COPD Robert Schilz DO, PhD Pulmonary, Critical Care and Sleep Medicine University Hospitals Case Medical Center
|
|
|
- Shauna Ferguson
- 6 years ago
- Views:
Transcription

1 COPD 2018 GOLD 2017 Report Global Initiative for Chronic Obstructive Lung D isease COPYRIGHTED MATERIAL- DO NOT COPY OR DISTRIBUTE GLOBAL STRATEGY FOR THE DIAGNOSIS, MANAGEMENT, AND PREVENTION OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE 2017 REPORT Robert Schilz DO, PhD Pulmonary, Critical Care and Sleep Medicine University Hospitals Case Medical Center
2 Conflict of Interest Declaration None
3 CHALLENGE: Re-evaluate your COPD treatment paradigm, therapies and documentation
4 Areas of Active Change in COPD Management and Approach 4x more drugs than in 2000 New guidelines (GOLD, ATS) as of 2016, 2017 Focus on risk classification, phenotyping and comorbidities Change management paradigm to favor long acting bronchodilators (Steroid Controversies) Introduce clear guidelines for follow up and evaluation of stable patients and exacerbations Make first time recommendations for management of severe patients with nocturnal ventilation and lung volume reduction surgery
5 Summary of GOLD 2017 Updates Chapter 1 The definition of COPD has been revised to include the impact of respiratory symptoms and the role of lung tissue and airway abnormalities in the development of COPD. The origin of COPD development is discussed relative to interactions of host factors and environmental exposures. Chapter 2 The ABCD assessment tool has been refined to utilize respiratory symptoms and exacerbations alone to assign ABCD categories. The role of spirometry in overall management of COPD has been updated. Chapter 3 Assessment and regular evaluation of inhaler technique has been added to attempt to improve therapeutic outcomes. Increased evidence for self-management, pulmonary rehabilitation, integrated care and palliative care is presented. Recommendations for noninvasive ventilation, oxygen therapy and lung volume reduction are provided based on new information. Chapter 4 Examination of symptoms and future risk of exacerbations should provide the map for pharmacologic management of stable COPD. A shift towards more personalized approach to treatment is introduced, with strategies for escalation and de-escalation of pharmacotherapy. Chapter 5 Detailed hospital discharge and follow up criteria are presented and include integrated team care. Chapter 6 The strategies for the management of cardiovascular and other important comorbidities are presented in detail. The complex issues of multimorbidity and polypharmacy are outlined. From the Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) Available from:
 Reduce Symptoms Relieve symptoms")


6 2011+ Paradigm Shift in Global Recommendations for COPD Management 1) Reduce Symptoms Relieve symptoms FEV1 Based Management Strategy with Some Escalation Based on Symptom Control Improve exercise tolerance Improve health status 2) Reduce Risk Prevent disease progression Prevent and treat exacerbations Reduce mortality
7 Previous Treatment Paradigm: Therapy at Each Stage of COPD * I: Mild FEV 1 /FVC < 70% FEV 1 > 80% predicted II: Moderate FEV 1 /FVC < 70% 50% < FEV 1 < 80% predicted III: Severe FEV 1 /FVC < 70% 30% < FEV 1 < 50% predicted Active reduction of risk factor(s); influenza vaccination Add short-acting bronchodilator (when needed) IV: Very Severe FEV 1 /FVC < 70% FEV 1 < 30% predicted or FEV 1 < 50% predicted plus chronic respiratory failure Add regular treatment with one or more long-acting bronchodilators (when needed); Add rehabilitation Add inhaled glucocorticosteroids if repeated exacerbations *Postbronchodilator FEV 1 is recommended for the diagnosis and assessment of severity of COPD Add long term oxygen if chronic respiratory failure. Consider surgical treatments
8 Exacerbation Frequency and Severity Both Increase Mortality Risk Probability of surviving A P< B P=0.069 C P< Probability of surviving (1) NS (2) P=0.005 (3) NS (4) P< P< Time (months) Time (months) Group A Group B Group C patients with no acute exacerbations patients with 1 2 acute exacerbations requiring hospital management patients with 3 acute exacerbations Group (1) Group (2) Group (3) Group (4) no acute exacerbations acute exacerbations requiring emergency service visits without admission patients with acute exacerbations requiring one hospital admission patients with acute exacerbations requiring readmissions Soler-Cataluña JJ, et al. Thorax. 2005;60:
9 Combined Assessment of COPD Risk (GOLD Classification of Airflow Limitation) (C) (D) (A) (B) CAT < 10 CAT > 10 Symptoms 2 or > 1 leading to hospital admission 1 (not leading to hospital admission) 0 Risk (Exacerbation history) If GOLD 3 or 4 or 2 exacerbations per year or > 1 leading to hospital admission: High Risk (C or D) If GOLD 1 or 2 and only 0 or 1 exacerbations per year (not leading to hospital admission): Low Risk (A or B) mmrc 0 1 mmrc > 2 Breathlessness 2015 Global Initiative for Chronic Obstructive Lung Disease
10 Tools Involved in Risk Assessment in Current GOLD Treatment Paradigm Simple spirometry COPD Assessment Test (CAT) Modified Medical Research Council Dyspnea Scale (mmrc)
11 Global Strategy for Diagnosis, Management and Prevention of COPD Classification of Severity of Airflow Limitation in COPD* GOLD 1 Mild FEV 1 > 80% predicted GOLD 2 Moderate 50% < FEV 1 < 80% predicted GOLD 3 Severe 30% < FEV 1 < 50% predicted GOLD 4 Very Severe FEV 1 < 30% predicted *Based on Post-Bronchodilator FEV Global Initiative for Chronic Obstructive Lung Disease

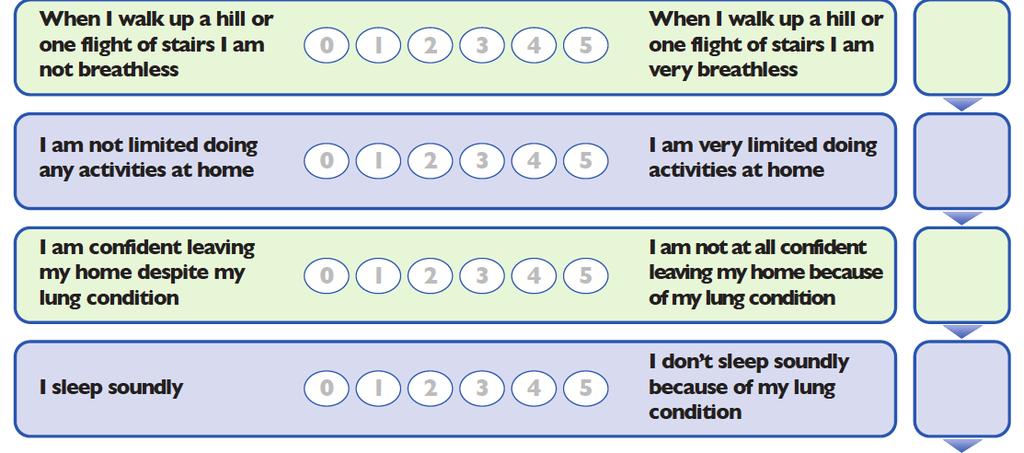
12 COPD Assessment Test (CAT)
13 Modified Medical Research Council Dyspnea Scale (mmrc) Grade 0: breathless with strenuous exercise Grade I: short of breath when hurrying on the level or walking up a slight hill Grade II: walking slower than people of the same age on the level because of breathlessness or having to stop for breath when walking at own pace on the level Grade III: stopping for breath after walking about 100 yards or after a few minutes on the level Grade IV: too breathless to leave the house or breathless when dressing or undressing
14 Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD When assessing risk, choose the highest risk according to GOLD grade or exacerbation history. One or more hospitalizations for COPD exacerbations should be considered high risk.) Patient Characteristic Spirometric Classification Exacerbations per year CAT mmrc A B C Low Risk Less Symptoms Low Risk More Symptoms High Risk Less Symptoms GOLD < GOLD > 10 > 2 GOLD 3-4 > 2 < D High Risk More Symptoms GOLD 3-4 > 2 > 10 > Global Initiative for Chronic Obstructive Lung Disease

15 BODE Index for COPD Survival
 Index Celli, B. et al.")
16 Variables and Point Values Used for the Computation of the Body-Mass Index, Degree of Airflow Obstruction and Dyspnea, and Exercise Capacity (BODE) Index Celli, B. et al. N Engl J Med 2004;350:
17 Kaplan-Meier Survival Curves for the Four Quartiles of the Body-Mass Index, Degree of Kaplan-Meier Airflow Obstruction Survival and Curves Dyspnea, for the and Four Exercise Quartiles Capacity of the Body-Mass Index (Panel Index, A) and Degree the Three of Airflow Stages Obstruction of Severity and of Chronic Dyspnea, Obstructive and Exercise Pulmonary Capacity Disease Index (Panel as Defined A) and by the the Three Stages of Severity American of Chronic Thoracic Obstructive Society Pulmonary (Panel B) Disease as Defined by the American Thoracic Society (Panel B) Celli, B. et al. N Engl J Med 2004;350:
18 An Example of Updated Office Documentation for COPD 1) COPD FEV1 = 40% predicted, GOLD Spirometry Class 3, CAT Score = 8, Type C, BODE 5 ( ).
19 COPD Treatment
20 Number of Drugs FDA Approved for COPD by Year Cumulative # of FDA Drugs Atrovent Combivent Advair Foradil,, Duoneb Spiriva Brovana Symbicort
21 Current FDA Approved COPD Combination Agents Short-acting anticholinergics + short acting beta agonists (SABA/SAMA) Ipratropium bromide + albuterol (Combivent, Duoneb) Long-acting beta agonists + Long-acting anti-muscarinics (LABA/LAMA) Umeclidinium + Villaterol (Anoro Elipta) Indacaterol + Glycopyrrolate (Utibron Neohaler) Olodaterol + Tiotropium Bromide (Stiolto Respimat ) Formoterol + Glycopyrrolate (Bevespi Aerosphere ) Long-acting beta agonists + Long acting Inhaled corticosteroids (LABA/ICS) Salmeterol + Fluticasone (Advair ) Formoterol + Budesonide (Symbicort ) Fluticasone furoate + vilanterol (Breo Ellipta ) Long-acting beta agonists + Long-acting anti-muscarinics + Long-acting inhaled corticosteroids (LABA/LAMA/ICS) Vilanterol + Umeclidinium + Fluticasone furoate (Trelegy Elipta )
22 Roflumilast (Daliresp) Phosphodiesterase E4 inhibitor Approval: 2011 Indicated as a treatment to reduce the risk of COPD exacerbations in patients with severe COPD associated with chronic bronchitis and a history of exacerbations. Dose 500 ug once daily
23 Q: Does the recent proliferation of new therapeutic agents for really change our treatment of COPD? A: Probably Q: Should I think about COPD Patients Differently? A: Almost Certainly


24 Summary 2017 GOLD Pharmacologic Therapy C D A Continue, stop or try alternative class of bronchodilator B Evaluate Effect A bronchodilator
25 Global Strategy for Diagnosis, Management and Prevention of COPD Manage Stable COPD: Non-pharmacologic Patient Group Essential Recommended Depending on local guidelines A Smoking cessation (can include pharmacologic treatment) Physical activity Flu vaccination Pneumococcal vaccination B, C, D Smoking cessation (can include pharmacologic treatment) Pulmonary rehabilitation Physical activity Flu vaccination Pneumococcal vaccination 2014 Global Initiative for Chronic Obstructive Lung Disease

26 2017 GOLD Group A Pharmacologic Therapy Continue, stop or try alternative class of bronchodilator Evaluate Effect A bronchodilator
27 Short Acting Bronchodilators DRUG TRADE NAME Mechanism of Action DOSING INTERVAL MISC Albuterol Proventil Proair Short Acting Beta 2 Agonist (SABA) Q 4-6 hours Also available as nebulized agent Pirbuterol Maxair Short Acting Beta 2 Agonist (SABA) Q 4-6 hours Ipratropium Bromide Atrovent Short Acting Antimuscarinic (SAMA) Q 4-6 hours Also available as nebulized agent Albuterol + Ipratropium Bromide Combivent SABA + SAMA Q 6 hours Also available as nebulized agent
28 Group B COPD Patients Patients have more significant symptoms but still a low risk of exacerbations Long-acting bronchodilators are recommended as first choice Choice is dependent on individual patient s perception of symptom relief In patients with severe breathlessness, a combination of long-acting bronchodilators is recommended as second choice Alternative choices include short-acting bronchodilators and theophylline B Long-acting anticholinergic or Long-acting beta 2 -agonist Long-acting anticholinergic and long-acting beta 2 -agonist Short-acting beta 2 -agonist and/or Short-acting anticholinergic Theophylline From the Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease, Global Initiative for Chronic Obstructive Lung Disease (GOLD) Available from: Global Initiative for Chronic Obstructive Lung Disease, all rights reserved.
29 2017 GOLD Group B Pharmacologic Therapy LAMA + LABA Persistent Symptoms A long-acting bronchodilator (LAMA or LABA)




30 Long Acting Antimuscarinics (LAMA)
31 Long Acting Anti-muscarinics (LAMA) DRUG TRADE NAME INDICATION DOSING INTERVAL MISC Tiotropium Bromide Spiriva Bronchodilation qd Decreased exacerbations Umeclidinium Incruse Ellipta Bronchodilation qd Decreased exacerbations Aclidinium Tudorza Pressair Bronchodilation BID Decreased exacerbations Glycopyrrolate Seebri Neohaler Broncho- Dilation BID Maintained bronchodilation




32 Long Acting Beta- Agonist (LABA)
33 Long Acting Beta- Agonist (LABA) DRUG TRADE NAME INDICATION Formoterol Foradil Performist Bronchodilation DOSING INTERVAL BID MISC Decreased exacerbations, nebulized Olodaterol Incruse Ellipta Bronchodilation qd Decreased exacerbations Indacaterol Arcapta Bronchodilation qd Salmeterol Serevent Bronchodilation BID Aformoterol Brovana Bronchodilation BID Neubulized only Villaterol qd Only in combination


34 Combination LABA/LAMA
35 Combination LABA/LAMA DRUG TRADE NAME INDICATION DOSING INTERVAL MISC Indacaterol + Glycopyrronium Olodaterol + Tiotropium Bromide Formoterol + Glycopyrrolate Villaterol + Umeclidinium Ultibro Breezehaler Stiolto Respimat Bevespi Aerosphere Anoro Ellipta Maintenance qd Bronchodilation Maintenance qd Bronchodilation Maintenance BID Bronchodilation Maintenance qd Bronchodilation
36 From the Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease, Global Initiative for Chronic Obstructive Lung Disease (GOLD) Available from: Global Initiative for Chronic Obstructive Lung Disease, all rights reserved. Group C COPD Patients Long-acting anticholinergic and long-acting beta 2 - agonist C Inhaled corticosteroid + long-acting beta 2 - agonist or Long-acting anticholinergic or Long-acting anticholinergic and phosphodiesterase 4 inhibitor or Long-acting beta2- agonist and phosphodiesterase inhibitor Short-acting beta 2 - agonist and/or Short-acting anticholinergic Theophylline
37 2017 GOLD Group C Pharmacologic Therapy LAMA + LABA LABA + ICS Persistent Symptoms LAMA


38 Combination LABA/ICS
39 Long Acting Combination LABA + Inhaled Corticosteroids (ICS) DRUG TRADE NAME INDICATION Fluticasone Propionate + Salmeterol Budesonide + Formoterol Fluticasone furoate + vilanterol Advair Symbicort Breo Ellipta Maintenance + Decrease Exacerbations Maintenance + Decrease Exacerbations Maintenance + Decrease Exacerbations DOSING INTERVAL 1 puff BID 2 puffs BID 1 puff qd
40 Long Acting Combination LABA + LAMA + Inhaled Corticosteroids (ICS) DRUG TRADE NAME INDICATION Fluticasone Propionate + Salmeterol Budesonide + Formoterol Fluticasone furoate + vilanterol Fluticasone furoate + vilanterol + Umclidinium Advair Symbicort Breo Ellipta Trelegy Ellipta Maintenance + Decrease Exacerbations Maintenance + Decrease Exacerbations Maintenance + Decrease Exacerbations Reducing exacerbations + improving lung function + health related quality of life DOSING INTERVAL 1 puff BID 2 puffs BID 1 puff qd 1 puff qd
41 Inhaled Steroids in COPD Pros Exacerbation reduction when added to LABA in placebocontrolled trials Improvement in FEV 1 in combination with beta-agonists Burge PS, et al. BMJ. 2000;320(7245): Calverley PM, et al. NEJM. 2007;356: Festic E, et al. AJRCCM. 2015;191: Kaplan AG. Int J COPD. 2015;10: Suissa S, et al. EurResp J. 2015;46: Cons Clinical trial evidence No reduction in COPD progression No mortality reduction Side effect profile Risk of pneumonia Risk of osteoporosis, adrenal suppression Oral Thrush
42 Increased risk of pneumonia with ICS use in patients with COPD: metaanalysis Significantly increased risk of serious pneumonia for ICS vs placebo: risk ratio 1.51 (95%CI ) 285 events/3,881 patients vs 180 events/3,633 patients ICS + LABA vs LABA: risk ratio 1.72 (95%CI ) 356 events/4,754 patients vs 217 events/4,728 patients Total: ICS vs no ICS: risk ratio 1.60 (95%CI ) 641 events/8,635 patients vs 397 events/8,361 patients OR 1.56, 95% CI 1.30 to 1.86, 6235 participants* CI, confidence interval; COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroid; LABA, long-acting β 2 -agonist. Singh S, et al. Arch Intern Med 2009;169: Yang IA, Clarke MS, Sim EH, Fong KM. Inhaled corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2012; 7(7): CD
43 Inhaled corticosteroids do not improve symptoms of breathlessness Mean breathlessness symptom score after 52 weeks Fluticasone propionate p=ns Placebo ns = not significant Calverley PMA et al. Lancet 2003;361:449 56
44 Group D COPD Patients D Inhaled corticosteroid + long-acting beta 2 -agonist and/or Long-acting anticholinergic Inhaled corticosteroid plus long-acting anticholinergic and longacting beta 2 -agonist or Inhaled corticosteroid plus long-acting beta 2 agonist and phosphodiesterase 4 inhibitor or Long-acting beta 2 agonist and long-acting anticholinergic or Long-acting anticholinergic and phosphodiesterase 4 inhibitor Carbocysteine Short-acting beta 2 - agonist and/or Short-acting anticholinergic Theophylline
 Further exacerbations Persistent symptoms and/or further exacerbations LAMA + LABA +ICS LAMA LAMA + LABA LABA +")
45 2017 GOLD Group D Pharmacologic Therapy Consider roflumilast if FEV 1 < 50% and patient has chronic bronchitis Consider macrolide (in former smokers) Further exacerbations Persistent symptoms and/or further exacerbations LAMA + LABA +ICS LAMA LAMA + LABA LABA + ICS
46 Roflumilast (Daliresp) Phosphodiesterase E4 inhibitor Approval: 2011 Indicated as a treatment to reduce the risk of COPD exacerbations in patients with severe COPD associated with chronic bronchitis and a history of exacerbations. Dose 500 ug once daily
47 Recommendations for Use of Roflumilast in Primary Care Clear identification of patients eligible for roflumilast Phenotyping of patients in primary care lung function measurement (FEV1<50%) accurate health status classification At least 1 exacerbation last year Smoking > 20 pk/years recording of chronic cough and regular sputum production Price, D et al. Prim Care Respir J Mar;20(1):45.
48 Additional Concerns with Roflumilast Roflumilast and suicidal thoughts or depression 20% of patients in trial had 5-10% weight loss GI Side effects
49 A Word About Co-morbidities Cardiovascular disease Systolic or Diastolic HF 20%-70%* PVD 8.8%** Osteoporosis Lung Cancer (Screening) Anxiety and Depression Metabolic Syndrome GERD *Bhatt SP, Dransfield MT. Transl Res 2013; 162(4): **Houben-Wilke S, Jorres RA, Bals R, et al. Am J Respir Crit Care Med 2016; EPub 17 Aug 2016
50 Multifactorial Approach to the COPD Patient Kevin Gruffydd-Jones Primary Care Respiratory Journal (2012) 21,
51 An Example of Updated Office Documentation for COPD 1) COPD FEV1 = 40% predicted, GOLD Spirometry Class 3, CAT Score = 8, Type C, BODE 5 ( ). a) Currently on LABA and LAMA. b) Completed pulmonary rehab (Or needs) c) Not LVRS candidate. (If FEV %) d) Currently with adequate oxygenation at rest, sleep and ambulation. (Or needs testing) e) Assessed cardiac, malignancy risks (Needs )
52 Miscellaneous Topics in Management
53 Non-Pharmacologic Treatments for COPD Smoking Cessation Pulmonary Rehabilitation Oxygen Therapy Ventilatory Support Lung Volume Reduction Surgery Lung Transplantation Vaccination From: Global Strategy for Diagnosis, Management and Prevention of COPD. GOLD Slideset 2015
54 USPSTF Low Dose Lung Cancer Screening Recommendation Annual screening until: a person has not smoked for 15 years or develops a health problem that substantially limits life expectancy or the ability or willingness to have curative lung surgery Aged 55 to 80 years 30 pack-year smoking history Currently smoke or have quit within the past 15 years.

55 Exacerbation Care Exacerbation Acute Care Acute steroids < 30 days Acute Pulmonary Rehab <4 weeks Discuss treatment regimen Assess oxygen needs 1-4 Week Follow Up Evaluate ability to cope and perform ADLs Review Treatment Plan Reassess inhaler techniques Reassess Oxygen needs Reassess Comorbidity Sttus Week Follow Up All 1-4 Week Perform FEV 1 Chronic Care A,B,C,D Risk Stratification and Treatment Assess CAT, mmrc All 1-4 week assessments
56 Summary
57 Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD When assessing risk, choose the highest risk according to GOLD grade or exacerbation history. One or more hospitalizations for COPD exacerbations should be considered high risk.) Patient Characteristic Spirometric Classification Exacerbations per year CAT mmrc A B C Low Risk Less Symptoms Low Risk More Symptoms High Risk Less Symptoms GOLD < GOLD > 10 > 2 GOLD 3-4 > 2 < D High Risk More Symptoms GOLD 3-4 > 2 > 10 > Global Initiative for Chronic Obstructive Lung Disease
58 Multifactorial Approach to the COPD Patient Kevin Gruffydd-Jones Primary Care Respiratory Journal (2012) 21,

59 Global Strategy for Diagnosis, Management and Prevention of COPD Manage Stable COPD: Goals of Therapy Relieve symptoms Improve exercise tolerance Improve health status Prevent disease progression Prevent and treat exacerbations Reduce mortality Reduce symptoms Reduce risk 2015 Global Initiative for Chronic Obstructive Lung Disease
60 Global Strategy for Diagnosis, Management and Prevention of COPD Manage Stable COPD: Key Points Identification and reduction of exposure to risk factors are important steps in prevention and treatment. Individualized assessment of symptoms, airflow limitation, and future risk of exacerbations should be incorporated into the management strategy. All COPD patients benefit from rehabilitation and maintenance of physical activity. Pharmacologic therapy is used to reduce symptoms, reduce frequency and severity of exacerbations, and improve health status and exercise tolerance Global Initiative for Chronic Obstructive Lung Disease
61 Global Strategy for Diagnosis, Management and Prevention of COPD Manage Stable COPD: Key Points Long-acting formulations of beta 2 -agonists and anticholinergics are preferred over short-acting formulations. Based on efficacy and side effects, inhaled bronchodilators are preferred over oral bronchodilators. Long-term treatment with inhaled corticosteroids added to long-acting bronchodilators is recommended for patients with high risk of exacerbations Global Initiative for Chronic Obstructive Lung Disease
62 Global Strategy for Diagnosis, Management and Prevention of COPD Manage Stable COPD: Key Points Long-term monotherapy with oral or inhaled corticosteroids is not recommended in COPD. The phospodiesterase-4 inhibitor roflumilast may be useful to reduce exacerbations for patients with FEV 1 < 50% of predicted, chronic bronchitis, and frequent exacerbations Global Initiative for Chronic Obstructive Lung Disease
63 Q: Does the recent proliferation of new therapeutic agents for really change our treatment of COPD? A: Quite Possibly Q: Should I think about COPD Patients Differently? A: Almost Certainly
64 Appendix and Supplementary Slides
65 Benefits of Pulmonary Rehab In Patients with COPD Improve exercise capacity Enhance quality of life (QOL) Decrease exacerbations within 30 days of discharge Impact on Hospitalization and Mortality* *Inconsistently shown
66 Mortality Benefits of Pulmonary Rehabilitation (N=246) Endpoint (-) Rehab (+) Rehab Hospitial LOS for Respiratory Related Illness 25% 20% Mortality for Respiratory Related Illness 39% 7% BODE Score 4% (worsened) 19% (improved Cote CG, Celli BR Pulmonary rehabilitation and the BODE index in COPD. Eur Respir J. 2005;26(4):630
67 Surgical Options for Advanced COPD Lung Volume Reduction Surgery Lung Transplantation
68 Lung Volume Reduction Surgery Only for Select Emphysema Patients Selection Criteria 45% < FEV1 < 25% TLC >100% RV > 150% Post Rehab Exercise Capacity 6MW > 140m CPET with < 40 watts(men), <25 watts(women)


69 LVRS Results FEV1 = 1.60 L (37%) FEV1 = 2.23 L (52%)
70 LVRS Results Pulmonary Testing Pre-LVRS Post-LVRS FEV 1 (L/min 1.60 (37%) 2.23 (52%) FVC (L) 4.29 (76%) 4.70 (84%) TLC (L) 9.21 (113%) 7.73 (94%) RV(L) 4.77 (186%) 2.97 (116%)
71 Lung Volume Reduction Surgery Exclusions BMI, > 31.1 kg/m 2 (men) or > 32.3 kg/m 2 (women) PCO 2, > 60 mm Hg PO 2, < 45 mm Hg on room air Active Smoking or quit < 4 months Alpha 1 Antitrypsin Disease Non-Apical Distribution of Emphysema
72 Kaplan Meier Estimates of the Probability of Death as a Function of the Number of Months after Randomization (Upper Lobe Disease with Low Exercise Capacity After Rehabilitation N=290) National Emphysema Treatment Trial Research Group, N Engl J Med 2003;348: National Emphysema Treatment Trial Research Group, N Engl J Med 2003;348:
73 Global Strategy for Diagnosis, Management and Prevention of COPD Asthma COPD Overlap Syndrome Characterized by some element of fixed obstruction and multiple features of both COPD and asthma. Suggested to be relatively common Q:Why should we care? May represent a distinct clinical entity / prognosis. May open the door to earlier and more prominent use of inhaled steroids in ACOS or modulation of allergic type pathways. May need to be eliminated from therapeutic trials in COPD. Especially those impacting inflammatory pathways. Recognition may shed light on frequent exacerbators and triggers.

74 Risk Factors for Asthma and COPD and the Influence of Environment and Aging. Postma DS, Rabe KF. N Engl J Med 2015;373:
 q Symptoms vary overminutes, hours or days q Worse during night or early morning qtriggered by")




75 Features that (when present) favor asthma or COPD Feature Favors asthma Favors COPD Age of onset qbefore age 20 years qafter age 40 years Pattern of respiratory symptoms Lung function Past history or family history Time course GINA 2014, Box 5-2B (3/3) q Symptoms vary overminutes, hours or days q Worse during night or early morning qtriggered by exercise, emotions including laughter, dust, or exposure to allergens qno worseningof symptoms over time. Symptoms vary seasonally, or from year to year qmay improve spontaneously, or respond immediately to BD or to ICS over weeks q Symptoms persist despite treatment qgood and bad days, but always daily symptoms and exertional dyspnea qchronic cough and sputum preceded onset of dyspnea, unrelated to triggers Syndromic diagnosis of airways disease The shaded columns list features that, when present, best distinguish between qrecord of variable airflow limitation asthma and COPD. (spirometry, peak flow) For a patient, qnormal count between the number symptoms of check boxes in each column. If 3 or qmore Previous boxes doctor are diagnosis checked of for asthma either asthma or COPD, that diagnosis is suggested. qfamily history of asthma, and other allergic If there conditions are similar (allergic numbers rhinitis of or checked eczema) boxes in each column, the diagnosis of ACOS should be considered. qrecord of persistent airflow limitation (post-bd FEV 1 /FVC <0.7) q Abnormal between symptoms qprevious doctor diagnosis of COPD, chronic bronchitis or emphysema qheavy exposure to a risk factor: tobacco smoke, biomass fuels qsymptomsslowly worsening over time (progressive course over years) qrapid-acting bronchodilator treatment provides only limited relief Chest X-ray q Normal q Severe hyperinflation Global Initiative for Asthma
76 Global Strategy for Diagnosis, Management and Prevention of COPD Manage Stable COPD: Pharmacologic Therapy OTHER POSSIBLE TREATMENTS C D GOLD 4 GOLD 3 GOLD 2 GOLD 1 A SABA and/or SAMA Theophylline Theophylline Carbocysteine N-acetylcysteine SABA and/or SAMA Theophylline B SABA and/or SAMA Theophylline 2 or more or > 1 leading to hospital admission 1 (not leading to hospital admission) 0 Exacerbations per year CAT < 10 mmrc 0-1 CAT > 10 mmrc > Global Initiative for Chronic Obstructive Lung Disease
Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management. Colleen Sakon, PharmD BCPS September 27, 2018
 Management. Colleen Sakon, PharmD BCPS September 27, 2018") Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management Colleen Sakon, PharmD BCPS September 27, 2018 Disclosures I have no actual or potential conflicts of interest 2 Objectives Summarize
Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management Colleen Sakon, PharmD BCPS September 27, 2018 Disclosures I have no actual or potential conflicts of interest 2 Objectives Summarize
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
COPD Update. Plus New and Improved Products for Inhaled Therapy. Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor
 COPD Update Plus New and Improved Products for Inhaled Therapy Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose concerning possible financial
COPD Update Plus New and Improved Products for Inhaled Therapy Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose concerning possible financial
COPD: Treatment Update Property of Presenter. Not for Reproduction. Barry Make, MD Professor of Medicine National Jewish Health
 COPD: Treatment Update Barry Make, MD Professor of Medicine National Jewish Health Disclosures Advisory board, consultant, multi-center trial, research funding, Data Safety Monitoring Board (DSMB), or
COPD: Treatment Update Barry Make, MD Professor of Medicine National Jewish Health Disclosures Advisory board, consultant, multi-center trial, research funding, Data Safety Monitoring Board (DSMB), or
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Three s Company - The role of triple therapy in chronic obstructive pulmonary
 Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) October 26 th, 2018 Zahava Picado, PharmD PGY1 Pharmacy Resident Central Texas Veterans Healthcare System Zahava.Picado@va.gov
Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) October 26 th, 2018 Zahava Picado, PharmD PGY1 Pharmacy Resident Central Texas Veterans Healthcare System Zahava.Picado@va.gov
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
STRIVERDI RESPIMAT (olodaterol hcl) aerosol
 aerosol") STRIVERDI RESPIMAT (olodaterol hcl) aerosol Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
STRIVERDI RESPIMAT (olodaterol hcl) aerosol Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
Pharmacotherapy for COPD
 10/3/2017 Topics to be covered Pharmacotherapy for chronic treatment Pharmacotherapy for COPD Dr. W C Yu 3rd September 2017 Commonly used drugs Guidelines for their use Inhaled corticosteroids (ICS) in
10/3/2017 Topics to be covered Pharmacotherapy for chronic treatment Pharmacotherapy for COPD Dr. W C Yu 3rd September 2017 Commonly used drugs Guidelines for their use Inhaled corticosteroids (ICS) in
4 "Practice Changers" in Pulmonary Medicine for 2016
 4 "Practice Changers" in Pulmonary Medicine for 2016 Robert Schilz DO, PhD Pulmonary, Critical Care and Sleep Medicine University Hospitals Case Medical Center Faculty Disclosures Grant Support: - Roche
4 "Practice Changers" in Pulmonary Medicine for 2016 Robert Schilz DO, PhD Pulmonary, Critical Care and Sleep Medicine University Hospitals Case Medical Center Faculty Disclosures Grant Support: - Roche
If you require this document in another format such as Braille, large print, audio or another language please contact the Trusts Communications Team
 MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
Changing Landscapes in COPD New Zealand Respiratory Conference
 Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
Wirral COPD Prescribing Guidelines
 Wirral COPD Prescribing Guidelines (To be read in conjunction with the Wirral COPD Supplementary Information) STEP 1: Assess symptoms COPD Assessment Test (CAT) [Link for CAT-test Online] is a patient-completed
Wirral COPD Prescribing Guidelines (To be read in conjunction with the Wirral COPD Supplementary Information) STEP 1: Assess symptoms COPD Assessment Test (CAT) [Link for CAT-test Online] is a patient-completed
2017 GOLD Report. Is it worth its weight in GOLD??? CSHP-NB Fall Education Day September 30, 2017
 2017 GOLD Report Is it worth its weight in GOLD??? CSHP-NB Fall Education Day September 30, 2017 Lauren Munro; BSc(Pharm) Amanda Burns; BSc(Pharm) Pharmacy Residents The Moncton Hospital Objectives Explain
2017 GOLD Report Is it worth its weight in GOLD??? CSHP-NB Fall Education Day September 30, 2017 Lauren Munro; BSc(Pharm) Amanda Burns; BSc(Pharm) Pharmacy Residents The Moncton Hospital Objectives Explain
Clinical Policy: Roflumilast (Daliresp) Reference Number: CP.PMN.46 Effective Date: Last Review Date: 08.18
 Reference Number: CP.PMN.46 Effective Date: Last Review Date: 08.18") Clinical Policy: (Daliresp) Reference Number: CP.PMN.46 Effective Date: 11.01.11 Last Review Date: 08.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Daliresp) Reference Number: CP.PMN.46 Effective Date: 11.01.11 Last Review Date: 08.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Turning Science into Real Life Roflumilast in Clinical Practice. Roland Buhl Pulmonary Department Mainz University Hospital
 Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
COPD: Preventable and Treatable. Lecture Outline. Diagnosis of COPD. COPD: Defining Terms
 COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
TRELEGY ELLIPTA (fluticasone-umeclidinium-vilanterol) aerosol powder
 aerosol powder") TRELEGY ELLIPTA (fluticasone-umeclidinium-vilanterol) aerosol powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
TRELEGY ELLIPTA (fluticasone-umeclidinium-vilanterol) aerosol powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy f the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy f the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Defining COPD. Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist
 Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Test Your Inhaler Knowledge
 A Breath of Fresh Air: Updates in COPD Management Jennifer Austin Szwak, PharmD, BCPS, DPLA University of Chicago Medicine The speaker has nothing to disclose Abbreviations COPD: Chronic obstructive pulmonary
A Breath of Fresh Air: Updates in COPD Management Jennifer Austin Szwak, PharmD, BCPS, DPLA University of Chicago Medicine The speaker has nothing to disclose Abbreviations COPD: Chronic obstructive pulmonary
THE COPD PRESCRIBING TOOL
 THE COPD PRESCRIBING TOOL Revised edition, 2017 www.bpac.org.nz/copd CLASSIFICATION The COPD prescribing tool This tool provides pharmacological treatment options for patients with COPD based on their
THE COPD PRESCRIBING TOOL Revised edition, 2017 www.bpac.org.nz/copd CLASSIFICATION The COPD prescribing tool This tool provides pharmacological treatment options for patients with COPD based on their
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university
 What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
Asthma COPD Update 2018
 Asthma COPD Update 2018 Roger Hefflinger, Pharm.D. Clinical Associate Professor ISU COP Clinical Teaching Pharmacist Family Medicine Residency of Idaho In support of improving patient care, Idaho State
Asthma COPD Update 2018 Roger Hefflinger, Pharm.D. Clinical Associate Professor ISU COP Clinical Teaching Pharmacist Family Medicine Residency of Idaho In support of improving patient care, Idaho State
Balanced information for better care. Helping patients with COPD breathe easier
 Balanced information for better care Helping patients with COPD breathe easier COPD is the third-leading cause of death in the U.S., following cancer and heart disease 1 FIGURE 1. Women now have a higher
Balanced information for better care Helping patients with COPD breathe easier COPD is the third-leading cause of death in the U.S., following cancer and heart disease 1 FIGURE 1. Women now have a higher
Treatment Responses. Ronald Dahl, Aarhus University Hospital, Denmark
 Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
COPD GOLD Guidelines & Barnet inhaler choices. Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust
 COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 CHRONIC OBSTRUCTIVE PULMONARY DISEASE INCIDENCE UP TO 380,000 PEOPLE IN IRELAND HSE FIGURES 110,000 DIAGNOSED AND 200,000 UNDIAGNOSED. AFFECTS MORE MEN THAN WOMEN BUT RATES ARE RISING 1500 DEATHS PER YEAR
CHRONIC OBSTRUCTIVE PULMONARY DISEASE INCIDENCE UP TO 380,000 PEOPLE IN IRELAND HSE FIGURES 110,000 DIAGNOSED AND 200,000 UNDIAGNOSED. AFFECTS MORE MEN THAN WOMEN BUT RATES ARE RISING 1500 DEATHS PER YEAR
Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD)
") Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) Zahava Picado, PharmD PGY1 Pharmacy Practice Resident Central Texas Veterans Healthcare System Temple, TX October
Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) Zahava Picado, PharmD PGY1 Pharmacy Practice Resident Central Texas Veterans Healthcare System Temple, TX October
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Improving Outcomes in COPD
 Neil MacIntyre MD Duke University Durham NC Current treatment guidelines f COPD focus Barriers to providing optimal treatment Diagnosis of COPD EXPOSURE TO RISK FACTORS AND/ OR SYMPTOMS sputum cough dyspnea
Neil MacIntyre MD Duke University Durham NC Current treatment guidelines f COPD focus Barriers to providing optimal treatment Diagnosis of COPD EXPOSURE TO RISK FACTORS AND/ OR SYMPTOMS sputum cough dyspnea
COPD: GOLD guidelines Ijlal Babar, MD Medical Director Pulmonary CCM, Pulmonary Hypertension Center SRHS
 COPD: GOLD guidelines 2017 Ijlal Babar, MD Medical Director Pulmonary CCM, Pulmonary Hypertension Center SRHS Introduction The Global Initiative for Chronic Obstructive Lung Disease (GOLD) program was
COPD: GOLD guidelines 2017 Ijlal Babar, MD Medical Director Pulmonary CCM, Pulmonary Hypertension Center SRHS Introduction The Global Initiative for Chronic Obstructive Lung Disease (GOLD) program was
A Visual Approach to Simplifying Respiratory Drug Regimens
 A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP 3 Main Categories Inhaled Respiratory Drugs Binds to beta-2 receptors Relaxation of smooth muscles in the lung
A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP 3 Main Categories Inhaled Respiratory Drugs Binds to beta-2 receptors Relaxation of smooth muscles in the lung
Choosing an inhaler for COPD made simple. Dr Simon Hart Castle Hill Hospital
 Choosing an inhaler for COPD made simple Dr Simon Hart Castle Hill Hospital 1 Declaration of interests I have received speaker fees, sponsorship to attend conferences, and funding for research from companies
Choosing an inhaler for COPD made simple Dr Simon Hart Castle Hill Hospital 1 Declaration of interests I have received speaker fees, sponsorship to attend conferences, and funding for research from companies
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015
 David CL Lam Department of Medicine University of Hong Kong October, 2015") Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide
 VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
Management of COPD Updates and Evidence
 Management of COPD Updates and Evidence Providence Alaska Medical Center PGY1 Pharmacy Practice Residents Ann-Chee Cheng, PharmD Kaite Kammers, PharmD http://www.fpnotebook.com/_media/lungxsgraybb962.gif
Management of COPD Updates and Evidence Providence Alaska Medical Center PGY1 Pharmacy Practice Residents Ann-Chee Cheng, PharmD Kaite Kammers, PharmD http://www.fpnotebook.com/_media/lungxsgraybb962.gif
What is this patient s diagnosis?
 Asthma and COPD KANTA VELAMURI, MD ASSOCIATE PROFESSOR OF MEDICINE PULMONARY, CRITICAL CARE AND SLEEP MEDICINE SECTION MICHAEL E. DEBAKEY VA MEDICAL CENTER BAYLOR COLLEGE OF MEDICINE Disclosures None Case
Asthma and COPD KANTA VELAMURI, MD ASSOCIATE PROFESSOR OF MEDICINE PULMONARY, CRITICAL CARE AND SLEEP MEDICINE SECTION MICHAEL E. DEBAKEY VA MEDICAL CENTER BAYLOR COLLEGE OF MEDICINE Disclosures None Case
Curriculum Vitae. Head of Public Wing HCU - RSCM. Head of ICU Sari Asih Ciledug Hospital
 Curriculum Vitae Name : Dr. Ceva W. Pitoyo,SpPD,K-P,KIC,FINASIM POB / DOB : Jakarta, March 8th 1968 Education : o General Practitioner : FKUI 1993 o Internist : FKUI 2002 o Pulmonology Consultant : PAPDI-UI
Curriculum Vitae Name : Dr. Ceva W. Pitoyo,SpPD,K-P,KIC,FINASIM POB / DOB : Jakarta, March 8th 1968 Education : o General Practitioner : FKUI 1993 o Internist : FKUI 2002 o Pulmonology Consultant : PAPDI-UI
Potential risks of ICS use
 Potential risks of ICS use Randomised controlled trial Observational study Systematic review Pneumonia Tuberculosis Bone fracture Skin thinning/easy bruising Cataract Diabetes No effect on fracture risk
Potential risks of ICS use Randomised controlled trial Observational study Systematic review Pneumonia Tuberculosis Bone fracture Skin thinning/easy bruising Cataract Diabetes No effect on fracture risk
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines
 Treatment Guidelines") Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
Surveillance report Published: 6 April 2016 nice.org.uk. NICE All rights reserved.
 Surveillance report 2016 Chronic obstructive pulmonary disease in over 16s: diagnosis and management (2010) NICE guideline CG101 Surveillance report Published: 6 April 2016 nice.org.uk NICE 2016. All rights
Surveillance report 2016 Chronic obstructive pulmonary disease in over 16s: diagnosis and management (2010) NICE guideline CG101 Surveillance report Published: 6 April 2016 nice.org.uk NICE 2016. All rights
Provider Respiratory Inservice
 Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
COPD The New Epidemic. Peter Lin MD CCFP Director Primary Care Initiatives Canadian Heart Research Centre
 COPD The New Epidemic Peter Lin MD CCFP Director Primary Care Initiatives Canadian Heart Research Centre Conflict Disclosure Information Speaker: Dr. Peter Lin Title of Talk: COPD The New Epidemic Financial
COPD The New Epidemic Peter Lin MD CCFP Director Primary Care Initiatives Canadian Heart Research Centre Conflict Disclosure Information Speaker: Dr. Peter Lin Title of Talk: COPD The New Epidemic Financial
TORCH: Salmeterol and Fluticasone Propionate and Survival in COPD
 TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
Chronic Obstructive Pulmonary Disease
 Quality Department Guidelines for Clinical Care Ambulatory COPD Guideline Team Team Leader Davoren A Chick, MD General Medicine Team Members Paul J Grant, MD General Medicine R Van Harrison, PhD Learning
Quality Department Guidelines for Clinical Care Ambulatory COPD Guideline Team Team Leader Davoren A Chick, MD General Medicine Team Members Paul J Grant, MD General Medicine R Van Harrison, PhD Learning
Algorithm for the use of inhaled therapies in COPD Version 2 May 2017
 Algorithm for the use of inhaled therapies in COPD This document has been revised by the Berkshire West Respiratory Network to support clinicians in selecting the most appropriate, cost effective treatments
Algorithm for the use of inhaled therapies in COPD This document has been revised by the Berkshire West Respiratory Network to support clinicians in selecting the most appropriate, cost effective treatments
Asthma/COPD Update with Inhaler Workshop
 Asthma/COPD Update with Inhaler Workshop October 8, 2017 Nathan Samsa, DO, Pharm D, RPh, FACOI None Disclosures Agenda Asthma Updates COPD Updates Inhaler Workshop Asthma Updates Asthma Updates SMART Trial
Asthma/COPD Update with Inhaler Workshop October 8, 2017 Nathan Samsa, DO, Pharm D, RPh, FACOI None Disclosures Agenda Asthma Updates COPD Updates Inhaler Workshop Asthma Updates Asthma Updates SMART Trial
CHARM Guidelines for the diagnosis and
 \ CHARM Guidelines for the diagnosis and management of COPD City and Hackney CCG Homerton University Hospital NHS Foundation Trust Written by: Miss Hetal Dhruve, Specialist Pharmacist Respiratory Medicine,
\ CHARM Guidelines for the diagnosis and management of COPD City and Hackney CCG Homerton University Hospital NHS Foundation Trust Written by: Miss Hetal Dhruve, Specialist Pharmacist Respiratory Medicine,
COPD Medications Coverage Summary Non-Insured Health Benefits Coverage SABA Bricanyl turbuhaler Yes Yes
 COPD Medications Coverage Summary Drug Non-Insured Health Benefits Coverage SABA Bricanyl turbuhaler Yes Yes Ventolin MDI + generics Yes Yes Ventolin Diskus NO NO Yukon Pharmacare/Chronic Disease Program
COPD Medications Coverage Summary Drug Non-Insured Health Benefits Coverage SABA Bricanyl turbuhaler Yes Yes Ventolin MDI + generics Yes Yes Ventolin Diskus NO NO Yukon Pharmacare/Chronic Disease Program
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) TREATMENT GUIDELINES
 TREATMENT GUIDELINES") CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) TREATMENT GUIDELINES Document Description Document Type Service Application Version Guidelines All healthcare professionals(hcps) caring for patients with asthma
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) TREATMENT GUIDELINES Document Description Document Type Service Application Version Guidelines All healthcare professionals(hcps) caring for patients with asthma
Asthma & COPD Medication Review. Hutchison Disclosures 2/16/2017. Objectives
 Asthma & COPD Medication Review Anna Meador, PharmD, BCACP Assistant Professor/ Pharmacy Director McWhorter School of Pharmacy/ Christ Health Center Amber Hutchison, PharmD, BCPS Assistant Clinical Professor
Asthma & COPD Medication Review Anna Meador, PharmD, BCACP Assistant Professor/ Pharmacy Director McWhorter School of Pharmacy/ Christ Health Center Amber Hutchison, PharmD, BCPS Assistant Clinical Professor
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC
 KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC") Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
QUANTITY LIMIT CRITERIA. BROVANA (arformoterol tartrate) SEREVENT DISKUS (salmeterol) STRIVERDI RESPIMAT (olodaterol)
 SEREVENT DISKUS (salmeterol) STRIVERDI RESPIMAT (olodaterol)") Carelirst. +.V Family of health care plans DRUG CLASS COMBINATIONS QUANTITY LIMIT CRITERIA LONG ACTING BETA2-ADRENERGIC AGONIST, ORAL INHALATION BRAND NAME (generic) LONG-ACTING BETA2-ADRENERGIC AGONISTS:
Carelirst. +.V Family of health care plans DRUG CLASS COMBINATIONS QUANTITY LIMIT CRITERIA LONG ACTING BETA2-ADRENERGIC AGONIST, ORAL INHALATION BRAND NAME (generic) LONG-ACTING BETA2-ADRENERGIC AGONISTS:
Algorithm for the use of inhaled therapies in COPD
 Berkshire West Integrated Care System Representing Berkshire West Clinical Commisioning Group Royal Berkshire NHS Foundation Trust Berkshire Healthcare NHS Foundation Trust Berkshire West Primary Care
Berkshire West Integrated Care System Representing Berkshire West Clinical Commisioning Group Royal Berkshire NHS Foundation Trust Berkshire Healthcare NHS Foundation Trust Berkshire West Primary Care
A Visual Approach to Simplifying Respiratory Drug Regimens
 A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP October 23, 2017 Learning Objectives Be able to list at least 3 major adverse effects of inhaled medications
A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP October 23, 2017 Learning Objectives Be able to list at least 3 major adverse effects of inhaled medications
COPD. Stan Kellar, MD. Physiology 11/4/2014. Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine
 Stan Kellar, MD Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine COPD Physiology The lungs are filters Filter in oxygen Filter out carbon dioxide (Vascular filter, not part of this discussion)
Stan Kellar, MD Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine COPD Physiology The lungs are filters Filter in oxygen Filter out carbon dioxide (Vascular filter, not part of this discussion)
A Visual Approach to Simplifying Respiratory Drug Regimens
 Adverse Effects of Inhaled Medications A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP June 28, 2017 Drug Category Beta 2 agonists antagonists Adverse Effects
Adverse Effects of Inhaled Medications A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP June 28, 2017 Drug Category Beta 2 agonists antagonists Adverse Effects
Medicines Management of Chronic Obstructive Pulmonary Disease (COPD)
") Medicines Management of Chronic Obstructive Pulmonary Disease (COPD) (Chronic & Acute) Guidelines for Primary Care Guideline Authors: Shaneez Dhanji (Wandsworth CCG) Samantha Prigmore (St George s Hospital)
Medicines Management of Chronic Obstructive Pulmonary Disease (COPD) (Chronic & Acute) Guidelines for Primary Care Guideline Authors: Shaneez Dhanji (Wandsworth CCG) Samantha Prigmore (St George s Hospital)
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
Asthma/COPD Update with Inhaler Workshop
 Asthma/COPD Update with Inhaler Workshop October 8, 2017 Nathan Samsa, DO, Pharm D, RPh, FACOI None Disclosures Agenda Asthma Updates COPD Updates Inhaler Workshop Medication Acronyms SABA: Short acting
Asthma/COPD Update with Inhaler Workshop October 8, 2017 Nathan Samsa, DO, Pharm D, RPh, FACOI None Disclosures Agenda Asthma Updates COPD Updates Inhaler Workshop Medication Acronyms SABA: Short acting
Chronic Obstructive Pulmonary Disease: What s New in Therapeutic Management?
 Chronic Obstructive Pulmonary Disease: What s New in Therapeutic Management? Sabrina Sherwood, PharmD PGY2 Internal Medicine Resident University of Utah Health September 29, 2018 Disclosures Relevant disclosures
Chronic Obstructive Pulmonary Disease: What s New in Therapeutic Management? Sabrina Sherwood, PharmD PGY2 Internal Medicine Resident University of Utah Health September 29, 2018 Disclosures Relevant disclosures
COPD. Understanding. An educational health series from National Jewish Health IN THIS ISSUE. What is COPD? 2. How is COPD Managed?
 Understanding COPD The Mount Sinai National Jewish Health Respiratory Institute was formed by the nation s leading respiratory hospital National Jewish Health, based in Denver, and top ranked academic
Understanding COPD The Mount Sinai National Jewish Health Respiratory Institute was formed by the nation s leading respiratory hospital National Jewish Health, based in Denver, and top ranked academic
Take My Breath Away: COPD Update. Jason Henderson D.O. Warren Clinic Pulmonary & Critical Care
 Take My Breath Away: Update Jason Henderson D.O. Warren Clinic Pulmonary & Critical Care Objectives 1. Recognize clinical signs and symptoms associated with chronic bronchitis and emphysema. 2. Describe
Take My Breath Away: Update Jason Henderson D.O. Warren Clinic Pulmonary & Critical Care Objectives 1. Recognize clinical signs and symptoms associated with chronic bronchitis and emphysema. 2. Describe
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
PFT s / 2017 Pulmonary Update. Eric S. Papierniak, DO University of Florida NF/SG VHA
 PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
Ferris State University College of Pharmacy MPA CE Symposium 2016 Paul Thill, PharmD, BCPS
 Ferris State University College of Pharmacy MPA CE Symposium 2016 Paul Thill, PharmD, BCPS Objectives Categorize the new asthma and COPD inhalers in to existing or newly created categories Discuss the
Ferris State University College of Pharmacy MPA CE Symposium 2016 Paul Thill, PharmD, BCPS Objectives Categorize the new asthma and COPD inhalers in to existing or newly created categories Discuss the
Michelle Zeidler, MD, MS
 7/1/18 Chronic Obstructive Pulmonary Disease: Optimizing Outpatient Care & Reducing Exacerbations Michelle Zeidler, MD, MS Professor of Medicine, Pulmonary, Critical Care Medicine & Sleep Medicine, VA
7/1/18 Chronic Obstructive Pulmonary Disease: Optimizing Outpatient Care & Reducing Exacerbations Michelle Zeidler, MD, MS Professor of Medicine, Pulmonary, Critical Care Medicine & Sleep Medicine, VA
Incorporating Newer Therapies and Strategies to Improve COPD Outcomes: A Practical Guide for Pharmacists. Learning Objectives.
 Incorporating Newer Therapies and Strategies to Improve COPD Outcomes: A Practical Guide for Pharmacists Learning Objectives Identify the risk factors for COPD and the clinical features that differentiate
Incorporating Newer Therapies and Strategies to Improve COPD Outcomes: A Practical Guide for Pharmacists Learning Objectives Identify the risk factors for COPD and the clinical features that differentiate
Medications for Managing COPD in Hospice Patients. Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources
 Medications for Managing COPD in Hospice Patients Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources Goal of medications in COPD Decrease symptoms and/or complications Reduce frequency
Medications for Managing COPD in Hospice Patients Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources Goal of medications in COPD Decrease symptoms and/or complications Reduce frequency
COPD Prescribing Guidelines
 Cannock Chase Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group East Staffordshire Clinical Commissioning
Cannock Chase Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group East Staffordshire Clinical Commissioning
At-A-Glance Outpatient Management Reference for Chronic Obstructive Pulmonary Disease (COPD)
") At-A-Glance Outpatient Management Reference f Chronic Obstructive Pulmonary Disease (COPD) BASED ON THE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT AND PREVENTION OF COPD GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE
At-A-Glance Outpatient Management Reference f Chronic Obstructive Pulmonary Disease (COPD) BASED ON THE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT AND PREVENTION OF COPD GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE
MEDICAL COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 07/05/18 SECTION: DRUGS LAST REVIEW DATE: LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 CINQAIR (reslizumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
CINQAIR (reslizumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
SABA: VENTOLIN EVOHALER (SALBUTAMOL) SAMA: ATROVENT IPRATROPIUM. Offer LAMA (discontinue SAMA) OR LABA
 SAMA: ATROVENT IPRATROPIUM. Offer LAMA (discontinue SAMA) OR LABA") COPD GUIDELINES DIAGNOSIS >35 years of age Symptoms of cough, breathlessness, sputum, wheeze, Risk factor (SMOKING) Spirometry (post bronchodilator) FEV1/FVC = 0.7 ENCOURAGE PATIENTS TO BRING INHALERS
COPD GUIDELINES DIAGNOSIS >35 years of age Symptoms of cough, breathlessness, sputum, wheeze, Risk factor (SMOKING) Spirometry (post bronchodilator) FEV1/FVC = 0.7 ENCOURAGE PATIENTS TO BRING INHALERS
Select Inhaled Respiratory Agents
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Advancing COPD treatment strategies with evidencebased. 17:15 19:15 Monday 11 September 2017 ERS 2017, Milan, Italy
 Advancing COPD treatment strategies with evidencebased approaches 17:15 19:15 Monday 11 September 2017 ERS 2017, Milan, Italy Increasing understanding of COPD and the effect on guideline evolution. GOLD
Advancing COPD treatment strategies with evidencebased approaches 17:15 19:15 Monday 11 September 2017 ERS 2017, Milan, Italy Increasing understanding of COPD and the effect on guideline evolution. GOLD
Pharmacist Objectives. Pulmonary Update. Outline. Technician Objectives. GOLD Guidelines. COPD Diagnosis 9/22/2017
 Pharmacist Objectives Pulmonary Update Patty Marshik, PharmD Associate Professor University of New Mexico College of Pharmacy pmarshik@salud.unm.edu Discuss the new Global Initiative for Chronic Obstructive
Pharmacist Objectives Pulmonary Update Patty Marshik, PharmD Associate Professor University of New Mexico College of Pharmacy pmarshik@salud.unm.edu Discuss the new Global Initiative for Chronic Obstructive
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable
 THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
Co. Durham & Darlington Respiratory Network COPD Treatment Guide
 Co. Durham & Darlington Respiratory Network COPD Treatment Guide Age > 35, Productive cough, Breathless, Smoking Hx Spirometry (post-bronchodilator) COPD Advice Intensive smoking cessation support Vaccination
Co. Durham & Darlington Respiratory Network COPD Treatment Guide Age > 35, Productive cough, Breathless, Smoking Hx Spirometry (post-bronchodilator) COPD Advice Intensive smoking cessation support Vaccination
Class Update: Asthma / COPD Medications
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Inhaled Corticosteroids Drug Class Prior Authorization Protocol
 Inhaled Corticosteroids Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Inhaled Corticosteroids Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
WINDY CITY WHEEZE: A PREVENTATIVE APPROACH TO COPD MANAGEMENT
 WINDY CITY WHEEZE: A PREVENTATIVE APPROACH TO COPD MANAGEMENT Thursday, October 25, 2018 Sarah Sungurlu DO Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures I have no actual
WINDY CITY WHEEZE: A PREVENTATIVE APPROACH TO COPD MANAGEMENT Thursday, October 25, 2018 Sarah Sungurlu DO Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures I have no actual
Address Comorbidities
 Greater Manchester COPD Management Plan Non-pharmacological management for ALL patients Smoking Cessation Annual Flu Vaccination Pulmonary Rehabilitation Increase daily activity Inhaler Technique Measure
Greater Manchester COPD Management Plan Non-pharmacological management for ALL patients Smoking Cessation Annual Flu Vaccination Pulmonary Rehabilitation Increase daily activity Inhaler Technique Measure
Objectives. Advances in Managing COPD Patients
 4:45 5:30pm Advances in Managing Patients SPEAKER Nicola Hanania, MD, FCCP, FRCP, FACP Presenter Disclosure Information The following relationships exist related to this presentation: Nicola Hanania, MD,
4:45 5:30pm Advances in Managing Patients SPEAKER Nicola Hanania, MD, FCCP, FRCP, FACP Presenter Disclosure Information The following relationships exist related to this presentation: Nicola Hanania, MD,
Assessing Severity. Management of Stable COPD. General Approach. Short Acting Bronchodilators. Staging System (GOLD)
") William P. Saliski Jr. DO Montgomery Pulmonary Consultants Management of Stable COPD Pharmacotherapy Oxygen Smoking Cessation Vaccinations Rehabilitation Surgery Future Discussions Assessing Severity Staging
William P. Saliski Jr. DO Montgomery Pulmonary Consultants Management of Stable COPD Pharmacotherapy Oxygen Smoking Cessation Vaccinations Rehabilitation Surgery Future Discussions Assessing Severity Staging
Inhaled Corticosteroids Drug Class Prior Authorization Protocol
 Inhaled Corticosteroids Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Inhaled Corticosteroids Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
COPD/Asthma. Prudence Twigg, AGNP
 COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease CareOregon Pharmacy Abridged sample of presentation content Home Equipment Pathophysiology Exacerbations Guidelines Lifestyle Modification Medication Management Sample
Chronic Obstructive Pulmonary Disease CareOregon Pharmacy Abridged sample of presentation content Home Equipment Pathophysiology Exacerbations Guidelines Lifestyle Modification Medication Management Sample
COPD and Asthma Update. April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute
 COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
II: Moderate Worsening airflow limitations Dyspnea on exertion, cough, and sputum production; patient usually seeks medical
 Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
11/27/18. Challenges in Pulmonary and Critical Care: COPD So Much is New! Faculty. Disclosures
 Challenges in Pulmonary and Critical Care: 2018 COPD So Much is New! 1 Faculty Anas Hadeh, MD, FCCP Director, Pulmonary and Critical Care Medicine Fellowship Program Affiliate Assistant Professor of Clinical
Challenges in Pulmonary and Critical Care: 2018 COPD So Much is New! 1 Faculty Anas Hadeh, MD, FCCP Director, Pulmonary and Critical Care Medicine Fellowship Program Affiliate Assistant Professor of Clinical
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Seebri Neohaler) Reference Number: CP.CPA.150 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Seebri Neohaler) Reference Number: CP.CPA.150 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy
Prescribing guidelines: Management of COPD in Primary Care
 Prescribing guidelines: Management of COPD in Primary Care Establish diagnosis of COPD in patients 35 years with appropriate symptoms with history, examination and spirometry (FEV1/FVC ratio < 70%) Establish
Prescribing guidelines: Management of COPD in Primary Care Establish diagnosis of COPD in patients 35 years with appropriate symptoms with history, examination and spirometry (FEV1/FVC ratio < 70%) Establish