Non Cystic Fibrosis Bronchiectasis: How to Proceed?
|
|
|
- William Boyd
- 5 years ago
- Views:
Transcription
, European Diplomate of Pediatric Respiratory")
 Consultant Pediatric Pulmonologist BLK Super Specialty Hospital Formerly")
1 Non Cystic Fibrosis Bronchiectasis: How to Proceed? Dr Ankit Parakh MD, DNB, MNAMS, RCPCH Fellow (UK), European Diplomate of Pediatric Respiratory Medicine ERS Fellowship Pediatric Medicine & NIV (GOSH, London, UK) APSR fellowship Sleep Medicine (Brisbane, Australia) Consultant Pediatric Pulmonologist BLK Super Specialty Hospital Formerly Assistant Professor Kalawati Saran Children s Hospital
2 Plan of the Talk.. Clarifying the terms: Wet cough, protracted bacterial bronchitis, suppurative lung disease, bronchiectasis When to investigate? Etiology Diagnosis: Imaging Specific Investigations for etiological diagnosis Treatment

3 What Is Wet Cough? Even when airway secretions are present, young children rarely expectorate sputum. Hence wet/moist cough is the preferable term rather than productive cough. Pediatr Pulmonol. 2008; 43:

4 Definitions Protracted Bacterial Bronchitis History of isolated chronic moist cough with no specific cough pointers beyond 3-4 weeks AND Response to antibiotic treatment with resolution of the cough within 2 weeks Chronic suppurative lung disease Persistent chronic wet cough >6 months but without confirmatory c-hrct findings. Bronchiectasis Persistent or progressive condition characterized by dilated thick-walled irreversibly damaged bronchi.
5
6 Which children should be investigated for bronchiectasis/csld? Chronic productive or moist cough every day for >8 weeks or less than <8 weeks but worsening British Thoracic Society guideline for non-cf bronchiectasis. Thorax Jul;65 Suppl 1:i1-58.
7 Which children should be investigated for bronchiectasis? Symptoms attributed to asthma that are atypical or which respond poorly to conventional treatment Cough variant asthma Localised chronic bronchial obstruction. Long standing foreign body British Thoracic Society guideline for non-cf bronchiectasis. Thorax Jul;65 Suppl 1:i1-58.
8 Which children should be investigated for Post severe pneumonia bronchiectasis? Incomplete resolution of symptoms, physical signs or radiological changes. Recurrent pneumonia Persistent and unexplained physical signs or chest radiographic abnormalities. British Thoracic Society guideline for non-cf bronchiectasis. Thorax Jul;65 Suppl 1:i1-58.
9 Which children should be investigated for bronchiectasis? Respiratory symptoms with any clinical features of CF, PCD or immunodeficiency. British Thoracic Society guideline for non-cf bronchiectasis. Thorax Jul;65 Suppl 1:i1-58.
10 Etiology of Bronchiectasis in Children POST Infections Muco-Ciliary Disorders Immuno-Deficiency Causes Severe Necrotizing Pneumonia Viral pneumonia (measles, adenovirus), Post-pertussis Post Tubercular Cystic Fibrosis Primary Ciliary Dyskinesia HIV XLA, CVID Hyper IgM Job s Syndrome Important Clinical Findings Allergic/Fungal Allergic Bronchopulmonary Aspergillosis Past Asthma/CF Temporal relationship of identified infections to the onset of chronic respiratory symptoms Stool issues/ftt Chronic Upper airway symptoms (Rhinorrhea, otitis) Serious, persistent or recurrent infections, particularly involving multiple sites, or infections with opportunist organisms Other/Rare Congenital disorders, Alpha-one Antitrypsin def, Ataxia-Telengectasia


11 Etiology of Bronchiectasis in Children Kapur N. Paediatr Respir Rev Jun;12(2):91-6.
12 Diagnosis and Investigations To prove the diagnosis of CSLD: Chest Xray HRCT Chest To prove the etiology of CSLD: Specific Investigations: sweat test, PCD studies, Immunological tests etc To evaluate the airway microbiology: Sputum/Bronchoscopy BAL To evaluate disease extent/progression: Lung Function/follow up Radiology




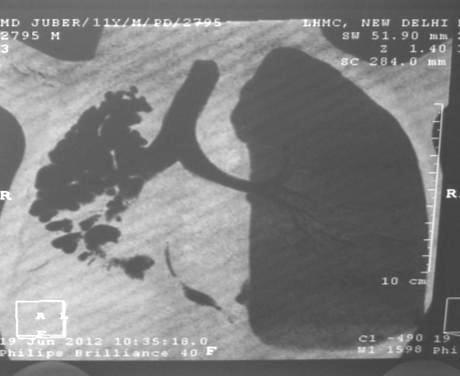
13 Imaging of diseases of chest Hansell 5 th ed Plugged & thickened centrilobular bronchioles ( treein-bud sign) Nontapering or flaring of bronchi Crowding of bronchi with associated volume loss Areas of decreased attenuation reflecting small airways obliteration Signet Ring Sign Mucus-filled dilated bronchi ( flame and blob sign); Large Airways 25

14 Signet Sign Dilated bronchus Bronchial artery 40
15 Etiology of Bronchiectasis in Children POST Infections Muco-Ciliary Disorders Immuno-Deficiency Causes Severe Necrotizing Pneumonia Viral pneumonia (measles, adenovirus), Post-pertussis Post TB Cystic Fibrosis Primary Ciliary Dyskinesia HIV XLA, CVID Hyper IgM Job s Syndrome Radiological Pointers Usually in location of Pneumonia or Tuberculosis Can be more diffuse with viral Pan Bronchiectasis Sinusitis Small airway disease Non-Specific Can involve one or all lobes Allergic/Fungal Allergic Bronchopulmonary Aspergillosis Central Bronchiectasis, Bronchoceles, HAM, Tree-in-bud
16 Investigations Etiology POST Infections Muco-Ciliary Disorders Immuno-Deficiency Causes Severe Necrotizing Pneuminia Viral pneumonia (measles, adenovirus), Post-pertussis Post TB Cystic Fibrosis Primary Ciliary Dyskinesia HIV XLA, CVID Hyper IgM Job s Syndrome Investigations History and temporal relation Sweat Test, Genetics VideoMicroscopy, EM, Genetics HIV Testing Ig Profile CD3, CD4, CD8, CD19 etc Allergic/Fungal Allergic Bronchopulmonary Aspergillosis Serum IgE Aspergillus Specific IgE/IgG Radiological Findings Other/Rare
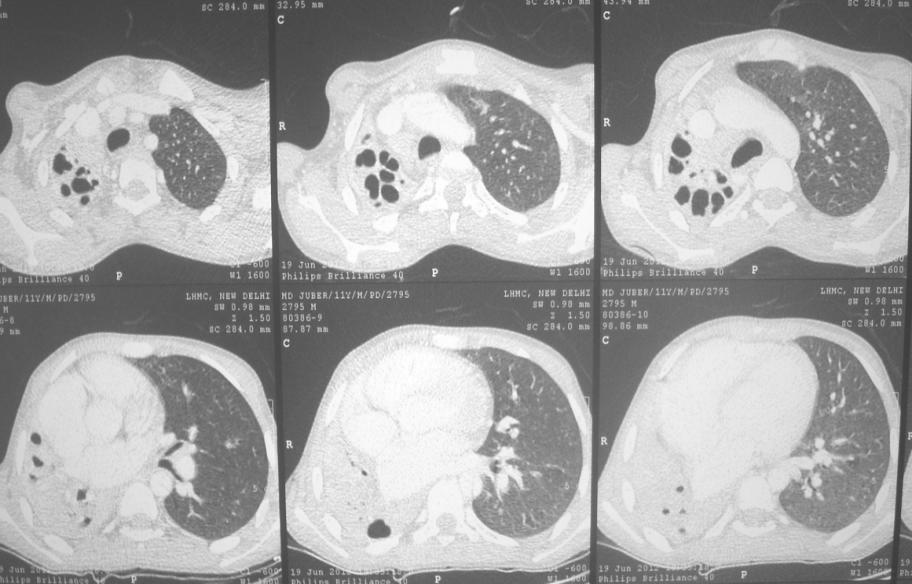
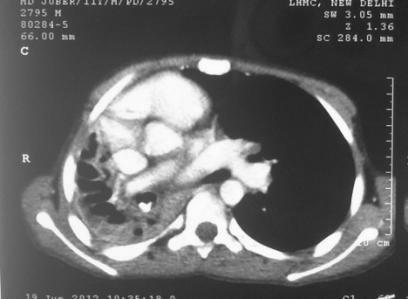
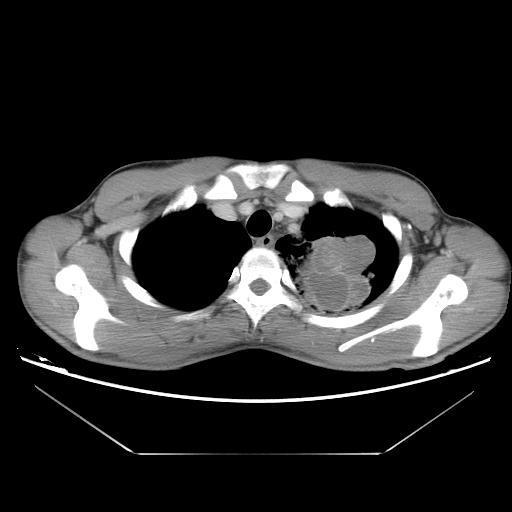
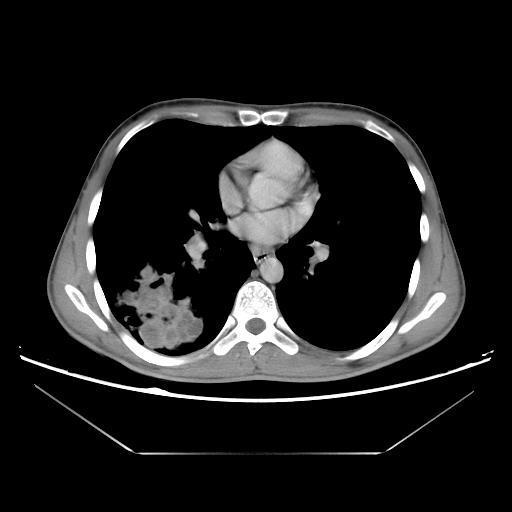
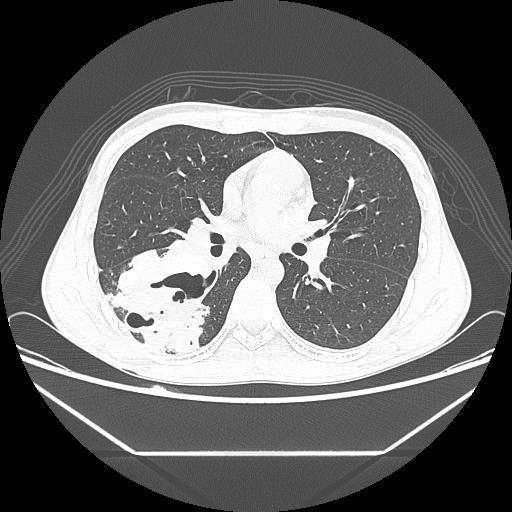
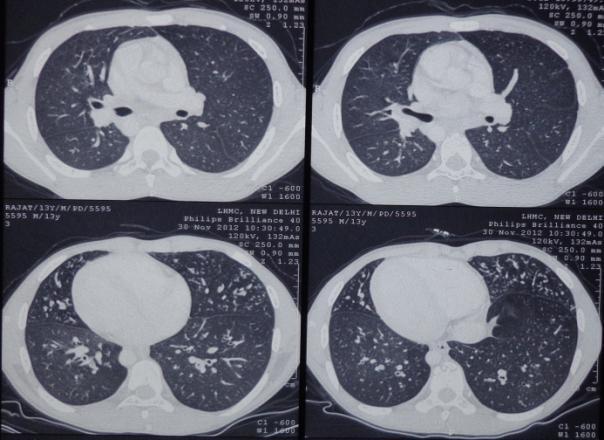
17 11y boy Presented in June 2012 Recurrent episodes of cough/ fever/fb X 5 years Already has taken ATT twice in 2006 and 2011 for clinical complaints and radiological opacities No clear improvement in either clinical picture Radiological opacities increasing



18


19
20
21

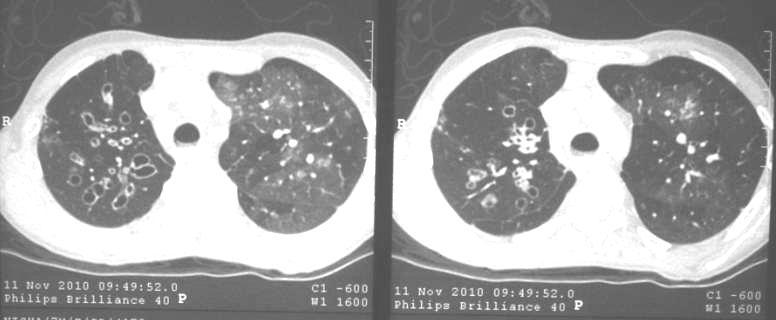
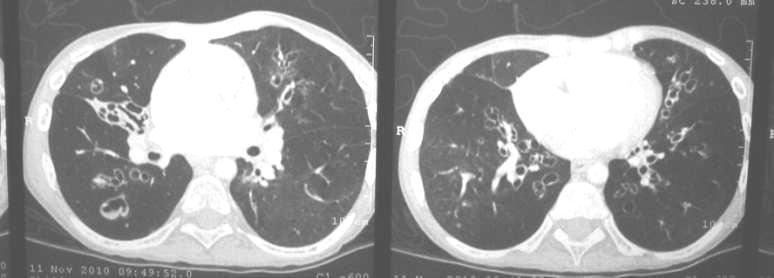
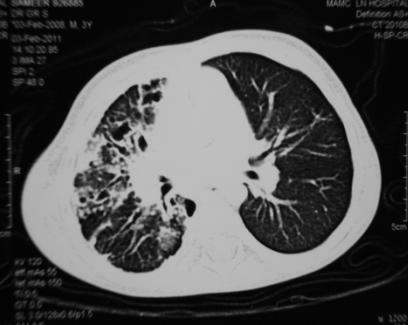
22 17 y boy Cough with sputum 15d Fever Hemoptysis few episodes No h/o contact with TB Sputum X 2 specimen negative Mantoux 14 mm

23

24
25 Further Investigations Serum IgE: 2684 Kua/L Aspergillus IgE: 8.29 kua/l (normal <0.35) Aspergillus IgG: (normal <8.00) Treatment Oral steroids + Itraconazole Antibiotics
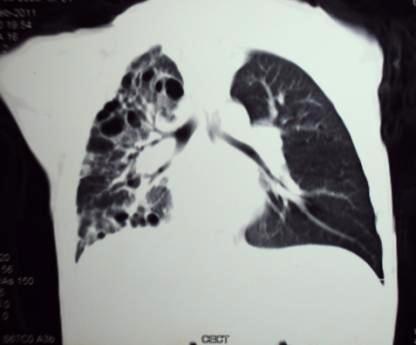
26 15 y old girl Chronic wet cough since age of 1 year Having exacerbations in between 4-5 per year Child treated for TB 2 years back Diagnosed as case of Atelectobronchiectasis secondary to tuberculosis
27 Admitted with Increased fever/cough/increased sputum purulence and volume Examination: Short stature Delayed puberty Wheezing Liver 3 cm spleen 7 cm
28 Investigations HIV NR Sweat Chloride 32 meq/l Sputum AFB Negative Mantoux negative FOB : bilateral tree shows mucopurulent secretions and few ulcerations at carina and left main bronchus
29
30 Investigations Immunoglobin profile IgA not detectable ( mg/dl) IgG ( mg/dl) IgM 3.4 ( mg/dl) CD3: 51.88% (57-85%); 514/microL ( ) CD8: 39.84% (5-23%); 395/microL (90-640)
31 2
32 12y boy Presented to Department of ENT November 2011 Chronic nasal obstruction Nasal discharge 3-4 years Exam: Inferior turbinate hypertrophy with nasal discharge
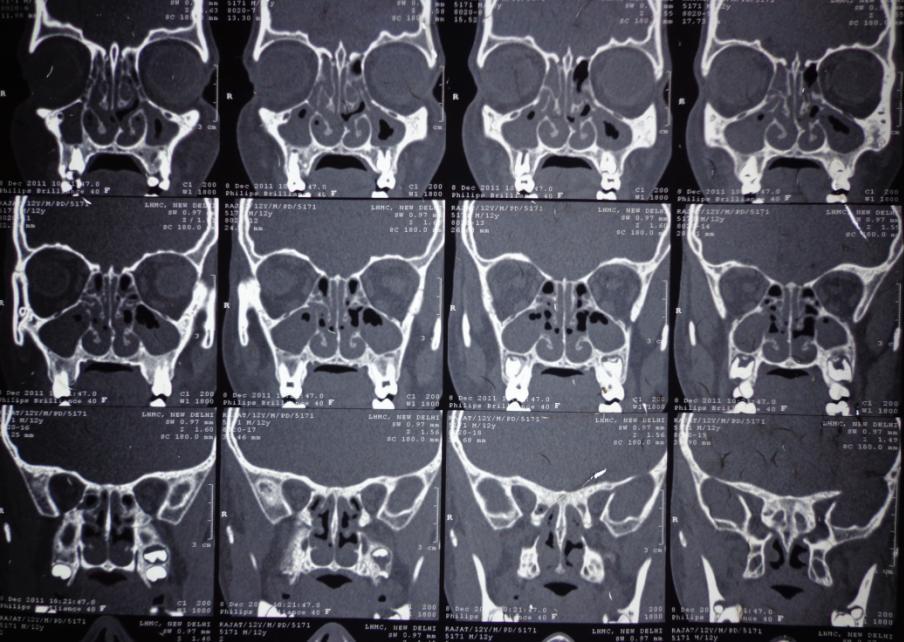
33
34 Severe persistent asthma with rhinosinusitis All modifiable factors checked multiple times Evaluated on difficult asthma protocol
35 March 2012 April 2012 May 2012


36


37
38 Management General approach and treatment of the specific underlying cause Education for patients and parents of children Airway clearance Physiotherapy and exercise Mucolytic and hyperosmolar therapies Airway drug therapy Bronchodilation Anti-inflammatory Antibiotic therapy Surgical management
39 Goals of treatment Identify and treat underlying cause to prevent disease progression. [D] Maintain or improve pulmonary function. [D] Reduce exacerbations. [D] Improve quality of life by reducing daily symptoms & exacerbations. [D] Achieve normal growth and development. [D] Patients with immune deficiency should be under joint care with a clinical immunologist. [D] Patients with CF should be referred to a CF specialist centre. [D] British Thoracic Society guideline for non-cf bronchiectasis. Thorax Jul;65 Suppl 1:i1-58.
40 Airway clearance techniques Passive: Postural drainage with percussion Active: PEP devices, Acapella, Active Cycles of Breathing Techniques The duration and frequency of the airway clearance technique should be specific to the needs of the individual. This may alter with periods of infective exacerbation. Airway clearance therapy should be for min once or twice daily.
41 Airway clearance techniques Postural drainage and percussion (PD&P) Active cycle of breathing technique (ACBT) Autogenic drainage (AD) Positive expiratory pressure (PEP) High frequency chest wall oscillation (HFCWO) Exercises None is superior to the other. Compliance and correct technique is important


42 Definition: Paediatric Bronchiectasis Exacerbation Kapur N et al. Pediatr Pulmonol Jan;47(1): British Thoracic Society guideline for non-cf bronchiectasis. Thorax Jul;65 Suppl 1:i1-58.
43 Treatment of Exacerbations When to Admit? Empirical Antibiotics: What to use? Sputum Microbiology Duration Severe Respiratory Distress Hypoxia Hypercapnic Respiratory Failure Non Improvement with oral Antibiotics Amoxicillin for oral Ceftriaxone/Cefuroxime for IV If can produce sputum, else BAL might be required Organism Targeted Therapy to be used Usually days
44 Chang AB. MJA 2008; 189:
45 Adjuvants Adjuvant Is it helpful? Reference Oral Azithromycin Bronchodilators (LABA) Reduce frequency of exacerbations and improve quality of life No Data. Can consider on the airway hyper-responsiveness Kelly C. Cochrane Database Syst Rev Mar 15;3:CD Goyal V. Cochrane Database Syst Rev Jun 10;(6):CD Inhaled Steroids No studies (acute stage or long term) Kapur N. Cochrane Database Syst Rev May 16;5:CD N-Acetyl Cysteine No significant benefit Tarrant BJ et al. Respirology Aug;22(6): Hypertonic Saline Nebulization (3 % or 7%) Limited Benefit outside CF settings Tarrant BJ et al. Respirology Aug;22(6): RNAse Not Recommended Tarrant BJ et al. Respirology Aug;22(6):
46 Follow Up-3 to 6 monthly Assessment of Severity Identify & manage complications & comorbidities Vaccinations Nutrition Avoid smoke Exacerbation frequency Exercise tolerance Signs of right heart failure Pulse oximetry Spirometry GERD Asthma Sleep- disordered breathing and cardiac complications. Annual Influenza Pneumococcal 13 and 23 valent Adequate growth monitoring and advice Active and passive smoking; biomass fuels Chang AB. MJA 2008; 189:
47 Take Home Messages Recognition of chronic wet cough is important Adequate treatment of PBB/CSLD might prevent bronchiectasis Think about etiology!!! Adequate chest PT and treatment of exacerbations are mainstay of treatment.
48 Thank You!!
Bronchiectasis: An Imaging Approach
 Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Bronchiectasis in Adults - Suspected
 Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
A Place For Airway Clearance Therapy In Today s Healthcare Environment
 A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
Bronchiectasis. Examples include: Viral infections (measles, adenovirus, influenza)
") Bronchiectasis What is Bronchiectasis? Bronchiectasis (pronounced bron-kee-ek'-tas-is) is a condition of the airways in the lungs. These airways (bronchial tubes) are tubelike structures that branch from
Bronchiectasis What is Bronchiectasis? Bronchiectasis (pronounced bron-kee-ek'-tas-is) is a condition of the airways in the lungs. These airways (bronchial tubes) are tubelike structures that branch from
NON-CYSTIC FIBROSIS BRONCHIECTASIS
 NON-CYSTIC FIBROSIS BRONCHIECTASIS MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the
NON-CYSTIC FIBROSIS BRONCHIECTASIS MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the
NON-CF BRONCHIECTASIS IN ADULTS
 Séminaire de Pathologie Infectieuse Jeudi 25 juin 2008 Cliniques Universitaires UCL de Mont-Godinne, Yvoir NON-CF BRONCHIECTASIS IN ADULTS Dr Robert Wilson Royal Brompton Hospital, London, UK Aetiology
Séminaire de Pathologie Infectieuse Jeudi 25 juin 2008 Cliniques Universitaires UCL de Mont-Godinne, Yvoir NON-CF BRONCHIECTASIS IN ADULTS Dr Robert Wilson Royal Brompton Hospital, London, UK Aetiology
Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX
 Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX Pioneer of Respiratory Medicine 2016 marked 200th anniversary of his
Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX Pioneer of Respiratory Medicine 2016 marked 200th anniversary of his
Bronchiectasis. What is bronchiectasis? What causes bronchiectasis?
 This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c)
 Diffuse bronchiectasis b) Cystic fibrosis c)") Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c) Bronchiolitis obliterans d) Complicated acute pneumonia e)
Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c) Bronchiolitis obliterans d) Complicated acute pneumonia e)
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
Dr Conroy Wong. Professor Richard Beasley. Dr Sarah Mooney. Professor Innes Asher
 Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Pulmonary
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Pulmonary 1. GOAL: Diagnose and manage patients with asthma. 2. GOAL: Understand the role of the pediatrician in preventing
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Pulmonary 1. GOAL: Diagnose and manage patients with asthma. 2. GOAL: Understand the role of the pediatrician in preventing
Disease spectrum. IPA Invasive pulmonary aspergillosis
 Aspergillus & ABPA Disease spectrum IPA Invasive pulmonary aspergillosis ABPA ABPA pathophysiology conidia of Aspergillus trapped in mucous and narrowed airways of asthmatics/cf germinate to form hyphae
Aspergillus & ABPA Disease spectrum IPA Invasive pulmonary aspergillosis ABPA ABPA pathophysiology conidia of Aspergillus trapped in mucous and narrowed airways of asthmatics/cf germinate to form hyphae
Chronic suppurative lung disease in adults
 Case Report Chronic suppurative lung disease in adults Mark L. Metersky 1, Antranik Mangardich 2 1 Division of Pulmonary and Critical Care Medicine, University of Connecticut School of Medicine, Farmington,
Case Report Chronic suppurative lung disease in adults Mark L. Metersky 1, Antranik Mangardich 2 1 Division of Pulmonary and Critical Care Medicine, University of Connecticut School of Medicine, Farmington,
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Starship Paediatric Respiratory and Sleep Medicine Department Outpatient Referral Criteria General Principles
 Starship Paediatric Respiratory and Sleep Medicine Department Outpatient Referral Criteria General Principles This document provides guidance for elective outpatient referrals to the Starship Tertiary
Starship Paediatric Respiratory and Sleep Medicine Department Outpatient Referral Criteria General Principles This document provides guidance for elective outpatient referrals to the Starship Tertiary
Bronchiectasis. Grant Waterer. Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago
 Bronchiectasis Grant Waterer MBBS PhD MBA FRACP FCCP Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago Conflicts of Interest I have
Bronchiectasis Grant Waterer MBBS PhD MBA FRACP FCCP Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago Conflicts of Interest I have
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
The Respiratory System
 130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
BTS Guideline for non-cf Bronchiectasis
 ISSN 2040-2023 July 2010 BTS Guideline for non-cf Bronchiectasis A Quick Reference Guide British Thoracic Society www.brit-thoracic.org.uk BTS GUIDELINE FOR NON-CF BRONCHIECTASIS A QUICK REFERENCE GUIDE
ISSN 2040-2023 July 2010 BTS Guideline for non-cf Bronchiectasis A Quick Reference Guide British Thoracic Society www.brit-thoracic.org.uk BTS GUIDELINE FOR NON-CF BRONCHIECTASIS A QUICK REFERENCE GUIDE
Dr.Sivaramakrishnan PICU KKCTH
 Dr.Sivaramakrishnan PICU KKCTH CASE 1 11/2 year old female child Known wheezer on intermittent bronchodilators Admitted with h/o cough for 2 days Increased work of breathing for 1 day Afebrile/sick looking
Dr.Sivaramakrishnan PICU KKCTH CASE 1 11/2 year old female child Known wheezer on intermittent bronchodilators Admitted with h/o cough for 2 days Increased work of breathing for 1 day Afebrile/sick looking
Wheeze. Respiratory Tract Symptoms. Prof RJ Green Department of Paediatrics. Cough. Wheeze/noisy breathing. Acute. Tight chest. Shortness of breath
 Wheeze Prof RJ Green Department of Paediatrics Respiratory Tract Symptoms Cough Tight chest Wheeze/noisy breathing Shortness of breath Acute Chronic Respiratory rate Most important sign of respiratory
Wheeze Prof RJ Green Department of Paediatrics Respiratory Tract Symptoms Cough Tight chest Wheeze/noisy breathing Shortness of breath Acute Chronic Respiratory rate Most important sign of respiratory
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
4.6 Small airways disease
 4.6 Small airways disease Author: Jean-Marc Fellrath 1. INTRODUCTION Small airways are defined as any non alveolated and noncartilaginous airway that has an internal diameter of 2 mm. Several observations
4.6 Small airways disease Author: Jean-Marc Fellrath 1. INTRODUCTION Small airways are defined as any non alveolated and noncartilaginous airway that has an internal diameter of 2 mm. Several observations
Corporate Medical Policy
 Corporate Medical Policy Oscillatory Devices for the Treatment of Respiratory Conditions File Name: Origination: Last CAP Review: Next CAP Review: Last Review: oscillatory_devices_for_treatment_of_respiratory_conditions
Corporate Medical Policy Oscillatory Devices for the Treatment of Respiratory Conditions File Name: Origination: Last CAP Review: Next CAP Review: Last Review: oscillatory_devices_for_treatment_of_respiratory_conditions
Session Guidelines. This is a 15 minute webinar session for CNC physicians and staff
 Respiratory Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars monthly to address topics related to risk adjustment documentation and coding
Respiratory Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars monthly to address topics related to risk adjustment documentation and coding
Asthma. - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness.
 Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Recent advances in diagnosis and management of ABPA. Arindam SR(Pulmonary Medicine)
") Recent advances in diagnosis and management of ABPA Arindam SR(Pulmonary Medicine) Conventional diagnostic criteria for ABPA Primary Episodic bronchial obstruction (asthma) Peripheral blood eosinophilia
Recent advances in diagnosis and management of ABPA Arindam SR(Pulmonary Medicine) Conventional diagnostic criteria for ABPA Primary Episodic bronchial obstruction (asthma) Peripheral blood eosinophilia
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
Bronchiectasis. Introduction. Key points
 15 Bronchiectasis Introduction i Key points Patients with bronchiectasis typically have chronic airway infection, punctuated by acute exacerbations and accompanied by progressive airflow obstruction. Bronchiectasis
15 Bronchiectasis Introduction i Key points Patients with bronchiectasis typically have chronic airway infection, punctuated by acute exacerbations and accompanied by progressive airflow obstruction. Bronchiectasis
CYSTIC FIBROSIS OBJECTIVES NO CONFLICT OF INTEREST TO DISCLOSE
 CYSTIC FIBROSIS Madhu Pendurthi MD MPH Staff Physician, Mercy Hospital Springfield, MO NO CONFLICT OF INTEREST TO DISCLOSE OBJECTIVES Epidemiology of Cystic Fibrosis (CF) Genetic basis and pathophysiology
CYSTIC FIBROSIS Madhu Pendurthi MD MPH Staff Physician, Mercy Hospital Springfield, MO NO CONFLICT OF INTEREST TO DISCLOSE OBJECTIVES Epidemiology of Cystic Fibrosis (CF) Genetic basis and pathophysiology
Evaluating a child with recurrent cough and nighttime symptoms
 Evaluating a child with recurrent cough and nighttime symptoms CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep
Evaluating a child with recurrent cough and nighttime symptoms CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep
High Frequency Chest Wall Oscillating Devices (HFCWO) (Airway Clearance Systems)
 (Airway Clearance Systems)") High Frequency Chest Wall Oscillating Devices (HFCWO) (Airway Clearance Systems) Date of Origin: 05/2015 Last Review Date: 07/26/2017 Effective Date: 07/26/2017 Dates Reviewed: 07/2016 Developed By: Medical
High Frequency Chest Wall Oscillating Devices (HFCWO) (Airway Clearance Systems) Date of Origin: 05/2015 Last Review Date: 07/26/2017 Effective Date: 07/26/2017 Dates Reviewed: 07/2016 Developed By: Medical
Evaluation of Patients with Diffuse Bronchiectasis
 Evaluation of Patients with Diffuse Bronchiectasis Dr. Patricia Eshaghian, MD Assistant Clinical Professor of Medicine Director, UCLA Adult Cystic Fibrosis Affiliate Program UCLA Division of Pulmonary
Evaluation of Patients with Diffuse Bronchiectasis Dr. Patricia Eshaghian, MD Assistant Clinical Professor of Medicine Director, UCLA Adult Cystic Fibrosis Affiliate Program UCLA Division of Pulmonary
Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis
 Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
Rhinosinusitis. John Ramey, MD Joseph Russell, MD
 Rhinosinusitis John Ramey, MD Joseph Russell, MD Disclosure Statement RSFH as a continuing medical education provider, accredited by the South Carolina Medical Association, it is the policy of RSFH to
Rhinosinusitis John Ramey, MD Joseph Russell, MD Disclosure Statement RSFH as a continuing medical education provider, accredited by the South Carolina Medical Association, it is the policy of RSFH to
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
The Use of Active Cycle of Breathing Technique (ACBT) In Pulmonary Physiotherapy: A Critical Review of the Literature Lauro G. Villegas Jr.
 In Pulmonary Physiotherapy: A Critical Review of the Literature Lauro G. Villegas Jr.") The Use of Active Cycle of Breathing Technique (ACBT) In Pulmonary Physiotherapy: A Critical Review of the Literature Lauro G. Villegas Jr., PTRP Keywords: Active Cycle of Breathing Technique (ACBT), Pulmonary
The Use of Active Cycle of Breathing Technique (ACBT) In Pulmonary Physiotherapy: A Critical Review of the Literature Lauro G. Villegas Jr., PTRP Keywords: Active Cycle of Breathing Technique (ACBT), Pulmonary
Historical perspective
 Bronchiectasis Dilated airways with frequently thickened walls Faculty/Presenter Disclosure Faculty: Dr. Alan Kaplan Relationships with commercial interests (12 months) Grants/research support: N/A Speakers
Bronchiectasis Dilated airways with frequently thickened walls Faculty/Presenter Disclosure Faculty: Dr. Alan Kaplan Relationships with commercial interests (12 months) Grants/research support: N/A Speakers
Update on bronchiectasis guidelines. James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK
 Update on bronchiectasis guidelines James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK University of Dundee Bronchiectasis guidelines 2017 2010 2006 2008 2015 2015 Currently valid guidelines
Update on bronchiectasis guidelines James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK University of Dundee Bronchiectasis guidelines 2017 2010 2006 2008 2015 2015 Currently valid guidelines
COUGH. Jim Reid University of Otago Medical School Dunedin, New Zealand
 COUGH Jim Reid University of Otago Medical School Dunedin, New Zealand COUGH One of five most common presentations in general practice Remember the law of probability Common things occur commonly But
COUGH Jim Reid University of Otago Medical School Dunedin, New Zealand COUGH One of five most common presentations in general practice Remember the law of probability Common things occur commonly But
Eosinophilic lung diseases
 Eosinophilic lung diseases Chai Gin Tsen Department of Respiratory and Critical Care Medicine Tan Tock Seng Hospital The eyes do not see what the mind does not know Not very common A high index of suspicion
Eosinophilic lung diseases Chai Gin Tsen Department of Respiratory and Critical Care Medicine Tan Tock Seng Hospital The eyes do not see what the mind does not know Not very common A high index of suspicion
Swyer-James Syndrome: An Infrequent Cause Of Bronchiectasis?
 ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 12 Number 1 Swyer-James Syndrome: An Infrequent Cause Of Bronchiectasis? A Huaringa, S Malek, M Haro, L Tapia Citation A Huaringa, S Malek, M
ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 12 Number 1 Swyer-James Syndrome: An Infrequent Cause Of Bronchiectasis? A Huaringa, S Malek, M Haro, L Tapia Citation A Huaringa, S Malek, M
A. Service Specifications
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No: 170050S Service Primary Ciliary Dyskinesia Management Service (adults) Commissioner Lead Provider Lead 1. Scope 1.1 Prescribed
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No: 170050S Service Primary Ciliary Dyskinesia Management Service (adults) Commissioner Lead Provider Lead 1. Scope 1.1 Prescribed
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Disclosure. Evaluation of Chronic Cough in the Pediatric Patient
 Evaluation of Chronic Cough in the Pediatric Patient Kyle McCallin, D.O. Pediatric Pulmonology Kaiser Permanente Fontana Medical Center Disclosure None of the faculty or planners associated with this activity
Evaluation of Chronic Cough in the Pediatric Patient Kyle McCallin, D.O. Pediatric Pulmonology Kaiser Permanente Fontana Medical Center Disclosure None of the faculty or planners associated with this activity
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
Total collapse of the lung in aspergillosis
 Thorax (1965), 20, 118. Total collapse of the lung in aspergillosis R. H. ELLIS From the Gloucestershire Royal Hospital, Pulmonary aspergillosis can be divided conveniently into two main types, allergic
Thorax (1965), 20, 118. Total collapse of the lung in aspergillosis R. H. ELLIS From the Gloucestershire Royal Hospital, Pulmonary aspergillosis can be divided conveniently into two main types, allergic
Management of Common Respiratory Disorders in Children. Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016
 Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children. Disclosures. Roadmap 6/10/2016
 Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Chronic Obstructive Pulmonary Disease (COPD) Copyright 2014 by Mosby, an imprint of Elsevier Inc.
 Copyright 2014 by Mosby, an imprint of Elsevier Inc.") Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Northumbria Healthcare NHS Foundation Trust. Bronchiectasis. Issued by Respiratory Medicine
 Northumbria Healthcare NHS Foundation Trust Bronchiectasis Issued by Respiratory Medicine The aim of this booklet is to help you manage your bronchiectasis. It contains information which you should find
Northumbria Healthcare NHS Foundation Trust Bronchiectasis Issued by Respiratory Medicine The aim of this booklet is to help you manage your bronchiectasis. It contains information which you should find
Changes in the management of children with Cystic Fibrosis. Caroline Murphy & Deirdre O Donovan CF Nurses
 Changes in the management of children with Cystic Fibrosis Caroline Murphy & Deirdre O Donovan CF Nurses What Is Cystic Fibrosis? Cystic fibrosis (CF) is an inherited chronic disease that primarily affects
Changes in the management of children with Cystic Fibrosis Caroline Murphy & Deirdre O Donovan CF Nurses What Is Cystic Fibrosis? Cystic fibrosis (CF) is an inherited chronic disease that primarily affects
Interesting cases in fungal asthma
 Interesting cases in fungal asthma Ritesh Agarwal MD, DM Professor of Pulmonary Medicine Postgraduate Institute of Medical Education and Research Chandigarh, India Fungal asthma Broadly defined as the
Interesting cases in fungal asthma Ritesh Agarwal MD, DM Professor of Pulmonary Medicine Postgraduate Institute of Medical Education and Research Chandigarh, India Fungal asthma Broadly defined as the
Clinical Commissioning Policy: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages)
") Clinical Commissioning Policy: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages) Reference: NHS England: 16029/P NHS England INFORMATION READER BOX Directorate Medical Operations and
Clinical Commissioning Policy: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages) Reference: NHS England: 16029/P NHS England INFORMATION READER BOX Directorate Medical Operations and
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Care of the Patient with a Respiratory Disorder
 Care of the Patient with a Respiratory Disorder 1 Slide 1 Overview of Anatomy and Physiology External respiration Exchange of oxygen and carbon dioxide between the lung and the environment Internal respiration
Care of the Patient with a Respiratory Disorder 1 Slide 1 Overview of Anatomy and Physiology External respiration Exchange of oxygen and carbon dioxide between the lung and the environment Internal respiration
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
Respiratory system. Applied Anatomy &Physiology
 Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
What is Cystic Fibrosis? CYSTIC FIBROSIS. Genetics of CF
 What is Cystic Fibrosis? CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Chronic, progressive and life limiting autosomal recessive genetic disease characterized by chronic
What is Cystic Fibrosis? CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Chronic, progressive and life limiting autosomal recessive genetic disease characterized by chronic
5/5/2013. The Respiratory System. Chapter 16 Notes. The Respiratory System. Nasal Cavity. Sinuses
 The Respiratory System Chapter 16 Notes The Respiratory System Objectives List the general functions of the respiratory system. Identify the organs of the respiratory system. Describe the functions of
The Respiratory System Chapter 16 Notes The Respiratory System Objectives List the general functions of the respiratory system. Identify the organs of the respiratory system. Describe the functions of
PIDS AND RESPIRATORY DISORDERS
 PRIMARY IMMUNODEFICIENCIES PIDS AND RESPIRATORY DISORDERS PIDS AND RESPIRATORY DISORDERS 1 PRIMARY IMMUNODEFICIENCIES ABBREVIATIONS COPD CT MRI IG PID Chronic obstructive pulmonary disease Computed tomography
PRIMARY IMMUNODEFICIENCIES PIDS AND RESPIRATORY DISORDERS PIDS AND RESPIRATORY DISORDERS 1 PRIMARY IMMUNODEFICIENCIES ABBREVIATIONS COPD CT MRI IG PID Chronic obstructive pulmonary disease Computed tomography
Cystic Fibrosis. Jennifer McDaniel, BS, RRT-NPS
 Cystic Fibrosis Jennifer McDaniel, BS, RRT-NPS Overview Cystic fibrosis is the most common fatal, inherited disease in the U. S. CF results from a defective autosomal recessive gene One copy of gene =
Cystic Fibrosis Jennifer McDaniel, BS, RRT-NPS Overview Cystic fibrosis is the most common fatal, inherited disease in the U. S. CF results from a defective autosomal recessive gene One copy of gene =
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER
 MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
The Bacteriology of Bronchiectasis in Australian Indigenous children
 The Bacteriology of Bronchiectasis in Australian Indigenous children Kim Hare, Amanda Leach, Peter Morris, Heidi Smith-Vaughan, Anne Chang Presentation outline What is bronchiectasis? Our research at Menzies
The Bacteriology of Bronchiectasis in Australian Indigenous children Kim Hare, Amanda Leach, Peter Morris, Heidi Smith-Vaughan, Anne Chang Presentation outline What is bronchiectasis? Our research at Menzies
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
Bronchiectasis Domiciliary treatment. Prof. Adam Hill Royal Infirmary and University of Edinburgh
 Bronchiectasis Domiciliary treatment Prof. Adam Hill Royal Infirmary and University of Edinburgh Plan of talk Background of bronchiectasis Who requires IV antibiotics Domiciliary treatment Results to date.
Bronchiectasis Domiciliary treatment Prof. Adam Hill Royal Infirmary and University of Edinburgh Plan of talk Background of bronchiectasis Who requires IV antibiotics Domiciliary treatment Results to date.
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS
 DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS INTRDUCTION In the last lecture we discussed the difference between restrictive and obstructive lung
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS INTRDUCTION In the last lecture we discussed the difference between restrictive and obstructive lung
Physiotherapy in lung disease - top tips for clinicians. Sita Kansagra Specialist Outpatient Physiotherapist
 Physiotherapy in lung disease - top tips for clinicians Sita Kansagra Specialist Outpatient Physiotherapist Aims: Run through current physiotherapy practice Airway clearance Pulmonary rehabilitation Dysfunctional
Physiotherapy in lung disease - top tips for clinicians Sita Kansagra Specialist Outpatient Physiotherapist Aims: Run through current physiotherapy practice Airway clearance Pulmonary rehabilitation Dysfunctional
FEP Medical Policy Manual
 FEP Medical Policy Manual Effective Date: October 15, 2018 Related Policies: None Oscillatory Devices for the Treatment of Cystic Fibrosis and Other Description Oscillatory devices are alternatives to
FEP Medical Policy Manual Effective Date: October 15, 2018 Related Policies: None Oscillatory Devices for the Treatment of Cystic Fibrosis and Other Description Oscillatory devices are alternatives to
WF RESPIRATORY SYSTEM. RESPIRATORY MEDICINE
 WF RESPIRATORY SYSTEM. RESPIRATORY MEDICINE 1 Societies 11 History 13 Dictionaries. Encyclopaedias. Bibliographies Use for general works only. Classify with specific aspect where possible 15 Classification.
WF RESPIRATORY SYSTEM. RESPIRATORY MEDICINE 1 Societies 11 History 13 Dictionaries. Encyclopaedias. Bibliographies Use for general works only. Classify with specific aspect where possible 15 Classification.
DIFFICULT ASTHMA. Dr. Prathyusha Dr. S.Balasubramanian KKCTH
 DIFFICULT ASTHMA Dr. Prathyusha Dr. S.Balasubramanian KKCTH CASE SUMMARY 11 yr old girl, Neyveli Treated as moderate persistent asthma x 5 years On Seroflo [ LABA + steroid ] 250 2 puffs BD and intermittent
DIFFICULT ASTHMA Dr. Prathyusha Dr. S.Balasubramanian KKCTH CASE SUMMARY 11 yr old girl, Neyveli Treated as moderate persistent asthma x 5 years On Seroflo [ LABA + steroid ] 250 2 puffs BD and intermittent
Pulmonary function abnormalities in adult patients with acute exacerbation of bronchiectasis: A retrospective risk factor analysis
 Original Article Pulmonary function abnormalities in adult patients with acute exacerbation of bronchiectasis: A retrospective risk factor analysis Chronic Respiratory Disease 2015, Vol. 12(3) 222 229
Original Article Pulmonary function abnormalities in adult patients with acute exacerbation of bronchiectasis: A retrospective risk factor analysis Chronic Respiratory Disease 2015, Vol. 12(3) 222 229
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
Focus on Cystic Fibrosis. Cystic Fibrosis. Cystic Fibrosis
 Focus on (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Autosomal recessive, multisystem
Focus on (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Autosomal recessive, multisystem
People with asthma who smoke. The combination of asthma, a chronic airway disease, and smoking increases the risk of COPD even more.
 COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
2014/03/04. An Approach to the Child with Recurrent Respiratory Tract Infections. RRTI s: Frustrating parents
 An Approach to the Child with Recurrent Respiratory Tract Infections andré van niekerk paediatrician & paediatric pulmonologist clinton & alberlito hospitals RRTI s: Frustrating parents A common problem.
An Approach to the Child with Recurrent Respiratory Tract Infections andré van niekerk paediatrician & paediatric pulmonologist clinton & alberlito hospitals RRTI s: Frustrating parents A common problem.
Evaluating a child with recurrent cough and night time symptoms
 Evaluating a child with recurrent cough and night time symptoms CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep
Evaluating a child with recurrent cough and night time symptoms CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Overview of Cystic fibrosis in children. Apeksha Sathyaprasad, MD Pediatric pulmonologist
 Overview of Cystic fibrosis in children Apeksha Sathyaprasad, MD Pediatric pulmonologist No conflicts of interest OBJECTIVES Review pathophysiology of pulmonary disease in cystic fibrosis Review diagnostic
Overview of Cystic fibrosis in children Apeksha Sathyaprasad, MD Pediatric pulmonologist No conflicts of interest OBJECTIVES Review pathophysiology of pulmonary disease in cystic fibrosis Review diagnostic
Paediatric Wheeze and pneumonia. RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa
 Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
R eview. Cough: Controversies and Consensus Brian s Case. Acute Cough
 R eview Cough: Controversies and Consensus 2011 Copyright Not for Sale or Commercial Distribution Irvin Mayers, MD, FRCPC Unauthorised use prohibited. Authorised users can download, display, view and print
R eview Cough: Controversies and Consensus 2011 Copyright Not for Sale or Commercial Distribution Irvin Mayers, MD, FRCPC Unauthorised use prohibited. Authorised users can download, display, view and print
Management of URTI s in Children
 Management of URTI s in Children Robin J Green PhD Antibiotics - Dilemmas for General Practitioners Antibiotic overuse = Resistance Delay in antibiotic use = Mortality Patient expectation Employer expectation
Management of URTI s in Children Robin J Green PhD Antibiotics - Dilemmas for General Practitioners Antibiotic overuse = Resistance Delay in antibiotic use = Mortality Patient expectation Employer expectation
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Autogenic Drainage versus Acapella for Airway Clearance in Patients with Bronchiectasis: Randomized
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Autogenic Drainage versus Acapella for Airway Clearance in Patients with Bronchiectasis: Randomized
Allergic Bronchopulmonary Aspergillosis: An Unusual Complication of Bronchial Asthma
 Allergic Bronchopulmonary Aspergillosis: An Unusual Complication of Bronchial Asthma Pages with reference to book, From 329 To 331 S. Fayyaz Hussain, Javaid A. Khan ( Department of Medicine, The Aga Khan
Allergic Bronchopulmonary Aspergillosis: An Unusual Complication of Bronchial Asthma Pages with reference to book, From 329 To 331 S. Fayyaz Hussain, Javaid A. Khan ( Department of Medicine, The Aga Khan
Group B: Directed self-study Group C: Anatomy lab. Lecture: Structure and function of larynx. Lecture: Dead space & compliance of lungs
 Timetable Week 1 (1 st January 2018) Theme: Structure and functions of the lungs Group A: Anatomy lab Group C: Histology lab Upper Group B: Anatomy lab Group C: Anatomy lab Group A: Histology lab Upper
Timetable Week 1 (1 st January 2018) Theme: Structure and functions of the lungs Group A: Anatomy lab Group C: Histology lab Upper Group B: Anatomy lab Group C: Anatomy lab Group A: Histology lab Upper
Allergic bronchopulmonary Aspergillosis mimicking as bilateral cavitatory pulmonary tuberculosis.
 INTERNATIONAL JOURNAL OF CURRENT RESEARCH IN BIOLOGY AND MEDICINE ISSN: 2455-944X www.darshanpublishers.com DOI:10.22192/ijcrbm Volume 3, Issue 3-2018 Original Research Article DOI: http://dx.doi.org/10.22192/ijcrbm.2018.03.03.004
INTERNATIONAL JOURNAL OF CURRENT RESEARCH IN BIOLOGY AND MEDICINE ISSN: 2455-944X www.darshanpublishers.com DOI:10.22192/ijcrbm Volume 3, Issue 3-2018 Original Research Article DOI: http://dx.doi.org/10.22192/ijcrbm.2018.03.03.004
High Frequency Chest Wall Oscillation Devices
 High Frequency Chest Wall Oscillation Devices Policy Number: Original Effective Date: MM.01.007 07/15/2003 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 12/18/2015 Section: DME
High Frequency Chest Wall Oscillation Devices Policy Number: Original Effective Date: MM.01.007 07/15/2003 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 12/18/2015 Section: DME
ATHLETES & PRESCRIBING PHYSICIANS PLEASE READ TUE APPLICATION CHECKLIST POST INFECTIOUS COUGH
 ATHLETES & PRESCRIBING PHYSICIANS PLEASE READ USADA can grant a Therapeutic Use Exemption (TUE) in compliance with the World Anti- Doping Agency International Standard for TUEs. The TUE application process
ATHLETES & PRESCRIBING PHYSICIANS PLEASE READ USADA can grant a Therapeutic Use Exemption (TUE) in compliance with the World Anti- Doping Agency International Standard for TUEs. The TUE application process
Approach to a child with recurrent infections. Dave le Roux 9 March 2012
 Approach to a child with recurrent infections Dave le Roux 9 March 2012 Jeffrey Modell Foundation http://www.info4pi.org Primary immune deficiencies: myths PID s are very very rare Selective IgA 1:333
Approach to a child with recurrent infections Dave le Roux 9 March 2012 Jeffrey Modell Foundation http://www.info4pi.org Primary immune deficiencies: myths PID s are very very rare Selective IgA 1:333
Vascular Lung Diseases
 Vascular Lung Diseases SESSION SPECIFIC OBJECTIVES List the major types of vascular lung disease Recognize and describe the pathology of vascular lung disease: Pulmonary embolism, thrombosis, hypertension,
Vascular Lung Diseases SESSION SPECIFIC OBJECTIVES List the major types of vascular lung disease Recognize and describe the pathology of vascular lung disease: Pulmonary embolism, thrombosis, hypertension,
Fungal (Aspergillus and Candida) infections in Cystic fibrosis
 infections in Cystic fibrosis") Fungal (Aspergillus and Candida) infections in Cystic fibrosis Malena Cohen-Cymberknoh, MD CF Center Hadassah-Hebrew University Medical Center Jerusalem, Israel Israeli Annual CF Conference, Herzlyia,
Fungal (Aspergillus and Candida) infections in Cystic fibrosis Malena Cohen-Cymberknoh, MD CF Center Hadassah-Hebrew University Medical Center Jerusalem, Israel Israeli Annual CF Conference, Herzlyia,
BPCO/COPD. Andrea Bellone UOC di Pronto Soccorso Ospedale Sant'Anna di Como
 BPCO/COPD Andrea Bellone UOC di Pronto Soccorso Ospedale Sant'Anna di Como Definition of COPD (1) COPD is a preventable and treatable disease state characterised by airflow limitation that is not fully
BPCO/COPD Andrea Bellone UOC di Pronto Soccorso Ospedale Sant'Anna di Como Definition of COPD (1) COPD is a preventable and treatable disease state characterised by airflow limitation that is not fully
Management of Respiratory Issues in the School Setting. Pediatric Indicators of High Risk 8/7/2015. Facts about Pediatric Respiratory Failure
 Management of Respiratory Issues in the School Setting Toni B. Vento, MS, RN, NCSN Supervisor of Health Services Medford Public Schools Pediatric Indicators of High Risk Anatomic features of the immature
Management of Respiratory Issues in the School Setting Toni B. Vento, MS, RN, NCSN Supervisor of Health Services Medford Public Schools Pediatric Indicators of High Risk Anatomic features of the immature
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
USAID Health Care Improvement Project. pneumonia) respiratory infections through improved case management (amb/hosp)
 respiratory infections through improved case management (amb/hosp)") Improvement objective: : decrease morbidity and mortality due to acute upper (rhinitis, sinusitis, pharyngitis) and lower (bronchitis, pneumonia) respiratory infections through improved case management
Improvement objective: : decrease morbidity and mortality due to acute upper (rhinitis, sinusitis, pharyngitis) and lower (bronchitis, pneumonia) respiratory infections through improved case management
Section: Durable Medical Equipment Last Reviewed Date: June Policy No: 45 Effective Date: September 1, 2014
 Medical Policy Manual Topic: Oscillatory Devices for the Treatment of Cystic Fibrosis and Other Respiratory Disorders Date of Origin: May 26, 2011 Section: Durable Medical Equipment Last Reviewed Date:
Medical Policy Manual Topic: Oscillatory Devices for the Treatment of Cystic Fibrosis and Other Respiratory Disorders Date of Origin: May 26, 2011 Section: Durable Medical Equipment Last Reviewed Date: