Asthma Pathophysiology and Treatment
|
|
|
- Caroline Stevenson
- 5 years ago
- Views:
Transcription

1 Asthma Pathophysiology and Treatment Bharat Prakash, MD Assistant Professor, Pulmonary and Critical Care Medicine Texas Tech University Health Sciences Center Transmountain Campus- El Paso
2 Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
3 Definition of Asthma The word asthma is derived from the ancient Greek word for panting The earliest feature described was the labored, rapid breathing typical of asthmatic attacks Measurement of maximal expiratory flow led to recognition of reversible airflow obstruction as a characteristic feature that is often reversible either spontaneously or with treatment
4 Definition of Asthma Chronic inflammatory disorder of the airways in which many cells and cellular elements play a role ( mast cells, eosinophils, T lymphocytes, macrophages, neutrophils and epithelial cells) In susceptible individuals, inflammation causes episodes of wheezing, breathlessness, chest tightness and coughing The inflammation also causes an increase in bronchial hyperresponsiveness to a variety of stimuli
5 Definition of Asthma National Institute of Health ( NIH) 1991: Chronic inflammatory disorder of the airways in which many cells and cellular elements are involved, with an associated increase in airway hyperresponsiveness that leads to recurrent wheezing, breathlessness, chest tightness and cough, particularly at night and early morning 2007: Updated guidelines emphasize the role of inflammation in Asthma and focus on evidence that the patterns and degrees of inflammation are variable, resulting in phenotypic differences that have important influences on response to therapy
6 Epidemiology of Asthma Prevalence of Asthma has been increasing worldwide over the past several decades Etiology is likely multifactorial Obesity exposure to allergens ( house dust mites, mold and tobacco smoke ) Atopy and allergic rhinitis ( exposure to allergens at an early age likely contribute to increased incidence of asthma )
7 Epidemiology of Asthma During the period from 1982 to 1992, the overall annual ageadjusted prevalence rate of self-reported asthma increased by 42 percent, from 34.7 to 49.4 per During the years 2001 through 2009, the age-adjusted prevalence of asthma increased from 73 to 82 per thousand Data from the CDC have shown that the prevalence of asthma increased in the United States from the early 1980s to the mid 1990s. During the years 2001 through 2009, the prevalence of asthma increased more gradually, and then remained stable in the years 2009 to 2012 with a decline in 2013
8 Epidemiology of Asthma The reasons for the plateau and potential decrease in prevalence of asthma in some countries remain unclear. It has been hypothesized that the rapidly changing exposures and lifestyles led to asthma developing in susceptible individuals in the latter half of the past century, but the proportion of the population that is susceptible to developing asthma is now reaching capacity
9 Epidemiology of Asthma There are important racial differences in the prevalence and morbidity of asthma National Health Interview Survey (NHIS)2011 Females had a higher prevalence rate than males Boys under 18 years old had a higher prevalence than girls

10 Epidemiology of Asthma Asthma related deaths steadily increased in the USA and world-wide between 1980 and the mid-1990s Although recent death rates have been declining asthma-related morbidity and mortality continue to be a significant problem World-wide approximately 180,000 deaths are attributable to asthma each year 4000 deaths/yr in the USA are attributed to asthma Moorman JE, Rudd RA, Johnson CA, et al. National surveillance for asthma-united States, MMWR Surveill Summ 2007; 56:1.
11 Epidemiology of Asthma Females had a 45% higher risk of dying from asthma than males Puerto Ricans were the most likely to die of asthma ( death rate 3.6 times higher than non-hispanics whites ) Non-hispanics blacks had an asthma death rate twice as high as non-hispanics whites
12 Risk Factors of Asthma Hygiene Hypothesis Infections Atopy Obesity Genetics Tobacco use and environmental exposure
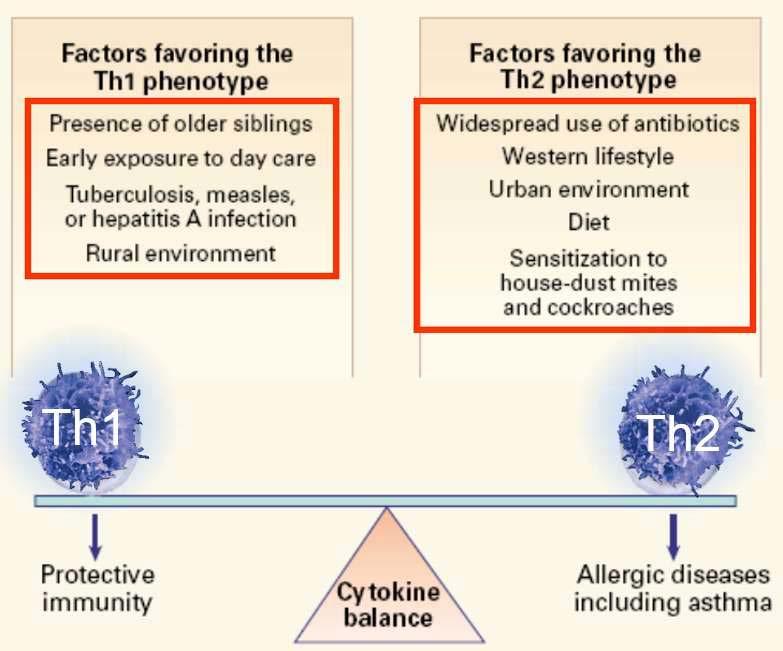
13 Risk Factors of Asthma Hygiene Hypothesis Infections early in life results in the development of a predominately T-helper (Th1)-mediated immune response and down regulation of the Th2-mediated response ( increased allergic rhinitis and atopy )
14
15 Risk Factors of Asthma Infections Exposure to microbes early in life may be protective The relationship between infections and development of atopy and asthma is complex and highly dependent on the type of infection RSV is the most common cause of bronchiolitis and is associated with an increase risk of developing subsequent asthma Rhinovirus is also a very important predictor of asthma if the infection occurs early in life
16 Risk Factors of Asthma Infections Atypical bacterial pathogens are implicated in triggering acute asthma and propagating chronic asthma Chlamydophylia pneumonia and mycoplasma pneumonia are present in the airways of chronic asthmatics
17 Risk Factors of Asthma Atopy Maternal or paternal atopy and the occurrence of asthma in children is controversial Several studies show that a family history of atopy is an important risk factor for atopy in children Obesity ( BMI > 30% ) Almost without exception more than 30 cross-sectional and casecontrol studies of the relationship between obesity and asthma since the 1990 s report an increase prevalence of asthma
18 Risk Factors of Asthma Genetics Advances in genomics have led to the discovery of several polymorphism that are important in the development of asthma and the response to therapy
19 Risk Factors of Asthma Tobacco use / environmental exposure There is increased evidence that both in utero and childhood exposure to tobacco results in detrimental effects on respiratory health ( increased risk of abnormal lung function and wheezing/ asthma in childhood ) Tobacco use is also associated with increase risk of developing asthma Environmental exposure in adults results in increased morbidity and poorer asthma control
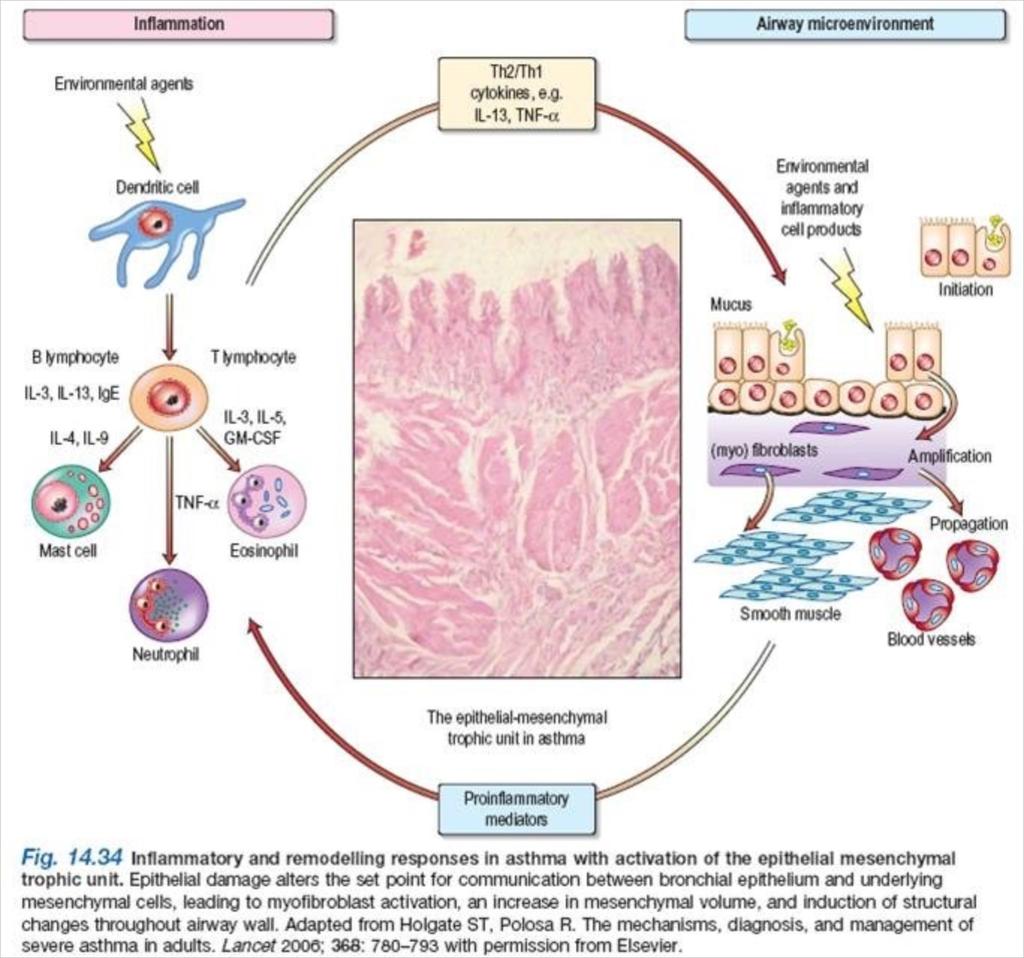
20 Pathophysiology of Asthma Inflammation is the cornerstone of the disease and is thought to result from inappropriate immune response to a variety of antigens in genetically susceptible individuals It involves many different cells ( e.g. neutrophils, basophils, eosinophils, mast cells, macrophages) and mediators ( e.g. cytokines, chemokines, histamine, leukotrienes and thromboxanes )
21
22 Pathophysiology of Asthma Airway remodeling is a pathologic feature of chronic asthma ( structural alteration of the airway with characteristics changes in the nature, content and distribution of airway elements ) The degree of airway remodeling is a function of disease severity over time
23
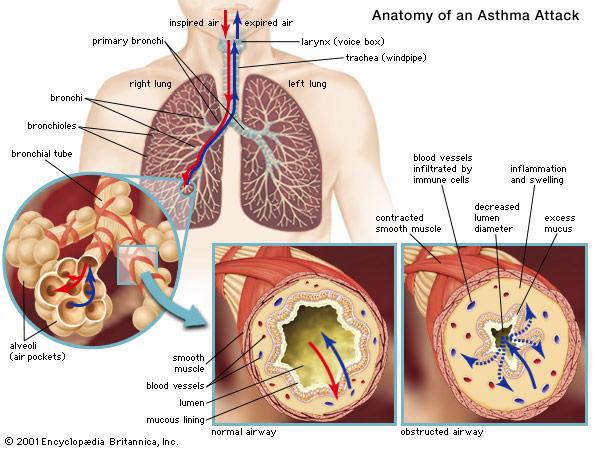
24 Physiology of Asthma During asthma exacerbation there is a diffuse narrowing of the airways thought to occur disproportionally in the small airways although recent studies suggest a prominent role for large and medium airways. As a result lung function test are abnormal, with an increase in airway resistance and a decline in maximal expiratory flow
25 Physiology of Asthma The work of breathing increases due to the decreased lung and chest wall compliance at higher thoracic lung volumes and greater effort required to overcome the resistance of the narrowed airways Acute severe asthma Arterial O2 tension (PaO2) < 70 mm Hg and arterial CO2 tension (PaCO2) initially falls as alveolar ventilation increases, follow up by normalization or elevated PaCO2 as muscle fatigue, a sign of impending respiratory failure
26 Physiology of Asthma Pulmonary Function Test: (PFT) PEF ( peak expiratory flow )measurement Spirometry Lung volumes Diffusing capacity Provocative Challenges and airway hyperresponsiveness test
27 Physiology of Asthma PEF ( peak expiratory flow) measurement recommended for daily monitoring of ambulatory patients and values should be compared to patient baseline measurement PEF % predicted is on average 10% higher than FEV1 with a great variability between measurements, greater predictive value for asthma exacerbations than the absolute PEF
28 Physiology of Asthma Spirometry: FEV1: The best and most standardized test of airflow obstruction Improvement in FEV1 > 12% and 200 ml after bronchodilator treatment indicate a reversible airflow obstruction and is suggestive, but not diagnostic of asthma Need to stop LABA x at least 12 hr and SABA x at least 6 hr
29 Physiology of Asthma Spirometry ( cont ): FEV1 may be normal between asthma flares FEV1/FVC ratio can be normal, unless patient is having a flare or patient has developed chronic airflow obstruction. FEF 25-75%, is not a well validated tool to diagnose or monitor asthma in adult population
30
31 Physiology of Asthma Lung volumes As a result of dynamic hyperinflation and consequent air trapping RV ( residual volume ), FRC ( functional residual capacity ) and TLC ( total lung capacity ) may be elevated Diffusing Capacity DLCO is a marker of CO gas transfer in the lungs and is reduced in most chronic lung disease In asthma DLCO is normal or elevated if airflow obstruction not severe
32 Physiology of Asthma Provocative Challenges/ Airway Hyperresponsiveness Patients suspected of having asthma despite normal lung function test usually develop bronchoconstriction in response to a provocative stimulus Nebulized Methacholine, delivered in doubling concentrations until FEV1 falls by more than 20%, ( PC20 < 16 mg/ml is consistent with mild AHR, <4 mg/ml moderate < 1 mg/ml severe )
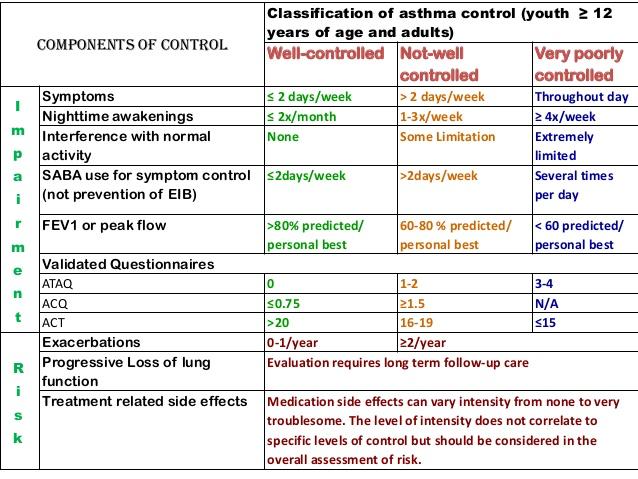
33 Management of Asthma Newer guidelines emphasize maintaining long-term control of symptoms through attention to environmental and social components of asthma and using treatments regimens tailored to the severity of each patient s symptoms Evaluation of severity Assessment of control Appropriate pharmacology therapy Identification and control of environmental factors that worsen symptoms or trigger exacerbations Creation of partnership between the patient and health care professional
34
35 Management of Asthma Pharmacologic therapy is subdivided into acute, short term reliever medications and chronic controller medications Therapy should be adjusted in a stepwise fashion to reduce daily symptoms and risk of exacerbations, while minimizing the use of medications Prominent role for controller medications
36 Management of Asthma Bronchodilators Inhaled Corticosteroids Leukotriene modifiers Phosphodiesterase 4 inhibitors ( Theophylline) Biologic agents Non pharmacologic therapy Additional management strategies
37 Management of Asthma Bronchodilators B2-Agonist: Short ( SABA ) and long acting (LABA ) agonist SABA should be used to treat symptoms not adequately controlled on a regimen of long acting agents Increase frequency of SABA use is a sign of inadequate control of symptoms or overreliance on rescue medication LABA can be added to an inhaled corticosteroid in patients with inadequately controlled asthma LABA s has been shown to improve lung function, reduce symptoms and reduce the frequency of exacerbations
38 Management of Asthma Bronchodilators B2-Agonist Adverse events include; tachycardia, arrhythmias, tremors and hypokalemia, lactic acidosis SMART trial, salmeterol multicenter asthma research trial, patient randomized to salmeterol or placebo plus usual care, there was no significant difference in risk of death in either group but subgroup analysis identified a small increase of death in African American subjects in the salmeterol arm
39 Management of Asthma Bronchodilators (cont) Anticholinergics Act as bronchodilators via competition with acetylcholine at neuromuscular junctions, blocking transmission of bronchoconstrictor reflexes Second line therapy however specific asthma phenotypes might be more likely to respond, including patients with fixed airway obstruction, advanced age or longer duration of disease Acceptable alternative for patients who do not tolerate B2-Agonist What is the role of tiotropium in asthma,chest 2015: non inferior to salmeterol and superior to placebo in patients with moderate to severe asthma who were not adequately controlled by ICS or ICS/salmeterol. Major benefit was an increase in lung function.
40 Management of Asthma Inhaled corticosteroids (ICS) Reduction in airway inflammation, for long term control of symptoms Centerpiece in any severity other than intermittent Compared to oral steroids, ICS minimize systemic toxicity Improves lung function Reduce asthma exacerbations Reduce hospitalizations Reduce risk of death
41 Management of Asthma Leukotriene modifiers ( LTM) LT have a modest bronchodilator effect and may improve asthma symptom and exacerbations rates Patients with aspirin-sensitive asthma may derive great benefit Data also suggest that LTM are adequate as single agents in mild persistent asthma Less efficacious than low dose ICS Primary role as adjuvant to ICS and its addition typically leads to a reduction in the corticosteroid dose or an improvement in asthma control Zileuton can cause hepatotoxicity, need to monitor LFTs
42 Management of Asthma Phosphodiesterase 4 Inhibitors ( Theophylline ) Mild anti-inflammatory properties Not longer a first line therapy due to its narrow therapeutic index Can be used in low dose as adjuvant treatment but has fallen out of favor: side effect profile and greater availability of other options Improves markers of control ( rescue inhalers use, lung function ) to a greater extent than LTMs. Side effects include anorexia, palpitations, dysrhythmias and seizure
43 Management of Asthma Biologic Agents Omalizumab: monoclonal antibody to Ig E Mepolizumab: Interleukin-5 Receptor Antagonist Reslizumab: Interleukin-5 Receptor Antagonist Benralizumab: Interleukin-5 Receptor Antagonist Dupulilumab: Interleukin-4 Receptor Antagonist
44 Anti IgE Therapy For patients with elevated IgE and sensitivity to perennial allergens Agent and target FDA-approved age Patient selection Route Dose Dosing interval Adverse effects For patients with elevated IgE and sensitivity to perennial allergens Omalizumab (anti-ige) 6 years IgE 30 to 700 IU/mL in United States; 30 to 1500 IU/mL in Europe SC Based on weight and IgE Doses 225 mg need to be divided over >1 injection site Maximal dose: 375 mg every 2 weeks in United States; 600 mg every 2 weeks in Europe 2 to 4 weeks depending on IgE level and body weight Local injection site reaction (severe 12%), usually within 1 hour Thromboembolic disease 3% Anaphylaxis, immediate or delayed <1% Antibody development (<1%)
45 Anti- Eosinophilic Agent and target FDA-approved age Patient selection Route Dose Dosing interval Adverse effects Mepolizumab (anti-il-5) Benralizumab (anti-il-5 receptor alpha) 12 years 12 years Peripheral blood eosinophils 150/microL Peripheral blood eosinophils 300/microL Dupilumab (anti-il-4 receptor subunit alpha) 12 years Peripheral blood eosinophils 150/microL Reslizumab (anti-il-5) 18 years Peripheral blood eosinophils 400/microL SC 100 mg 4 weeks SC SC Δ 30 mg First week, 2 doses of 200 mg (total 440 mg), then 200 mg every 2 weeks First week, 2 doses of 300 mg (total 600 mg), then 300 mg every 2 weeks 4 weeks for first 3 doses, then 8 weeks 2 weeks 2 weeks IV 3 mg/kg 4 weeks Headache (19%) Local injection site reaction (8 to 15%) Anaphylaxis: immediate or delayed <1% Human anti-human neutralizing antibody (<1%) Herpes zoster (<1%): Administration of zoster vaccine is suggested prior to initiation Human anti-human antibody development (13%; neutralizing 12%) Headache 8% Fever 3% Hypersensitivity (anaphylaxis, angioedema, urticaria) (3%): typically within hours of injection but can be delayed (3%) Human anti-human antibody development in patients receiving the 300 mg dose every 2 weeks for 52 weeks (6%; 2% neutralizing antibodies) and in patients taking 200 mg dose every 2 weeks for 52 weeks (9%; 4% neutralizing antibodies) Transient eosinophilia (4%); over 3000 cells/ml (1.2%) Anaphylaxis and other hypersensitivity reactions (<1%) Injection site reactions, conjunctivitis, keratitis, oral and other herpes simplex viral infections Human anti-human antibody development (5%) Anaphylaxis 0.3% during infusion or within 30 minutes after infusion; may occur as early as second dose or can be delayed Transient increase in creatine phosphokinase (20%)
46 Management of Asthma Non pharmacologic treatment Bronchial thermoplasty Thermal energy is delivered to the airway wall, resulting in reduction of airway smooth muscle mass ( characteristic feature of asthma ) Treatment leads to improvement in symptoms and quality of life and reduction in the use of rescue medication in patients with moderate or severe asthma Series of three bronchoscopies, exposing patients to the concomitant procedural risk and long term data outcome lacking though modality can work well in carefully selected patients.
47 Management of Asthma Additional management strategies Control of triggers Cigarette smoking decreases asthma control and reduces efficacy of corticosteroids Comorbid conditions, e.g. GERD and rhinosinusitis may worsen asthma symptoms and severity Reduction of allergen exposure ( most common dust mites and cat dander ) and provision of allergen immunotherapy

48
49 Key points Asthma is an important cause of disability, death and economic cost Asthma is increasing in developed countries Asthma is a disease of misdirected immunity, influenced by many genes and probably also by airway infections, especially viruses in the first few years of life The approach to the diagnosis, assessment and treatment of asthma has changed in response to the recognition of asthma as a chronic inflammatory disease punctuated by intermittent exacerbations
50 Key Points The therapies available are effective in controlling asthma, but their efficacy depends on fully engaging the patient More information is needed about the interplay between individuals genotypes and environmental stimuli that are responsible for the disease The combined use of anti-inflammatory and bronchodilators therapies, couple with measures to reduce environmental exposure can reduce the consequences and cost for the health care system
51 Thank you
Asthma Pathophysiology and Treatment. John R. Holcomb, M.D.
 Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Biologic Agents in the treatment of Severe Asthma
 Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
Clinical Implications of Asthma Phenotypes. Michael Schatz, MD, MS Department of Allergy
 Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Impact of Asthma in the U.S. per Year. Asthma Epidemiology and Pathophysiology. Risk Factors for Asthma. Childhood Asthma Costs of Asthma
 American Association for Respiratory Care Asthma Educator Certification Prep Course Asthma Epidemiology and Pathophysiology Robert C. Cohn, MD, FAARC MetroHealth Medical Center Cleveland, OH Impact of
American Association for Respiratory Care Asthma Educator Certification Prep Course Asthma Epidemiology and Pathophysiology Robert C. Cohn, MD, FAARC MetroHealth Medical Center Cleveland, OH Impact of
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ
 Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al.
 Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network
 Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma in Day to Day Practice
 Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Air Flow Limitation. In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation.
 Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Medicine Dr. Kawa Lecture 1 Asthma Obstructive & Restrictive Pulmonary Diseases Obstructive Pulmonary Disease Indicate obstruction to flow of air
 Medicine Dr. Kawa Lecture 1 Asthma Obstructive & Restrictive Pulmonary Diseases Obstructive Pulmonary Disease Indicate obstruction to flow of air through the airways. As asthma, COPD ( chronic bronchitis
Medicine Dr. Kawa Lecture 1 Asthma Obstructive & Restrictive Pulmonary Diseases Obstructive Pulmonary Disease Indicate obstruction to flow of air through the airways. As asthma, COPD ( chronic bronchitis
Treatment Options for Complicated/Severe Asthma. Henry J. Kanarek, MD Kanarek Allergy Asthma Immunology
 Treatment Options for Complicated/Severe Asthma Henry J. Kanarek, MD Kanarek Allergy Asthma Immunology www.kallergy.com 913-451-8555 Asthma Epidemiology World Health Organization, Asthma is one of the
Treatment Options for Complicated/Severe Asthma Henry J. Kanarek, MD Kanarek Allergy Asthma Immunology www.kallergy.com 913-451-8555 Asthma Epidemiology World Health Organization, Asthma is one of the
Asthma and Vocal Cord Dysfunction
 Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Asthma 2015: Establishing and Maintaining Control
 Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Significance. Asthma Definition. Focus on Asthma
 Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Speaker Disclosure. Identification and Diagnosis of Asthma. Definition of Asthma. Objectives 11/9/2017
 Speaker Disclosure Identification and Diagnosis of Asthma Isabel L. Virella Lowell, MD, Associate Professor, Pulmonology and Sleep Medicine, University of Alabama at Birmingham Isabel Virella-Lowell, MD
Speaker Disclosure Identification and Diagnosis of Asthma Isabel L. Virella Lowell, MD, Associate Professor, Pulmonology and Sleep Medicine, University of Alabama at Birmingham Isabel Virella-Lowell, MD
Asthma in Pediatric Patients. DanThuy Dao, D.O., FAAP. Disclosures. None
 Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
What is Asthma? Chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Night time or early morning coughing
 Asthma What is Asthma? Chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Night time or early morning coughing Episodes are usually associated with widespread, but
Asthma What is Asthma? Chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Night time or early morning coughing Episodes are usually associated with widespread, but
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Asthma. Rachel Miller, MD, FAAAAI Director Allergy and Immunology New York Presbyterian Hospital. Figure 1 Asthma Prevalence,
 Asthma Rachel Miller, MD, FAAAAI Director Allergy and Immunology New York Presbyterian Hospital Figure 1 Asthma Prevalence, 1980-2000 * Gap between 1995-1996 and 1997 indicates a break in trend due to
Asthma Rachel Miller, MD, FAAAAI Director Allergy and Immunology New York Presbyterian Hospital Figure 1 Asthma Prevalence, 1980-2000 * Gap between 1995-1996 and 1997 indicates a break in trend due to
Pathology of Asthma Epidemiology
 Asthma A Presentation on Asthma Management and Prevention What Is Asthma? A chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Nighttime or early morning coughing Pathology
Asthma A Presentation on Asthma Management and Prevention What Is Asthma? A chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Nighttime or early morning coughing Pathology
Diagnosis, Treatment and Management of Asthma
 Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Asthma in the college health setting: diagnosis, treatment, pitfalls
 Asthma in the college health setting: diagnosis, treatment, pitfalls A 20-year-old college student with a history of asthma and allergic rhinitis, which were diagnosed in childhood, presents with cough
Asthma in the college health setting: diagnosis, treatment, pitfalls A 20-year-old college student with a history of asthma and allergic rhinitis, which were diagnosed in childhood, presents with cough
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Asthma in the Athlete
 Asthma in the Athlete Jorge E. Gomez, MD Associate Professor Texas Children s Hospital Baylor College of Medicine Assist Team Physician UH Understand how we diagnose asthma Objectives Be familiar with
Asthma in the Athlete Jorge E. Gomez, MD Associate Professor Texas Children s Hospital Baylor College of Medicine Assist Team Physician UH Understand how we diagnose asthma Objectives Be familiar with
Bronchial asthma. MUDr. Mojmír Račanský Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL
 Bronchial asthma MUDr. Mojmír Račanský Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL DEFINITION ASTHMA BRONCHIALE = Asthma is a chronic inflammatory disorder of the airways in which
Bronchial asthma MUDr. Mojmír Račanský Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL DEFINITION ASTHMA BRONCHIALE = Asthma is a chronic inflammatory disorder of the airways in which
Meeting the Challenges of Asthma
 Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
COPD and Asthma Update. April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute
 COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
Do We Need Biologics in Pediatric Asthma Management?
 Do We Need Biologics in Pediatric Asthma Management? Ting Fan LEUNG, MBChB, MD, FRCPCH, FAAAAI Professor and Chairman Department of Paediatrics The Chinese University of Hong Kong Asthma and Allergy by
Do We Need Biologics in Pediatric Asthma Management? Ting Fan LEUNG, MBChB, MD, FRCPCH, FAAAAI Professor and Chairman Department of Paediatrics The Chinese University of Hong Kong Asthma and Allergy by
1. What is delayed sequence intubation? Can it be used for severe Asthma exacerbation? 2. What about pregnancy and Asthma is so important?
 Chapter 073 Asthma Episode Overview 1. 10 different causes of a wheeze. 2. List 8 risk factors for death from asthma 3. List 6 objective findings of severe asthma 4. 10 therapies for an acute severe asthma
Chapter 073 Asthma Episode Overview 1. 10 different causes of a wheeze. 2. List 8 risk factors for death from asthma 3. List 6 objective findings of severe asthma 4. 10 therapies for an acute severe asthma
Emily DiMango, MD Asthma II
 Emily DiMango, MD Asthma II Director John Edsall/John Wood Asthma Center Columbia University Medical Center HP 2000 Goal: 2.25/1,000 Comparison of Asthma Hospitalization Rates in Children Aged 0-14 in
Emily DiMango, MD Asthma II Director John Edsall/John Wood Asthma Center Columbia University Medical Center HP 2000 Goal: 2.25/1,000 Comparison of Asthma Hospitalization Rates in Children Aged 0-14 in
Systems Pharmacology Respiratory Pharmacology. Lecture series : General outline
 Systems Pharmacology 3320 2017 Respiratory Pharmacology Associate Professor Peter Henry (Rm 1.34) Peter.Henry@uwa.edu.au Division of Pharmacology, School of Biomedical Sciences Lecture series : General
Systems Pharmacology 3320 2017 Respiratory Pharmacology Associate Professor Peter Henry (Rm 1.34) Peter.Henry@uwa.edu.au Division of Pharmacology, School of Biomedical Sciences Lecture series : General
COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013
 COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013 None Disclosures Definitions Asthma Asthma is a chronic inflammatory
COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013 None Disclosures Definitions Asthma Asthma is a chronic inflammatory
7/7/2015. Somboon Chansakulporn, MD. History of variable respiratory symptoms. 1. Documented excessive variability in PFT ( 1 test)
") Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
Exercise-Induced Bronchospasm. Michael A Lucia, MD, FCCP Asst Clinical Professor, UNR School of Medicine Sierra Pulmonary & Sleep Institute
 Exercise-Induced Bronchospasm Michael A Lucia, MD, FCCP Asst Clinical Professor, UNR School of Medicine Sierra Pulmonary & Sleep Institute EIB Episodic bronchoconstriction with exercise May be an exacerbation
Exercise-Induced Bronchospasm Michael A Lucia, MD, FCCP Asst Clinical Professor, UNR School of Medicine Sierra Pulmonary & Sleep Institute EIB Episodic bronchoconstriction with exercise May be an exacerbation
Life-long asthma and its relationship to COPD. Stephen T Holgate School of Medicine University of Southampton
 Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Improving Outcomes in the Management & Treatment of Asthma. April 21, Spring Managed Care Forum
 Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Respiratory Pharmacology
 Allergy Targets of allergies Type I Histamine Leukotrienes Prostaglandins Bradykinin Hypersensitivity reactions Asthma Characterised by Triggered by Intrinsic Extrinsic (allergic) Mediators Result Early
Allergy Targets of allergies Type I Histamine Leukotrienes Prostaglandins Bradykinin Hypersensitivity reactions Asthma Characterised by Triggered by Intrinsic Extrinsic (allergic) Mediators Result Early
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016
 Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Asthma Description. Asthma is a disease that affects the lungs defined as a chronic inflammatory disorder of the airways.
 Asthma Asthma Description Asthma is a disease that affects the lungs defined as a chronic inflammatory disorder of the airways. Symptoms of asthma In susceptible individuals, this inflammation causes recurrent
Asthma Asthma Description Asthma is a disease that affects the lungs defined as a chronic inflammatory disorder of the airways. Symptoms of asthma In susceptible individuals, this inflammation causes recurrent
Omalizumab (Xolair ) ( Genentech, Inc., Novartis Pharmaceuticals Corp.) September Indication
 ( Genentech, Inc., Novartis Pharmaceuticals Corp.) September Indication") ( Genentech, Inc., Novartis Pharmaceuticals Corp.) September 2003 Indication The FDA recently approved Omalizumab on June 20, 2003 for adults and adolescents (12 years of age and above) with moderate to
( Genentech, Inc., Novartis Pharmaceuticals Corp.) September 2003 Indication The FDA recently approved Omalizumab on June 20, 2003 for adults and adolescents (12 years of age and above) with moderate to
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Asthma. chapter 7. Overview
 chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
Asthma Update I have no professional or personal financial conflicts of interest to disclose.
 Asthma Update 2018 Disclosures Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center I have
Asthma Update 2018 Disclosures Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center I have
Asthma Update Jennifer W. McCallister, MD, FACP, FCCP
 Asthma Update 2018 Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center Disclosures I have
Asthma Update 2018 Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center Disclosures I have
Asthma for Primary Care: Assessment, Control, and Long-Term Management
 Asthma for Primary Care: Assessment, Control, and Long-Term Management Learning Objectives After participating in this educational activity, participants should be better able to: 1. Choose the optimal
Asthma for Primary Care: Assessment, Control, and Long-Term Management Learning Objectives After participating in this educational activity, participants should be better able to: 1. Choose the optimal
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL
 DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
COPD and Asthma: Similarities and differences Prof. Peter Barnes
 and Asthma: Similarities and Differences and Asthma: 1 Imperial College Peter Barnes FRS, FMedSci, National Heart & Lung Institute Imperial College, London, UK p.j.barnes@imperial.ac.uk Royal Brompton
and Asthma: Similarities and Differences and Asthma: 1 Imperial College Peter Barnes FRS, FMedSci, National Heart & Lung Institute Imperial College, London, UK p.j.barnes@imperial.ac.uk Royal Brompton
Global Initiative for Asthma (GINA) What s new in GINA 2016?
 What s new in GINA 2016?") Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Cynthia S. Kelly, M.D. Professor of Pediatrics Eastern Virginia Medical School Division Director Allergy Children s Hospital of The King s Daughters
 Cynthia S. Kelly, M.D. Professor of Pediatrics Eastern Virginia Medical School Division Director Allergy Children s Hospital of The King s Daughters Disclosures Speakers bureau of Novartis and Genentech
Cynthia S. Kelly, M.D. Professor of Pediatrics Eastern Virginia Medical School Division Director Allergy Children s Hospital of The King s Daughters Disclosures Speakers bureau of Novartis and Genentech
Asthma: Chronic Management. Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015
 Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
New Therapies for Asthma
 New Therapies for Asthma Tracy Bridges, MD Speaker Disclosure: Dr. Bridges participates in speaker bureaus for Teva, Genetech & Astra Zeneca. Objectives: Discuss the use of LAMA s for Asthma Detail the
New Therapies for Asthma Tracy Bridges, MD Speaker Disclosure: Dr. Bridges participates in speaker bureaus for Teva, Genetech & Astra Zeneca. Objectives: Discuss the use of LAMA s for Asthma Detail the
Connecting Health & Housing: Asthma and the Home. Presented by: The California-Nevada Public Health Training Center
 Connecting Health & Housing: Asthma and the Home Presented by: The California-Nevada Public Health Training Center Funded by Grant #UB6HP20202 from the Health Resources and Services Administration, U.S.
Connecting Health & Housing: Asthma and the Home Presented by: The California-Nevada Public Health Training Center Funded by Grant #UB6HP20202 from the Health Resources and Services Administration, U.S.
Defining COPD. Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist
 Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Searching for Targets to Control Asthma
 Searching for Targets to Control Asthma Timothy Craig Distinguished Educator Professor Medicine and Pediatrics Penn State University Hershey, PA, USA Inflammation and Remodeling in Asthma The most important
Searching for Targets to Control Asthma Timothy Craig Distinguished Educator Professor Medicine and Pediatrics Penn State University Hershey, PA, USA Inflammation and Remodeling in Asthma The most important
Asthma in Pregnancy. Asthma. Chronic Airway Inflammation. Objective Measures of Airflow. Peak exp. flow rate (PEFR)
") Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
The Asthma Guidelines: Diagnosis and Assessment of Asthma
 The Asthma Guidelines: Diagnosis and Assessment of Asthma Christopher H. Fanta, M.D. Partners Asthma Center Brigham and Women s Hospital Harvard Medical School Objectives Know how the diagnosis of asthma
The Asthma Guidelines: Diagnosis and Assessment of Asthma Christopher H. Fanta, M.D. Partners Asthma Center Brigham and Women s Hospital Harvard Medical School Objectives Know how the diagnosis of asthma
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
Asma e BPCO: le strategie terapeutiche
 Asma e BPCO: le strategie terapeutiche Dott. Marco Contoli ctm@unife.it Sezione di Medicina Interna e Cardio-Respiratoria Dipartimento di Scienze Mediche Università di Ferrara COPD Definition Chronic Obstructive
Asma e BPCO: le strategie terapeutiche Dott. Marco Contoli ctm@unife.it Sezione di Medicina Interna e Cardio-Respiratoria Dipartimento di Scienze Mediche Università di Ferrara COPD Definition Chronic Obstructive
Improving the Management of Asthma to Improve Patient Adherence and Outcomes
 Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Is reslizumab effective in improving quality of life and asthma control in adolescent and adult patients with poorly controlled eosinophilic asthma?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2018 Is reslizumab effective in improving
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2018 Is reslizumab effective in improving
Clinical Practice Guideline: Asthma
 Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline
 Pathology of Asthma Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline Bronchial Asthma Definition: chronic, relapsing inflammatory lung disorder characterised by reversible
Pathology of Asthma Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline Bronchial Asthma Definition: chronic, relapsing inflammatory lung disorder characterised by reversible
Function of the Respiratory System. Exchange CO2 (on expiration) for O2 (on inspiration)
 for O2 (on inspiration)") Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION
 Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD
 Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
THE NHLBI GUIDELINES: WHERE DO WE STAND AND WHAT IS THE NEW DIRECTION FROM THE NAEPP?
 THE NHLBI GUIDELINES: WHERE DO WE STAND AND WHAT IS THE NEW DIRECTION FROM THE NAEPP? Peter S. Creticos, MD ABSTRACT In 1991 and 1997, the National Heart, Lung, and Blood Institute s National Asthma Education
THE NHLBI GUIDELINES: WHERE DO WE STAND AND WHAT IS THE NEW DIRECTION FROM THE NAEPP? Peter S. Creticos, MD ABSTRACT In 1991 and 1997, the National Heart, Lung, and Blood Institute s National Asthma Education
Bronchial Provocation Results: What Does It Mean?
 Bronchial Provocation Results: What Does It Mean? Greg King 1 Department of Respiratory Medicine, Royal North Shore Hospital, St Leonards 2065 2 Woolcock Institute of Medical Research and Sydney Medical
Bronchial Provocation Results: What Does It Mean? Greg King 1 Department of Respiratory Medicine, Royal North Shore Hospital, St Leonards 2065 2 Woolcock Institute of Medical Research and Sydney Medical
I have no perceived conflicts of interest or commercial relationships to disclose.
 ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
Joint Session ACOFP and AOASM: Exercise Induced Asthma. Bruce Dubin, DO, JD, FCLM, FACOI
 Joint Session ACOFP and AOASM: Exercise Induced Asthma Bruce Dubin, DO, JD, FCLM, FACOI ACOFP FULL DISCLOSURE FOR CME ACTIVITIES Please check where applicable and sign below. Provide additional pages as
Joint Session ACOFP and AOASM: Exercise Induced Asthma Bruce Dubin, DO, JD, FCLM, FACOI ACOFP FULL DISCLOSURE FOR CME ACTIVITIES Please check where applicable and sign below. Provide additional pages as
PFT s / 2017 Pulmonary Update. Eric S. Papierniak, DO University of Florida NF/SG VHA
 PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER
 MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
The Acute & Maintenance Treatment of Asthma via Aerosolized Medications
 The Acute & Maintenance Treatment of Asthma via Aerosolized Medications Douglas S. Gardenhire, EdD, RRT-NPS, FAARC Associate Professor and Chairman Department of Respiratory Therapy Objectives Define Asthma.
The Acute & Maintenance Treatment of Asthma via Aerosolized Medications Douglas S. Gardenhire, EdD, RRT-NPS, FAARC Associate Professor and Chairman Department of Respiratory Therapy Objectives Define Asthma.
HealthPartners Care Coordination Clinical Care Planning and Resource Guide ASTHMA
 The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
Bronchial asthma. E. Cserháti 1 st Department of Paediatrics. Lecture for english speaking students 5 February 2013
 Bronchial asthma E. Cserháti 1 st Department of Paediatrics Lecture for english speaking students 5 February 2013 Epidemiology of childhood bronchial asthma Worldwide prevalence of 7-8 and 13-14 years
Bronchial asthma E. Cserháti 1 st Department of Paediatrics Lecture for english speaking students 5 February 2013 Epidemiology of childhood bronchial asthma Worldwide prevalence of 7-8 and 13-14 years
Asthma ASTHMA. Current Strategies for Asthma and COPD
 Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
THE PROMISE OF NEW AND NOVEL DRUGS. Pyng Lee Respiratory & Critical Care Medicine National University Hospital
 THE PROMISE OF NEW AND NOVEL DRUGS Pyng Lee Respiratory & Critical Care Medicine National University Hospital Pyng_lee@nuhs.edu.sg Asthma Prevalence, Morbidity, Mortality 235 million suffer from asthma
THE PROMISE OF NEW AND NOVEL DRUGS Pyng Lee Respiratory & Critical Care Medicine National University Hospital Pyng_lee@nuhs.edu.sg Asthma Prevalence, Morbidity, Mortality 235 million suffer from asthma
Current Asthma Management: Opportunities for a Nutrition-Based Intervention
 Current Asthma Management: Opportunities for a Nutrition-Based Intervention Stanley J. Szefler, MD Approximately 22 million Americans, including 6 million children, have asthma. It is one of the most prevalent
Current Asthma Management: Opportunities for a Nutrition-Based Intervention Stanley J. Szefler, MD Approximately 22 million Americans, including 6 million children, have asthma. It is one of the most prevalent
Using Patient Characteristics to Individualize and Improve Asthma Care
 Using Patient Characteristics to Individualize and Improve Asthma Care Leonard B. Bacharier, M.D. Associate Professor of Pediatrics Clinical Director, Division of Allergy, Immunology, & Pulmonary Medicine
Using Patient Characteristics to Individualize and Improve Asthma Care Leonard B. Bacharier, M.D. Associate Professor of Pediatrics Clinical Director, Division of Allergy, Immunology, & Pulmonary Medicine
Asthma Upate 2018: What s New Since the 2007 Asthma Guidelines of NAEPP?
 10:50-11:50am Asthma Update 2018: What s New Since the 2007 National Asthma Guidelines? SPEAKER Christopher H. Fanta, MD Disclosures The following relationships exist related to this presentation: Christopher
10:50-11:50am Asthma Update 2018: What s New Since the 2007 National Asthma Guidelines? SPEAKER Christopher H. Fanta, MD Disclosures The following relationships exist related to this presentation: Christopher
Known Allergies: Shellfish. Symptoms: abdominal pain, nausea, diarrhea, or vomiting. congestion, trouble breathing, or wheezing.
 CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
The Link Between Viruses and Asthma
 The Link Between Viruses and Asthma CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep Disorders Center SUNY Stony
The Link Between Viruses and Asthma CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep Disorders Center SUNY Stony
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN. Dr Lại Lê Hưng Respiratory Department
 TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN Dr Lại Lê Hưng Respiratory Department Literature review current through: Feb 2013. This topic last updated: Aug 14, 2012 INTRODUCTION Wheezing
TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN Dr Lại Lê Hưng Respiratory Department Literature review current through: Feb 2013. This topic last updated: Aug 14, 2012 INTRODUCTION Wheezing
2010 Health Press Ltd.
 Fast Facts Fast Facts: Asthma Third edition Stephen T Holgate MD DSc FRCP FMedSci MRC Clinical Professor of Immunopharmacology School of Medicine Southampton General Hospital Southampton, UK Jo Douglass
Fast Facts Fast Facts: Asthma Third edition Stephen T Holgate MD DSc FRCP FMedSci MRC Clinical Professor of Immunopharmacology School of Medicine Southampton General Hospital Southampton, UK Jo Douglass
Difficult Asthma Assessment: A systematic approach
 Difficult Asthma Assessment: A systematic approach Dr Naghmeh Radhakrishna Respiratory, Sleep & Allergy Physician Allergy, Asthma & Clinical Immunology Service The Alfred Hospital Melbourne, Australia
Difficult Asthma Assessment: A systematic approach Dr Naghmeh Radhakrishna Respiratory, Sleep & Allergy Physician Allergy, Asthma & Clinical Immunology Service The Alfred Hospital Melbourne, Australia
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss