Learning Objectives 4/26/2012. Review normal lung function and COPD pathophysiology Discuss pharmacological management
|
|
|
- Chloe Rosa Lester
- 6 years ago
- Views:
Transcription
1 Marliese Gibson PharmD HospiScript, a Catalyst Rx Company May 16, 2012 Chronic Obstructive Pulmonary Disease Learning Objectives Review normal lung function and COPD pathophysiology Discuss pharmacological management of COPD in hospice patients Identify effective inhaler techniques for aerosol and dry powder inhalers Describe dyspnea management for hospice patients with COPD 1
2 Prevalence 4 th leading cause of death in United States Expected to be 3 rd by % of the population have been diagnosed Estimated that 25% actually have air flow limitation without diagnosis Healthcare Utilization Overall patients in million physician and hospital visits 1.5 million emergency department visits 673,000 hospitalizations Hospice patients ,029,000 patients total all diagnoses 85,407 (8.3%) patients with lung disease COPD Definition COPD is a preventable and treatable disease with some significant extrapulmonary effects that may contribute to the severity in individual patients. Its pulmonary component is characterized by airflow limitation that is not fully reversible. The airflow limitation is usually progressive and associated with an abnormal inflammatory response of the lung to noxious particles or gases. Global Initiative for Chronic Obstructive Lung Disease,











3 Other Names for COPD Emphysema Destruction of alveoli Pathological term Chronic bronchitis Presence of cough and sputum production for at least 3 months in each of 2 consecutive years Lung Anatomy Lungs Located on each side of the chest Encased in the pleura Bronchi Bronchioles Alveoli Conducting airways Conduct air from the trachea to the alveoli Lung Functions Gas exchange Blood Air interface Two cell layers thick 300 million alveoli square feet of surface area Filtering and detoxification Metabolic/Synthetic functions Surfactant Mucopolysaccharides Angiotensin i conversion Endocrine functions 3
4 Normal Lung Function and Elasticity Lungs tend to collapse to a smaller size Chest wall tends to expand outward Lung expansion is maintained by a negative pressure in the pleural space Lungs distend easily with little pressure Air Movement During Inspiration The diaphragm contracts Pushes down on abdominal contents Lengthens the thoracic cavity Intercostal muscles contract Raise and lift ribs outward Expand the chest laterally Result is negative pressure in the chest Air flows in easily to fill the empty space Air Movement during Expiration Respiratory muscles relax Chest wall moves inward Elastic recoil pulls the lung inward Pressure within the chest increases Air flows outward passively 4






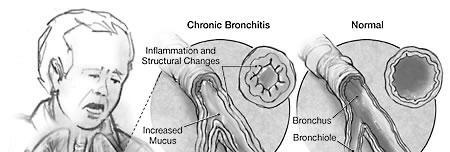
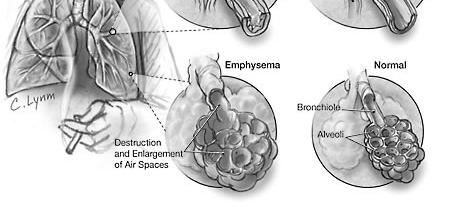
5 Air Movement in COPD Lungs are chronically overinflated Chest wall and diaphragm move less Less negative pressure is generated in inspiration Patients use accessory muscles or arms to lift and lengthen thoracic cavity Elastic recoil is reduced Positive pressure in expiration is reduced Expiration no longer passive, requires effort Airways are narrowed by inflammation Airways may collapse Expiration is slower Expiration takes more effort Normal Lungs vs. COPD Lungs Stages of COPD Stage I: Mild FEV1/FVC < 70%; FEV1 80% predicted Stage II: Moderate FEV1/FVC < 70%; 50% FEV1 < 80% predicted Mild airflow limitation Symptoms of cough and sputum production may be present, but not always. The individual is usually unaware that his/her lung function is abnormal. SOB on exertion Cough and sputum production sometimes es present Patients typically seek medical attention due to chronic respiratory symptoms or an exacerbation of their disease. Stage III: Severe FEV1/FVC < 70%; 30% FEV1 < 50% predicted Stage IV: Very Severe FEV1/FVC < 70%; FEV1 < 30% predicted or FEV1 < 50% predicted plus chronic respiratory failure SOB, reduced exercise capacity, fatigue, and repeated exacerbations that almost always impact QOL Respiratory failure may lead to effects on the heart 5
6 End-Stage COPD: Hospice Eligibility Patient has ALL of the following: Disabling dyspnea at rest or with minimal exertion Little or no response to bronchodilators Decreased functional capacity AND Progression of disease (physician visits, ER visits, hospitalizations) Documentation of one of the following in the past 3 months Hypoxemia (po2 < 55mmHg or O2 sat. <88%) Hypercapnia (pco2 > 50mmHg) Causes of Death in COPD Infection Ventilatory failure Heart failure Treatments for COPD Bronchodilators Beta 2 agonists Anticholinergics Methylxanthines (theophylline) Corticosteroids Phosphodiesterase-4 Enzyme Inhibitor 6
7 Bronchodilators Less benefit in end-stage disease Nebulizers vs. multi-dose inhalers +/- spacer Beta 2 agonists Anticholinergics Theophylline Patient may become psychologically dependent Beta 2 Agonists: Short-acting Albuterol (Proventil, Ventolin, ProAir HFA) ProAir HFA inhaler: 90mcg/act 2 puffs every 4-6 hours ($88/30 DS) Nebs: 0.63mg, 2.5mg/3ml 1 vial every 4-6 hours Levalbuterol (Xopenex) Inhaler: 45mcg/act 2 puffs every 4-6 hours ($316, $140/30 DS) ($120/30 DS) Nebs: 0.31mg, 0.62mg, 1.25mg/3ml 1 vial every 6-8 hours ($605 - $675/30 DS) Beta 2 Agonists: Long-acting Salmeterol (Serevent) Inhaled powder: 50mcg/act Every 12 hours ($181/30 DS) Formoterol (Foradil Aerolizer) Inhaled powder: 12mcg/capsule Every 12 hours ($176/30 DS) Arformoterol (Brovana) Nebs: 15mcg/2ml Every 12 hours ($280/30 DS) Indacaterol (Arcapta Neohaler) Inhaled powder: 75mcg/capsule Every 24 hours ($195/30DS) 7
8 Anticholinergics Ipratropium (Atrovent, Atrovent HFA) Inhaler: 17mcg/act 2 puffs every 6 hours ($172/30 DS) Nebs: 0.02% 1 vial every 6-8 hours ($70/30 DS) Tiotropium (Spiriva) Inhaled powder: 18mcg/capsule Every 24 hours ($246/30 DS) Theophylline Bronchodilator Exact mechanism unknown Thought to non-specifically inhibit all phosphodiesterase enzymes Inexpensive 200mg CR tablets ($25/30 DS) Narrow therapeutic index Consider 3 rd line therapy due to side-effects and potential toxicity Side-effects include: tachycardia, headache, restlessness, seizures, nausea/vomiting, reflux, tremor Inhaled Corticosteroids Fluticasone (Flovent) HFA inhaler: 44mcg, 110mcg, 220mcg/act ($120, $154, $247/30 DS) Aerosol discs: 50mcg, 100mcg, 250mcg ($115, $116, $155/30 DS) Every 12 hours Budesonide (Pulmicort, Pulmicort Flexhaler) Aerosol inhaler: 90mcg, 180mcg/act ($122, $160/30 DS) Nebs: 0.25mg, 0.5mg/2ml ($412, $520/30 DS) Every 12 hours Beclomethasone (QVAR) Inhaler: 40mcg, 80mcg/act ($92, $110/30 DS) Every 12 hours Mometasone (Asmanex Twisthaler) Aerosol powder: 110mcg, 220mcg/act ($131, $234/30 DS) Every 12 to 24 hours Oral corticosteroids are more cost-effective than inhaled corticosteroids in end-stage disease. 8
9 Oral Corticosteroids Prednisone 10-20mg daily Dexamethasone 2-4mg daily ($12/30 DS) ($22/30 DS) Multiple palliative benefits Improvement of shortness of breath due to inflammation Improvement of inflammatory pain Appetite stimulation Use caution with brittle diabetics or recent GI bleed Combination Products Albuterol & Ipratropium Combivent inhaler: 90-18mcg/act ($280/30 DS) Duoneb nebs: mg/3ml ($160/30 DS) Every 6 hours Fluticasone & Salmeterol (Advair Diskus, Advair HFA) Inhaler: 45-21mcg, mcg/act, mcg/act ($209-$304/30 DS) Aerosol powder: mcg/dose ($186/30 DS) Aerosol powder: mcg/dose ($216/30 DS) Aerosol powder: mcg/dose ($317/30 DS) Every 12 hours Budesonide & Formoterol (Symbicort) Inhaler: mcg, mcg/act ($197, $230/30 DS) Every 12 hours Mometasone & Formoterol (Dulera) Inhaler: 100-5mcg, 200-5mcg/act ($188/30 DS) Every 12 hours Phosphodiesterase-4 Enzyme Inhibitor Daliresp (Roflumilast) FDA approved in 2011 for severe COPD First and only selective PDE-4 inhibitor Anti-inflammatory inflammatory activity Oral tablet 500mcg once daily $250/30 DS Oral corticosteroids are still the preferred antiinflammatory therapy for hospice patients with COPD 9
10 Inhaled vs. Nebulized Treatments Inhalers Available as aerosol or dry powder inhalers Requires coordination Requires variable inhalation effort Rescue inhalers may still be appropriate for ambulatory patients Nebulizers Solution is placed in the nebulizer machine Patient breathes normally through the mouth for the duration of the treatment Mouthpiece or mask used for inhalation Nebulizer treatments are preferred in hospice patients to successfully deliver medications to the lungs. Factors for Device Selection Ability to use device Cognitive function Dexterity and strength Medication availability in desired device Cost and reimbursement Patient preferences and device considerations Educational challenges Importance of Inhaler Technique 2008 observational study of dry powder inhaler use in 224 patients Diskus, Handihaler, Turbohaler, Aerolizer Observed for ineffective inhaler use Technical errors Inadequate respiratory flow 67 patients with COPD 33 patients GOLD I or II 34 patients GOLD III or IV 10

 Significance")





 Inhaler Technique")






11 Results: Influence of Age Error rate increased with age (p<0.01) Significance remained even after adjustment for severity of obstruction and type of training (p<0.05) Results: Influence of Severity Error rate increased with severity of obstruction for the whole group (p<0.01) Error rate also increased within COPD group alone (p<0.05) Inhaler Technique Aerosol Inhalers Require priming before first use Exhale as much air as possible Inhale slowly and deeply while depressing canister Hold breath for 10 seconds Breathe normally Dry Powder Inhalers Require various methods of readying the dose Breath out fully Inhale quickly and deeply Hold breath for 10 seconds Breathe out slowly 11












12 Inhaler Technique Demonstration Volunteers Please! Aerosol inhaler Advair Diskus Spiriva Handihaler Aerosol Inhalers Priming the inhaler Before first use, if not used in 14 days, or if dropped Shake well before each puff Wait at least 1 minute between puffs Cleaning the inhaler Running actuator under warm water for 30 seconds Must be done at least weekly Advair Diskus Open, Click, Inhale Open by sliding thumb grip Click lever away from you Inhale Tips Always keep inhaler level Never breath out into the inhaler 12












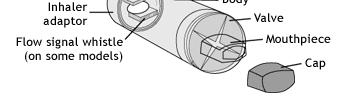
13 Spiriva Handihaler Open Release cap and lift mouthpiece Insert capsule Open immediately before use Pierce the capsule Hold inhaler upright Do not pierce more than once Do not shake Inhale dose Must inhale twice Capsule should rattle inside of inhaler Benefits of a Spacer Helps to overcome common technique problems in the elderly Slows aerosol spray Allows propellant to evaporate, reducing particle size Reduces oropharyngeal deposition Holds dose until inhaled Reduces need for hand-breath coordination Some signal when inhalation is occurring to quickly Downside of a Spacer Bulky Require assembly Increased dexterity may be needed Walls of spacer may have electrostatic Walls of spacer may have electrostatic charges attracting drug particles Reduces size of available dose Minimized by weekly washing and air drying 13

14 Spacer Use Discontinuing Inhalers Video Dyspnea Dyspnea is the sensation of difficulty breathing Mechanism is not entirely clear Occurs in 70-80% of hospice patients Often not successfully treated 14
15 Dyspnea May represent abnormal relationships between neuromuscular effort and air movement in the lung Respiratory muscle fatigue may contribute Patient perception of the underlying cause may increase distress May occur with or without cardiac or lung disease Palliative Care of Dyspnea Identify potentially reversible causes Bronchospasm, congestive heart disease (CHF), infection, pulmonary embolism, effusion, anemia Treat reversible causes, if appropriate Evaluate for use of oxygen or a fan Consider bronchodilators Especially if bilateral wheezing Consider corticosteroids COPD, pulmonary fibrosis, asthma or tumor are present Benzodiazepines for Dyspnea Schedule ATC with higher dose at bedtime Anxiety is always a component of feeling short of breath Start low and titrate up Lorazepam (Ativan) mg every 6-8 hours Alprazolam (Xanax) mg every 6-8 hours Diazepam (Valium) 1-2.5mg every 8-12 hours Goal is to relieve anxiety and calm patient Appropriate doses should not sedate 15
16 Opioids for Dyspnea Use morphine unless contraindicated Oxycodone is preferred in renal failure Start with morphine 2.5-5mg every 1-2 hours prn For opioid naïve patients Higher starting dose may be needed for opioid tolerant patients Schedule every 4 hours if needed frequently Continue to have prn doses available Seldom need more than 5-10mg every 4 hours in an opioid naïve patient Increase benzodiazepine before going above 10-20mg every 4 hours Risk of Treating Dyspnea Easy to overdose if treating physical signs rather than symptoms Treat patient reports of discomfort Not respiratory rate or effort Goal is to relieve subjective symptoms of distress Not necessary to decrease respiratory rate for comfort Role of Oxygen in Dyspnea Duke University Medical Center For those who do benefit from oxygen therapy, researchers discovered that regular room air was just as effective as pure oxygen. The results of the study suggest that any air streams directed toward the nose offer relief from shortness of breath, and that in some cases, a room fan might even be as effective as an oxygen mask. 16



















17 Patient Case 72 yo male with end stage COPD, CHF, osteoarthritis, glaucoma, and gout PPS 30% Bedbound, normal swallowing, requires total care NKDA Medications: Advair 250/50: Inhale 1 puff BID Spiriva 18mcg: Inhale content of 1 cap daily Metoprolol tartrate 25mg: take 1 tab PO BID Lisinopril 20mg: take 1 tab PO daily Allopurinol 100mg: take 1 tab PO daily Ibuprofen 200mg: take 2 tablets PO q8h Tylenol 500mg: Take 1 tab PO q4h prn pain or fever Xalatan 0.005% soln: Instill 1 drop in each eye at bedtime Patient Case SOB symptoms have worsened over the last few weeks. Upon observation of this patient s inhaler technique, you notice patient is having difficulty inhaling gquickly and forcefully when using Advair and Spiriva inhalers. Patient is also not able to consistently rinse mouth after use of Advair. What recommendations would you make for this patient? Questions?? 17
18 References Advair Diskus (fluticasone propionate) package insert. Research Triangle Park, NC: GlaxoSmithKline;2010. Barrons R, Pegram A, Borries A. Inhaler device selection: special considerations in elderly patient with chronic obstructive pulmonary disease. AJHP 2011;68: Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) Available from: Grauer P, Shuster J, Protus BM. Palliative care consultant: a reference guide for palliative care. 3 rd ed. United States: Kendall/Hunt; p. Kamal AH, Maguire JM, Wheeler JL, et al. Dyspnea review for the palliative care professional: treatment goals and therapeutic options. J Pall Med 2012;15: LexiComp Online. Lexi-Drugs Online, Hudson, Ohio: Lexi-Comp,Inc; April 24, Lung disease and respiratory health center. WebMD Available at: ProAir HFA (albuterol sulfate) package insert. Horsham, PA: Teva: Spiriva HandiHaler (tiotropium bromide) package insert. Ridgefield, CT: Boehringer Ingelheim; Thomas JR, von Gunten CF. Management of dyspnea. Supportive Onc. 2003;1: Wieshammer S, Dreyhaupt J. Dry powder inhalers: which factors determine the frequency of handling errors? Respiration 2008;75:
Medications for Managing COPD in Hospice Patients. Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources
 Medications for Managing COPD in Hospice Patients Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources Goal of medications in COPD Decrease symptoms and/or complications Reduce frequency
Medications for Managing COPD in Hospice Patients Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources Goal of medications in COPD Decrease symptoms and/or complications Reduce frequency
A Visual Approach to Simplifying Respiratory Drug Regimens
 A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP October 23, 2017 Learning Objectives Be able to list at least 3 major adverse effects of inhaled medications
A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP October 23, 2017 Learning Objectives Be able to list at least 3 major adverse effects of inhaled medications
A Visual Approach to Simplifying Respiratory Drug Regimens
 Adverse Effects of Inhaled Medications A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP June 28, 2017 Drug Category Beta 2 agonists antagonists Adverse Effects
Adverse Effects of Inhaled Medications A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP June 28, 2017 Drug Category Beta 2 agonists antagonists Adverse Effects
A Visual Approach to Simplifying Respiratory Drug Regimens
 A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP 3 Main Categories Inhaled Respiratory Drugs Binds to beta-2 receptors Relaxation of smooth muscles in the lung
A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP 3 Main Categories Inhaled Respiratory Drugs Binds to beta-2 receptors Relaxation of smooth muscles in the lung
The Medical Letter. on Drugs and Therapeutics
 The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
Inhaled bronchodilators relax constricted airways and treat the noisy part of asthma: coughing, wheezing, choking and shortness of breath.
 Inhaled bronchodilators relax constricted airways and treat the noisy part of asthma: coughing, wheezing, choking and shortness of breath. AccuNeb inhalation 0.021% solution: 0.63mg/3mL 3-4 times solution
Inhaled bronchodilators relax constricted airways and treat the noisy part of asthma: coughing, wheezing, choking and shortness of breath. AccuNeb inhalation 0.021% solution: 0.63mg/3mL 3-4 times solution
Correct Use of Inhaler Devices
 PL Detail-Document #300206 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER February 2014 Correct Use of
PL Detail-Document #300206 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER February 2014 Correct Use of
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Diagnosis and Management of Asthma
 Supporting Evidence: Diagnosis and Management of Asthma The subdivision of this section is: Appendix B Tables Copyright 2016 by 1 Eleventh Edition/December 2016 Appendix B Asthma Summary Tables Class:
Supporting Evidence: Diagnosis and Management of Asthma The subdivision of this section is: Appendix B Tables Copyright 2016 by 1 Eleventh Edition/December 2016 Appendix B Asthma Summary Tables Class:
Ferris State University College of Pharmacy MPA CE Symposium 2016 Paul Thill, PharmD, BCPS
 Ferris State University College of Pharmacy MPA CE Symposium 2016 Paul Thill, PharmD, BCPS Objectives Categorize the new asthma and COPD inhalers in to existing or newly created categories Discuss the
Ferris State University College of Pharmacy MPA CE Symposium 2016 Paul Thill, PharmD, BCPS Objectives Categorize the new asthma and COPD inhalers in to existing or newly created categories Discuss the
Select Inhaled Respiratory Agents
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
II: Moderate Worsening airflow limitations Dyspnea on exertion, cough, and sputum production; patient usually seeks medical
 Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
How to Use Inhaled Medications for Asthma and COPD
 How to Use Inhaled Medications for Asthma and COPD This information is not intended to diagnose health problems or to take the place of medical advice or care you receive from your physician or other health
How to Use Inhaled Medications for Asthma and COPD This information is not intended to diagnose health problems or to take the place of medical advice or care you receive from your physician or other health
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease CareOregon Pharmacy Abridged sample of presentation content Home Equipment Pathophysiology Exacerbations Guidelines Lifestyle Modification Medication Management Sample
Chronic Obstructive Pulmonary Disease CareOregon Pharmacy Abridged sample of presentation content Home Equipment Pathophysiology Exacerbations Guidelines Lifestyle Modification Medication Management Sample
End Stage COPD Guidance Document
 End Stage COPD Guidance Document Suggested Guidelines for the Determination of Hospice Eligibility A patient with severe chronic pulmonary disease that meets the following criteria may be eligible for
End Stage COPD Guidance Document Suggested Guidelines for the Determination of Hospice Eligibility A patient with severe chronic pulmonary disease that meets the following criteria may be eligible for
Your Inhaler Devices & You
 1 Your Inhaler Devices & You COUNSEL ON THE APPROPRIATE USE OF A: METERED DOSE INHALER (MDI) DRY POWDER INHALER (DPI) DISCUSS THE APPROPRIATE USAGE OF A PEAK FLOW METER AND SPACER/HOLDING CHAMBER DEVICE
1 Your Inhaler Devices & You COUNSEL ON THE APPROPRIATE USE OF A: METERED DOSE INHALER (MDI) DRY POWDER INHALER (DPI) DISCUSS THE APPROPRIATE USAGE OF A PEAK FLOW METER AND SPACER/HOLDING CHAMBER DEVICE
TRELEGY ELLIPTA (fluticasone-umeclidinium-vilanterol) aerosol powder
 aerosol powder") TRELEGY ELLIPTA (fluticasone-umeclidinium-vilanterol) aerosol powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
TRELEGY ELLIPTA (fluticasone-umeclidinium-vilanterol) aerosol powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
What You Need to Know about Metered-Dose Inhalers and the HFA Propellant
 What You Need to Know about Metered- Inhalers and the HFA Propellant There are a number ways to deliver inhaled medication. They include: Metered-dose inhaler () Metered-dose inhaler with spacer/holding
What You Need to Know about Metered- Inhalers and the HFA Propellant There are a number ways to deliver inhaled medication. They include: Metered-dose inhaler () Metered-dose inhaler with spacer/holding
COPD Medicine. No one ever showed me how to use this. Wendy Happel; RRT, COPD Educator Krystal Fedoris; RRT-NPS, BA, COPD Educator
 Medicine. No one ever showed me how to use this. Wendy Happel; RRT, Educator Krystal Fedoris; RRT-NPS, BA, Educator 1 Taking prescriptions correctly Taking prescriptions can be a challenge Busy schedules
Medicine. No one ever showed me how to use this. Wendy Happel; RRT, Educator Krystal Fedoris; RRT-NPS, BA, Educator 1 Taking prescriptions correctly Taking prescriptions can be a challenge Busy schedules
STRIVERDI RESPIMAT (olodaterol hcl) aerosol
 aerosol") STRIVERDI RESPIMAT (olodaterol hcl) aerosol Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
STRIVERDI RESPIMAT (olodaterol hcl) aerosol Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
10/18/2012. Penn State University Children s Hospital JODIE STABINSKI CRNP MSN AE-C
 Penn State University Children s Hospital JODIE STABINSKI CRNP MSN AE-C Daily: Long-Term Control Corticosteroids (inhaled and systemic) Long-acting beta 2 -agonists (Serevent, Foradil) Methylxanthines
Penn State University Children s Hospital JODIE STABINSKI CRNP MSN AE-C Daily: Long-Term Control Corticosteroids (inhaled and systemic) Long-acting beta 2 -agonists (Serevent, Foradil) Methylxanthines
How to Use Inhaled Medications
 How to Use Inhaled Medications FOR ASTHMA AND COPD introduction Inhaled medications are an important part of controlling and treating asthma and chronic obstructive pulmonary disease (COPD). The medication
How to Use Inhaled Medications FOR ASTHMA AND COPD introduction Inhaled medications are an important part of controlling and treating asthma and chronic obstructive pulmonary disease (COPD). The medication
Improving Outcomes in COPD
 Neil MacIntyre MD Duke University Durham NC Current treatment guidelines f COPD focus Barriers to providing optimal treatment Diagnosis of COPD EXPOSURE TO RISK FACTORS AND/ OR SYMPTOMS sputum cough dyspnea
Neil MacIntyre MD Duke University Durham NC Current treatment guidelines f COPD focus Barriers to providing optimal treatment Diagnosis of COPD EXPOSURE TO RISK FACTORS AND/ OR SYMPTOMS sputum cough dyspnea
Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management. Colleen Sakon, PharmD BCPS September 27, 2018
 Management. Colleen Sakon, PharmD BCPS September 27, 2018") Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management Colleen Sakon, PharmD BCPS September 27, 2018 Disclosures I have no actual or potential conflicts of interest 2 Objectives Summarize
Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management Colleen Sakon, PharmD BCPS September 27, 2018 Disclosures I have no actual or potential conflicts of interest 2 Objectives Summarize
MANAGING ASTHMA. Nancy Davis, RRT, AE-C
 MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
MDI Bonanza. Dwayne Griffin, DO
 MDI Bonanza Dwayne Griffin, DO Bonanza 3. A MDI costing $200 - $500 per month SISYPHUS MDI Griffin Mountain Evolution of Deliver Systems for COPD in the US 2003 2009 2011 2013 2004 2012 2014 Prescribing
MDI Bonanza Dwayne Griffin, DO Bonanza 3. A MDI costing $200 - $500 per month SISYPHUS MDI Griffin Mountain Evolution of Deliver Systems for COPD in the US 2003 2009 2011 2013 2004 2012 2014 Prescribing
Provider Respiratory Inservice
 Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
COPD Update. Plus New and Improved Products for Inhaled Therapy. Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor
 COPD Update Plus New and Improved Products for Inhaled Therapy Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose concerning possible financial
COPD Update Plus New and Improved Products for Inhaled Therapy Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose concerning possible financial
Incorporating Newer Therapies and Strategies to Improve COPD Outcomes: A Practical Guide for Pharmacists. Learning Objectives.
 Incorporating Newer Therapies and Strategies to Improve COPD Outcomes: A Practical Guide for Pharmacists Learning Objectives Identify the risk factors for COPD and the clinical features that differentiate
Incorporating Newer Therapies and Strategies to Improve COPD Outcomes: A Practical Guide for Pharmacists Learning Objectives Identify the risk factors for COPD and the clinical features that differentiate
Appendix M: Device Technique
 Nursing Care of Dyspnea: The 6th Vital Sign in Individuals with Chronic Obstructive Pulmonary Disease (COPD) Appendix M: Device Technique Medications: Inhalation Devices Medications come in many forms.
Nursing Care of Dyspnea: The 6th Vital Sign in Individuals with Chronic Obstructive Pulmonary Disease (COPD) Appendix M: Device Technique Medications: Inhalation Devices Medications come in many forms.
Respiratory Medications and Devices Update 2/15
 Respiratory Medications and Devices Update 2/15 Dewey Hahlbohm, PA-C, AE-C Wendy Brown, Pharm.D., MPAS, PA-C, AE-C Objectives! Review mechanism of action for asthma pharmacologic agents! Describe key patient
Respiratory Medications and Devices Update 2/15 Dewey Hahlbohm, PA-C, AE-C Wendy Brown, Pharm.D., MPAS, PA-C, AE-C Objectives! Review mechanism of action for asthma pharmacologic agents! Describe key patient
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Seebri Neohaler) Reference Number: CP.CPA.150 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Seebri Neohaler) Reference Number: CP.CPA.150 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy
12/18/2017. Disclosures. Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Medications Affecting The Respiratory System
 Medications Affecting The Respiratory System Overview Asthma is a chronic inflammatory disorder of the airways. It is an intermittent and reversible airflow obstruction that affects the bronchioles. The
Medications Affecting The Respiratory System Overview Asthma is a chronic inflammatory disorder of the airways. It is an intermittent and reversible airflow obstruction that affects the bronchioles. The
QUANTITY LIMIT CRITERIA. BROVANA (arformoterol tartrate) SEREVENT DISKUS (salmeterol) STRIVERDI RESPIMAT (olodaterol)
 SEREVENT DISKUS (salmeterol) STRIVERDI RESPIMAT (olodaterol)") Carelirst. +.V Family of health care plans DRUG CLASS COMBINATIONS QUANTITY LIMIT CRITERIA LONG ACTING BETA2-ADRENERGIC AGONIST, ORAL INHALATION BRAND NAME (generic) LONG-ACTING BETA2-ADRENERGIC AGONISTS:
Carelirst. +.V Family of health care plans DRUG CLASS COMBINATIONS QUANTITY LIMIT CRITERIA LONG ACTING BETA2-ADRENERGIC AGONIST, ORAL INHALATION BRAND NAME (generic) LONG-ACTING BETA2-ADRENERGIC AGONISTS:
MEDICATION GUIDE. ADVAIR [ad vair] HFA 45/21 (fluticasone propionate 45 mcg and salmeterol 21 mcg) Inhalation Aerosol
![MEDICATION GUIDE. ADVAIR [ad vair] HFA 45/21 (fluticasone propionate 45 mcg and salmeterol 21 mcg) Inhalation Aerosol](/thumbs/78/76835983.jpg "MEDICATION GUIDE. ADVAIR [ad vair] HFA 45/21 (fluticasone propionate 45 mcg and salmeterol 21 mcg) Inhalation Aerosol") MEDICATION GUIDE ADVAIR [ad vair] HFA 45/21 (fluticasone propionate 45 mcg and salmeterol 21 mcg) Inhalation Aerosol ADVAIR HFA 115/21 (fluticasone propionate 115 mcg and salmeterol 21 mcg) Inhalation
MEDICATION GUIDE ADVAIR [ad vair] HFA 45/21 (fluticasone propionate 45 mcg and salmeterol 21 mcg) Inhalation Aerosol ADVAIR HFA 115/21 (fluticasone propionate 115 mcg and salmeterol 21 mcg) Inhalation
Common Inhaled Asthma Medications Dose Comparison and Tips for Use
 Detail-Document #210303 This Detail-Document accompanies the related article published in PHARMACIST S LETTER / PRESCRIBER S LETTER March 2005 ~ Volume 21 ~ Number 210303 Common Inhaled Asthma Medications
Detail-Document #210303 This Detail-Document accompanies the related article published in PHARMACIST S LETTER / PRESCRIBER S LETTER March 2005 ~ Volume 21 ~ Number 210303 Common Inhaled Asthma Medications
How can I benefit most from my COPD medications?
 Fact Sheet: COPD Medications and Delivery Devices How can I benefit most from my COPD medications? COPD medications can improve your symptoms. By taking the right medication at the right time, you can
Fact Sheet: COPD Medications and Delivery Devices How can I benefit most from my COPD medications? COPD medications can improve your symptoms. By taking the right medication at the right time, you can
MANAGEMENT OF ASTHMA SPRING Presented by:
 MEDS@Work MANAGEMENT OF ASTHMA SPRING 2013 Presented by: Lusia Fomuso PharmD candidate 2014 Olivia Sibailly PharmD candidate 2014 Kimberly Biedka PharmD candidate 2014 Dr. Donna Bartlett PharmD CGP RPh
MEDS@Work MANAGEMENT OF ASTHMA SPRING 2013 Presented by: Lusia Fomuso PharmD candidate 2014 Olivia Sibailly PharmD candidate 2014 Kimberly Biedka PharmD candidate 2014 Dr. Donna Bartlett PharmD CGP RPh
Overview. The Respiratory System. Chapter 18. Respiratory Emergencies 9/11/2012
 Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Reference Guide for Caring for Pediatric Patients with Asthma
 Reference Guide for Caring for Pediatric Patients with Asthma Co-Chair: Nancy Cantey Banasiak, DNP, PPCNP-BC, APRN Co-Chair: Deborah Hickman, DNP, APRN-CNP, CPNP-PC, NNP-BC Asthma and Allergy SIG Members
Reference Guide for Caring for Pediatric Patients with Asthma Co-Chair: Nancy Cantey Banasiak, DNP, PPCNP-BC, APRN Co-Chair: Deborah Hickman, DNP, APRN-CNP, CPNP-PC, NNP-BC Asthma and Allergy SIG Members
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
NEBULIZERS, METERED DOSE INHALERS, AND DRY POWDER INHALERS
 NEBULIZERS, METERED DOSE INHALERS, AND DRY POWDER INHALERS Douglas S. Gardenhire, Ed.D, RRT-NPS MODULE 1 Manipulate Small Volume Nebulizers by Order or Protocol 1 Objectives for Module 1 At the end of
NEBULIZERS, METERED DOSE INHALERS, AND DRY POWDER INHALERS Douglas S. Gardenhire, Ed.D, RRT-NPS MODULE 1 Manipulate Small Volume Nebulizers by Order or Protocol 1 Objectives for Module 1 At the end of
BREEZHALER. Medications available: Onbrez (indacaterol maleate) Seebri (glycopyrronium bromide) Ultibro (glycopyrronium bromide/ (indacaterol maleate)
 Seebri (glycopyrronium bromide) Ultibro (glycopyrronium bromide/ (indacaterol maleate)") Medications available: Onbrez (indacaterol maleate) Seebri (glycopyrronium bromide) Ultibro (glycopyrronium bromide/ (indacaterol maleate) BREEZHALER Please date initial after you have directly observed
Medications available: Onbrez (indacaterol maleate) Seebri (glycopyrronium bromide) Ultibro (glycopyrronium bromide/ (indacaterol maleate) BREEZHALER Please date initial after you have directly observed
Nancy Davis, RRT, AE-C
 Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
PATIENT INFORMATION. ADVAIR DISKUS [AD vair DISK us] (fluticasone propionate and salmeterol inhalation powder) for oral inhalation
![PATIENT INFORMATION. ADVAIR DISKUS [AD vair DISK us] (fluticasone propionate and salmeterol inhalation powder) for oral inhalation](/thumbs/74/71128680.jpg "PATIENT INFORMATION. ADVAIR DISKUS [AD vair DISK us] (fluticasone propionate and salmeterol inhalation powder) for oral inhalation") PATIENT INFORMATION ADVAIR DISKUS [AD vair DISK us] (fluticasone propionate and salmeterol inhalation powder) for oral inhalation What is ADVAIR DISKUS? ADVAIR DISKUS combines the inhaled corticosteroid
PATIENT INFORMATION ADVAIR DISKUS [AD vair DISK us] (fluticasone propionate and salmeterol inhalation powder) for oral inhalation What is ADVAIR DISKUS? ADVAIR DISKUS combines the inhaled corticosteroid
BREEZHALER. Medications available: Onbrez (indacaterol maleate) Seebri (glycopyrronium bromide) Ultibro (glycopyrronium bromide/ (indacaterol maleate)
 Seebri (glycopyrronium bromide) Ultibro (glycopyrronium bromide/ (indacaterol maleate)") Medications available: Onbrez (indacaterol maleate) Seebri (glycopyrronium bromide) Ultibro (glycopyrronium bromide/ (indacaterol maleate) BREEZHALER Please date initial after you have directly observed
Medications available: Onbrez (indacaterol maleate) Seebri (glycopyrronium bromide) Ultibro (glycopyrronium bromide/ (indacaterol maleate) BREEZHALER Please date initial after you have directly observed
BREEZHALER. Medications available: Onbrez (indacaterol maleate) Seebri (glycopyrronium bromide) Ultibro (glycopyrronium bromide/ (indacaterol maleate)
 Seebri (glycopyrronium bromide) Ultibro (glycopyrronium bromide/ (indacaterol maleate)") Medications available: Onbrez (indacaterol maleate) Seebri (glycopyrronium bromide) Ultibro (glycopyrronium bromide/ (indacaterol maleate) BREEZHALER Please date initial after you have directly observed
Medications available: Onbrez (indacaterol maleate) Seebri (glycopyrronium bromide) Ultibro (glycopyrronium bromide/ (indacaterol maleate) BREEZHALER Please date initial after you have directly observed
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy f the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy f the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
AIRDUO RESPICLICK (fluticasone-salmeterol) aerosol DULERA (mometasone furoate and formoterol fumarate dihydrate) aerosol
 aerosol DULERA (mometasone furoate and formoterol fumarate dihydrate) aerosol") DULERA (mometasone furoate and formoterol fumarate dihydrate) aerosol Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
DULERA (mometasone furoate and formoterol fumarate dihydrate) aerosol Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Asthma medications: Know your options - MayoClinic.com. Asthma medications: Know your options
 MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
Asthma. Definition. Symptoms
 Asthma Definition Asthma is a condition in which your airways narrow and swell and produce extra mucus. This can make breathing difficult and trigger coughing, wheezing and shortness of breath. For some
Asthma Definition Asthma is a condition in which your airways narrow and swell and produce extra mucus. This can make breathing difficult and trigger coughing, wheezing and shortness of breath. For some
Using an Inhaler and Nebulizer
 Using an Inhaler and Nebulizer Introduction An inhaler is a handheld device that is used to deliver medication directly to your airways. A nebulizer is an electric or battery powered machine that turns
Using an Inhaler and Nebulizer Introduction An inhaler is a handheld device that is used to deliver medication directly to your airways. A nebulizer is an electric or battery powered machine that turns
Function of the Respiratory System. Exchange CO2 (on expiration) for O2 (on inspiration)
 for O2 (on inspiration)") Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Assessing Severity. Management of Stable COPD. General Approach. Short Acting Bronchodilators. Staging System (GOLD)
") William P. Saliski Jr. DO Montgomery Pulmonary Consultants Management of Stable COPD Pharmacotherapy Oxygen Smoking Cessation Vaccinations Rehabilitation Surgery Future Discussions Assessing Severity Staging
William P. Saliski Jr. DO Montgomery Pulmonary Consultants Management of Stable COPD Pharmacotherapy Oxygen Smoking Cessation Vaccinations Rehabilitation Surgery Future Discussions Assessing Severity Staging
NHS Northern, Eastern and Western Devon Clinical Commissioning Group NHS South Devon and Torbay Clinical Commissioning Group
 NHS Northern, Eastern and Western Devon Clinical Commissioning Group NHS South Devon and Torbay Clinical Commissioning Group Inhaler technique and respiratory conditions Guidance Sheet 16 When diagnosed
NHS Northern, Eastern and Western Devon Clinical Commissioning Group NHS South Devon and Torbay Clinical Commissioning Group Inhaler technique and respiratory conditions Guidance Sheet 16 When diagnosed
Foundations of Pharmacology
 Pharmacologic Management of Asthma Objectives: 1. Review the physiological basis for asthma therapy 2. Discuss the differences between SABA and LABA 3. Discuss the role of inhaled and oral systemic corticosteroids
Pharmacologic Management of Asthma Objectives: 1. Review the physiological basis for asthma therapy 2. Discuss the differences between SABA and LABA 3. Discuss the role of inhaled and oral systemic corticosteroids
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be
 1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
Overview of COPD INTRODUCTION
 Overview of COPD INTRODUCTION Chronic obstructive pulmonary disease (COPD) is a common lung disease that affects millions of people, and it is the fourth leading cause of death in the United States. It
Overview of COPD INTRODUCTION Chronic obstructive pulmonary disease (COPD) is a common lung disease that affects millions of people, and it is the fourth leading cause of death in the United States. It
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Better Living with Obstructive Pulmonary Disease A Patient Guide
 Better Living with Obstructive Pulmonary Disease A Patient Guide Second Edition November 2012 Queensland Health a Better Living with Chronic Obstructive Pulmonary Disease A Patient Guide is a joint project
Better Living with Obstructive Pulmonary Disease A Patient Guide Second Edition November 2012 Queensland Health a Better Living with Chronic Obstructive Pulmonary Disease A Patient Guide is a joint project
Key features and changes to these four components of asthma care include:
 Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Women Beware-The Threat of COPD
 Page 1 Speaker: Catherine Cooke attained her Bachelor in Pharmacy from the University of Iowa and then went on to receive her Pharm.D. from the Medical University of South Carolina. Subsequently, she completed
Page 1 Speaker: Catherine Cooke attained her Bachelor in Pharmacy from the University of Iowa and then went on to receive her Pharm.D. from the Medical University of South Carolina. Subsequently, she completed
Asthma Education. The Keys to Asthma Prevention and Control. what to do when one s asthma is flared! Lucile Packard Children s Hospital.
 Asthma Education Lucile Packa r d Children s H o spit al Created by Rachel Lawler RN, MSN, cpnp, AE-C, NPAT Pulmonary Pediatric Nurse Practitioner Lucile Packard Children s Hospital The Keys to Asthma
Asthma Education Lucile Packa r d Children s H o spit al Created by Rachel Lawler RN, MSN, cpnp, AE-C, NPAT Pulmonary Pediatric Nurse Practitioner Lucile Packard Children s Hospital The Keys to Asthma
UPMC HEALTH PLAN COPD CLINICAL PRACTICE GUIDELINE
 Relevance to Population: COPD affects 12 million people in the United States, making it the 4 th leading cause of mortality and the 2 nd leading cause of disability. It is predicted that these statistics
Relevance to Population: COPD affects 12 million people in the United States, making it the 4 th leading cause of mortality and the 2 nd leading cause of disability. It is predicted that these statistics
Home Management Plan. Cover Page
 Home Management Plan Cover Page What is Asthma? Asthma is a chronic disease of the lungs caused by swelling and irritation in the lining of airways Tightness of the airway muscles Excess mucus in the airways
Home Management Plan Cover Page What is Asthma? Asthma is a chronic disease of the lungs caused by swelling and irritation in the lining of airways Tightness of the airway muscles Excess mucus in the airways
Drugs that Affect the Respiratory System BROOKE BENTLEY, PHD, APRN
 Drugs that Affect the Respiratory System BROOKE BENTLEY, PHD, APRN Goals of Therapy Asthma Prevent symptoms COPD Reduce COPD symptoms Decrease use of SABAs Maintain normal pulm function & prevent loss
Drugs that Affect the Respiratory System BROOKE BENTLEY, PHD, APRN Goals of Therapy Asthma Prevent symptoms COPD Reduce COPD symptoms Decrease use of SABAs Maintain normal pulm function & prevent loss
Respiratory Health. Asthma and COPD
 Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
Firefighter Pre-Hospital Care Program Recruit Presentation. Respiratory Emergencies
 Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
Women Beware The Threat of COPD
 Page 1 Women Beware The Threat of COPD Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. & Clinical Associate Professor, University of Maryland School of Pharmacy Supported by an education
Page 1 Women Beware The Threat of COPD Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. & Clinical Associate Professor, University of Maryland School of Pharmacy Supported by an education
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 CHRONIC OBSTRUCTIVE PULMONARY DISEASE INCIDENCE UP TO 380,000 PEOPLE IN IRELAND HSE FIGURES 110,000 DIAGNOSED AND 200,000 UNDIAGNOSED. AFFECTS MORE MEN THAN WOMEN BUT RATES ARE RISING 1500 DEATHS PER YEAR
CHRONIC OBSTRUCTIVE PULMONARY DISEASE INCIDENCE UP TO 380,000 PEOPLE IN IRELAND HSE FIGURES 110,000 DIAGNOSED AND 200,000 UNDIAGNOSED. AFFECTS MORE MEN THAN WOMEN BUT RATES ARE RISING 1500 DEATHS PER YEAR
primer on inhalers and nebulizers
 CREDIT: 2.0 Continuing Education EARN CE CREDIT FOR THIS ACTIVITY AT WWW.DRUGTOPICS.COM AN ONGOING CE PROGRAM OF THE UNIVERSITY OF CONNECTICUT SCHOOL OF PHARMACY AND DRUG TOPICS educational objectives
CREDIT: 2.0 Continuing Education EARN CE CREDIT FOR THIS ACTIVITY AT WWW.DRUGTOPICS.COM AN ONGOING CE PROGRAM OF THE UNIVERSITY OF CONNECTICUT SCHOOL OF PHARMACY AND DRUG TOPICS educational objectives
Dyspnea. Stephanie Lindsay
 Dyspnea Stephanie Lindsay What is dyspnea? An unpleasant sensation of difficult, labored breathing Shortness of air Dyspnea is not the same as tachypnea therefore patients may not present with rapid breathing
Dyspnea Stephanie Lindsay What is dyspnea? An unpleasant sensation of difficult, labored breathing Shortness of air Dyspnea is not the same as tachypnea therefore patients may not present with rapid breathing
Asthma COPD Update 2018
 Asthma COPD Update 2018 Roger Hefflinger, Pharm.D. Clinical Associate Professor ISU COP Clinical Teaching Pharmacist Family Medicine Residency of Idaho In support of improving patient care, Idaho State
Asthma COPD Update 2018 Roger Hefflinger, Pharm.D. Clinical Associate Professor ISU COP Clinical Teaching Pharmacist Family Medicine Residency of Idaho In support of improving patient care, Idaho State
Pharmacist Objectives. Pulmonary Update. Outline. Technician Objectives. GOLD Guidelines. COPD Diagnosis 9/22/2017
 Pharmacist Objectives Pulmonary Update Patty Marshik, PharmD Associate Professor University of New Mexico College of Pharmacy pmarshik@salud.unm.edu Discuss the new Global Initiative for Chronic Obstructive
Pharmacist Objectives Pulmonary Update Patty Marshik, PharmD Associate Professor University of New Mexico College of Pharmacy pmarshik@salud.unm.edu Discuss the new Global Initiative for Chronic Obstructive
Disclosure. Case. Objectives. Case Continued. Inhalers. Asthma: A GINA Update to the NAEPP 2007 Guidelines 1/20/2015
 Disclosure Asthma: A GINA Update to the NAEPP 2007 Guidelines Robert (RC) Hellinga, Pharm.D. PGY 1 Pharmacy Resident Wolfson Children s Hospital/Baptist Health I do not have a vested interest in or affiliation
Disclosure Asthma: A GINA Update to the NAEPP 2007 Guidelines Robert (RC) Hellinga, Pharm.D. PGY 1 Pharmacy Resident Wolfson Children s Hospital/Baptist Health I do not have a vested interest in or affiliation
How to use your QVAR RediHaler (beclomethasone dipropionate)
") (beclomethasone dipropionate) 40 mcg, 80 mcg What is my prescription? Special instructions Take every day to control your symptoms. Rinse mouth thoroughly with water and spit after each use. What can I
(beclomethasone dipropionate) 40 mcg, 80 mcg What is my prescription? Special instructions Take every day to control your symptoms. Rinse mouth thoroughly with water and spit after each use. What can I
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
Aerospan (flunisolide)
") STRENGTH DOSAGE FORM ROUTE GPID 80mcg/actuation HFA aerosol inhaler w/ Inhaled 35718 8.9 g/canister adapter MANUFACTURER Meda Pharmaceuticals INDICATION Aerospan Inhalation Aerosol is indicated for the
STRENGTH DOSAGE FORM ROUTE GPID 80mcg/actuation HFA aerosol inhaler w/ Inhaled 35718 8.9 g/canister adapter MANUFACTURER Meda Pharmaceuticals INDICATION Aerospan Inhalation Aerosol is indicated for the
Using Inhaled Corticosteroids as Needed for Asthma: giving patients relief or leaving them breathless?
 Using Inhaled Corticosteroids as Needed for Asthma: giving patients relief or leaving them breathless? Lindsay Thomas, Pharm.D. PGY2 Ambulatory Care Resident Department of Pharmacotherapy and Pharmacy
Using Inhaled Corticosteroids as Needed for Asthma: giving patients relief or leaving them breathless? Lindsay Thomas, Pharm.D. PGY2 Ambulatory Care Resident Department of Pharmacotherapy and Pharmacy
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
INHALERS for COPD INTRODUCTION. Types of inhalers. Inhaler technique. MDIs for COPD WET AEROSOLS. Dr Christopher Worsnop
 INHALERS for COPD Dr Christopher Worsnop Department of Respiratory Medicine Austin Hospital INTRODUCTION Most drugs for COPD are given via inhalers. This reduces the dose that needs to be given and delivers
INHALERS for COPD Dr Christopher Worsnop Department of Respiratory Medicine Austin Hospital INTRODUCTION Most drugs for COPD are given via inhalers. This reduces the dose that needs to be given and delivers
Asthma By Mayo Clinic staff
 MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
Question I was one of the first dry power devices available in the US Flovent, Serevent and Advair are all available in this device
 What Device am I Class Side Effects History Potpourri Monitoring Tools 10 10 10 10 10 20 20 20 20 20 30 30 30 30 30 40 40 40 40 40 50 50 50 50 50 WHAT KIND OF DEVICE AM I? I was one of the first dry power
What Device am I Class Side Effects History Potpourri Monitoring Tools 10 10 10 10 10 20 20 20 20 20 30 30 30 30 30 40 40 40 40 40 50 50 50 50 50 WHAT KIND OF DEVICE AM I? I was one of the first dry power
First to Market or 505 (b)2 CMC Considerations IPAC-RS/UF Orlando Inhalation Conference Orlando, Florida
2 CMC Considerations IPAC-RS/UF Orlando Inhalation Conference Orlando, Florida") First to Market or 505 (b)2 CMC Considerations IPAC-RS/UF Orlando Inhalation Conference Orlando, Florida Prasad Peri, Ph.D., Branch Chief, ONDQA, FDA March 19, 2014 1 Topics for discussion Introduction
First to Market or 505 (b)2 CMC Considerations IPAC-RS/UF Orlando Inhalation Conference Orlando, Florida Prasad Peri, Ph.D., Branch Chief, ONDQA, FDA March 19, 2014 1 Topics for discussion Introduction
MEDICAL COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 07/05/18 SECTION: DRUGS LAST REVIEW DATE: LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 CINQAIR (reslizumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
CINQAIR (reslizumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
COPD. Definitionn. make. when (bronchioles) in. the lungs. Wheezing Chest tightness. your lungs. greenish. Lack of energy
 in. the lungs. Wheezing Chest tightness. your lungs. greenish. Lack of energy") COPD Definitionn Emphysema and chronic bronchitis are the two most common conditions thatt make up COPD. Chronic bronchitis is an inflammation of the lining of your bronchial tubes, which carry air to
COPD Definitionn Emphysema and chronic bronchitis are the two most common conditions thatt make up COPD. Chronic bronchitis is an inflammation of the lining of your bronchial tubes, which carry air to
Prescribing guidelines: Management of COPD in Primary Care
 Prescribing guidelines: Management of COPD in Primary Care Establish diagnosis of COPD in patients 35 years with appropriate symptoms with history, examination and spirometry (FEV1/FVC ratio < 70%) Establish
Prescribing guidelines: Management of COPD in Primary Care Establish diagnosis of COPD in patients 35 years with appropriate symptoms with history, examination and spirometry (FEV1/FVC ratio < 70%) Establish
COPD Diagnosis, Management and Program
 COPD Diagnosis, Management and Program RYAN MARTIN, MD NEBRASKA PULMONARY SPECIALTIES Initial diagnosis Setting matters: Inpatient. Usually sicker, oftentimes avoiding healthcare. Outpatient. Often seeking
COPD Diagnosis, Management and Program RYAN MARTIN, MD NEBRASKA PULMONARY SPECIALTIES Initial diagnosis Setting matters: Inpatient. Usually sicker, oftentimes avoiding healthcare. Outpatient. Often seeking
Inhalation devices, proper technique and cleaning
 Preventing Your Symptoms and Taking Your Medications Inhalation devices, proper technique and cleaning Knowing how to use your medications properly is important because inhaled drugs are meant to get directly
Preventing Your Symptoms and Taking Your Medications Inhalation devices, proper technique and cleaning Knowing how to use your medications properly is important because inhaled drugs are meant to get directly
Chapter 10 The Respiratory System
 Chapter 10 The Respiratory System Biology 2201 Why do we breathe? Cells carry out the reactions of cellular respiration in order to produce ATP. ATP is used by the cells for energy. All organisms need
Chapter 10 The Respiratory System Biology 2201 Why do we breathe? Cells carry out the reactions of cellular respiration in order to produce ATP. ATP is used by the cells for energy. All organisms need
Asthma & COPD Medication Review. Hutchison Disclosures 2/16/2017. Objectives
 Asthma & COPD Medication Review Anna Meador, PharmD, BCACP Assistant Professor/ Pharmacy Director McWhorter School of Pharmacy/ Christ Health Center Amber Hutchison, PharmD, BCPS Assistant Clinical Professor
Asthma & COPD Medication Review Anna Meador, PharmD, BCACP Assistant Professor/ Pharmacy Director McWhorter School of Pharmacy/ Christ Health Center Amber Hutchison, PharmD, BCPS Assistant Clinical Professor
reslizumab (Cinqair )
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Respiratory Emergencies. Chapter 11
 Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
COPD. Stan Kellar, MD. Physiology 11/4/2014. Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine
 Stan Kellar, MD Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine COPD Physiology The lungs are filters Filter in oxygen Filter out carbon dioxide (Vascular filter, not part of this discussion)
Stan Kellar, MD Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine COPD Physiology The lungs are filters Filter in oxygen Filter out carbon dioxide (Vascular filter, not part of this discussion)
Learning Objective. Asthma. Discuss the pathophysiology, clinical presentation, diagnosis, and treatment of Asthma 2/22/2017
 Marianne Curran, PA C 3/1/17 Learning Objective Discuss the pathophysiology, clinical presentation, diagnosis, and treatment of Definition many variations Chronic Disorder with Reversible (Intermittent
Marianne Curran, PA C 3/1/17 Learning Objective Discuss the pathophysiology, clinical presentation, diagnosis, and treatment of Definition many variations Chronic Disorder with Reversible (Intermittent
Asthma in Pregnancy. Asthma. Chronic Airway Inflammation. Objective Measures of Airflow. Peak exp. flow rate (PEFR)
") Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Allergies and Asthma 5/21/2013. Objectives. Allergic Rhinitis (AR): Risk Factor for ASTHMA. Rhinitis and Asthma
: Risk Factor for ASTHMA. Rhinitis and Asthma") Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
Hospice High Dollar Medications and Possible Alternatives
 Hospice High Dollar Medications and Possible Alternatives Ly M. Dang, PharmD LDang@HospicePharmacySolutions.com Director of Pharmacy Operations Hospice Pharmacy Solutions Topics of Discussion Hospice Coverage
Hospice High Dollar Medications and Possible Alternatives Ly M. Dang, PharmD LDang@HospicePharmacySolutions.com Director of Pharmacy Operations Hospice Pharmacy Solutions Topics of Discussion Hospice Coverage