Taking Control of Asthma Through Proper Medication Selection and the Use of Asthma Action Plans Julie M. Koehler, Pharm.D., FCCP
|
|
|
- Wilfrid Tucker
- 6 years ago
- Views:
Transcription
1 Taking Control of Asthma Through Proper Medication Selection and the Use of Asthma Action Plans Julie M. Koehler, Pharm.D., FCCP Associate Dean for Clinical Education and External Affiliations & Professor of Pharmacy Practice, Butler University College of Pharmacy & Health Sciences & Ambulatory Care Clinical Pharmacist, Adult Ambulatory Care Center / Methodist Hospital, Indiana University Health
2 Objectives State the general recommendations for stepwise approach to asthma therapy as recommended by the 2007 NIH guidelines put forth by the NAEPP. Applying the 2007 NIH NAEPP guidelines, formulate a patient-specific therapeutic plan for both initial and ongoing medication therapy management of a patient with chronic asthma. Given the frequency of day and nighttime symptoms, classify a patient s asthma as either well controlled, not well controlled, or very poorly controlled, according to the 2007 NIH NAEPP guidelines.
3 Objectives Discuss the general process for providing asthma education: Explain what is meant by good asthma control; Explain how and when to take asthma medications; Explain how to monitor asthma symptoms and level of asthma control; and Develop a patient-provider partnership in asthma care through the use of the written Asthma Action Plan.
4 Asthma Statistics 7 million children and 18.7 million adults with asthma in the U.S. 1 in 13 children and 1 in 11 adults in Indiana >30,000 ED visits per year in Indiana related to asthma in 2010; 38% among children >8,000 asthma-related hospitalizations in 2010 Hospitalization (4x) and death (2.5x) more likely in African Americans 44.7% of school-age children with asthma missed school due to poor asthma control between 2006 and % of adults with asthma in Indiana missed work or experienced limitations in activities due to poor asthma control in 2010 Only 47.7% of children and 28.6% of adults with asthma in Indiana had a written Asthma Action Plan during
5 Initial Classification of Asthma Severity Severity = Intrinsic intensity of the disease Must consider: Impairment (Present) Frequency and intensity of symptoms Impact on quality of life Risk (Future) Exacerbations Loss of pulmonary function Risk of ADRs Clinically, classification of severity is most useful for initiating controller therapy
6 Classification of Severity: 1997/2002 vs NIH Recommendations 1997/2002 (EPR-2) Mild Intermittent 2007 (EPR-3) Intermittent Mild Persistent Mild Persistent Moderate Persistent Moderate Persistent Severe Persistent Severe Persistent
7 Perception of Risk of Death from Childhood Asthma is Underestimated Clinical Assessment of Asthma Severity in Children with Asthma Who Died Deaths (%) Mild Moderate Severe Robertson CF et al. Pediatr Pulmonol 1992; 13:
8 Goals of Therapy: Decreasing Impairment Prevent symptoms No need for reliever medications (2x or less per week) No daytime symptoms (2x or less per week) No nighttime symptoms (2x or less per week) Maintain normal pulmonary function Maintain normal activity/lifestyle No limitations in daily activities No limitations in exercise Meet patients and families expectations EPR-3
9 Goals of Therapy: Decreasing Risk Prevent recurrent exacerbations Decrease ED visits and hospitalizations Prevent progressive loss of lung function Achieve maximal pharmacotherapeutic benefit with minimal side effects / ADRs EPR-3
10 1997 NIH Asthma Guidelines: Concepts Still Applicable Today NEW CONCEPTS INTRODUCED IN 1997 Major emphasis on: Meeting patients expectations Providing patient education Developing a written, long-term action plan Using peak flow meters Avoiding asthma triggers
11 1997 NIH Asthma Guidelines: Concepts Still Applicable Today NEW CONCEPTS INTRODUCED IN 1997 New classification of drugs: quick relief vs. bronchodilators long-term control vs. anti-inflammatories Quick relief drugs are for TREATMENT! Long-term control drugs are for PREVENTION!
12 Classification of Meds Quick Relief Short-Acting ß 2 - Agonists Anticholinergics Systemic Corticosteroids Long-Term Control Inhaled Corticosteroids Mast Cell Stabilizers Long-Acting ß 2 -Agonists Methylxanthines Leukotriene modifiers Immunomodulators
13 General Approach to Treatment: Focus on Long-Term Control Inflammation plays a primary role in the pathogenesis of asthma Prevention and suppression of underlying inflammation: reduction of bronchial hyperresponsiveness prevention of airway remodeling improvement in long-term control and outcomes
 600 mcg b.i.d. Laitinen. J Allergy Clin Immunol.1992;90:32-42.")
14 Effects of Inhaled Corticosteroids on Inflammation E = Epithelium BM = Basement Membrane Pre and post 3-month treatment with budesonide (BUD) 600 mcg b.i.d. Laitinen. J Allergy Clin Immunol.1992;90:32-42.
15 Corticosteroids Inhaled Beclomethasone dipropionate (QVAR ) Budesonide (Pulmicort Flexhaler TM, Pulmicort Respules ) Ciclesonide (Alvesco ) Flunisolide (Aerobid, Aerospan ) Fluticasone (Flovent Diskus, Flovent HFA) Mometasone furoate (Asmanex ) Combination products containing steroid + LABA (Advair Diskus, Advair HFA, Symbicort, Dulera ) Systemic Methylprednisolone (Solu-Medrol, Medrol ) Prednisolone (Prelone, Orapred, Orapred ODT, Pediapred ) Prednisone (Deltasone )
16 Corticosteroid Indications Inhaled CS Long-term prevention of symptoms in mild, moderate, and severe persistent asthma Suppression, control, and reversal of inflammation Reduction of need for systemic CS Systemic CS Long-term prevention of symptoms in severe persistent asthma
17 Corticosteroid Mechanism of Action Anti-inflammatory Action: reduction in synthesis and release of proinflammatory cytokines reduction in inflammatory cell activation, recruitment, and infiltration reduction in vascular permeability Effect on Beta-receptors: increase in number of receptors improve receptor responsiveness to adrenergic stimulation
18 Growth Suppression with Inhaled Corticosteroids Precaution in PI of INH CS about possible growth suppression More likely with higher doses Is adult height affected? (i.e., does catchup growth occur?) Recommend use of lowest effective dose
19 Growth Suppression with Inhaled Corticosteroids 142 budesonide-treated children with asthma followed for average of nine years until adult height attained Compared to two control groups Significantly less growth noted during first two years of treatment with budesonide No overall differences in mean adult height noted Agertoft J, Pederson S. N Engl J Med 2000; 343: patients randomized to receive budesonide, nedocromil, or placebo x 4-6 yrs; followed for average of eight years until adult height attained (mean age 25 yrs) Significantly less growth noted during first two years of treatment with budesonide Mean adult height significantly lower (1.2cm) in budesonide group Kelly HW et al. N Engl J Med 2012 Sep 3; [Epub ahead of print].
20 Adverse Effects of CS Cough, dysphonia Oral thrush (candidiasis) Systemic effects (more likely to occur with high-dose corticosteroids) adrenal suppression/growth suppression osteoporosis skin thinning/easy bruising weight gain/fluid retention
21 Tips for CS Users Benefits of INH CS generally outweigh potential risks of adverse effects To reduce adverse effect potential: Administer INH CS with spacer (if using MDI)! Rinse mouth thoroughly following inhalation! Use lowest effective CS dose Consider adding a long-acting beta-agonist to low-tomed. dose of INH CS before maximizing INH CS dose Monitor growth in children Consider osteoporosis prophylaxis in adults
22 Available Product: cromolyn sodium (Intal ) Indications: Mast Cell Stabilizers Long-term prevention of symptoms Preventive treatment prior to exposure to exercise or known allergen Anti-inflammatory Mechanisms: stabilize mast cell membranes inhibit activation and release of inflammatory mediators from eosinophils block early and late reaction to allergen inhibit acute response to exercise, cold air, sulfur dioxide
23 Mast Cell Stabilizers Overall, extremely well-tolerated 15% to 20% of patients complained of unpleasant taste with nedocromil (removed from market due to low use) Overall, safety profile has been cited as the primary advantage of these agents...
24 Mast Cell Stabilizers Effective anti-inflammatory agents for mildpersistent asthma Have been used as alternatives to INH CS in patients where there is concern for toxicity (e.g., in pediatric patients) Can be used for exercise- or known allergeninduced bronchospasm Lack of recent evidence to suggest benefit over INH CS, or INH CS + other Tx; therefore, not preferred treatment (EPR-3)
25 Long-Acting Beta 2 -Agonists Products Approved for Asthma: Salmeterol (Serevent ) Formoterol (Foradil ) Albuterol Sustained-Release Tablets* Indications for Salmeterol & Formoterol: Long-term prevention of symptoms (especially nocturnal symptoms) IN ADDITION TO ANTI- INFLAMMATORY AGENTS Prevention of exercise-induced bronchospasm *Inhaled long-acting Beta 2 -Agonists are preferred over sustained-release tablets due to fewer side effects and longer duration of action.
26 Albuterol vs LABA s: Pharmacokinetics Albuterol Salmeterol Formoterol Onset 5 min 20 min 5 min? Duration 4-8 hrs 12 hrs 12 hrs LABA s should not be used to treat acute symptoms!
27 Salmeterol + Beclomethasone: Early Evidence of Benefit Salmeterol 50mcg bid + Beclomethasone 200mcg bid vs Beclomethasone 500mcg bid Similar asthma exacerbation frequency Greater improvement in salmeterol + beclomethasone group: Symptoms of asthma Symptoms requiring additional bronchodilators PEFR in am and pm nocturnal awakening Greening et al., Lancet 1994
28 Salmeterol + Beclomethasone Change in PEF (L/min) Change in PEF (am & pm) Over 6 Months Sal/Bec AM Sal/Bec PM Bec AM Bec PM Weeks of Treatment Greening et al., Lancet 1994
29 Salmeterol + Beclomethasone: Defining the role of LABA s CONCLUSION Adding a long-acting ß 2 -adrenergic agonist to INH CS treatment may be more effective than increasing the dose of INH CS. Greening et al., Lancet 1994
30 Salmeterol + Fluticasone Propionate (FP) vs Increased-Dose FP Salmeterol 42 mcg b.i.d. + FP 88 mcg b.i.d. (n = 221) FP 88 mcg b.i.d. (n = 437) Follow-up 2-4 week run-in FP 220 mcg b.i.d. (n = 216) 6-month treatment period Condemi JJ, et al. Ann Allergy Asthma Immunol. 1999;82:
31 AM Peak Expiratory Flow Salmeterol 42 mcg b.i.d. + FP 88 mcg b.i.d. FP 220 mcg b.i.d * * * * * 40 * *P < Condemi JJ, et al. Ann Allergy Asthma Immunol. 1999;82: Weeks of Treatment
32 Percent of Days Without Albuterol Days Without Albuterol (%) Salmeterol 42 mcg b.i.d. + FP 88 mcg b.i.d. * * * * FP 220 mcg b.i.d. * * *P < Condemi JJ, et al. Ann Allergy Asthma Immunol. 1999;82: Weeks of Treatment
33 Change in Percent of Symptom-Free Days Salmeterol + FP 88 mcg b.i.d. FP 220 mcg b.i.d * * * 10 *P P < Condemi JJ, et al. Ann Allergy Asthma Immunol. 1999;82: Weeks of Treatment
34 LABA Use in Children Salmeterol (Serevent Diskus ) FDA approved for prevention of bronchospasm and EIB in children as young as 4 years of age Dosage: one inhalation every 12 hours Formoterol (Foradil Aerolizer TM ) FDA approved for prevention of bronchospasm and EIB in children as young as 5 years of age Dose: one 12mcg capsule via inhalation every 12 hours
35 Current Controversy in Asthma Management: LABA Safety Profile Salmeterol Multi-center Asthma Research Trial (SMART) Compared the safety of salmeterol to placebo in patients with asthma over the course of 28 weeks RESULTS: Death-Rate Salmeterol-treated group: 13/13,176 patients Placebo-treated group: 3/13,179 patients Difference not significant Trial discontinued early CONCLUSION: Salmeterol may increase the risk of asthma-related death
36 SMART Results: Important Considerations Differences in Ethnic Groups: 71% of the study population were Caucasian No significant difference in deaths between salmeterol vs. placebo 17% of the study population were African American Statistically significant greater number of events (including death) in salmeterol treated group vs. placebo More severe asthma at baseline in African American group
37 SMART Results: Important Considerations Differences in Use of Inhaled Corticosteroids: 47% overall; 50% Caucasians; 38% African Americans No significant difference in deaths among those receiving inhaled corticosteroids Statistically significant difference (salmeterol > placebo) in those NOT receiving inhaled corticosteroids
38 Current Controversy in Asthma Management: LABA Safety Profile The Black Box Warning: LABA s should ONLY be used as additional therapy for patients not adequately controlled on other asthmacontroller medications LABA s are NOT a substitute for inhaled corticosteroids LABA s should NOT be used to treat acute symptoms LABA s should NOT be initiated in patients with significantly worsening or acutely deteriorating asthma, which may be a life-threatening condition
39 Most Recent FDA Advisory on LABA Use Issued Feb. 18, 2010 The use of LABAs is contraindicated without the use of an asthma controller medication such as inhaled corticosteroid. Single-agent LABAs should only be used in combination with an asthma controller medication; they should not be used alone; LABAs should only be used long-term in patients whose asthma cannot be adequately controlled on asthma controller medications; LABAs should be used for the shortest duration of time required to achieve control of asthma symptoms and discontinued, if possible, once asthma control is achieved. Patients should then be maintained on an asthma controller medication. Pediatric and adolescent patients who require a LABA in addition to an inhaled corticosteroid should use a combination product containing both an inhaled corticosteroid and a LABA to ensure compliance with both medications.
40 Post-EPR-3 Study on LABA Use in Children In a RDB triple-crossover trial, three step-up therapies evaluated in 165 children, ages 6 17 years who were poorly controlled on low-dose fluticasone (100mcg BID) alone: Step-up ICS to fluticasone 250mcg BID Low-dose ICS plus step-up with LABA 50mcg daily Low-dose ICS plus step-up with LTRA 5-10mg daily Primary Outcome = composite of change in FEV1, oral steroid use, and # of asthma-control days Results: 98% of children experienced improved asthma control; LABA best overall Tx response LABA vs. LTRA, 52% vs. 34% LABA vs. ICS, 54% vs. 32% Lemanske RF Jr et al. N Engl J Med. 2010;362:975.
41 Methylxanthines Available Products: Theophylline (sustained-release tablets and capsules) Indications: Long-term control and prevention of symptoms, especially nocturnal symptoms Mechanism: smooth muscle relaxation/bronchodilation via inhibition of phosphodiesterase
42 Potential Adverse Effects of Methylxanthines Effects associated with therapeutic doses: Insomnia GI upset/potentiation of gastroesophageal reflux possible hyperactivity in children Effects associated with toxic doses (dose-related): tachycardia, tachyarrhythmias nausea and vomiting CNS stimulation headache seizures hypokalemia
43 Methylxanthines: Place in Therapy Due to availability of better agents, theophylline is considered a third/last-line (adjunctive) drug Overall, relatively weak bronchodilating properties Lacks clinically important anti-inflammatory properties (?) Difficult to use: numerous potential drug interactions serum concentration monitoring mandatory (narrow therapeutic range: 5-15mcg/mL)
44 Leukotriene Modifiers Available Products: Zafirlukast (Accolate ) Zileuton (Zyflo, Zyflo CR TM ) Montelukast (Singulair ) Indication: Long-term control and prevention of symptoms in persistent asthma
45 Leukotriene Pathway 5-Lipoxygenase Zileuton (Zyflo, Zyflo CR TM ) Arachidonic Acid LTA 4 FLAP LTB 4 LTC 4 LTD 4 LTE 4 Chemotaxis Immunomodulation Zafirlukast (Accolate ) Montelukast (Singulair ) Bronchoconstriction Mucus secretion Edema Hyperresponsiveness Eosinophilia Holgate ST et al. J Allergy Clin Immunol 1996; 98: 1-13.
46 Drug Inter actions General Comparison of Leukotriene Modifiers Consideration Zafirlukast Zileuton Montelukast (Accolate ) (Zyflo, Zyflo CR TM ) (Singulair ) Age > 5 years > 12 years > 1 year Usual Dose 20mg bid (adults and children > 12 yrs); 10 mg bid (children 5-11 yrs) 600 mg qid (immed. release) 1200 mg bid (controlled release) 10mg qhs(adults) 5mg chewable qpm (kids 6-14 yrs); 4mg chewable or granules qpm (kids 1-5 yrs) None Warnings? Churg-Strauss Increased LFTs? LFTs (monitoring req d) Metabolism P450: 3A4, 2C9 P450: 1A2, 3A4, 2C9 P450: 3A4, 2C9 Dosing Considerations Empty stomach (food abs 40%) Within 1 hr of meals (CR) None
47 Low-Dose Fluticasone vs. Oral Montelukast for First-Line Treatment of Persistent Asthma Fluticasone 44 mcg b.i.d. (MDI) Run-in (n = 271) Pts remaining symptomatic while taking short-acting betaagonists Montelukast 10 mg daily (n = 262) 8-14 days Busse W, et al. J Allergy Clin Immunol 2001;107: weeks
48 Low-Dose Fluticasone vs. Oral Montelukast for First-Line Treatment of Persistent Asthma Fluticasone Montelukast * * * * * * * Baseline Treatment Week Busse W, et al. J Allergy Clin Immunol 2001;107: *P < 0.001
49 Salmeterol vs Oral Montelukast in Patients Using ICS ICS therapy for > 30 days prior to randomization Run-in Salmeterol 50 mcg b.i.d. (powder) + ICS n = 236 Montelukast 10 mg daily + ICS n = Weeks 12 Weeks Fish J, et al. Am J Respir Crit Care Med 2000; :A203.
50 AM PEFR Change From Baseline (L/min) * * * * * * * * Salmeterol * * Montelukast 0 *P < Weeks Fish J, et al. Am J Respir Crit Care Med. 2000; :A203. * *
51 Leukotriene Modifiers: Place in Therapy Possible initial therapy in mild persistent asthma as an alternative to INH CS or cromolyn Not superior to INH CS alone Possible adjunctive therapy in addition to INH CS at any level of asthma severity Not superior to LABA when combined with INH CS May be useful in children or adults with poor inhaler technique, or in younger children in whom LABA are not indicated
52 Immunomodulator Therapy: Omalizumab (Xolair ) First humanized antibody for treatment of asthma; approved by the FDA in June 2003 Indicated for adults and adolescents (12 years of age or older) with moderate-to-severe persistent asthma who: have had a positive skin test to a perennial aeroallergen, and have symptoms that are inadequately controlled with inhaled corticosteroids
53 Omalizumab (Xolair ): Mechanism of Action A recombinant DNA-derived humanized monoclonal antibody that selectively binds to human immunoglobulin E (IgE) Inhibits binding of IgE to high-affinity IgE receptors on the surface of mast cells and basophils, resulting in a decrease in the release of allergic response mediators May also reduce the number of high-affinity IgE receptors present on basophils
54 Omalizumab (Xolair ): Dosing and Administration 150 to 375mg subcutaneously every 2 to 4 weeks Dose and frequency determined by the serum total IgE level (IU/mL), measured before the start of treatment, and body weight (kg)
55 Omalizumab (Xolair ): Adverse Effects Malignancy (0.5% vs. 0.2% control) most patients observed for less than one year impact of long-term administration in higher risk patients unknown Anaphylaxis (<0.1%; 3 patients in pre-marketing clinical trials) Several post-marketing case reports Black Box Warning w/in 2 hrs of first or subsequent administration observation following injection required Other: injection site reaction (5-20%)
56 Omalizumab (Xolair ): Evidence-Based Medicine Pooled analysis of 3 multicenter, RDBCT (phase III) Adults/ adolescents: n=1071; Children, ages 6-12 (n=334) Inclusion: moderate-to-severe allergic asthma of at least one year duration total serum IgE level between 30 and 700 IU/mL (adolescents/adults), or 30 and 1300 IU/mL (children) positive skin prick test to dustmite, cockroach, dog, or cat J Allergy Clin Immunol 2003;111:87-90.
57 Omalizumab (Xolair ): Evidence-Based Medicine Intervention: Randomization: Omalizumab or placebo injections (subq) every 2-4 weeks Steroid-Stable Phase: Dosages of inhaled beclomethasone dipropionate (INH BDP) kept stable over first 16 weeks Steroid-Reduction Phase: INH BDP dosages reduced x 25% every two weeks over an eight week period, with the lowest effective dose maintained over for a further four weeks J Allergy Clin Immunol 2003;111:87-90.
58 Steroid-Stable Phase Exacerbations (% patients) P =.009 P <.001 P =.095 P <.001 Study 008 Study 009 Study 010 All studies Omalizumab Placebo J Allergy Clin Immunol 2003;111:87-90.
59 Steroid-Reduction Phase Exacerbations ( % patients ) P =.004 P <.001 P <.001 P <.001 Study 008 Study 009 Study 010 All studies Omalizumab Placebo J Allergy Clin Immunol 2003;111:87-90.
60 Results: Omalizumab (Xolair ): Evidence-Based Medicine Rate of unscheduled, asthma-related outpatient visits lower for omalizumab (rate ratio [95% CI], 0.60 [0.44,0.81];P < 0.01) Rate of asthma-related ED visits lower for omalizumab (rate ratio [95% CI], 0.47 [0.24,1.01];P = 0.05) Hospitalizations reduced in omalizumab group (rate ratio [95% CI], 0.08 [0.00,0.25];P < 0.01) J Allergy Clin Immunol 2003;111:87-90.
61 Comparison of Omalizumab to Standard of Care Double-blind, parallel group, multi-center study 419 patients inadequately controlled despite therapy with high-dose INH CS + LABA Randomized to receive omalizumab vs. placebo injections subq RESULTS: Omalizumab significantly reduced the rate of asthma exacerbations and ED visits vs. placebo Humbert M, et al. Allergy 2005;60:
62 Omalizumab (Xolair ): An Emerging Treatment Option? Only for patients with known allergy-induced asthma (documented positive skin test) who are poorly controlled on inhaled corticosteroids Benefit of reduced steroid dosage relative to total cost of therapy unclear Estimated cost: $ $10,000 per year! Risk of anaphylaxis must be considered Role of omalizumab better defined in new NIH asthma guidelines: After treatment has been maximized with high-dose INH CS + LABA



63 NAEPP Expert Panel Report Guidelines (EPR-3): Where are we today? National Asthma Education and Prevention Program. Executive summary of the NAEPP expert panel report (EPR-3): Guidelines for the diagnosis and management of asthma. Bethesda, MD: U.S. Department of Health and Human Services, Public Health Service, National Institutes of Health, National Heart, Lung, and Blood Institute, Full Report Available at
64 STEPWISE APPROACH FOR MANAGING ASTHMA IN YOUTHS > 12 YEARS AND ADULTS Intermittent Asthma Persistent Asthma: Daily Medication Consult with asthma specialist if step 4 or higher care is required Consider consultation at step 3 Quick-Relief Medication for All Patients SABA as needed for symptoms. Intensity of treatment depends on severity of symptoms: up to 3 treatments at 20-minute intervals as needed. Short course of systemic oral corticosteroids may be needed. Use of beta 2 -agonist >2 days a week for symptom control (not prevention of EIB) indicates inadequate control and the need to step up treatment. Step 1 Preferred: SABA prn Step 2 Preferred: Low-dose ICS Alternative: LTRA Cromolyn Theophylline Step 3 Preferred: Med-dose ICS OR Low-dose ICS+ either LABA, LTRA, Theophylline Or Zileutin Step 4 Preferred: Medium-dose ICS+LABA Alternative: Medium-dose ICS+either LTRA, Theophylline Or Zileutin Step 5 Preferred: High dose ICS + LABA AND Consider Omalizumab for patients with allergies Step 6 Preferred: High-dose ICS + LABA + oral Corticosteroid AND Consider Omalizumab for patients with allergies Step up if needed (check adherence, environmental control and comorbidities) Assess Control Step down if possible (if asthma well controlled for 3 months) Patient Education and Environmental Control at Each Step EPR-3
65 STEPWISE APPROACH FOR MANAGING ASTHMA IN CHILDREN 5-11 YEARS OF AGE Intermittent Asthma Persistent Asthma: Daily Medication Consult with asthma specialist if step 4 or higher care is required Consider consultation at step 3 Quick-Relief Medication for All Patients SABA as needed for symptoms. Intensity of treatment depends on severity of symptoms: up to 3 treatments at 20-minute intervals as needed. Short course of systemic oral corticosteroids may be needed. Use of beta 2 -agonist >2 days a week for symptom control (not prevention of EIB) indicates inadequate control and the need to step up treatment. Step 1 Preferred: SABA prn Step 2 Preferred: Low-dose ICS Alternative: LTRA Cromolyn Theophylline Step 3 Preferred : Low-dose ICS + either LABA, LTRA, or Theophylline OR Medium-dose ICS Step 4 Preferred: Medium-dose ICS+LABA Alternative: Medium-dose ICS+either LTRA, or Theophylline Step 5 Preferred: High dose ICS + LABA Alternative: High-dose ICS+ either LTRA or Theophylline Step 6 Preferred: High-dose ICS + LABA + oral Corticosteroid Alternative: High-dose ICS +either LTRA or Theophylline + oral corticosteroid Step up if needed (check adherence, environmental control and comorbidities) Assess Control Step down if possible (if asthma well controlled for 3 months) Patient Education and Environmental Control at Each Step EPR-3
66 STEPWISE APPROACH FOR MANAGING ASTHMA IN CHILDREN 0-4 YEARS OF AGE Intermittent Asthma Persistent Asthma: Daily Medication Consult with asthma specialist if step 3 or higher care is required Consider consultation at step 2 Quick-Relief Medication for All Patients SABA as needed for symptoms. Intensity of treatment depends on severity of symptoms: up to 3 treatments at 20-minute intervals as needed. Short course of systemic oral corticosteroids may be needed. Use of beta 2 -agonist >2 days a week for symptom control (not prevention of EIB) indicates inadequate control and the need to step up treatment. Step 1 Preferred: SABA prn Step 2 Preferred: Low-dose ICS Alternative: LTRA Cromolyn Step 3 Preferred: Medium-dose ICS Step 4 Preferred: Medium-dose ICS AND either LTRA OR LABA Step 5 Preferred: High dose ICS AND either LTRA OR LABA Step 6 Preferred: High dose ICS AND either LTRA OR LABA AND Oral Corticosteroid Step up if needed (check adherence, environmental control ) Assess Control Step down if possible (if asthma well controlled for 3 months) Patient Education and Environmental Control at Each Step EPR-3
67 ASSESSING ASTHMA CONTROL AND ADJUSTING THERAPY IN CHILDREN 0-4 YEARS OF AGE EPR-3 IMPAIRMENT Components of Control Symptoms Nighttime awakenings Interference with normal activity SABA use Classification of Asthma Control Well Controlled Not Well Controlled Very Poorly Controlled < 2 days/week > 2 days/week Throughout the day < 1/month > 2 x/month >2x/week none Some limitation Extremely limited < 2 days/week > 2 days/week Several times/day RISK Exacerbations requiring oral steroids Treatment-related adverse effects 0-1 per year 2-3 per year > 3 per year Medication-related sides effects can vary from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk. Recommended Action For Treatment Maintain current step REGULAR FOLLOW UP EVERY 3-6 MONTHS Consider step down if well controlled at least 3 months Step up 1 step Reevaluate in 2-6 weeks If no clear benefit in 4-6 wks, consider alt. dx or adjust therapy Consider oral steroids Step up (1-2 steps) and reevaluate in 2 weeks If no clear benefit in 4-6 wks, consider alt. dx or adjust therapy
68 ASSESSING ASTHMA CONTROL AND ADJUSTING THERAPY IN CHILDREN 5-11 YEARS OF AGE EPR-3 Components of Control IMPAIRMENT Symptoms Classification of Asthma Control Well Controlled < 2 days/wk, <1/day Not Well Controlled >2 days/wk or multiple times on < 2 days/wk Very Poorly Controlled Throughout the day Nighttime awakenings Interference with normal activity SABA use < 1/month none < 2 days/week > 2 x/month Some limitation > 2 days/week >2x/week Extremely limited Several times/day FEV 1 or peak flow > 80% predicted/ 60-80% predicted/ <60% predicted/ personal best personal best personal best FEV 1 /FVC > 80% predicted 75-80% predicted <75% predicted RISK Exacerbations lung growth Treatment-related adverse effects Recommended Action For Treatment 0-1/ year > 2 / year (Consider severity and interval) Evaluation requires long-term follow up care Medication-related sides effects can vary from none to to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk. Maintain current step; consider step down if well controlled x 3mos Step up 1 step Reevaluate in 2-6 weeks Consider oral steroids Step up 1-2 steps & reevaluate in 2 wks
69 ASSESSING ASTHMA CONTROL AND ADJUSTING THERAPY IN YOUTHS > 12 YEARS OF AGE AND ADULTS EPR-3 Components of Control Symptoms Nighttime awakenings Classification of Asthma Control Well Controlled Not Well Very Poorly Controlled Controlled < 2 days/week > 2 days/week Throughout the day < 2/month 1-3/week > 4/week IMPAIRMENT RISK Interference with normal activity SABA use FEV 1 or peak flow Validated questionnaires ATAQ/ACT Exacerbations Progressive lung function Treatment-related adverse effects none Some limitation Extremely limited < 2 days/week > 2 days/week Several times/day > 80% predicted/ personal best 60-80% predicted/ personal best <60% predicted/ personal best 0/> / /< per year >2 per year Evaluation requires long-term follow up care Medication-related sides effects can vary from none to to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk. Recommended Action For Treatment Maintain current step Consider step down if well controlled x 3 mos Step up 1 step Reevaluate in 2-6 weeks Consider oral steroids Step up 1-2 steps and reevaluate in 2 weeks
70 The 4 Components of Asthma Management Measures of Asthma Assessment and Monitoring Medications Control of Environmental Factors and Comorbid Conditions That Affect Asthma Education for a Partnership in Asthma Care EPR-3
71 Involving Patients in Their Own Asthma Care Dear Patient, The most important ingredient in your asthma care is YOU. It is important for you to understand your disease, know how to recognize your symptoms, and know how and when to take your medicine. Take control of your asthma. Don t let your asthma take control of you. I am here to help you learn how YOU can take control. Sincerely, Your Respiratory Therapist
72 Education for a Partnership in Asthma Care No matter how much WE as health care providers know about asthma, effective treatment of patients can only occur if the patients also comprehend and are willing to participate in their own care. Providing asthma education and encouraging self-management is crucial. A partnership between the patient and the clinician(s) should be established to promote effective asthma management.
73 The Role of the Respiratory Care Provider as a Partner in Asthma Care Promote open communication Good communication between patient and clinician helps identify patient concerns, makes patient teaching more effective and promotes patient self-confidence to follow the treatment plan Ensure patients have a basic and ACCURATE foundation of knowledge about asthma Ensure patients understand the treatment approach Ensure patients have the self-management skills necessary to monitor the disease objectively and take medications effectively Be a sympathetic coach
74 Health Care Team Approach at Multiple Points of Care The Primary Clinician(s) Introduce(s) key educational messages and negotiate(s) agreements with patients (goals of treatment, medications, actions to take to promote asthma control, etc.) The Health Care Team Includes ALL HEALTH CARE PROFESSIONALS who encounter asthma patients through multiple points of care Should reinforce key educational messages at every opportunity Points of Care Clinic visits, ED visits, pharmacy visits, telephone calls, in community centers, in schools
75 Key Educational Messages Basic Facts About Asthma What is asthma? What is meant by good asthma control? Role of Medications Patient Skills Ability to take medications properly Ability to monitor and recognize symptoms of worsening asthma Ability to understand and utilize Written Asthma Action Plan
76 Education: What is Good Asthma CONTROL? Few daytime symptoms 2x or less per week No nighttime awakenings 2x or less per month Limited need for quick-relief medications 2x or less per week Able to engage in normal activities No limitations in daily activities No limitations in exercise **Be sure to ask about the patients and families goals and expectations!
77 Education: What is the Role of Medications? Appropriate asthma management requires the proper use of long term control and quick relief medications. Terminology (quick relief vs. long-term control) and technique (MDI vs. DPI) are important! Patients need to understand the importance of taking daily long-term control medications. Inhaled corticosteroids are the most potent and consistently effective long-term control medications for persistent asthma.
78 Education: Self-Monitoring Skills How to recognize intensity and frequency of asthma symptoms How to use peak flow meter (if prescribed) Monitor for early S/Sx of worsening asthma: Nighttime or early morning awakening Increased medication use Decreased activity tolerance
79 Proper Monitoring: Symptoms vs. PEF Measurements Depends on patient and clinician preference PEF-based plans may be particularly useful for patients who have difficulty perceiving signs of worsening asthma Whether peak flow monitoring, symptom monitoring, or a combination of approaches is used, self-monitoring is important to the effective self-management of asthma (Evidence A). NHLBI. NAEPP EPR-3: Guidelines for the Diagnosis and Management of Asthma, Available at
80 Interpretation of Asthma Symptoms Green Zone Yellow Zone Red Zone PEF > 80% personal best 50% 79% personal best < 50% personal best Symptoms No coughing Coughing, OR Very SOB, OR & Activity No wheezing No chest tightness No SOB (day or night) Can do usual activities Wheezing, OR Chest tightness, OR SOB (day or night), OR Limitations in usual activities No relief from quickrelief medication, OR Cannot do usual activities, OR Symptoms are same or worse after 24 hours in Yellow Zone Interpretation Doing Well Asthma Is Getting Worse Medical Alert!!
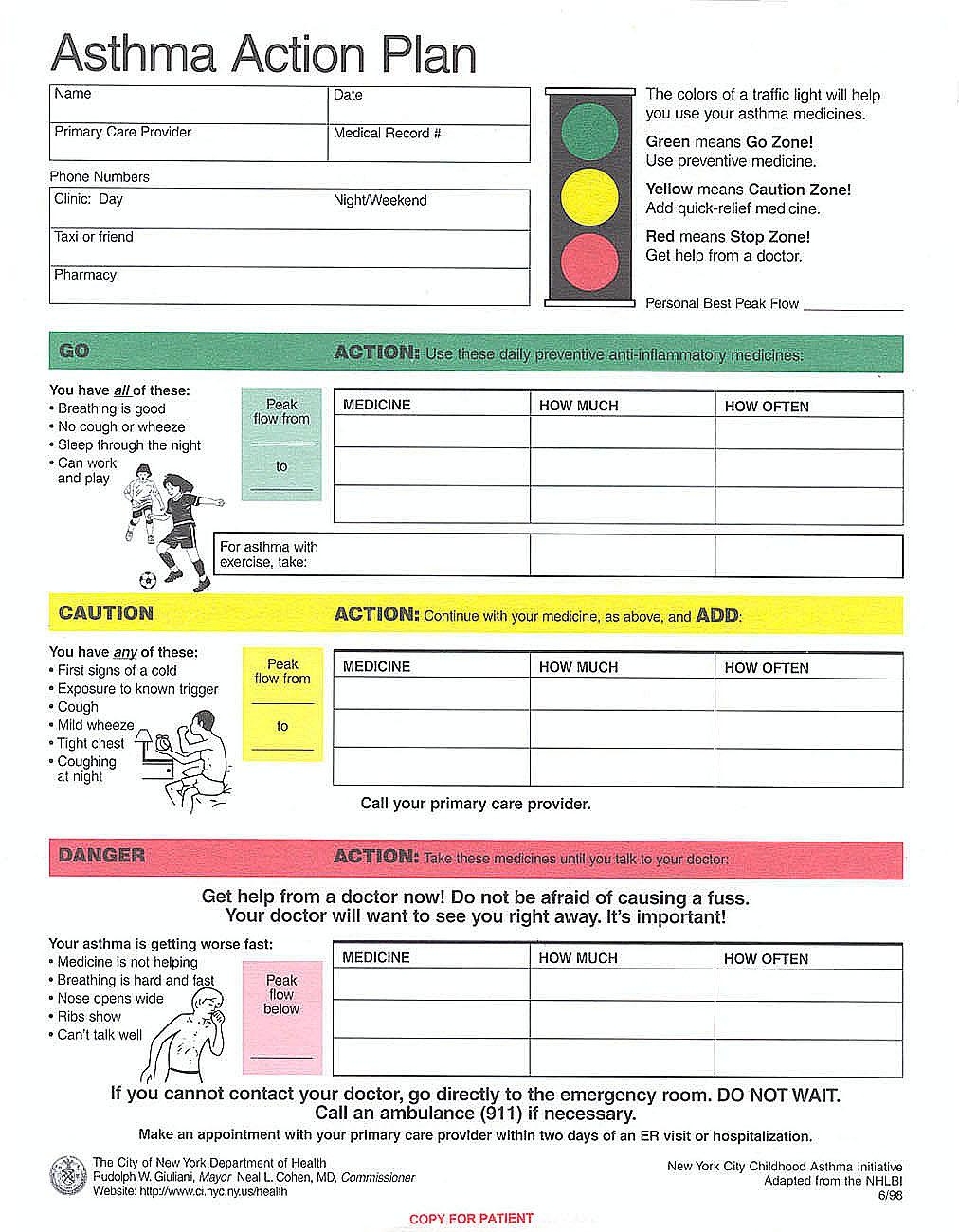
81 Key Elements of a Written Asthma Action Plan 1. Daily (Chronic) Management What medicine to take daily (include specific names, both brand and generic), how much to take, and when to take it What actions to take to control environmental factors that worsen asthma 2. Acute Management: How to Recognize and Manage Worsening Asthma What signs, symptoms, and PEF measurements indicated worsening asthma What symptoms and PEF measurements indicate the need for urgent medical attention Emergency contact information for MD, ED, and person/service to transport patient rapidly for medical care
82 Who Should Have a Written Asthma Action Plan? Patients with moderate or severe persistent asthma..? Patients with a history of severe asthma exacerbations..? Patients with poorly controlled asthma.? ALL patients* who have asthma should have a written Asthma Action Plan! *Only 47.7% of children and 28.6% of adults with asthma in Indiana had a written Asthma Action Plan during NAEPP Guidelines Implementation Report, December 2008
83 Case Studies in Asthma Management
84 According to the 2007 NIH asthma guidelines, which of the following medications is the preferred first-line controller medication for long-term control of asthma symptoms in a TWO YEAR OLD patient with MILD-PERSISTENT asthma? a. budesonide (low-dose) b. formoterol c. cromolyn d. theophylline e. montelukast
85 STEPWISE APPROACH FOR MANAGING ASTHMA IN CHILDREN 0-4 YEARS OF AGE Intermittent Asthma Persistent Asthma: Daily Medication Consult with asthma specialist if step 3 or higher care is required Consider consultation at step 2 Quick-Relief Medication for All Patients SABA as needed for symptoms. Intensity of treatment depends on severity of symptoms: up to 3 treatments at 20-minute intervals as needed. Short course of systemic oral corticosteroids may be needed. Use of beta 2 -agonist >2 days a week for symptom control (not prevention of EIB) indicates inadequate control and the need to step up treatment. Step 1 Preferred: SABA prn Step 2 Preferred: Low-dose ICS Alternative: LTRA Cromolyn Step 3 Preferred: Medium-dose ICS Step 4 Preferred: Medium-dose ICS AND either LTRA OR LABA Step 5 Preferred: High dose ICS AND either LTRA OR LABA Step 6 Preferred: High dose ICS AND either LTRA OR LABA AND Oral Corticosteroid Step up if needed (check adherence, environmental control ) Assess Control Step down if possible (if asthma well controlled for 3 months) Patient Education and Environmental Control at Each Step EPR-3
86 According to the 2007 NIH asthma guidelines, which of the following medications is the preferred first-line controller medication for long-term control of asthma symptoms in a TWO YEAR OLD patient with MILD-PERSISTENT asthma? a. budesonide (low-dose) b. formoterol c. cromolyn d. theophylline e. montelukast
87 For a 21 year old patient who is receiving only a MEDIUM-DOSE inhaled corticosteroid and whose asthma is not well controlled, which of following approaches is preferred, according to the 2007 NIH guidelines: a. Increase the dose of the inhaled corticosteroid b. Add a long-acting beta agonist c. Add a mast cell stabilizer d. Add a leukotriene modifier e. Add theophylline
88 STEPWISE APPROACH FOR MANAGING ASTHMA IN YOUTHS > 12 YEARS AND ADULTS Intermittent Asthma Persistent Asthma: Daily Medication Consult with asthma specialist if step 4 or higher care is required Consider consultation at step 3 Quick-Relief Medication for All Patients SABA as needed for symptoms. Intensity of treatment depends on severity of symptoms: up to 3 treatments at 20-minute intervals as needed. Short course of systemic oral corticosteroids may be needed. Use of beta 2 -agonist >2 days a week for symptom control (not prevention of EIB) indicates inadequate control and the need to step up treatment. Step 1 Preferred: SABA prn Step 2 Preferred: Low-dose ICS Alternative: LTRA Cromolyn Theophylline Step 3 Preferred: Med-dose ICS OR Low-dose ICS+ either LABA, LTRA, Theophylline Or Zileutin Step 4 Preferred: Medium-dose ICS+LABA Alternative: Medium-dose ICS+either LTRA, Theophylline Or Zileutin Step 5 Preferred: High dose ICS + LABA AND Consider Omalizumab for patients with allergies Step 6 Preferred: High-dose ICS + LABA + oral Corticosteroid AND Consider Omalizumab for patients with allergies Step up if needed (check adherence, environmental control and comorbidities) Assess Control Step down if possible (if asthma well controlled for 3 months) Patient Education and Environmental Control at Each Step EPR-3
89 For a 21 year old patient who is receiving only a MEDIUM-DOSE inhaled corticosteroid and whose asthma is not well controlled, which of following approaches is preferred, according to the 2007 NIH guidelines: a. Increase the dose of the inhaled corticosteroid b. Add a long-acting beta agonist c. Add a mast cell stabilizer d. Add a leukotriene modifier e. Add theophylline
90 JB is a 44 yof with asthma for which she takes daily fluticasone and has an albuterol inhaler for prn use. She presents to the clinic in no acute distress for a routine follow-up visit to assess her level of asthma control. During her visit she reports having to use her albuterol for symptom relief approximately 3 to 4 times per week during the daytime. She reports no limitations in her activities and no nighttime symptoms due to her asthma. She states that as far as she knows, her PEF s have been running at or above 80% of her personal best. Based on the information provided by JB about the frequency of her asthma symptoms, how would you classify the level of control of her asthma, according to NIH guidelines? a. Well Controlled b. Not Well Controlled c. Very Poorly Controlled d. Out of Control e. Intermittently Controlled
91 ASSESSING ASTHMA CONTROL AND ADJUSTING THERAPY IN YOUTHS > 12 YEARS OF AGE AND ADULTS EPR-3 Components of Control Symptoms Nighttime awakenings Classification of Asthma Control Well Controlled Not Well Very Poorly Controlled Controlled < 2 days/week > 2 days/week Throughout the day < 2/month 1-3/week > 4/week IMPAIRMENT RISK Interference with normal activity SABA use FEV 1 or peak flow Validated questionnaires ATAQ/ACT Exacerbations Progressive lung function Treatment-related adverse effects none Some limitation Extremely limited < 2 days/week > 2 days/week Several times/day > 80% predicted/ personal best 60-80% predicted/ personal best <60% predicted/ personal best 0/> / /< per year >2 per year Evaluation requires long-term follow up care Medication-related sides effects can vary from none to to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk. Recommended Action For Treatment Maintain current step Consider step down if well controlled x 3 mos Step up 1 step Reevaluate in 2-6 weeks Consider oral steroids Step up 1-2 steps and reevaluate in 2 weeks
92 JB is a 33 yof with asthma for which she takes daily fluticasone and has an albuterol inhaler for prn use. She presents to the clinic in no acute distress for a routine follow-up visit to assess her level of asthma control. During her visit she reports having to use her albuterol for symptom relief approximately 3 to 4 times per week during the daytime. She reports no limitations in her activities and no nighttime symptoms due to her asthma. She states that as far as she knows, her PEF s have been running at or above 80% of her personal best. Based on the information provided by JB about the frequency of her asthma symptoms, how would you classify the level of control of her asthma, according to NIH guidelines? a. Well Controlled b. Not Well Controlled c. Very Poorly Controlled d. Out of Control e. Intermittently Controlled
93 AB, a SIX year old patient who was initially diagnosed with mild persistent asthma and prescribed a low-dose inhaled corticosteroid and an albuterol MDI for prn use, returns to your clinic for follow-up and assessment of asthma control. The patient s mother indicates that AB needs to use her albuterol approximately three times per week to control her symptoms (cough and shortness of breath) during the day. The patient s mother also reports that AB is awakened a few (approximately 3) times per month due to a cough. When reviewing KB s peak flow records, you note that her peak flows have been averaging approximately 75 80% of her personal best. According to the 2007 NIH guidelines, which of the following is the most appropriate assessment of AB s asthma control and recommended action at this time? a. AB s asthma is well controlled ; maintain current therapy and reassess in 3 months b. AB s asthma is well controlled ; consider stepping down therapy at this time c. AB s asthma is not well controlled ; step up therapy and reevaluate in 3 months d. AB s asthma is not well controlled ; step up therapy and reevaluate in 2 to 6 weeks e. AB s asthma is very poorly controlled ; step up therapy, add oral methylprednisolone, and reassess in 2 weeks
94 ASSESSING ASTHMA CONTROL AND ADJUSTING THERAPY IN CHILDREN 5-11 YEARS OF AGE Components of Control IMPAIRMENT Symptoms Nighttime awakenings Interference with normal activity Classification of Asthma Control Well Controlled < 2 days/wk, <1/day Not Well Controlled >2 days/wk or multiple times on < 2 days/wk EPR-3 Very Poorly Controlled Throughout the day < 1/month > 2 x/month >2x/week none Some limitation Extremely limited SABA use < 2 days/week > 2 days/week Several times/day FEV 1 or peak flow > 80% predicted/ 60-80% predicted/ <60% predicted/ personal best personal best personal best FEV 1 /FVC > 80% predicted 75-80% predicted <75% predicted RISK Exacerbations lung growth Treatment-related adverse effects Recommended Action For Treatment 0-1/ year > 2 / year (Consider severity and interval) Evaluation requires long-term follow up care Medication-related sides effects can vary from none to to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk. Maintain current step; consider step down if well controlled x 3mos Step up 1 step Reevaluate in 2-6 weeks Consider oral steroids Step up 1-2 steps & reevaluate in 2 wks
95 KB, a SIX year old patient who was initially diagnosed with mild persistent asthma and prescribed a low-dose inhaled corticosteroid and an albuterol MDI for prn use, returns to your clinic for follow-up and assessment of asthma control. The patient s mother indicates that KB needs to use her albuterol approximately three times per week to control her symptoms (cough and shortness of breath) during the day. The patient s mother also reports that KB is awakened a few (approximately 3) times per month due to a cough. When reviewing KB s peak flow records, you note that her peak flows have been averaging approximately 75 80% of her personal best. According to the 2007 NIH guidelines, which of the following is the most appropriate assessment of KB s asthma control and recommended action at this time? a. KB s asthma is well controlled ; maintain current therapy and reassess in 3 months b. KB s asthma is well controlled ; consider stepping down therapy at this time c. KB s asthma is not well controlled ; step up therapy and reevaluate in 3 months d. KB s asthma is not well controlled ; step up therapy and reevaluate in 2 to 6 weeks e. KB s asthma is very poorly controlled ; step up therapy, add oral methylprednisolone, and reassess in 2 weeks
96 KM is a 45 year old female with moderate persistent asthma. She was hospitalized two days ago for treatment of an acute asthma exacerbation. She is being discharged today with prescriptions for the following medications: albuterol HFA, 2 puffs Q 6 h prn SOB Advair Diskus 250/50, 1 inhalation BID prednisone, 40 mg daily x 4 more days She has a peak flow meter at home. She is in need of a written Asthma Action Plan.
97 SAMPLE LONG-TERM TREATMENT PLAN FOR A 45 YEAR OLD ADULT WITH MODERATE PERSISTENT ASTHMA CLINICAL CONDITION Baseline Plan & When asthma is under control At FIRST sign of a cold or mild asthma symptoms At FIRST sign of a mild asthma attack For rapidly worsening asthma (severe attack) When there is no cough or wheeze for 3 months For cough or wheeze with exercise PEAK FLOW (% predicted) FEV 1 /FVC Above 80% 75 to 80% 50 to 75% Below 50% Over 80% for 3 months MEDICATION Reliever: Inhaled short-acting beta 2 -agonist 2 puffs as needed Albuterol HFA Controller: Inhaled med dose corticosteroid + LABA 1 puff 2x/day Advair 250/50 Corticosteroid Tablet or Syrup 0 Immunizations: Influenza annually, pneumococcal vaccine x 1
98 SAMPLE LONG-TERM TREATMENT PLAN FOR A 45 YEAR OLD ADULT WITH MODERATE PERSISTENT ASTHMA CLINICAL CONDITION PEAK FLOW (% predicted) FEV 1 /FVC Baseline Plan & When asthma is under control At FIRST sign of a cold or mild asthma symptoms At FIRST sign of a mild asthma attack For rapidly worsening asthma (severe attack) Above 80% 75 to 80% 50 to 75% Below 50% When there is no cough or wheeze for 3 months Over 80% for 3 months For cough or wheeze with exercise MEDICATION Reliever: Inhaled short-acting beta 2 -agonist Albuterol HFA Controller: Inhaled med dose corticosteroid + LABA Advair 250/50 Corticosteroid Tablet or Syrup 2 puffs as needed 1 puff 2x/day 0 2 puffs every 4 hr 1 puff 2x/day 0 4 puffs every 20 min x 3 doses, then 2-4 puffs every 4 hr 1 puff 2x/day Begin with 1-2 mg/kg/day 4-6 puffs every 20 min x 3 doses 1 puff 2x/day Prednisone 60 mg now 2 puffs as needed Consider step-down to Advair 100/50 2 puffs 5-10 minutes before exercise NOTIFY MD CALL 911 Immunizations: Influenza annually (last dose 11/10/11); pneumococcal vaccine complete (given 11/10/11) 0
99
100 Summary of Key Points Baseline assessment of asthma severity can help define initial asthma pharmacotherapy Ongoing assessment and management should focus on CONTROL, and therapy should be stepped up or stepped down accordingly INH CS are the preferred first-line agents for long-term control regardless of the age of the patient Current NIH guidelines provide for the option of titrating to a medium dose of INH CS before adding LABA Role of therapies for allergy-related asthma continue to be defined When asthma is well-controlled for a period of 3 months, consideration can be given to stepping down therapy. Education is essential all patients should have an individualized, written Asthma Action Plan!
101 Thank you for your attention! Questions?
12/18/2017. Disclosures. Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Key features and changes to these four components of asthma care include:
 Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Foundations of Pharmacology
 Pharmacologic Management of Asthma Objectives: 1. Review the physiological basis for asthma therapy 2. Discuss the differences between SABA and LABA 3. Discuss the role of inhaled and oral systemic corticosteroids
Pharmacologic Management of Asthma Objectives: 1. Review the physiological basis for asthma therapy 2. Discuss the differences between SABA and LABA 3. Discuss the role of inhaled and oral systemic corticosteroids
Learning the Asthma Guidelines by Case Studies
 Learning the Asthma Guidelines by Case Studies Timothy Craig, DO Professor of Medicine and Pediatrics Distinguished Educator Penn State University Hershey Medical Center Objectives 1. Learn the Asthma
Learning the Asthma Guidelines by Case Studies Timothy Craig, DO Professor of Medicine and Pediatrics Distinguished Educator Penn State University Hershey Medical Center Objectives 1. Learn the Asthma
Medications Affecting The Respiratory System
 Medications Affecting The Respiratory System Overview Asthma is a chronic inflammatory disorder of the airways. It is an intermittent and reversible airflow obstruction that affects the bronchioles. The
Medications Affecting The Respiratory System Overview Asthma is a chronic inflammatory disorder of the airways. It is an intermittent and reversible airflow obstruction that affects the bronchioles. The
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Adult Asthma Clinical Practice Guideline Summary
 Adult Asthma Clinical Practice Guideline Summary The following evidence-based guideline was developed to assist Primary Care physicians and other clinicians in the management of asthma in adults. It was
Adult Asthma Clinical Practice Guideline Summary The following evidence-based guideline was developed to assist Primary Care physicians and other clinicians in the management of asthma in adults. It was
Asthma medications: Know your options - MayoClinic.com. Asthma medications: Know your options
 MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
Effective Date: 4/27/2016 Version: 1.0 Approval By: CCC Clinical Delivery Steering Planned Review Date: 4/27/2017
 Protocol Title: Adult Asthma Protocol Effective Date: 4/27/2016 Version: 1.0 Approval By: CCC Clinical Delivery Steering Planned Review Date: 4/27/2017 1 Purpose & Objective This protocol provides evidence-based
Protocol Title: Adult Asthma Protocol Effective Date: 4/27/2016 Version: 1.0 Approval By: CCC Clinical Delivery Steering Planned Review Date: 4/27/2017 1 Purpose & Objective This protocol provides evidence-based
Asthma. Definition. Symptoms
 Asthma Definition Asthma is a condition in which your airways narrow and swell and produce extra mucus. This can make breathing difficult and trigger coughing, wheezing and shortness of breath. For some
Asthma Definition Asthma is a condition in which your airways narrow and swell and produce extra mucus. This can make breathing difficult and trigger coughing, wheezing and shortness of breath. For some
Dual-Controller Asthma Therapy: Rationale and Clinical Benefits
 B/1 Dual-Controller Asthma Therapy: Rationale and Clinical Benefits MODULE B The 1997 National Heart, Lung, and Blood Institute (NHLBI) Expert Panel guidelines on asthma management recommend a 4-step approach
B/1 Dual-Controller Asthma Therapy: Rationale and Clinical Benefits MODULE B The 1997 National Heart, Lung, and Blood Institute (NHLBI) Expert Panel guidelines on asthma management recommend a 4-step approach
Asthma in Pregnancy. Asthma. Chronic Airway Inflammation. Objective Measures of Airflow. Peak exp. flow rate (PEFR)
") Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Improving the Management of Asthma to Improve Patient Adherence and Outcomes
 Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
ASTHMA BEST PRACTICES FOR SCHOOL NURSES. School Nurses November 2015
 ASTHMA BEST PRACTICES FOR SCHOOL NURSES School Nurses November 2015 1 BACKGROUND AND CURRENT STATS General definitions and explanations 2 Incidence of Asthma Centers for Disease Control (CDC) - 1 in 12
ASTHMA BEST PRACTICES FOR SCHOOL NURSES School Nurses November 2015 1 BACKGROUND AND CURRENT STATS General definitions and explanations 2 Incidence of Asthma Centers for Disease Control (CDC) - 1 in 12
Alberta Childhood Asthma Pathway for Primary Care
 Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
10/18/2012. Penn State University Children s Hospital JODIE STABINSKI CRNP MSN AE-C
 Penn State University Children s Hospital JODIE STABINSKI CRNP MSN AE-C Daily: Long-Term Control Corticosteroids (inhaled and systemic) Long-acting beta 2 -agonists (Serevent, Foradil) Methylxanthines
Penn State University Children s Hospital JODIE STABINSKI CRNP MSN AE-C Daily: Long-Term Control Corticosteroids (inhaled and systemic) Long-acting beta 2 -agonists (Serevent, Foradil) Methylxanthines
Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies
 Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies Stanley J. Szefler, MD Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics, Head, Pediatric
Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies Stanley J. Szefler, MD Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics, Head, Pediatric
FIGURE 17. USUAL DOSAGES FOR LONG-TERM CONTROL MEDICATIONS*
 FIGURE 17. USUAL DOSAGES FOR LONG-TERM CONTROL MEDICATIONS* 0 4 Years Age and Adults Potential Adverse Effects Inhaled Corticosteroids (See Figure 18, Estimated Comparative Daily Dosages for ICSs. ) Oral
FIGURE 17. USUAL DOSAGES FOR LONG-TERM CONTROL MEDICATIONS* 0 4 Years Age and Adults Potential Adverse Effects Inhaled Corticosteroids (See Figure 18, Estimated Comparative Daily Dosages for ICSs. ) Oral
Clinical Policy: Omalizumab (Xolair) Reference Number: ERX.SPA.141 Effective Date: Last Review Date: 08.17
 Reference Number: ERX.SPA.141 Effective Date: Last Review Date: 08.17") Clinical Policy: (Xolair) Reference Number: ERX.SPA.141 Effective Date: 03.01.14 Last Review Date: 08.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Xolair) Reference Number: ERX.SPA.141 Effective Date: 03.01.14 Last Review Date: 08.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Asthma 2015: Establishing and Maintaining Control
 Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
MANAGING ASTHMA. Nancy Davis, RRT, AE-C
 MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
Pediatric Asthma Management
 Pediatric Asthma Management APRN Conference February 2016 Cheryl Kerrigan, MSN, CPNP Aimee Tiller RN, AE-C The Plan Definition Pathophysiology review Triggers & Risk Factors Incidence and Prevalence Making
Pediatric Asthma Management APRN Conference February 2016 Cheryl Kerrigan, MSN, CPNP Aimee Tiller RN, AE-C The Plan Definition Pathophysiology review Triggers & Risk Factors Incidence and Prevalence Making
Meeting the Challenges of Asthma
 Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Asthma Description. Asthma is a disease that affects the lungs defined as a chronic inflammatory disorder of the airways.
 Asthma Asthma Description Asthma is a disease that affects the lungs defined as a chronic inflammatory disorder of the airways. Symptoms of asthma In susceptible individuals, this inflammation causes recurrent
Asthma Asthma Description Asthma is a disease that affects the lungs defined as a chronic inflammatory disorder of the airways. Symptoms of asthma In susceptible individuals, this inflammation causes recurrent
Q: Should patients with mild asthma
 1-MINUTE CONSULT CME CREDIT EDUCATIONAL OBJECTIVE: Readers will consider prescribing inhaled corticosteroids to their patients who have mild persistent asthma brief answers to specific clinical questions
1-MINUTE CONSULT CME CREDIT EDUCATIONAL OBJECTIVE: Readers will consider prescribing inhaled corticosteroids to their patients who have mild persistent asthma brief answers to specific clinical questions
2014 CLINICAL PRACTICE GUIDELINES FOR ASTHMA
 2014 CLINICAL PRACTICE GUIDELINES FOR ASTHMA Updated guidelines for the diagnosis and management of asthma developed by the National Asthma Education and Prevention Program (EPP) were released in October
2014 CLINICAL PRACTICE GUIDELINES FOR ASTHMA Updated guidelines for the diagnosis and management of asthma developed by the National Asthma Education and Prevention Program (EPP) were released in October
Inhaled bronchodilators relax constricted airways and treat the noisy part of asthma: coughing, wheezing, choking and shortness of breath.
 Inhaled bronchodilators relax constricted airways and treat the noisy part of asthma: coughing, wheezing, choking and shortness of breath. AccuNeb inhalation 0.021% solution: 0.63mg/3mL 3-4 times solution
Inhaled bronchodilators relax constricted airways and treat the noisy part of asthma: coughing, wheezing, choking and shortness of breath. AccuNeb inhalation 0.021% solution: 0.63mg/3mL 3-4 times solution
Asthma By Mayo Clinic staff
 MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Fasenra) Reference Number: CP.PHAR.## Effective Date: 01.16.18 Last Review Date: 05.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Fasenra) Reference Number: CP.PHAR.## Effective Date: 01.16.18 Last Review Date: 05.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy
Clinical Policy: Omalizumab (Xolair) Reference Number: ERX.SPA.141 Effective Date:
 Reference Number: ERX.SPA.141 Effective Date:") Clinical Policy: (Xolair) Reference Number: ERX.SPA.141 Effective Date: 03.01.14 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Xolair) Reference Number: ERX.SPA.141 Effective Date: 03.01.14 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD
 Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Drug Class Monograph
 Drug Class Monograph Class: Inhaled Corticosteroids Drugs: Aerospan (flunisolide), Advair Diskus, Advair HFA (fluticasone/salmeterol), Alvesco (ciclesonide), Arnuity Ellipta (fluticasone furoate), Asmanex
Drug Class Monograph Class: Inhaled Corticosteroids Drugs: Aerospan (flunisolide), Advair Diskus, Advair HFA (fluticasone/salmeterol), Alvesco (ciclesonide), Arnuity Ellipta (fluticasone furoate), Asmanex
Asthma ASTHMA. Current Strategies for Asthma and COPD
 Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline UPDATE. Susan K. Ross RN, AE-C MDH Asthma Program.
 NAEPP 2007 Asthma Guideline UPDATE. Susan K. Ross RN, AE-C MDH Asthma Program.") National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline UPDATE Susan K. Ross RN, AE-C MDH Asthma Program 651-201 201-5629 Susan.Ross@health.state.mn.us 1 National Institutes of Health National
National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline UPDATE Susan K. Ross RN, AE-C MDH Asthma Program 651-201 201-5629 Susan.Ross@health.state.mn.us 1 National Institutes of Health National
Working Together to Better Manage Childhood Asthma
 Working Together to Better Manage Childhood Asthma Bennie McWilliams, M.D. Howard Rosenblatt, M.D. Meena Ganesh, M.D. Chris Valmores, B.S.C.S.M., R.R.P.T. Carol Reagan, R.Ph. Johnny Smith Johnny is a 5
Working Together to Better Manage Childhood Asthma Bennie McWilliams, M.D. Howard Rosenblatt, M.D. Meena Ganesh, M.D. Chris Valmores, B.S.C.S.M., R.R.P.T. Carol Reagan, R.Ph. Johnny Smith Johnny is a 5
Inhaler Confusion. Today s Speaker Dr. Randall Brown. Director of Asthma Programs 6/7/2016. Dr. Randall Brown March 31, 2016
 + Inhaler Confusion Dr. Randall Brown March 31, 2016 + Today s Speaker Dr. Randall Brown Director of Asthma Programs Center for Managing Chronic Disease University of Michigan 1 ASTHMA ESSENTIALS IN PRIMARY
+ Inhaler Confusion Dr. Randall Brown March 31, 2016 + Today s Speaker Dr. Randall Brown Director of Asthma Programs Center for Managing Chronic Disease University of Michigan 1 ASTHMA ESSENTIALS IN PRIMARY
II: Moderate Worsening airflow limitations Dyspnea on exertion, cough, and sputum production; patient usually seeks medical
 Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
MEDICAL COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 07/05/18 SECTION: DRUGS LAST REVIEW DATE: LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 CINQAIR (reslizumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
CINQAIR (reslizumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
Omalizumab (Xolair ) ( Genentech, Inc., Novartis Pharmaceuticals Corp.) September Indication
 ( Genentech, Inc., Novartis Pharmaceuticals Corp.) September Indication") ( Genentech, Inc., Novartis Pharmaceuticals Corp.) September 2003 Indication The FDA recently approved Omalizumab on June 20, 2003 for adults and adolescents (12 years of age and above) with moderate to
( Genentech, Inc., Novartis Pharmaceuticals Corp.) September 2003 Indication The FDA recently approved Omalizumab on June 20, 2003 for adults and adolescents (12 years of age and above) with moderate to
Nancy Davis, RRT, AE-C
 Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Provider Respiratory Inservice
 Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Tips on managing asthma in children
 Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Asthma Update A/Prof. John Abisheganaden. Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital
 Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
New Therapies for Asthma
 New Therapies for Asthma Tracy Bridges, MD Speaker Disclosure: Dr. Bridges participates in speaker bureaus for Teva, Genetech & Astra Zeneca. Objectives: Discuss the use of LAMA s for Asthma Detail the
New Therapies for Asthma Tracy Bridges, MD Speaker Disclosure: Dr. Bridges participates in speaker bureaus for Teva, Genetech & Astra Zeneca. Objectives: Discuss the use of LAMA s for Asthma Detail the
Global Initiative for Asthma (GINA) What s new in GINA 2016?
 What s new in GINA 2016?") Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Xolair (Omalizumab) Drug Prior Authorization Protocol (Medical Benefit & Part B Benefit)
 Drug Prior Authorization Protocol (Medical Benefit & Part B Benefit)") Line of Business: All Lines of Business Effective Date: August 16, 2017 Xolair (Omalizumab) Drug Prior Authorization Protocol (Medical Benefit & Part B Benefit) This policy has been developed through review
Line of Business: All Lines of Business Effective Date: August 16, 2017 Xolair (Omalizumab) Drug Prior Authorization Protocol (Medical Benefit & Part B Benefit) This policy has been developed through review
Adjustment of Inhaled Controller Therapy of Asthma in the Yellow Zone, Based on the Inhaler Product Used in the Green Zone Age 16 Years and Older
 Adjustment of Inhaled Controller Therapy of Asthma in the Yellow Zone, Based on the Inhaler Product Used in the Green Zone Age 16 Years and Older The Canadian Thoracic Society and other international asthma
Adjustment of Inhaled Controller Therapy of Asthma in the Yellow Zone, Based on the Inhaler Product Used in the Green Zone Age 16 Years and Older The Canadian Thoracic Society and other international asthma
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Preschool Asthma What you need to know in 10 minutes
 Preschool Asthma What you need to know in 10 minutes Alan Kaplan MD CCFP(EM) FCFP Family Physician Airways Group of Canada Respiratory Medicine section CFPC Faculty/Presenter Disclosure Faculty: Alan Kaplan
Preschool Asthma What you need to know in 10 minutes Alan Kaplan MD CCFP(EM) FCFP Family Physician Airways Group of Canada Respiratory Medicine section CFPC Faculty/Presenter Disclosure Faculty: Alan Kaplan
Drugs that Affect the Respiratory System BROOKE BENTLEY, PHD, APRN
 Drugs that Affect the Respiratory System BROOKE BENTLEY, PHD, APRN Goals of Therapy Asthma Prevent symptoms COPD Reduce COPD symptoms Decrease use of SABAs Maintain normal pulm function & prevent loss
Drugs that Affect the Respiratory System BROOKE BENTLEY, PHD, APRN Goals of Therapy Asthma Prevent symptoms COPD Reduce COPD symptoms Decrease use of SABAs Maintain normal pulm function & prevent loss
CLINICAL MEDICAL POLICY
 CLINICAL MEDICAL POLICY Policy Name: Xolair (omalizumab) Policy Number: MP-051-MD-DE Responsible Department(s): Medical Management; Clinical Pharmacy Provider Notice Date: 10/01/2017 Original Effective
CLINICAL MEDICAL POLICY Policy Name: Xolair (omalizumab) Policy Number: MP-051-MD-DE Responsible Department(s): Medical Management; Clinical Pharmacy Provider Notice Date: 10/01/2017 Original Effective
Improving Outcomes in the Management & Treatment of Asthma. April 21, Spring Managed Care Forum
 Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Clinical Policy: Dupilumab (Dupixent) Reference Number: ERX.SPA.49 Effective Date:
 Reference Number: ERX.SPA.49 Effective Date:") Clinical Policy: (Dupixent) Reference Number: ERX.SPA.49 Effective Date: 06.01.17 Last Review Date: 02.19 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Dupixent) Reference Number: ERX.SPA.49 Effective Date: 06.01.17 Last Review Date: 02.19 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Guideline for the Diagnosis, Evaluation, and Management of Adults and Children with Asthma
 Clinical Guideline for the Diagnosis, Evaluation, and Management of Adults and Children with Asthma - 2005 Criteria that suggest the diagnosis of Asthma: The symptoms of dyspnea, cough and/or wheezing,
Clinical Guideline for the Diagnosis, Evaluation, and Management of Adults and Children with Asthma - 2005 Criteria that suggest the diagnosis of Asthma: The symptoms of dyspnea, cough and/or wheezing,
National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline Expert Panel Report (EPR) 3
 NAEPP 2007 Asthma Guideline Expert Panel Report (EPR) 3") National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline Expert Panel Report (EPR) 3 Susan K. Ross RN, AE C MDH Asthma Program 651 201 201 5629 Susan.Ross@state.mn.us 1 National Institutes of Health
National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline Expert Panel Report (EPR) 3 Susan K. Ross RN, AE C MDH Asthma Program 651 201 201 5629 Susan.Ross@state.mn.us 1 National Institutes of Health
benralizumab (Fasenra )
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Respiratory Medications and Devices Update 2/15
 Respiratory Medications and Devices Update 2/15 Dewey Hahlbohm, PA-C, AE-C Wendy Brown, Pharm.D., MPAS, PA-C, AE-C Objectives! Review mechanism of action for asthma pharmacologic agents! Describe key patient
Respiratory Medications and Devices Update 2/15 Dewey Hahlbohm, PA-C, AE-C Wendy Brown, Pharm.D., MPAS, PA-C, AE-C Objectives! Review mechanism of action for asthma pharmacologic agents! Describe key patient
Improving asthma outcomes though education
 Improving asthma outcomes though education Segment 1 Clinical Aspects of Asthma and Long term Plan Primary Care and Asthma Most common chronic disease of childhood. Primary care providers are expected
Improving asthma outcomes though education Segment 1 Clinical Aspects of Asthma and Long term Plan Primary Care and Asthma Most common chronic disease of childhood. Primary care providers are expected
Allergies and Asthma 5/21/2013. Objectives. Allergic Rhinitis (AR): Risk Factor for ASTHMA. Rhinitis and Asthma
: Risk Factor for ASTHMA. Rhinitis and Asthma") Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
Pediatric Asthma: Pharmacotherapy. Joseph Spahn, MD Children s Hospital Colorado & University of Colorado Medical School Aurora, Colorado
 Pediatric Asthma: Pharmacotherapy Joseph Spahn, MD Children s Hospital Colorado & University of Colorado Medical School Aurora, Colorado Pediatric Asthma: Pharmacotherapy Disclosures/Conflicts of Interest:
Pediatric Asthma: Pharmacotherapy Joseph Spahn, MD Children s Hospital Colorado & University of Colorado Medical School Aurora, Colorado Pediatric Asthma: Pharmacotherapy Disclosures/Conflicts of Interest:
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007
 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
ASTHMA IN THE PEDIATRIC POPULATION
 ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
Asthma Pharmacotherapy 2017: Stepwise Approach to Managing Asthma
 Asthma Pharmacotherapy 2017: Stepwise Approach to Managing Asthma Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C Director, Commercial Care
Asthma Pharmacotherapy 2017: Stepwise Approach to Managing Asthma Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C Director, Commercial Care
Clinical Policy: Mepolizumab (Nucala) Reference Number: ERX.SPA.214 Effective Date:
 Reference Number: ERX.SPA.214 Effective Date:") Clinical Policy: (Nucala) Reference Number: ERX.SPA.214 Effective Date: 07.01.16 Last Review Date: 05.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Nucala) Reference Number: ERX.SPA.214 Effective Date: 07.01.16 Last Review Date: 05.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Nucala) Reference Number: CP.PHAR.200 Effective Date: 04.01.16 Last Review Date: 02.18 Line of Business: Commercial, Medicaid Coding Implications Revision Log See Important Reminder at
Clinical Policy: (Nucala) Reference Number: CP.PHAR.200 Effective Date: 04.01.16 Last Review Date: 02.18 Line of Business: Commercial, Medicaid Coding Implications Revision Log See Important Reminder at
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL
 DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
COPD COPD. Update on COPD and Asthma
 Update on COPD and Asthma Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco, CA COPD COPD
Update on COPD and Asthma Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco, CA COPD COPD
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Clinical Policy: Mepolizumab (Nucala) Reference Number: ERX.SPA.214 Effective Date:
 Reference Number: ERX.SPA.214 Effective Date:") Clinical Policy: (Nucala) Reference Number: ERX.SPA.214 Effective Date: 07.01.16 Last Review Date: 02.19 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Nucala) Reference Number: ERX.SPA.214 Effective Date: 07.01.16 Last Review Date: 02.19 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
BUDESONIDE AND FORMOTEROL (SYMBICORT ): Α A REVIEW
: Α A REVIEW") Volume 23, Issue 3 December 2007 BUDESONIDE AND FORMOTEROL (SYMBICORT ): A REVIEW Donna L. Smith, Pharm. D. Candidate More than 22 million people in the United States have asthma according to the Centers
Volume 23, Issue 3 December 2007 BUDESONIDE AND FORMOTEROL (SYMBICORT ): A REVIEW Donna L. Smith, Pharm. D. Candidate More than 22 million people in the United States have asthma according to the Centers
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION
 Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management
Step up if needed (first, check adherence, environmental control and comorbid conditions) Patients ASSESS CONTROL. Step down if possible
 Patients ASSESS CONTROL. Step down if possible") 12/9/212 Pharmacogenomics Treating the Individual Asthma Patient Elliot Israel, M.D. Professor of Medicine Harvard Medical School Brigham & Women s Hospital Partners Asthma Center Too much of a good thing?
12/9/212 Pharmacogenomics Treating the Individual Asthma Patient Elliot Israel, M.D. Professor of Medicine Harvard Medical School Brigham & Women s Hospital Partners Asthma Center Too much of a good thing?
Peak Expiratory Flow Rate (PEFR) for ED Management of Acute Asthma Exacerbation
 for ED Management of Acute Asthma Exacerbation") Peak Expiratory Flow Rate (PEFR) for ED Management of Acute Asthma Exacerbation PI: Brian Driver, MD Checklist Reviewed Inclusion and Exclusion Criteria Confirm pertinent exclusion criteria with PMP Engage
Peak Expiratory Flow Rate (PEFR) for ED Management of Acute Asthma Exacerbation PI: Brian Driver, MD Checklist Reviewed Inclusion and Exclusion Criteria Confirm pertinent exclusion criteria with PMP Engage
Medicine Dr. Kawa Lecture 4 - Treatment of asthma :
 Medicine Dr. Kawa Lecture 4 - Treatment of asthma : Avoiding allergens. Hyposensitization :Subcutaneous injections of inially very small, but gradually increasing doses of allergens (desensitization or
Medicine Dr. Kawa Lecture 4 - Treatment of asthma : Avoiding allergens. Hyposensitization :Subcutaneous injections of inially very small, but gradually increasing doses of allergens (desensitization or
Emily DiMango, MD Asthma II
 Emily DiMango, MD Asthma II Director John Edsall/John Wood Asthma Center Columbia University Medical Center HP 2000 Goal: 2.25/1,000 Comparison of Asthma Hospitalization Rates in Children Aged 0-14 in
Emily DiMango, MD Asthma II Director John Edsall/John Wood Asthma Center Columbia University Medical Center HP 2000 Goal: 2.25/1,000 Comparison of Asthma Hospitalization Rates in Children Aged 0-14 in
Using Inhaled Corticosteroids as Needed for Asthma: giving patients relief or leaving them breathless?
 Using Inhaled Corticosteroids as Needed for Asthma: giving patients relief or leaving them breathless? Lindsay Thomas, Pharm.D. PGY2 Ambulatory Care Resident Department of Pharmacotherapy and Pharmacy
Using Inhaled Corticosteroids as Needed for Asthma: giving patients relief or leaving them breathless? Lindsay Thomas, Pharm.D. PGY2 Ambulatory Care Resident Department of Pharmacotherapy and Pharmacy
Question I was one of the first dry power devices available in the US Flovent, Serevent and Advair are all available in this device
 What Device am I Class Side Effects History Potpourri Monitoring Tools 10 10 10 10 10 20 20 20 20 20 30 30 30 30 30 40 40 40 40 40 50 50 50 50 50 WHAT KIND OF DEVICE AM I? I was one of the first dry power
What Device am I Class Side Effects History Potpourri Monitoring Tools 10 10 10 10 10 20 20 20 20 20 30 30 30 30 30 40 40 40 40 40 50 50 50 50 50 WHAT KIND OF DEVICE AM I? I was one of the first dry power
Biologic Agents in the treatment of Severe Asthma
 Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
Asthma Upate 2018: What s New Since the 2007 Asthma Guidelines of NAEPP?
 10:50-11:50am Asthma Update 2018: What s New Since the 2007 National Asthma Guidelines? SPEAKER Christopher H. Fanta, MD Disclosures The following relationships exist related to this presentation: Christopher
10:50-11:50am Asthma Update 2018: What s New Since the 2007 National Asthma Guidelines? SPEAKER Christopher H. Fanta, MD Disclosures The following relationships exist related to this presentation: Christopher
FASENRA (benralizumab)
") FASENRA (benralizumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
FASENRA (benralizumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
LONG-ACTING BETA AGONISTS
 LONG-ACTING BETA AGONISTS AND ICS/LABA COMBINATIONS DISCLOSURE Dr. Francisco has no financial interest in any commercial entity discussed in this presentation Dr. Francisco will not discuss experimental
LONG-ACTING BETA AGONISTS AND ICS/LABA COMBINATIONS DISCLOSURE Dr. Francisco has no financial interest in any commercial entity discussed in this presentation Dr. Francisco will not discuss experimental
The proposal is to add text/statements in red and to delete text/statements with strikethrough: POLICY
 Omalizumab DESCRIPTION Omalizumab is a recombinant DNA-derived humanized IgG1κ monoclonal antibody which selectively binds to immunoglobulin E (IgE). High serum levels of IgE are found in individuals with
Omalizumab DESCRIPTION Omalizumab is a recombinant DNA-derived humanized IgG1κ monoclonal antibody which selectively binds to immunoglobulin E (IgE). High serum levels of IgE are found in individuals with
Nucala (mepolizumab injection for subcutaneous use)
") Nucala (mepolizumab injection for subcutaneous use) Policy Number: 5.01.612 Last Review: 01/2018 Origination: 02/2016 Next Review: 02/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will
Nucala (mepolizumab injection for subcutaneous use) Policy Number: 5.01.612 Last Review: 01/2018 Origination: 02/2016 Next Review: 02/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will
Asthma training. Mike Levin Division of Asthma and Allergy Red Cross Hospital
 Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma in Pediatric Patients. DanThuy Dao, D.O., FAAP. Disclosures. None
 Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Respiratory Health. Asthma and COPD
 Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
ANTINEOPLASTIC DRUGS CHAPTER 21. Antineoplastic drugs - designed to treat malignancies, now also used to treat diseases with inflammatory component
 ANTINEOPLASTIC DRUGS CHAPTER 21 Antineoplastic drugs - designed to treat malignancies, now also used to treat diseases with inflammatory component Tx of malignancies Antineoplastic drugs: methotrexate
ANTINEOPLASTIC DRUGS CHAPTER 21 Antineoplastic drugs - designed to treat malignancies, now also used to treat diseases with inflammatory component Tx of malignancies Antineoplastic drugs: methotrexate
December 7, 2010 Future Use of Biologics in Allergy and Asthma
 December 7, 2010 Future Use of Biologics in Allergy and Asthma Lanny J. Rosenwasser, M.D. Dee Lyons/Missouri Endowed Chair in Immunology Research Professor of Pediatrics Allergy-Immunology Division Childrens
December 7, 2010 Future Use of Biologics in Allergy and Asthma Lanny J. Rosenwasser, M.D. Dee Lyons/Missouri Endowed Chair in Immunology Research Professor of Pediatrics Allergy-Immunology Division Childrens
Asthma. Rachel Miller, MD, FAAAAI Director Allergy and Immunology New York Presbyterian Hospital. Figure 1 Asthma Prevalence,
 Asthma Rachel Miller, MD, FAAAAI Director Allergy and Immunology New York Presbyterian Hospital Figure 1 Asthma Prevalence, 1980-2000 * Gap between 1995-1996 and 1997 indicates a break in trend due to
Asthma Rachel Miller, MD, FAAAAI Director Allergy and Immunology New York Presbyterian Hospital Figure 1 Asthma Prevalence, 1980-2000 * Gap between 1995-1996 and 1997 indicates a break in trend due to
UNIVERSAL ACTIVITY NUMBER (UAN): H04-P. 1.5 Contact Hours 0.15 CEUs expiration date: 12/12/2015
: H04-P. 1.5 Contact Hours 0.15 CEUs expiration date: 12/12/2015") Asthma Maintenance Whitney Hanks, Pharm.D. Candidate 2012 Stephen Jamison, Pharm.D. Candidate 2012 Brett Parrish, Pharm.D. Candidate 2012 Bernie R. Olin, Pharm.D., Associate Clinical Professor and Director
Asthma Maintenance Whitney Hanks, Pharm.D. Candidate 2012 Stephen Jamison, Pharm.D. Candidate 2012 Brett Parrish, Pharm.D. Candidate 2012 Bernie R. Olin, Pharm.D., Associate Clinical Professor and Director
The methodology behind GINA and EPR-3 medication recommendations: Stepwise treatment in asthma
 The methodology behind GINA and EPR-3 medication recommendations: Stepwise treatment in asthma Maureen George PhD RN AE-C FAAN Columbia University mg3656@cumc.columbia.edu Faculty Disclosures Maureen George
The methodology behind GINA and EPR-3 medication recommendations: Stepwise treatment in asthma Maureen George PhD RN AE-C FAAN Columbia University mg3656@cumc.columbia.edu Faculty Disclosures Maureen George
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
Adult asthma management: focus on control
 Adult asthma management: focus on control Jennifer W. McCallister, MD Associate Professor Pulmonary, Allergy, Critical Care & Sleep Medicine The Ohio State University Wexner Medical Center Objectives Apply
Adult asthma management: focus on control Jennifer W. McCallister, MD Associate Professor Pulmonary, Allergy, Critical Care & Sleep Medicine The Ohio State University Wexner Medical Center Objectives Apply
Significance. Asthma Definition. Focus on Asthma
 Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Respiratory Pharmacology
 Allergy Targets of allergies Type I Histamine Leukotrienes Prostaglandins Bradykinin Hypersensitivity reactions Asthma Characterised by Triggered by Intrinsic Extrinsic (allergic) Mediators Result Early
Allergy Targets of allergies Type I Histamine Leukotrienes Prostaglandins Bradykinin Hypersensitivity reactions Asthma Characterised by Triggered by Intrinsic Extrinsic (allergic) Mediators Result Early
Breathe Easy: Ensuring Care Coordination for Patients with Asthma
 Breathe Easy: Ensuring Care Coordination for Patients with Asthma Target Audience: Pharmacists ACPE#: 0202-0000-18-051-L01-P Activity Type: Application-based Disclosures Lauren E. Bode none Dennis Williams
Breathe Easy: Ensuring Care Coordination for Patients with Asthma Target Audience: Pharmacists ACPE#: 0202-0000-18-051-L01-P Activity Type: Application-based Disclosures Lauren E. Bode none Dennis Williams
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
reslizumab (Cinqair )
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided