In the name of God. Asthma
|
|
|
- Rudolph Farmer
- 5 years ago
- Views:
Transcription
1 In the name of God Asthma
2 Objectives- at the end of this 2 sessions you should be able to: Discriminate between obstructive and restrictive airway disease. Define pathophysiology and symptoms of asthma. Know goals of therapy Monitor pt on therapy List different therapy and their differences Educate pt with asthma on different formulations
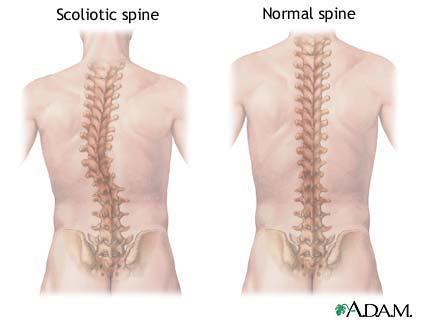
3 Pulmonary disorders Restrictive disease: limits airflow during inspiration inability to expand the lung. Loss of elasticity (fibrosis, pneumonia) Physical deformity of the chest (kyphoscoliosis) Obstructive disease: limits airflow during expirationincrease resistance to air flow, create air turbulence, narrow air passage Bronchitis Asthma
4
5 ASTHMA Asthma is a chronic inflammatory disorder of the airways Many cells and cellular elements play a role: mast cells, eosinophils, T-lymphocytes, macrophages, neutrtophils, and epithelial cells. In susceptible individuals, this inflammation causes recurrent episodes of wheezing, breathlessness, chest tightness, and coughing, particularly night or in the early morning. These episodes are usually associated with airflow obstruction that is often reversible either spontaneously or with treatment. Increase In the existing bronchial hyperresponsiveness to a variety of stimuli is seen.
6 early-phase asthma produces immediate bronchoconstriction (measured by a drop in peak expiratory flow [PEF] or FEV 1 ) that: spontaneously improves over an hour or is reversed easily by inhalation of a β 2 -agonist
7 late-phase asthma late asthmatic response (LAR) is a second bronchoconstrictive response often occurs 4 to 12 hours later, more severe, more prolonged & more difficult to reverse with bronchodilators (influx of inflammatory cells & mediators)
8 early asthmatic response (EAR), late asthmatic response (LAR) EAR is blocked by preadministration of β 2 - agonists, cromolyn, or theophylline Bronchodilators do not block the LAR to allergen challenge, Corticosteroids block the LAR but do not affect the EAR Cromolyn blocks both
9
10 Natural History 30-70% of children with asthma will improve markedly or become symptom-free by early adulthood; Frequent wheezing during the first 3 years of life and either one major risk factor (e.g., parental history of asthma or eczema) or two of three minor risk factors (e.g., eosinophilia, wheezing without colds, and allergic rhinitis).
11 Epidemiology of asthma the global prevalence of asthma ranges from 1% to 18% of the population in different countries estimated 300 million affected individuals
12 Factors Influencing the Development and Expression of Asthma
13 HOST FACTORS Genetic, e.g., Genes pre-disposing to atopy Genes pre-disposing to airwayhyperresponsiveness Obesity Sex
 Occupational sensitizers Tobacco smoke Passive smoking Active smoking Outdoor/Indoor Air Pollution Diet Emotions Exercise")
14 ENVIRONMENTAL FACTORS Allergens Indoor: Domestic mites, furred animals (dogs, cats, mice), cockroach allergen, fungi, molds, yeasts Outdoor: Pollens, fungi, molds, yeasts Infections (predominantly viral) Occupational sensitizers Tobacco smoke Passive smoking Active smoking Outdoor/Indoor Air Pollution Diet Emotions Exercise Drugs/preservatives
15 Hyperreactivity Defined as an exaggerated response of muscles to trigger stimuli Is pathogonomic of asthma
16 Airway Inflammation In Asthma inflammation affects all airways including in most patients the upper respiratory tract and nose but its physiological effects are most pronounced in medium-sized bronchi. The pattern of inflammation in the airways appears to be similar in all clinical forms of asthma, whether allergic, non-allergic, or aspirin-induced, and at all ages.
17 Difficult to- treat asthma poor compliance with treatment physchological & psychiatric disorders. genetic factors? Many pts have from the onset of the disease, rather than progressing from milder asthma.
18 Tobacco smoking more difficult to control, more frequent exacerbations and hospital admissions, and produces a more rapid decline in lung function and an increased risk of death. Asthma patients who smoke may have a neutrophil-predominant inflammation in their airways and are poorly responsive to glucocorticosteroids.
19 Exercise-induced bronchoconstriction. Typically develops within 5-10 minutes after completing exercise (rarely during exercise). asthma symptoms, or cough, resolve spontaneously within minutes. More common in dry, cold air.
20 Occupational Asthma A relationship between symptoms and the workplace (improvement in symptoms away from work and worsening of symptoms on returning to work) can be helpful in establishing a link between suspected sensitizing agents and asthma
21 Spirometry FEV1- Forced Expiratory Volume in the first second: The volume of air that can be forced out in one second after taking a deep breath PEF- Peak expiratory flow: The maximum airflow during a forced expiration beginning with the lungs fully inflated. FVC-Forced vital capacity: The total volume of air that can be exhaled during a maximal forced expiration effort.
22 FEV1 Has low variability and during acute bronchospasm shows best correlation with clinical symptoms. Gold Std. for bronchodilator efficacy.

23 Peak expiratory flow measurements are made using a peak flow meter and can be an important aid in both diagnosis and monitoring of asthma.

24
25 Reversibility rapid improvements in FEV1 (or PEF), measured within minutes after inhalation of a rapid-acting bronchodilator for example after ug salbutamol or more sustained improvement over days or weeks after the introduction of effective controller treatment such as ICS.
26 Variability improvement or deterioration in symptoms and lung function occurring over time. Variability may be experienced over the course of one day (when it is called diurnal variability), from day to day, from month to month, or seasonally.
27 The degree of reversibility in FEV1 Indicates a diagnosis of asthma It is generally accepted as 12% and 200 ml from the pre-bronchodilator value.
28 PEF to confirm the diagnosis of asthma a 60 L/min (or 20% or more of prebronchodilator PEF) improvement after inhalation of a bronchodilator, or diurnal variation in PEF of more than 20% (with twice daily readings, more than 10%) suggests a diagnosis of asthma.
29 Measurement of airway responsiveness. For patients with symptoms consistent with asthma, but normal lung function, measurements of airway responsiveness to direct airway challenges such as inhaled methacholine and histamine or indirect airway challenges such as inhaled mannitol or exercise challenge provocative concentration (or dose) of the agonist causing a given fall (often 20%) in FEV1
30 Classification of Asthma Severity by Clinical Features Before Treatment
31 Step 1 Mild Intermittent Asymptomatic between exacerbations Exacerbations brief (from a few hours to a few days); intensity may vary Nocturnal 2 times/mo FEV1 or PEF 80% predicted Symptoms less than once a week PEF or FEV1 variability < 20%
32 Step 2 Mild Persistent Symptoms more than once a week but less than once a day Exacerbations may affect activity and sleep Nocturnal symptoms more than twice a month FEV1 or PEF 80% predicted PEF or FEV1 variability < 20 30%
33 Step 3 Moderate Persistent Symptoms daily Exacerbations may affect activity and sleep Nocturnal symptoms more than once a week Daily use of inhaled SABAs FEV1 or PEF 60-80% predicted PEF or FEV1 variability > 30%
34 Step 4 Severe Persistent Symptoms daily Frequent exacerbations Frequent nocturnal asthma symptoms Limitation of physical activities FEV1 or PEF 60% predicted PEF or FEV1 variability > 30%

35

36

37
38 Following short-acting bronchodilators FEV1 < 1 L improvement of 250 ml Otherwise 20% improvement in FEV1 is considered a relief. Plus patient s subjective impression.
39 Medications to treat asthma Controllers (maintenance) are medications taken daily on a long-term basis to keep asthma under clinical control chiefly through their anti-inflammatory effects. Relievers (rescue) are medications used on an as-needed basis that act quickly to reverse bronchoconstriction and relieve its symptoms.
40 Controllers inhaled and systemic, glucocorticosteroids, leukotriene modifiers, long-acting inhaled beta 2-agonists in combination with inhaled glucocorticosteroids, sustained-release theophylline, cromones, anti-ige, and other systemic steroid-sparing therapies.
41 Relievers rapid-acting inhaled beta 2- agonists, inhaled anticholinergics, short-acting theophylline, and short-acting oral beta 2-agonists.
42 Route of asthma meds administration Inhaled, Orally Parenterally
43 AEROSOL THERAPY FOR ASTHMA Site-specific Enhancing the therapeutic ratio. More rapid bronchodilation than either parenteral or oral administration
44 Inhaled medications for asthma pressurized Metered-dose inhalers (pmdis), Breath-actuated MDIs, Dry powder inhalers (DPIs), Soft mist inhalers Nebulized or wet aerosols.
45 Inhaled medications Pressurized MDIs: patients with any severity, including during exacerbations. Breathactuated aerosols: patients who have difficulty using the press and breathe pressurized MDI. Soft mist inhalers: require less coordination. Dry powder inhalers: easier to use, but require a minimal inspiratory flow rate and may prove difficult for some patients. DPIs differ with respect to the fraction of exactuator dose delivered to the lung. For some drugs, the dose may need to be adjusted when switching from an MDI to a DPI. Nebulized aerosols are rarely indicated for the treatment of chronic asthma in adults.
46 For pmdis containing propellants (CFC, HFA) Bronchodilators: the switch from CFC to HFA inhalers No change in efficacy Glucocorticosteroids, the HFA formulations: smaller particle size less oral deposition reduction in oral side effects greater lung deposition greater systemic efficacy greater systemic exposure and risk of side effects
47
48 Steps for using inhaler Remove the cap and hold inhaler upright Shake according to package insert (Pulmicort inhalers should not be shaken!) May need to prime the inhaler before you use it the first time Tilt your head back and breathe out slowly Position your mouth in front of the mouthpiece (3 methods) Press down the inhaler as you breathe in slowly (3-5 sec) Hold your breath Allow one min between puffs
49 Avoid common inhaler mistakes. Breathe out before pressing your inhaler. Inhale slowly, Breathe in through your mouth, not your nose Press down on your inhaler at the start of inhalation (or within the first second of inhalation). Keep inhaling as you press down on inhaler. Press your inhaler only once while you are inhaling (one breath for each puff).. Make sure you breathe in evenly and deeply. Different types of inhalers require different techniques.
50 What should be the interval between the two puffs of salbutamol MDI? 1 to 2 minutes The first puff takes that much time to dilate the airways. The second puff, penetrates the lungs further down and so it is more effective
51 If both salbutamol and steroid MDIs are prescribed, which one should be taken first? Salbutamol and after about 5 minutes of that, the steroid inhalation. Salbutamol by dilating the bronchi, allows the steroid to penetrate the most peripheral parts of the lungs; this provides more relief.
52 DRY-POWDER INHALERS (DPIs) breath-actuated and require minimal hand-lung coordination. Mouth rinsing following treatment is important. in acute distress pts will be unable to actuate the devices adequately. In general require higher aspiratory (>60 L/min) Change in inhalation technique i.e., deep, forceful inspiration for optimal actuation is needed. Powder may be irritating and may produce cough.
53 NEBULIZERS Nebulizers come in two basic forms, the jet nebulizer and the ultrasonic nebulizer. JNs produce an aerosol from a liquid solution or suspension placed in a cup. Fill volume of 3-6 ml N/S is usually recommended to dilute the medication Approximately 10% the dose placed in a nebulizer is delivered to the patient s lung, Less efficient delivering drug to the lung than MDIs Use of a facemask versus a mouthpiece significantly reduces lung delivery by either method due to nasal filtering.
54 Holding-chamber/ Spacer Devices Allows evaporation of the propellant before inhalation. Allows inhalation after actuation. Obviates the need for good hand-lung coordination. Large particles which deposit in oropharynx rain out in the spacer ADRs. (thrush, hoarseness, HPA axis suppression).
55 Holding-chamber/ Spacer Devices They are useful for all pts especially very young and very old or pts using ICSs. Permits more drug particles to achieve a respirable drug size.
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70 LUNG DEPOSITION Devices for delivering therapeutic aerosols generate particles with aerodynamic diameters from µm. Particles between 5-10 deposit in the trachea and large bronchi, particles 1-5 µm reach the lower airways, and particles smaller (0.5) act as a gas and are exhaled. In asthma, the airways, not the alveoli, are the target for delivery.
71 Controllers
72 Inhaled Corticosteroids (ICS) most effective anti-inflammatory medications in adults, systemic effects of inhaled glucocorticosteroids are not a problem at doses of 400 g or less budesonide or equivalent daily. At medium- and high-doses, twice-daily dosing is necessary for most but not all ICS. With budesonide, efficacy may be improved with more frequent dosing (QID)
73 Side effects from inhaled glucocorticosteroids: Oropharyngeal candidiasis, dysphonia, and occasionally coughing Interventions: spacer devices, mouth washing, prodrugs that are activated in the lungs but not in the pharynx (e.g., ciclesonide), and new formulations and devices that reduce oropharyngeal deposition
74
75 Dosing of steroids Inhaled: Beginning dose dependent on asthma control then titrated down over 2-3 months to lowest effective dose once control is achieved. Tablets: For daily control use lowest effective dose 5-40 mg of prednisone equivalent in a.m. or qod. For acute attacks mg daily in 1 or 2 divided doses for adults or 1-2 mg/kg daily in children.
76 Leukotriene modifiers include cysteinylleukotriene (CysLT1) receptor antagonists (montelukast, pranlukast, and zafirlukast) and a 5-lipoxygenase inhibitor (zileuton). an alternative treatment for adult patients with mild persistent asthma, reduce the dose of ICSs in moderate to severe asthma Some patients with aspirin-sensitive asthma respond well to leukotriene modifiers. anti-inflammatory effect is weak Alone as controller cannot substitute for low doses of ICS, & less effective than LABAs as add-on therapy Zileuton, Zafirlukast: liver toxicity, LFT is recommended (There are reports with others)

77
78 Long-acting beta 2-agonists (LABAs) beta-adrenergis sympathomimetics LABAs Inhaled: Formoterol (F) DPI -F: 1 inhalation (12 mcg) bid. MDI- F: 2 puffs bid. Salmeterol (Sm) DPI-Sm: 1 inhalation (50 mcg) bid. MDI-Sm: 2 puffs bid.
79 LABAs Have been associated with an increased risk of severe exacerbations and asthma deaths when added to usual therapy. Salmeterol NOT to be used to treat acute attacks. Should not use as monotherapy for controller therapy. Always use as adjunct to ICS therapy. Formoterol has onset similar to salbutamol and has been used as needed for acute symptoms.
80 combination formulation In moderate to severe persistent asthma, combination more effective than doubling the ICS dose. Budesonide/formoterol (Symbicort TM) Turbohaler: may be used for both rescue and maintenance. Salmeterol/fluticasone propionate (SeretideTM) - Diskus inhaler Limited data in children 4-11 yrs No data in children < 4 yrs.
81 Theophylline bronchodilator lower dose (anti-inflammatory) SR once- or twice-daily SR: little effect as a first-line controller. may provide benefit as add-on therapy in those not achieve control on ICS alone
82 Short-acting theophylline Aminophylline 7 mg/kg loading dose over 20 min followed by 0.4 mg/kg/hr continuous infusion. S.E.: Nausea, vomiting, headache. At higher serum concentrations: seizures, tachycardia, and arrhythmias. TDM is required.
83 Cromones: Up: sodium cromoglycate Down: nedocromil
84 Cromones: sodium cromoglycate and nedocromil sodium. SE: coughing upon inhalation and sore throat. long-term role?? mild persistent asthma and exercise-induced bronchospasm. anti-inflammatory effect is weak less effective than a low dose of ICS
85 Oral Beta Agonists slow release formulations of salbutamol, terbutaline, and bambuterol, a prodrug that is converted to terbutaline in the body.
86 Anti-IgE (omalizumab) In patients with elevated IgE. indicated for patients with severe allergic asthma who are uncontrolled on ICS,
87 Oral anti-allergic compounds. introduced in some countries for mild to moderate allergic asthma. tranilast, repirinast, tazanolast, pemirolast, ozagrel, celatrodast, amlexanox, and ibudilast., Side effects - Sedation
88 Other controller therapies low-dose methotrexate Cyclosporin gold The macrolide, troleandromycin, has a small steroid-sparing effect when used with methylprednisolone, but its effect may result from the macrolide decreasing metabolism of the glucocorticosteroid
89 Relievers
90 Rapid-acting inhaled 2-agonists or Short-acting beta2-agonists (SABAs) Albuterol/salbutamol Fenoterol Levalbuterol Metaproterenol Pirbuterol Terbutaline
91 SABAs Choice for acute bronchospasm. Inhaled route has faster onset and is more effective than tablet or syrup. The regular use of beta 2-agonists may lead to relative refractoriness Poor asthma control: Increasing use, lack of expected effect, or use of > 1 canister a month indicate; adjust long-term therapy accordingly. Use of 2 canisters per month is associated with an increased risk of a severe, life-threatening asthma attack.
92 Systemic glucocorticosteroids prevent progression of the asthma exacerbation, reduce the need for referral to emergency departments and hospitalization, prevent early relapse after emergency treatment, and reduce the morbidity of the illness. The main effects of systemic steroids in acute asthma are only evident after 4 to 6 hours mg prednisolone given daily for 5 to 10 days
93 Anticholinergics Ipratropium bromide (IB) Oxitropium bromide (OB) May provide additive effects to beta 2- agonist but has slower onset of action. Is an alternative for patients with intolerance for beta 2-agonists. IB-MDI 4-6 puffs q6h or q20 min in the ED. Nebulizer 500 mcg q20min x 3 then q2-4hrs for adults and mcg for children.
94 Short-acting theophylline for relief of asthma symptoms In exacerbations remains controversial. may provide no additive bronchodilator effect over adequate doses of SABA, but it may benefit respiratory drive. should NOT be administered to patients already on long-term treatment with SR form TDM recommended
95 SABAs dosing For prn symptomatic use and pretreatment before exercise 2 puffs MDI or 1 inhalation DPI. For asthma attacks 4-8 puffs q2-4h, may administer q20min x 3 with medical supervision or the equivalent of 5 mg salbutamol by nebulizer.
96 Hints.. <= 5 years, combination therapy has been less well studied and the addition of a LABA may not be as effective as increasing the dose of ICS in reducing exacerbation When asthma is controlled with a combination of ICS and LABA, the preferred approach to is to begin by reducing the dose of ICS by approximately 50% while continuing the LABA
97 Hints Controller treatment may be stopped if the patient asthma remains controlled on the lowest dose of controller and no recurrence of symptoms occurs for one year
98 Atopy Genetic predisposition for the development of immunoglobulin E (IgE)-mediated response to common aeroallergens. Atopy is the strongest predisposing factor in the development of asthma. A very common presentation of asthma is a child with a positive family history of asthma and allergy to tree and grass pollen, house dust mites, household pets, and molds.
99 Gastroesophageal reflux. is nearly 3 times as prevalent in patients with asthma compared to the general population. Medical management should be given for the relief of reflux symptoms, although this does not consistently improve asthma control.
100 Aspirin-induced asthma Up to 28 percent of adults with asthma, but rarely children, suffer from asthma exacerbations in response to aspirin and other NSAIDs. The diagnosis: aspirin challenge, which must be conducted in a facility with cardiopulmonary resuscitation capabilities. Complete avoidance of the drugs that cause symptoms is the standard management.

101

102

103
104 Combivent Indicated for COPD Each actuation meters 21 mcg of ipratropium bromide and 120 mcg of albuterol sulfate from the valve and delivers 18 mcg of ipratropium bromide and 103 mcg of albuterol sulfate (equivalent to 90 mcg albuterol base) from
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
Asthma in Pregnancy. Asthma. Chronic Airway Inflammation. Objective Measures of Airflow. Peak exp. flow rate (PEFR)
") Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Asthma Description. Asthma is a disease that affects the lungs defined as a chronic inflammatory disorder of the airways.
 Asthma Asthma Description Asthma is a disease that affects the lungs defined as a chronic inflammatory disorder of the airways. Symptoms of asthma In susceptible individuals, this inflammation causes recurrent
Asthma Asthma Description Asthma is a disease that affects the lungs defined as a chronic inflammatory disorder of the airways. Symptoms of asthma In susceptible individuals, this inflammation causes recurrent
Asthma training. Mike Levin Division of Asthma and Allergy Red Cross Hospital
 Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Respiratory Health. Asthma and COPD
 Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
I have no perceived conflicts of interest or commercial relationships to disclose.
 ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
MANAGING ASTHMA. Nancy Davis, RRT, AE-C
 MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
II: Moderate Worsening airflow limitations Dyspnea on exertion, cough, and sputum production; patient usually seeks medical
 Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
12/18/2017. Disclosures. Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
Significance. Asthma Definition. Focus on Asthma
 Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Foundations of Pharmacology
 Pharmacologic Management of Asthma Objectives: 1. Review the physiological basis for asthma therapy 2. Discuss the differences between SABA and LABA 3. Discuss the role of inhaled and oral systemic corticosteroids
Pharmacologic Management of Asthma Objectives: 1. Review the physiological basis for asthma therapy 2. Discuss the differences between SABA and LABA 3. Discuss the role of inhaled and oral systemic corticosteroids
Respiratory Pharmacology
 Allergy Targets of allergies Type I Histamine Leukotrienes Prostaglandins Bradykinin Hypersensitivity reactions Asthma Characterised by Triggered by Intrinsic Extrinsic (allergic) Mediators Result Early
Allergy Targets of allergies Type I Histamine Leukotrienes Prostaglandins Bradykinin Hypersensitivity reactions Asthma Characterised by Triggered by Intrinsic Extrinsic (allergic) Mediators Result Early
Medicine Dr. Kawa Lecture 4 - Treatment of asthma :
 Medicine Dr. Kawa Lecture 4 - Treatment of asthma : Avoiding allergens. Hyposensitization :Subcutaneous injections of inially very small, but gradually increasing doses of allergens (desensitization or
Medicine Dr. Kawa Lecture 4 - Treatment of asthma : Avoiding allergens. Hyposensitization :Subcutaneous injections of inially very small, but gradually increasing doses of allergens (desensitization or
Nancy Davis, RRT, AE-C
 Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Medications Affecting The Respiratory System
 Medications Affecting The Respiratory System Overview Asthma is a chronic inflammatory disorder of the airways. It is an intermittent and reversible airflow obstruction that affects the bronchioles. The
Medications Affecting The Respiratory System Overview Asthma is a chronic inflammatory disorder of the airways. It is an intermittent and reversible airflow obstruction that affects the bronchioles. The
Asthma in the Athlete
 Asthma in the Athlete Jorge E. Gomez, MD Associate Professor Texas Children s Hospital Baylor College of Medicine Assist Team Physician UH Understand how we diagnose asthma Objectives Be familiar with
Asthma in the Athlete Jorge E. Gomez, MD Associate Professor Texas Children s Hospital Baylor College of Medicine Assist Team Physician UH Understand how we diagnose asthma Objectives Be familiar with
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Asthma By Mayo Clinic staff
 MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma and Vocal Cord Dysfunction
 Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Asthma. Definition. Symptoms
 Asthma Definition Asthma is a condition in which your airways narrow and swell and produce extra mucus. This can make breathing difficult and trigger coughing, wheezing and shortness of breath. For some
Asthma Definition Asthma is a condition in which your airways narrow and swell and produce extra mucus. This can make breathing difficult and trigger coughing, wheezing and shortness of breath. For some
Asthma. chapter 7. Overview
 chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
Using an Inhaler and Nebulizer
 Using an Inhaler and Nebulizer Introduction An inhaler is a handheld device that is used to deliver medication directly to your airways. A nebulizer is an electric or battery powered machine that turns
Using an Inhaler and Nebulizer Introduction An inhaler is a handheld device that is used to deliver medication directly to your airways. A nebulizer is an electric or battery powered machine that turns
Diagnosis, Treatment and Management of Asthma
 Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Asthma in Pediatric Patients. DanThuy Dao, D.O., FAAP. Disclosures. None
 Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Prescribing guidelines: Management of COPD in Primary Care
 Prescribing guidelines: Management of COPD in Primary Care Establish diagnosis of COPD in patients 35 years with appropriate symptoms with history, examination and spirometry (FEV1/FVC ratio < 70%) Establish
Prescribing guidelines: Management of COPD in Primary Care Establish diagnosis of COPD in patients 35 years with appropriate symptoms with history, examination and spirometry (FEV1/FVC ratio < 70%) Establish
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Function of the Respiratory System. Exchange CO2 (on expiration) for O2 (on inspiration)
 for O2 (on inspiration)") Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
Asthma Update A/Prof. John Abisheganaden. Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital
 Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Glossary of Asthma Terms
 HealthyKidsExpress@bjc.org Asthma Words to Know Developed in partnership with Health Literacy Missouri Airways (Bronchi, Bronchial Tubes): The tubes in the lungs that let air in and out of the body. Airway
HealthyKidsExpress@bjc.org Asthma Words to Know Developed in partnership with Health Literacy Missouri Airways (Bronchi, Bronchial Tubes): The tubes in the lungs that let air in and out of the body. Airway
Alberta Childhood Asthma Pathway for Primary Care
 Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
Asthma medications: Know your options - MayoClinic.com. Asthma medications: Know your options
 MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
Tips on managing asthma in children
 Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Clinical Practice Guideline: Asthma
 Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Global Initiative for Asthma (GINA) What s new in GINA 2016?
 What s new in GINA 2016?") Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Clinical Implications of Asthma Phenotypes. Michael Schatz, MD, MS Department of Allergy
 Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
10/18/2012. Penn State University Children s Hospital JODIE STABINSKI CRNP MSN AE-C
 Penn State University Children s Hospital JODIE STABINSKI CRNP MSN AE-C Daily: Long-Term Control Corticosteroids (inhaled and systemic) Long-acting beta 2 -agonists (Serevent, Foradil) Methylxanthines
Penn State University Children s Hospital JODIE STABINSKI CRNP MSN AE-C Daily: Long-Term Control Corticosteroids (inhaled and systemic) Long-acting beta 2 -agonists (Serevent, Foradil) Methylxanthines
Medications for Managing COPD in Hospice Patients. Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources
 Medications for Managing COPD in Hospice Patients Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources Goal of medications in COPD Decrease symptoms and/or complications Reduce frequency
Medications for Managing COPD in Hospice Patients Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources Goal of medications in COPD Decrease symptoms and/or complications Reduce frequency
Asthma in Day to Day Practice
 Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Air Flow Limitation. In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation.
 Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Clinical Guideline for the Diagnosis, Evaluation, and Management of Adults and Children with Asthma
 Clinical Guideline for the Diagnosis, Evaluation, and Management of Adults and Children with Asthma - 2005 Criteria that suggest the diagnosis of Asthma: The symptoms of dyspnea, cough and/or wheezing,
Clinical Guideline for the Diagnosis, Evaluation, and Management of Adults and Children with Asthma - 2005 Criteria that suggest the diagnosis of Asthma: The symptoms of dyspnea, cough and/or wheezing,
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
Asthma 2015: Establishing and Maintaining Control
 Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Your Guide to MANAGING ASTHMA
 Your Guide to MANAGING ASTHMA Asthma affects more than 24 MILLION AMERICANS. It is a chronic disease that causes your airways to become inflamed, making it hard to breathe. There is no cure for asthma.
Your Guide to MANAGING ASTHMA Asthma affects more than 24 MILLION AMERICANS. It is a chronic disease that causes your airways to become inflamed, making it hard to breathe. There is no cure for asthma.
Asthma Pathophysiology and Treatment. John R. Holcomb, M.D.
 Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
History & Development
 RSPT 2317 Anticholinergic Bronchodilators () History & Development Prototypical parasympatholytic agent is atropine an alkaloid found naturally in the plants Atropa belladona (nightshade) and Datura species
RSPT 2317 Anticholinergic Bronchodilators () History & Development Prototypical parasympatholytic agent is atropine an alkaloid found naturally in the plants Atropa belladona (nightshade) and Datura species
Adult Asthma Clinical Practice Guideline Summary
 Adult Asthma Clinical Practice Guideline Summary The following evidence-based guideline was developed to assist Primary Care physicians and other clinicians in the management of asthma in adults. It was
Adult Asthma Clinical Practice Guideline Summary The following evidence-based guideline was developed to assist Primary Care physicians and other clinicians in the management of asthma in adults. It was
Bronchial asthma. E. Cserháti 1 st Department of Paediatrics. Lecture for english speaking students 5 February 2013
 Bronchial asthma E. Cserháti 1 st Department of Paediatrics Lecture for english speaking students 5 February 2013 Epidemiology of childhood bronchial asthma Worldwide prevalence of 7-8 and 13-14 years
Bronchial asthma E. Cserháti 1 st Department of Paediatrics Lecture for english speaking students 5 February 2013 Epidemiology of childhood bronchial asthma Worldwide prevalence of 7-8 and 13-14 years
From Chronic Lung Disease of Infancy to Asthma
 From Chronic Lung Disease of Infancy to Asthma Mollie V. Anderson, CPNP Certified Pediatric Nurse Practitioner Pediatric Lung Care Bon Secours Medical Group St. Mary s Hospital 1 Mollie V. Anderson, CPNP
From Chronic Lung Disease of Infancy to Asthma Mollie V. Anderson, CPNP Certified Pediatric Nurse Practitioner Pediatric Lung Care Bon Secours Medical Group St. Mary s Hospital 1 Mollie V. Anderson, CPNP
Improving the Management of Asthma to Improve Patient Adherence and Outcomes
 Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Bronchial asthma. MUDr. Mojmír Račanský Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL
 Bronchial asthma MUDr. Mojmír Račanský Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL DEFINITION ASTHMA BRONCHIALE = Asthma is a chronic inflammatory disorder of the airways in which
Bronchial asthma MUDr. Mojmír Račanský Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL DEFINITION ASTHMA BRONCHIALE = Asthma is a chronic inflammatory disorder of the airways in which
Improving Outcomes in the Management & Treatment of Asthma. April 21, Spring Managed Care Forum
 Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
ASTHMA IN THE PEDIATRIC POPULATION
 ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION
 POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2018 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2018 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide
 VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
Exercise-Induced Bronchospasm. Michael A Lucia, MD, FCCP Asst Clinical Professor, UNR School of Medicine Sierra Pulmonary & Sleep Institute
 Exercise-Induced Bronchospasm Michael A Lucia, MD, FCCP Asst Clinical Professor, UNR School of Medicine Sierra Pulmonary & Sleep Institute EIB Episodic bronchoconstriction with exercise May be an exacerbation
Exercise-Induced Bronchospasm Michael A Lucia, MD, FCCP Asst Clinical Professor, UNR School of Medicine Sierra Pulmonary & Sleep Institute EIB Episodic bronchoconstriction with exercise May be an exacerbation
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma
 with asthma") Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016
 Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Respiratory Therapy. Medical/Scientific/General Background
 Respiratory Therapy Medical/Scientific/General Background Marketing Europe Dr. Rainer Jakobs PMM Europe 1 Dr. Rainer Jakobs, PMM Europe RT Medical/Scientific/General Background 2 Dr. Rainer Jakobs, PMM
Respiratory Therapy Medical/Scientific/General Background Marketing Europe Dr. Rainer Jakobs PMM Europe 1 Dr. Rainer Jakobs, PMM Europe RT Medical/Scientific/General Background 2 Dr. Rainer Jakobs, PMM
Pharmacology of drugs used in bronchial asthma & COPD
 Pharmacology of drugs used in bronchial asthma & COPD By Prof. Hanan Hagar Pharmacology Unit King Saud University ILOs: The students should be able to 1. Different types of drugs used for treatment of
Pharmacology of drugs used in bronchial asthma & COPD By Prof. Hanan Hagar Pharmacology Unit King Saud University ILOs: The students should be able to 1. Different types of drugs used for treatment of
Allergies and Asthma 5/21/2013. Objectives. Allergic Rhinitis (AR): Risk Factor for ASTHMA. Rhinitis and Asthma
: Risk Factor for ASTHMA. Rhinitis and Asthma") Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
Asthma: Chronic Management. Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015
 Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
FIGURE 17. USUAL DOSAGES FOR LONG-TERM CONTROL MEDICATIONS*
 FIGURE 17. USUAL DOSAGES FOR LONG-TERM CONTROL MEDICATIONS* 0 4 Years Age and Adults Potential Adverse Effects Inhaled Corticosteroids (See Figure 18, Estimated Comparative Daily Dosages for ICSs. ) Oral
FIGURE 17. USUAL DOSAGES FOR LONG-TERM CONTROL MEDICATIONS* 0 4 Years Age and Adults Potential Adverse Effects Inhaled Corticosteroids (See Figure 18, Estimated Comparative Daily Dosages for ICSs. ) Oral
Meeting the Challenges of Asthma
 Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Drugs acting on the respiratory tract
 Drugs acting on the respiratory tract Antiasthmatic drugs Asthma Asthma is a chronic inflammatory disease characterized by episodes of reversible airways obstruction due to bronchial hyperresponsiveness;
Drugs acting on the respiratory tract Antiasthmatic drugs Asthma Asthma is a chronic inflammatory disease characterized by episodes of reversible airways obstruction due to bronchial hyperresponsiveness;
ASTHMA PROTOCOL CELLO
 ASTHMA PROTOCOL CELLO Leiden May 2011 1 Introduction This protocol includes an explanation of the clinical picture, diagnosis, objectives, non medical and medical therapy and a scheme for inhaler dosage.
ASTHMA PROTOCOL CELLO Leiden May 2011 1 Introduction This protocol includes an explanation of the clinical picture, diagnosis, objectives, non medical and medical therapy and a scheme for inhaler dosage.
Q. What are metered-dose inhalers? A. These are devices that dispense medicines directly into the lungs, in the form of a mist or aerosol in a
 1 2 Q. What are metered-dose inhalers? A. These are devices that dispense medicines directly into the lungs, in the form of a mist or aerosol in a specific dosage. In an MDI, the medicine is suspended
1 2 Q. What are metered-dose inhalers? A. These are devices that dispense medicines directly into the lungs, in the form of a mist or aerosol in a specific dosage. In an MDI, the medicine is suspended
Pathology of Asthma Epidemiology
 Asthma A Presentation on Asthma Management and Prevention What Is Asthma? A chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Nighttime or early morning coughing Pathology
Asthma A Presentation on Asthma Management and Prevention What Is Asthma? A chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Nighttime or early morning coughing Pathology
How can I benefit most from my COPD medications?
 Fact Sheet: COPD Medications and Delivery Devices How can I benefit most from my COPD medications? COPD medications can improve your symptoms. By taking the right medication at the right time, you can
Fact Sheet: COPD Medications and Delivery Devices How can I benefit most from my COPD medications? COPD medications can improve your symptoms. By taking the right medication at the right time, you can
Asthma. The prevalence of asthma has been increasing worldwide, but why this is happening is not known.
 Asthma What is asthma? Asthma is a chronic disorder of the airways of the lungs. The airways are reactive and may be inflamed even when symptoms are not present. The extent and severity of airway irritation
Asthma What is asthma? Asthma is a chronic disorder of the airways of the lungs. The airways are reactive and may be inflamed even when symptoms are not present. The extent and severity of airway irritation
Ivax Pharmaceuticals UK Sponsor Submission to the National Institute for Health and Clinical Excellence
 Ivax Pharmaceuticals UK Sponsor Submission to the National Institute for Health and Clinical Excellence Clinical and cost-effectiveness of QVAR for the treatment of chronic asthma in adults and children
Ivax Pharmaceuticals UK Sponsor Submission to the National Institute for Health and Clinical Excellence Clinical and cost-effectiveness of QVAR for the treatment of chronic asthma in adults and children
ASTHMA BEST PRACTICES FOR SCHOOL NURSES. School Nurses November 2015
 ASTHMA BEST PRACTICES FOR SCHOOL NURSES School Nurses November 2015 1 BACKGROUND AND CURRENT STATS General definitions and explanations 2 Incidence of Asthma Centers for Disease Control (CDC) - 1 in 12
ASTHMA BEST PRACTICES FOR SCHOOL NURSES School Nurses November 2015 1 BACKGROUND AND CURRENT STATS General definitions and explanations 2 Incidence of Asthma Centers for Disease Control (CDC) - 1 in 12
(Asthma) Diagnosis, monitoring and chronic asthma management
 Diagnosis, monitoring and chronic asthma management") Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Asthma. Don Hayes, Jr., MD, FAAP, FACP
 Asthma Don Hayes, Jr., MD, FAAP, FACP Director, University of Kentucky Asthma Center Kentucky Children s Hospital & Assistant Professor of Pediatrics & Internal Medicine University of Kentucky College
Asthma Don Hayes, Jr., MD, FAAP, FACP Director, University of Kentucky Asthma Center Kentucky Children s Hospital & Assistant Professor of Pediatrics & Internal Medicine University of Kentucky College
Key features and changes to these four components of asthma care include:
 Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Practical Approach to Managing Paediatric Asthma
 Practical Approach to Managing Paediatric Asthma Dr Andrew Tai FRACP, PhD Paediatric Respiratory and Sleep Specialist Women's and Children's Hospital, Adelaide Approaching the patient Check the diagnosis
Practical Approach to Managing Paediatric Asthma Dr Andrew Tai FRACP, PhD Paediatric Respiratory and Sleep Specialist Women's and Children's Hospital, Adelaide Approaching the patient Check the diagnosis
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER
 MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
Effective Date: 4/27/2016 Version: 1.0 Approval By: CCC Clinical Delivery Steering Planned Review Date: 4/27/2017
 Protocol Title: Adult Asthma Protocol Effective Date: 4/27/2016 Version: 1.0 Approval By: CCC Clinical Delivery Steering Planned Review Date: 4/27/2017 1 Purpose & Objective This protocol provides evidence-based
Protocol Title: Adult Asthma Protocol Effective Date: 4/27/2016 Version: 1.0 Approval By: CCC Clinical Delivery Steering Planned Review Date: 4/27/2017 1 Purpose & Objective This protocol provides evidence-based
Getting Asthma treatment right. Dr David Cremonesini Specialist Pediatrician American Hospital
 Getting Asthma treatment right Dr David Cremonesini Specialist Pediatrician American Hospital cdavid@ahdubai.com } Consultant Paediatrician from UK of 5.5 years } Speciality in Allergy / Asthma (PG Certificate)
Getting Asthma treatment right Dr David Cremonesini Specialist Pediatrician American Hospital cdavid@ahdubai.com } Consultant Paediatrician from UK of 5.5 years } Speciality in Allergy / Asthma (PG Certificate)
Get Healthy Stay Healthy
 Asthma Management WHAT IS ASTHMA? Asthma causes swelling and inflammation in the breathing passages that lead to your lungs. When asthma flares up, the airways tighten and become narrower. This keeps the
Asthma Management WHAT IS ASTHMA? Asthma causes swelling and inflammation in the breathing passages that lead to your lungs. When asthma flares up, the airways tighten and become narrower. This keeps the
Ventamol CFC-Free 100 micrograms, Pressurised Inhalation, Suspension (Salbutamol)
") Ventamol CFC-Free 100 micrograms, Pressurised Inhalation, Suspension (Salbutamol) For inhalation use Important: Read instructions carefully Wash your inhaler once a week and allow to dry What you need
Ventamol CFC-Free 100 micrograms, Pressurised Inhalation, Suspension (Salbutamol) For inhalation use Important: Read instructions carefully Wash your inhaler once a week and allow to dry What you need
Impact of Asthma in the U.S. per Year. Asthma Epidemiology and Pathophysiology. Risk Factors for Asthma. Childhood Asthma Costs of Asthma
 American Association for Respiratory Care Asthma Educator Certification Prep Course Asthma Epidemiology and Pathophysiology Robert C. Cohn, MD, FAARC MetroHealth Medical Center Cleveland, OH Impact of
American Association for Respiratory Care Asthma Educator Certification Prep Course Asthma Epidemiology and Pathophysiology Robert C. Cohn, MD, FAARC MetroHealth Medical Center Cleveland, OH Impact of
Objectives. Asthma in Primary Care. Definition. Epidemiology. Pathophysiology
 Objectives Asthma in Primary Care Jed Grant, PA-C Program Director, SJVC PA Program Staff PA, AMCH Emergency Department Apply the NAEPP guideline measures of severity and control including current impairment
Objectives Asthma in Primary Care Jed Grant, PA-C Program Director, SJVC PA Program Staff PA, AMCH Emergency Department Apply the NAEPP guideline measures of severity and control including current impairment
Treatment of Acute Asthma Exacerbations in Adults in the Primary Care or Urgent Care Setting Clinical Practice Guideline MedStar Health.
 Treatment of Acute Asthma Exacerbations in Adults in the Primary Care or Urgent Care Setting Clinical Practice Guideline MedStar Health Background: These guidelines are provided to assist physicians and
Treatment of Acute Asthma Exacerbations in Adults in the Primary Care or Urgent Care Setting Clinical Practice Guideline MedStar Health Background: These guidelines are provided to assist physicians and
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL
 DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007
 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Position within the Organisation
 ASTHMA TREATMENT GUIDELINES Document Description Document Type Service Application Guidelines All healthcare professionals(hcps) caring for patients with asthma Version 4.0 Ratification date September
ASTHMA TREATMENT GUIDELINES Document Description Document Type Service Application Guidelines All healthcare professionals(hcps) caring for patients with asthma Version 4.0 Ratification date September
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al.
 Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma
Respiratory Pharmacology PCTH 400 Asthma and β-agonists
 Respiratory Pharmacology PCTH 400 Asthma and β-agonists Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Director, Centre of
Respiratory Pharmacology PCTH 400 Asthma and β-agonists Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Director, Centre of
Disclosure. Case. Objectives. Case Continued. Inhalers. Asthma: A GINA Update to the NAEPP 2007 Guidelines 1/20/2015
 Disclosure Asthma: A GINA Update to the NAEPP 2007 Guidelines Robert (RC) Hellinga, Pharm.D. PGY 1 Pharmacy Resident Wolfson Children s Hospital/Baptist Health I do not have a vested interest in or affiliation
Disclosure Asthma: A GINA Update to the NAEPP 2007 Guidelines Robert (RC) Hellinga, Pharm.D. PGY 1 Pharmacy Resident Wolfson Children s Hospital/Baptist Health I do not have a vested interest in or affiliation
ASTHMA PRESCRIBING GUIDELINES FOR ADULTS AND CHILDREN OVER 12
 North Hampshire CCG Asthma Prescribing Guidelines June 2015 ASTHMA PRESCRIBING GUIDELINES FOR ADULTS AND CHILDREN OVER 12 These guidelines are based on the British Thoracic Society (BTS) and Scottish Intercollegiate
North Hampshire CCG Asthma Prescribing Guidelines June 2015 ASTHMA PRESCRIBING GUIDELINES FOR ADULTS AND CHILDREN OVER 12 These guidelines are based on the British Thoracic Society (BTS) and Scottish Intercollegiate
Childhood Asthma. The pathophysiology of asthma is an interplay. CME Case Study. Case Study. By Moyez B. Ladhani, MD, CCFP, FAAP, FRCPC
 CME Case Study Childhood Asthma By Moyez B. Ladhani, MD, CCFP, FAAP, FRCPC Case Study A two-year-old child presents to your office with a cough, which has been present for three weeks. It is worse at nighttime
CME Case Study Childhood Asthma By Moyez B. Ladhani, MD, CCFP, FAAP, FRCPC Case Study A two-year-old child presents to your office with a cough, which has been present for three weeks. It is worse at nighttime
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD