Annual Rheumatology & Therapeutics Review for Organizations & Societies
|
|
|
- Christine Terry
- 5 years ago
- Views:
Transcription

1 Annual Rheumatology & Therapeutics Review for Organizations & Societies
2 Opportunistic Infections and Tuberculosis Risk Management
3 Learning Objectives Define the risks of TB and non-tb opportunistic infections, identifying the differences depending on the type of TNF inhibitor Identify which patients have the highest risk for infection
4 Biologics in Rheumatoid Arthritis Agent Biologic Target Construct Infliximab TNF Chimeric MAb Etanercept TNF IgG-p75 receptor Adalimumab TNF Human MAb Goliumumab TNF Human MAb Certolizumab TNF Peg-Fab Abatacept T-cell costim IgG-CTLA4 fusion Rituximab B-cells Chimeric MAb Anakinra IL-1 IL-1 Recpt antag Tocilizumab IL-6 Anti-IL6 Recept MAb * Tofacitinib is NOT a Biologic
5 Scope of Infections Associated with Biologic Use Anti-TNF Anakinra Abatacept Rituximab Tocilizumab Tofacitinib NSIE SIE Bacterial TB & Myco * * * Fungal & Opportunistic * * Hepatitis B * * Hepatitis C * H. Zoster * * * PML * Increased risk from PI, RCTs & Registries * Few cases reported NSIE: nonserious infectious events (URI, etc) SIE: serious infectious events PML: progressive multifocal leukoencephalopathy
6 The Problem with Steroids 30-60% of RA patients take prednisone Demonstrable clinical and radiographic benefits Steroids significantly increase the odds of: Non-serious infections Serious bacterial infections Mycobacteria (TB, NTM) Other opportunistic infections (eg, PCP, Zoster) Dose-dependent risk factor. Risk increased even at lowest doses (<5mg/day) Blunt/obscure fever, signs/sxs Used frequently long term Recommended for short term use
7 Prednisone and Tuberculosis General Practice Research Database, UK TB cases and controls Current glucocorticoid use *OR 4.9 ( ) <15mg/day *OR 2.8 ( ) >15mg/day *OR 7.7 ( ) *Adjusted for smoking, BMI, lung disease, diabetes, anti-rheumatic therapy, other TB risk factors Controls matched for age, sex, residence, time clinically followed Jick et al. Arthritis Rheum 2006
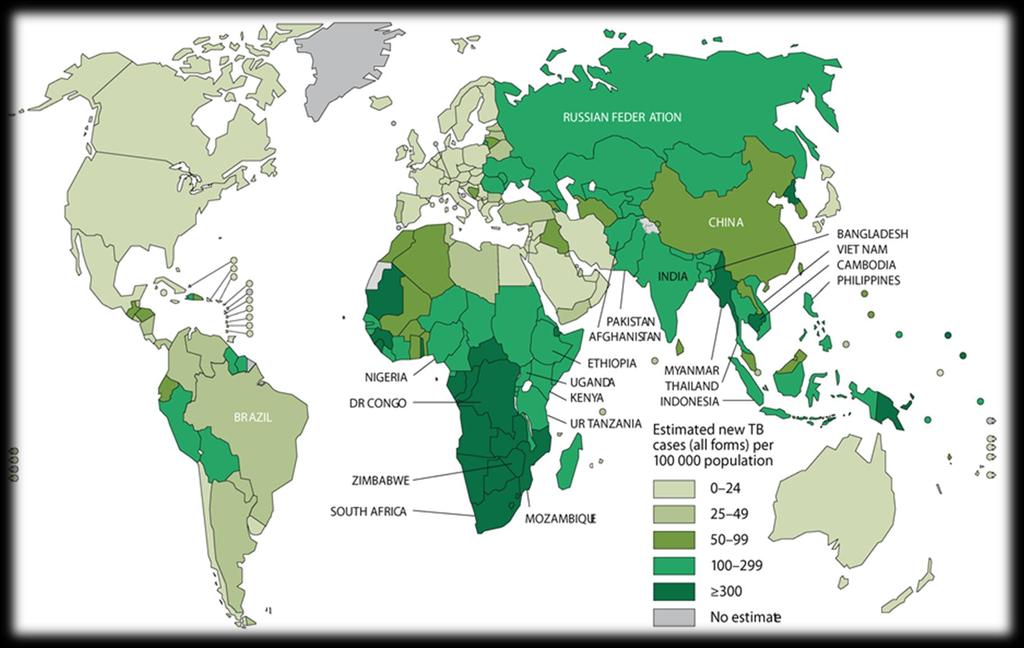


8 Global TB Epidemiology Courtesy of World Health Organization
9 TB Risk Risk of prior TB exposure Prior contact to case 30 Relative Risk RA +TNF Birth or extended living (>3 months) in countries where TB is endemic Regions other than North America, Western Europe, Australia/NZ Living or working in Homeless shelters 9 RA +TNF RA No TNF Jail/prison Health care settings (where TB is seen) Increased risk of TB disease varies 5-10 fold or more TB risk # /100,000pt-yrs 2 RA No TNF NL NL 1. Winthrop K. EULAR 2005, #SP0005; 2. Askling J, et al. Arthritis Rheum 52: , Seong SS, et al Apr;34(4): Singh JA, etl. Cochrane Reviews 2011 Baronnet et al. / Joint Bone Spine 78 (2011) Sweden Korea
10 Cumulative Incidence UK Biologic Registry 1% Incident TB Nelson-Aalen plot ADA 0.5% INF ETA 0% DMARD Drug Dixon WG et al. Ann Rheum Dis 2010:69: Days since registration Registration (entry to study) 1 year (365 days) 2 years (730 days) 3 years (1095 days) 4 years (1460 days) DMARD ETA INF ADA
11 Table 1. Crude incidence rates of tuberculosis and nontuberculous mycobacterial disease (NTM) among anti-tnf users, Kaiser Permanente Northern California, Crude incidence rate (95% CI)* Tuberculosis NTM 1 All Anti-TNF users 49 (18-79) 74 (37-111) a Etanercept users 17 (0-41) 35 (1-69) b Infliximab users 83 (10-156) 116 (30-203) c Adalimumab users 61 (0-145) 122 (3-241) 2 Anti-TNF users 50 years old 64 (26-132) 118 (63-202) *rate per 100,000 patient years (95% confidence interval) 1 All anti-tnf users: 10 Tuberculosis cases/20,409 person-years, 15 NTM cases/20,270 person-years; a Etanercept users: 2 Tuberculosis /11,765 person-years, 4 NTM cases/11,429 person-years; b Infliximab users: 5 Tuberculosis cases/6,024 person-years, 7 NTM cases/6,035 person-years; c Adalimumab users: 2 Tuberculosis cases/3,279 person-years, 4 NTM cases/3,279 person-years; 2 Anti-TNF users 50 years old; 7 Tuberculosis cases/11,011 person-years, 13 NTM cases/11,017 person-years Winthrop K et al. ARD 2013
12 Survival (%) Log 10 cfu Survival (%) Log 10 cfu Granuloma Penetration A 100 Survival of acutely infected mice B 9.0 Bacterial burden in the lungs MP6-XT22 hi mtnfr2-fc hi lgg1 hi MP6-XT22 lo mtnfr2-fc lo lgg1 lo MP6-XT22 mtnfr2-fc lgg Days after injection Days after injection D Survival of chronically infected mice Bacterial burden in lungs mg/dose MP6-XT mg/dose mtnfr2-fc 0.5 mg/dose mtnfr2-fc 60 7 Control C MP6 0.5 mg/dose mtnfr2-fc 0.2 mg/dose mtnfr2-fc 0.5 mg/dose Control Days after first injection Days after first injection Plessner HL et al JID 2007
13 Mycobacteria with Newer RA Biologics Rituximab Cases of TB and NTM reported in case-series fashion. Most on prednisone Abatacept Clinical trial program, 7 TB cases reported (rate 60/100,000) Tocilizumab Clinical development program, 10 TB cases (rate 100/100,000). Post-marketing surveillance in Japan, 4 cases (rate 220/100,000) Simon TA et al. Arth Res Ther 2010; Koike T et al. ARD 2011; Winthrop K et al. CID 2009
14 Tofacitinib in RA JAK 1/3 inhibition Tuberculosis rate = 173/100,000 37/100,000 (North America/Western Europe) Most cases at 10mg BID dose All cases screened negative prior to trial entry Mechanism? Macrophage control of TB Interferon signaling? Winthrop et al abstract, American College of Rheumatology (ACR), Washington DC, Nov 2012



15 Interferon-gamma Release Assays (IGRAs)
16 IGRAs Specificity ESAT CFP M.tuberculosis + + M. africanum + + M. bovis + + BCG substrain Gothenburg - - Moreau - - Tice - - Tokyo - - Danish - - Glaxo - - Montreal - - Pasteur - - Andersen, et al. Lancet 2000;356(9235):1099. ESAT CFP M. abcessus - - M. avium - - M. branderi - - M. celatum - - M. chelonae - - M. fortuitum - - M. gordonii - - M. intracellulare - - M. kansasii + + M. malmoense - - M. marinum + + M. oenavense - - M. smegmatis - - M. scrofulaceum - - M. szulgai + + M. terrae - - M. vaccae - - M. xenopi - -
17 Comparison of LTBI Screening Methods TST in vivo Poor specificity of PPD False positives with BCG 2 patient visits results in 2-3 days Difficult to place and read read in hrs false negative results occur in immunosuppressed IGRA in vitro Higher specificity in those with BCG 1 patient visit results in 24 hrs lab variability IND and false negative results occur in immunosuppressed
18 Relative Sensitivity of IGRA Case-control study, Peru 80% BCG use in both groups High prednisone use among RA group RA (n = 101) Controls (n = 93) TST+ 27 (27%) a 61 (66%) QFT-IT+ 45 (45%) 55 (59%) Ponce de Leon D et al. J Rheumatol. 2008;35:
19 Golimumab and TB N= 2,282 RA, PsA, AS development program Screened with TST and QFT-IT 5 patients developed active TB All 5 screened negative at baseline 2 with TST of 5mm or 15mm (negative by local standards) 317 screened positive INH and golimumab No TB cases Hsia E et al. Arth Rheum 2012
20 B C TST TST QFT-GIT + 71 QFT-GIT + 72 Figure 1. Overlap of screening test results and rates of positivity from the tuberculin skin test (TST) and an interferon-γ release assay (i.e., the QuantiFERON-TB Gold In-Tube [QFT-GIT] test) for the detection of latent tuberculosis infection in all patients (A), bacillus Calmette-Guérin (BCG)- vaccinated patients (B), and non-bcg-vaccinated patients (C). Hsia E et al. Arth Rheum 2012
21 IGRAs in the Immunocompromised Anergy with TST and IGRAs IGRAs less affected by prednisone? False negative with IGRA in patients already receiving anti-tnf therapy 1 Indeterminate results 2 QFT-IT and T-SPOT.TB in 2-5% LTBI sensitivity 2 QFT-IT similar to T.SPOT.TB (and probably greater than TST) 1. Hamdi H et al. Arthritis Res Ther. 2006;8:R Lalvani A, Millington KA. Autoimmun Rev Epub ahead of print.
22 Figure American College of Rheumatology recommandations update for tuberculosis (TB) screening with biologic agent use. Depending on a patient's current therapy. the management may begin at an appropriate rectangle in the figure. rather than only at the top of the figure. The level of evidence supporting each recommendation for TB reactivation was "C." except for initiation of biologic agents in patients being treated for latent TB infection, where the level of evidence was "B." Anergy panel testing is not recommended. t Interferon-?-release assay (IGRA) is preferred if the patient has a history of BCG vaccination. Risk factors for TB exposure are defined based on a publication from the US Centers for Disease Control and Prevention as: close contacts of persons known or suspected to have active TB: foreign-born persons from areas that have a high incidence of active TB (e.g.. Africa. Asia, Eastern Europe. Latin America, and Russia): persons who visit areas with a high prevalence of active TB. especially if visits are frequent or prolonged: residents and employees of congregate settings whose clients are at an increased risk for active TB (e.g.. correctional facilities, long-term care facilities, and homeless shelters): health care workers who serve clients who are at an increased risk for active TB: populations defined locally as having an increased incidence of latent Mycobacterium tuberculosis infection or active TB, possibly including medically undersorved. low-income populations, or persons who abuse drugs or alcohol: and infants, children. and adolescents exposed to adults who are at an increased risk for latent M tuberculosis infection or active TB (14). If the patient is immunosuppressed and false-negative results are more likely. consider repeating screening testis) with tuberculin skin test (TST) or IGRA. I Chest radiograph may also be considered when clinically indicated in patients with risk factors. even with a negative repeat TST or IGRA. * Obtain respiratory (e.g., sputum, bronchoalveolar lavage fluid) or other samples as clinically appropriate for acid-fast bacilli (AFB) smear and culture and consider referral to a TB specialist for further evaluation and treatment. * In a patient diagnosed with latent or active TB. consider referral to a specialist for the recommended treatment Patients who test positive for TST or IGRA at baseline often remain positive for these tests even after successful treatment of TB. These patients need monitoring for clinical signs and symptoms of recurrent TB disease, since repeating tests will not allow help in diagnosis of recurrent TB.
23 Screening in the Biologics Setting: Words to Live by A priori probability reigns supreme If they should be positive, then they probably are If they shouldn t be positive, they probably aren t If risk factors and immunosuppressed, consider using two screening tests Maximize sensitivity If you don t believe your test result, REPEAT it!
24 Rate per 100 patient-years TB Screening Lowers TB Rates >80% Pre-screening Adalimumab RA Clinical Trials Post-screening Phase 1 2 Phase 3 and extension ReACT All cases No. of cases Exposure (pt yrs) + = *Through December 2003 Biobadaser ,729 RA pts (7,825 pt-yrs TNFi Rx) Before screening guidelines: 32/6,126 TB rate 522/100,000 PY After screening guidelines: 2/1,699 TB Rate 117/100,000 PY Carmona L. Arthritis Rheum.2005;52:
25 Physicans who follow TB test guidlines, % Rheumatologists are Smartest Rheumatologists Gastroenterologists Dermatologists 92% 85% 80% 76% 73% 76% G5 Non-G5 Figure 2 Percentage of rheumatologists, gastroenterologists and dermatologists who reported following guidelines for TB testing of their patients prior to prescribing anti-tnf agents: G5 vs. non-g5 EU member countries, TB = tuberculosis; G5 = the five foremost industrialized economies; TNF = tumor necrosis factor; EU = European Union. Smith MY et al. IJTLD 2012
26 Treatment of LTBI Duration (mos) Evidence Completion Hepatitis Risk INH 9 A 45-60% INH 6 B 55-57% 3.8% RIF 4 B 69-78% 0.7% INH/RIF* Hi dose weekly 3 B 75% Unknown INH: Isoniazid; RIF: Rifampin *Horsburgh CR, Rubin EJ, NEJM 2011: 364:15
27 New Therapy Option INH and Rifapentine 3 months, once weekly (directly observed) Table 2. Number of Subjects with Tuberculosis and Event Rates.* Population and Study Group No. of Subjects Subjects with Tuberculosis Difference in Cumulative Rate Upper Limit of 95% Cl for Difference in Cumulative Rate No. No. per patient-yr Cumulative rate Modified intention-to-treat analysis Isoniazid only Combination therapy Per-protocol analysis Isoniazid only Combination therapy *Combination therapy consisted of 3 months of directly observed once-weekly therapy with rifapentine (900 mg) plus Isoniazid (900 mg). Isoniazid-only therapy consisted of 9 months of self-administered daily isoniazid (300 mg). Data are shown for a period up to 33 months after study enrollment. The difference is the rate in the combination-therapy group minus the rate in the isoniazid-only group Sterling T et al. NEJM 2011
28 Nontuberculous (NTM) Disease Environmental mycobacteria Drinking water and soil Lung, skin/soft tissue, disseminated disease M. avium, M. kansasii Rapid growers M. abscessus Pulmonary NTM Elderly female predominance Underlying lung disease (e.g. RA) No defined way to screen for NTM Suspect in elderly women with unexplained chronic cough
29 FDA MedWatch Reported Characteristics of Anti-TNF Therapy Associated Nontuberculous Mycobacterial (NTM) Cases Pulmonary (n=59) Extrapulmonary (n=46) M. avium 43 (73%) 9 (20%) RGM* 6 (10%) 15 (33%) Age (years) Sex (female) 41 (73%) 25 (54%) RA ± 48 (81%) 25 (54%) Infliximab 40 (68%) 33 (72%) Etanercept 13 (22%) 12 (26%) +p value < 0.05 for comparison between pulmonary and extrapulmonary disease *Rapidly growing mycobacteria (RGM) ±Rheumatoid arthritis (RA) Winthrop KL Emerg Infect Dis 2009
30 Crude incidence rate per 100,000 patient years Figure NTM Tuberculosis 95% Cl General population General population 50 years old RA population, no anti-tnf use RA population, no anti-tnf therapy exposed Winthrop KL et al. Ann Rheum Dis 2012; Winthrop KL Nat Rheum Rev 2013
31 Many Other Types of Opportunistic Infections Reported with DMARDs mtb ntm Clostridial Salmonella Nocardia Legionella Listeriosis Hepatitis B, Hepatitis C Herpes simplex virus HIV Varicella Zoster CMV Ebstein-Barr virus Human papilloma virus TNF Inhibitors Histoplasmosis Coccidioidomycosis Candidiasis Aspergillosis Cryptococcosis Pneumocystis Toxoplasmosis Strongyloidosis Leishmaniasis Rituximab Rare TB, mycobacterial JC Virus (PML) Reactivation HBV New/reactivated viral infx; CMV, HSV, Parvo B19, VZV, W. Nile, Hep C Abatacept TB, Reactivation HBV Aspergillosis, candidiasis Tocilizumab TB, reactivation HBV Tofacitinib H.Zoster TB, CMV, BK virus Ustekinumab mycobacteria, Salmonella, and Bacillus Calmette-Guerin (BCG) Ali T, et al. Drug Healthc Patient Saf. 2013; 5:
32 Population-based Estimates of OI Risk Table 2. The biologic era: rates and risks of opportunistic infections in RA patients Using anti-tnf therapy from European and North American observational cohort studies. Crude Incidence per 100,000 pt-yrs. Crude Incidence per 100,000 pt-yrs. Country/year Outcome studied Anti-TNF treated Non-biologic comparator Adj. RR (95% CI) 33 UK, 2006 OI NR 93 France, 2006 OI 152* NR NR 92 US,2010 OI ( ) * Rate adjusted for age and sex Cohorts restricted to RA patients + Rate not published, but rather estimated using data provided within paper OI outcomes did not include tuberculosis NR, not reported; UNDEF, undefined Winthrop K, Rheum Clin North Am 2012
33 SABER Non-viral OIs TNFi starters 270/100,000 Non-biologics 170/100,000 PJP crude incidence TNFi starters, 56/100,000 Table 2. Distribution of non-viral opportunistic infections (n=80) all disease indications Infection Frequency (%) Pneumocystosis 16 (20) Nocardiosis/Actinonmycosis 12 (15) Tuberculosis 10 (12.5) Histoplasmosis 9 (11.3) Nontuberculosis Mycobacteria 9 (11.3) Salmonellosis 8 (10) Listeriosis 4 (5) Legionellosis 4 (5) Cryptococcosis 3 (3.8) Endemic Fungal Infection 1 1 (1.3) Toxoplasmosis 1 (1.3) Coccidioidomycosis 1 (1.3) Baddley J, Winthrop KL et al. Presented IDSA 2011 Baddley/Winthrop et al. ARD 2014 Blastomycosis 1 (1.3) Aspergillosis 1 (1.3)
34 Number of Cases Histoplasmosis Infections with anti-tnf FDA analysis prompted by reports of histoplasmosis deaths in patients receiving anti-tnf Rx; Medwatch AERS thru 2/29/08 N=240 cases (207 IFX; 16 ETN; 17 ADA) Complete data on 21 cases All (21) Dx and Rx delayed 5 died without Rx; 7 neg. C/S Pulm. 10%, disseminated 76% Death occurred in 45/240 (19%) 85% of cases occurred in endemic areas (OH/MS river valley) Concern about delayed diagnosis of fungal infection in anti-tnf Rx pts Summary: Patients living in endemic areas are at risk FDA conclusion: Clinicians should consider initiating empiric fungal therapy while evaluating at-risk individuals with undiagnosed systemic illnesses Unrecognized Histoplasmosis Cases Total cases Death cases Infliximab Etanercept Adalimumab Diak P et al., FDA 2008
35 Herpes Zoster (Shingles) Reactivation of varicella zoster virus (VZV) Prior exposure to VZV ubiquitous in those >40 years Lifetime risk of reactivation = 33% 0.4 and 1.1 events per 100 patient-years depending on age Decline in VZV-specific cell-mediated immunity Acute and chronic pain, dermatomal rash Post-herpetic neuralgia (15%), visual loss Disseminated disease (1%) RA patients Risk elevated 2-3 fold Vs. non-ra VZV vaccination is recommended, but rare (1%) Harpaz et al. MMWR 2008; Yawn et al. Mayo Clin Proc 2007 ; Levin et al. J ID 2003; Weinberg et al. J ID 2009; Smitten et al. Arthritis Rheum 2007;chmajuk et al. JAMA 2011; Zhang et al. ART 2011
36 Age, gender standardized incidence rate for herpes zoster/1000pys Figure: Age standardized incidence rate for herpes zoster per 1000pys (standardized to the U.S census) Healthy SLE IBD RA PsA PsO AS Gout Diabetes Curtis J et al, EULAR abstract 2014

37 European and US Studies Differ re: HZ risk with TNFi Author N Rate & TNFi BSRBR Strangfeld McDonald , Wolfe , Smitten , Winthrop Galloway , Hazard Ratios for VZV Infection BSRBR Strangfeld Smitten Wolfe McDonald & IIRR per 1000 pt-yrs (Population rate ~5/1000 PY*) Statistically significant p < All TNFi ETN ADA INF H.Zoster (VZV) infections are increased w/ TNF blockade, age, steroid, comorbidities Galloway J. #421 ACR 2010 Strangfeld A. JAMA 2009; 301:737 Smitten A&R : McDonald. Clin Infect Dis :1364 Wolfe F. Rheumatology 2006; 45:1370 Winthrop JAMA 2013 Galloway Ann Rheum Dis 2013; 72:229
38 Table 2: Events, absolute incidence rate and adjusted hazard ratio of herpes zoster infection by different types of biologics and other RA Medication Biologic Exposures Events Person years (pys) Absolute incidence rate per 100 pys (95% CI) Adjusted hazard ratio* (95% CI) Non-Anti TNF mechanism of action Abatacept ( ) 1.00 (Ref) Rituximab ( ) 1.20 ( ) Tocilizumab ( ) 1.05 ( ) Anti-TNF mechanism of action Adalimumab ( ) 1.04 ( ) Certolizumab ( ) 1.30 ( ) Etanercept ( ) 1.26 ( ) Golimumab ( ) 0.91 ( ) Infliximab ( ) 0.98 ( ) Other RA Medications Methotrexate No ( ) 1.00 (Ref) Yes ( ) 1.07 ( ) Oral Glucocorticoids (prednisoneequivalent dose) None ( ) 1.00 (Ref) 7.5mg/day ( ) 1.55 ( ) > 7.5mg/day ( ) 2.35 ( ) Yun H et al, Arth Car Res, In Press
39 Herpes Zoster and Tofacitinib Table 4. Crude incidence rates of HZ overall and by geographic region of Enrollment in the phase II, phase III, and long-term extension studies HZ events Patient-years of exposure HZ incidence rate (95% CI)* Global rheumatoid arthritis program 239 5, ( ) By region US/Canada/Australia 40 1, ( ) Western Europe ( ) Eastern Europe 43 1, ( ) Latin America ( ) Asia 107 1, ( ) Within Asian countries Japan/Korea ( ) India ( ) Thailand/Malaysia/Philippines ( ) China/Taiwan ( ) *The crude incidence rates of herpes zoster (HZ) events, with 95% confidence intervals (95% CIs), are expressed per 100 patient-years. Winthrop et al Arth and Rheumatol 2014 Winthrop K et al Arth and Rheumatol 2014
40 Zostavax RA vaccination rate is low Safety and efficacy in RA? Table 3. Herpes Zoster Incidence Rate for Unvaccinated and After Vaccination a >42 Days Since Vaccination Unvaccinated HZ Cases, No. HZ IR HZ Cases, No. HZ IR Overall ( ) ( ) Medications, mutually exclusive groups b Biologics, regardless of oral glucocorticoids ( ) ( ) Anti-TNF therapies ( ) ( ) DMARDs, without biologics but regardless of oral glucocorticoids ( ) ( ) Oral glucocorticoids alone ( ) ( ) Abbreviation: DMARDs, disease-modifying antirheumatic drugs; HZ, herpes zoster; IR, incidence rate per 1,000 person-years; TNF, tumor necrosis factor. a More than 42 days after vaccination. b Classified using the following hierarchy: biologics with or without nonbiologic DMARDs or oral glucocorticoids; nonbiologic DMARDs with or without oral Glucoccorticoids; oral glicocorticoids only. Jie J et al. JAMA 2012
41 ACIP and ACR Recs for Zostavax Recommended in >60 years old Licensed > 50 years Not contra-indicated MTX (<0.4mg/kg/wk), Prednisone (<20mg daily), azathioprine (<3.0mg/kg/day) Contraindicated Biologics Tofacitinib not specifically discussed (pre-approval) MMWR. November 11, ; ;

42
43 Reactivation of Hepatitis B During Immunosuppressive Therapy: Potentially Fatal Yet Preventable RHEUMATOLOGISTS USA % routinely screen before non-biologic DMARD 69% before biologic DMARD 7% observed reactivation event IDEAS AND OPINIONS Anna S.F. Lock, MD; John W. Ward, MD; Robert P. Perrillo, MD; Brian J. McMahon, MD; and T. Jake Liang, MD Stine JG, et al. Arthritis Care Res. 2010;62:
44 Table 1c. Proposed functional HBV categorization of patients based on screening test results Screening test results Risk of progression during biologic therapy Management considerations Never infected HBV vaccinated Resolved HBV* Chronic HBV HBcAB negative HBsAg negative, HBsAb negative HBcAB negative HBsAg negative, HBsAb positive HBcAB positive HBsAg negative, HBsAb positive HBcAB positive HBsAg negative, HBsAb negative HBsAg positive (regardless of other results) None None + Immunity suggested Low risk (but not zero) γ Immunity not clear. Low to moderate risk of progression High Consider HBV vaccination if at risk for acquiring HBV N/A Obtain baseline HBV DNA If positive: -patient has chronic HBV. If negative: -periodic monitoring of HBV DNA levels and liver function tests during biologic therapy - If biologic therapy is not avoidable, then refer to GI or ID specialist for concurrent and appropriate anti-hbv therapy - Periodic monitoring of HBV DNA levels and liver function tests during biologic therapy + Patient s with HBsAb positivity have likely cleared their virus, although there still exists a small risk of seroreversion and reactivation during immunonosuppression[8]. γ In the case of HBsAb negativity, this substantially increases the risk that a patient has not cleared their HBV infection. Some proportion of these patients have either occult viremia (detectable serum HBV DNA) or can reactivate later during immunosuppression in which HBV DNA and/or surface antigen will become detectable. *Patients in this category may also rarely be antihbs positive in isolation
45 HBV Reactivation Reported with ALL biologics Risk probably highest with RTX Extrapolation from lymphoma literature Patients with prior exposure who lack surface antibody at highest risk Screen periodically (LFTs, HBV DNA) If reactivation Concomitant anti-viral with biologic appears safe Winthrop KL, Calabrese LH. Ann Rheum Dis. 2011;70:1701-3
46 PML Incidence among IMID without HIV or malignancy 0.2/100, confirmed cases of PML in IMID 17 SLE, 10 RA, 7 other 14 RTX, 6 TNFi Only 1 RTX treated case lacked other potential cause Concomitant drugs, lymphopenia, cancer There is no rationale for screening prior to biologic use in rheumatology patients Bharat A et al. Arth Res Care 2012; Molloy ES et al Arth Rheum 2012
Tuberculosis and Biologic Therapies: Risk and Prevention
 Tuberculosis and Biologic Therapies: Risk and Prevention Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health and Preventive Medicine Oregon Health & Science
Tuberculosis and Biologic Therapies: Risk and Prevention Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health and Preventive Medicine Oregon Health & Science
Tuberculosis Update. Topics to be Addressed
 Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Tuberculosis and TNF Inhibitors
 Tuberculosis and TNF Inhibitors Sundari Mase MD, MPH Medical Team Lead CDC/DTBE/FSEB January 18, 2011 Objectives Discuss the association between and epidemiology of TNF inhibitors and TB Discuss the challenges
Tuberculosis and TNF Inhibitors Sundari Mase MD, MPH Medical Team Lead CDC/DTBE/FSEB January 18, 2011 Objectives Discuss the association between and epidemiology of TNF inhibitors and TB Discuss the challenges
Tuberculosis in Non-HIV Infected Immunosuppresed Hosts. TNFα inhibitors and beyond
 Tuberculosis in Non-HIV Infected Immunosuppresed Hosts TNFα inhibitors and beyond David E. Griffith, MD Assistant Medical Director Heartland National TB Center Professor of Medicine University of Texas
Tuberculosis in Non-HIV Infected Immunosuppresed Hosts TNFα inhibitors and beyond David E. Griffith, MD Assistant Medical Director Heartland National TB Center Professor of Medicine University of Texas
Opportunistic Infections and Tuberculosis Risk Management
 Opportunistic Infections and Tuberculosis Risk Management Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health, and Preventive Medicine Oregon Health & Science
Opportunistic Infections and Tuberculosis Risk Management Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health, and Preventive Medicine Oregon Health & Science
Making the Diagnosis of Tuberculosis
 Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Pathogenesis of Rheumatoid Arthritis. Smolen, J. S. et al. (2012) Nat. Rev. Rheumatol. doi: /nrrheum
 Nat. Rev. Rheumatol. doi: /nrrheum") 1 Pathogenesis of Rheumatoid Arthritis 2 Smolen, J. S. et al. (2012) Nat. Rev. Rheumatol. doi:10.1038/nrrheum 2012.23 Biologic therapies used in the treatment of rheumatoid arthritis 3 Etanercept Infliximab
1 Pathogenesis of Rheumatoid Arthritis 2 Smolen, J. S. et al. (2012) Nat. Rev. Rheumatol. doi:10.1038/nrrheum 2012.23 Biologic therapies used in the treatment of rheumatoid arthritis 3 Etanercept Infliximab
Infections and Biologics
 Overview Infections and Biologics James Galloway What is the risk of infection with biologics? Are some patients at greater risk? Are some drugs safer? Case scenario You recently commenced Judith, a 54
Overview Infections and Biologics James Galloway What is the risk of infection with biologics? Are some patients at greater risk? Are some drugs safer? Case scenario You recently commenced Judith, a 54
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA)
 and Interferon-gamma Release Assays (IGRA)") Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2019 Bob Belknap M.D. Director, Denver Metro TB Program Disclosures No relevant financial relationships Objectives Be able to
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2019 Bob Belknap M.D. Director, Denver Metro TB Program Disclosures No relevant financial relationships Objectives Be able to
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA)
 and Interferon-gamma Release Assays (IGRA)") Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2018 Bob Belknap M.D. Director, Denver Metro TB Program No Disclosures Objectives be able to describe: 1. Who should get tested
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2018 Bob Belknap M.D. Director, Denver Metro TB Program No Disclosures Objectives be able to describe: 1. Who should get tested
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University
 Lloyd Friedman, M.D. Milford Hospital Yale University") Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
JAK Inhibitors and Safety
 JAK Inhibitors and Safety Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health, and Preventive Medicine Oregon Health & Science University Learning Objectives
JAK Inhibitors and Safety Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health, and Preventive Medicine Oregon Health & Science University Learning Objectives
Diagnosis and Medical Management of LTBI
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Diagnosis and Medical Management of LTBI Barbara Seaworth, MD December 8, 2009 CLINICAL DIAGNOSIS AND MANAGEMENT OF LATENT TB INFECTION Barbara
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Diagnosis and Medical Management of LTBI Barbara Seaworth, MD December 8, 2009 CLINICAL DIAGNOSIS AND MANAGEMENT OF LATENT TB INFECTION Barbara
TB Nurse Case Management San Antonio, Texas March 7 9, Clinical Diagnosis and
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Clinical Diagnosis and Management of LTBI Lynn Horvath, MD March 7, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Clinical Diagnosis and Management of LTBI Lynn Horvath, MD March 7, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict
Contemporary Views of the Impact of Biologic Therapy on Infection Risk
 Contemporary Views of the Impact of Biologic Therapy on Infection Risk Cezarina Mindru, M.D. Assistant Professor of Medicine Baylor College of Medicine VA Michel E. Debakey, Houston, TX Faculty Disclosures
Contemporary Views of the Impact of Biologic Therapy on Infection Risk Cezarina Mindru, M.D. Assistant Professor of Medicine Baylor College of Medicine VA Michel E. Debakey, Houston, TX Faculty Disclosures
TUBERCULOSIS AND THE TNF-α INHIBITORS. Lloyd Friedman, M.D. Yale University Milford Hospital
 TUBERCULOSIS AND THE TNF-α INHIBITORS Lloyd Friedman, M.D. Yale University Milford Hospital Outline TNF-α Anti-TNF-α medications Rates of tuberculosis Lower rates with etanercept Screening for latent tuberculosis
TUBERCULOSIS AND THE TNF-α INHIBITORS Lloyd Friedman, M.D. Yale University Milford Hospital Outline TNF-α Anti-TNF-α medications Rates of tuberculosis Lower rates with etanercept Screening for latent tuberculosis
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
Transmission and Pathogenesis of Tuberculosis
 Transmission and Pathogenesis of Tuberculosis 2011 John Bernardo, M.D. Pulmonary Center Boston University School of Medicine Massachusetts Department of Public Health Division of TB Prevention and Control
Transmission and Pathogenesis of Tuberculosis 2011 John Bernardo, M.D. Pulmonary Center Boston University School of Medicine Massachusetts Department of Public Health Division of TB Prevention and Control
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
TB Intensive Tyler, Texas December 2-4, 2008
 TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
Latent TB Infection (LTBI)
") Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without
Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without
Utility of PPD or IGRA to answer the age old question of "TB or not TB
 Utility of PPD or IGRA to answer the age old question of "TB or not TB Thomas S. Alexander, Ph.D., D(ABMLI) Immunologist Summa Health alexandt@summahealth.org Yes, The reservation is in the name of Dr.
Utility of PPD or IGRA to answer the age old question of "TB or not TB Thomas S. Alexander, Ph.D., D(ABMLI) Immunologist Summa Health alexandt@summahealth.org Yes, The reservation is in the name of Dr.
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lynn Horvath, MD November 11, 2014 Lynn Horvath, MD has the following disclosures to
TB Intensive San Antonio, Texas November 11 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lynn Horvath, MD November 11, 2014 Lynn Horvath, MD has the following disclosures to
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI)
") Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Cimzia (certolizumab pegol) Data Showed Broad and Rapid Relief From Burden of Symptoms In Rheumatoid Arthritis Patients
 Data Showed Broad and Rapid Relief From Burden of Symptoms In Rheumatoid Arthritis Patients") Cimzia (certolizumab pegol) Data Showed Broad and Rapid Relief From Burden of Symptoms In Rheumatoid Arthritis Patients Rapid, sustained and clinically meaningful improvement in wideranging patient-reported
Cimzia (certolizumab pegol) Data Showed Broad and Rapid Relief From Burden of Symptoms In Rheumatoid Arthritis Patients Rapid, sustained and clinically meaningful improvement in wideranging patient-reported
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers
 Questions and Answers for Health Care Providers") Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis Pathogenesis and Treatment f Latent TB Infection Lynn Horvath, MD October 15, 2013 Lynn Horvath, MD has the following disclosures to make: No
TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis Pathogenesis and Treatment f Latent TB Infection Lynn Horvath, MD October 15, 2013 Lynn Horvath, MD has the following disclosures to make: No
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
Jennifer Lam MPH candidate 2009 Johns Hopkins Bloomberg School of Public Health. Preceptors: Wendy Cronin, PhD MT(ASCP), Cathy Goldsborough, RN
, Cathy Goldsborough, RN") Jennifer Lam MPH candidate 2009 Johns Hopkins Bloomberg School of Public Health Preceptors: Wendy Cronin, PhD MT(ASCP), Cathy Goldsborough, RN Phase Symposium: May 6, 2009 Background & Rationale Maryland
Jennifer Lam MPH candidate 2009 Johns Hopkins Bloomberg School of Public Health Preceptors: Wendy Cronin, PhD MT(ASCP), Cathy Goldsborough, RN Phase Symposium: May 6, 2009 Background & Rationale Maryland
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: golimumab_simponi 8/2013 2/2018 2/2019 3/2018 Description of Procedure or Service Golimumab (Simponi and
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: golimumab_simponi 8/2013 2/2018 2/2019 3/2018 Description of Procedure or Service Golimumab (Simponi and
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
DENOMINATOR: All patients aged 18 and older with a diagnosis of inflammatory bowel disease
 Measure #274: Inflammatory Bowel Disease (IBD): Testing for Latent Tuberculosis (TB) Before Initiating Anti-TNF (Tumor Necrosis Factor) Therapy National Quality Strategy Domain: Effective Clinical Care
Measure #274: Inflammatory Bowel Disease (IBD): Testing for Latent Tuberculosis (TB) Before Initiating Anti-TNF (Tumor Necrosis Factor) Therapy National Quality Strategy Domain: Effective Clinical Care
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents
 New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
Actemra (tocilizumab) CG-DRUG-81
 CG-DRUG-81") Market DC Actemra (tocilizumab) CG-DRUG-81 Override(s) Prior Authorization Approval Duration 1 year Medications Line of Business Quantity Limit Actemra (tocilizumab) vials VA MCD and All L-AGP May be subject
Market DC Actemra (tocilizumab) CG-DRUG-81 Override(s) Prior Authorization Approval Duration 1 year Medications Line of Business Quantity Limit Actemra (tocilizumab) vials VA MCD and All L-AGP May be subject
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
What prescribers need to know
 HUMIRA Citrate-free presentations in an Electronic Medical Record (EMR) What prescribers need to know 2 / This is your guide to identifying HUMIRA Citrate-free presentations in your Electronic Medical
HUMIRA Citrate-free presentations in an Electronic Medical Record (EMR) What prescribers need to know 2 / This is your guide to identifying HUMIRA Citrate-free presentations in your Electronic Medical
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Announcing HUMIRA. Psoriasis Starter Package
 Announcing HUMIRA (adalimumab) Psoriasis Starter Package HUMIRA is indicated for the treatment of adult patients with moderate to severe chronic plaque psoriasis who are candidates for systemic therapy
Announcing HUMIRA (adalimumab) Psoriasis Starter Package HUMIRA is indicated for the treatment of adult patients with moderate to severe chronic plaque psoriasis who are candidates for systemic therapy
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Amjevita (adalimumab-atto) CG-DRUG-64, CG-DRUG-65
 CG-DRUG-64, CG-DRUG-65") Market DC Amjevita (adalimumab-atto) CG-DRUG-64, CG-DRUG-65 Override(s) Prior Authorization Quantity Limit Medications Amjevita 20 mg/0.4 ml prefilled syringe Amjevita (adalimumab-atto) 40 mg/0.8 ml 2
Market DC Amjevita (adalimumab-atto) CG-DRUG-64, CG-DRUG-65 Override(s) Prior Authorization Quantity Limit Medications Amjevita 20 mg/0.4 ml prefilled syringe Amjevita (adalimumab-atto) 40 mg/0.8 ml 2
LTBI Treatment and Anti TNF alpha
 LTBI Treatment and Anti TNF alpha Therapy Julie Higashi, MD PhD Director, TB Control Section San Francisco Department of Public Health TNF alpha is important for the immune response against TB Macrophages
LTBI Treatment and Anti TNF alpha Therapy Julie Higashi, MD PhD Director, TB Control Section San Francisco Department of Public Health TNF alpha is important for the immune response against TB Macrophages
(2) 83.3% b/w TST and T-SPOT, (2) 77.4% b/w TST and T-SPOT. 77.7% b/w TST and QFT-GIT. QFT-GIT, 22.2% in T-SPOT. TSPOT vs. TST (> 5 mm) vs.
 83.3% b/w TST and T-SPOT, (2) 77.4% b/w TST and T-SPOT. 77.7% b/w TST and QFT-GIT. QFT-GIT, 22.2% in T-SPOT. TSPOT vs. TST (> 5 mm) vs.") Supplementary Table 1. Study characteristics of the included literature Low to moderate TB endemic region Shovman et al. (2009) [21] Minguez et al. (2012) [16], type 35 RA 35 RA 53 Patients with s (RA
Supplementary Table 1. Study characteristics of the included literature Low to moderate TB endemic region Shovman et al. (2009) [21] Minguez et al. (2012) [16], type 35 RA 35 RA 53 Patients with s (RA
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
TB Prevention Who and How to Screen
 TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
DRAFT. Remission rates, calculated using observed case (OC) analyses were as follows: Year 1 Year 2 Year 3 Year 4 All patients 62.
 analyses were as follows: Year 1 Year 2 Year 3 Year 4 All patients 62.") DRAFT New Efficacy Data Shows Cimzia (certolizumab pegol) Provides Long-Term Remission of Moderate to Severe Crohn s Disease Regardless of Prior Anti-TNF Exposure, According to Data Presented at DDW Oral
DRAFT New Efficacy Data Shows Cimzia (certolizumab pegol) Provides Long-Term Remission of Moderate to Severe Crohn s Disease Regardless of Prior Anti-TNF Exposure, According to Data Presented at DDW Oral
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
Please distribute a copy of this information to each provider in your organization.
 HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
Interpretation of TST & IGRA results. Objectives
 Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
11/1/2017. Disclosures. Update In Tuberculosis, Indiana Outline/Objectives. Pathogenesis of M.tb Global/U.S. TB Burden, 2016
 Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Peggy Leslie-Smith, RN
 Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
ATS/CDC Guidelines for Treating Latent TB Infection
 TB Intensive Tyler, Texas June 2-4, 2010 ATS/CDC Guidelines for Treating Latent TB Infection Timothy R. Aksamit, MD June 2, 2010 ATS/CDC Guidelines for Treating LTBI Tuberculosis Intensive University of
TB Intensive Tyler, Texas June 2-4, 2010 ATS/CDC Guidelines for Treating Latent TB Infection Timothy R. Aksamit, MD June 2, 2010 ATS/CDC Guidelines for Treating LTBI Tuberculosis Intensive University of
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 TB Partial Update Appendix 1 - Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial
TB Partial Update Appendix 1 - Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]
![CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]](/thumbs/89/99628771.jpg "CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]") CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
Infectious and Other Complications of New Immunobiologic Agents Used by HIV-Infected Individuals
 Infectious and Other Complications of New Immunobiologic Agents Used by HIV-Infected Individuals Peter Chin-Hong, MD Professor of Medicine University of California San Francisco San Francisco, CA Learning
Infectious and Other Complications of New Immunobiologic Agents Used by HIV-Infected Individuals Peter Chin-Hong, MD Professor of Medicine University of California San Francisco San Francisco, CA Learning
Disclosures. Updates in TB for the PCP: Opportunities for Prevention. Objectives PART 1: WHY TEST? 4/14/2016. None
 Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Regulatory Status FDA- approved indication: Simponi and Simponi ARIA are tumor necrosis factor (TNF) blockers indicated for the treatment of: (2-3)
 blockers indicated for the treatment of: (2-3)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 9 Last Review Date: March 16, 2018 Simponi / Simponi
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 9 Last Review Date: March 16, 2018 Simponi / Simponi
A Clinician s Perspective: Improving Rheumatology Patient Care Using the T-SPOT.TB Test
 A Clinician s Perspective: Improving Rheumatology Patient Care Using the T-SPOT.TB Test Solomon Forouzesh, MD, FACD, FACR Medical Director Arthritis Care & Treatment Center Clinical Associate Professor
A Clinician s Perspective: Improving Rheumatology Patient Care Using the T-SPOT.TB Test Solomon Forouzesh, MD, FACD, FACR Medical Director Arthritis Care & Treatment Center Clinical Associate Professor
Infectious and Other Complications of Immunobiologic Agents Used by Individuals With HIV Infection
 Infectious and Other Complications of Immunobiologic Agents Used by Individuals With HIV Infection Peter Chin-Hong, MD Professor of Medicine University of California San Francisco San Francisco, California
Infectious and Other Complications of Immunobiologic Agents Used by Individuals With HIV Infection Peter Chin-Hong, MD Professor of Medicine University of California San Francisco San Francisco, California
TB Update: March 2012
 TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
New Cimzia data, with sites in the US, demonstrate safety and efficacy, increased participation in social activities for adult RA patients
 Long-term Cimzia (certolizumab pegol) data demonstrated rapid sustained improvements in clinical outcomes and quality of life in moderate to severe rheumatoid arthritis (RA) patients New Cimzia data, with
Long-term Cimzia (certolizumab pegol) data demonstrated rapid sustained improvements in clinical outcomes and quality of life in moderate to severe rheumatoid arthritis (RA) patients New Cimzia data, with
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial update) 1.1 Short title Tuberculosis
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial update) 1.1 Short title Tuberculosis
Testing for Tuberculosis Infection and Disease: The Expanding Role of Blood-based Assays
 Complimentary CME Testing for Tuberculosis Infection and Disease: The Expanding Role of Blood-based Assays POWERED BY Program Description Screening and testing guidelines are an important component in
Complimentary CME Testing for Tuberculosis Infection and Disease: The Expanding Role of Blood-based Assays POWERED BY Program Description Screening and testing guidelines are an important component in
Tuberculosis: update 2013
 Tuberculosis: update 2013 William R. Bishai, MD, PhD Center for TB Research Division of Infectious Diseases Department of Medicine Johns Hopkins School of Medicine Question 1 A TB speaker at a major conference
Tuberculosis: update 2013 William R. Bishai, MD, PhD Center for TB Research Division of Infectious Diseases Department of Medicine Johns Hopkins School of Medicine Question 1 A TB speaker at a major conference
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines
 Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas August 2, 2011 ATS/CDC Guidelines for Treating LTBI Timothy Aksamit, MD April 6, 2011 Timothy Aksamit, MD has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 2, 2011 ATS/CDC Guidelines for Treating LTBI Timothy Aksamit, MD April 6, 2011 Timothy Aksamit, MD has the following disclosures to make: No conflict of interests
Safety of biologics in rheumatoid arthritis
 Placebo-controlled trials of biological therapies in the treatment of rheumatoid arthritis have demonstrated significant efficacy with acceptable safety profiles. Nevertheless, while biologic treatment
Placebo-controlled trials of biological therapies in the treatment of rheumatoid arthritis have demonstrated significant efficacy with acceptable safety profiles. Nevertheless, while biologic treatment
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
HELPING YOU AND YOUR PATIENTS TALK OPENLY ABOUT MODERATELY TO SEVERELY ACTIVE RA
 SIMPONI ARIA (golimumab) is indicated for the treatment of adults with moderately to severely active rheumatoid arthritis (RA) in combination with MTX, active psoriatic arthritis, and active ankylosing
SIMPONI ARIA (golimumab) is indicated for the treatment of adults with moderately to severely active rheumatoid arthritis (RA) in combination with MTX, active psoriatic arthritis, and active ankylosing
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Latent TB Infection (LTBI) Strategies for Detection and Management
 Strategies for Detection and Management") Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Welcome to Rheumatology Highlights Report; I m Dr. Len Calabrese from the R.J. Fasenmyer Center for Clinical Immunology. And, in the next 15 minutes
 Welcome to Rheumatology Highlights Report; I m Dr. Len Calabrese from the R.J. Fasenmyer Center for Clinical Immunology. And, in the next 15 minutes I m going to update you on the safety of biologics.
Welcome to Rheumatology Highlights Report; I m Dr. Len Calabrese from the R.J. Fasenmyer Center for Clinical Immunology. And, in the next 15 minutes I m going to update you on the safety of biologics.
Latent Tuberculosis Best Practices
 Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Regulatory Status FDA-approved indication: Orencia is a selective T cell costimulation modulator indicated for: (1)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.18 Subject: Orencia Page: 1 of 8 Last Review Date: March 16, 2018 Orencia Description Orencia (abatacept)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.18 Subject: Orencia Page: 1 of 8 Last Review Date: March 16, 2018 Orencia Description Orencia (abatacept)
PRIOR AUTHORIZATION REQUEST GUIDE
 PRIOR AUTHORIZATION REQUEST GUIDE Drafting a Prior Authorization Request The following information is presented for informational purposes only and is not intended to provide reimbursement or legal advice.
PRIOR AUTHORIZATION REQUEST GUIDE Drafting a Prior Authorization Request The following information is presented for informational purposes only and is not intended to provide reimbursement or legal advice.
TB Intensive. San San Antonio, Texas. December 1-3, 2010
 TB Intensive San Antonio, Texas December 1-3, 2010 ATS/CDC Guidelines for Treating Latent TB Infection Timothy Aksamit, MD; Mayo Clinic December 1, 2010 ATS/CDC Guidelines for Treating LTBI Tuberculosis
TB Intensive San Antonio, Texas December 1-3, 2010 ATS/CDC Guidelines for Treating Latent TB Infection Timothy Aksamit, MD; Mayo Clinic December 1, 2010 ATS/CDC Guidelines for Treating LTBI Tuberculosis
Les 2 articles qui peuvent changer votre pratique sur: Vaccination et biothérapies
 Les 2 articles qui peuvent changer votre pratique sur: Vaccination et biothérapies VZV Epidemiology and Pathogenesis 98% adults Respiratory spread 1,000,000/year and increasing CMI continuously boosted
Les 2 articles qui peuvent changer votre pratique sur: Vaccination et biothérapies VZV Epidemiology and Pathogenesis 98% adults Respiratory spread 1,000,000/year and increasing CMI continuously boosted
Treat to a Target The New Paradigm in the Management of RA. Boulos Haraoui, MD FRCPC Université de Montréal Institut de rhumatologie de Montréal
 Treat to a Target The New Paradigm in the Management of RA Boulos Haraoui, MD FRCPC Université de Montréal Institut de rhumatologie de Montréal Disclosure Dr Boulos Haraoui Advisor/Research Grants/Speakers
Treat to a Target The New Paradigm in the Management of RA Boulos Haraoui, MD FRCPC Université de Montréal Institut de rhumatologie de Montréal Disclosure Dr Boulos Haraoui Advisor/Research Grants/Speakers