Chronic Obstructive Pulmonary Disease:
|
|
|
- Georgia Flowers
- 5 years ago
- Views:
Transcription
1 Chronic Obstructive Pulmonary Disease: THE BASICS PROF.G.E. ERHABOR Consultant Chest Physician Obafemi Awolowo University Teaching Hospital Complex, Ile-Ife, Nigeria. 1
2 BASICS IS THE ESSENCE OF GREATNESS, THE MOTHER OF ALL KNOWLEDGE. Dr. G. E. Erhabor B U R D E N O F C O P D COPD is the 4th leading cause of death in the USA (behind heart disease, cancer, and cerebrovascular disease). In 2000, the WHO estimated 274 million deaths worldwide from COPD In 1990, COPD was ranked 12th as a burden of disease by 2020 it is projected to rank 5th. Prevalence and morbidity data greatly underestimate the total burden of COPD because the disease is usually not diagnosed until it is clinically apparent and moderately advanced. The WHO estimate 1.1 billion smokers worldwide, increasing to 1.6 billion in In low and middle income countries rates are increasing at an alarming rate. COPD is the only chronic disease that is showing progressive upward trend in both mortality and morbidity. Cigarette smoking is the primary cause of COPD although in low income countries, indoor pollution may be a primary causative factor. In Algeria, the prevalence of tuberculosis and acute respiratory infections has decreased since 1965; an increase in COPD and asthma has been observed in the last decade. COPD is a more costly disease than asthma, and depending on country, 50-75% of the costs are for services associated with exacerbation. Despite this burden, COPD is a Cinderella condition that receives limited recognition from both patients and physicians Respiratory Medicine 2002; 96: S1-S31 2


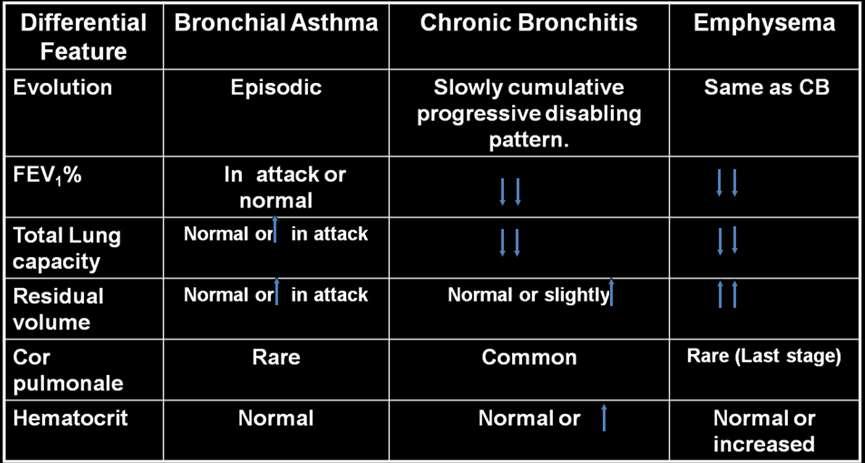
3 Disease Trajectory of a Patients with COPD Chronic bronchitis Chronic bronchitis is defined clinically as the presence of a cough productive of sputum not attributable to other causes on most days for at least three months over two consecutive years 3


4 Emphysema Emphysema is defined anatomically as a permanent and destructive enlargement of airspaces distal to the terminal bronchioles without obvious fibrosis and with loss of normal architecture 4
5 DEFINITION OF COPD Chronic obstructive pulmonary disease (COPD) is a preventable and treatable disease state characterized by a airflow limitation that is not fully reversible. The airflow limitation is usually progressive and is associated with an abnormal inflammatory response of the lungs to noxious particles or gases, primarily caused by cigarette smoking. Although COPD affects the lungs, it also produce significant systemic consequences. The current GOLD and ATS/ERS definition for airflow limitation is an FEV1/FVC ratio of < 70% ( FEV1 predicted < 80%) COPD TWO HISTORICAL HYPOTHESIS DUTCH HYPOTHESIS- A group from Groningen led by Professor Orie introduced the term Chronic non-specific Lung in This approach called Dutch hypothesis which states that airway obstruction like Asthma, chronic bronchitis, COPD and emphysema is related to a different expression of primary abnormality in the airways. BRITISH HYPOTHESIS- Propose that smoking causes mucous hypersecretion and impaired host defenses leading to Chronic infections, disseminated bronchiolar obstruction and emphysema. 5




6 Diagrammatic representation of the four main conditions that comprises COPD The decline in lung function as part of the normal ageing process and as accelerated by cigarette smoking 6

7 Loss of lung function over 11 years in the Lung Health Study for continuous smokers ( ) intermittent quitters ( ) and sustained quitters ( ). FEV1:L forced expiratory volume in one second. Figured reproduced with permission from [18]. INFLAMMATION Small airway disease Airway inflammation Airway remodeling Parenchymal destruction Loss of alveolar attachments Decrease of elastic recoil AIRFLOW LIMITATION 7

8 ASTHMA Sensitizing agent COPD Noxious agent Asthmatic airway inflammation CD4+ T-lymphocytes Eosinophils COPD airway inflammation CD8+ T-lymphocytes Macrophages Neutrophils Completely reversible Airflow limitation Completely irreversible Pathogenesis of COPD Noxious particles and gases Anti-oxidants Lung inflammation Host factors Anti-proteinases Oxidative stress Proteinases 8 COPD pathology Repair mechanisms


9 Causes of Airflow Limitation Irreversible Fibrosis and narrowing of the airways Loss of elastic recoil due to alveolar destruction Destruction of alveolar support that maintains patency of small airways Causes of Airflow Limitation Reversible Accumulation of inflammatory cells, mucus, and plasma exudates in bronchi Smooth muscle contraction in peripheral and central airways Dynamic hyperinflation during exercise Cells and Mediators Involved in the Pathogenesis of COPD RISK FACTORS FOR CHRONIC OBSTRUCTIVE PULMONARY DISEASE Host factors Genetic factors Sex Exposures Smoking Socio-economic state 9
10 Airway hyper reactivity 1gE and asthma Occupation Environmental pollution Perinatal events and childhood illness. Infections Recurrent Bronchopulmonary Aspergillosis Diet Assess and Monitor Disease: Key Points Indoor pollution e.g. Cooking indoors Diagnosis of COPD is based on a history of exposure to risk factors and the presence of airflow limitation that is not fully reversible, with or without the presence of symptoms. Patients who have chronic cough and sputum production with a history of exposure to risk factors should be tested for airflow limitation, even if they do not have dyspnea. For the diagnosis and assessment of COPD, spirometry is the gold standard. Health care workers involved in the diagnosis and management of COPD patients should have access to spirometry. DIAGNOSIS OF COPD 10

11 Consideration in Performing Spirometry 1 Preparation Spirometers need calibration on a regular basis. Spirometers should produce hard copy to permit detection of technical errors. The supervisor of the test needs training in its effective performance. Maximal patient effort in performing the test is required to avoid errors in diagnosis and management Performance Spirometry should be performed using techniques that meet published standards. The expiratory volume/time traces should be smooth and free from irregularities. The recording should go on long enough for a volume plateau to be reached, which may take more than 12 seconds in severe disease. Both FVC and FEV1 should be the largest value obtained from any of 3 technically satisfactory curves and the FVC and FEV1 values in these three curves should vary by no more than 5% or 100 ml, whichever is greater 11
12 Evaluation Spirometry measurements are evaluated by comparison of the results with appropriate reference values based on age, height, sex, and race The presence of a postbronchodilator FEV1 < 80% predicted together with an FEV1/FVC < 70% confirms the presence of airflow limitation that is not fully reversible. In patients with FEV1 80% predicted, FEV1/FVC < 70% may be an early indicator of developing airflow limitation. Bronchodilator Reversibility Testing 1 Preparation Test should be performed when patients are clinically stable and free from respiratory infection. Patients should not have taken inhaled short-acting bronchodilators in the previous six hours, long-acting β2 agonists in the previous 12 hours, or sustained release theophyllines in the previous 24 hours. Spirometry FEV1 should be measured before a bronchodilator is given. The bronchodilator should be given by metered dose inhaler through a spacer device or by nebulizer to be certain it has been inhaled. The bronchodilator dose should be selected to be high on the dose/response curve. Suitable dosage protocols are 400 µg β2-agonist, 80 µg anticholinergic, or the two comined. FEV1 should be measured again minutes after the bronchodilator is given. Results 12


13 An increase in FEV1 that is both greater than 200 ml and 12% above the prebronchodilator FEV1 is considered significant. 13

14 Impaired Lung Function is an excellent predictor of: 1. Morbidity 2. Mortality 3. The development of lung cancer 4. Functional impairment 5. Elevated C-reactive protein 6. Osteoporosis 7. Death 14
15 15
16 16

17 Objectives of COPD Management Prevent disease progression Relieve symptoms Improve exercise tolerance Improve health status Prevent and treat exacerbations Prevent and treat complications Reduce mortality Minimize side effects from treatment MANAGEMENT Goals of the therapy: 1. Education 2. Retard the process of airflow limitation 3. Minimizing airflow limitation 4. Eliminate and prevent infection 17
18 5. Correction of complications like hypoxaemia and Cor pulmonale 6. Rehabilitation physical, occupational, psychological. 7. Surgery Spirometric Classification of Chronic obstructive pulmonary disease (COPD) Severity Postbronchodilator FEV 1 %pred FEV 1 /FVC At risk # > Mild COPD Moderate COPD Severe COPD Very severe 0.7 <30 FEV1: forced expiratory volume in one; FVC: forced vital capacity. #: patients who smoke or have exposure to pollutants, have cough, sputum or dyspnea BTS AND GOLD CLASSIFICATIONS OF SEVERITY OF COPD BTS Classification GOLD Classification Mild disease FEV %predicted FEV1>80% predicted but FEV1/FVC >70% (stage1) Moderate disease FEV %predicted FEV % predicted (stage IIA) predicted + respiratory or Right heart failure (stage IIB) Severe disease FEV1<40% predicted FEV1<30%predicted or FEV1<50% predicted + 18


19 respiratory or right heart failure. Management of COPD Stage 0: At Risk Characteristic Recommended treatment Management of COPD Stage I: Mild COPD Characteristics Recommended Treatment 19



20 Management of COPD Stage II: Moderate COPD Characteristics Recommended Treatment Management of COPD Stage IV: Very Severe COPD Characteristics Recommended Treatment 20
 received no oxygen; the NOTT subject (.")
 subjects (- - -) received oxygen for 24 hours in the 24 hour day (on average, 19 hours). (From Flenley DC: Long-term oxygen therapy. Chest 87:99-193, 1985).")
21 OXYGEN THERAPY Cumulative percent survival of patients in the Nocturnal Oxygen Therapy Trial (NOTT) and Medical Research Council (MRC) controlled trials of long-term domiciliary therapy for men aged over 70. The control subject (. -.) received no oxygen; the NOTT subject (...) received oxygen for 12 hours in the 24-hour day, including the sleeping hours; MRC O 2 subjects ( ) received oxygen for 15 hours in the 24 hour day, including the sleeping hours; and continuous oxygen therapy (COT) subjects (- - -) received oxygen for 24 hours in the 24 hour day (on average, 19 hours). (From Flenley DC: Long-term oxygen therapy. Chest 87:99-193, 1985). MANAGEMENT OF COPD ADVANTAGES / ADMINISTRATION OF VARIOUS FORMS OF THERAPEUTIC INTERVENTION ADVANTAGES ADMINISTRATION Smoking morbidity and mortality 1. Ask Cessation Improved pulmonary function 2. Advice 21
22 Improved subjective symptom 3. Assess - willingness to quit More drastic in mild COPD 4. Assist quit plan Counseling Social support Pharmacotherapy Anti depressant bupropion 5. Arrange: Follow-up contact Bronchodilators 1.Smooth muscle relaxation SA (Short acting βagonist) + anti cholinergic 2. Improved lung emptying Combined LA-BD/SA-BD during tidal breathing 3. Increase (small in FEV1) LA-BD + ICS + theophyline 4. Large changes in lung Vol. Tiotropium is more effective than Ipratropium bromide. 5. Reduced residual volume 6. Delay asset of dynamic hyperinflation 7. Reduced perceived Breathlessness Anti cholinergic may also have Some anti inflammatory properties 22

23 ADVANTAGES ADMINISTRATION ADVANTAGES ADMINISTRATION 23

24 24
25 ADVANTAGES ADMINISTRATION 25


26 ADVANTAGES ADMINISTRATION LONG-TERM EFFECT OF INHALED STEROID STUDY MULTICENTRE STUDY NO. OF PATIENTS ENROLLED RATE OF FEV 1 DECLINED PLACEBO HEALTH OUTCOMES Euroscope NEJM June people recruited, 1277 participated, mean age 52 years (Fluticasone 800µg/day placebo) Small difference between two groups overall 3 years decline in FEV 1 140ml in the budesonide group and 180ml in placebo Not evaluated Initial improvement for 6/12 followed by a similar decline 9-36mts. 26
27 Isolide Lancet May pts mild moderate fluticasone 500µg twice daily with placebo in moderate/severe COPD 3years period) FEV 1 decline 133L in fluticasone group FEV litres in placebo improvement marked 6-9mts later revert to similar levels. Exacerbation low in fluticasone group. Steroid group had slower rate of decline of health status. STUDY MULTICENTRE STUDY NO. OF PATIENTS ENROLLED RATE OF FEV 1 DECLINED PLACEBO HEALTH OUTCOMES Copenhagen Lung study Lancet May 1999 Vestibo et al, budesonide 800µg per day/placebo. Mild improvement of lung function Decline in FEV 1 was identical 46ml per year for budesonide 48ml placebo. No Charge Isolide Lancet May patients with mild COPD FEV 1 68 percent predicted) and treated with inhaled steroid tramcinolone placebo for (3years) No effect in decline of FEV 1. Symptoms Bone density in steroid group Increased skin bruising Reduced hospitalization 27
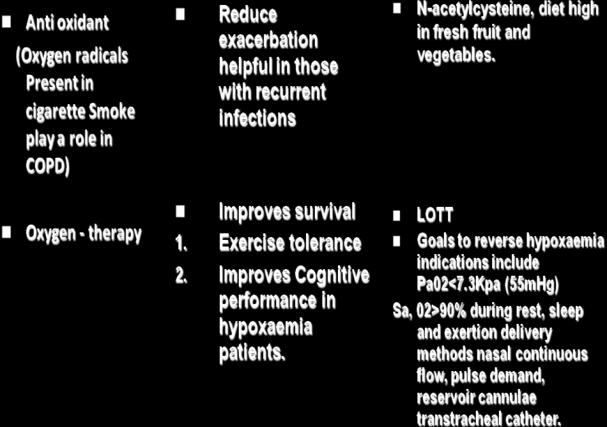
28 Effect of commonly used medications on important clinical outcomes in chronic obstructive pulmonary disease FEV1 Lung volume Dyspne a HRQo L AE Exercise enduran ce Disease modifie r by FEV1 Mort ality Side effect Shortacting β - agonist Yes (A) Yes (B) Yes (A) NA NA Yes (B) NA NA Some Ipratropium bromide Yes (A) Yes (B) Yes (A) NO (B) Yes (B) Yes (B) NO NA Some Long-acting β -agonist Yes (A) Yes (A) Yes (A) Yes (A) Yes (A) Yes (B) (NO) NA Minimal Tiotropium Yes (A) Yes (A) Yes (A) Yes (A) Yes (A) Yes (B) NA NA Minimal Inhaled corticostero ids Yes (A) NA Yes (B) Yes (A) Yes (A) NA NO NA Some Theophylin e Yes (A) Yes (B) Yes (A) Yes (B) NA Yes (B) NA NA Important FEV1 : forced expiratory volume in one second; health related quality of life; AE: exacerbation of COPD; NA: evidence not available Gold grade levels are indicated in bracts. 28
29 Therapy at Each Stage of COPD Patients must be taught how and when to use tier treatment and treatments being prescribed for other conditions should be reviewed. Beta-blocking agents (including eye drop formulations) should be avoided. All Stages Avoid risk factors Education Influenza vaccine once or twice yearly Stage 0: At Risk Spirometry normal Chronic symptoms (cough, sputum production) Stage I: Mild COPD FEV1/FVC < 70% FEV1? 80% predicted Short-acting bronchodilator as needed With or without chronic symptoms (cough, sputum production) Stage II: Moderate COPD FEV1/FVC < 70% 30%? FEV1 < 80% predicted With or without chronic symptoms (cough, sputum production, dyspnea) If symptomatic Regular bronchodilator treatment plus short-acting bronchodilator as needed 29
30 Consider inhaled glucocorticosteroids Rehabilitation Stage III: Severe COPD FEV1/FVC < 70% FEV1 < 30% predicted OR Fev1 < 50% predicted plus respiratory failure or clinical signs of right heart failure Regular bronchodilator treatment plus short-acting bronchodilator as needed Consider inhaled glucocorticosteroids Rehabilitation Long-term oxygen therapy if respiratory failure is present Consider surgical treatments INDICATION FOR LONG-TERM DOMICILLARY OXYGEN THERAPY (LTOT) 1. Patients Should Not Smoke. 2. PaO2 / 7.5kpa (56mmHg) when clinically stable (i.e. at 4-5 weeks after exacerbation. 30
31 3. PaO2 / 5.0kpa (38mmHg) when clinically stable (i.e. at least 4-5 weeks after exacerbations. 4. Previous Cor-pulmonale (ankle Oedema/raised jugular venous pressure abnormal blood gases) 5. Forced expiratory volume in 1 sec/1.5 litres and forced vital capacity of 72 litres. PROGNOSTIC SURVIVAL / FACTORS Aged under 60 and FEV1 above 50% predicted 90% 3-year survival Aged over 60 and FEV1 above 50% predicted 80% 3-year survival Aged over 60 and FEV % predicted 75% 3-year survival 3 Levels of Management of Acute Exacerbations Level I - Outpatient Treatment Level II - Treatment for Hospitalized patients 31
32 Level III - Treatment in patients requiring special or intensive care unit Clinical history, physical findings and diagnostic procedures in patients with exacerbation of chronic obstructive pulmonary disease (COPD) Clinical history Level 1 Level II Level III Co-morbid conditions# History of frequent exacerbation Severity of COPD Mild /moderate Moderate /severe Severe Physical findings Haemodynamic Stable Stable Stable evaluation /unstable Use accessory respiratory Not present muscles, tachypnoea Persistent symptoms after No initial therapy Level 1 Level I Level III Diagnostic procedures Oxygen saturation Yes Yes Yes Arterial blood gases No Yes Yes Chest radiograph No Yes Yes Blood tests No Yes Yes 32
33 Serum drug if applicable if application If applicable concentration + Sputum gram stain and No Yes Yes culture Electrocardiogram No Yes Yes +: unlikely to be present; ++: likely to be present; +++: very likely to be present. #: the more common co-morbid conditions associated with poor prognosis in exacerbations are congestive heart failure, coronary artery disease, diabetes mellitus, renal and liver failure; blood tests include cell blood count, serum electrolytes, renal and liver function; +: serum drug concentration, consider if patients are using theophylline, warfarin, carbamezepine, digoxin; consider if patient has recently been on antibiotics Indications for Hospital Assessment or Admission for Acute Exacerbations of COPD* Marked increase in intensity of symptoms, such as sudden development of resting dyspnoea Severe background COPD Onset of new physical signs (e.g. Cyanosis, peripheral edema) Failure of exacerbation to respond to initial medical management Significant co morbidities Newly occurring arrhythmias Diagnostic uncertainty Older age Insufficient home support Indications for ICU Admission of Patients with Acute Exacerbations of COPD Severe dyspnea that respond inadequately to initial emergency therapy 33
34 Confusion, lethargy, coma Persistent or worsening hypoxemia (pao2 < 6.7 kpa, 50 mm hg) despite supplemental oxygen, and/or severe/worsening hypercapnia (paco2 > 9.3 kpa, 70 mm hg) and/or severe/worsening respiratory acidosis (ph < 7.30) Management of Severe but Not Life-threatening Exacerbations of COPD in the Emergency Department or the Respiratory Ward* Assess severity of symptoms, blood gases, chest X-ray Administer controlled oxygen therapy repeat arterial blood gas measurement after 30 minutes Bronchodilators: - Increase dose or frequency - Combine β2-agonists and anticholinergics - Use spacers or air-driven nebulizers - Consider adding intravenous aminophylline, if needed Glucocorticosteroids Oral or intravenous Antibiotics - When signs of bacterial infection, oral or occasionally intravenous Consider mechanical ventilation At all times - Monitor fluid balance and nutrition - Consider subcutaneous heparin - Identify and treat associated condition (e.g. heart failure, arrhythmias) - Closely monitor condition of the patient 34
35 *The management of acute exacerbations of COPD in the hospital depends on the facilities of the local hospital. Indications for Invasive Mechanical Ventilation Indications for Invasive Mechanical Ventilation Severe dyspnea with use of accessory muscles and paradoxical abdominal motion. Respiratory Frequency > 35 breaths per minute Life-threatening hypoxemia (PaO 2 < 5.3 kpa, 40 mm Hg or PaO 2 /FiO 2 < 200) Severe acidosis (ph < 7.25) and hypercapnia (PaCO 2 > 8.0 kpa, 60 mm Hg) Respiratory arrest Somnolence, impaired mental status Cardiovascular complications (hypertension, shock, heart failure) Other complications (metabolic abnormalities, sepsis, pneumonia, pulmonary embolism, barotrauma massive pleural effusion)nippv failure (or exclusion criteria,) NIPPV failure (or exclusion criteria,) 35

36 Selection and Exclusion Criteria for NIPPV Discharge Criteria for Patients with Acute Exacerbations of COPD Inhaled β2-agonist therapy is required no more frequently than every 4 hours Patient, if previously ambulatory, is able to walk across room Patient is able to eat and sleep without frequent awakening by dyspnoea Patient has been clinically stable for hours Arterial blood gases have been stable for hours Patients (or home caregiver) fully understands correct use of medications Follow-up and home care arrangements have been completed (e.g. visiting nurse, oxygen delivery, meal provisions) Patient, family, and physician are confident patient can manage successfully 36
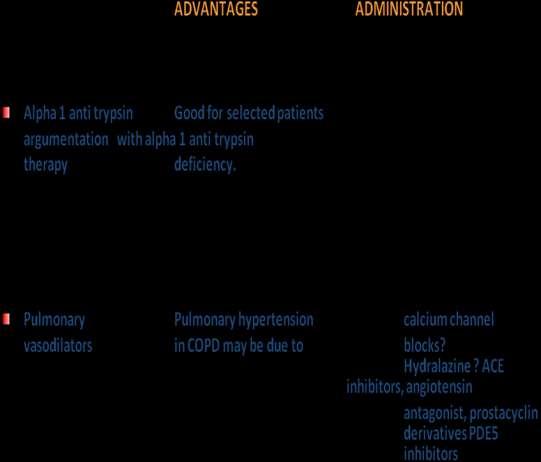
37 Follow-up Assessment 4-6 Weeks After Discharge from Hospital for an Acute Exacerbation of COPD Ability to cope in usual environment Measurement of FEV1 Reassessment of inhaler technique Understanding of recommended treatment regimen COPD) Need for long-term oxygen therapy and/or home nebulizer (for patients with severe Opportunities for Preventing COPD Primary: Preventing development of disease Smoking abstinence Smoking cessation Minimize indoor pollution Secondary: Early detection and prevention of symptomatic disease Smoking cessation Spirometric measurement of expiratory flow rate and nonspirometric measurement of force expiratory time in high-risk persons (smokers) α1-antitrypsin replacement therapy for person at risk for emphysema because of a genetic deficiency syndrome* Tertiary: Reducing complications in symptomatic disease Smoking cessation Influenza and pneumococcal vaccination Pulmonary rehabilitation Supplemental oxygen for patients with hypoxemia * α1-antitrypsin replacement therapy is indicated only for persons with proven α1-antitrypsin deficiency and evidence of abnormal lung function. Such replacement therapy, however, has not yet been proved to prevent the progression of disease. 37
38 Addendum: Brief Strategies to Help the Patient Willing to Quit Smoking 1. ASK: Systematically identify all tobacco users at every visit. Implement an office-wide system that ensures that, for EVERY patient at EVERY clinic visit, tobacco-use status is queried and documented 2. ADVISE: Strongly urge all tobacco users to quit. In a clear, strong, and personalized manner, urge every tobacco user to quit. 3. ASSESS: Determine willingness to make a quit attempt Ask every tobacco user if he or she is willing to make a quit attempt at this time (e.g. within the next 30 days) 4. ASSIST: Aid the patient in quitting Help the patient with a quit plan; provide practical counseling; provide intra-treatment social support; help the patient obtain extratreatment social support; recommend use of approved pharmacotherapy except in special circumstances; provide supplementary materials. 5. ARRANGE: Schedule follow-up contact Schedule follow-up contact, either in person or via telephone. 38
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
You ve come a long way, baby.
 COPD Dr Badri Paudel Dept of Medicine GMC/CHRC 4/22/12 badri@gmc 2 You ve come a long way, baby. Wayne McLaren Former Marlboro Man 4/22/12 badri@gmc 3 Age 30 a robust young man Age 51 riding into the sunset
COPD Dr Badri Paudel Dept of Medicine GMC/CHRC 4/22/12 badri@gmc 2 You ve come a long way, baby. Wayne McLaren Former Marlboro Man 4/22/12 badri@gmc 3 Age 30 a robust young man Age 51 riding into the sunset
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Treatment. Assessing the outcome of interventions Traditionally, the effects of interventions have been assessed by measuring changes in the FEV 1
 58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide
 VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
Course Handouts & Disclosure
 COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Chronic Obstructive Pulmonary Disease (COPD).
.") Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
COPD Management in LTC: Presented By: Jessica Denney RRT
 COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
COPD: Preventable and Treatable. Lecture Outline. Diagnosis of COPD. COPD: Defining Terms
 COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
Over the last several years various national and
 Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Chronic Obstructive Pulmonary Disease (COPD) Copyright 2014 by Mosby, an imprint of Elsevier Inc.
 Copyright 2014 by Mosby, an imprint of Elsevier Inc.") Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
COPD in primary care: reminder and update
 COPD in primary care: reminder and update Managing COPD continues to be a major feature of primary care, particularly in practices with a high proportion of M ori and Pacific peoples. COPDX clinical practice
COPD in primary care: reminder and update Managing COPD continues to be a major feature of primary care, particularly in practices with a high proportion of M ori and Pacific peoples. COPDX clinical practice
CARE OF THE ADULT COPD PATIENT
 CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
COPD exacerbation. Chiara Maruggi, PGY2
 COPD exacerbation Chiara Maruggi, PGY2 Learning objectives At the end of this lecture students will be able to: 1) Critically assess patients for COPD and design a management plan. 2) Develop a step-wise
COPD exacerbation Chiara Maruggi, PGY2 Learning objectives At the end of this lecture students will be able to: 1) Critically assess patients for COPD and design a management plan. 2) Develop a step-wise
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease
 HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
Defining COPD. Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist
 Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Exacerbations of COPD. Dr J Cullen
 Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities
 Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities Jann Mortensen Final Phil meeting, 29 april 2004 Obstructive disease Definition Epidemiologi Mechanisms Natural history
Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities Jann Mortensen Final Phil meeting, 29 april 2004 Obstructive disease Definition Epidemiologi Mechanisms Natural history
COPD UPDATE ıdr Shitrit David ıhead of the Pulmonary Department ımeir Medical Center
 COPD UPDATE 2012 ıdr Shitrit David ıhead of the Pulmonary Department ımeir Medical Center Definition of COPD COPD is a preventable and treatable disease with some significant extra pulmonary effects that
COPD UPDATE 2012 ıdr Shitrit David ıhead of the Pulmonary Department ımeir Medical Center Definition of COPD COPD is a preventable and treatable disease with some significant extra pulmonary effects that
Chronic Obstructive Pulmonary Disease Guidelines and updates
 Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC
 KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC") Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
PDF of Trial CTRI Website URL -
 Clinical Trial Details (PDF Generation Date :- Wed, 31 Oct 2018 11:13:48 GMT) CTRI Number Last Modified On 17/01/2015 Post Graduate Thesis Type of Trial Type of Study Study Design Public Title of Study
Clinical Trial Details (PDF Generation Date :- Wed, 31 Oct 2018 11:13:48 GMT) CTRI Number Last Modified On 17/01/2015 Post Graduate Thesis Type of Trial Type of Study Study Design Public Title of Study
COPD/Asthma. Prudence Twigg, AGNP
 COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Management of Acute Exacerbations
 15 Management of Acute Exacerbations Cenk Kirakli Izmir Dr. Suat Seren Chest Diseases and Surgery Training Hospital Turkey 1. Introduction American Thoracic Society (ATS) and European Respiratory Society
15 Management of Acute Exacerbations Cenk Kirakli Izmir Dr. Suat Seren Chest Diseases and Surgery Training Hospital Turkey 1. Introduction American Thoracic Society (ATS) and European Respiratory Society
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX
 MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX") CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
Anyone who smokes and/or has shortness of breath and sputum production could have COPD
 COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research
 Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
Pathophysiology of COPD 건국대학교의학전문대학원
 Pathophysiology of COPD 건국대학교의학전문대학원 내과학교실 유광하 Rate per 100 0,000 population 550 500 450 400 350 300 250 200 150 100 50 0 Heart disease Cancer Stroke 1970 1974 1978 1982 1986 1990 1994 1998 2002 Year of
Pathophysiology of COPD 건국대학교의학전문대학원 내과학교실 유광하 Rate per 100 0,000 population 550 500 450 400 350 300 250 200 150 100 50 0 Heart disease Cancer Stroke 1970 1974 1978 1982 1986 1990 1994 1998 2002 Year of
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
Decramer 2014 a &b [21]
![Decramer 2014 a &b [21]](/thumbs/90/101390504.jpg "Decramer 2014 a &b [21]") Buhl 2015 [19] Celli 2014 [20] Decramer 2014 a &b [21] D Urzo 2014 [22] Maleki-Yazdi 2014 [23] Inclusion criteria: Diagnosis of chronic obstructive pulmonary disease; 40 years of age or older; Relatively
Buhl 2015 [19] Celli 2014 [20] Decramer 2014 a &b [21] D Urzo 2014 [22] Maleki-Yazdi 2014 [23] Inclusion criteria: Diagnosis of chronic obstructive pulmonary disease; 40 years of age or older; Relatively
TORCH: Salmeterol and Fluticasone Propionate and Survival in COPD
 TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
Chronic obstructive pulmonary disease
 Chronic obstructive pulmonary disease Abstract Whittaker C, BPharm, MRPharmS Amayeza Info Centre Chronic obstructive pulmonary disease affects millions of people, has a major impact on quality of life
Chronic obstructive pulmonary disease Abstract Whittaker C, BPharm, MRPharmS Amayeza Info Centre Chronic obstructive pulmonary disease affects millions of people, has a major impact on quality of life
Presented by UIC College of Nursing
 Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long-acting inhalers and emergency use inhalers.
Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long-acting inhalers and emergency use inhalers.
Chronic Obstructive Pulmonary Disease 1/18/2018
 Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long acting inhalers and emergency use inhalers.
Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long acting inhalers and emergency use inhalers.
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015
 David CL Lam Department of Medicine University of Hong Kong October, 2015") Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Chronic Obstructive Lung Disease - Dr. Kawa Chronic Bronchitis & Emphysema
 Chronic Obstructive Lung Disease - Dr. Kawa Chronic Bronchitis & Emphysema COPD Definition COPD is a chronic, slowly progressive disorder characterized by airflow obstruction. (FEV1 is less than 80% of
Chronic Obstructive Lung Disease - Dr. Kawa Chronic Bronchitis & Emphysema COPD Definition COPD is a chronic, slowly progressive disorder characterized by airflow obstruction. (FEV1 is less than 80% of
COPD COPD. C - Chronic O - Obstructive P - Pulmonary D - Disease OBJECTIVES
 COPD C - Chronic O - Obstructive P - Pulmonary D - Disease 1 OBJECTIVES Following this presentation the participant should be able to demonstrate understanding of chronic lung disease by successful completion
COPD C - Chronic O - Obstructive P - Pulmonary D - Disease 1 OBJECTIVES Following this presentation the participant should be able to demonstrate understanding of chronic lung disease by successful completion
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
A typical COPD exacerbation?
 K. Kostikas 1 A.I. Papaioannou 1 A. Dimoulis 1 S. Loukides 2 K.I. Gourgoulianis 1 A typical COPD exacerbation? 1 Respiratory Medicine Dept, University of Thessaly Medical School, Larissa, and 2 2nd Respiratory
K. Kostikas 1 A.I. Papaioannou 1 A. Dimoulis 1 S. Loukides 2 K.I. Gourgoulianis 1 A typical COPD exacerbation? 1 Respiratory Medicine Dept, University of Thessaly Medical School, Larissa, and 2 2nd Respiratory
Fighting for Air, In Emphysema
 Fighting for Air, The Mechanism of Shortness of Breath In Emphysema Albert A. Rizzo, MD FCCP FACP Speaker, Nationwide Assembly of the American Lung Association & Section Chief Pulmonary/Critical Care Medicine
Fighting for Air, The Mechanism of Shortness of Breath In Emphysema Albert A. Rizzo, MD FCCP FACP Speaker, Nationwide Assembly of the American Lung Association & Section Chief Pulmonary/Critical Care Medicine
Chronic respiratory disease: towards better treatments
 Chronic respiratory disease: towards better treatments Alaina J. Ammit PhD Alaina.Ammit@uts.edu.au Professor of Respiratory Pharmacology, UTS Director, Woolcock Emphysema Centre, Woolcock Institute of
Chronic respiratory disease: towards better treatments Alaina J. Ammit PhD Alaina.Ammit@uts.edu.au Professor of Respiratory Pharmacology, UTS Director, Woolcock Emphysema Centre, Woolcock Institute of
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 CHRONIC OBSTRUCTIVE PULMONARY DISEASE DEFINITION Chronic obstructive pulmonary disease (COPD) is a common preventable and treatable disease characterized by airflow limitation that is usually progressive
CHRONIC OBSTRUCTIVE PULMONARY DISEASE DEFINITION Chronic obstructive pulmonary disease (COPD) is a common preventable and treatable disease characterized by airflow limitation that is usually progressive
COPD. Stan Kellar, MD. Physiology 11/4/2014. Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine
 Stan Kellar, MD Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine COPD Physiology The lungs are filters Filter in oxygen Filter out carbon dioxide (Vascular filter, not part of this discussion)
Stan Kellar, MD Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine COPD Physiology The lungs are filters Filter in oxygen Filter out carbon dioxide (Vascular filter, not part of this discussion)
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease Catherine Whittaker (BPharm, MRPharmS) Abstract Chronic Obstructive Pulmonary Disease affects millions of people, has a major impact on quality of life and has become
Chronic Obstructive Pulmonary Disease Catherine Whittaker (BPharm, MRPharmS) Abstract Chronic Obstructive Pulmonary Disease affects millions of people, has a major impact on quality of life and has become
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Chronic obstructive pulmonary disease: the management of adults with chronic obstructive pulmonary disease in primary and secondary
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Chronic obstructive pulmonary disease: the management of adults with chronic obstructive pulmonary disease in primary and secondary
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease CareOregon Pharmacy Abridged sample of presentation content Home Equipment Pathophysiology Exacerbations Guidelines Lifestyle Modification Medication Management Sample
Chronic Obstructive Pulmonary Disease CareOregon Pharmacy Abridged sample of presentation content Home Equipment Pathophysiology Exacerbations Guidelines Lifestyle Modification Medication Management Sample
COPD GOLD Guidelines & Barnet inhaler choices. Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust
 COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
Integrated Cardiopulmonary Pharmacology Third Edition
 Integrated Cardiopulmonary Pharmacology Third Edition Chapter 13 Pharmacologic Management of Asthma, Chronic Bronchitis, and Emphysema Multimedia Directory Slide 7 Slide 12 Slide 60 COPD Video Passive
Integrated Cardiopulmonary Pharmacology Third Edition Chapter 13 Pharmacologic Management of Asthma, Chronic Bronchitis, and Emphysema Multimedia Directory Slide 7 Slide 12 Slide 60 COPD Video Passive
Living well with COPD
 This factsheet aims to show people with chronic obstructive pulmonary disease (COPD) and their friends and family how they can live a full life with this disease. What is COPD? COPD is a condition that
This factsheet aims to show people with chronic obstructive pulmonary disease (COPD) and their friends and family how they can live a full life with this disease. What is COPD? COPD is a condition that
RESPIRATORY PHYSIOLOGY Pre-Lab Guide
 RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
Advances in Chronic Obstructive Pulmonary Disease
 Advances in Chronic Obstructive Pulmonary Disease By Dave C. Todd, MD; and Darcy D. Marciniuk, MD, FRCPC The case of Nina Nina, 64, presents to the clinic with a three- to fouryear history of progressive,
Advances in Chronic Obstructive Pulmonary Disease By Dave C. Todd, MD; and Darcy D. Marciniuk, MD, FRCPC The case of Nina Nina, 64, presents to the clinic with a three- to fouryear history of progressive,
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable
 THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
If you require this document in another format such as Braille, large print, audio or another language please contact the Trusts Communications Team
 MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
Chronic Obstructive Pulmonary Disease
 Scope of Problem Chronic Obstructive Pulmonary Disease Marianne J. Davies, RN, MSN, APRN Yale University School of Medicine Yale Comprehensive Cancer Center Nevada Cancer Institute 2005 Hospitalizations
Scope of Problem Chronic Obstructive Pulmonary Disease Marianne J. Davies, RN, MSN, APRN Yale University School of Medicine Yale Comprehensive Cancer Center Nevada Cancer Institute 2005 Hospitalizations
Roflumilast (Daxas) for chronic obstructive pulmonary disease
 for chronic obstructive pulmonary disease") Roflumilast (Daxas) for chronic obstructive pulmonary disease August 2009 This technology summary is based on information available at the time of research and a limited literature search. It is not intended
Roflumilast (Daxas) for chronic obstructive pulmonary disease August 2009 This technology summary is based on information available at the time of research and a limited literature search. It is not intended
Known Allergies: Shellfish. Symptoms: abdominal pain, nausea, diarrhea, or vomiting. congestion, trouble breathing, or wheezing.
 CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
Chronic obstructive pulmonary disease
 National Institute for Clinical Excellence Issue date: February 2004 Quick reference guide Chronic obstructive pulmonary disease Management of chronic obstructive pulmonary disease in adults in primary
National Institute for Clinical Excellence Issue date: February 2004 Quick reference guide Chronic obstructive pulmonary disease Management of chronic obstructive pulmonary disease in adults in primary
Internal medicine. Lec #: 4 Date: COPD-Definition
 Internal medicine Topic: COPD Dr: mousa malkawy Lec #: 4 Date: 26-10-2009 COPD-Definition A disease state characterized by airflow limitation that is not fully reversible and usually it is progressive
Internal medicine Topic: COPD Dr: mousa malkawy Lec #: 4 Date: 26-10-2009 COPD-Definition A disease state characterized by airflow limitation that is not fully reversible and usually it is progressive
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น
 รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น COPD Guideline Changing concept in COPD management Evidences that we can offer COPD patients better life COPD Guidelines
รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น COPD Guideline Changing concept in COPD management Evidences that we can offer COPD patients better life COPD Guidelines
AECOPD: Management and Prevention
 Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene
 Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
American Thoracic Society (ATS) Perspective
 Perspective") National Surveillance System for Chronic Lung Disease (CLD): American Thoracic Society (ATS) Perspective Gerard J. Criner, M.D. Chronic Obstructive Pulmonary Disease (COPD) l Definition: Group of chronic
National Surveillance System for Chronic Lung Disease (CLD): American Thoracic Society (ATS) Perspective Gerard J. Criner, M.D. Chronic Obstructive Pulmonary Disease (COPD) l Definition: Group of chronic
The development of chronic obstructive pulmonary
 THE PATHOGENESIS AND PATHOLOGY OF COPD: IDENTIFYING RISK FACTORS AND IMPROVING MORBIDITY AND MORTALITY * Paul D. Scanlon, MD ABSTRACT Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory
THE PATHOGENESIS AND PATHOLOGY OF COPD: IDENTIFYING RISK FACTORS AND IMPROVING MORBIDITY AND MORTALITY * Paul D. Scanlon, MD ABSTRACT Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory
COPD: Change in Definition. COPD Pathology with 3D Interactive. COPD: Definitions of 21st Century 1. COPD Includes Chronic Bronchitis 2
 COPD: Change in Definition COPD Pathology with 3D Interactive by Scott Cerreta, BS, RRT Director of Education www.copdfoundation.org COPD used to include 5 disease processes 1 1 Chronic Bronchitis 2 Emphysema
COPD: Change in Definition COPD Pathology with 3D Interactive by Scott Cerreta, BS, RRT Director of Education www.copdfoundation.org COPD used to include 5 disease processes 1 1 Chronic Bronchitis 2 Emphysema
CLINICAL PATHWAY. Acute Medicine. Chronic Obstructive Pulmonary Disease
 CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
Provider Respiratory Inservice
 Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Turning Science into Real Life Roflumilast in Clinical Practice. Roland Buhl Pulmonary Department Mainz University Hospital
 Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
Disclosures. Chronic Obstructive Pulmonary Disease. Chronic Obstructive Pulmonary Disease (COPD)
") Chronic Obstructive Pulmonary Disease May 14, 2016 Orlando, FL COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United States. Alarmingly, COPD recently became
Chronic Obstructive Pulmonary Disease May 14, 2016 Orlando, FL COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United States. Alarmingly, COPD recently became
Management of Acute Exacerbations of COPD
 MiCMRC Educational Webinar Management of Acute Exacerbations of COPD August 22, 2018 MiCMRC Educational Webinar Management of Acute Exacerbations of COPD Expert Presenter: Catherine A. Meldrum PhD RN MS
MiCMRC Educational Webinar Management of Acute Exacerbations of COPD August 22, 2018 MiCMRC Educational Webinar Management of Acute Exacerbations of COPD Expert Presenter: Catherine A. Meldrum PhD RN MS
Chronic Obstructive Pulmonary Disease (COPD)
") Chronic Obstructive Pulmonary Disease (COPD) Scope: The guideline provides strategies for the improved diagnosis and management of adults with chronic bronchitis and emphysema (chronic obstructive pulmonary
Chronic Obstructive Pulmonary Disease (COPD) Scope: The guideline provides strategies for the improved diagnosis and management of adults with chronic bronchitis and emphysema (chronic obstructive pulmonary
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
COPD- pulmonary hyperinflation- the diaphragms are at the level of the eleventh posterior ribs and appear flat.
 COPD COPD Hallmark symptom - Dyspnea Chronic productive cough Minor hemoptysis pink puffer blue bloater COPD- pulmonary hyperinflation- the diaphragms are at the level of the eleventh posterior ribs and
COPD COPD Hallmark symptom - Dyspnea Chronic productive cough Minor hemoptysis pink puffer blue bloater COPD- pulmonary hyperinflation- the diaphragms are at the level of the eleventh posterior ribs and
Managing COPD --- New Standard of Care
 Managing COPD --- New Standard of Care Introduction Pathophysiology Recent advance in treatment Pharmacology Pulmonary rehabilitation Surgical treat Facts About COPD COPD is the 4 th leading cause of death
Managing COPD --- New Standard of Care Introduction Pathophysiology Recent advance in treatment Pharmacology Pulmonary rehabilitation Surgical treat Facts About COPD COPD is the 4 th leading cause of death