BLEEDING (PLATELET) DISORDER. IAP UG Teaching slides
|
|
|
- Jeffrey Wood
- 5 years ago
- Views:
Transcription
1 BLEEDING (PLATELET) DISORDER 1
2 APPROACH The initial set of questions should establish the following: (1) the most common site and type of bleeding (e.g., mucocutaneous versus articular or deep muscle), (2) bleeding on hemostatic challenge such as surgeries or trauma, and (3) family history of bleeding. 2
3 Clinical Characteristic Site of bleeding Primary Hemostatic Defect Skin, mucous membranes Clotting Factor Deficiency Soft tissues, muscles, joints Bleeding after Yes Rare minor cuts Petechiae present absent Ecchymosis Small, superficial Large, deep, palpable Hemarthrosis Rare Common Bleeding after trauma/surgery Immediate Delayed 3

4 PLATELET IN VASCULAR INJURY 4 4
5 HISTORY Large bruises without previous significant trauma, disseminated petechiae,intramuscular hematomas, hemarthrosis (joint effusion, warmth, and pain with passive movement) usually indicate a bleeding disorder In young children, refusal to walk is often a sign for an extremity related bleed and could represent the first sign of hemarthrosis in a boy with hemophilia 5
6 HISTORY Symptoms of bleeding disorders, could be easy bruising and mucosal bleeding (e.g. Epistaxis,menorrhagia,oropharyngeal) Inflicted trauma is most likely to manifest over the head, chest, back, and long bones (and may retain the outlines of the instrument used to inflict harm), whereas bruises associated with primary hemostasis defects are usually located over areas of typical childhood trauma, such as bony protuberances of extremities or spinous processes 6
7 HISTORY Epistaxis is a frequent presenting sign in children with hemostatic disorders Epistaxis is also a common complaint among healthy children, usually the result of local aggravating factors (dry nasal mucosa, trauma, allergic rhinitis). 7
8 HISTORY Menorrhagia is also a frequent presenting sign for mild or moderate bleeding disorders (including VWD, platelet function disorders, and other coagulopathies) and can quickly lead to severe anaemia and decreased quality of life. 8
9 HISTORY Profuse bleeding into soft tissues or joints suggests deficiency of a coagulation factor (such as factors VIII or IX). Umbilical stump bleeding is typically seen with factor XIII deficiency, but it may also occur with deficiencies of prothrombin, factor X, and fibrinogen 9
10 HISTORY The main categories to be considered should include anatomic abnormalities, quantitative and qualitative platelet defects affecting platelet plug formation (primary hemostasis), and quantitative and qualitative defects of clot propagation (secondary hemostasis). Differentiation also must be made between inherited and acquired disorders. 10
11 HISTORY Information about the patient s previous response to hemostatic challenges (e.g., surgical procedures, invasive dental work, traumatic injuries) is an essential part of the initial evaluation Family history is also a key component in establishing both the likelihood of an inherited bleeding disorder and its specific nature. 11
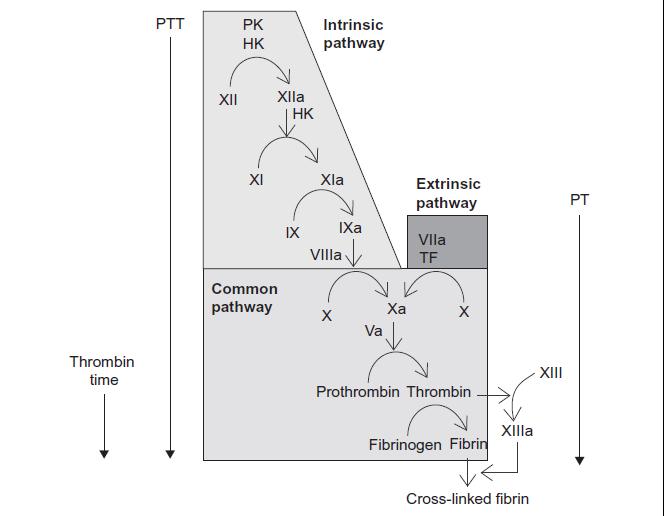
12 The three phases of coagulation occur on different cell surfaces: initiation on the tissue factor bearing cell; amplification on the platelet as it becomes activated; and propagation on the activated platelet surface 12
13 HISTORY A sick child with fever, shock, and mucocutaneous purpura may have disseminated intravascular coagulation (DIC) associated with bacteremia. Hemophilia should be considered in a male toddler who has just started crawling and exhibits subcutaneous or joint bleeding, or who bleeds after circumcision. A girl who has had severe menorrhagia since menarche may have VWD. 13
14 HISTORY A well appearing child covered with petechiae likely has immune thrombocytopenia, but if the lesions are localized to the buttocks, ankles, and feet, and they present as palpable bruises, Henoch Schönlein purpura should be considered The prevalence of bleeding disorders in women with menorrhagia is as high as 20%, and menorrhagia is a common initial symptom in women with VWD (approximately 90% of female patients) 14
15 HISTORY Medical disorder that may affect hemostasis, hepatic or renal disease, Malabsorption syndrome, or Ehlers Danlos syndrome (EDS) or another connective tissue disorder. Generally, early age of onset correlates with more severe bleeding and may indicate a congenital cause. Bleeding that develops later in childhood may indicate either an acquired problem or a milder congenital bleeding disorder 15 15
16 HISTORY An X linked recessive inheritance pattern (maternal cousins, uncles, and grandfather) suggests a diagnosis of hemophilia A or B, Autosomal dominant pattern would be more consistent with VWD or hereditary haemorrhagic telangiectasia. Most other clinically relevant clotting factor deficiencies are inherited in an autosomal recessive manner 16
17 HISTORY A number of drugs can cause thrombocytopenia (e.g., quinine or quinidine, rifampin, trimethoprimsulfamethoxazole, carbamazepine, cimetidine, ranitidine, valproic acid) platelet dysfunction (nonsteroidal anti inflammatory drugs [NSAIDs] such as ibuprofen [reversible effect] and aspirin [irreversible]). 17
18 PHYSICAL EXAMINATION Signs of severe bleeding related anaemia or intravascular volume loss, such as tachycardia (early finding) or hypotension (late finding). observe the pattern of bleeding stigmata the presence of petechiae indicates a defect in primary hemostasis (platelet number or function or vascular integrity). 18
19 PHYSICAL EXAMINATION Ecchymoses are palpable purplish lesions induced by subcutaneous bleeding and usually indicate a defect in secondary hemostasis (clot propagation), such as deficiency of a coagulation factor Hemarthrosis, associated with severe coagulation factor deficiency 19
20 PHYSICAL EXAMINATION Hepatomegaly and splenic enlargement may point toward coagulopathy associated with systemic disorders such as leukaemia or hepatocellular disease. 20
21 LAB Complete blood count with evaluation of platelet number, size, morphology, PT, APTT, and thrombin time (TT) to help in the process of differential diagnosis 21
22 LAB 22
23 23
24 LAB 24
25 PLATELETS Size: 1 4 μm (younger platelets are larger). Distribution: one third in the spleen, two thirds in circulation Average lifespan: 9 10 days Platelets critical component for the first phase of hemostasis (formation of the platelet plug), which can halt the loss of blood from vessels whose endothelial integrity has been interrupted 25
26 PLATELETS Typically involve the skin or mucous membranes and include petechiae, ecchymosis, epistaxis, menorrhagia, and gastrointestinal hemorrhage. Intracranial bleeding can occur, but it is infrequent Inherited platelet disorders can involve a qualitative and/or quantitative defect and are often broadly classified according to one of these two categories 26
27 BERNAD SOULIER SYNDROME Bernard Soulier syndrome, a severe congenital platelet function disorder, is caused by absence or severe deficiency of the VWF receptor (GPIb complex) on the platelet membrane. Thrombocytopenia, with giant platelets and markedly prolonged bleeding time (>20 min) or PFA 100 closure time. Platelet aggregation tests show absent ristocetininduced platelet aggregation, but normal aggregation to all other agonists. 27
28 GLANZMANN THROMBASTHENIA Glanzmann thrombasthenia is a congenital disorder associated with severe platelet dysfunction that yields prolonged bleeding time and a normal platelet count. Platelets have normal size and morphologic features on the peripheral blood smear, and closure times for PFA 100 or bleeding time are markedly abnormal 28
29 GLANZMANN THROMBASTHENIA This disorder is caused by deficiency of the platelet fibrinogen receptor αiib β3, the major integrin complex on the platelet surface that undergoes conformational changes by inside out signalling when platelets are activated 29
30 Dense body deficiency is characterized by absence of the granules that contain ADP, ATP, Ca2+, and serotonin. This disorder is diagnosed by the finding that ATP is not released on platelet aggregation studies and ideally is characterized by electron microscopic studies. Gray platelet syndrome is caused by the absence of platelet α granules, resulting in platelets that appear gray on Wright stain of peripheral blood. In this rare syndrome, aggregation and release are absent with most agonists other than thrombin and ristocetin. 30
31 For both Bernard Soulier syndrome and Glanzmann thrombasthenia, the diagnosis is confirmed by flow cytometric analysis of the patient's platelet glycoproteins. For individuals with Bernard Soulier syndrome or Glanzmann thrombasthenia, platelet transfusions of 1 U/5 10 kg corrects the defect in hemostasis and may be lifesaving. Desmopressin 0.3 µg/kg IV may be used for mild to moderate bleeding episodes. 31
32 WISKOTT ALDRICH SYNDROME This syndrome has X linked inheritance and has the classic features of thrombocytopenia, eczema, recurrent bacterial and viral infections WAS has abnormal T cell function and a propensity to develop autoimmune disorders 32
33 WISKOTT ALDRICH SYNDROME Recurrent pyogenic infections, including otitis media, pneumonia and skin infections. There is also lowered resistance to nonbacterial infections, including herpes simplex and Pneumocystis jiroveci (formerly carinii) pneumonia Thrombocytopenia (platelet count 10, ,000/mm3); microthrombocytes; low mean platelet volume (MPV). 33
34 CAMT Congenital Amegakaryocytic Thrombocytopenia (CAMT) is a bone marrow failure syndrome that presents with isolated thrombocytopenia in the neonatal period. Inheritance is autosomal recessive. The most common age at diagnosis of the thrombocytopenia is within the first month, because of petechiae and other bleeding symptoms. The diagnosis of CAMT, however, is not usually made until the infant is several weeks or months old when the bone marrow is examined. 34
35 TYPE 2 b VWD Type 2B von Willebrand Disease. Type 2B VWD is due to a mutant VWF molecule that binds spontaneously to platelets under physiologic shear. This results in clearance of the highest molecularweight multimers and usually mild thrombocytopenia 35
36 ITP Immune thrombocytopenia is a disorder caused by antiplatelet antibodies which lead to an accelerated destruction of platelets and an inhibition of the production of platelets. ITP is the most common cause of thrombocytopenia in children. Peak occurrence is between 2 and 5 years of age. In most children the disease is self limited, with resolution in 80% of patients within 6 12 months from diagnosis 36
37 ITP Antibody mediated destruction: Most of the identified autoantibodies are directed against GPIIb GPIIIa, GPIb GPIX and GPIa Iia Impaired megakaryopoiesis Antibody and cellular cytotoxicity and immune cellderived cytokines have been implicated in impairment of megakaryocytes 37
38 CLINICAL FEATURES Typically patients are otherwise well and present with petechiae, purpura and no palpable ecchymosis 1 3 weeks after a viral infection. It may also occur after rubella, rubeola, chickenpox or live virus vaccination. Occasionally patients may present with mucosal bleeding (hematuria, hematochezia, Menometrorrhagia, or epistaxis). Most often, bleeding symptoms are mild, but rarely patients may develop severe bleeding including intracranial hemorrhage 38
39 American Society of Hematology (ASH) DEFINITIONS Primary ITP was defined by the IWG as a platelet count less than 100 X 10 9/L The IWG also defines ITP as newly diagnosed (diagnosis to 3 months), persistent (3 to 12 months from diagnosis), or chronic (lasting for more than 12 months). Complete response (CR) :A platelet count 100 X 10 9 /L measured on 2 occasions 7 days apart and the absence of bleeding. 39
40 ASH DEFINITIONS Response (R) :A platelet count 30 X 10 9 /L and a greater than 2 fold increase in platelet count from baseline measured on 2 occasions 7 days apart and the absence of bleeding No response (NR) :A platelet count 30 X 10 9 /L or a less than 2 fold increase in platelet count from baseline or the presence of bleeding. Platelet count must be measured on 2 occasions more than a day apart. 40
 and increased numbers of megakaryocytes, many of which appear immature (bone marrow aspirate")
41 Blood smear and bone marrow aspirate from a child who had ITP showing large platelets (blood smear [left]) and increased numbers of megakaryocytes, many of which appear immature (bone marrow aspirate 41
42 TREATMENT No therapy other than education and counselling of the family and patient for patients A single dose of IVIG [intravenous immunoglobulin] ( g/kg) 1 2 days Prednisone. Doses of prednisone of 1 4 mg/kg/24 hr appear to induce a more rapid rise in platelet count than in untreated patients with ITP 42
43 TREATMENT Intravenous anti D therapy. For Rh positive patients, IV anti D at a dose of μg/kg causes a rise in platelet count to > /L in 80 90% of patients within hr The role of splenectomy in ITP should be reserved for 1 of 2 circumstances. The older child ( 4 yr) with severe ITP that has lasted >1 yr (chronic ITP) and whose symptoms are not easily controlled with therapy is a candidate for splenectomy 43
44 ASH GUIDELINES Bone marrow examination is unnecessary in children and adolescents with the typical features of ITP (grade 1B). Bone marrow examination is not necessary in children who fail IV Ig therapy (grade 1B). 44

45 Thank You 45
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College
 Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN
 Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
Coagulation Disorders. Dr. Muhammad Shamim Assistant Professor, BMU
 Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Bleeding disorders. Hemostatic failure: Inappropriate and excessive bleeding either spontaneous or in response to injury.
 1 Bleeding disorders Objectives: 1. Discuss briefly the physiology of hemostasis. 2. Define the mechanisms of thrombocytopenia and the relative bleeding risk at any given platelet count. 3. Be able to
1 Bleeding disorders Objectives: 1. Discuss briefly the physiology of hemostasis. 2. Define the mechanisms of thrombocytopenia and the relative bleeding risk at any given platelet count. 3. Be able to
Bleeding Disorders. Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph
 Bleeding Disorders Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph Normal hemostasis The normal hemostatic response involves interactions among: The blood vessel wall (endothelium)
Bleeding Disorders Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph Normal hemostasis The normal hemostatic response involves interactions among: The blood vessel wall (endothelium)
Haemostasis & Coagulation disorders Objectives:
 Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Platelet Disorders. By : Saja Al-Oran
 Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Hemostatic System - general information
 PLATELET DISORDERS Hemostatic System - general information Normal hemostatic system vessel wall circulating blood platelets blood coagulation and fibrynolysis Bleeding Diathesis inherited or acquired defects
PLATELET DISORDERS Hemostatic System - general information Normal hemostatic system vessel wall circulating blood platelets blood coagulation and fibrynolysis Bleeding Diathesis inherited or acquired defects
BLEEDING DISORDERS Simple complement:
 BLEEDING DISORDERS Simple complement: 1. Select the statement that describe the thrombocytopenia definition: A. Marked decrease of the Von Willebrandt factor B. Absence of antihemophilic factor A C. Disorder
BLEEDING DISORDERS Simple complement: 1. Select the statement that describe the thrombocytopenia definition: A. Marked decrease of the Von Willebrandt factor B. Absence of antihemophilic factor A C. Disorder
EDUCATIONAL COMMENTARY PLATELET DISORDERS
 EDUCATIONAL COMMENTARY PLATELET DISORDERS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Earn
EDUCATIONAL COMMENTARY PLATELET DISORDERS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Earn
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
Y. Helen Zhang, MD Andy Nguyen, MD 10/28/2012
 Y. Helen Zhang, MD Andy Nguyen, MD 10/28/2012 Clinical History Patient: 23-year-old female Clinical course: status-post cholecystectomy, complicated by retained common bile duct stones. Following three
Y. Helen Zhang, MD Andy Nguyen, MD 10/28/2012 Clinical History Patient: 23-year-old female Clinical course: status-post cholecystectomy, complicated by retained common bile duct stones. Following three
Easy Bleeding General Presentation
 Easy Bleeding General Presentation It is not uncommon for children to bleed and bruise after experiencing trauma. However, a child may also have an underlying coagulopathy, which results in easy and possibly
Easy Bleeding General Presentation It is not uncommon for children to bleed and bruise after experiencing trauma. However, a child may also have an underlying coagulopathy, which results in easy and possibly
Congenital bleeding disorders
 Congenital bleeding disorders Overview Factor VIII von Willebrand Factor Complex factor VIII von Willebrand factor (vwf) complex circulate as a complex + factor IX intrinsic pathway Platelets bind via
Congenital bleeding disorders Overview Factor VIII von Willebrand Factor Complex factor VIII von Willebrand factor (vwf) complex circulate as a complex + factor IX intrinsic pathway Platelets bind via
Approach to bleeding disorders &treatment. by RAJESH.N General medicine post graduate
 Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Easy bruising vs Coagulopathy
 Easy bruising vs Coagulopathy Sept. 19, 2015 Lakehead Summer School Chris Hillis, MD MSc FRCPC hillis@hhsc.ca @HemeHillis Aim & Objectives Aim: To increase comfort in detecting non-pathologic bleeding
Easy bruising vs Coagulopathy Sept. 19, 2015 Lakehead Summer School Chris Hillis, MD MSc FRCPC hillis@hhsc.ca @HemeHillis Aim & Objectives Aim: To increase comfort in detecting non-pathologic bleeding
Haemorrhagic Disorders. Dr. Bashar Department of Pathology Mosul Medical College
 Haemorrhagic Disorders Dr. Bashar Department of Pathology Mosul Medical College Hemorrhagic Disorders These include Disorders of platelets. Disorders of blood vessels. Disorders of coagulation & fibrinolysis.
Haemorrhagic Disorders Dr. Bashar Department of Pathology Mosul Medical College Hemorrhagic Disorders These include Disorders of platelets. Disorders of blood vessels. Disorders of coagulation & fibrinolysis.
Bleeding Disorders: (Hemorrhagic Diatheses) Tests used to evaluate different aspects of hemostasis are the following:
 Tests used to evaluate different aspects of hemostasis are the following:") Bleeding Disorders: (Hemorrhagic Diatheses) Excessive bleeding can result from: 1. Increased fragility of vessels. 2. Platelet deficiency or dysfunction. 3. Derangement of coagulation. 4. Combinations
Bleeding Disorders: (Hemorrhagic Diatheses) Excessive bleeding can result from: 1. Increased fragility of vessels. 2. Platelet deficiency or dysfunction. 3. Derangement of coagulation. 4. Combinations
Bleeding Disorders HOPE Maram Al-anbar
 Bleeding Disorders HOPE Maram Al-anbar 9-9 - 2014 ^^ Attention Please ^^ We ( correction team of pediatric package^hope/2010^ ) had decided to make one lecture of bleeding disorders in place of the two
Bleeding Disorders HOPE Maram Al-anbar 9-9 - 2014 ^^ Attention Please ^^ We ( correction team of pediatric package^hope/2010^ ) had decided to make one lecture of bleeding disorders in place of the two
Guidelines for Shared Care Centres and Community Staff
 Reference: CG1410 Written by: Dr Jeanette Payne Peer reviewer Dr Jenny Welch Approved: February 2016 Approved by D&TC: 8th January 2016 Review Due: February 2019 Intended Audience This document contains
Reference: CG1410 Written by: Dr Jeanette Payne Peer reviewer Dr Jenny Welch Approved: February 2016 Approved by D&TC: 8th January 2016 Review Due: February 2019 Intended Audience This document contains
Acute Immune Thrombocytopenic Purpura (ITP) in Childhood
 in Childhood") Acute Immune Thrombocytopenic Purpura (ITP) in Childhood Guideline developed by Robert Saylors, MD, in collaboration with the ANGELS team. Last reviewed by Robert Saylors, MD September 22, 2016. Key Points
Acute Immune Thrombocytopenic Purpura (ITP) in Childhood Guideline developed by Robert Saylors, MD, in collaboration with the ANGELS team. Last reviewed by Robert Saylors, MD September 22, 2016. Key Points
Sysmex Educational Enhancement and Development No
 SEED Coagulation Sysmex Educational Enhancement and Development No 2 2016 An approach to the bleeding patient The purpose of this newsletter is to provide an overview of the approach to the bleeding patient
SEED Coagulation Sysmex Educational Enhancement and Development No 2 2016 An approach to the bleeding patient The purpose of this newsletter is to provide an overview of the approach to the bleeding patient
Approach To A Bleeding Patient
 ABDUL MAJEED, RAHUL RAJEEV REVIEW ARTICLE INTRODUCTION Hemostasis is the process of forming clots in the walls of damaged blood vessels and preventing blood loss while maintaining blood in a fluid state
ABDUL MAJEED, RAHUL RAJEEV REVIEW ARTICLE INTRODUCTION Hemostasis is the process of forming clots in the walls of damaged blood vessels and preventing blood loss while maintaining blood in a fluid state
The LaboratoryMatters
 Laboratory Medicine Newsletter for clinicians, pathologists & clinical laboratory technologists. A Initiative. HEMOSTASIS AND THE LABORATORY This issue highlights: Primary Hemostasis Screening Tests Case
Laboratory Medicine Newsletter for clinicians, pathologists & clinical laboratory technologists. A Initiative. HEMOSTASIS AND THE LABORATORY This issue highlights: Primary Hemostasis Screening Tests Case
HAEMORRHAGIA Bleeding
 HAEMORRHAGIA Bleeding Cassification Size Location pathomechanism Hematoma: external or may be enclosed within a tissue petechiae : 1-2 mm hemorrhages into skin, mucous membranes, or serosal surfaces increased
HAEMORRHAGIA Bleeding Cassification Size Location pathomechanism Hematoma: external or may be enclosed within a tissue petechiae : 1-2 mm hemorrhages into skin, mucous membranes, or serosal surfaces increased
The Child with a Hematologic Alteration
 47 The Child with a Hematologic Alteration HELPFUL HINT Review the anatomy and physiology of the hematologic system in an anatomy and physiology textbook. MATCHING KEY TERMS Match the term with the correct
47 The Child with a Hematologic Alteration HELPFUL HINT Review the anatomy and physiology of the hematologic system in an anatomy and physiology textbook. MATCHING KEY TERMS Match the term with the correct
Bleeding and Thrombotic Disorders. Kristine Krafts, M.D.
 Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
GOOD MORNING! Thursday, July Heidi Murphy, MD Leslie Carter-King, MD
 GOOD MORNING! Thursday, July 10 2014 Heidi Murphy, MD Leslie Carter-King, MD PREP QUESTION Almost all infants experience a transient increase in bilirubin concentrations known as physiologic jaundice during
GOOD MORNING! Thursday, July 10 2014 Heidi Murphy, MD Leslie Carter-King, MD PREP QUESTION Almost all infants experience a transient increase in bilirubin concentrations known as physiologic jaundice during
There are two main causes of a low platelet count
 Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
Pathology note 8 BLEEDING DISORDER
 Pathology note 8 BLEEDING DISORDER Slide75 ( Types of clotting factors deficiency): Today we will talk about public public factor deficiency it could be acquired or inherited, acquired diseases are more
Pathology note 8 BLEEDING DISORDER Slide75 ( Types of clotting factors deficiency): Today we will talk about public public factor deficiency it could be acquired or inherited, acquired diseases are more
BLEEDING DISORDERS. JC Opperman 2012
 BLEEDING DISORDERS JC Opperman 2012 Primary and Secondary Clotting Laboratory Tests Routine screening tests Prothrombin time (PT) (INR) increased in neonates (12-18 sec) Partial thromboplastin time (PTT)
BLEEDING DISORDERS JC Opperman 2012 Primary and Secondary Clotting Laboratory Tests Routine screening tests Prothrombin time (PT) (INR) increased in neonates (12-18 sec) Partial thromboplastin time (PTT)
Commonly Encountered Hematologic Chief Complaints in the Pediatric Pa8ent Black Hills Pediatric Symposium 6/23/17 Sam Milanovich, MD Pediatric
 Commonly Encountered Hematologic Chief Complaints in the Pediatric Pa8ent Black Hills Pediatric Symposium 6/23/17 Sam Milanovich, MD Pediatric Hematology/Oncology Sanford Children s Specialty Clinic Sioux
Commonly Encountered Hematologic Chief Complaints in the Pediatric Pa8ent Black Hills Pediatric Symposium 6/23/17 Sam Milanovich, MD Pediatric Hematology/Oncology Sanford Children s Specialty Clinic Sioux
INHERITED COAGULOPATHY
 Disorder Etiology Pathophysiology and Presentation Lab Findings and Diagnosis Treatment INHERITED COAGULOPATHY HEMOPHILIA A and B Hemophilia A: deficiency in XIII (85%) Hemophilia B: deficiency in IX (15%)
Disorder Etiology Pathophysiology and Presentation Lab Findings and Diagnosis Treatment INHERITED COAGULOPATHY HEMOPHILIA A and B Hemophilia A: deficiency in XIII (85%) Hemophilia B: deficiency in IX (15%)
HAEMORRHAGIA Bleeding
 HAEMORRHAGIA Bleeding Cassification Size Location pathomechanism Hematoma: external or may be enclosed within a tissue petechial rash (spot) : 1-2 mm hemorrhages into skin, mucous membranes, or serosal
HAEMORRHAGIA Bleeding Cassification Size Location pathomechanism Hematoma: external or may be enclosed within a tissue petechial rash (spot) : 1-2 mm hemorrhages into skin, mucous membranes, or serosal
von Willebrand Disease
 von Willebrand Disease Jeremy Robertson Paediatric Haematologist Royal Children s s Hospital & Pathology Queensland Foglo,, April 1924: the journey begins Oskar and Augusta sail to Helsinki... ...to o
von Willebrand Disease Jeremy Robertson Paediatric Haematologist Royal Children s s Hospital & Pathology Queensland Foglo,, April 1924: the journey begins Oskar and Augusta sail to Helsinki... ...to o
Wiskott-Aldrich Syndrome
 chapter 7 Wiskott-Aldrich Syndrome Wiskott-Aldrich syndrome is a primary immunodeficiency disease involving both T- and B-lymphocytes. In addition, the blood cells that help control bleeding, called platelets
chapter 7 Wiskott-Aldrich Syndrome Wiskott-Aldrich syndrome is a primary immunodeficiency disease involving both T- and B-lymphocytes. In addition, the blood cells that help control bleeding, called platelets
V.N. KARAZIN KHARKOV NATIONAL UNIVERSITY
 V.N. KARAZIN KHARKOV NATIONAL UNIVERSITY Kharkov Regional Centre of Cardiovascular surgery V.N. Karazin Kharkov National University Department of Internal Medicine Immune thrombocytopenic purpura Abduyeva
V.N. KARAZIN KHARKOV NATIONAL UNIVERSITY Kharkov Regional Centre of Cardiovascular surgery V.N. Karazin Kharkov National University Department of Internal Medicine Immune thrombocytopenic purpura Abduyeva
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust
 Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
Contemporary perspectives and initial management of pediatric ITP. William Beau Mitchell, MD Weill Cornell Medical College New York, NY USA
 Contemporary perspectives and initial management of pediatric ITP William Beau Mitchell, MD Weill Cornell Medical College New York, NY USA Case Presentation 5 year old female Bruises on trunk, extremities
Contemporary perspectives and initial management of pediatric ITP William Beau Mitchell, MD Weill Cornell Medical College New York, NY USA Case Presentation 5 year old female Bruises on trunk, extremities
Miss. kamlah ahmed 1
 Miss. kamlah ahmed 1 Anatomy & Physiology Blood has two compartments: 1- a fluid portion called plasma. 2- a cellular portion known as the formed elements of the blood. Which are RBC (erythrocytes), WBC
Miss. kamlah ahmed 1 Anatomy & Physiology Blood has two compartments: 1- a fluid portion called plasma. 2- a cellular portion known as the formed elements of the blood. Which are RBC (erythrocytes), WBC
GLANZMANN S THROMBASTHENIA. Stacey Shiovitz January 13, 2012
 GLANZMANN S THROMBASTHENIA Stacey Shiovitz January 13, 2012 HELP!! MY PATIENTHASGT DO YOU EVEN KNOW WHAT THAT IS? CASE 27yo woman presented tdto gynecology clinic i for menorrhagia x 10 days Bleeding started
GLANZMANN S THROMBASTHENIA Stacey Shiovitz January 13, 2012 HELP!! MY PATIENTHASGT DO YOU EVEN KNOW WHAT THAT IS? CASE 27yo woman presented tdto gynecology clinic i for menorrhagia x 10 days Bleeding started
Hematologic Disorders. Assistant professor of anesthesia
 Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
TREATMENT & MANAGEMENT OF VON WILLEBRAND DISEASE
 TREATMENT & MANAGEMENT OF VON WILLEBRAND DISEASE Dr Susan Russell Director HTC Sydney Children s Hospital, Randwick HFA Meeting 2015 What is von Willebrand Factor? VWF is a large multimeric protein Two
TREATMENT & MANAGEMENT OF VON WILLEBRAND DISEASE Dr Susan Russell Director HTC Sydney Children s Hospital, Randwick HFA Meeting 2015 What is von Willebrand Factor? VWF is a large multimeric protein Two
GUIDELINE: ASSESSMENT OF BRUISING & BLEEDING IN CHILDREN. All children in whom there is concern regarding bruising / bleeding
 GUIDELINE: ASSESSMENT OF BRUISING & BLEEDING IN CHILDREN Reference: Bruising / Bleeding / NAI Version No: 1 Applicable to All children in whom there is concern regarding bruising / bleeding Classification
GUIDELINE: ASSESSMENT OF BRUISING & BLEEDING IN CHILDREN Reference: Bruising / Bleeding / NAI Version No: 1 Applicable to All children in whom there is concern regarding bruising / bleeding Classification
A s doctors who care for children, we have a
 1163 PERSONAL PRACTICE The bleeding child; is it NAI? A E Thomas... As a paediatric haematologist, the question of whether a child has been abused or whether they might have a bleeding diathesis is a question
1163 PERSONAL PRACTICE The bleeding child; is it NAI? A E Thomas... As a paediatric haematologist, the question of whether a child has been abused or whether they might have a bleeding diathesis is a question
Coagulation an Overview Dr.Abdolreza Abdolr Afrasiabi Thal assem a & Heamophili hilia G ene i tic R esearc C en er Shiraz Medical Medic University
 In The Name God Coagulation an Overview Dr.Abdolreza Afrasiabi Thalassemia & Heamophilia Genetic Research hcenter Shiraz Medical University Bleeding Clotting Hemostasis Review of platelet function Platelets
In The Name God Coagulation an Overview Dr.Abdolreza Afrasiabi Thalassemia & Heamophilia Genetic Research hcenter Shiraz Medical University Bleeding Clotting Hemostasis Review of platelet function Platelets
Hemostasis. PHYSIOLOGICAL BLOOD CLOTTING IN RESPONSE TO INJURY OR LEAK no disclosures
 Hemostasis PHYSIOLOGICAL BLOOD CLOTTING IN RESPONSE TO INJURY OR LEAK no disclosures Disorders of Hemostasis - Hemophilia - von Willebrand Disease HEMOPHILIA A defect in the thrombin propagation phase
Hemostasis PHYSIOLOGICAL BLOOD CLOTTING IN RESPONSE TO INJURY OR LEAK no disclosures Disorders of Hemostasis - Hemophilia - von Willebrand Disease HEMOPHILIA A defect in the thrombin propagation phase
Bleeding Disorders.2 MS Abdallah Awidi Abbadi.MD. FRCP.FRCPath Feras Fararjeh MD
 Bleeding Disorders.2 MS4.25.02.2019 Abdallah Awidi Abbadi.MD. FRCP.FRCPath Feras Fararjeh MD Email: abdalla.awidi@gmail.com Case 6: GT 18 yr old female was admitted with pallor, abdominal pain and gum
Bleeding Disorders.2 MS4.25.02.2019 Abdallah Awidi Abbadi.MD. FRCP.FRCPath Feras Fararjeh MD Email: abdalla.awidi@gmail.com Case 6: GT 18 yr old female was admitted with pallor, abdominal pain and gum
Form 2033 R3.0: Wiskott-Aldrich Syndrome Pre-HSCT Data
 Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: Has this patient's data been previously reported to USIDNET? USIDNET ID: Today's Date: - - Date of HSCT for which
Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: Has this patient's data been previously reported to USIDNET? USIDNET ID: Today's Date: - - Date of HSCT for which
COAGULATIONS. Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin)
, FRCP(Edin)") COAGULATIONS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin) Haemostasis-blood must be maintained in a fluid state in order to function as a transport system, but must be able to solidify to form a clot following
COAGULATIONS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin) Haemostasis-blood must be maintained in a fluid state in order to function as a transport system, but must be able to solidify to form a clot following
Platelet vs. Coagulation Bleeding. Qualitative and Quantitative Platelet Disorders. Laboratory Tests. Platelet Signaling. Jeffrey S. Jhang, M.D.
 Qualitative and Quantitative Platelet isorders Platelet vs. Coagulation Bleeding Findings Petechiae Hematomas and Hemarthroses elayed Bleeding Coagulation Rare Common Common Platelet Common Rare Rare Bleeding
Qualitative and Quantitative Platelet isorders Platelet vs. Coagulation Bleeding Findings Petechiae Hematomas and Hemarthroses elayed Bleeding Coagulation Rare Common Common Platelet Common Rare Rare Bleeding
What are InherIted platelet FunCtIon disorders?
 What are InherIted platelet FunCtIon disorders? Published by the World Federation of Hemophilia (WFH) World Federation of Hemophilia, 2010 This publication was developed by the WFH and reviewed by Dr.
What are InherIted platelet FunCtIon disorders? Published by the World Federation of Hemophilia (WFH) World Federation of Hemophilia, 2010 This publication was developed by the WFH and reviewed by Dr.
Approach to bleeding
 Approach to bleeding By Assoc. Prof. Darintr Sosothikul, MD Pediatric Hematology-Oncology division, King Chulalongkorn Memorial Hospital, Faculty of Medicine, Chulalongkorn University The mechanism of
Approach to bleeding By Assoc. Prof. Darintr Sosothikul, MD Pediatric Hematology-Oncology division, King Chulalongkorn Memorial Hospital, Faculty of Medicine, Chulalongkorn University The mechanism of
Introduction to von Willebrand Disease Mary Lesh RN, MS, CPNP
 Introduction to von Willebrand Disease Mary Lesh RN, MS, CPNP OVERVIEW Von Willebrand Disease (VWD) is the most common hereditary bleeding disorder in humans, with an estimated prevalence ranging upward
Introduction to von Willebrand Disease Mary Lesh RN, MS, CPNP OVERVIEW Von Willebrand Disease (VWD) is the most common hereditary bleeding disorder in humans, with an estimated prevalence ranging upward
Wiskott-Aldrich Registry Data Collection Form Patient Identification: Patient Name (first, middle, last)
") Patient Identification: Patient Name (first, middle, last) Patient s USIDNET Registry Number assigned after online enrollment Date of Birth / / (mm/dd/yyyy) or Year of Birth Gender: male [ ], female [
Patient Identification: Patient Name (first, middle, last) Patient s USIDNET Registry Number assigned after online enrollment Date of Birth / / (mm/dd/yyyy) or Year of Birth Gender: male [ ], female [
LAMA SHATAT TTP, ITP, DIC
 TTP, ITP, DIC Reduction in platelet number (thrombocytopenia) constitutes an important cause of generalized bleeding. A count less than 100,000 platelets/μl is generally considered to constitute thrombocytopenia.
TTP, ITP, DIC Reduction in platelet number (thrombocytopenia) constitutes an important cause of generalized bleeding. A count less than 100,000 platelets/μl is generally considered to constitute thrombocytopenia.
Evaluating for Suspected Child Abuse: Conditions That Predispose to Bleeding
 FROM THE AMERICAN ACADEMY OF PEDIATRICS TECHNICAL REPORT Evaluating for Suspected Child Abuse: Conditions That Predispose to Bleeding Shannon L. Carpenter, MD, MS, Thomas C. Abshire, MD, James D. Anderst,
FROM THE AMERICAN ACADEMY OF PEDIATRICS TECHNICAL REPORT Evaluating for Suspected Child Abuse: Conditions That Predispose to Bleeding Shannon L. Carpenter, MD, MS, Thomas C. Abshire, MD, James D. Anderst,
GUIDELINES. for the diagnosis and management of von Willebrand disease (VWD)
") GUIDELINES for the diagnosis and management of von Willebrand disease (VWD) The Canadian Hemophilia Society (CHS) is committed to improve the health and quality of life of all people with inherited bleeding
GUIDELINES for the diagnosis and management of von Willebrand disease (VWD) The Canadian Hemophilia Society (CHS) is committed to improve the health and quality of life of all people with inherited bleeding
Thrombocytopenia. Dr Lynda Vandertuin May 6, 2014
 Dr Lynda Vandertuin May 6, 2014 1 Presentation 1. Definition 2. Platelet Physiology, Thromboiesis, & Platelet Function 3. Bleeding Risk 4. Clinical Diagnosis 5. Differential Diagnosis 6. Classification
Dr Lynda Vandertuin May 6, 2014 1 Presentation 1. Definition 2. Platelet Physiology, Thromboiesis, & Platelet Function 3. Bleeding Risk 4. Clinical Diagnosis 5. Differential Diagnosis 6. Classification
Platelet Dysfunction- What a Physician
 Platelet Dysfunction- What a Physician Should Know 10 : 5 Mathew Thomas, Trivandrum Abstract Platelet functional disorders are on the increase. The basic platelet functions are a continuous process starting
Platelet Dysfunction- What a Physician Should Know 10 : 5 Mathew Thomas, Trivandrum Abstract Platelet functional disorders are on the increase. The basic platelet functions are a continuous process starting
Platelet disorders. Information for families. Great Ormond Street Hospital for Children NHS Foundation Trust
 Platelet disorders Information for families Great Ormond Street Hospital for Children NHS Foundation Trust Platelets are the cells responsible for making blood clot so platelet disorders mean that injured
Platelet disorders Information for families Great Ormond Street Hospital for Children NHS Foundation Trust Platelets are the cells responsible for making blood clot so platelet disorders mean that injured
Hemostasis Haemostasis means prevention of blood loss from blood vessels.
 ١ Hemostasis Haemostasis means prevention of blood loss from blood vessels. Bleeding is stopped by several mechanisms, which are: 1. Local vasoconstriction 2. Formation of platelet plug 3. Blood coagulation
١ Hemostasis Haemostasis means prevention of blood loss from blood vessels. Bleeding is stopped by several mechanisms, which are: 1. Local vasoconstriction 2. Formation of platelet plug 3. Blood coagulation
L iter diagnostico di laboratorio nelle coagulopatie congenite emorragiche
 L iter diagnostico di laboratorio nelle coagulopatie congenite emorragiche Armando Tripodi Angelo Bianchi Bonomi Hemophilia and Thrombosis Center Dept. of Clinical Sciences and Community Health University
L iter diagnostico di laboratorio nelle coagulopatie congenite emorragiche Armando Tripodi Angelo Bianchi Bonomi Hemophilia and Thrombosis Center Dept. of Clinical Sciences and Community Health University
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
HENOCH SCHÖNLEIN PURPURA (VASCULAR PURPURA, ANAPHYLACTOID PURPURA) IN CHILDREN Single choice tests (SC)
 IN CHILDREN Single choice tests (SC)") HENOCH HÖNLEIN PURPURA (VAULAR PURPURA, ANAPHYLACTOID PURPURA) IN CHILDREN Single choice tests () 1. Choose the type of bleeding characteristic for the Henoch Schönlein purpura (vascular purpura, anaphylactoid
HENOCH HÖNLEIN PURPURA (VAULAR PURPURA, ANAPHYLACTOID PURPURA) IN CHILDREN Single choice tests () 1. Choose the type of bleeding characteristic for the Henoch Schönlein purpura (vascular purpura, anaphylactoid
BLEEDING DISORDER IN CHILDREN
 BLEEDING DISORDER IN CHILDREN Platelets Coagulation factors Blood vessels integrity Blood is kept in a liquid form because the endothelium produce inhibitory factors to deactivate the platelets and coagulation
BLEEDING DISORDER IN CHILDREN Platelets Coagulation factors Blood vessels integrity Blood is kept in a liquid form because the endothelium produce inhibitory factors to deactivate the platelets and coagulation
Dental Management of Patients with Bleeding Disorders
 Dental Management of Patients with Bleeding Disorders Sandra D Amato-Palumbo, RDH, MPS Continuing Education Units: 3 hours Online Course: www.dentalcare.com/en-us/dental-education/continuing-education/ce319/ce319.aspx
Dental Management of Patients with Bleeding Disorders Sandra D Amato-Palumbo, RDH, MPS Continuing Education Units: 3 hours Online Course: www.dentalcare.com/en-us/dental-education/continuing-education/ce319/ce319.aspx
M B Garvey. University of Toronto
 Do I really need that test??? M B Garvey Professor Emeritus University of Toronto St Michael s Hospital No relevant conflicts of interest 1 HEMOSTASIS IS LIKE LOVE Everybody talks about it, nobody understands
Do I really need that test??? M B Garvey Professor Emeritus University of Toronto St Michael s Hospital No relevant conflicts of interest 1 HEMOSTASIS IS LIKE LOVE Everybody talks about it, nobody understands
Pediatric Coagulation Disorders
 Pediatric Coagulation Disorders Vilmarie Rodriguez, MD,* Deepti Warad, MBBS* *Division of Pediatric Hematology-Oncology, Mayo Clinic Children s Center, Mayo Clinic Comprehensive Hemophilia Center, Mayo
Pediatric Coagulation Disorders Vilmarie Rodriguez, MD,* Deepti Warad, MBBS* *Division of Pediatric Hematology-Oncology, Mayo Clinic Children s Center, Mayo Clinic Comprehensive Hemophilia Center, Mayo
Overview 5/8/2017. Management Strategies for Bleeding and Thrombocytopenia in the Neonate
 Management Strategies for Bleeding and Thrombocytopenia in the Neonate Kyle Annen, DO Medical Director Blood Bank, Transfusion Service and Hematology Mount Sinai Beth Israel Assistant Professor, Department
Management Strategies for Bleeding and Thrombocytopenia in the Neonate Kyle Annen, DO Medical Director Blood Bank, Transfusion Service and Hematology Mount Sinai Beth Israel Assistant Professor, Department
This slide belongs to iron lecture and it is to clarify the iron cycle in the body and the effect of hypoxia on erythropoitein secretion
 This slide belongs to iron lecture and it is to clarify the iron cycle in the body and the effect of hypoxia on erythropoitein secretion Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms
This slide belongs to iron lecture and it is to clarify the iron cycle in the body and the effect of hypoxia on erythropoitein secretion Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms
Dr. Apoorva Jayarangaiah MARSHFIELD CLINIC- Saint Joseph s Hospital
 Dr. Apoorva Jayarangaiah MARSHFIELD CLINIC- Saint Joseph s Hospital A 30 year old G1P0 female of Korean descent was referred by her OBGYN during her 2 nd trimester to the Hematology Clinic for evaluation
Dr. Apoorva Jayarangaiah MARSHFIELD CLINIC- Saint Joseph s Hospital A 30 year old G1P0 female of Korean descent was referred by her OBGYN during her 2 nd trimester to the Hematology Clinic for evaluation
HEMOSTASIS/THROMBOSIS II
 HEMOSTASIS/THROMBOSIS II Congenital/Acquired Hemorrhagic Disorders & Their Treatment COAGULATION TESTING!Bleeding time primary screening test for platelet function!if bleeding time abnormal!platelet Aggregation
HEMOSTASIS/THROMBOSIS II Congenital/Acquired Hemorrhagic Disorders & Their Treatment COAGULATION TESTING!Bleeding time primary screening test for platelet function!if bleeding time abnormal!platelet Aggregation
Document Title: Hemostasis: Platelet and Coagulation Disorders. Author(s): Joseph H. Hartmann (University of Michigan), DO 2012
: Joseph H. Hartmann (University of Michigan), DO 2012") Project: Ghana Emergency Medicine Collaborative Document Title: Hemostasis: Platelet and Coagulation Disorders Author(s): Joseph H. Hartmann (University of Michigan), DO 2012 License: Unless otherwise
Project: Ghana Emergency Medicine Collaborative Document Title: Hemostasis: Platelet and Coagulation Disorders Author(s): Joseph H. Hartmann (University of Michigan), DO 2012 License: Unless otherwise
Routine preoperative coagulation tests: are they necessary?
 Routine preoperative coagulation tests: are they necessary? Dr Azzah Alzahrani MD Pediatrics Hematology /Oncology PSMMS Outline Introduction. Brief review of hemostatic mechanisms. A clinical aspect of
Routine preoperative coagulation tests: are they necessary? Dr Azzah Alzahrani MD Pediatrics Hematology /Oncology PSMMS Outline Introduction. Brief review of hemostatic mechanisms. A clinical aspect of
Pediatric Bleeding Disorders and Thrombocytopenia. David Simon, MD Pediatric Hematology/Oncology Kaiser Permanente Downey Medical Center
 Pediatric Bleeding Disorders and Thrombocytopenia David Simon, MD Pediatric Hematology/Oncology Kaiser Permanente Downey Medical Center 1 2 Case Presentations Case 1 12 month old male, no personal or family
Pediatric Bleeding Disorders and Thrombocytopenia David Simon, MD Pediatric Hematology/Oncology Kaiser Permanente Downey Medical Center 1 2 Case Presentations Case 1 12 month old male, no personal or family
Hemostasis Haemostasis means prevention of blood loss from blood vessels.
 1 Hemostasis Haemostasis means prevention of blood loss from blood vessels. Bleeding is stopped by several mechanisms, which are: 1. Local vasoconstriction 2. Formation of platelet plug 3. Blood coagulation
1 Hemostasis Haemostasis means prevention of blood loss from blood vessels. Bleeding is stopped by several mechanisms, which are: 1. Local vasoconstriction 2. Formation of platelet plug 3. Blood coagulation
Moath Darweesh. Omar Sami. Saleem Khreisha. 1 P a g e
 7 Moath Darweesh Omar Sami Saleem Khreisha 1 P a g e -First of all, I want to give a quick revision to simplify the whole hemostasis mechanism, it will be much easier here with me. Enjoy (you can skip
7 Moath Darweesh Omar Sami Saleem Khreisha 1 P a g e -First of all, I want to give a quick revision to simplify the whole hemostasis mechanism, it will be much easier here with me. Enjoy (you can skip
Evaluation Of Bleeding Disorders /AAP Baton Rouge. Raj Warrier
 Evaluation Of Bleeding Disorders /AAP Baton Rouge Raj Warrier Evaluation and approach to management of a bleeding child Raj Warrier Ochsner /Tulane/LSU Manipal University University Of Queenland Objectives
Evaluation Of Bleeding Disorders /AAP Baton Rouge Raj Warrier Evaluation and approach to management of a bleeding child Raj Warrier Ochsner /Tulane/LSU Manipal University University Of Queenland Objectives
Clinical & Laboratory Assessment
 Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Rare Bleeding Disorders
 Rare Bleeding Disorders Item type Authors Publisher Other Irish Haemophilia Society (IHS) Irish Haemophilia Society (IHS) Downloaded 20-Jun-2018 06:21:18 Link to item http://hdl.handle.net/10147/575445
Rare Bleeding Disorders Item type Authors Publisher Other Irish Haemophilia Society (IHS) Irish Haemophilia Society (IHS) Downloaded 20-Jun-2018 06:21:18 Link to item http://hdl.handle.net/10147/575445
Case Studies: Congenital Platelet Disorders
 Case Studies: Congenital Platelet Disorders Presented to Atlanta Wednesday, November 2, 2016 Disclosures for Michele P. Lambert, MD, MTR In compliance with COI policy, ISTH requires the following disclosures
Case Studies: Congenital Platelet Disorders Presented to Atlanta Wednesday, November 2, 2016 Disclosures for Michele P. Lambert, MD, MTR In compliance with COI policy, ISTH requires the following disclosures
PCCN Review Hematology
 PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Topics of today lectures: Hemostasis
 Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms of hemostasis - Vascular contraction - Platelets plug - Blood coagulation (clotting) - Structure and functions of platelets - Blood
Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms of hemostasis - Vascular contraction - Platelets plug - Blood coagulation (clotting) - Structure and functions of platelets - Blood
It s a bird, It s a plane, No It s a. Presented by Julie Kirkegaard & Miche Swofford
 It s a bird, It s a plane, No It s a Presented by Julie Kirkegaard & Miche Swofford 55 year old woman admitted 11/23/2015 for colon cancer that metastasized to her liver History of 3 pregnancies Surgery
It s a bird, It s a plane, No It s a Presented by Julie Kirkegaard & Miche Swofford 55 year old woman admitted 11/23/2015 for colon cancer that metastasized to her liver History of 3 pregnancies Surgery
December Best Practice in Platelet Function Testing Stan McCormick, MD
 December 2012 Best Practice in Platelet Function Testing Stan McCormick, MD The indications for platelet function testing have expanded in recent years as improved testing technologies have become available
December 2012 Best Practice in Platelet Function Testing Stan McCormick, MD The indications for platelet function testing have expanded in recent years as improved testing technologies have become available
QUICK REFERENCE Clinical Practice Guideline on the Evaluation and Management of Immune Thrombocytopenia (ITP)
") QUICK REFERENCE 2011 Clinical Practice Guideline on the Evaluation and Management of Immune Thrombocytopenia (ITP) Presented by the American Society of Hematology, adapted from: The American Society of
QUICK REFERENCE 2011 Clinical Practice Guideline on the Evaluation and Management of Immune Thrombocytopenia (ITP) Presented by the American Society of Hematology, adapted from: The American Society of
Catherine P. M. Hayward, MD PhD FRCPC Professor, Pathology & Molecular Medicine, & Medicine, McMaster University Head, Coagulation, Hamilton Regional
 Catherine P. M. Hayward, MD PhD FRCPC Professor, Pathology & Molecular Medicine, & Medicine, McMaster University Head, Coagulation, Hamilton Regional Laboratory Medicine Program No relevant disclosures
Catherine P. M. Hayward, MD PhD FRCPC Professor, Pathology & Molecular Medicine, & Medicine, McMaster University Head, Coagulation, Hamilton Regional Laboratory Medicine Program No relevant disclosures
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13
 Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
WISKOTT-ALDRICH SYNDROME. An X-linked Primary Immunodeficiency
 WISKOTT-ALDRICH SYNDROME An X-linked Primary Immunodeficiency WHAT IS WISKOTT ALDRICH SYNDROME? Wiskott-Aldrich Syndrome (WAS) is a serious medical condition that causes problems both with the immune system
WISKOTT-ALDRICH SYNDROME An X-linked Primary Immunodeficiency WHAT IS WISKOTT ALDRICH SYNDROME? Wiskott-Aldrich Syndrome (WAS) is a serious medical condition that causes problems both with the immune system
Pediatric Bleeding Questionnaire (PBQ)
") Date Patient Number Patient Name Gender Male Female Age DOB (dd/mm/yy) Ethnic Background of: Father Mother Presenting complaint of bleeding or bruising today? Ever been diagnosed with a bleeding disorder?
Date Patient Number Patient Name Gender Male Female Age DOB (dd/mm/yy) Ethnic Background of: Father Mother Presenting complaint of bleeding or bruising today? Ever been diagnosed with a bleeding disorder?
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89
 Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Hemostasis. Learning objectives Dr. Mária Dux. Components: blood vessel wall thrombocytes (platelets) plasma proteins
 plasma proteins") Hemostasis Learning objectives 14-16 Dr. Mária Dux Components: blood vessel wall thrombocytes (platelets) plasma proteins Hemostatic balance! procoagulating activity anticoagulating activity 1 Thrombocytes
Hemostasis Learning objectives 14-16 Dr. Mária Dux Components: blood vessel wall thrombocytes (platelets) plasma proteins Hemostatic balance! procoagulating activity anticoagulating activity 1 Thrombocytes
, Malcolm Tait, Barry Frank Jacobson, Evashin Pillay and Susan J. Louw. Elizabeth Sarah Mayne *
 Mayne et al. Thrombosis Journal (2018) 16:30 https://doi.org/10.1186/s12959-018-0184-2 CASE REPORT Open Access Combination of acquired von Willebrand syndrome (AVWS) and Glanzmann thrombasthenia in monoclonal
Mayne et al. Thrombosis Journal (2018) 16:30 https://doi.org/10.1186/s12959-018-0184-2 CASE REPORT Open Access Combination of acquired von Willebrand syndrome (AVWS) and Glanzmann thrombasthenia in monoclonal
Chapter 19. Hemostasis
 Chapter 19 Hemostasis Hemostasis Hemostasis is the cessation of bleeding stopping potentially fatal leaks important in small blood vessels not effective in hemorrhage excessive bleeding from large blood
Chapter 19 Hemostasis Hemostasis Hemostasis is the cessation of bleeding stopping potentially fatal leaks important in small blood vessels not effective in hemorrhage excessive bleeding from large blood
Thrombocytopenia: a practial approach
 Thrombocytopenia: a practial approach Dr. med. Jeroen Goede FMH Innere Medizin, Medizinische Onkologie, Hämatologie FAMH Hämatologie Chefarzt Hämatologie Kantonsspital Winterthur Outline Introduction and
Thrombocytopenia: a practial approach Dr. med. Jeroen Goede FMH Innere Medizin, Medizinische Onkologie, Hämatologie FAMH Hämatologie Chefarzt Hämatologie Kantonsspital Winterthur Outline Introduction and