Bronchospasm & SOB. Kim Kilmurray Senior Clinical Teaching Fellow
|
|
|
- Arlene Rodgers
- 6 years ago
- Views:
Transcription

1 Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow
2 LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum of asthma severities & describe stepwise asthma management Describe COPD management & how it might differ from that of asthma List the signs of anaphylaxis, concerning features and key steps in management
3 B on ABCDE assessment RR Oxygen saturations Respiratory distress Use of respiratory muscles Tachypnoea Speaking in sentences Cyanosis Tripod position Drooling Stridor Wheeze
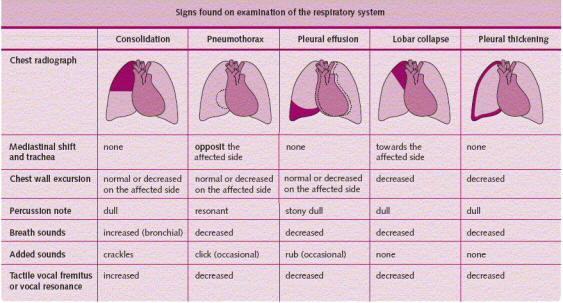
4 Respiratory examination Inspection Signs of respiratory distress Pallor Cyanosis Finger clubbing Tremor Chest wall shape Palpation Trachea position Cervical lymphadenopathy Chest expansion Tactile vocal fremitis
5 Respiratory examination Percussion Dullness Hyperresonance Auscultation Breath sounds Vocal resonance 2 zones anteriorly 3 zones posteriorly Axilla Compare right with left
6

7 Remember to always examine the back!
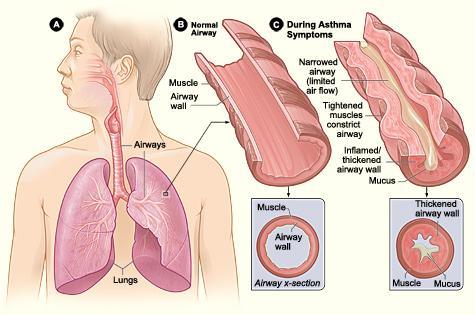
8 Bronchospasm Constriction of bronchi & bronchioles Caused by: a spasm in the smooth muscles of bronchi and bronchioles an inflammation of the airways excessive production of mucous due to: an allergic reaction irritation caused by mechanical friction of air, overcooling or drying of airways
9 Symptoms Difficulty breathing Wheezing Coughing Dyspnoea
10 Case 1 24 year old female presents by ambulance with a 3 day history of a cough productive of green sputum, coryza, intermittent temperatures and difficulty breathing. PMH Asthma Observations Temp 38.7 ⁰C Pulse 124 bpm BP 124/76 RR 34 Oxygen saturations 94% in RA PEFR 240 ml (normal 440ml)
11 What s abnormal in her observations? Pyrexia Tachycardia Tachypnoea Hypoxia PEFR < 50% normal
12 On examination Speaking in phrases Using respiratory accessory muscles Chest Reduced AE throughout Widespread expiratory wheeze
13 Treatment Salbutamol nebuliser 5mg Ipratropium Bromide nebuliser 500 mcg Prednisolone 50 mg Oxygen therapy to maintain saturations > 94%
14 She s not improving what s next? Back to back salbutamol nebulisers IV Magnesium Sulphate 2g Antibiotics IV amoxicillin 1g?Salbutamol IV infusion
15 Diagnosis Infective acute severe exacerbation of asthma
16
17 How do you grade asthma exacerbations? Moderate Severe Life Threatening Near Fatal
18 Moderate Asthma Increasing symptoms PEF >50 75% best or predicted No features of acute severe asthma
19 Acute Severe Asthma Any one of: PEFR 33 50% best or predicted Respiratory rate 25/min Heart rate 110/min Inability to complete sentences in one breath
20 Life Threatening Asthma PEFR < 33% best or predicted SpO 2 < 92% PaO 2 < 8 kpa Normal PaCO 2 ( kpa) Silent chest Cyanosis Poor respiratory effort Arrhythmia Exhaustion Altered conscious level Hypotension
21 Near Fatal Asthma Raised PaCO 2 and/or requiring mechanical Ventilation with raised inflation pressures
22 Case 2 59 year old male presents with a 5 day history of a cough productive of green sputum, intermittent temperatures and breathlessness. PMH : COPD Observations: Temperature 38 ⁰ C Pulse 104 bpm BP 134/86 RR 36 Oxygen saturations 86% in RA
23 What are his abnormal observations? Pyrexia Tachycardia Tachypnoea Hypoxia
24 On examination Speaking in words Central cyanosis Using respiratory accessory muscles Chest AE equal and bilateral Widespread expiratory wheeze
25 ABG po₂ 7.2 kpa pco₂ 12.4 kpa H+ 64 mmol HCO₃ 32 mmol
26 ABG Type 2 Respiratory Failure Hypoxia (low oxygen) Hypercapnia (high carbon dioxide) Respiratory Acidosis High hydrogen ion concentration High carbon dioxide
27 How does your treatment differ from asthma? Controlled oxygen therapy 24 28% oxygen No improvement after 1 hour, consider NIV Otherwise management is the same as severe asthma Salbutamol nebulisers 5 mg Ipratropium nebulisers 500 mcg Prednisolone 50 mg IV Magnesium Sulphate 2 g

28

29 Venturi masks
30 Case 3 18 year old female presents with a sudden onset of difficulty breathing, an itchy rash, lip and tongue swelling that started 20 minutes ago. She had been eating chicken satay 10 minutes prior to her symptoms starting No known PMH, DH and NKDA Observations: Temp 37.4 o C Pulse 126 bpm BP 90 / 60 RR 32 Oxygen saturations 90 % in RA
31 What are her abnormal observations? Tachycardia Hypotension Tachypnoea Hypoxia
32 Airway noises Wheeze Caused by lower airway swelling Expiratory Whistling Stridor Caused by upper airway swelling Inspiratory Harsh, high pitched
33 Causes of wheeze Asthma COPD Bronchiolitis Viral induced wheeze Bronchiectasis
34 Causes of stridor Anaphylaxis Angio-oedema Croup Laryngitis Severe tonsillitis Inhaled foreign body Epiglottitis Vocal cord dysfunction
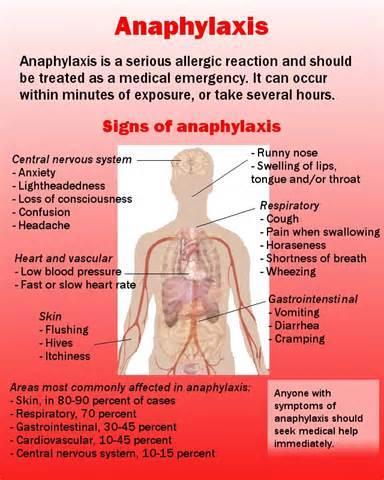
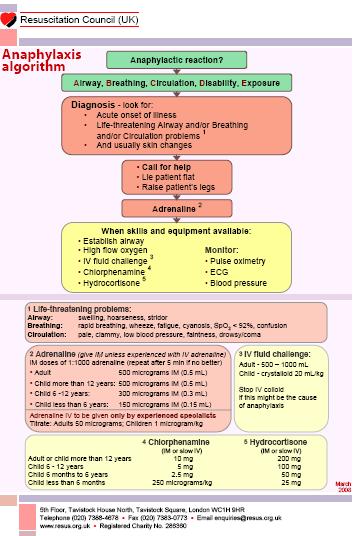
35 ANAPHYLAXIS Signs & symptoms Wheeze Hoarseness Chest tightness Urticaria Angio-oedema Stridor Respiratory collapse Confusion Agitation Hypotension Cyanosis
36



37

38
39
40 Treatment Give intramuscular (IM) adrenaline 1: mg (0.5ml) Repeat IM adrenaline at 5 minute intervals until there has been an adequate response. Consider nebulised adrenaline 5mg (5ml 1:1000) Oxygen therapy via NRM 15 L IV Chlorphenamine 10mg IV Hydrocortisone 200mg IV Fluids 1 L
41
42 Beware!!! The Biphasic reaction A delayed reaction with further symptoms developing 4 8 hours after the initial presentation.
43 SUMMARY Covered how to perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identified the spectrum of asthma severities & describe stepwise asthma management Described COPD management & how it might differ from that of asthma Listed the signs of anaphylaxis, concerning features and key steps in management

44 QUESTIONS
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Asthma/wheeze management plan
 Asthma/wheeze management plan Name of Patient Date of Birth NHS Number GP surgery Telephone Next appointment Children s Assessment unit/ward telephone Out of hours call 111 Open access Y/N Until date Some
Asthma/wheeze management plan Name of Patient Date of Birth NHS Number GP surgery Telephone Next appointment Children s Assessment unit/ward telephone Out of hours call 111 Open access Y/N Until date Some
Title Protocol for the Management of Asthma
 Document Control Title Protocol for the Management of Asthma Author Author s job title Professional Lead, Minor Injuries Unit Directorate Emergency Services, Logistics and Resilience Department Version
Document Control Title Protocol for the Management of Asthma Author Author s job title Professional Lead, Minor Injuries Unit Directorate Emergency Services, Logistics and Resilience Department Version
Anaphylaxis: Treatment in the Community
 : Treatment in the Community is likely if a patient who, within minutes of exposure to a trigger (allergen), develops a sudden illness with rapidly progressing skin changes and life-threatening airway
: Treatment in the Community is likely if a patient who, within minutes of exposure to a trigger (allergen), develops a sudden illness with rapidly progressing skin changes and life-threatening airway
Wash your hands, introduce yourself, obtain consent.
 Introduction At the start: Wash your hands, introduce yourself, obtain consent. Patient position: Sitting upright (45 o ) & adequately exposed (undress to waist). NB: if you have a female patient, the
Introduction At the start: Wash your hands, introduce yourself, obtain consent. Patient position: Sitting upright (45 o ) & adequately exposed (undress to waist). NB: if you have a female patient, the
Anaphylaxis: treatment in the community
 : treatment in the community Item Type Guideline Authors Health Service Executive Citation Health Service Executive. : treatment in the community. Dublin: Health Service Executive;. 5p. Publisher Health
: treatment in the community Item Type Guideline Authors Health Service Executive Citation Health Service Executive. : treatment in the community. Dublin: Health Service Executive;. 5p. Publisher Health
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
Firefighter Pre-Hospital Care Program Recruit Presentation. Respiratory Emergencies
 Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
Exacerbations. Ronald Dahl, Aarhus University Hospital, Denmark
 1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
Management of acute asthma in children in emergency department. Moderate asthma
 152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
Respiratory Medicine
 Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
Exacerbations of COPD. Dr J Cullen
 Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Anaphylaxis/Latex Allergy
 Children s Acute Transport Service CATS Clinical Guideline Anaphylaxis/Latex Allergy Document Control Information Author D Lutman Author Position Consultant Document Owner E Polke Document Owner Position
Children s Acute Transport Service CATS Clinical Guideline Anaphylaxis/Latex Allergy Document Control Information Author D Lutman Author Position Consultant Document Owner E Polke Document Owner Position
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Appendix (i) The ABCDE approach to the sick patient
 The ABCDE approach to the sick patient") Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Asthma. chapter 7. Overview
 chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
It s as easy as ABC. Dr Andrew Smith
 It s as easy as ABC Dr Andrew Smith ABCDE A simple method to apply to your assessment of patients. It is a good failsafe in all situations i.e. At an end of an OSCE when you re put under pressure! Correct
It s as easy as ABC Dr Andrew Smith ABCDE A simple method to apply to your assessment of patients. It is a good failsafe in all situations i.e. At an end of an OSCE when you re put under pressure! Correct
a. Will not suppress respiratory drive in acute asthma
 Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Shelley Westwood, RN, BSN
 Shelley Westwood, RN, BSN The body requires a constant supply of oxygen for survival. AMERICAN RED CROSS FIRST AID RESPONDING TO EMERGENCIES FOURTH EDITION Copyright 2006 by The American National Red Cross
Shelley Westwood, RN, BSN The body requires a constant supply of oxygen for survival. AMERICAN RED CROSS FIRST AID RESPONDING TO EMERGENCIES FOURTH EDITION Copyright 2006 by The American National Red Cross
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
PAEDIATRIC ACUTE CARE GUIDELINE. Croup. This document should be read in conjunction with this DISCLAIMER
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Croup Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Croup Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Respiratory system. Applied Anatomy &Physiology
 Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Management of acute severe asthma in adults in general practice. Moderate asthma Acute severe asthma Life-threatening asthma INITIAL ASSESSMENT
 British guideline on the management of asthma Annex 2 Management of acute severe asthma in adults in general practice Many deaths from asthma are preventable. Delay can be fatal. Factors leading to poor
British guideline on the management of asthma Annex 2 Management of acute severe asthma in adults in general practice Many deaths from asthma are preventable. Delay can be fatal. Factors leading to poor
Clinical guideline for acute wheeze & asthma in children 5 years and over Hospital care
 Clinical guideline for acute wheeze & asthma in children years and over Hospital care Airedale NHS Trust Bradford Teaching Hospitals NHS Foundation Trust NHS Bradford and Airedale DOB: A&E/Hospital : Weight:
Clinical guideline for acute wheeze & asthma in children years and over Hospital care Airedale NHS Trust Bradford Teaching Hospitals NHS Foundation Trust NHS Bradford and Airedale DOB: A&E/Hospital : Weight:
The Goal of the Respiratory Assessment. Two Parts of the Respiratory Assessment
 The Respiratory System Respiratory Assessment of the Adult Patient Mary Douglas, MSN, RN Nurse Educator Minneapolis VA Health Care System Respiratory system: moves oxygen into the body and carbon dioxide
The Respiratory System Respiratory Assessment of the Adult Patient Mary Douglas, MSN, RN Nurse Educator Minneapolis VA Health Care System Respiratory system: moves oxygen into the body and carbon dioxide
ASTHMA (SEE BTS GUIDELINES NEXT PAGE)
") ASTHMA (SEE BTS GUIDELINES NEXT PAGE) RESPIRATORY Signs of Severe asthma Unable to speak in sentences? Peak flow < 50% predicted or best? Respiratory Rate >25/min? Pulse>110/min? Sa0 2
ASTHMA (SEE BTS GUIDELINES NEXT PAGE) RESPIRATORY Signs of Severe asthma Unable to speak in sentences? Peak flow < 50% predicted or best? Respiratory Rate >25/min? Pulse>110/min? Sa0 2
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Airway and Ventilation. Emergency Medical Response
 Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Significance. Asthma Definition. Focus on Asthma
 Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Acute Respiratory Emergencies. Martin Johnson Consultant Physician Gartnavel / Western
 Acute Respiratory Emergencies Martin Johnson Consultant Physician Gartnavel / Western Summary What to expect - what are the common respiratory emergencies? How to recognise the problem? How to manage the
Acute Respiratory Emergencies Martin Johnson Consultant Physician Gartnavel / Western Summary What to expect - what are the common respiratory emergencies? How to recognise the problem? How to manage the
Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong
 Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
COPD Challenge CASE PRESENTATION
 Chronic obstructive pulmonary disease (COPD) exacerbations may make up more than 10% of acute medical admissions [1], and they are increasingly recognised as a cause of significant morbidity and mortality
Chronic obstructive pulmonary disease (COPD) exacerbations may make up more than 10% of acute medical admissions [1], and they are increasingly recognised as a cause of significant morbidity and mortality
Chapter 16. Objectives. Objectives. Respiratory Emergencies
 Chapter 16 Respiratory Emergencies Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key
Chapter 16 Respiratory Emergencies Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key
Respiratory Emergencies. Lesson Goal. Lesson Objectives 9/10/2012
 Respiratory Emergencies Lesson Goal Assess and provide timely treatment & transport to patients experiencing respiratory emergencies Lesson Objectives List parts of respiratory system and how they work
Respiratory Emergencies Lesson Goal Assess and provide timely treatment & transport to patients experiencing respiratory emergencies Lesson Objectives List parts of respiratory system and how they work
AIRWAY MANAGEMENT Anaesthetics & Recovery 2015
 AIRWAY MANAGEMENT Anaesthetics & Recovery 2015 INITIAL ASSESSMENT ON ARRIVAL TO THE PACU, THE PATIENT IS ATTACHED TO MONITORING AND O2, THE PACU NURSE RECEIVES CLINICAL HANDOVER FROM THE ANAESTHETIC TEAM
AIRWAY MANAGEMENT Anaesthetics & Recovery 2015 INITIAL ASSESSMENT ON ARRIVAL TO THE PACU, THE PATIENT IS ATTACHED TO MONITORING AND O2, THE PACU NURSE RECEIVES CLINICAL HANDOVER FROM THE ANAESTHETIC TEAM
 β 2004 2004 o β β β β 2004 β β β β β β β β β 2004 2004 2004 2004 2004 β 2004 2004 2004 2004 β β 2004 β β β β β β β 2004 β β β β β β 2004 β β β β STEP 5: CONTINUOUS OR FREQUENT USE OF ORAL
β 2004 2004 o β β β β 2004 β β β β β β β β β 2004 2004 2004 2004 2004 β 2004 2004 2004 2004 β β 2004 β β β β β β β 2004 β β β β β β 2004 β β β β STEP 5: CONTINUOUS OR FREQUENT USE OF ORAL
Respiratory Distress/Failure - General
 Respiratory Distress/Failure - General Criteria: Dyspnea WITHOUT a clear etiology O 2 V/S and SpO 2 (with and without Oxygen therapy if possible) Blood glucose analysis: if less than 80 mg/dl, refer to
Respiratory Distress/Failure - General Criteria: Dyspnea WITHOUT a clear etiology O 2 V/S and SpO 2 (with and without Oxygen therapy if possible) Blood glucose analysis: if less than 80 mg/dl, refer to
Croup (Laryngo-tracheo-bronchitis)
") Croup (Laryngo-tracheo-bronchitis) 1a 2a 2b Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of
Croup (Laryngo-tracheo-bronchitis) 1a 2a 2b Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of
CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2
 CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2 M1 Objectives To understand how resuscitation techniques should be modified in the special circumstances of: Hypothermia Immersion and submersion Poisoning Pregnancy
CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2 M1 Objectives To understand how resuscitation techniques should be modified in the special circumstances of: Hypothermia Immersion and submersion Poisoning Pregnancy
Problem Based Learning Session. Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days.
 Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
Managing Exacerbations of COPD (Version 3.0)
") Managing Exacerbations of COPD (Version 3.0) Guideline Readership This guideline is intended for use in patients with a confirmed diagnosis of a chronic obstructive pulmonary disease (COPD) exacerbation.
Managing Exacerbations of COPD (Version 3.0) Guideline Readership This guideline is intended for use in patients with a confirmed diagnosis of a chronic obstructive pulmonary disease (COPD) exacerbation.
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
Management of Acute Asthma Exacerbations in Children 2012 Update. Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch
 Management of Acute Asthma Exacerbations in Children 2012 Update Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch Acknowledgements BTS/SIGN guidelines GINA guidelines NAEPP guidelines
Management of Acute Asthma Exacerbations in Children 2012 Update Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch Acknowledgements BTS/SIGN guidelines GINA guidelines NAEPP guidelines
Oxygen: Is there a problem? Tom Heaps Acute Physician
 Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
ANAPHYLAXIS Following Vaccination. A Severe Adverse Event. Developed for the Grampians Infection Control Group (GRICG) Version 2.
 Version 2.") ANAPHYLAXIS Following Vaccination A Severe Adverse Event Developed for the Grampians Infection Control Group () Version 2.0:2014 Adverse Event Following Immunisation Adverse event following immunisation
ANAPHYLAXIS Following Vaccination A Severe Adverse Event Developed for the Grampians Infection Control Group () Version 2.0:2014 Adverse Event Following Immunisation Adverse event following immunisation
Guideline on the Management of Asthma in adults SHSCT
 CLINICAL GUIDELINES ID TAG Title: Author: Speciality / Division: Directorate: Management of Asthma in adults Dr A John, Dr J Lindsay Respiratory Medicine/ MUSC Medicine Date Uploaded: 23/11/15 Review Date
CLINICAL GUIDELINES ID TAG Title: Author: Speciality / Division: Directorate: Management of Asthma in adults Dr A John, Dr J Lindsay Respiratory Medicine/ MUSC Medicine Date Uploaded: 23/11/15 Review Date
patient group direction
 SALBUTAMOL v01 1/12 SALBUTAMOL PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner
SALBUTAMOL v01 1/12 SALBUTAMOL PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner
2 nd Year Revision Respiratory. Michael Hodkinson
 2 nd Year Revision Respiratory Michael Hodkinson Before we start This is a quick run through of topics Obviously there will be more to learn than what s in these slides but hopefully it will provide a
2 nd Year Revision Respiratory Michael Hodkinson Before we start This is a quick run through of topics Obviously there will be more to learn than what s in these slides but hopefully it will provide a
AIRWAY & HEART ANOTOMY
 Objectives I CAN T BREATH Respiratory Emergencies Review of anatomical structures related to heart & lungs Differentiate differences between adult and pediatric airways Identify the need for airway assistance
Objectives I CAN T BREATH Respiratory Emergencies Review of anatomical structures related to heart & lungs Differentiate differences between adult and pediatric airways Identify the need for airway assistance
Clinical Director for Women s and Children s Division
 UPPER AIRWAY OBSTRUCTION (UAO) (INCLUDING CROUP) CHILDREN & YOUNG PEOPLE 0-16 CLINICAL GUIDELINES Register No: 10097 Status: Public Developed in response to: Guideline Review CQC Fundamental Standard:
UPPER AIRWAY OBSTRUCTION (UAO) (INCLUDING CROUP) CHILDREN & YOUNG PEOPLE 0-16 CLINICAL GUIDELINES Register No: 10097 Status: Public Developed in response to: Guideline Review CQC Fundamental Standard:
Emergency Asthma Care
 Emergency Asthma Care Contents Introduction 3 Why good emergency asthma care is important 4 Access to emergency asthma care 5 How to improve emergency asthma care 6 Developing emergency asthma treatment
Emergency Asthma Care Contents Introduction 3 Why good emergency asthma care is important 4 Access to emergency asthma care 5 How to improve emergency asthma care 6 Developing emergency asthma treatment
Anaphylaxis 5/31/2015
 1 Definition of anaphylaxis Anaphylaxis Jon Kyle Andersen Anaphylaxis is a severe, life-threatening, generalised or systemic hypersensitivity reaction. It is characterised by rapidly developing, life-threatening
1 Definition of anaphylaxis Anaphylaxis Jon Kyle Andersen Anaphylaxis is a severe, life-threatening, generalised or systemic hypersensitivity reaction. It is characterised by rapidly developing, life-threatening
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Upper Airway Obstruction
 Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Chapter 20 - Immunologic Emergencies
 1 2 3 4 5 6 7 8 9 10 National EMS Education Standard Competencies (1 of 2) Medicine Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an
1 2 3 4 5 6 7 8 9 10 National EMS Education Standard Competencies (1 of 2) Medicine Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an
Glossary of Asthma Terms
 HealthyKidsExpress@bjc.org Asthma Words to Know Developed in partnership with Health Literacy Missouri Airways (Bronchi, Bronchial Tubes): The tubes in the lungs that let air in and out of the body. Airway
HealthyKidsExpress@bjc.org Asthma Words to Know Developed in partnership with Health Literacy Missouri Airways (Bronchi, Bronchial Tubes): The tubes in the lungs that let air in and out of the body. Airway
Medical Emergencies and Current Management in Dentistry. Prof. Mark Greenwood Newcastle University
 Medical Emergencies and Current Management in Dentistry Prof. Mark Greenwood Newcastle University Lancaster 1.02.12 PREVENTION! Attitude and environment Usually a clue in the history PREVENTION! Attitude
Medical Emergencies and Current Management in Dentistry Prof. Mark Greenwood Newcastle University Lancaster 1.02.12 PREVENTION! Attitude and environment Usually a clue in the history PREVENTION! Attitude
CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM
 CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM Pages 244-247 DO NOW What structures, do you think, are active participating in the breathing process? 2 WHAT ARE WE DOING IN TODAY S CLASS Finishing Digestion
CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM Pages 244-247 DO NOW What structures, do you think, are active participating in the breathing process? 2 WHAT ARE WE DOING IN TODAY S CLASS Finishing Digestion
Managing Medical Emergencies in a Dental Practice
 Managing Medical Emergencies in a Dental Practice To download a copy of this handout, or for further information please visit www.backtolife.co.uk/resources Back to Life Ltd, Milton Heath House, Westcott
Managing Medical Emergencies in a Dental Practice To download a copy of this handout, or for further information please visit www.backtolife.co.uk/resources Back to Life Ltd, Milton Heath House, Westcott
RESPIRATORY ASSESSMENT JENNY CASEY RESPIRATORY SERVICES LEAD ACE
 RESPIRATORY ASSESSMENT JENNY CASEY RESPIRATORY SERVICES LEAD ACE What does respiratory assessment involve? Subjective Assessment Objective Assessment Inspection, palpation, percussion and auscultation
RESPIRATORY ASSESSMENT JENNY CASEY RESPIRATORY SERVICES LEAD ACE What does respiratory assessment involve? Subjective Assessment Objective Assessment Inspection, palpation, percussion and auscultation
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Respiratory distress in children
 Respiratory distress in children Joey Gassen, MD Overview Backgroundand definition First five minutes History and physical exam Key historical features Signs and symptoms Possible causes and differential
Respiratory distress in children Joey Gassen, MD Overview Backgroundand definition First five minutes History and physical exam Key historical features Signs and symptoms Possible causes and differential
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Arterial Blood Gas Interpretation Routine Assessment Inspection Palpation Auscultation Labs Na 135-145 K 3.5-5.3 Chloride 95-105 CO2 22-31 BUN 10-26 Creat.5-1.2 Glu 80-120 Arterial Blood Gases WBC 5-10K
Arterial Blood Gas Interpretation Routine Assessment Inspection Palpation Auscultation Labs Na 135-145 K 3.5-5.3 Chloride 95-105 CO2 22-31 BUN 10-26 Creat.5-1.2 Glu 80-120 Arterial Blood Gases WBC 5-10K
THE BREATHLESS CHILD. Dr Rhiannon Furr Paediatric Consultant Oxford Children s Hospital
 THE BREATHLESS CHILD Dr Rhiannon Furr Paediatric Consultant Oxford Children s Hospital 3 rd November 2016 Causes of breathing difficulties? Asthma/VIW Croup Bronchiolitis Pneumonia Pertussis Inhaled foreign
THE BREATHLESS CHILD Dr Rhiannon Furr Paediatric Consultant Oxford Children s Hospital 3 rd November 2016 Causes of breathing difficulties? Asthma/VIW Croup Bronchiolitis Pneumonia Pertussis Inhaled foreign
Management of an immediate adverse event following immunisation
 Management of an immediate adverse event following immunisation The vaccinated person should remain under observation for a short interval to ensure that they do not experience an immediate adverse event.
Management of an immediate adverse event following immunisation The vaccinated person should remain under observation for a short interval to ensure that they do not experience an immediate adverse event.
Chapter 15 - Respiratory Emergencies
 1 2 3 4 5 6 7 National EMS Education Standard Competencies (1 of 5) Medicine Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
1 2 3 4 5 6 7 National EMS Education Standard Competencies (1 of 5) Medicine Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
Respiratory Emergencies. Chapter 11
 Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Type: Clinical Guideline Register No: Status: Public MANAGEMENT OF ACUTE ASTHMA IN CHILDREN MORE THAN 2 YEARS IN HOSPITAL
 MANAGEMENT OF ACUTE ASTHMA IN CHILDREN MORE THAN 2 YEARS IN HOSPITAL Type: Clinical Guideline Register No: 09055 Status: Public Developed in Response to: Best practice CQC Fundamental Standard: 9, 12,
MANAGEMENT OF ACUTE ASTHMA IN CHILDREN MORE THAN 2 YEARS IN HOSPITAL Type: Clinical Guideline Register No: 09055 Status: Public Developed in Response to: Best practice CQC Fundamental Standard: 9, 12,
IAEM Clinical Guideline 9 Laryngomalacia. Version 1 September, Author: Dr Farah Mustafa
 IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
10/17/16. Acute Respiratory Failure in the Acute Care Setting. Margaret Rosales, APRN-CNP, FNP
 Acute Respiratory Failure in the Acute Care Setting Margaret Rosales, APRN-CNP, FNP Margaret_r1965@yahoo.com 918-448-5887 1 Definition: Respiratory failure is a syndrome in which the respiratory system
Acute Respiratory Failure in the Acute Care Setting Margaret Rosales, APRN-CNP, FNP Margaret_r1965@yahoo.com 918-448-5887 1 Definition: Respiratory failure is a syndrome in which the respiratory system
Asthma training. Mike Levin Division of Asthma and Allergy Red Cross Hospital
 Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
BRONCHIOLITIS PEDIATRIC
 DEFINITION Bronchiolitis is typically defined as the first episode of wheezing in infants < 24 months of age. It is a viral illness of the lower respiratory tract that causes tachypnea, bronchospasm, and
DEFINITION Bronchiolitis is typically defined as the first episode of wheezing in infants < 24 months of age. It is a viral illness of the lower respiratory tract that causes tachypnea, bronchospasm, and
Have you ever managed patients who have experienced an adverse reaction to transfusion?
 Have you ever managed patients who have experienced an adverse reaction to transfusion? A. Yes, often B. Yes, occasionally C. No A. 1 in 30 units? B. 1 in 100? C. 1 in 1000? D. 1 in 10,000? SHOT collects
Have you ever managed patients who have experienced an adverse reaction to transfusion? A. Yes, often B. Yes, occasionally C. No A. 1 in 30 units? B. 1 in 100? C. 1 in 1000? D. 1 in 10,000? SHOT collects
An Illustrated Guide For Respiratory System Examination. Bedside Teaching for 2 nd year medical Students
 An Illustrated Guide For Respiratory System Examination Bedside Teaching for 2 nd year medical Students Prepared by: Dr. Farid Ghalli Clinical Teacher (Hon) 2016 Respiratory System Examination Inspection
An Illustrated Guide For Respiratory System Examination Bedside Teaching for 2 nd year medical Students Prepared by: Dr. Farid Ghalli Clinical Teacher (Hon) 2016 Respiratory System Examination Inspection
ACUTE ASTHMA (WARD) Paediatrics > Scenario 5
 Paediatrics > Scenario 5") ACUTE ASTHMA (WARD) MODULE: BREATHING TARGET: ALL PAEDIATRIC TRAINEES; ED NURSING STAFF BACKGROUND: Acute asthma is a common presentation in the Emergency Department, and many of these children are admitted
ACUTE ASTHMA (WARD) MODULE: BREATHING TARGET: ALL PAEDIATRIC TRAINEES; ED NURSING STAFF BACKGROUND: Acute asthma is a common presentation in the Emergency Department, and many of these children are admitted
Allergic Reactions and Envenomations. Chapter 16
 Allergic Reactions and Envenomations Chapter 16 Allergic Reactions Allergic reaction Exaggerated immune response to any substance Histamines and leukotrienes Chemicals released by the immune system Anaphylaxis
Allergic Reactions and Envenomations Chapter 16 Allergic Reactions Allergic reaction Exaggerated immune response to any substance Histamines and leukotrienes Chemicals released by the immune system Anaphylaxis
Medicine Dr. Kawa Lecture 4 - Treatment of asthma :
 Medicine Dr. Kawa Lecture 4 - Treatment of asthma : Avoiding allergens. Hyposensitization :Subcutaneous injections of inially very small, but gradually increasing doses of allergens (desensitization or
Medicine Dr. Kawa Lecture 4 - Treatment of asthma : Avoiding allergens. Hyposensitization :Subcutaneous injections of inially very small, but gradually increasing doses of allergens (desensitization or
Chapter Effects of Smoke on the Respiratory System Part 1 pages
 Chapter 18.1 Effects of Smoke on the Respiratory System Part 1 pages 412-416 ETS (Environmental Tobacco Smoke) Environmental Tobacco Smoke = ETS The smoke exhaled by active smokers. This smoke affects
Chapter 18.1 Effects of Smoke on the Respiratory System Part 1 pages 412-416 ETS (Environmental Tobacco Smoke) Environmental Tobacco Smoke = ETS The smoke exhaled by active smokers. This smoke affects
BRONCHIOLITIS. See also the PSNZ guideline - Wheeze & Chest Infections in infants under 1 year (www.paediatrics.org.nz)
") Definition What is Bronchiolitis? Assessment Management Flow Chart Admission Guidelines Investigations Management Use of Bronchodilators Other treatments Discharge Planning Bronchiolitis & Asthma References
Definition What is Bronchiolitis? Assessment Management Flow Chart Admission Guidelines Investigations Management Use of Bronchodilators Other treatments Discharge Planning Bronchiolitis & Asthma References
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
The RESPIRATORY System. Unit 3 Transportation Systems
 The RESPIRATORY System Unit 3 Transportation Systems The Respiratory System Functions of the Respiratory System Warms, moistens, and filters incoming air Nasal cavity Resonating chambers for speech and
The RESPIRATORY System Unit 3 Transportation Systems The Respiratory System Functions of the Respiratory System Warms, moistens, and filters incoming air Nasal cavity Resonating chambers for speech and
Core Subject Part 4. Identify the principles of approaching the sick patient.
 The Role of The Dental Care Professional During a Medical Emergency: General Dental Council Standards and The Management of The Collapsed Patient Using the ABCDE Approach Aims: Core Subject Part 4 To provide
The Role of The Dental Care Professional During a Medical Emergency: General Dental Council Standards and The Management of The Collapsed Patient Using the ABCDE Approach Aims: Core Subject Part 4 To provide
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Non-invasive Ventilation protocol For COPD
 NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
Acute respiratory emergencies: recognition and management
 Acute respiratory emergencies: recognition and management Dr Ben Creagh-Brown Consultant in Intensive Care and Respiratory Medicine September 2017, Royal College of Psychiatrists Disclosures / conflicts
Acute respiratory emergencies: recognition and management Dr Ben Creagh-Brown Consultant in Intensive Care and Respiratory Medicine September 2017, Royal College of Psychiatrists Disclosures / conflicts
3. Identify the importance in the prehospital setting for the administration of nebulized bronchodilator.
 TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Anatomy Review. Anatomy Review. Respiratory Emergencies CHAPTER 16
 CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review 1 Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons
CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review 1 Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons
Respiratory Emergencies
 CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons for
CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons for
Interpreting Spirometry. Vikki Knowles BSc(Hons) RGN Respiratory Nurse Consultant G & W`CCG
 RGN Respiratory Nurse Consultant G & W`CCG") Interpreting Spirometry Vikki Knowles BSc(Hons) RGN Respiratory Nurse Consultant G & W`CCG Why Spirometry? supports diagnosis classifies defect - obstructive/restrictive assesses -severity of defect -
Interpreting Spirometry Vikki Knowles BSc(Hons) RGN Respiratory Nurse Consultant G & W`CCG Why Spirometry? supports diagnosis classifies defect - obstructive/restrictive assesses -severity of defect -
Respiratory Pharmacology
 Allergy Targets of allergies Type I Histamine Leukotrienes Prostaglandins Bradykinin Hypersensitivity reactions Asthma Characterised by Triggered by Intrinsic Extrinsic (allergic) Mediators Result Early
Allergy Targets of allergies Type I Histamine Leukotrienes Prostaglandins Bradykinin Hypersensitivity reactions Asthma Characterised by Triggered by Intrinsic Extrinsic (allergic) Mediators Result Early
The RESPIRATORY System. Unit 3 Transportation Systems
 The RESPIRATORY System Unit 3 Transportation Systems Functions of the Respiratory System Warm, moisten, and filter incoming air Resonating chambers for speech and sound production Oxygen and Carbon Dioxide
The RESPIRATORY System Unit 3 Transportation Systems Functions of the Respiratory System Warm, moisten, and filter incoming air Resonating chambers for speech and sound production Oxygen and Carbon Dioxide