Guideline on the Management of Asthma in adults SHSCT
|
|
|
- Clarissa Eaton
- 5 years ago
- Views:
Transcription
1 CLINICAL GUIDELINES ID TAG Title: Author: Speciality / Division: Directorate: Management of Asthma in adults Dr A John, Dr J Lindsay Respiratory Medicine/ MUSC Medicine Date Uploaded: 23/11/15 Review Date 30/11/2018 Clinical Guideline ID CG0198 Guideline on the Management of Asthma in adults SHSCT As per British Thoracic Society & Scottish Intercollegiate Guidelines Network British Guideline on the Management of Asthma (October 2014) Global Initiative for Asthma ( Introduction: Asthma is a serious public health problem throughout the world, affecting people of all ages. When uncontrolled, asthma can place severe limits on daily life, and is sometimes fatal. Asthma is a common condition which produces a significant workload for general practice, hospital outpatient clinics and inpatient admissions. It is clear that much of this morbidity relates to poor management particularly the under use of preventative medicine.
2 Asthma is a chronic inflammatory disorder of the airways in which many cells and cellular elements play a role. The chronic inflammation is associated with airway hyper responsiveness that leads to recurrent episodes of wheezing, breathlessness, chest tightness, and coughing, particularly at night or in the early morning. These episodes are usually associated with widespread, but variable, airflow obstruction within the lung that is often reversible either spontaneously or with treatment. Clinical manifestations of asthma can be controlled with appropriate treatment. When asthma is controlled, there should be no more than occasional flare-ups and severe exacerbations should be rare. Although from the perspective of both the patient and society the cost to control asthma seems high, the cost of not treating asthma correctly is even higher. The Global Initiative for Asthma (GINA) defines asthma as a heterogeneous disease, usually characterised by chronic airflow inflammation. It is defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness and cough that vary over time and in intensity, together with variable expiratory airflow limitation. The clinical spectrum of asthma is highly variable, and different cellular patterns have been observed, but the presence of airway inflammation remains a consistent feature. On account of this high variability in inflammation and in symptoms, there is no standardised definition of the asthma phenotype The diagnosis of asthma is a clinical one The absence of a gold standard definition means that it is not possible to make clear evidence based recommendations on how to make a diagnosis of asthma Initial diagnosis should be based on a careful assessment of symptoms and a measure of airflow obstruction. Spirometry is the preferred initial test to assess the presence and severity of airflow obstruction in adults. Clinical Clues to Diagnosis of Asthma More than one of the following symptoms: wheeze, breathlessness, chest tightness and cough, particularly if: symptoms worse at night and in the early morning symptoms in response to exercise, allergen exposure and cold air symptoms after taking aspirin or beta blockers History of atopic disorder Family history of asthma and/or atopic disorder Widespread wheeze heard on auscultation of the chest Otherwise unexplained low FEV1 or PEF (Peak Expiratory Flow) Variability in FEV1 : FEV1 may be reduced when patients are symptomatic or exacerbating Otherwise unexplained peripheral blood eosinophilia (Elevated Fractional Exhaled Nitric Oxide (FeNO) >25parts per billion (ppb). Can aid diagnosis, and is sensitive but not specific use with care). Features that lower the probability of asthma
3 Prominent symptom being dizziness, light-headedness, peripheral tingling Chronic productive cough in the absence of wheeze or breathlessness Repeatedly normal physical examination of chest when symptomatic Voice disturbance Symptoms with colds only Significant smoking history (ie >20 pack-years) Cardiac disease Normal PEF or spirometry when symptomatic* * A normal spirometry when not symptomatic does not exclude the diagnosis of asthma. Repeated measurements of lung function are often more informative than a single assessment.* Fixed airflow obstruction more likely to be COPD, but can occur in the context of chronic asthma. Differential diagnosis of asthma With airflow obstruction COPD Bronchiectasis Inhaled foreign body Obliterative bronchiolitis Lung cancer Sarcoidosis Without airflow obstruction Hyperventilation syndrome Vocal cord dysfunction Rhinitis Gastro-oesophageal reflux Heart failure Pulmonary fibrosis In adults, initial diagnosis should be based on a careful assessment of symptoms and a measure of airflow obstruction. In patients with a high probability of asthma move straight to a trial of treatment. Reserve further testing for those whose response to a trial of treatment is poor. In patients with a low probability of asthma, whose symptoms are thought to be due to an alternative diagnosis, investigate and manage accordingly. Reconsider
4 the diagnosis of asthma in those who do not respond. In patients with an intermediate probability of asthma, the preferred approach is to carry out further investigations, including an explicit trial of treatments for a specified period, before confirming a diagnosis and establishing maintenance treatment. CARE PATHWAY FOR ASTHMA
5 Criteria for specialist referral in adults: Diagnosis unclear
6 Unexpected clinical findings (ie crackles, clubbing, cyanosis, cardiac disease) Unexplained restrictive spirometry Suspected occupational asthma Persistent non-variable breathlessness Monophonic wheeze or stridor Prominent systemic features (myalgia, fever, weight loss) Chronic sputum production CXR shadowing Marked blood eosinophilia (>1 x 109/l) Poor response to asthma treatment Severe asthma exacerbation MONITORING IN PRIMARY CARE Asthma is best monitored in primary care by routine clinical review on atleast an annual basis The factors that should be monitored and recorded include: Symptomatic asthma control: best assessed using directive questions such as the RCP 3 questions, or the Asthma Control Questionnaire or Asthma Control Test, since broad non-specific questions may underestimate symptoms Lung function, assessed by spirometry or by PEF. Reduced lung function compared to previously recorded values may indicate current bronchoconstriction or a long term decline in lung function and should prompt detailed assessment Exacerbations, oral corticosteroid use and time off work or school since last assessment inhaler technique Compliance which can be assessed by reviewing prescription refill frequency bronchodilator reliance which can be assessed by reviewing prescription refill frequency Possession of and use of self management plan/personal action plan Management of Asthma The aim of asthma management is control of the disease. Control of asthma is defined as: no daytime symptoms no night time awakening due to asthma no need for rescue medication no exacerbations no limitations on activity including exercise normal lung function (in practical terms FEV1 and/or PEF >80% predicted or best) with minimal side effects. In clinical practice patients may have different goals and may wish to balance the aims of asthma management against the potential side effects or inconvenience of taking medication necessary to achieve perfect control. Weight reduction is recommended in obese patients with asthma to promote general health and to improve asthma control.
7 In adults the following factors should be monitored and recorded in primary care: symptomatic asthma control lung function assessed by spirometry or by PEF asthma attacks, oral corticosteroid use and time off work or school since last assessment inhaler technique adherence bronchodilator reliance possession of and use of a self management plan/personal action plan. Self-management and education Successful asthma management is more than just prescribing medications to treat symptoms It involves education and explanation empowering the patient to help themselves Self-management education, as part of regular medication review, is recommended in the GINA and BTS/SIGN Asthma Guidelines 1,2 1. GINA. Global initiative for asthma. A pocket guide for asthma management and prevention. Updated British Thoracic Society, Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma: A National Clinical Guideline. Revised Edition April


8 Peak flow monitoring Identifying poor control Deterioration in asthma control
9 Primary care practices should ensure that they have trained professionals and an environment conducive to providing supported self management. Implementation of self-management interventions is challenging in the non-specialist environment of primary care and needs to consider not only specific training in selfmanagement skills, but also the logistics of when and how self management education is incorporated into routine care. Strategies that have been used in effective interventions include:.. the use of proactive triggers to ensure routine reviews.. structured protocols for asthma reviews.. support of community pharmacists.. routine mailing of educational resources.. telephone calls to provide ongoing support and advice.. IT-based education and monitoring.. involvement of community workers to support clinical teams in deprived and/or ethnic minority communities. Good practice points Every asthma consultation is an opportunity to review, reinforce and extend both the patient s knowledge and skills. This is true whether the patient is seen in primary care, the ED or the outpatient clinic. It is important to recognise that education is a process and not a single event. A hospital admission represents a window of opportunity to review selfmanagement skills. No patient should leave hospital without a written personalised asthma action plan.. An acute consultation offers the opportunity to determine what action the patient has already taken to deal with the asthma attack. Their selfmanagement strategy may be reinforced or refined and the need for consolidation at a routine follow up considered.. A consultation for an upper respiratory tract infection or other known trigger is an opportunity to rehearse with the patient their self management in the event of their asthma deteriorating.. Education should include personalised discussion of issues such as trigger avoidance and achieving a smoke-free environment to support people and their families living with asthma.. Brief simple education linked to patient goals is most likely to be acceptable to patients.
10 Classification of Asthma Severity by Clinical Features Before Treatment Mild Intermittent Symptoms less than once a week Brief exacerbations Nocturnal symptoms not more than twice a month FEV1 or PEF = 80% predicted PEF or FEV1 variability < 20% Mild Persistent Symptoms more than once a week but less than once a day Exacerbations may affect activity and sleep Nocturnal symptoms more than twice a month FEV1 or PEF = 80% predicted PEF or FEV1 variability < 20 30% Classification of Asthma Severity by Clinical Features Before Treatment Moderate Persistent Symptoms daily Exacerbations may affect activity and sleep Nocturnal symptoms more than once a week Daily use of inhaled short-acting beta2-agonist FEV1 or PEF 60-80% predicted PEF or FEV1 variability > 30% Severe Persistent Symptoms daily Frequent exacerbations Frequent nocturnal asthma symptoms Limitation of physical activities FEV1 or PEF = 60% predicted PEF or FEV1 variability > 30%

11 STEPWISE ESCALATION & DE-ESCALATION OF TREATMENT OF ASTHMA Summary of step 3: Add-on therapy
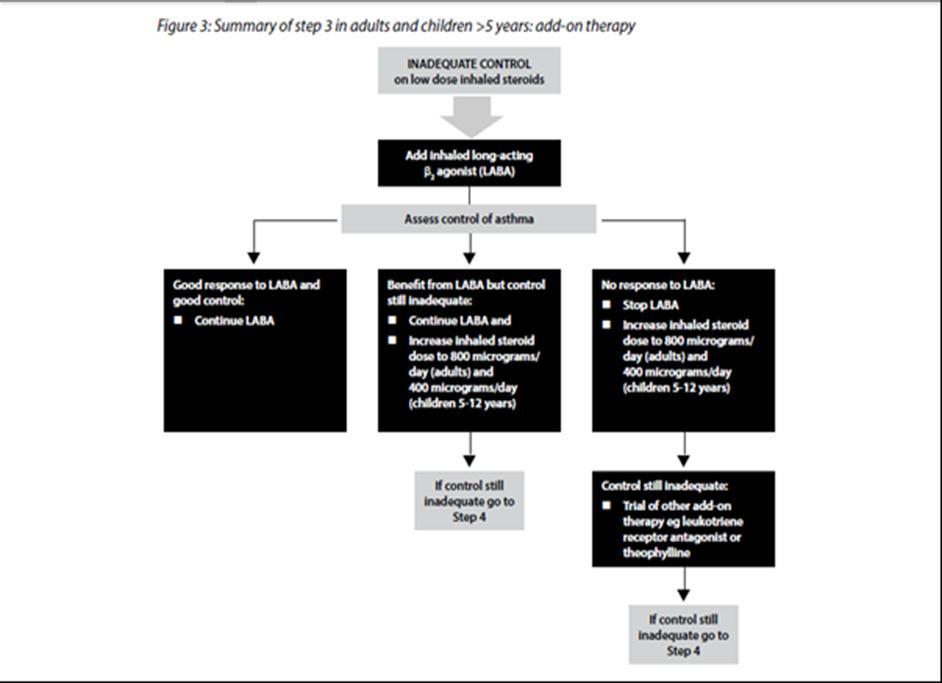
12
13 STEPPING DOWN Is recommended, once asthma control achieved prevents overtreatment no trials to suggest optimal strategy of stepping down Halve steroid dose every 3 months Goal of asthma treatment is to achieve and maintain clinical control
14 GINA :Classification of asthma by levels of control
15

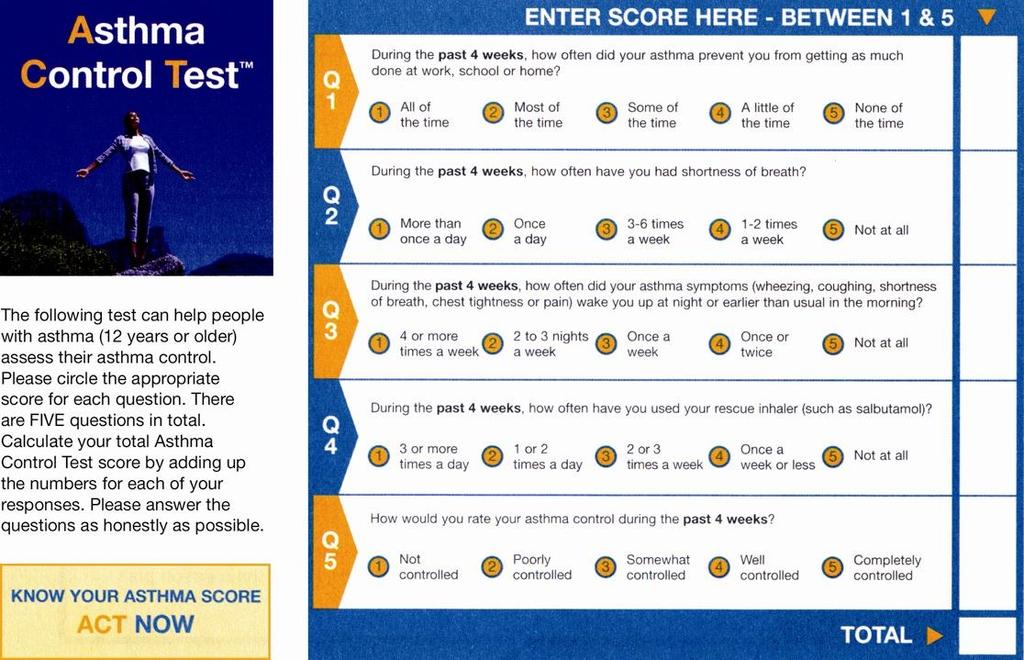
16 The Asthma Control Test TM 2002, by QualityMetric Incorporated. Asthma Control Test is a trademark of QualityMetric Incorporated. "US English version modified for use in UK"
17

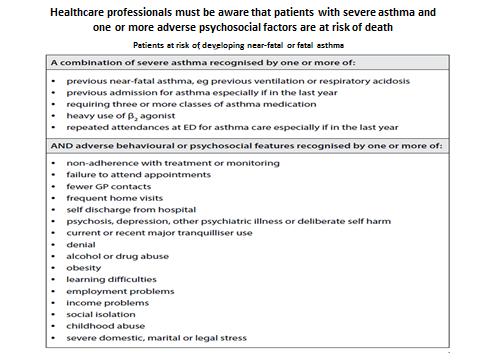
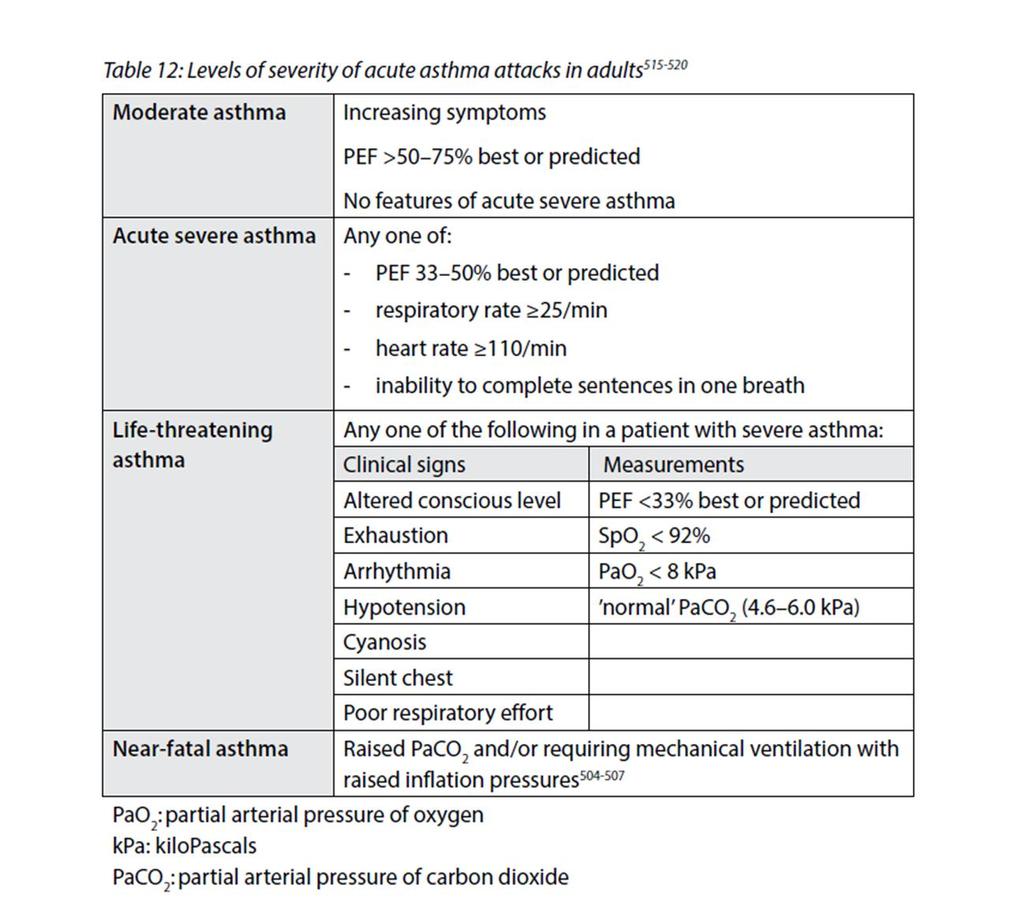
18 Levels of severity of acute asthma exacerbations Patients at risk of developing near-fatal or fatal asthma A COMBINATION OF SEVERE ASTHMA recognised by one or more of: previous near-fatal asthma, eg previous ventilation or respiratory acidosis previous admission for asthma especially if in the last year requiring three or more classes of asthma medication heavy use of β2 agonist repeated attendances at ED for asthma care especially if in the last year brittle asthma.
19 And ADVERSE BEHAVIOURAL OR PSYCHOSOCIAL FEATURES recognised by one or more of: non-compliance with treatment or monitoring failure to attend appointments, self discharge from hospital psychosis, depression, other psychiatric illness or deliberate self harm, current or recent major tranquilliser use denial, alcohol or drug abuse, obesity learning difficulties, social isolation, childhood abuse, severe domestic, marital or legal stress. Initial assessment - the role of symptoms, signs and measurements Clinical features, symptoms and respiratory and cardiovascular signs can identify some patients with severe asthma, eg severe breathlessness (including too breathless to complete sentences in one breath), tachypnea, tachycardia, silent chest, cyanosis or collapse. None of these singly or together is specific and their absence does not exclude a severe attack. PEF or FEV1 Measurements of airway calibre improve recognition of the degree of severity, the appropriateness or intensity of therapy, and decisions about management in hospital or at home. PEF or FEV1 are both useful and valid measures of airway calibre. PEF is more convenient and cheaper. Pulse oximetry Measure oxygen saturation (SpO2) with a pulse oximeter to determine the adequacy of oxygen therapy and the need for arterial blood gas (ABG) measurement. The aim of oxygen therapy is to maintain SpO2 92%. Blood gases (ABG) Patients with SpO2 <92% or other features of life threatening asthma require ABG measurement. Chest X-ray Chest X-ray is not routinely recommended in patients in the absence of: suspected pneumo-mediastinum or pneumothorax suspected consolidation life threatening asthma failure to respond to treatment satisfactorily requirement for ventilation.
20
21 CRITERIA FOR ADMISSION Admit patients with any feature of a life threatening or near-fatal attack. Admit patients with any feature of a severe attack persisting after initial treatment. Patients whose peak flow is greater than 75% best or predicted one hour after initial treatment may be discharged from A&E unless they meet any of the following criteria, when admission may be appropriate: still have significant symptoms concerns about compliance living alone/socially isolated psychological problems physical disability or learning difficulties previous near-fatal or brittle asthma exacerbation despite adequate dose steroid tablets pre-presentation presentation at night pregnancy. REFERRAL TO INTENSIVE CARE Patients who are failing to respond to therapy, as evidenced by: deteriorating PEF persisting or worsening hypoxia hypercapnea arterial blood gas analysis showing fall in ph exhaustion, feeble respiration drowsiness, confusion
22 coma or respiratory arrest NON-INVASIVE VENTILATION.. is Not recommended IF IN DOUBT CHECK WITH SENIOR COLLEAGUES/ CONSULTANT ON CALL. Patients of Bronchial Asthma when discharged from A&E should be instructed to attend their GP within 48 hours. Patients admitted to hospital with acute severe Asthma should have review arrangements in the respiratory clinic. Advise and opinion regarding care of asthmatic patients can also be obtained during working hours from the respiratory consultant or associate specialist or respiratory ST or respiratory nurses at Craigavon Area Hospital or at Daisy Hill Hospital. Disclaimer: Whilst every care has been taken to ensure that the format of this guideline is correct, the Trust can accept no responsibility whatsoever for the actual content of the guideline. Developed by: Dr A John, Consultant Respiratory Physician, SHSCT & Dr J Lindsay, Specialist Trainee, Respiratory Medicine
23
24
25
Pathway diagrams Annex F
 Pathway diagrams Annex F Fig 1 Asthma: The patient journey Asthma is diagnosed Making the diagnosis of asthma Confirming the diagnosis may depend on history, response to treatment, measurement of airflow
Pathway diagrams Annex F Fig 1 Asthma: The patient journey Asthma is diagnosed Making the diagnosis of asthma Confirming the diagnosis may depend on history, response to treatment, measurement of airflow
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1
 ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016
 Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
British Guideline on the Management of Asthma
 British Thoracic Society Scottish Intercollegiate Guidelines Network British Guideline on the Management of Asthma A national clinical guideline The College of Emergency Medicine May 2008 BRITISH GUIDELINE
British Thoracic Society Scottish Intercollegiate Guidelines Network British Guideline on the Management of Asthma A national clinical guideline The College of Emergency Medicine May 2008 BRITISH GUIDELINE
Allwin Mercer Dr Andrew Zurek
 Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Update on management of respiratory symptoms. Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT
 Update on management of respiratory symptoms Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT Topics The common respiratory symptoms Cough: causes, diagnosis and therapy Update
Update on management of respiratory symptoms Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT Topics The common respiratory symptoms Cough: causes, diagnosis and therapy Update
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Title Protocol for the Management of Asthma
 Document Control Title Protocol for the Management of Asthma Author Author s job title Professional Lead, Minor Injuries Unit Directorate Emergency Services, Logistics and Resilience Department Version
Document Control Title Protocol for the Management of Asthma Author Author s job title Professional Lead, Minor Injuries Unit Directorate Emergency Services, Logistics and Resilience Department Version
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
Clinical Practice Guideline: Asthma
 Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong
 Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma: diagnosis and monitoring
 Asthma: diagnosis and monitoring NICE guideline: short version Draft for second consultation, July 01 This guideline covers assessing, diagnosing and monitoring suspected or confirmed asthma in adults,
Asthma: diagnosis and monitoring NICE guideline: short version Draft for second consultation, July 01 This guideline covers assessing, diagnosing and monitoring suspected or confirmed asthma in adults,
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
(Asthma) Diagnosis, monitoring and chronic asthma management
 Diagnosis, monitoring and chronic asthma management") Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL
 DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
REFERRAL GUIDELINES RESPIRATORY
 REFERRAL GUIDELINES RESPIRATORY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
REFERRAL GUIDELINES RESPIRATORY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
Diagnostics Assessment Programme. Measurement of exhaled nitric oxide concentration in asthma; NIOX MINO and NObreath. Final scope
 Diagnostics Assessment Programme Measurement of exhaled nitric oxide concentration in asthma; NIOX MINO and NObreath Final scope February 2013 1. Introduction The Medical Technologies Advisory Committee
Diagnostics Assessment Programme Measurement of exhaled nitric oxide concentration in asthma; NIOX MINO and NObreath Final scope February 2013 1. Introduction The Medical Technologies Advisory Committee
PCRS-UK briefing document Asthma guidelines. November 2017
 PCRS-UK briefing document Asthma guidelines November 2017 1 1. Background The Scottish Intercollegiate Guidelines Network (SIGN) and British Thoracic Society (BTS) have been collaborating on producing
PCRS-UK briefing document Asthma guidelines November 2017 1 1. Background The Scottish Intercollegiate Guidelines Network (SIGN) and British Thoracic Society (BTS) have been collaborating on producing
National Asthma Educator Certification Board Detailed Content Outline
 I. THE ASTHMA CONDITION 9 20 1 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
I. THE ASTHMA CONDITION 9 20 1 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
Commissioning for Better Outcomes in COPD
 Commissioning for Better Outcomes in COPD Dr Matt Kearney Primary Care & Public Health Advisor Respiratory Programme, Department of Health General Practitioner, Runcorn November 2011 What are the Commissioning
Commissioning for Better Outcomes in COPD Dr Matt Kearney Primary Care & Public Health Advisor Respiratory Programme, Department of Health General Practitioner, Runcorn November 2011 What are the Commissioning
Public Dissemination
 1. THE ASTHMA CONDITION 9 18 3 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
1. THE ASTHMA CONDITION 9 18 3 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS
 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Recommendation PULMONARY FUNCTION TESTING (SPIROMETRY) Conditional: The Expert Panel that spirometry measurements FEV1,
TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Recommendation PULMONARY FUNCTION TESTING (SPIROMETRY) Conditional: The Expert Panel that spirometry measurements FEV1,
How to distinguish between uncontrolled and severe asthma
 How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
Life-long asthma and its relationship to COPD. Stephen T Holgate School of Medicine University of Southampton
 Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ
 Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
In 2002, it was reported that 72 of 1000
 REPORTS Aligning Patient Care and Asthma Treatment Guidelines Eric Cannon, PharmD Abstract This article describes how the National Asthma Education and Prevention Program Guidelines for the Diagnosis and
REPORTS Aligning Patient Care and Asthma Treatment Guidelines Eric Cannon, PharmD Abstract This article describes how the National Asthma Education and Prevention Program Guidelines for the Diagnosis and
7/7/2015. Somboon Chansakulporn, MD. History of variable respiratory symptoms. 1. Documented excessive variability in PFT ( 1 test)
") Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
ASTHMA. Dr Liz Gamble BRI
 ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
Exacerbations. Ronald Dahl, Aarhus University Hospital, Denmark
 1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
GUIDELINES LET S TALK ABOUT THE ASTHMA ...MADE MORE PRACTICAL GUIDELINES FOR PRACTICE...
 LET S TALK ABOUT THE ASTHMA GUIDELINES GUIDELINES FOR PRACTICE......MADE MORE PRACTICAL NICE quality standard QOF asthma indicators BTS/SIGN guidelines Provided as a service to medicine by Teva UK Limited.
LET S TALK ABOUT THE ASTHMA GUIDELINES GUIDELINES FOR PRACTICE......MADE MORE PRACTICAL NICE quality standard QOF asthma indicators BTS/SIGN guidelines Provided as a service to medicine by Teva UK Limited.
Some Facts About Asthma
 Some Facts About Asthma Contents What is asthma? Diagnosing asthma Asthma symptoms Asthma triggers Thanks What is asthma?? Asthma is a chronic lung-disease that inflames and narrows the airways (tubes
Some Facts About Asthma Contents What is asthma? Diagnosing asthma Asthma symptoms Asthma triggers Thanks What is asthma?? Asthma is a chronic lung-disease that inflames and narrows the airways (tubes
Anyone who smokes and/or has shortness of breath and sputum production could have COPD
 COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
Management of acute asthma in children in emergency department. Moderate asthma
 152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
patient group direction
 SALBUTAMOL v01 1/12 SALBUTAMOL PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner
SALBUTAMOL v01 1/12 SALBUTAMOL PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner
This is a cross-sectional analysis of the National Health and Nutrition Examination
 SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
Referring for specialist respiratory input. Dr Melissa Heightman Consultant respiratory physician, UCLH,WH, CNWL
 Referring for specialist respiratory input Dr Melissa Heightman Consultant respiratory physician, UCLH,WH, CNWL Respiratory Specialist- who? GPSI Community Team Secondary Care Respiratory physician and
Referring for specialist respiratory input Dr Melissa Heightman Consultant respiratory physician, UCLH,WH, CNWL Respiratory Specialist- who? GPSI Community Team Secondary Care Respiratory physician and
Bronchospasm & SOB. Kim Kilmurray Senior Clinical Teaching Fellow
 Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
Asthma: Chronic Management. Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015
 Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER
 MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
ASTHMA RESOURCE PACK Section 3. Chronic Cough Guidelines
 ASTHMA RESOURCE PACK Section 3 Chronic Cough Guidelines NHS Fife Guidelines for the Management of Chronic Cough in Adults In this section: 1. Introduction 2. Scope Guidelines for Management of Chronic
ASTHMA RESOURCE PACK Section 3 Chronic Cough Guidelines NHS Fife Guidelines for the Management of Chronic Cough in Adults In this section: 1. Introduction 2. Scope Guidelines for Management of Chronic
Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Managing Exacerbations of COPD (Version 3.0)
") Managing Exacerbations of COPD (Version 3.0) Guideline Readership This guideline is intended for use in patients with a confirmed diagnosis of a chronic obstructive pulmonary disease (COPD) exacerbation.
Managing Exacerbations of COPD (Version 3.0) Guideline Readership This guideline is intended for use in patients with a confirmed diagnosis of a chronic obstructive pulmonary disease (COPD) exacerbation.
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
Administration of Short-Acting Beta-agonists for Acute Episodes of Moderate or Severe Asthma by Practice Nurses
 1. Clinical Condition or situation to which this Patient Group Direction applies Definition of clinical condition/situation Adults and children aged 2 years and above presenting with increasing symptoms
1. Clinical Condition or situation to which this Patient Group Direction applies Definition of clinical condition/situation Adults and children aged 2 years and above presenting with increasing symptoms
NG80. Asthma: diagnosis, monitoring and chronic asthma management (NG80)
") Asthma: diagnosis, monitoring and chronic asthma management (NG80) NG80 NICE has checked the use of its content in this product and the sponsor has had no influence on the content of this booklet. NICE
Asthma: diagnosis, monitoring and chronic asthma management (NG80) NG80 NICE has checked the use of its content in this product and the sponsor has had no influence on the content of this booklet. NICE
Presented by the California Academy of Family Physicians 2013/California Academy of Family Physicians
 Family Medicine and Patient-Centered Asthma Care Presented by the California Academy of Family Physicians Faculty: Hobart Lee, MD Disclosures: Jeffrey Luther, MD, Program Director, Memorial Family Medicine
Family Medicine and Patient-Centered Asthma Care Presented by the California Academy of Family Physicians Faculty: Hobart Lee, MD Disclosures: Jeffrey Luther, MD, Program Director, Memorial Family Medicine
Optimising the management of wheeze in preschool children
 Optimising the management of wheeze in preschool children McVea S, Bourke T. Optimising the management of wheeze in preschool children. Practitioner 2016;260(1794):11-14 Dr Steven McVea MB BCh BAO MRCPCH
Optimising the management of wheeze in preschool children McVea S, Bourke T. Optimising the management of wheeze in preschool children. Practitioner 2016;260(1794):11-14 Dr Steven McVea MB BCh BAO MRCPCH
What s new in Asthma? Dr Alexandra Nanzer-Kelly Consultant Respiratory Physician Royal Brompton and Harefield Hospitals
 What s new in Asthma? Dr Alexandra Nanzer-Kelly Consultant Respiratory Physician Royal Brompton and Harefield Hospitals Asthma is an inflammatory disease Relaxed smooth muscles Air trapped in alveoli Tightened
What s new in Asthma? Dr Alexandra Nanzer-Kelly Consultant Respiratory Physician Royal Brompton and Harefield Hospitals Asthma is an inflammatory disease Relaxed smooth muscles Air trapped in alveoli Tightened
Asthma Assessment & Review
 ASTHMA RESOURCE PACK Section 5B Asthma Assessment & Review In this section: 1. Primary Care initial assessment and review Asthma Resource Pack Section 5B: Asthma Assessment & Review Version 3.0 Last Updated:
ASTHMA RESOURCE PACK Section 5B Asthma Assessment & Review In this section: 1. Primary Care initial assessment and review Asthma Resource Pack Section 5B: Asthma Assessment & Review Version 3.0 Last Updated:
Get Healthy Stay Healthy
 Asthma Management WHAT IS ASTHMA? Asthma causes swelling and inflammation in the breathing passages that lead to your lungs. When asthma flares up, the airways tighten and become narrower. This keeps the
Asthma Management WHAT IS ASTHMA? Asthma causes swelling and inflammation in the breathing passages that lead to your lungs. When asthma flares up, the airways tighten and become narrower. This keeps the
Managing adults with asthma in primary care: the four-stage consultation
 Respiratory conditions Managing adults with asthma in primary care: the four-stage consultation Key practice points: A four-stage consultation is recommended as a framework for managing patients with asthma
Respiratory conditions Managing adults with asthma in primary care: the four-stage consultation Key practice points: A four-stage consultation is recommended as a framework for managing patients with asthma
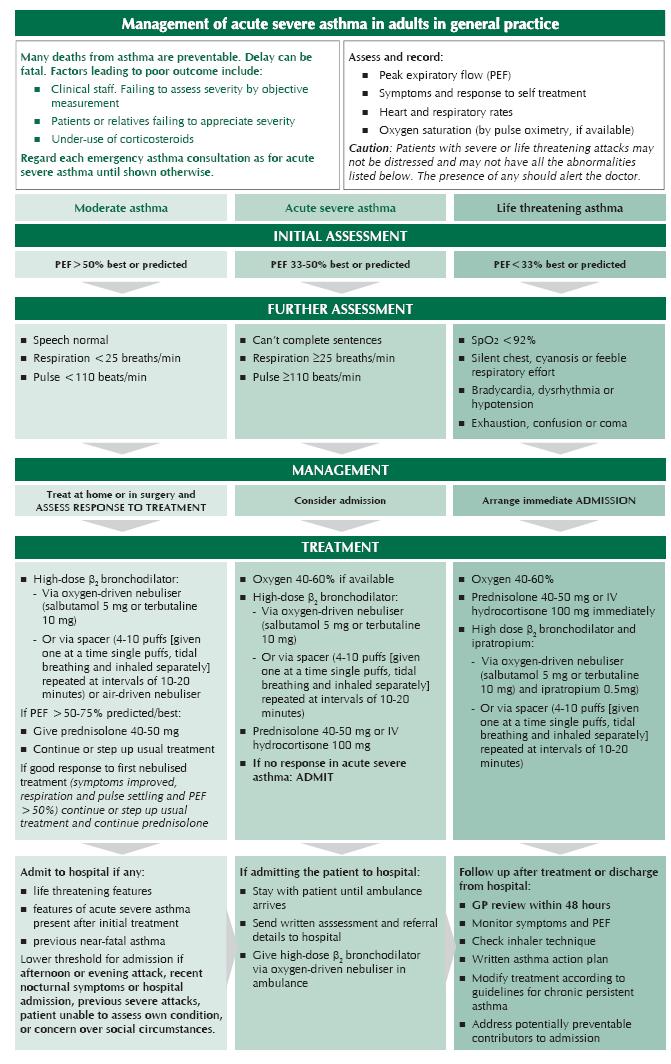
Management of acute severe asthma in adults in general practice. Moderate asthma Acute severe asthma Life-threatening asthma INITIAL ASSESSMENT
 British guideline on the management of asthma Annex 2 Management of acute severe asthma in adults in general practice Many deaths from asthma are preventable. Delay can be fatal. Factors leading to poor
British guideline on the management of asthma Annex 2 Management of acute severe asthma in adults in general practice Many deaths from asthma are preventable. Delay can be fatal. Factors leading to poor
P01. Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) P01 Guideline for Peak flow recording
 P01 Guideline for Peak flow recording") Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Guideline for Peak flow recording Caroline Youle,
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Guideline for Peak flow recording Caroline Youle,
Asthma. chapter 7. Overview
 chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
Chronic Obstructive Pulmonary Disease. Information about medication and an Action Plan to use if your condition gets worse due to an infection
 Chronic Obstructive Pulmonary Disease Information about medication and an Action Plan to use if your condition gets worse due to an infection Information about your medication Your usual treatment Inhalers
Chronic Obstructive Pulmonary Disease Information about medication and an Action Plan to use if your condition gets worse due to an infection Information about your medication Your usual treatment Inhalers
Asthma Update A/Prof. John Abisheganaden. Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital
 Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Wheeze. Respiratory Tract Symptoms. Prof RJ Green Department of Paediatrics. Cough. Wheeze/noisy breathing. Acute. Tight chest. Shortness of breath
 Wheeze Prof RJ Green Department of Paediatrics Respiratory Tract Symptoms Cough Tight chest Wheeze/noisy breathing Shortness of breath Acute Chronic Respiratory rate Most important sign of respiratory
Wheeze Prof RJ Green Department of Paediatrics Respiratory Tract Symptoms Cough Tight chest Wheeze/noisy breathing Shortness of breath Acute Chronic Respiratory rate Most important sign of respiratory
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
Diagnosis, Treatment and Management of Asthma
 Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Function of the Respiratory System. Exchange CO2 (on expiration) for O2 (on inspiration)
 for O2 (on inspiration)") Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Asthma 2015: Establishing and Maintaining Control
 Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Outpatient Guideline for the Diagnosis and Management of Asthma
 Outpatient Guideline for the Diagnosis and Management of Asthma Initial Visit Follow-Up Visits See page 2 Asthma Diagnosis See page 3 Classifying Asthma Severity and Initiating Treatment See pages 2 and
Outpatient Guideline for the Diagnosis and Management of Asthma Initial Visit Follow-Up Visits See page 2 Asthma Diagnosis See page 3 Classifying Asthma Severity and Initiating Treatment See pages 2 and
Asthma - An update BTS Asthma Guidelines 2016
 Asthma - An update BTS Asthma Guidelines 2016 Dr Ian Clifton Overview Diagnosis Supported self-management Non-pharmacological management Drugs / inhaled therapy Difficult asthma services Case discussions
Asthma - An update BTS Asthma Guidelines 2016 Dr Ian Clifton Overview Diagnosis Supported self-management Non-pharmacological management Drugs / inhaled therapy Difficult asthma services Case discussions
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Chronic Obstructive Pulmonary Disease (COPD)
") James Paget University Hospitals NHS Foundation Trust Great Yarmouth and Waveney Clinical Commissioning Group HealthEast Chronic Obstructive Pulmonary Disease (COPD) Information and Advice for Patients
James Paget University Hospitals NHS Foundation Trust Great Yarmouth and Waveney Clinical Commissioning Group HealthEast Chronic Obstructive Pulmonary Disease (COPD) Information and Advice for Patients
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic Cough. Dr Peter George Consultant Respiratory Physician Royal Brompton and Harefield Hospitals
 Chronic Cough Dr Peter George Consultant Respiratory Physician Royal Brompton and Harefield Hospitals Overview Common causes of chronic cough Important diagnoses not to miss How to investigate a cough
Chronic Cough Dr Peter George Consultant Respiratory Physician Royal Brompton and Harefield Hospitals Overview Common causes of chronic cough Important diagnoses not to miss How to investigate a cough
Bronchial asthma. E. Cserháti 1 st Department of Paediatrics. Lecture for english speaking students 5 February 2013
 Bronchial asthma E. Cserháti 1 st Department of Paediatrics Lecture for english speaking students 5 February 2013 Epidemiology of childhood bronchial asthma Worldwide prevalence of 7-8 and 13-14 years
Bronchial asthma E. Cserháti 1 st Department of Paediatrics Lecture for english speaking students 5 February 2013 Epidemiology of childhood bronchial asthma Worldwide prevalence of 7-8 and 13-14 years
Air Flow Limitation. In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation.
 Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
The Asthma Guidelines: Diagnosis and Assessment of Asthma
 The Asthma Guidelines: Diagnosis and Assessment of Asthma Christopher H. Fanta, M.D. Partners Asthma Center Brigham and Women s Hospital Harvard Medical School Objectives Know how the diagnosis of asthma
The Asthma Guidelines: Diagnosis and Assessment of Asthma Christopher H. Fanta, M.D. Partners Asthma Center Brigham and Women s Hospital Harvard Medical School Objectives Know how the diagnosis of asthma
Chronic Obstructive Pulmonary Disease (COPD) Measures Document
 Measures Document") Chronic Obstructive Pulmonary Disease (COPD) Measures Document COPD Version: 3 - covering patients discharged between 01/10/2017 and present. Programme Lead: Jo Higgins Clinical Lead: Dr Paul Albert Number
Chronic Obstructive Pulmonary Disease (COPD) Measures Document COPD Version: 3 - covering patients discharged between 01/10/2017 and present. Programme Lead: Jo Higgins Clinical Lead: Dr Paul Albert Number
Improving the Management of Asthma to Improve Patient Adherence and Outcomes
 Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
SCREENING AND PREVENTION
 These protocols are designed to implement standard guidelines, based on the best evidence, that provide a consistent clinical experience for AHC II Integrated Clinical Delivery Network patients and allow
These protocols are designed to implement standard guidelines, based on the best evidence, that provide a consistent clinical experience for AHC II Integrated Clinical Delivery Network patients and allow
Over the last several years various national and
 Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Tips on managing asthma in children
 Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
WEBINAR. Difficult-to-treat and severe asthma: changing the paradigm
 WEBINAR Difficult-to-treat and severe asthma: changing the paradigm A multidisciplinary discussion on new therapies, and how to identify and manage difficult-to-treat and severe asthma DIFFICULT-TO-TREAT
WEBINAR Difficult-to-treat and severe asthma: changing the paradigm A multidisciplinary discussion on new therapies, and how to identify and manage difficult-to-treat and severe asthma DIFFICULT-TO-TREAT
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Pulmonary
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Pulmonary 1. GOAL: Diagnose and manage patients with asthma. 2. GOAL: Understand the role of the pediatrician in preventing
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Pulmonary 1. GOAL: Diagnose and manage patients with asthma. 2. GOAL: Understand the role of the pediatrician in preventing
Asthma training. Mike Levin Division of Asthma and Allergy Red Cross Hospital
 Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Significance. Asthma Definition. Focus on Asthma
 Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Global Initiative for Asthma (GINA) What s new in GINA 2016?
 What s new in GINA 2016?") Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD
 Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
CLINICAL PATHWAY. Acute Medicine. Chronic Obstructive Pulmonary Disease
 CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
Asthma: Evaluate and Improve Your Practice
 Potential Barriers and Suggested Ideas for Change Key Activity: Initial assessment and management Rationale: The history and physical examination obtained from the patient and family interviews form the
Potential Barriers and Suggested Ideas for Change Key Activity: Initial assessment and management Rationale: The history and physical examination obtained from the patient and family interviews form the
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
CHALLENGES OF REAL LIFE ASTHMA MANAGEMENT. Dr Chris Lewis Respiratory Physician and Director of Prevocational Training Auckland District Health Board
 CHALLENGES OF REAL LIFE ASTHMA MANAGEMENT Dr Chris Lewis Respiratory Physician and Director of Prevocational Training Auckland District Health Board CONFLICT OF INTEREST Employee of Auckland District Health
CHALLENGES OF REAL LIFE ASTHMA MANAGEMENT Dr Chris Lewis Respiratory Physician and Director of Prevocational Training Auckland District Health Board CONFLICT OF INTEREST Employee of Auckland District Health
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al.
 Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma