NON-CYSTIC FIBROSIS BRONCHIECTASIS
|
|
|
- Lisa Webb
- 5 years ago
- Views:
Transcription

1 NON-CYSTIC FIBROSIS BRONCHIECTASIS MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the University of Connecticut school of Medicine in the Division of Pulmonary and Critical Care and is Director of UCONN Center for Bronchiectasis Care. Dr. Metersky has long standing interest in pulmonary infections, including pneumonia and bronchiectasis and has published and presented extensively on diagnosis, treatment and prevention of pneumonia and bronchiectasis. He served on the Technical Expert Panel for the CMS National Pneumonia Project and was the American Thoracic Society Co-Chair of the writing panel for the Management of Adults with Hospital-acquired and Ventilatorassociated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society and is a member of the Community-Acquired Pneumonia Guideline panel. In his spare time, he enjoys fencing and skiing. He is not a wine connoisseur, but plans to make up for that deficiency during this meeting. OBJECTIVES: Participants should be better able to: 1. At the conclusion of the talk, the participant will be able to list common etiologies of bronchiectasis; 2. At the conclusion of the talk, the participant will be able to describe clinical characteristics of bronchiectasis related to specific underlying etiologies; 3. At the conclusion of the talk, the participant will understand the treatment options available treatments for bronchiectasis and some of their limitations. SATURDAY, MARCH 25, :45 AM
2 Dr. Metersky has received research grants from Aradigm and Bayer and serves as a consultant for Insmed, but these do not create a conflict related to the following presentation. Mark L. Metersky, MD Director, Center for Bronchiectasis Care, Chief, Division of Pulmonary, Critical Care and Sleep Medicine, University of Connecticut 1
3 Clinical trial participant Gilead Bayer Aradigm Consultant Grifols Insmed There are many recommended diagnostic protocols Most assume that all patients are alike The longer the list of tests recommended for all patients, the more skeptical one should be Evaluation may vary depending upon Patient age Severity/character of disease Resource availability Distance 2
 Idiopathic 48 Postinfectious 25 Immunodeficiency (various) 8 Allergic bronchopulmonary aspergillosis 7 Primary ciliary dyskinesia 5")

4 Reported etiologies of bronchiectasis pooled from three cohort studies Etiologies Among Three Large Cohorts Percent of Patients (n = 418 patients) Idiopathic 48 Postinfectious 25 Immunodeficiency (various) 8 Allergic bronchopulmonary aspergillosis 7 Primary ciliary dyskinesia 5 Young syndrome 3 Rheumatoid arthritis 2 Ulcerative colitis 2 Aspiration or gastroesophageal reflux 2 Yellow nail syndrome 1 Non-tuberculous mycobacterial infection 1 Cystic fibrosis 1 Diffuse panbronchiolitis 1 Congenital <1 Quast, Dis Mon, 2008 Pasteur, AJRCCM, 2000 Nicotra, Chest,
5 Other Reported Etiologies Acquired immunodeficiency Lymphoma HIV-related Organ or bone marrow transplant Autoimmune Relapsing polychondritis Ankylosing spondylitis Sjogren s Syndrome Chronic obstructive pulmonary disease Congenital or genetic 1 -Antitrypsin deficiency Job syndrome (hyper immunoglobulin E syndrome) Marfan syndrome Mounier-Kuhn syndrome (tracheobronchomegaly) Williams-Campbell syndrome Endobronchial obstruction Neoplasm Foreign body Extrinsic compression by lymph nodes Inhalational exposure Smoke Ammonia Chlorine Traction Pulmonary fibrosis Sarcoidosis Metersky, Clin Chest Med, 2012 Unrecalled prior infection? Double hit hypothesis? 1 CFTR mutation Bienvenu, AJRCCM, 2010 Heterozygote alpha-1 antitrypsin deficiency Mannose binding lectin deficiency Litzman, Clin Exp Immun, 2008 Chalmers, Lancet Respir Med, 2013 IgG subclass deficiency Epithelial sodium channel (ENaC) mutations Fajac, Respir Research,
6 Patients want to know Genetic counseling In two cohort studies, patients received a diagnosis that either resulted in a change in therapy (15%) or potentially would (37%) ABPA CF GERD CVID Pasteur, AJRCCM, 2000 Shoemark, Respir Med, 2007 Among patients who were being cared for by either a pulmonologist or ID specialist and did not have a specific diagnosis N=44 ABPA 1 M. avium complex 2 Alpha-1-PI-ZZ 2 Hyper IgE syndrome 1 Cystic fibrosis 1 Total 7 (16%)* *Two additional probable CF (sweat Chloride >60) One recent confirmation of IgM deficiency with qualitative immunoglobulin defect Ashraf, AJRCCM, 2013 (Abstract) 5
7 Age Younger patients more likely to have a congenital cause CF, primary ciliary dyskinesia, congenital immunodeficiency Prior severe infection Autoimmune disease Sjogren s, RA, ulcerative colitis Paranasal sinus disease ABPA, CF, ciliary dyskinesia, immunodeficiency, Job syndrome (HIES) Fertility problems CF, ciliary dyskinesia, Young s syndrome Certain findings suggestive of specific diagnoses Predominantly upper lobe disease- CF Nodules, tree-in-bud, cavities-ntm Middle lobe/lingula disease- NTM Emphysema-α-1- antitrypsin deficiency Focal disease-endobronchial obstruction 6

8 What is the most likely cause of bronchiectasis in this 26 year old female with a 3 year history of cough and sputum with recent hemoptysis? 1. Allergic bronchopulmonary aspergillosis 2. Severe combined immunodeficiency 3 Cystic fibrosis 4. Primary ciliary dyskinesia 5. Idiopathic 1. Allergic bronchopulmonary aspergillosis 2. Severe combined immunodeficiency 3. Cystic fibrosis 4. Primary ciliary dyskinesia 5. Idiopathic 0% 0% 0% 0% 0%
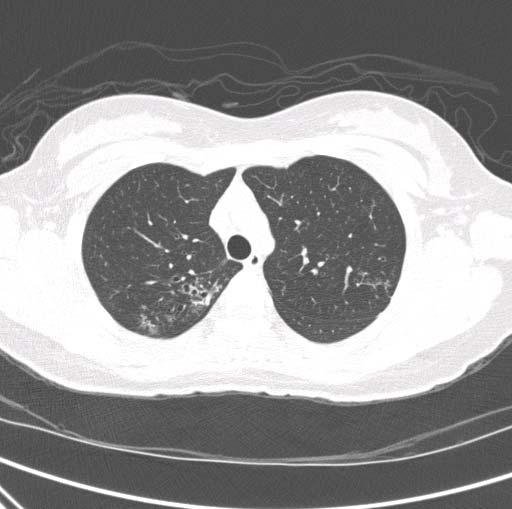

9 8


10 Predominant upper lobe disease Young patient CF must be considered A mutation screen showed her to be heterozygote for ΔF508, with no other mutations What is the next step? 9


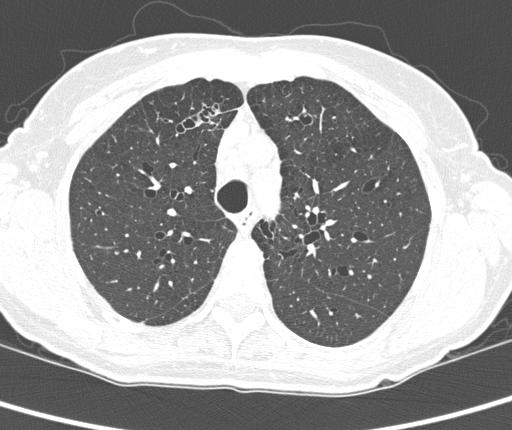
11 What is the most likely cause of bronchiectasis in this 68 year old female? 1. M. avium 2. Idiopathic 3. Alpha-1-anti-trypsin deficiency 4. Cystic fibrosis 5. Common variable immunodeficiency 10
12 1. M. avium 2. Idiopathic 3. Alpha-1-anti-trypsin deficiency 4. Cystic fibrosis 5. Common variable immunodeficiency 0% 0% 0% 0% 0% % of the patients had bronchiectasis High prevalence of CFTR mutations Kim RD, AJRCCM,



13 12

14 13

15 Has been controversial as to how common/clinically significant this is Some studies have shown no increased prevalence in large cohorts of patients with bronchiectasis 14
16 A different picture emerges when one studies a large cohort of α-1-anti-trypsin patients Among 74 Pi-ZZ patients 70 had some bronchiectasis 20 (27%) had at least 3 lung segments involved A bronchiectasis predominant phenotype was identified CT findings of bronchiectasis correlated with: Increased sputum production Increased frequency of exacerbations Lower QOL Parr, AJRCCM, 2007 HRCT of chest PFTs Sputum for bacteria, AFB, fungus CBC with differential Quantitative Immunoglobulins IgG, IgA, IgM IgE level Metersky, Clin Chest Med,
17 α-1-anti-trypsin level CF screening Sweat chloride or Nasal potential difference or CF mutation screen Metersky, Clin Chest Med, 2012 Aspergillus-specific IgG, IgE and/or skin testing Bronchoscopy (focal disease, NTM suspected) Ciliary biopsy, nasal nitric oxide Immunologic evaluation Serologies for autoimmune disease Metersky, Clin Chest Med,
18 Determining etiology often leads to changes in therapy Systematic evaluation recommended Nonetheless, this evaluation should be tailored to the specific patient being evaluated Therapeutic approach for bronchiectasis is not highly evidence-based BTS guidelines, largely expert opinion-based We will discuss potential treatment options I will then reveal what I did and the results (good and bad) I hope to prompt spirited discussion 17


19 A 58 year old female pediatrician is referred in 2012 for evaluation after a chest radiograph and subsequent CT are found to be abnormal She has had a few respiratory tract infections over the years Her only complaint is a bothersome dry cough, persistent over years, but recently worse She worries about its effect on her patients perception of her She is very physically active and otherwise feels well Nothing to suggest GERD 18

20 Her physical examination is unrevealing Her PFTs are supernormal Laboratory testing for the usual suspects is unrevealing She is unable to produce a sputum sample Bronchoscopy reveals no secretions and the corrugation pattern associated with Mounier-Kuhn No organisms of any type are cultured 19
21 What would you provide her for treatment? 1. Nothing, she is doing well 2. Airway clearance regimen, eg. with Acapella 3. Chronic macrolide therapy 4. Empiric treatment for GERD 5. Hypertonic saline nebulization 6. Other intervention 1. Nothing, she is doing well 2. Airway clearance regimen, eg. with Acapella 3. Chronic macrolide therapy 4. Empiric treatment for GERD 5. Hypertonic saline nebulization 6. Other intervention 0% 0% 0% 0% 0% 0%

22 She began treatment with Azithromycin, 250 mg TIW Returns 3 months later Cough 50-75% improved Coworkers spontaneously note her improved cough, not knowing she was on therapy Had to stop temporarily secondary to vaginal candidiasis, Sx worsened and improved with restart 21


23 Wu, Respirology, 2014 A 53 year old female is referred for bronchiectasis in 2003 She has been coughing 1-2 teaspoons of variably colored sputum daily for several years Exacerbations 1-2 times a year characterized by fever, chest pain and increased purulence Each responds quickly to oral antibiotics No systemic complaints She is active, works full time Physical examination, laboratory testing unrevealing PFTs normal She grows pan-sensitive Pseudomonas only She is prescribed a flutter valve and uses it intermittently 22
 3. Inhaled hypertonic saline 4. High frequency chest wall oscillation 5.")
24 What additional therapies would you have prescribed (2003, pre-macrolide era)? 1. Nothing, she is doing well 2. Inhaled tobramycin (2003, other options now) 3. Inhaled hypertonic saline 4. High frequency chest wall oscillation 5. Attempt at eradication of Pseudomonas 23

25 1. Nothing, she is doing well 2. Inhaled tobramycin (2003, other options now) 3. Inhaled hypertonic saline 4. High frequency chest wall oscillation 5. Attempt at eradication of Pseudomonas 0% 0% 0% 0% 0% She is now 66, happily retired We tried azithromycin, no benefit, so stopped Still coughs 1-2 teaspoons a day, usually green Still 1-2 exacerbations a year, quickly respond to levofloxacin (although now intermediate sensitivity in vitro) PFTs stable Grew MAC once, not subsequently Overall, no change in almost 12 years, essentially without therapy Would her QOL be better with inhaled antibiotics? 24
26 Aztreonam for inhalation solution in patients with non-cystic fibrosis bronchiectasis (AIR-BX1 and AIR-BX2): two randomized double-blind, placebo-controlled phase 3 trials No clinically significant benefit Increased treatment-related adverse events and discontinuations in aztreonam group Lancet Respir Med, 2014 Inhaled colistin in patients with bronchiectasis and chronic Pseudomonas aeruginosa infection Failed to reach primary endpoint (exacerbation rate), although significant decrease in the most compliant patients Clinically significant improvement in SGRQ Haworth, AJRCCM,
27 Dry powder ciprofloxacin Met primary endpoint of time to exacerbation in Phase 3 study in 14 day on and 14 day off arm, not 28 day arm De Soyza, CHEST, 2016 (Abstract only) Liposomal ciprofloxacin preparation Met time to exacerbation endpoint in one Phase 3 study, not the other. Aradigm Press release 69 year old male self-referred with long history of bronchiectasis Sputum grows MSSA and MAC Never grows MAC again Next seen 2 years later (he has a primary pulmonologist) 26

28 Sputum production has increased Grows MSSA/Pseudomonas on multiple cultures over the next year. About 3 exacerbations a year characterized by increased sputum without systemic complaints Using Acapella BID Respond well to levofloxacin Condition is quite similar to patient in case 2 except: His girlfriend wants to be more proactive 27
29 Enrolled in inhaled mannitol study No obvious benefit Grows Pseudomonas repeatedly What would you do next? 1. Start TIW azithromycin (it has been 4 years since he grew MAC) 2. Switch from Acapella to HFCWO 3. Start inhaled antibiotic 4. Start inhaled hypertonic saline 28
30 1. Start TIW azithromycin (it has been 4 years since he grew MAC) 2. Switch from Acapella to HFCWO 3. Start inhaled antibiotic 4. Start inhaled hypertonic saline 0% 0% 0% 0% Started on inhaled tobramycin Chronic sputum production completely remits Life changing Creatinine increases from 0.9 to 1.4 Switched to inhaled aztreonam Develops diffuse papular rash within several days Try to enroll him in liposomal cipro study Grows MSSA only, so is a screen failure Currently doing well on Augmentin 10 days each month 29
31 When to escalate to high frequency chest wall oscillation from Acapella/Flutter, etc? When to start nebulized antibiotics? When to consider hypertonic saline? When to STOP azithromycin in patients who do not appear to have responded? 30
Bronchiectasis: An Imaging Approach
 Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Evaluation of Patients with Diffuse Bronchiectasis
 Evaluation of Patients with Diffuse Bronchiectasis Dr. Patricia Eshaghian, MD Assistant Clinical Professor of Medicine Director, UCLA Adult Cystic Fibrosis Affiliate Program UCLA Division of Pulmonary
Evaluation of Patients with Diffuse Bronchiectasis Dr. Patricia Eshaghian, MD Assistant Clinical Professor of Medicine Director, UCLA Adult Cystic Fibrosis Affiliate Program UCLA Division of Pulmonary
Bronchiectasis. What is bronchiectasis? What causes bronchiectasis?
 This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
Bronchiectasis. Grant Waterer. Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago
 Bronchiectasis Grant Waterer MBBS PhD MBA FRACP FCCP Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago Conflicts of Interest I have
Bronchiectasis Grant Waterer MBBS PhD MBA FRACP FCCP Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago Conflicts of Interest I have
Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX
 Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX Pioneer of Respiratory Medicine 2016 marked 200th anniversary of his
Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX Pioneer of Respiratory Medicine 2016 marked 200th anniversary of his
NON-CF BRONCHIECTASIS IN ADULTS
 Séminaire de Pathologie Infectieuse Jeudi 25 juin 2008 Cliniques Universitaires UCL de Mont-Godinne, Yvoir NON-CF BRONCHIECTASIS IN ADULTS Dr Robert Wilson Royal Brompton Hospital, London, UK Aetiology
Séminaire de Pathologie Infectieuse Jeudi 25 juin 2008 Cliniques Universitaires UCL de Mont-Godinne, Yvoir NON-CF BRONCHIECTASIS IN ADULTS Dr Robert Wilson Royal Brompton Hospital, London, UK Aetiology
Dr Conroy Wong. Professor Richard Beasley. Dr Sarah Mooney. Professor Innes Asher
 Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
CCLI. Bronchiectasis Treatment Antibiotics. Charles Haworth. Physician / Patient Conference, Georgetown University, May 2017
 Physician / Patient Conference, Georgetown University, May 2017 Bronchiectasis Treatment Antibiotics Charles Haworth CCLI Cambridge Centre for Lung Infection Disclosures Educational talks and / or consultancy
Physician / Patient Conference, Georgetown University, May 2017 Bronchiectasis Treatment Antibiotics Charles Haworth CCLI Cambridge Centre for Lung Infection Disclosures Educational talks and / or consultancy
Bronchiectasis. Examples include: Viral infections (measles, adenovirus, influenza)
") Bronchiectasis What is Bronchiectasis? Bronchiectasis (pronounced bron-kee-ek'-tas-is) is a condition of the airways in the lungs. These airways (bronchial tubes) are tubelike structures that branch from
Bronchiectasis What is Bronchiectasis? Bronchiectasis (pronounced bron-kee-ek'-tas-is) is a condition of the airways in the lungs. These airways (bronchial tubes) are tubelike structures that branch from
Bronchiectasis in Adults - Suspected
 Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
How To Assess Severity and Prognosis
 How To Assess Severity and Prognosis Gregory Tino, M.D. Chief, Department of Medicine Penn Presbyterian Medical Center Associate Professor of Medicine Perelman School of Medicine at the University of Pennsylvania
How To Assess Severity and Prognosis Gregory Tino, M.D. Chief, Department of Medicine Penn Presbyterian Medical Center Associate Professor of Medicine Perelman School of Medicine at the University of Pennsylvania
Chronic suppurative lung disease in adults
 Case Report Chronic suppurative lung disease in adults Mark L. Metersky 1, Antranik Mangardich 2 1 Division of Pulmonary and Critical Care Medicine, University of Connecticut School of Medicine, Farmington,
Case Report Chronic suppurative lung disease in adults Mark L. Metersky 1, Antranik Mangardich 2 1 Division of Pulmonary and Critical Care Medicine, University of Connecticut School of Medicine, Farmington,
C.S. HAWORTH 1, A. WANNER 2, J. FROEHLICH 3, T. O'NEAL 3, A. DAVIS 4, I. GONDA 3, A. O'DONNELL 5
 Inhaled Liposomal Ciprofloxacin in Patients With Non-Cystic Fibrosis Bronchiectasis and Chronic Pseudomonas aeruginosa: Results From Two Parallel Phase III Trials (ORBIT-3 and -4) C.S. HAWORTH 1, A. WANNER
Inhaled Liposomal Ciprofloxacin in Patients With Non-Cystic Fibrosis Bronchiectasis and Chronic Pseudomonas aeruginosa: Results From Two Parallel Phase III Trials (ORBIT-3 and -4) C.S. HAWORTH 1, A. WANNER
NTM AND BRONCHIECTASIS (BXSIS): THE CHICKEN AND THE EGG
: THE CHICKEN AND THE EGG") REMINGTON WINTER COURSE IN ID VAIL, CO FEBRUARY, 2010 NONTUBERCULOSIS MYCOBACTERIA AND BRONCHIECTASIS: Revised 1/28/10 10:31 AM- CQ MICHAEL D. ISEMAN, MD OR In some cases NTMs invade pre-existing BXSIS
REMINGTON WINTER COURSE IN ID VAIL, CO FEBRUARY, 2010 NONTUBERCULOSIS MYCOBACTERIA AND BRONCHIECTASIS: Revised 1/28/10 10:31 AM- CQ MICHAEL D. ISEMAN, MD OR In some cases NTMs invade pre-existing BXSIS
Cystic Fibrosis the future
 Cystic Fibrosis the future Pathophysiologic cascade Abnormal Gene Abnormal CFTR Therapy Gene replacement Protein replacement Gene read through therapy Abnormal sodium chloride & water movement through
Cystic Fibrosis the future Pathophysiologic cascade Abnormal Gene Abnormal CFTR Therapy Gene replacement Protein replacement Gene read through therapy Abnormal sodium chloride & water movement through
Bronchiectasis Domiciliary treatment. Prof. Adam Hill Royal Infirmary and University of Edinburgh
 Bronchiectasis Domiciliary treatment Prof. Adam Hill Royal Infirmary and University of Edinburgh Plan of talk Background of bronchiectasis Who requires IV antibiotics Domiciliary treatment Results to date.
Bronchiectasis Domiciliary treatment Prof. Adam Hill Royal Infirmary and University of Edinburgh Plan of talk Background of bronchiectasis Who requires IV antibiotics Domiciliary treatment Results to date.
Non Cystic Fibrosis Bronchiectasis: How to Proceed?
 Non Cystic Fibrosis Bronchiectasis: How to Proceed? Dr Ankit Parakh MD, DNB, MNAMS, RCPCH Fellow (UK), European Diplomate of Pediatric Respiratory Medicine ERS Fellowship Pediatric Medicine & NIV (GOSH,
Non Cystic Fibrosis Bronchiectasis: How to Proceed? Dr Ankit Parakh MD, DNB, MNAMS, RCPCH Fellow (UK), European Diplomate of Pediatric Respiratory Medicine ERS Fellowship Pediatric Medicine & NIV (GOSH,
2018 Vindico Medical Education. Non-tuberculous Mycobacteria: Circumventing Difficulties in Diagnosis and Treatment
 Activity presentations are considered intellectual property. These slides may not be published or posted online without permission from Vindico Medical Education (cme@vindicocme.com). Please be respectful
Activity presentations are considered intellectual property. These slides may not be published or posted online without permission from Vindico Medical Education (cme@vindicocme.com). Please be respectful
Nontuberculous Mycobacterial Lung Disease
 Non-TB Mycobacterial Disease Jeffrey P. Kanne, MD Nontuberculous Mycobacterial Lung Disease Jeffrey P. Kanne, M.D. Consultant Disclosures Perceptive Informatics Royalties (book author) Amirsys, Inc. Wolters
Non-TB Mycobacterial Disease Jeffrey P. Kanne, MD Nontuberculous Mycobacterial Lung Disease Jeffrey P. Kanne, M.D. Consultant Disclosures Perceptive Informatics Royalties (book author) Amirsys, Inc. Wolters
CYSTIC FIBROSIS OBJECTIVES NO CONFLICT OF INTEREST TO DISCLOSE
 CYSTIC FIBROSIS Madhu Pendurthi MD MPH Staff Physician, Mercy Hospital Springfield, MO NO CONFLICT OF INTEREST TO DISCLOSE OBJECTIVES Epidemiology of Cystic Fibrosis (CF) Genetic basis and pathophysiology
CYSTIC FIBROSIS Madhu Pendurthi MD MPH Staff Physician, Mercy Hospital Springfield, MO NO CONFLICT OF INTEREST TO DISCLOSE OBJECTIVES Epidemiology of Cystic Fibrosis (CF) Genetic basis and pathophysiology
Nontuberculous Mycobacteria (NTM) in Patients with Cystic Fibrosis
 in Patients with Cystic Fibrosis") Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/cystic-fibrosis-in-focus/nontuberculous-mycobacteria-ntm-in-patientswith-cystic-fibrosis/8337/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/cystic-fibrosis-in-focus/nontuberculous-mycobacteria-ntm-in-patientswith-cystic-fibrosis/8337/
A Place For Airway Clearance Therapy In Today s Healthcare Environment
 A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
What is Cystic Fibrosis? CYSTIC FIBROSIS. Genetics of CF
 What is Cystic Fibrosis? CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Chronic, progressive and life limiting autosomal recessive genetic disease characterized by chronic
What is Cystic Fibrosis? CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Chronic, progressive and life limiting autosomal recessive genetic disease characterized by chronic
Update on bronchiectasis guidelines. James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK
 Update on bronchiectasis guidelines James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK University of Dundee Bronchiectasis guidelines 2017 2010 2006 2008 2015 2015 Currently valid guidelines
Update on bronchiectasis guidelines James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK University of Dundee Bronchiectasis guidelines 2017 2010 2006 2008 2015 2015 Currently valid guidelines
Management of bronchiectasis in adults
 STATE OF THE ART MANAGEMENT OF BRONCHIECTASIS IN ADULTS Management of bronchiectasis in adults James D. Chalmers 1, Stefano Aliberti 2 and Francesco Blasi 3 Affiliations: 1 Tayside Respiratory Research
STATE OF THE ART MANAGEMENT OF BRONCHIECTASIS IN ADULTS Management of bronchiectasis in adults James D. Chalmers 1, Stefano Aliberti 2 and Francesco Blasi 3 Affiliations: 1 Tayside Respiratory Research
Bronchiectasis. Introduction. Key points
 15 Bronchiectasis Introduction i Key points Patients with bronchiectasis typically have chronic airway infection, punctuated by acute exacerbations and accompanied by progressive airflow obstruction. Bronchiectasis
15 Bronchiectasis Introduction i Key points Patients with bronchiectasis typically have chronic airway infection, punctuated by acute exacerbations and accompanied by progressive airflow obstruction. Bronchiectasis
Cystic Fibrosis Care Guidelines for Challenging Cystic Fibrosis
 Cystic Fibrosis Care Guidelines for Challenging Cystic Fibrosis APRIL 2018 Authors Steve Kent MD, CF Clinic Director, Victoria General Hospital (VGH), Victoria Mark Chilvers MD, CF Clinic Director, B.C.
Cystic Fibrosis Care Guidelines for Challenging Cystic Fibrosis APRIL 2018 Authors Steve Kent MD, CF Clinic Director, Victoria General Hospital (VGH), Victoria Mark Chilvers MD, CF Clinic Director, B.C.
For Those Who Lover Sputum: Bronchiectasis
 For Those Who Lover Sputum: Bronchiectasis Douglas B. Hornick, MD Pulmonologist w/ an Infectious Attitude Division of Pulmonary/Critical Care & Occ Med Carver UI College of Medicine Objectives Increase
For Those Who Lover Sputum: Bronchiectasis Douglas B. Hornick, MD Pulmonologist w/ an Infectious Attitude Division of Pulmonary/Critical Care & Occ Med Carver UI College of Medicine Objectives Increase
Nontuberculous Mycobacteria (NTM)
") Nontuberculous Mycobacteria (NTM) Bacteria, like plants and animals, have been classified into similar groups. The groups are called "families." One such family of bacteria is known as the Mycobacteriaceae.
Nontuberculous Mycobacteria (NTM) Bacteria, like plants and animals, have been classified into similar groups. The groups are called "families." One such family of bacteria is known as the Mycobacteriaceae.
Overview of Cystic fibrosis in children. Apeksha Sathyaprasad, MD Pediatric pulmonologist
 Overview of Cystic fibrosis in children Apeksha Sathyaprasad, MD Pediatric pulmonologist No conflicts of interest OBJECTIVES Review pathophysiology of pulmonary disease in cystic fibrosis Review diagnostic
Overview of Cystic fibrosis in children Apeksha Sathyaprasad, MD Pediatric pulmonologist No conflicts of interest OBJECTIVES Review pathophysiology of pulmonary disease in cystic fibrosis Review diagnostic
Diagnostic Evaluation of NTM and Bronchiectasis
 Division of Pulmonary, Critical Care and Sleep Medicine Diagnostic Evaluation of NTM and Bronchiectasis Ashwin Basavaraj, MD, FCCP NTM patient education program November 9, 2016 Involves a combination
Division of Pulmonary, Critical Care and Sleep Medicine Diagnostic Evaluation of NTM and Bronchiectasis Ashwin Basavaraj, MD, FCCP NTM patient education program November 9, 2016 Involves a combination
Cystic Fibrosis: Progress in Treatment Management. Patrick A. Flume, M.D. Medical University of South Carolina
 Cystic Fibrosis: Progress in Treatment Management Patrick A. Flume, M.D. Medical University of South Carolina Disclosures Grant support Mpex Pharmaceuticals, Inc Gilead Sciences, Inc Bayer Healthcare AG
Cystic Fibrosis: Progress in Treatment Management Patrick A. Flume, M.D. Medical University of South Carolina Disclosures Grant support Mpex Pharmaceuticals, Inc Gilead Sciences, Inc Bayer Healthcare AG
4.6 Small airways disease
 4.6 Small airways disease Author: Jean-Marc Fellrath 1. INTRODUCTION Small airways are defined as any non alveolated and noncartilaginous airway that has an internal diameter of 2 mm. Several observations
4.6 Small airways disease Author: Jean-Marc Fellrath 1. INTRODUCTION Small airways are defined as any non alveolated and noncartilaginous airway that has an internal diameter of 2 mm. Several observations
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
INHALED ANTIBIOTICS THERAPY IN NON-CF LUNG DISEASE
 INHALED ANTIBIOTICS THERAPY IN NON-CF LUNG DISEASE Hannah Blau MBBS Pulmonary Institute and Graub CF Center SCHNEIDER CHILDREN S MEDICAL CENTER OF ISRAEL Chipap 18 th February 2015 Inhaled antibiotic therapy:
INHALED ANTIBIOTICS THERAPY IN NON-CF LUNG DISEASE Hannah Blau MBBS Pulmonary Institute and Graub CF Center SCHNEIDER CHILDREN S MEDICAL CENTER OF ISRAEL Chipap 18 th February 2015 Inhaled antibiotic therapy:
Inhaled Antibiotics in Non-CF. Dr Michael Loebinger Host Defence Unit Royal Brompton Hospital London, United Kingdom
 Inhaled Antibiotics in Non-CF Dr Michael Loebinger Host Defence Unit Royal Brompton Hospital London, United Kingdom Advantages Increased drug concentrations locally Reduced systemic adverse effects Home
Inhaled Antibiotics in Non-CF Dr Michael Loebinger Host Defence Unit Royal Brompton Hospital London, United Kingdom Advantages Increased drug concentrations locally Reduced systemic adverse effects Home
Bronchiectasis exacerbations; differences and management. Michael Loebinger Royal Brompton Imperial College
 Bronchiectasis exacerbations; differences and management Michael Loebinger Royal Brompton Imperial College Plan Bronchiectasis background and burden Exacerbation and Management Longer term Management Cases
Bronchiectasis exacerbations; differences and management Michael Loebinger Royal Brompton Imperial College Plan Bronchiectasis background and burden Exacerbation and Management Longer term Management Cases
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
Efficacy of Pseudomonas aeruginosa eradication regimens in bronchiectasis
 Efficacy of Pseudomonas aeruginosa eradication regimens in bronchiectasis Vallières, E., Tumelty, K., Tunney, M. M., Hannah, R., Hewitt, O., Elborn, J. S., & Downey, D. G. (2017). Efficacy of Pseudomonas
Efficacy of Pseudomonas aeruginosa eradication regimens in bronchiectasis Vallières, E., Tumelty, K., Tunney, M. M., Hannah, R., Hewitt, O., Elborn, J. S., & Downey, D. G. (2017). Efficacy of Pseudomonas
Cystic Fibrosis Panel Applications (Dornase Alfa) Contents
 Contents") Cystic Fibrosis Panel Applications (Dornase Alfa) Contents Page 2-4: Entry and Stopping Criteria for Treatment with Dornase Alfa Page 5-9: Application and consent forms for a one month trail and long term
Cystic Fibrosis Panel Applications (Dornase Alfa) Contents Page 2-4: Entry and Stopping Criteria for Treatment with Dornase Alfa Page 5-9: Application and consent forms for a one month trail and long term
Understanding the heterogeneity of the disease
 Symposium: Bronchiectasis in Europe: an update from the European Bronchiectasis Network (EMBARC) Understanding the heterogeneity of the disease Stefano Aliberti Health Science Department University of
Symposium: Bronchiectasis in Europe: an update from the European Bronchiectasis Network (EMBARC) Understanding the heterogeneity of the disease Stefano Aliberti Health Science Department University of
Fungal (Aspergillus and Candida) infections in Cystic fibrosis
 infections in Cystic fibrosis") Fungal (Aspergillus and Candida) infections in Cystic fibrosis Malena Cohen-Cymberknoh, MD CF Center Hadassah-Hebrew University Medical Center Jerusalem, Israel Israeli Annual CF Conference, Herzlyia,
Fungal (Aspergillus and Candida) infections in Cystic fibrosis Malena Cohen-Cymberknoh, MD CF Center Hadassah-Hebrew University Medical Center Jerusalem, Israel Israeli Annual CF Conference, Herzlyia,
Pulmonary Exacerbations:
 Pulmonary Exacerbations: Better Understanding Needed Michael Tracy, MD Clinical Assistant Professor Pediatric Pulmonary CF Pulmonary Exacerbations Definition Importance Causes Treatment Research opportunities
Pulmonary Exacerbations: Better Understanding Needed Michael Tracy, MD Clinical Assistant Professor Pediatric Pulmonary CF Pulmonary Exacerbations Definition Importance Causes Treatment Research opportunities
How Do I Manage Nontuberculous Mycobacterial (NTM) Lung Disease Patients?
 Lung Disease Patients?") How Do I Manage Nontuberculous Mycobacterial (NTM) Lung Disease Patients? David E. Griffith, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Potential COI Statement I was a
How Do I Manage Nontuberculous Mycobacterial (NTM) Lung Disease Patients? David E. Griffith, M.D. Professor of Medicine University of Texas Health Science Center, Tyler Potential COI Statement I was a
BTS Guideline for non-cf Bronchiectasis
 ISSN 2040-2023 July 2010 BTS Guideline for non-cf Bronchiectasis A Quick Reference Guide British Thoracic Society www.brit-thoracic.org.uk BTS GUIDELINE FOR NON-CF BRONCHIECTASIS A QUICK REFERENCE GUIDE
ISSN 2040-2023 July 2010 BTS Guideline for non-cf Bronchiectasis A Quick Reference Guide British Thoracic Society www.brit-thoracic.org.uk BTS GUIDELINE FOR NON-CF BRONCHIECTASIS A QUICK REFERENCE GUIDE
EMBARC Baseline v3.0 April_2016 1
 Essential Data is data which is deemed by the study team as crucial in achieving the objectives of the registry. Specifying an essential data set does not imply in any way the additional data points are
Essential Data is data which is deemed by the study team as crucial in achieving the objectives of the registry. Specifying an essential data set does not imply in any way the additional data points are
Inhalational antibacterial regimens in non-cystic fibrosis patients. Jeff Alder Bayer HealthCare
 Inhalational antibacterial regimens in non-cystic fibrosis patients Jeff Alder Bayer HealthCare Alder - Inhaled therapy for non-cf - EMA 25-26 Oct 2012 1 Inhalational antibacterials: two approaches 1.
Inhalational antibacterial regimens in non-cystic fibrosis patients Jeff Alder Bayer HealthCare Alder - Inhaled therapy for non-cf - EMA 25-26 Oct 2012 1 Inhalational antibacterials: two approaches 1.
Cystic Fibrosis Foundation Patient Registry 2013
 5/9/2015 Targeting CFTR to Treat Cystic Fibrosis: Small Molecule Therapy Mary Ellen Kleinhenz, MD Director, UCSF Adult Cystic Fibrosis Program Professor of Medicine UCSF Division of Pulmonary, Critical
5/9/2015 Targeting CFTR to Treat Cystic Fibrosis: Small Molecule Therapy Mary Ellen Kleinhenz, MD Director, UCSF Adult Cystic Fibrosis Program Professor of Medicine UCSF Division of Pulmonary, Critical
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Chronic Obstructive Pulmonary Disease (COPD Emphysema, Chronic Bronchitis) Bronchiectasis Smoking Related Problems Lung Cancer Screening
 Bronchiectasis Smoking Related Problems Lung Cancer Screening") Chest, Lung & COPD Chest, Lung & COPD Do you have difficulty breathing? Shortness of breath? Even COPD? Our experts can find the exact problem so you can breathe easier. Here s a guide if you would like
Chest, Lung & COPD Chest, Lung & COPD Do you have difficulty breathing? Shortness of breath? Even COPD? Our experts can find the exact problem so you can breathe easier. Here s a guide if you would like
Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c)
 Diffuse bronchiectasis b) Cystic fibrosis c)") Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c) Bronchiolitis obliterans d) Complicated acute pneumonia e)
Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c) Bronchiolitis obliterans d) Complicated acute pneumonia e)
Cystic Fibrosis. Cystic Fibrosis. Cystic Fibrosis 5/01/2011 CYSTIC FIBROSIS OF THE PANCREAS AND ITS RELATION TO CELIAC DISEASE. D ANDERSEN.
 1938 OF THE PANCREAS AND ITS RELATION TO CELIAC DISEASE. D ANDERSEN. American Journal Diseases Children. : The beginning May 1938: 49 cases 25 20 15 Nos of cases 10 5 0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 Age
1938 OF THE PANCREAS AND ITS RELATION TO CELIAC DISEASE. D ANDERSEN. American Journal Diseases Children. : The beginning May 1938: 49 cases 25 20 15 Nos of cases 10 5 0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 Age
Cystic Fibrosis. Jennifer McDaniel, BS, RRT-NPS
 Cystic Fibrosis Jennifer McDaniel, BS, RRT-NPS Overview Cystic fibrosis is the most common fatal, inherited disease in the U. S. CF results from a defective autosomal recessive gene One copy of gene =
Cystic Fibrosis Jennifer McDaniel, BS, RRT-NPS Overview Cystic fibrosis is the most common fatal, inherited disease in the U. S. CF results from a defective autosomal recessive gene One copy of gene =
Rhinosinusitis: Current Concepts. Frederick S. Rosen, MD Matthew Ryan, MD
 Rhinosinusitis: Current Concepts Frederick S. Rosen, MD Matthew Ryan, MD Introduction 2 Introduction The medical condition most commonly reported by US Census Department Major Factors: Facial pain/pressure,
Rhinosinusitis: Current Concepts Frederick S. Rosen, MD Matthew Ryan, MD Introduction 2 Introduction The medical condition most commonly reported by US Census Department Major Factors: Facial pain/pressure,
Clinical Study Synopsis
 Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Alpha-1 Antitrypsin Deficiency Alpha-1 Lung Disease
 Alpha-1 Antitrypsin Deficiency Alpha-1 Lung Disease Chronic obstructive pulmonary disease (COPD) affects millions of people each year. Chronic means long term, obstructive means it is hard to get air in
Alpha-1 Antitrypsin Deficiency Alpha-1 Lung Disease Chronic obstructive pulmonary disease (COPD) affects millions of people each year. Chronic means long term, obstructive means it is hard to get air in
Goals Basic defect Pathophysiology Clinical i l signs and symptoms Therapy
 CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Goals Basic defect Pathophysiology Clinical i l signs and symptoms Therapy What is Cystic Fibrosis? Chronic, progressive
CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Goals Basic defect Pathophysiology Clinical i l signs and symptoms Therapy What is Cystic Fibrosis? Chronic, progressive
JUERGEN FROEHLICH, JANICE DAHMS, DAVID CIPOLLA,
 Reduction in Frequency of Pulmonary Exacerbations With Inhaled ARD-315 in Non-Cystic Fibrosis Bronchiectasis (NCFB) Patients is Independent of Pseudomonas aeruginosa Susceptibility at Baseline JUERGEN
Reduction in Frequency of Pulmonary Exacerbations With Inhaled ARD-315 in Non-Cystic Fibrosis Bronchiectasis (NCFB) Patients is Independent of Pseudomonas aeruginosa Susceptibility at Baseline JUERGEN
Recent advances in diagnosis and management of ABPA. Arindam SR(Pulmonary Medicine)
") Recent advances in diagnosis and management of ABPA Arindam SR(Pulmonary Medicine) Conventional diagnostic criteria for ABPA Primary Episodic bronchial obstruction (asthma) Peripheral blood eosinophilia
Recent advances in diagnosis and management of ABPA Arindam SR(Pulmonary Medicine) Conventional diagnostic criteria for ABPA Primary Episodic bronchial obstruction (asthma) Peripheral blood eosinophilia
Bronchiectasis it s effects on the NZ population and what we can do to address this
 NZ Respiratory Conference - 2017 Bronchiectasis it s effects on the NZ population and what we can do to address this Conroy Wong Middlemore Hospital Auckland, NZ Bronchiectasis in NZ and new developments
NZ Respiratory Conference - 2017 Bronchiectasis it s effects on the NZ population and what we can do to address this Conroy Wong Middlemore Hospital Auckland, NZ Bronchiectasis in NZ and new developments
RADIOLOGIC EVALUATION OF PULMONARY NTM INFECTION. Tilman Koelsch, MD National Jewish Health - Department of Radiology
 Pr N op ot e fo rty rr o f ep Pr ro es du en ct te io r n RADIOLOGIC EVALUATION OF PULMONARY NTM INFECTION Tilman Koelsch, MD National Jewish Health - Department of Radiology Disclosures None Goals Identify
Pr N op ot e fo rty rr o f ep Pr ro es du en ct te io r n RADIOLOGIC EVALUATION OF PULMONARY NTM INFECTION Tilman Koelsch, MD National Jewish Health - Department of Radiology Disclosures None Goals Identify
Northumbria Healthcare NHS Foundation Trust. Bronchiectasis. Issued by Respiratory Medicine
 Northumbria Healthcare NHS Foundation Trust Bronchiectasis Issued by Respiratory Medicine The aim of this booklet is to help you manage your bronchiectasis. It contains information which you should find
Northumbria Healthcare NHS Foundation Trust Bronchiectasis Issued by Respiratory Medicine The aim of this booklet is to help you manage your bronchiectasis. It contains information which you should find
COPD Bronchiectasis Overlap Syndrome.
 COPD Bronchiectasis Overlap Syndrome. John R Hurst 1, J Stuart Elborn 2, and Anthony De Soyza 3 on Behalf of the BRONCH-UK Consortium (D Bilton, J Bradley, JS Brown, J Duckers, F Copeland, A Floto, J Foweraker,
COPD Bronchiectasis Overlap Syndrome. John R Hurst 1, J Stuart Elborn 2, and Anthony De Soyza 3 on Behalf of the BRONCH-UK Consortium (D Bilton, J Bradley, JS Brown, J Duckers, F Copeland, A Floto, J Foweraker,
Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis
 Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
PEARLS IN PULMONARY MEDICINE. Kellie R. Jones, MD Associate Professor University of Oklahoma Health Sciences Center
 PEARLS IN PULMONARY MEDICINE Kellie R. Jones, MD Associate Professor University of Oklahoma Health Sciences Center Case 1 While moonlighting in the ER, you are asked to evaluate a lady for shortness of
PEARLS IN PULMONARY MEDICINE Kellie R. Jones, MD Associate Professor University of Oklahoma Health Sciences Center Case 1 While moonlighting in the ER, you are asked to evaluate a lady for shortness of
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
US FDA approved ARIKAYCE (amikacin liposome inhalation suspension) antibacterial drug to treat a serious lung disease approved on 28 th Sept 2018
 antibacterial drug to treat a serious lung disease approved on 28 th Sept 2018") US FDA approved ARIKAYCE (amikacin liposome inhalation suspension) antibacterial drug to treat a serious lung disease approved on 28 th Sept 2018 Lung Infection due to MAC Burden Lung Infection Signs &
US FDA approved ARIKAYCE (amikacin liposome inhalation suspension) antibacterial drug to treat a serious lung disease approved on 28 th Sept 2018 Lung Infection due to MAC Burden Lung Infection Signs &
Respiratory Pharmacology: Treatment of Cystic Fibrosis
 Respiratory Pharmacology: Treatment of Cystic Fibrosis Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
Respiratory Pharmacology: Treatment of Cystic Fibrosis Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
A review of Cystic Fibrosis
 A review of Cystic Fibrosis Jennifer Landry md F.R.C.P.(C) Pulmonary & Critical Care Medicine McGill University Health Center Cystic Fibrosis One of the most common lethal inherited AR disorders in the
A review of Cystic Fibrosis Jennifer Landry md F.R.C.P.(C) Pulmonary & Critical Care Medicine McGill University Health Center Cystic Fibrosis One of the most common lethal inherited AR disorders in the
Imaging Small Airways Diseases: Not Just Air trapping. Eric J. Stern MD University of Washington
 Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
SCLERODERMA LUNG DISEASE: WHAT THE PATIENT SHOULD KNOW
 SCLERODERMA LUNG DISEASE: WHAT THE PATIENT SHOULD KNOW Lung disease can be a serious complication of scleroderma. The two most common types of lung disease in patients with scleroderma are interstitial
SCLERODERMA LUNG DISEASE: WHAT THE PATIENT SHOULD KNOW Lung disease can be a serious complication of scleroderma. The two most common types of lung disease in patients with scleroderma are interstitial
The team. Medical staff Dr Adam Hill Vacant post- Dr Lithgow Dr Ruzanna Frangulyan Specialist Trainee
 Bronchiectasis The team Medical staff Dr Adam Hill Vacant post- Dr Lithgow Dr Ruzanna Frangulyan Specialist Trainee Specialist staff Kim Turnbull Denise Gillian Jenny Scott Jo Pentland Research nurses
Bronchiectasis The team Medical staff Dr Adam Hill Vacant post- Dr Lithgow Dr Ruzanna Frangulyan Specialist Trainee Specialist staff Kim Turnbull Denise Gillian Jenny Scott Jo Pentland Research nurses
Rayos Prior Authorization Program Summary
 Rayos Prior Authorization Program Summary FDA APPROVED INDICATIONS AND DOSAGE FDA-Approved Indications: 1 Agent Indication Dosage Rayos (prednisone delayedrelease tablet) as an anti-inflammatory or immunosuppressive
Rayos Prior Authorization Program Summary FDA APPROVED INDICATIONS AND DOSAGE FDA-Approved Indications: 1 Agent Indication Dosage Rayos (prednisone delayedrelease tablet) as an anti-inflammatory or immunosuppressive
British Thoracic Society Guidelines for Bronchiectasis in adults. Available for public consultation from 13 March 2018 to 16 April 2018
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 British Thoracic Society Guidelines for Bronchiectasis in adults On behalf of the BTS Bronchiectasis in adults Guideline Development Group Available for public consultation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 British Thoracic Society Guidelines for Bronchiectasis in adults On behalf of the BTS Bronchiectasis in adults Guideline Development Group Available for public consultation
Nontuberculous Mycobacteria
 Nontuberculous Mycobacteria Epidemiology and Clinical Management Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health and Preventive Medicine Oregon Health &
Nontuberculous Mycobacteria Epidemiology and Clinical Management Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health and Preventive Medicine Oregon Health &
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
Historical perspective
 Bronchiectasis Dilated airways with frequently thickened walls Faculty/Presenter Disclosure Faculty: Dr. Alan Kaplan Relationships with commercial interests (12 months) Grants/research support: N/A Speakers
Bronchiectasis Dilated airways with frequently thickened walls Faculty/Presenter Disclosure Faculty: Dr. Alan Kaplan Relationships with commercial interests (12 months) Grants/research support: N/A Speakers
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Cystic fibrosis: From childhood to adulthood. Eitan Kerem Department of Pediatrics and CF Center Hadassah University Hospital Jerusalem Israel
 Cystic fibrosis: From childhood to adulthood Eitan Kerem Department of Pediatrics and CF Center Hadassah University Hospital Jerusalem Israel Vas deference H 2 O Cl - Na + H 2 O Na + Cl - Cl - Cl -
Cystic fibrosis: From childhood to adulthood Eitan Kerem Department of Pediatrics and CF Center Hadassah University Hospital Jerusalem Israel Vas deference H 2 O Cl - Na + H 2 O Na + Cl - Cl - Cl -
ARIKAYCE IMPORTANT SAFETY INFORMATION
 ARIKAYCE The first and only FDA-approved medication for the treatment of refractory (difficult to treat) MAC lung disease as part of a combination antibacterial drug treatment plan MAC=Mycobacterium avium
ARIKAYCE The first and only FDA-approved medication for the treatment of refractory (difficult to treat) MAC lung disease as part of a combination antibacterial drug treatment plan MAC=Mycobacterium avium
10/05/2017. Learning Objectives. Etiology and Prevalence. Diagnosis of Cystic Fibrosis. Disease of Childhood? Survival in Cystic Fibrosis
 Management of the Cystic Fibrosis Patient Jessica Goggin, MAS, RN Nurse Manager UC San Diego Adult Cystic Fibrosis Program Learning Objectives 1. Describe the symptoms associated with Cystic Fibrosis (CF).
Management of the Cystic Fibrosis Patient Jessica Goggin, MAS, RN Nurse Manager UC San Diego Adult Cystic Fibrosis Program Learning Objectives 1. Describe the symptoms associated with Cystic Fibrosis (CF).
Appendix D Clinical specialist statement template
 Appendix D Colistimethate sodium powder and tobramycin powder for inhalation for the treatment of pseudomonas lung infection in cystic fibrosis Thank you for agreeing to give us a statement on your organisation
Appendix D Colistimethate sodium powder and tobramycin powder for inhalation for the treatment of pseudomonas lung infection in cystic fibrosis Thank you for agreeing to give us a statement on your organisation
NATIONAL ASSOCIATION FOR CONTINUING EDUCATION
 Outcome Report NATIONAL ASSOCIATION FOR CONTINUING EDUCATION Presented at: Cleveland Clinic Florida Weston, Florida December 4, 21 Report Date: 2/18/11 Course Director Franck Rahaghi, MD, MHS Director,
Outcome Report NATIONAL ASSOCIATION FOR CONTINUING EDUCATION Presented at: Cleveland Clinic Florida Weston, Florida December 4, 21 Report Date: 2/18/11 Course Director Franck Rahaghi, MD, MHS Director,
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
4/17/2010 C ini n ca c l a Ev E a v l a ua u t a ion o n of o ILD U dat a e t e i n I LDs
 Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
Novel Therapies for NTM
 NTM Lecture Series for Providers Novel Therapies for NTM Kenneth N Olivier, MD, MPH Laboratory of Chronic Airway Infection Chief, Pulmonary Branch/DIR October 20, 2017 Disclosures Past: Cooperative Research
NTM Lecture Series for Providers Novel Therapies for NTM Kenneth N Olivier, MD, MPH Laboratory of Chronic Airway Infection Chief, Pulmonary Branch/DIR October 20, 2017 Disclosures Past: Cooperative Research
Cystic fibrosis: From the gene to the disease
 Cystic fibrosis: From the gene to the disease Christiane Knoop, MD, PhD Institut de Mucoviscidose de l ULB Hôpital Erasme christiane.knoop@erasme.ulb.ac.be Cystic fibrosis «The infant that tastes of salt
Cystic fibrosis: From the gene to the disease Christiane Knoop, MD, PhD Institut de Mucoviscidose de l ULB Hôpital Erasme christiane.knoop@erasme.ulb.ac.be Cystic fibrosis «The infant that tastes of salt
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
COMMON VARIABLE IMMUNODEFICIENCY
 COMMON VARIABLE IMMUNODEFICIENCY This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist. 1 COMMON VARIABLE IMMUNODEFICIENCY Also available
COMMON VARIABLE IMMUNODEFICIENCY This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist. 1 COMMON VARIABLE IMMUNODEFICIENCY Also available
Nintedanib and Pirfenidone: New Medications in the Management of Idiopathic Pulmonary Fibrosis
 Nintedanib and Pirfenidone: New Medications in the Management of Idiopathic Pulmonary Fibrosis Brad Zimmermann, PharmD, MBA Pharmacy Grand Rounds May 02, 2017 Rochester, Minnesota 2017 MFMER slide-1 Objectives
Nintedanib and Pirfenidone: New Medications in the Management of Idiopathic Pulmonary Fibrosis Brad Zimmermann, PharmD, MBA Pharmacy Grand Rounds May 02, 2017 Rochester, Minnesota 2017 MFMER slide-1 Objectives
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
Rare Association of Childhood Bronchiectasis with VACTERL Anomalies; a Case Report
 Rare Association of Childhood Bronchiectasis with VACTERL Anomalies; a Case Report Authors Details: Author's Details: (1) Dushantha Madegedara (2) Asela Rasika Bandara (3) R.M.D.H.M.RATHNAYAKE (1)(2)(3)(4)
Rare Association of Childhood Bronchiectasis with VACTERL Anomalies; a Case Report Authors Details: Author's Details: (1) Dushantha Madegedara (2) Asela Rasika Bandara (3) R.M.D.H.M.RATHNAYAKE (1)(2)(3)(4)
Eosinophils and effusion: a clinical conundrum
 Ruth Sobala, Kevin Conroy, Hilary Tedd, Salem Elarbi kevin.peter.conroy@gmail.com Respiratory Dept, Queen Elizabeth Hospital, Gateshead, UK. Eosinophils and effusion: a clinical conundrum Case report A
Ruth Sobala, Kevin Conroy, Hilary Tedd, Salem Elarbi kevin.peter.conroy@gmail.com Respiratory Dept, Queen Elizabeth Hospital, Gateshead, UK. Eosinophils and effusion: a clinical conundrum Case report A
Starship Paediatric Respiratory and Sleep Medicine Department Outpatient Referral Criteria General Principles
 Starship Paediatric Respiratory and Sleep Medicine Department Outpatient Referral Criteria General Principles This document provides guidance for elective outpatient referrals to the Starship Tertiary
Starship Paediatric Respiratory and Sleep Medicine Department Outpatient Referral Criteria General Principles This document provides guidance for elective outpatient referrals to the Starship Tertiary
Rhinosinusitis. John Ramey, MD Joseph Russell, MD
 Rhinosinusitis John Ramey, MD Joseph Russell, MD Disclosure Statement RSFH as a continuing medical education provider, accredited by the South Carolina Medical Association, it is the policy of RSFH to
Rhinosinusitis John Ramey, MD Joseph Russell, MD Disclosure Statement RSFH as a continuing medical education provider, accredited by the South Carolina Medical Association, it is the policy of RSFH to
Disease spectrum. IPA Invasive pulmonary aspergillosis
 Aspergillus & ABPA Disease spectrum IPA Invasive pulmonary aspergillosis ABPA ABPA pathophysiology conidia of Aspergillus trapped in mucous and narrowed airways of asthmatics/cf germinate to form hyphae
Aspergillus & ABPA Disease spectrum IPA Invasive pulmonary aspergillosis ABPA ABPA pathophysiology conidia of Aspergillus trapped in mucous and narrowed airways of asthmatics/cf germinate to form hyphae