COPD exacerbation. Chiara Maruggi, PGY2
|
|
|
- Rosa Cox
- 5 years ago
- Views:
Transcription
1 COPD exacerbation Chiara Maruggi, PGY2
2 Learning objectives At the end of this lecture students will be able to: 1) Critically assess patients for COPD and design a management plan. 2) Develop a step-wise approach to the diagnosis and treatment of COPD exacerbations including interpretation of clinical and objective data.
3 COPD - The Global Initiative for Chronic Obstructive Lung Disease (GOLD) defines COPD as: common preventable and treatable a disease characterized by persistent respiratory symptoms and airflow limitation due to airway and/or alveolar abnormalities caused by significant exposure to noxious particles or gases. - Chronic inflammationà large airway inflammation (chronic bronchitis) + narrowing of small airways (obstructive bronchiolitis) with decreased elastic recoil of the lung (d/t proteases) + enlargement of airspaces w/ loss of diffusing surface area (emphysema)à air trapping (dynamic hyperinflation)+ static hyperinflationà progressive airflow limitation with impaired gas exchange - Risk factors include: tobacco smoking, environmental exposure (burning of biomass fuels), genetic factors (ex. alpha-1 antitrypsin deficiency)
4 COPD Subtypes Subtypes include: - Emphysema - Chronic bronchitis - Chronic obstructive asthma (reversible airway disease) Most patients have a combination of emphysema (parenchymal destruction) and obstructive bronchiolitis (small airway disease): the contribution of each varies from person to person

5 Chronic bronchitis Definition: Chronic productive cough x 3 months in 2 successive years in a patient in whom other causes have been ruled out Image source:

6 Image source: Emphysema Pathological term referring to the structural changes sometimes seen in COPD patients= enlargement of airspaces distal to the terminal bronchioles and alveolar destruction
7 COPD-Asthma overlap syndrome Characterized by persistent airflow limitation with several features associated with asthma and several features associated with COPD (GOLD and GINA issued definition) Great review article by NEJM on COPD-Asthma Overlap syndrome published in 2015:
8 Symptoms of COPD - 3 features of COPD: - Dyspnea - Chronic cough - Sputum production - Patient may initially present with respiratory complaints including a chronic cough (may be productive of mucous) and dyspnea with exertion which is progressive. Patient often state that the morning time is the worst.
 - Decreased breath sounds -")
9 Image source: Physical exam - Early in the disease the physical exam may be normal but as the disease progresses: - Increased resonance to percussion (due to hyperinflation) - Decreased breath sounds - Wheezing and crackles at lung bases - Barrel-shaped chest (severe disease) - Patients with end-stage COPD may be seen sitting leaning forward with arms outstretched (tripoding) with use of accessory muscles, expiration through pursed lips, or signs of cyanosis
10 Evaluation - Patients reporting dyspnea, a chronic cough, chronic sputum production or a gradual decrease in exertional activity +/- history of exposure to smoke (tobacco, factories, etc) should be screened. - All patients should be evaluated by spirometry and some patients should also have imaging and lab testing (which may include: CBC, BNP, alpha-1 antitrypsin) - Suspect AAT deficiency in young patient (<45 y/o) with emphysema, emphysema in a non-smoker or minimal smoker, emphysema with mostly basilar changes on CXR, or family history of emphysema
11 Assessment Based on 3 parameters: 1. Severity of obstruction on spirometry testing 2. Patient symptoms rated on either the CAT (COPD Assessment Test) or the mmrc (modified Medical Research Council Dyspnea scale) 3. Frequency of exacerbation 4. Presence of comorbidities
12 Spirometry - Essential test to confirm the diagnosis and stage COPD - Perform bronchodilator challenge with albuterol 400mcg: if the airflow obstruction is only partially reversed or not reversed at all then it is suggestive of COPD rather than asthma - Post-bronchodilator FEV1/FVC ratio < 0.7 or < LLN is used to establish the presence of airflow limitation
13 GOLD Severity scale (spirometry) In the presence of FEV1/FVC evidence of airflow limitation (FEV1/FVC<0.7): - GOLD 1: Mild (FEV1 80% or greater predicted) - GOLD 2: Moderate (FEV % predicted) - GOLD 3: Severe (FEV % predicted) - GOLD 4: Very severe (FEV 1 < 30% predicted)


14 Patient symptoms: CAT, mmrc scales mmrc dyspnea scale: 0-4 scale, score of 4 indicating highest degree of exercise intolerance CAT scale: 0-40 scale with score >10 indicating COPD symptoms that limit quality of life Image source:
15 Frequency of exacerbation GOLD guideline combined spirometry findings and likelihood of exacerbations into 4 groups (Group A, B, C, D) - However, studies showed that the ABCD assessment was no better in predicting mortality or health outcomes than spirometric grades. - So in 2017 the GOLD guidelines separated the spirometry testing from symptom evaluation. - Now patients undergo spirometry testing followed by assessment with either the CAT or mmrc tool and history of exacerbations to form a revised ABCD assessment tool
16 Image source:
: multidimensional grading system that can be used to predict the risk of death from any cause and from a respiratory cause in patients with COPD Kaplan Meier Survival Curves for the Four")
17 Presence of comorbidities The presence of other conditions (cardiovascular, musculoskeletal, etc) needs to be documented in patients with COPD BODE index (BMI, airflow Obstruction, Dyspnea, Exercise): multidimensional grading system that can be used to predict the risk of death from any cause and from a respiratory cause in patients with COPD Kaplan Meier Survival Curves for the Four Quartiles of the Body-Mass Index, Degree of Airflow Obstruction and Dyspnea, and Exercise Capacity Index (Panel A). Quartile 1: BODE score 0-2, Quartile 2: BODE score 3-4, Quartile 3: BODE score 5-6, Quartile 4: BODE score
18 Nonpharmacological management - Smoking cessation - Reduce environmental risk factors - Vaccination - PPSV23 (pneumovax) for patients < 65 yo; PCV13 (prevnar) + PPSV23 for patients 65 yo+ - Annual influenza vaccine - Oxygen therapy - If PaO2 of 55mmHg or less or SaO2 88% or less on RA - If patient has cor pulmonale, PaO2 of 59mmHg or less or SaO2 of 89% or less - Continuous O2 therapy increases lifespan if used for the above criteria - Pulmonary rehab - Improves symptoms and quality of life and decreases number of hospitalizations - Lung volume reduction surgery
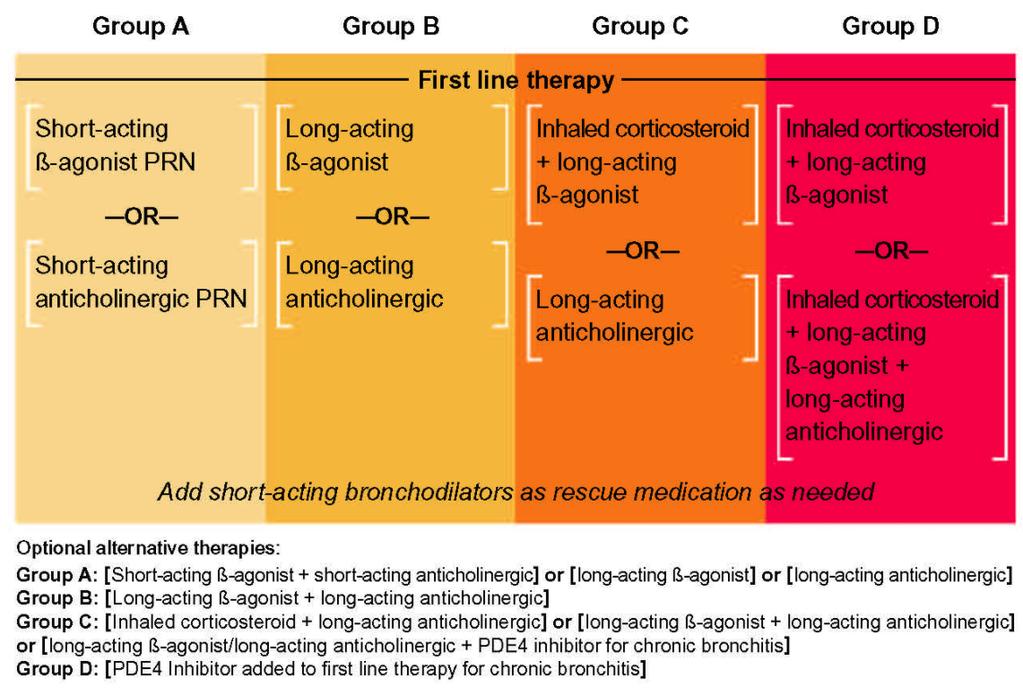
19 Pharmacologic therapy, GOLD criteria - For all patients with COPD, the use of short-acting bronchodilators PRN - For category A patients: - SABA PRN. A combination SABA-SAMA may be used if a single agent is not enough. (SABA ex. Albuterol, SAMA ex. Atrovent, Ipratropium) - For category B patients: - regular treatment with LABA or LAMA. SABA PRN. (ex. LABA salmeterol, LAMA spiriva, tiotropium) - For category C patients: - regular treatment with LAMA or LABA + ICS. SABA PRN. - Roflumilast can be used in patients with chronic bronchitis - For category D patients: - regular treatment with LABA +/- LAMA + ICS. SABA PRN. - Roflumilast can also be used if chronic bronchitis present
20 Image source:
21 Features of COPD exacerbation - Diffuse wheezing, distant breath sounds, barrel-shaped chest, tachypnea, tachycardia - Features of severe respiratory decline: - Use of accessory muscles - Brief, fragmented speech - Inability to lie flat - Profound diaphoresis - Agitation - Failure to improve with initial emergency treatment
22 Image source: Triggers for COPD exacerbation - Infections account for ~70% of COPD exacerbations - Environmental pollution - Pulmonary embolism - Unknown etiology
23 COPD exacerbation management - Inhaled short-acting bronchodilator therapy - Short-acting beta adrenergic agonists (eg albuterol) are the mainstay of therapy +/- short-acting anticholinergic (eg ipratropium) (combination usually advised during severe exacerbations) - Systemic glucocorticoids x 5 days (GOLD guidelines) - Patients not requiring ICU admission: Prednisone mg PO daily - Patient requiring ICU admission: IV Methylprednisolone 60mg 1-4x/day - Study looking at mortality of patients receiving 240mg/day of IV methylprednisolone vs. <240mg/day showed no change in mortality but shorter hospital stay in ICU patients - Antibiotics (next slide) - Mucoactive agents, methylxanthines, and mechanical techniques to augment sputum clearance have not been shown to provide benefit in a COPD exacerbation
24

25 Image source: Supplemental oxygen - Target oxygen saturation: 88 to 92% - BiPAP improves clinical outcomes in patients having an acute exacerbation of COPD complicated by hypercapnic acidosis (do not start non-invasive ventilation in patients that do not have a respiratory acidosis) - After starting NIV patient should have a decreased respiratory rate, increased tidal volume, and increased minute ventilation. - 8cm H20 inspiratory pressure, 3cm H20 expiratory pressure
26 Interpreting ABG in a COPD exacerbation ph = 7.25 (normal ) PaCO 2 = 75 mmhg (normal 35-45mmHg) HCO 3 - = 30 mmol/l (normal 21-27) PaO 2 = 39 mmhg FiO 2 = 0.21 ph is acidotic The HCO3 could not account for the acidosis but the high PaCO2 can. This points at a respiratory cause of acidosis. Also, while the HCO3 is elevated, it has not had time to respond to the ph pointing at a likely acute disorder. Severe hypoxemia likely secondary to elevated PaCO2.
27 MKSAP Question 1 A 62-year-old woman is evaluated in the hospital after being admitted 4 days ago for an acute exacerbation of COPD. She has responded well to treatment and is ready to be discharged today. Her medical history is notable for moderate-severity COPD, heart failure, depression, osteoporosis, hypertension, and hyperlipidemia. Her discharge medications are lisinopril, carvedilol, simvastatin, sertraline, alendronate, vitamin D, calcium, tiotropium, levofloxacin, prednisone, and albuterol. On physical examination, temperature is normal, blood pressure is 120/84 mm Hg, pulse rate is normal, and respiration rate is 18/min. Oxygen saturation is 93% breathing ambient air. No jugular venous distention is noted. Pulmonary examination reveals a few scattered wheezes and a few basal crackles. She is not using accessory muscles of breathing. Trace pedal edema is noted. She ambulates well without oxygen.
28 Which of the following factors increases this patient s risk for early hospital readmission for COPD? A) Adequacy of discharge medications for COPD B) Female gender C) Length of hospitalization D) Multiple comorbid conditions
29 Which of the following factors increases this patient s risk for early hospital readmission for COPD? A) Adequacy of discharge medications for COPD B) Female gender C) Length of hospitalization D) Multiple comorbid conditions
30 MKSAP Question 2 A 59-year-old woman is evaluated in follow-up in November after being diagnosed with moderate COPD 3 months ago. She has never received the influenza or pneumococcal vaccine. She has no allergies. Her medications are a long-acting inhaled anticholinergic agent and an as-needed short-acting β2-agonist inhaler. On physical examination, vital signs and the remainder of the physical examination are normal.
31 Which of the following vaccinations are recommended for this patient? A) Inactivated influenza vaccine and 13-valent pneumococcal conjugate vaccine (PCV13) B) Inactivated influenza vaccine and 23-valent pneumococcal conjugate vaccine (PPSV23) C) Inactivated influenza vaccine, PPSV23, and PCV13 D) Live attenuated influenza vaccine and PPSV13 E) Live attenuated influenza vaccine, PPSV23, and PCV13
32 Which of the following vaccinations are recommended for this patient? A) Inactivated influenza vaccine and 13-valent pneumococcal conjugate vaccine (PCV13) B) Inactivated influenza vaccine and 23-valent pneumococcal conjugate vaccine (PPSV23) C) Inactivated influenza vaccine, PPSV23, and PCV13 D) Live attenuated influenza vaccine and PPSV13 E) Live attenuated influenza vaccine, PPSV23, and PCV13 Patients with COPD should receive an annual inactivated influenza vaccine. Patients with COPD age 19 to 64 should receive PPSV23 with revaccination at age 65 or older if 5 years have elapsed since the previous pneumococcal vaccine. PCV13 should be given at age 65+ if 1 year has elapsed since the last PPSV23 immunization. (If a patient with COPD received the PPSV23 vaccine at age 65+ they do not need revaccination)
33 MKSAP Question 3 A 67-year-old woman is evaluated in the emergency department for a 2-day history of fever, dyspnea, and increased cough with production of green sputum. She has severe COPD, which was diagnosed 2 years ago. She used albuterol several times yesterday with no relief of dyspnea, and she was unable to sleep last night. Her last spirometry, performed 6 months ago, showed an FEV1 of 48% of predicted. She is a current smoker with a 24-pack-year history. Medications are tiotropium and as-needed albuterol. On physical examination, temperature is 38.9 C (102.0 F), blood pressure is 124/80 mm Hg, pulse rate is 118/min, and respiration rate is 30/min. Oxygen saturation is 82% breathing ambient air. Pulmonary examination reveals bilateral diffuse expiratory wheezing. After an albuterol nebulizer treatment and breathing 2 L of oxygen by nasal cannula, oxygen saturation is 91%. She remains tachypneic with bilateral expiratory wheezing. Chest radiograph shows no infiltrate.
34 In addition to continuing this patient's supplemental oxygen and short-acting bronchodilator, which of the following is the most appropriate treatment? A) Azithromycin and prednisone B) Clarithromycin and fluticasone C) Doxycycline and salmeterol/fluticasone D) Erythromycin and roflumilast
35 In addition to continuing this patient's supplemental oxygen and short-acting bronchodilator, which of the following is the most appropriate treatment? A) Azithromycin and prednisone B) Clarithromycin and fluticasone C) Doxycycline and salmeterol/fluticasone D) Erythromycin and roflumilast Antibiotics and systemic glucocorticoids (prednisone) are indicated for the treatment of COPD exacerbations along with short acting bronchodilators and oxygen as needed. Most COPD exacerbations are due to bacterial or viral infections the most common bacterial pathogens are H. influenzae, H. parainfluenzae, Strep pneumoniae, and Moraxella catarrhalis. Common antibiotics includes: advanced macrolide, cephalosporin, or doxycycline. The prednisone course is typically 40mg/d x 5 days.
36 Questions
37 Resources UpToDate Management of COPD Chronic obstructive pulmonary disease: Definition, clinical manifestations, diagnosis, and staging Management of exacerbations of COPD Management of stable COPD NEJM Resident 360: COPD NEJM review articles The Asthma-COPD Overlap syndrome The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in COPD MKSAP 17 COPD overview and questions MedStudy Internal Medicine Review: Core curriculum COPD
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX
 MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX") CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
COPD/Asthma. Prudence Twigg, AGNP
 COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
COPD: Preventable and Treatable. Lecture Outline. Diagnosis of COPD. COPD: Defining Terms
 COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic
 COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Chronic Obstructive Pulmonary Disease (COPD) Copyright 2014 by Mosby, an imprint of Elsevier Inc.
 Copyright 2014 by Mosby, an imprint of Elsevier Inc.") Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Chronic Obstructive Pulmonary Disease
 Scope of Problem Chronic Obstructive Pulmonary Disease Marianne J. Davies, RN, MSN, APRN Yale University School of Medicine Yale Comprehensive Cancer Center Nevada Cancer Institute 2005 Hospitalizations
Scope of Problem Chronic Obstructive Pulmonary Disease Marianne J. Davies, RN, MSN, APRN Yale University School of Medicine Yale Comprehensive Cancer Center Nevada Cancer Institute 2005 Hospitalizations
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
CARE OF THE ADULT COPD PATIENT
 CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC
 KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC") Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
COPD Update. Muhammad Talha Khan MD. COPD Exacerbations. COPD Clinical Importance. COPD Pathophysiology. Overview/Objectives
 Overview/Objectives COPD Update Muhammad Talha Khan MD Pulmonologist St Croix Regional Medical Center, St Croix Falls, WI. Overview of COPD and disease impact Classification of COPD Severity Treatment
Overview/Objectives COPD Update Muhammad Talha Khan MD Pulmonologist St Croix Regional Medical Center, St Croix Falls, WI. Overview of COPD and disease impact Classification of COPD Severity Treatment
Chronic Obstructive Pulmonary Disease Guidelines and updates
 Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015
 David CL Lam Department of Medicine University of Hong Kong October, 2015") Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Predicaments in Primary Care Peter F. Bidey, DO
 Pulmonary Predicaments in Primary Care Peter F. Bidey, DO Pulmonary Predicaments in Primary Care Peter F. Bidey, D.O. Clinical Instructor -Family Medicine Philadelphia College of Osteopathic Medicine
Pulmonary Predicaments in Primary Care Peter F. Bidey, DO Pulmonary Predicaments in Primary Care Peter F. Bidey, D.O. Clinical Instructor -Family Medicine Philadelphia College of Osteopathic Medicine
You ve come a long way, baby.
 COPD Dr Badri Paudel Dept of Medicine GMC/CHRC 4/22/12 badri@gmc 2 You ve come a long way, baby. Wayne McLaren Former Marlboro Man 4/22/12 badri@gmc 3 Age 30 a robust young man Age 51 riding into the sunset
COPD Dr Badri Paudel Dept of Medicine GMC/CHRC 4/22/12 badri@gmc 2 You ve come a long way, baby. Wayne McLaren Former Marlboro Man 4/22/12 badri@gmc 3 Age 30 a robust young man Age 51 riding into the sunset
Defining COPD. Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist
 Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
COPD. Stan Kellar, MD. Physiology 11/4/2014. Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine
 Stan Kellar, MD Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine COPD Physiology The lungs are filters Filter in oxygen Filter out carbon dioxide (Vascular filter, not part of this discussion)
Stan Kellar, MD Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine COPD Physiology The lungs are filters Filter in oxygen Filter out carbon dioxide (Vascular filter, not part of this discussion)
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
Chronic Obstructive Pulmonary Disease (COPD)
") Chronic Obstructive Pulmonary Disease (COPD) Definition of COPD Airflow obstruction that is: o Not fully reversible o Progressive o Does not change markedly over several months Combination of airway and
Chronic Obstructive Pulmonary Disease (COPD) Definition of COPD Airflow obstruction that is: o Not fully reversible o Progressive o Does not change markedly over several months Combination of airway and
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
COPD GOLD Guidelines & Barnet inhaler choices. Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust
 COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
& Guidelines. For The Management Of. Chronic Obstructive Air Way Disease (COPD)
") Guidelines For The Management Of Chronic Obstructive Air Way Disease (COPD) By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs
Guidelines For The Management Of Chronic Obstructive Air Way Disease (COPD) By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs
COPD Management in LTC: Presented By: Jessica Denney RRT
 COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
Provider Respiratory Inservice
 Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
If you require this document in another format such as Braille, large print, audio or another language please contact the Trusts Communications Team
 MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Management of Acute Exacerbations of COPD
 MiCMRC Educational Webinar Management of Acute Exacerbations of COPD August 22, 2018 MiCMRC Educational Webinar Management of Acute Exacerbations of COPD Expert Presenter: Catherine A. Meldrum PhD RN MS
MiCMRC Educational Webinar Management of Acute Exacerbations of COPD August 22, 2018 MiCMRC Educational Webinar Management of Acute Exacerbations of COPD Expert Presenter: Catherine A. Meldrum PhD RN MS
Integrated Cardiopulmonary Pharmacology Third Edition
 Integrated Cardiopulmonary Pharmacology Third Edition Chapter 13 Pharmacologic Management of Asthma, Chronic Bronchitis, and Emphysema Multimedia Directory Slide 7 Slide 12 Slide 60 COPD Video Passive
Integrated Cardiopulmonary Pharmacology Third Edition Chapter 13 Pharmacologic Management of Asthma, Chronic Bronchitis, and Emphysema Multimedia Directory Slide 7 Slide 12 Slide 60 COPD Video Passive
Course Handouts & Disclosure
 COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD- pulmonary hyperinflation- the diaphragms are at the level of the eleventh posterior ribs and appear flat.
 COPD COPD Hallmark symptom - Dyspnea Chronic productive cough Minor hemoptysis pink puffer blue bloater COPD- pulmonary hyperinflation- the diaphragms are at the level of the eleventh posterior ribs and
COPD COPD Hallmark symptom - Dyspnea Chronic productive cough Minor hemoptysis pink puffer blue bloater COPD- pulmonary hyperinflation- the diaphragms are at the level of the eleventh posterior ribs and
Presented by UIC College of Nursing
 Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long-acting inhalers and emergency use inhalers.
Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long-acting inhalers and emergency use inhalers.
Chronic Obstructive Pulmonary Disease 1/18/2018
 Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long acting inhalers and emergency use inhalers.
Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long acting inhalers and emergency use inhalers.
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
Fact. Objectives 1/6/2016. Reducing Hospital Readmissions for Chronic Obstructive Pulmonary Disease (COPD)
") Reducing Hospital Readmissions for Chronic Obstructive Pulmonary Disease (COPD) Jin S. Oh, PharmD Larkin Community Hospital January 10, 2016 Fact COPD is the third leading cause of death in the United
Reducing Hospital Readmissions for Chronic Obstructive Pulmonary Disease (COPD) Jin S. Oh, PharmD Larkin Community Hospital January 10, 2016 Fact COPD is the third leading cause of death in the United
CHRONIC OBSTRUCTIVE LUNG DISEASE (COPD), BRONCHIAL ASTHMA
, BRONCHIAL ASTHMA") CHRONIC OBSTRUCTIVE LUNG DISEASE (COPD), BRONCHIAL ASTHMA GOLD GINA Chronic Obstructive Pulmonary Disease (COPD) COPD is currently the fourth leading cause of death in the world.1 COPD is projected to
CHRONIC OBSTRUCTIVE LUNG DISEASE (COPD), BRONCHIAL ASTHMA GOLD GINA Chronic Obstructive Pulmonary Disease (COPD) COPD is currently the fourth leading cause of death in the world.1 COPD is projected to
How to distinguish between uncontrolled and severe asthma
 How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
COPD: GOLD guidelines Ijlal Babar, MD Medical Director Pulmonary CCM, Pulmonary Hypertension Center SRHS
 COPD: GOLD guidelines 2017 Ijlal Babar, MD Medical Director Pulmonary CCM, Pulmonary Hypertension Center SRHS Introduction The Global Initiative for Chronic Obstructive Lung Disease (GOLD) program was
COPD: GOLD guidelines 2017 Ijlal Babar, MD Medical Director Pulmonary CCM, Pulmonary Hypertension Center SRHS Introduction The Global Initiative for Chronic Obstructive Lung Disease (GOLD) program was
Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management. Colleen Sakon, PharmD BCPS September 27, 2018
 Management. Colleen Sakon, PharmD BCPS September 27, 2018") Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management Colleen Sakon, PharmD BCPS September 27, 2018 Disclosures I have no actual or potential conflicts of interest 2 Objectives Summarize
Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management Colleen Sakon, PharmD BCPS September 27, 2018 Disclosures I have no actual or potential conflicts of interest 2 Objectives Summarize
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide
 VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
COPD in primary care: reminder and update
 COPD in primary care: reminder and update Managing COPD continues to be a major feature of primary care, particularly in practices with a high proportion of M ori and Pacific peoples. COPDX clinical practice
COPD in primary care: reminder and update Managing COPD continues to be a major feature of primary care, particularly in practices with a high proportion of M ori and Pacific peoples. COPDX clinical practice
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017
 Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
Chronic Obstructive Pulmonary Disease:
 Chronic Obstructive Pulmonary Disease: THE BASICS PROF.G.E. ERHABOR Consultant Chest Physician Obafemi Awolowo University Teaching Hospital Complex, Ile-Ife, Nigeria. 1 BASICS IS THE ESSENCE OF GREATNESS,
Chronic Obstructive Pulmonary Disease: THE BASICS PROF.G.E. ERHABOR Consultant Chest Physician Obafemi Awolowo University Teaching Hospital Complex, Ile-Ife, Nigeria. 1 BASICS IS THE ESSENCE OF GREATNESS,
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
COPD Diagnosis, Management and Program
 COPD Diagnosis, Management and Program RYAN MARTIN, MD NEBRASKA PULMONARY SPECIALTIES Initial diagnosis Setting matters: Inpatient. Usually sicker, oftentimes avoiding healthcare. Outpatient. Often seeking
COPD Diagnosis, Management and Program RYAN MARTIN, MD NEBRASKA PULMONARY SPECIALTIES Initial diagnosis Setting matters: Inpatient. Usually sicker, oftentimes avoiding healthcare. Outpatient. Often seeking
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy f the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy f the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
HOSPITAL RECORD ABSTRACTION FORM
 HOSPITAL RECORD ABSTRACTION FORM ID NUMBER: VERSION: A 10/23/2015 0a. Form Completion Date... / / 0b. Staff Code... 0c. Event ID: 0d. Event Date: / / Instructions: Answers are derived from the medical
HOSPITAL RECORD ABSTRACTION FORM ID NUMBER: VERSION: A 10/23/2015 0a. Form Completion Date... / / 0b. Staff Code... 0c. Event ID: 0d. Event Date: / / Instructions: Answers are derived from the medical
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable
 THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
AECOPD: Management and Prevention
 Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
COPD and Asthma Update. April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute
 COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
Objectives. Advances in Managing COPD Patients
 4:45 5:30pm Advances in Managing Patients SPEAKER Nicola Hanania, MD, FCCP, FRCP, FACP Presenter Disclosure Information The following relationships exist related to this presentation: Nicola Hanania, MD,
4:45 5:30pm Advances in Managing Patients SPEAKER Nicola Hanania, MD, FCCP, FRCP, FACP Presenter Disclosure Information The following relationships exist related to this presentation: Nicola Hanania, MD,
WINDY CITY WHEEZE: A PREVENTATIVE APPROACH TO COPD MANAGEMENT
 WINDY CITY WHEEZE: A PREVENTATIVE APPROACH TO COPD MANAGEMENT Thursday, October 25, 2018 Sarah Sungurlu DO Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures I have no actual
WINDY CITY WHEEZE: A PREVENTATIVE APPROACH TO COPD MANAGEMENT Thursday, October 25, 2018 Sarah Sungurlu DO Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures I have no actual
COPD exacerbation. Dr. med. Frank Rassouli
 Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
3. Identify the importance in the prehospital setting for the administration of nebulized bronchodilator.
 TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
CLINICAL PATHWAY. Acute Medicine. Chronic Obstructive Pulmonary Disease
 CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
Chronic Obstructive Pulmonary Disease: What s New in Therapeutic Management?
 Chronic Obstructive Pulmonary Disease: What s New in Therapeutic Management? Sabrina Sherwood, PharmD PGY2 Internal Medicine Resident University of Utah Health September 29, 2018 Disclosures Relevant disclosures
Chronic Obstructive Pulmonary Disease: What s New in Therapeutic Management? Sabrina Sherwood, PharmD PGY2 Internal Medicine Resident University of Utah Health September 29, 2018 Disclosures Relevant disclosures
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Care Process Model. Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease WHAT IS MULTIDISCIPLINARY CARE? Multidisciplinary care is agreed upon, interdisciplinary, patient-centered, disease-focused, care delivery systems that are informed
Chronic Obstructive Pulmonary Disease WHAT IS MULTIDISCIPLINARY CARE? Multidisciplinary care is agreed upon, interdisciplinary, patient-centered, disease-focused, care delivery systems that are informed
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Over the last several years various national and
 Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 Page 1 of 9 PURPOSE To assure that DOP inmates with Pulmonary Diseases are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers and Chronic Disease Nurses are
Page 1 of 9 PURPOSE To assure that DOP inmates with Pulmonary Diseases are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers and Chronic Disease Nurses are
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease CareOregon Pharmacy Abridged sample of presentation content Home Equipment Pathophysiology Exacerbations Guidelines Lifestyle Modification Medication Management Sample
Chronic Obstructive Pulmonary Disease CareOregon Pharmacy Abridged sample of presentation content Home Equipment Pathophysiology Exacerbations Guidelines Lifestyle Modification Medication Management Sample
COPD UPDATE ıdr Shitrit David ıhead of the Pulmonary Department ımeir Medical Center
 COPD UPDATE 2012 ıdr Shitrit David ıhead of the Pulmonary Department ımeir Medical Center Definition of COPD COPD is a preventable and treatable disease with some significant extra pulmonary effects that
COPD UPDATE 2012 ıdr Shitrit David ıhead of the Pulmonary Department ımeir Medical Center Definition of COPD COPD is a preventable and treatable disease with some significant extra pulmonary effects that
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
Acute respiratory failure
 Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Chronic Obstructive Pulmonary Disease (COPD).
.") Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
Advancing COPD treatment strategies with evidencebased. 17:15 19:15 Monday 11 September 2017 ERS 2017, Milan, Italy
 Advancing COPD treatment strategies with evidencebased approaches 17:15 19:15 Monday 11 September 2017 ERS 2017, Milan, Italy Increasing understanding of COPD and the effect on guideline evolution. GOLD
Advancing COPD treatment strategies with evidencebased approaches 17:15 19:15 Monday 11 September 2017 ERS 2017, Milan, Italy Increasing understanding of COPD and the effect on guideline evolution. GOLD
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
Disclosure Statement. Epidemiological Data
 EVALUATION OF THE MEDICATION UTILIZATION OF COPD PATIENTS AT THE MIAMI VA HEALTHCARE SYSTEM Simone Edgerton, PharmD. PGY 1 Pharmacy Resident Miami VA Healthcare System Miami, Florida Simone.edgerton2@va.gov
EVALUATION OF THE MEDICATION UTILIZATION OF COPD PATIENTS AT THE MIAMI VA HEALTHCARE SYSTEM Simone Edgerton, PharmD. PGY 1 Pharmacy Resident Miami VA Healthcare System Miami, Florida Simone.edgerton2@va.gov
Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD)
") Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) Zahava Picado, PharmD PGY1 Pharmacy Practice Resident Central Texas Veterans Healthcare System Temple, TX October
Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) Zahava Picado, PharmD PGY1 Pharmacy Practice Resident Central Texas Veterans Healthcare System Temple, TX October
Management of Acute Exacerbations
 15 Management of Acute Exacerbations Cenk Kirakli Izmir Dr. Suat Seren Chest Diseases and Surgery Training Hospital Turkey 1. Introduction American Thoracic Society (ATS) and European Respiratory Society
15 Management of Acute Exacerbations Cenk Kirakli Izmir Dr. Suat Seren Chest Diseases and Surgery Training Hospital Turkey 1. Introduction American Thoracic Society (ATS) and European Respiratory Society
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013
 COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013 None Disclosures Definitions Asthma Asthma is a chronic inflammatory
COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013 None Disclosures Definitions Asthma Asthma is a chronic inflammatory
Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
 10:50-11:50am Case Studies in Pulmonary Medicine for the Primary Care Clinician SPEAKERS Timothy J. Scialla, MD Common Shortcuts/Common Misperceptions Smoking + Dyspnea = COPD Hospitalization for cough
10:50-11:50am Case Studies in Pulmonary Medicine for the Primary Care Clinician SPEAKERS Timothy J. Scialla, MD Common Shortcuts/Common Misperceptions Smoking + Dyspnea = COPD Hospitalization for cough
TLALELETSO. Chronic Lung Disease
 dates for your practice June, 2013. Vol 2, Issue 18 TLALELETSO Chronic Lung Disease This issue is focused on chronic lung disease. We discuss diagnosis, management and prevention, focusing on the importance
dates for your practice June, 2013. Vol 2, Issue 18 TLALELETSO Chronic Lung Disease This issue is focused on chronic lung disease. We discuss diagnosis, management and prevention, focusing on the importance
People with asthma who smoke. The combination of asthma, a chronic airway disease, and smoking increases the risk of COPD even more.
 COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
2017 GOLD Report. Is it worth its weight in GOLD??? CSHP-NB Fall Education Day September 30, 2017
 2017 GOLD Report Is it worth its weight in GOLD??? CSHP-NB Fall Education Day September 30, 2017 Lauren Munro; BSc(Pharm) Amanda Burns; BSc(Pharm) Pharmacy Residents The Moncton Hospital Objectives Explain
2017 GOLD Report Is it worth its weight in GOLD??? CSHP-NB Fall Education Day September 30, 2017 Lauren Munro; BSc(Pharm) Amanda Burns; BSc(Pharm) Pharmacy Residents The Moncton Hospital Objectives Explain
Advances in Chronic Obstructive Pulmonary Disease
 Advances in Chronic Obstructive Pulmonary Disease By Dave C. Todd, MD; and Darcy D. Marciniuk, MD, FRCPC The case of Nina Nina, 64, presents to the clinic with a three- to fouryear history of progressive,
Advances in Chronic Obstructive Pulmonary Disease By Dave C. Todd, MD; and Darcy D. Marciniuk, MD, FRCPC The case of Nina Nina, 64, presents to the clinic with a three- to fouryear history of progressive,