luxon, MD, Ph.D. Anton and Margaret Fuisz Chair in Medicine Professor and Chair Department of Medicine Georgetown University
 Bruce A. Luxon, MD, PhD, FACG Bruce A. Luxon, MD, Ph.D. Anton and Margaret Fuisz Chair in Medicine Professor and Chair Department of Medicine Georgetown University Dr. Luxon is on the speakers p bureau
Bruce A. Luxon, MD, PhD, FACG Bruce A. Luxon, MD, Ph.D. Anton and Margaret Fuisz Chair in Medicine Professor and Chair Department of Medicine Georgetown University Dr. Luxon is on the speakers p bureau
Clinical Cases Hepatitis C Naïve Patients. Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona.
 Clinical Cases Hepatitis C Naïve Patients Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona. Case study 1 27 year old woman, Diagnosed with Chronic Hepatitis C 3 years ago
Clinical Cases Hepatitis C Naïve Patients Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona. Case study 1 27 year old woman, Diagnosed with Chronic Hepatitis C 3 years ago
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret
 New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
Predictors of Response to Hepatitis C Therapy in the DAA Era. Pablo Barreiro Servicio de Enfermedades Infecciosas Hospital Carlos III, Madrid
 Predictors of Response to Hepatitis C Therapy in the DAA Era Pablo Barreiro Servicio de Enfermedades Infecciosas Hospital Carlos III, Madrid Why Predicting HCV Response? Select candidates for therapy Prioritizing
Predictors of Response to Hepatitis C Therapy in the DAA Era Pablo Barreiro Servicio de Enfermedades Infecciosas Hospital Carlos III, Madrid Why Predicting HCV Response? Select candidates for therapy Prioritizing
Hepatitis C Virus Treatments: Present and Future
 Hepatitis C Virus Treatments: Present and Future Charles D. Howell, M.D., A.G.A.F Professor of Medicine University of Maryland School of Medicine Baltimore, MD Charles Howell Disclosures Boehringer Ingelheim,
Hepatitis C Virus Treatments: Present and Future Charles D. Howell, M.D., A.G.A.F Professor of Medicine University of Maryland School of Medicine Baltimore, MD Charles Howell Disclosures Boehringer Ingelheim,
New developments in HCV research and their implications for front-line practice
 New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
My HCV patient is co-infected with HIV: how to manage?
 EASL «White Nights of Hepatology 2016» My HCV patient is co-infected with HIV: how to manage? A.V. Кravchenko MD, Professor Russia AIDS Federal Center Central Research Institute of Epidemiology St.-Petersburg,
EASL «White Nights of Hepatology 2016» My HCV patient is co-infected with HIV: how to manage? A.V. Кravchenko MD, Professor Russia AIDS Federal Center Central Research Institute of Epidemiology St.-Petersburg,
Martel-Laferrière V, Brinkley S, Bichoupan K, Posner S, Stivala A, Perumalswami P, Schiano T, Sulkowski M, Dieterich DT, Branch AD
 On-treatment and Sustained Virologic Response Rates of Telaprevir-based HCV Treatments Do Not Differ Between HIV/HCV Co-infected and HCV Mono-infected Patients Martel-Laferrière V, Brinkley S, Bichoupan
On-treatment and Sustained Virologic Response Rates of Telaprevir-based HCV Treatments Do Not Differ Between HIV/HCV Co-infected and HCV Mono-infected Patients Martel-Laferrière V, Brinkley S, Bichoupan
HIV/HCV Co-Infection
 HIV/HCV Co-Infection 2015 Kentucky Conference on Viral Hepatitis Matt Cave, M.D. Associate Professor Department of Medicine Division of Gastroenterology, Hepatology, & Nutrition Department of Pharmacology
HIV/HCV Co-Infection 2015 Kentucky Conference on Viral Hepatitis Matt Cave, M.D. Associate Professor Department of Medicine Division of Gastroenterology, Hepatology, & Nutrition Department of Pharmacology
HIV Prevention. David Cooper, MD, DSc Director and Professor, Kirby Institute University of New South Wales Sydney, Australia
 HIV Prevention David Cooper, MD, DSc Director and Professor, Kirby Institute University of New South Wales Sydney, Australia HIV Care/Prevention Continuum Test Engage, Counsel, Monitor and Support Retain,
HIV Prevention David Cooper, MD, DSc Director and Professor, Kirby Institute University of New South Wales Sydney, Australia HIV Care/Prevention Continuum Test Engage, Counsel, Monitor and Support Retain,
Learning Objective. After completing this educational activity, participants should be able to:
 Learning Objective After completing this educational activity, participants should be able to: Use patient characteristics and preferences to select HCV treatment strategies that maximize the potential
Learning Objective After completing this educational activity, participants should be able to: Use patient characteristics and preferences to select HCV treatment strategies that maximize the potential
Tratamiento de la Hepatitis C Rafael Esteban Hospital General Universitario Valle de Hebrón Barcelona
 Tratamiento de la Hepatitis C Rafael Esteban Hospital General Universitario Valle de Hebrón Barcelona rrent HCV Therapy 8% % sustained response 6% 4% 2% % 54-61% 41% 34% 25% 16% 6% IFN 24w IFN 48w Peg
Tratamiento de la Hepatitis C Rafael Esteban Hospital General Universitario Valle de Hebrón Barcelona rrent HCV Therapy 8% % sustained response 6% 4% 2% % 54-61% 41% 34% 25% 16% 6% IFN 24w IFN 48w Peg
New Therapies on the Horizon in Hepatitis C Patients Paul Y. Kwo, MD
 Viral Targets for HCV New Therapies on the Horizon in Hepatitis C Patients Paul Y. Kwo, MD Sites for development of inhibitors Metalloproteinase Serine protease (trans) Core E E2 NS2 NS3 NS4a/NS4b NS5a/NS5b
Viral Targets for HCV New Therapies on the Horizon in Hepatitis C Patients Paul Y. Kwo, MD Sites for development of inhibitors Metalloproteinase Serine protease (trans) Core E E2 NS2 NS3 NS4a/NS4b NS5a/NS5b
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
SAVINO BRUNO, MD Director Internal Medicine and Hepatology Unit AO Fatebenefratelli e Oftalmico, Milano
 SAVINO BRUNO, MD Director Internal Medicine and Hepatology Unit AO Fatebenefratelli e Oftalmico, Milano Market wheretelaprevir has not yet launched Victrelis is still launching January 29 th 214 Developed
SAVINO BRUNO, MD Director Internal Medicine and Hepatology Unit AO Fatebenefratelli e Oftalmico, Milano Market wheretelaprevir has not yet launched Victrelis is still launching January 29 th 214 Developed
EASL and The Future of HCV Treatment
 EASL and The Future of HCV Treatment Douglas T. Dieterich, M.D Professor of Medicine Division of Liver Diseases, Gastroenterology and Infectious Diseases Department of Medicine Mount Sinai School of Medicine
EASL and The Future of HCV Treatment Douglas T. Dieterich, M.D Professor of Medicine Division of Liver Diseases, Gastroenterology and Infectious Diseases Department of Medicine Mount Sinai School of Medicine
SYNOPSIS Final Clinical Study Report for Study AI444031
 Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Name of Active Ingredient: () Individual Study Table Referring to the Dossier (For National Authority Use Only) SYNOPSIS for Study
Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Name of Active Ingredient: () Individual Study Table Referring to the Dossier (For National Authority Use Only) SYNOPSIS for Study
Treatments of Genotype 2, 3,and 4: Now and in the future
 Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Clinical Management: Treatment of HCV Mono-infection
 Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Professor Massimo Puoti
 Five Nations Conference on HIV and Hepatitis in partnership with Professor Massimo Puoti Universita of Brescia, Italy Massimo Puoti Dept. of Infectious Diseases AO Ospedale Niguarda Cà Granda Milan, Italy
Five Nations Conference on HIV and Hepatitis in partnership with Professor Massimo Puoti Universita of Brescia, Italy Massimo Puoti Dept. of Infectious Diseases AO Ospedale Niguarda Cà Granda Milan, Italy
Les Inhibiteurs de Protéase du VHC
 Les Inhibiteurs de Protéase du VHC Pr Jean-Michel Pawlotsky National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital University of Paris-Est
Les Inhibiteurs de Protéase du VHC Pr Jean-Michel Pawlotsky National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital University of Paris-Est
Learning Objectives. Disclosures (Activity w/i 12 months) WHY DISCUSS HCV/HIV COINFECTION? HCV/HIV Effect on Health Utilization in A5001
 WHY DISCUSS HCV/HIV COINFECTION? HCV/HIV Effect on Health Utilization in A5001") Learning Objectives HCV/HIV COINFECTION Soup to Nuts Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine At the
Learning Objectives HCV/HIV COINFECTION Soup to Nuts Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine At the
Viral hepatitis in patients living with HIV: can we still speak of special population?
 Viral hepatitis in patients living with HIV: can we still speak of special population? Maurizio Bonacini, M.D., A.G.A.F. Mission Gastroenterology and Hepatology San Francisco, CA YES for HBV Excluded by
Viral hepatitis in patients living with HIV: can we still speak of special population? Maurizio Bonacini, M.D., A.G.A.F. Mission Gastroenterology and Hepatology San Francisco, CA YES for HBV Excluded by
Dr Janice Main Imperial College Healthcare NHS Trust, London
 BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
Triple therapy with telaprevir or boceprevir: management of side effects
 Triple therapy with telaprevir or boceprevir: management of side effects Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
Triple therapy with telaprevir or boceprevir: management of side effects Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
Co-infection, Opportunistic Infections and Malignancies
 BHIVA Best of CROI Feedback Meetings London North East England North West England Edinburgh Birmingham BHIVA Best of CROI Feedback Meetings 2012 Co-infection, Opportunistic Infections and Malignancies
BHIVA Best of CROI Feedback Meetings London North East England North West England Edinburgh Birmingham BHIVA Best of CROI Feedback Meetings 2012 Co-infection, Opportunistic Infections and Malignancies
HCV Treatment: Why to Wait
 HCV Treatment: Why to Wait Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital University of Paris-Est
HCV Treatment: Why to Wait Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital University of Paris-Est
Program Disclosure. Provider is approved by the California Board of Registered Nursing, Provider #13664, for 1.5 contact hours.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Areas of Interest. HCV Epidemiology, Natural History HCV Treatment. HBV Epidemiology and Prevention. Monoinfected Coinfected
 CROI 2011 UPDATE Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases Univ. of Cincinnati College of Medicine Areas of Interest HCV Epidemiology, Natural History
CROI 2011 UPDATE Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases Univ. of Cincinnati College of Medicine Areas of Interest HCV Epidemiology, Natural History
Pivotal New England Journal of Medicine papers 2014 Phase 3 Trial data
 4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
Treatment of Patients with HCV and HIV
 Treatment of Patients with HCV and HIV BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY Four Questions Is HIV/HCV
Treatment of Patients with HCV and HIV BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY Four Questions Is HIV/HCV
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C First Generation Agents Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Hepatitis C First Generation Agents Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Transformation of Chronic Hepatitis C Treatment
 Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
Treating HCV Genotype 2 & 3
 Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
DRUG-DRUG INTERACTIONS WITH GRAZOPREVIR/ELBASVIR: PRACTICAL CONSIDERATIONS FOR THE CARE OF HIV/HCV CO-INFECTED PATIENTS
 DRUG-DRUG INTERACTIONS WITH GRAZOPREVIR/ELBASVIR: PRACTICAL CONSIDERATIONS FOR THE CARE OF HIV/HCV CO-INFECTED PATIENTS Wendy W. Yeh, M.D. on behalf of the Merck HCV Doublet Team Translational Pharmacology/Translational
DRUG-DRUG INTERACTIONS WITH GRAZOPREVIR/ELBASVIR: PRACTICAL CONSIDERATIONS FOR THE CARE OF HIV/HCV CO-INFECTED PATIENTS Wendy W. Yeh, M.D. on behalf of the Merck HCV Doublet Team Translational Pharmacology/Translational
Associate Professor of Medicine University of Chicago
 Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2)
") Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) Goals for Hepatitis C Therapy Compared to PegIFN α/rbv, new treatment regimens for chronic hepatitis C should offer: Improved efficacy Efficacy
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) Goals for Hepatitis C Therapy Compared to PegIFN α/rbv, new treatment regimens for chronic hepatitis C should offer: Improved efficacy Efficacy
Potential Issues in Treating HIV/HCV co-infection with new HCV antivirals
 State of the Art in Hepatitis C Virus Infection in HIV/HCV-Coinfected Patients FORMATTED: 11/17/15 David L. Wyles, MD Associate Professor of Medicine University of California San Diego San Diego, California
State of the Art in Hepatitis C Virus Infection in HIV/HCV-Coinfected Patients FORMATTED: 11/17/15 David L. Wyles, MD Associate Professor of Medicine University of California San Diego San Diego, California
Professor Douglas Dieterich Mount Sinai School of Medicine, New York, USA
 17 TH ANNUAL CONFERENCE OF THE BRITISH HIV ASSOCIATION (BHIVA) Professor Douglas Dieterich Mount Sinai School of Medicine,, USA 6-8 April 2011, Bournemouth International Centre 17 TH ANNUAL CONFERENCE
17 TH ANNUAL CONFERENCE OF THE BRITISH HIV ASSOCIATION (BHIVA) Professor Douglas Dieterich Mount Sinai School of Medicine,, USA 6-8 April 2011, Bournemouth International Centre 17 TH ANNUAL CONFERENCE
November 2013 AASLD Investor Event 4 November
 November 2013 AASLD Investor Event 4 November Maris Hartmanis, President and CEO Charlotte Edenius, EVP Development Bertil Samuelsson, CSA Rein Piir, EVP Corporate Affairs & IR Corporate presentation,
November 2013 AASLD Investor Event 4 November Maris Hartmanis, President and CEO Charlotte Edenius, EVP Development Bertil Samuelsson, CSA Rein Piir, EVP Corporate Affairs & IR Corporate presentation,
Ledipasvir-Sofosbuvir (Harvoni)
") HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
Safety of Treatment in Cirrhotics in the Era of New Antiviral Therapies for Hepatitis C Virus
 Safety of Treatment in Cirrhotics in the Era of New Antiviral Therapies for Hepatitis C Virus JEFFREY NADELSON MD, ALAN EPSTEIN MD, THOMAS SEPE MD BOSTON UNIVERSITY SCHOOL OF MEDICINE ROGER WILLIAMS MEDICAL
Safety of Treatment in Cirrhotics in the Era of New Antiviral Therapies for Hepatitis C Virus JEFFREY NADELSON MD, ALAN EPSTEIN MD, THOMAS SEPE MD BOSTON UNIVERSITY SCHOOL OF MEDICINE ROGER WILLIAMS MEDICAL
Personalised Treatment with Telaprevir in Graham R Foster Professor of Hepatology Queen Marys University of London
 Personalised Treatment with Telaprevir in 2014 Graham R Foster Professor of Hepatology Queen Marys University of London Telaprevir in 2014 Disclaimers I have received funds from: BI, BMS, Janssen, Novarts,
Personalised Treatment with Telaprevir in 2014 Graham R Foster Professor of Hepatology Queen Marys University of London Telaprevir in 2014 Disclaimers I have received funds from: BI, BMS, Janssen, Novarts,
Professor David Back
 THIRD JOINT CONFERENCE OF BHIVA AND BASHH 2014 Professor David Back University of Liverpool 1-4 April 2014, Arena and Convention Centre Liverpool THIRD JOINT CONFERENCE OF BHIVA AND BASHH 2014 Professor
THIRD JOINT CONFERENCE OF BHIVA AND BASHH 2014 Professor David Back University of Liverpool 1-4 April 2014, Arena and Convention Centre Liverpool THIRD JOINT CONFERENCE OF BHIVA AND BASHH 2014 Professor
Interferon-based and interferon-free new treatment options
 Interferon-based and interferon-free new treatment options White Nights of Hepatology St. Petersburg, 7. June 2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Medizinische Klinik I Frankfurt
Interferon-based and interferon-free new treatment options White Nights of Hepatology St. Petersburg, 7. June 2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Medizinische Klinik I Frankfurt
HIV-HCV Co-Infection. George Mason University Falls Church, Virginia. Overview. Prevalence of HCV co-infection Incidence and Recent Trends
 HIV-HCV Co-Infection Zobair Younossi MD, MPH, FACG, AGAF, FAASLD Chairman, Department of Medicine, Inova Fairfax Hospital Vice President for Research, Inova Health System Professor of Medicine, VCU-Inova
HIV-HCV Co-Infection Zobair Younossi MD, MPH, FACG, AGAF, FAASLD Chairman, Department of Medicine, Inova Fairfax Hospital Vice President for Research, Inova Health System Professor of Medicine, VCU-Inova
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on