Participant Objectives. Airway Anatomy. Airway Anatomy. Airway Anatomy: Pediatric Considerations. Airway Anatomy: Pediatric Considerations
|
|
|
- Brianne Willis
- 5 years ago
- Views:
Transcription


1 Common Pediatric Respiratory Emergencies NAPNAP Chicago Session 314 Wednesday, March 21, 2018 Participant Objectives Discuss upper airway illness in the pediatric population Discuss lower airway illness in the pediatric population Discuss the acute obstructive process and intervention Discuss the management of respiratory distress Valarie Eichler, MSN, RN, CPNP-AC/PC Pediatric Nurse Practitioner Critical Care Services Children s Health Children s Medical Center Dallas Airway Anatomy Upper Airway Supraglottic Nose, nasopharynx, epiglottis Glottis Airway Anatomy Vocal cords, subglottic region, cervical trachea Lower Airway Intrathoracic Thoracic trachea, mainstem bronchi, lungs Airway Anatomy: Pediatric Considerations Large occiput Small mouth and large tongue Anterior Infants are obligatory nose breathers until around 5-6 months of age Narrow passages leads to increased airway resistance Airway Anatomy: Pediatric Considerations Right mainstem slightly larger than the left and angles in a more vertical position Distal airway is less developed and smaller Distal bronchioles continue to branch in the first year of life Alveoli continue to multiply in number and size through ~8 years of life Crichoid ring is the narrowest portion in infants and children 1
 Retropharyngeal Abscess Peritonsilar Abscess")
2 Pediatric vs Adult Airway Anatomy Airway Anatomy: Adult Considerations Longer mainstem bronchus Posterior Teeth Larger mouth General Assessment General appearance Color Work of breathing Respiratory rate Breath sounds Use of accessory muscles Pulse oximetry Infectious Etiologies of the Upper Airway Upper Airway Croup (Laryngotracheobronchitis) Retropharyngeal Abscess Peritonsilar Abscess Epiglottitis Viruses Upper Airway Viral Conditions RSV Rhinovirus/Enterovirus Parainfluenza Human Metapneumovirus Influenza A/B Adenovirus Pertussis 2

3 Croup: Presentation Barky or brassy cough Inspiratory stridor Stertor Retractions Persistent low grade fever Worsens at night and on day 2 3 Steeple Sign on PA/AP xray Croup Inflammation & Edema Croup: Pathophysiology Cellular infiltration of Lymphocytes, histocytes & neutrophils Endothelial damage Loss of ciliary function Mucus plugging Vocal Cord Edema Further contributes to the hoarseness VQ mismatch Hypoxemia Croup: Etiology & Epidemiology Generally viral in nature Parainfluenza Adenovirus RSV Peak season is usually late fall to early winter but can present year round Peak age 6 mo 36mo Rare after 5 6 yrs but can be seen in adolescents and adults Affects males slightly more than females 1.4:1 Dexamethasone Single dose (outpatient) 24hr dose (inpatient) Racemic Epinephrine Cool mist Croup: Management Retropharyngeal Abscess: Presentation Fever Sore throat Pain isolated to one side Dysphagia Tracheal deviation +/ Generalized edema Palpable fluctuant mass +/ Trismus Drooling Stridor Muffled voice 3




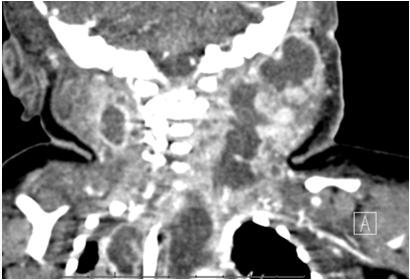
4 Retropharyngeal Abscess: Presentation History is important Retropharyngeal Abscess: Radiographically AP/PA film may see deviated trachea Recent prior intubation Trauma from foreign object in the oral cavity Dental procedures Recent infections Retropharyngeal Abscess: Radiographically Retropharyngeal Abscess: Radiographically Shifted mediastinal structures Retropharyngeal Abscess: Radiographically Retropharyngeal Abscess: Radiographically 4




5 Retropharyngeal Abscess: Radiographically Retropharyngeal Abscess: Radiographic Presentation Retropharyngeal Abscess: Radiographically Retropharyngeal Abscess: Epidemiology/Etiology Commonly bacterial H. Flu Strep Pneumoniae & Pyogenes Staph Aureus Often seen in toddlers & children ages 1 5 Retropharyngeal Abscess: Evaluation CBC w/diff Blood culture Inflammatory markers Plain films CT w/contrast Retropharyngeal Abscess: Management Do not upset or stimulate child Let them assume position of comfort Airway person should be your most experienced Empiric IV antibiotics May need surgical drainage Monitored in the PICU 5

6 Peri or in front of tonsils Peritonsillar Abscess Presents much like retropharyngeal abscess Local pain Sore throat, Trismus Difficulty swallowing Muffled voice Deviated uvula to unaffected side Peritonsillar Abscess Most common cause: GAS Can by associated with other bacteria and/or EBV More common in older children and adolescents Rarely causes UAW obstruction May have recent h/o pharyngitis Ominous signs: Drooling Tripod position CBC w/diff Peritonsillar Abscess: Evaluation Inflammatory markers Blood culture Throat culture Tissue/fluid culture if I&D performed CT neck with contrast Peritonsilar Abscess: Management Do not upset or stimulate child Let them assume position of comfort Airway person should be your most experienced Empiric IV antibiotics May need surgical drainage Monitored in the PICU Sudden onset Severe sore throat Toxic child Dysphagia Fever Agitation Epiglottitis: Presentation Thumb Sign on lateral xray Epiglottitis Can rapidly progress to total UAW obstruction Tripod position Drooling Muffled voice Stridor 6
7 Epiglottitis: Epidemiology/Etiology Epiglottitis: Management Toddler to child age group, 1 5 yrs Usually bacterial H. Flu Strep Pneumoniae Staph Aureus GAS Do not upset or stimulate child Let them assume position of comfort Immediate consult to ENT and/or anesthesia Airway person should be your most experienced Establish IV and obtain blood culture and labs Empiric IV antibiotics 7 10 days Steroids +/ Monitored in the PICU Viral Conditions: Presentation Infectious Etiologies of the Lower Airway Cough Inspiratory stridor +/ Stertor Retractions (depending on the degree of distress) Wheezing +/ Fever Tachycardia Tachypnea Toxic appearing Increased nasal secretions Hypoxia Viral Conditions: Presentation May exacerbate underlying pulmonary disease such as: Asthma Pulmonary Hypertension Laryngomalacia Tracheomalacia Tracheal Stenosis Vocal Cord Paralysis Rings/Slings TEF Chronic Lung Disease Viral Conditions: Presentation May exacerbate underlying cardiac or neuromuscular disease such as: Myocarditis Duchene's MD SMA Congenital heart disease Restrictive lung disease 7

8 Viral Conditions: Pathophysiology Respiratory Syncytial Virus (RSV) Leading cause of lower respiratory tract infections in the infant and young child populations. Actually begins in the UAW Virus attaches to the epithelial cells of the respiratory tract Cell to cell transfer via intracytoplasmic bridges called syncytia into the lower respiratory tract Often accompanied by secondary bacterial or super infection Viral Conditions: Etiology and Epidemiology Respiratory Syncytial Virus (RSV) Daycare Older siblings that attends school Cigarette smoke exposure Prematurity and multiple births Associated with bronchiolitis and viral pneumonia Peak incidence: 2 8 months 4 5 million cases in children <4 yrs of age in the US alone >125K admissions per year Viral Conditions: Evaluation Viral Conditions: General Management RSV Peribronchial Cuffing Usually supportative care Bronchodilators Steroids +/- Respiratory support (non-invasive) Heated high flow NC BIPAP CPAP Viral Conditions: RSV Management Ribavirin extreme conditions RSV IVIG no longer available Palivizumab for prophylaxis No vaccine available Status Asthmaticus: Presentation Wheezing No wheezes ominous sign Retractions Intercostal Suprasternal Subcostal Prolonged expiratory phase Nasal flaring Anxious Hypoxic 8

 Heliox (controversial) Aminophylline drip Ketamine drip")


9 Status Asthmaticus: Status Asthmaticus: Stepwise Management Supplemental O2 Stacked inhaled bronchodilators Prednisone or Methylprednisolone Continuous inhaled bronchodilators MgSO4 as bolus Terbutaline (controversial) Heliox (controversial) Aminophylline drip Ketamine drip Pulmonary consult Status Asthmaticus: Stepwise Management Status Asthmaticus: Stepwise Management Noninvasive ventilation Heated High Flow Nasal Cannula BiPAP Intubation and mechanical ventilation as a last resort Inhaled anesthetic ECMO Status Asthmaticus: Stepwise Management Status Asthmaticus: Stepwise Management 9


10 Status Asthmaticus: Pathophysiology Status Asthmaticus: Pathophysiology Bronchospasm Bronchoconstriction Airway edema Increased mucus production/secretion Cellular infiltration of the airway walls, esp eosinophils Cytokine release inflammatory response Epithelial injury to the airway Status Asthmaticus: Etiology Status Asthmaticus: Epidemiology Genetics IgE mediated allergens Food/nuts Pet dander Environmental factors Tree/grass pollens Smoke Cockroach feces and saliva Peak age: 6 mo to 3 years Slightly higher predominance in males to females Status Asthmaticus: Discharge Planning Foreign Body Aspiration: Partial Obstruction Asthma Action Plan Required by Joint Commission for hospital discharge Environmental controls Algorithm for use of long term and rescue medications Medication regimens and rescue meds Plan of action when treatment is not effective When to seek emergent care Can be UAW or LAW positioning Esophageal positioning Not usually life threatening but causes respiratory distress 10


11 Foreign Body Aspiration Foreign Body Aspiration: Complete Obstruction Foreign Body Toddler age Infant with older sibling Acute cough Sudden onset of choking Difficulty breathing Cyanosis Severe wheezing Stridor Inspiratory films ENT consult DLB Caution with transport, as object could progress and obstruct airway. Surgical emergency for bronchoscopy in the OR. However children with UAW foreign bodies and esophageal foreign bodies that are compressing the airway are more likely to develop acute life threatening respiratory failure They tend to move and completely obstruct Or erode and perforate LAW FBA will have unilateral wheezing Roach aspiration Foreign Body Aspiration If there was significant UAW obstruction there is an increased risk of Post Obstructive Pulmonary Edema Negative Pressure Capillary leak Obstruction relieved Frothy pink secretions Facial edema Urticaria N/V Abdominal pain Altered LOC Syncope Wheezing Anxious SOB Hypotension Shock Anaphylaxis: Presentation Anaphylaxis Most common causes are food allergies and medications Dye or contrast also a common offender May be severe life threatening events Usually happens ~1 hour after exposure but can be within a few minutes 11
12 Anaphylaxis: Pathophysiology Edema involving the retropharynx and/or the larynx Bronchospasm Edema of LAW IgE mediated response or direct mast cell activation Leads to massive release of inflammatory factors Cytokine Histamine Prostaglandins Leukotrienes Anaphylaxis: Pathophysiology Target organs include the heart, vasculature, GI tract, lungs and the integumentary Vasodilatation Decreased CO and Coronary Artery perfusion Ischemia Hypotension Shock Anaphylaxis: Management Regardless of MOA treatment is the same ABCs Anaphylaxis: Management Epinephrine IM or SQ (Max single dose child: 0.3mg; adolescent: 0.5mg) May repeat every 5 15 min as needed IV access and fluid bolus(es) Diphenhydramine Albuterol Methylprednisolone Ranitidine Anaphylaxis: Management Benefits of Non-Invasive Ventilation If you are not sure always err on the side of caution. GIVE THE EPI!!!! CPAP & BiPAP Improved hypoxemia Improved gas exchange Augments fatigued respiratory muscles Provides + pressure support CPAP: inspiratory support BiPAP: bi level inspiratory and expiratory support 12
13 Indications for Intubation High 0 2 requirement Impending failure or s/s of exhaustion Failure to adequately ventilate Increasing CO 2 (>50 acutely) Inability to maintain airway Altered LOC &/or GCS <8 Therapeutic hyperventilation Hemodynamic Instability/Acidosis Respiratory depression Summary Many causes of acute respiratory distress and/or failure in the pediatric population Be suspicious Prompt recognition and action is key to successful outcomes Always form a list of differential diagnoses Remember that NIV has side effects as well and should not be taken lightly 13
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
STRIDOR. Respiratory system. Lecture
 STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
Simulation 01: Two Year-Old Child in Respiratory Distress (Croup)
") Simulation 01: Two Year-Old Child in Respiratory Distress (Croup) Flow Chart Opening Scenario 2 year-old child in respiratory distress - assess Section 1 Type: IG audible stridor with insp + exp wheezing;
Simulation 01: Two Year-Old Child in Respiratory Distress (Croup) Flow Chart Opening Scenario 2 year-old child in respiratory distress - assess Section 1 Type: IG audible stridor with insp + exp wheezing;
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction. Nathan Page, MD Pediatrics in the Red Rocks June?
 Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
5/26/10. Upper Airway Emergencies Identify life threatening upper airway infections Recognize and treat anaphylaxis and airway burns in children
 Andi Marmor, MD Assistant Clinical Professor, Pediatrics University of California, San Francisco Upper Airway Emergencies Identify life threatening upper airway infections Recognize and treat anaphylaxis
Andi Marmor, MD Assistant Clinical Professor, Pediatrics University of California, San Francisco Upper Airway Emergencies Identify life threatening upper airway infections Recognize and treat anaphylaxis
PEDIATRIC RESPIRATORY ILLNESS MADE SIMPLE
 Copyright 2012 Joel Berezow, MD and The Pediatrics for Emergency Physicians Network All rights reserved. Duplication in whole or in part, or electronic transmission in any form, is prohibited THE PEDIATRICS
Copyright 2012 Joel Berezow, MD and The Pediatrics for Emergency Physicians Network All rights reserved. Duplication in whole or in part, or electronic transmission in any form, is prohibited THE PEDIATRICS
Simulation 1: Two Year-Old Child in Respiratory Distress
 Simulation 1: Two Year-Old Child in Respiratory Distress Opening Scenario (Links to Section 1) You are the respiratory therapist in a 300 bed community hospital working the evening shift. At 8:30 PM you
Simulation 1: Two Year-Old Child in Respiratory Distress Opening Scenario (Links to Section 1) You are the respiratory therapist in a 300 bed community hospital working the evening shift. At 8:30 PM you
Upper Airway Emergencies
 Upper Airway Emergencies Selena Hariharan, M.D. Assistant Professor of Pediatrics Division of Pediatric Emergency Medicine Cincinnati Children s Hospital Medical Center CASE # 1 A 9 year old boy, previously
Upper Airway Emergencies Selena Hariharan, M.D. Assistant Professor of Pediatrics Division of Pediatric Emergency Medicine Cincinnati Children s Hospital Medical Center CASE # 1 A 9 year old boy, previously
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
Respiratory Management in Pediatrics
 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Transporting Children With Serious Respiratory Illness: A Presentation For Non-Specialty Teams
 Transporting Children With Serious Respiratory Illness: A Presentation For Non-Specialty Teams Laurie Gehrke, R.N., BSN, CPEN, CEN, CMTE Pediatric Transport Team Blank Children s Hospital Des Moines, Iowa
Transporting Children With Serious Respiratory Illness: A Presentation For Non-Specialty Teams Laurie Gehrke, R.N., BSN, CPEN, CEN, CMTE Pediatric Transport Team Blank Children s Hospital Des Moines, Iowa
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis. Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine
 Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Evaluation and Management of Pediatric Stridor
 Evaluation and Management of Pediatric Stridor Pamela Nicklaus, MD FACS Associate Professor Fellowship Director Pediatric Otolaryngology Children s Mercy Hospital and Clinics 2013 Children's 2013 Mercy
Evaluation and Management of Pediatric Stridor Pamela Nicklaus, MD FACS Associate Professor Fellowship Director Pediatric Otolaryngology Children s Mercy Hospital and Clinics 2013 Children's 2013 Mercy
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
Upper Airway Obstruction
 Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Common Pediatric Respiratory Illness and Emergencies
 Common Pediatric Respiratory Illness and Emergencies Rob Cloutier, MD Assistant Professor Emergency Medicine & Pediatrics Oregon Health & Science University Overview Review key differences between pediatric
Common Pediatric Respiratory Illness and Emergencies Rob Cloutier, MD Assistant Professor Emergency Medicine & Pediatrics Oregon Health & Science University Overview Review key differences between pediatric
Function of the Respiratory System. Exchange CO2 (on expiration) for O2 (on inspiration)
 for O2 (on inspiration)") Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Pediatric Airway and Respiratory Emergencies. Objectives 30/01/2009
 Objectives Pediatric Airway and Respiratory Emergencies Patrick Mahar, MD Review the anatomical differences between adult and pediatric airways Recognize different causes of respiratory comprise in pediatric
Objectives Pediatric Airway and Respiratory Emergencies Patrick Mahar, MD Review the anatomical differences between adult and pediatric airways Recognize different causes of respiratory comprise in pediatric
The RESPIRATORY System. Unit 3 Transportation Systems
 The RESPIRATORY System Unit 3 Transportation Systems Functions of the Respiratory System Warm, moisten, and filter incoming air Resonating chambers for speech and sound production Oxygen and Carbon Dioxide
The RESPIRATORY System Unit 3 Transportation Systems Functions of the Respiratory System Warm, moisten, and filter incoming air Resonating chambers for speech and sound production Oxygen and Carbon Dioxide
PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department
 PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department Overview Roles of the EMS in Pediatric Care Growth and Development Assessment Airway Adjuncts and Intravenous Access
PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department Overview Roles of the EMS in Pediatric Care Growth and Development Assessment Airway Adjuncts and Intravenous Access
Video Cases in Pediatrics. Ran Goldman, MD BC Children s Hospital University of British
 Video Cases in Pediatrics Ran Goldman, MD BC Children s Hospital University of British Columbia @Dr_R_Goldman Bronchiolitis Viral infection of the lower respiratory tract characterized by acute inflammation,
Video Cases in Pediatrics Ran Goldman, MD BC Children s Hospital University of British Columbia @Dr_R_Goldman Bronchiolitis Viral infection of the lower respiratory tract characterized by acute inflammation,
PALS Pulseless Arrest Algorithm.
 PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
Infectious Upper Airway Obstruction
 Infectious Upper Airway Obstruction Prof. Muhi K. Al-Janabi MRCPCH; DCH; FICMS Consultant Pediatric Pulmonologist Objectives Viral croup Objectives 1. Know and understand the aetiology and natural history
Infectious Upper Airway Obstruction Prof. Muhi K. Al-Janabi MRCPCH; DCH; FICMS Consultant Pediatric Pulmonologist Objectives Viral croup Objectives 1. Know and understand the aetiology and natural history
The RESPIRATORY System. Unit 3 Transportation Systems
 The RESPIRATORY System Unit 3 Transportation Systems The Respiratory System Functions of the Respiratory System Warms, moistens, and filters incoming air Nasal cavity Resonating chambers for speech and
The RESPIRATORY System Unit 3 Transportation Systems The Respiratory System Functions of the Respiratory System Warms, moistens, and filters incoming air Nasal cavity Resonating chambers for speech and
Acute Laryngitis in Childhood
 Acute Laryngitis in Childhood Hany Simon Junior Viral croup Definition The term croup syndrome characterizes a group of diseases with variable anatomic involvement and etiology, and is clinically manifested
Acute Laryngitis in Childhood Hany Simon Junior Viral croup Definition The term croup syndrome characterizes a group of diseases with variable anatomic involvement and etiology, and is clinically manifested
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Andrea Losier OTTAWA ON 332 PEDS ER CASES Pediatric ED Cases
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Andrea Losier OTTAWA ON 332 PEDS ER CASES Pediatric ED Cases
Firefighter Pre-Hospital Care Program Recruit Presentation. Respiratory Emergencies
 Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
PAEDIATRIC ACUTE CARE GUIDELINE. Croup. This document should be read in conjunction with this DISCLAIMER
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Croup Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Croup Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Management of Respiratory Issues in the School Setting. Pediatric Indicators of High Risk 8/7/2015. Facts about Pediatric Respiratory Failure
 Management of Respiratory Issues in the School Setting Toni B. Vento, MS, RN, NCSN Supervisor of Health Services Medford Public Schools Pediatric Indicators of High Risk Anatomic features of the immature
Management of Respiratory Issues in the School Setting Toni B. Vento, MS, RN, NCSN Supervisor of Health Services Medford Public Schools Pediatric Indicators of High Risk Anatomic features of the immature
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Respiratory distress in children
 Respiratory distress in children Joey Gassen, MD Overview Backgroundand definition First five minutes History and physical exam Key historical features Signs and symptoms Possible causes and differential
Respiratory distress in children Joey Gassen, MD Overview Backgroundand definition First five minutes History and physical exam Key historical features Signs and symptoms Possible causes and differential
Shelley Westwood, RN, BSN
 Shelley Westwood, RN, BSN The body requires a constant supply of oxygen for survival. AMERICAN RED CROSS FIRST AID RESPONDING TO EMERGENCIES FOURTH EDITION Copyright 2006 by The American National Red Cross
Shelley Westwood, RN, BSN The body requires a constant supply of oxygen for survival. AMERICAN RED CROSS FIRST AID RESPONDING TO EMERGENCIES FOURTH EDITION Copyright 2006 by The American National Red Cross
Chapter 15 - Respiratory Emergencies
 1 2 3 4 5 6 7 National EMS Education Standard Competencies (1 of 5) Medicine Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
1 2 3 4 5 6 7 National EMS Education Standard Competencies (1 of 5) Medicine Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
Pediatric Bronchiolitis. Janie Robles, PharmD, AE-C Assistant Professor of Pharmacy Practice Pediatrics School of Pharmacy TTUHSC Lubbock, Texas
 This PowerPoint file is a supplement to the video presentation. Some of the educational content of this program is not available solely through the PowerPoint file. Participants should use all materials
This PowerPoint file is a supplement to the video presentation. Some of the educational content of this program is not available solely through the PowerPoint file. Participants should use all materials
Chapter 13. Respiratory Emergencies
 Chapter 13 Respiratory Emergencies Introduction Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine. Even for physician in
Chapter 13 Respiratory Emergencies Introduction Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine. Even for physician in
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Nursing care for children with respiratory dysfunction
 Nursing care for children with respiratory dysfunction 1 Lung Development Specific Immunity to Respiratory Infection Secretory IgA in mucosal immunity IgG in systemic immunity Risk Factors Associated with
Nursing care for children with respiratory dysfunction 1 Lung Development Specific Immunity to Respiratory Infection Secretory IgA in mucosal immunity IgG in systemic immunity Risk Factors Associated with
Respiratory Emergencies. Lesson Goal. Lesson Objectives 9/10/2012
 Respiratory Emergencies Lesson Goal Assess and provide timely treatment & transport to patients experiencing respiratory emergencies Lesson Objectives List parts of respiratory system and how they work
Respiratory Emergencies Lesson Goal Assess and provide timely treatment & transport to patients experiencing respiratory emergencies Lesson Objectives List parts of respiratory system and how they work
IAEM Clinical Guideline 9 Laryngomalacia. Version 1 September, Author: Dr Farah Mustafa
 IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
Respiratory system. Applied Anatomy &Physiology
 Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER
 MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
Bronchospasm & SOB. Kim Kilmurray Senior Clinical Teaching Fellow
 Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Author(s): Matt Dawson & Zach Sturges (University of Utah) 2008
: Matt Dawson & Zach Sturges (University of Utah) 2008") Project: Ghana Emergency Medicine Collaborative Document Title: ENT Case Files (2008) Author(s): Matt Dawson & Zach Sturges (University of Utah) 2008 License: Unless otherwise noted, this material is made
Project: Ghana Emergency Medicine Collaborative Document Title: ENT Case Files (2008) Author(s): Matt Dawson & Zach Sturges (University of Utah) 2008 License: Unless otherwise noted, this material is made
Pediatric Respiratory Distress. Dr. Karen Forward Dr. Mike Peddle
 Pediatric Respiratory Distress Dr. Karen Forward Dr. Mike Peddle Objectives Discuss epidemiology & causes of respiratory distress in pediatric patients Identify differences between the pediatric and adult
Pediatric Respiratory Distress Dr. Karen Forward Dr. Mike Peddle Objectives Discuss epidemiology & causes of respiratory distress in pediatric patients Identify differences between the pediatric and adult
Croup (Laryngo-tracheo-bronchitis)
") Croup (Laryngo-tracheo-bronchitis) 1a 2a 2b Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of
Croup (Laryngo-tracheo-bronchitis) 1a 2a 2b Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of
Respiratory Distress/Failure - General
 Respiratory Distress/Failure - General Criteria: Dyspnea WITHOUT a clear etiology O 2 V/S and SpO 2 (with and without Oxygen therapy if possible) Blood glucose analysis: if less than 80 mg/dl, refer to
Respiratory Distress/Failure - General Criteria: Dyspnea WITHOUT a clear etiology O 2 V/S and SpO 2 (with and without Oxygen therapy if possible) Blood glucose analysis: if less than 80 mg/dl, refer to
5/5/2013. The Respiratory System. Chapter 16 Notes. The Respiratory System. Nasal Cavity. Sinuses
 The Respiratory System Chapter 16 Notes The Respiratory System Objectives List the general functions of the respiratory system. Identify the organs of the respiratory system. Describe the functions of
The Respiratory System Chapter 16 Notes The Respiratory System Objectives List the general functions of the respiratory system. Identify the organs of the respiratory system. Describe the functions of
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM
 CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM Pages 244-247 DO NOW What structures, do you think, are active participating in the breathing process? 2 WHAT ARE WE DOING IN TODAY S CLASS Finishing Digestion
CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM Pages 244-247 DO NOW What structures, do you think, are active participating in the breathing process? 2 WHAT ARE WE DOING IN TODAY S CLASS Finishing Digestion
Chapter 16. Objectives. Objectives. Respiratory Emergencies
 Chapter 16 Respiratory Emergencies Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key
Chapter 16 Respiratory Emergencies Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key
Pulmonary Emergencies. Lower Airway Structures Trachea Bronchial tree Primary bronchi Secondary bronchi Bronchioles Alveoli Lungs
 Pulmonary Emergencies Lower Airway Structures Trachea Bronchial tree Primary bronchi Secondary bronchi Bronchioles Alveoli Lungs Pulmonary Surfactant Thin film that coats alveoli Prevents alveoli from
Pulmonary Emergencies Lower Airway Structures Trachea Bronchial tree Primary bronchi Secondary bronchi Bronchioles Alveoli Lungs Pulmonary Surfactant Thin film that coats alveoli Prevents alveoli from
Discuss the benefits for developing an outpatient bronchiolitis clinic.
 Diana L Mark, RRT Pediatric Clinical Specialist Respiratory Care Wesley Medical Center Discuss the benefits for developing an outpatient bronchiolitis clinic. 1 Definition Inflammation of the bronchioles
Diana L Mark, RRT Pediatric Clinical Specialist Respiratory Care Wesley Medical Center Discuss the benefits for developing an outpatient bronchiolitis clinic. 1 Definition Inflammation of the bronchioles
Emergency Department Guideline. Anaphylaxis
 Emergency Department Guideline Inclusion criteria: 1. Acute onset of an illness (minutes to hours) with a AND (b OR c): a. Skin and/or mucosa (pruritus, flushing, hives, angioedema) b. Respiratory compromise
Emergency Department Guideline Inclusion criteria: 1. Acute onset of an illness (minutes to hours) with a AND (b OR c): a. Skin and/or mucosa (pruritus, flushing, hives, angioedema) b. Respiratory compromise
Overview of COPD INTRODUCTION
 Overview of COPD INTRODUCTION Chronic obstructive pulmonary disease (COPD) is a common lung disease that affects millions of people, and it is the fourth leading cause of death in the United States. It
Overview of COPD INTRODUCTION Chronic obstructive pulmonary disease (COPD) is a common lung disease that affects millions of people, and it is the fourth leading cause of death in the United States. It
Overview. The Respiratory System. Chapter 18. Respiratory Emergencies 9/11/2012
 Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Differentiating Bronchoconstriction Out of a Sea of Wheezes
 Differentiating Bronchoconstriction Out of a Sea of Wheezes Disclosure Statement I have no affiliation with any drug company medical equipment provider or whatever Cardinal Glennon Children s Medical Center
Differentiating Bronchoconstriction Out of a Sea of Wheezes Disclosure Statement I have no affiliation with any drug company medical equipment provider or whatever Cardinal Glennon Children s Medical Center
The Respiratory System Structures of the Respiratory System Structures of the Respiratory System Structures of the Respiratory System Nose Sinuses
 CH 14 D.E. Human Biology The Respiratory System The Respiratory System OUTLINE: Mechanism of Breathing Transport of Gases between the Lungs and the Cells Respiratory Centers in the Brain Function Provides
CH 14 D.E. Human Biology The Respiratory System The Respiratory System OUTLINE: Mechanism of Breathing Transport of Gases between the Lungs and the Cells Respiratory Centers in the Brain Function Provides
Wheeze. Respiratory Tract Symptoms. Prof RJ Green Department of Paediatrics. Cough. Wheeze/noisy breathing. Acute. Tight chest. Shortness of breath
 Wheeze Prof RJ Green Department of Paediatrics Respiratory Tract Symptoms Cough Tight chest Wheeze/noisy breathing Shortness of breath Acute Chronic Respiratory rate Most important sign of respiratory
Wheeze Prof RJ Green Department of Paediatrics Respiratory Tract Symptoms Cough Tight chest Wheeze/noisy breathing Shortness of breath Acute Chronic Respiratory rate Most important sign of respiratory
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
Acute respiratory failure
 Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
AIRWAY & HEART ANOTOMY
 Objectives I CAN T BREATH Respiratory Emergencies Review of anatomical structures related to heart & lungs Differentiate differences between adult and pediatric airways Identify the need for airway assistance
Objectives I CAN T BREATH Respiratory Emergencies Review of anatomical structures related to heart & lungs Differentiate differences between adult and pediatric airways Identify the need for airway assistance
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Why do you breathe? What is oxygen used for? Where does CO2 come from?
 RESPIRATORY SYSTEM How You Breathe Why do you breathe? What is oxygen used for? Where does CO2 come from? Respiration: exchange of gases between air & your body cells 1. Outside air (O2) lungs metabolism
RESPIRATORY SYSTEM How You Breathe Why do you breathe? What is oxygen used for? Where does CO2 come from? Respiration: exchange of gases between air & your body cells 1. Outside air (O2) lungs metabolism
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
Phases of Respiration. Chapter 18: The Respiratory System. Structures of the Respiratory System. Structures of the Respiratory System
 Phases of Respiration Chapter 18: The Respiratory System Respiration Process of obtaining oxygen from environment and delivering it to cells Phases of Respiration 1. Pulmonary ventilation between air and
Phases of Respiration Chapter 18: The Respiratory System Respiration Process of obtaining oxygen from environment and delivering it to cells Phases of Respiration 1. Pulmonary ventilation between air and
LUNGS. Requirements of a Respiratory System
 Respiratory System Requirements of a Respiratory System Gas exchange is the physical method that organisms use to obtain oxygen from their surroundings and remove carbon dioxide. Oxygen is needed for aerobic
Respiratory System Requirements of a Respiratory System Gas exchange is the physical method that organisms use to obtain oxygen from their surroundings and remove carbon dioxide. Oxygen is needed for aerobic
Respiratory System. Respiratory System Overview. Component 3/Unit 11. Health IT Workforce Curriculum Version 2.0/Spring 2011
 Component 3-Terminology in Healthcare and Public Health Settings Unit 11-Respiratory System This material was developed by The University of Alabama at Birmingham, funded by the Department of Health and
Component 3-Terminology in Healthcare and Public Health Settings Unit 11-Respiratory System This material was developed by The University of Alabama at Birmingham, funded by the Department of Health and
Asthma- THE most common Pediatric Disease JENNIFER MCDANIEL, RRT- NPS
 Asthma- THE most common Pediatric Disease JENNIFER MCDANIEL, RRT- NPS Asthma Usually acquire before the age of 10 These patients exhibit hyper-reactive airways Spasm Constriction Swelling Secretions are
Asthma- THE most common Pediatric Disease JENNIFER MCDANIEL, RRT- NPS Asthma Usually acquire before the age of 10 These patients exhibit hyper-reactive airways Spasm Constriction Swelling Secretions are
Phases of Respiration
 Phases of Respiration We get oxygen from the environment and it goes to our cells, there. Pulmonary ventilation External exchange of gases Internal exchange of gases Overview of respiration. In ventilation,
Phases of Respiration We get oxygen from the environment and it goes to our cells, there. Pulmonary ventilation External exchange of gases Internal exchange of gases Overview of respiration. In ventilation,
Chapter 11 The Respiratory System
 Biology 12 Name: Respiratory System Per: Date: Chapter 11 The Respiratory System Complete using BC Biology 12, page 342-371 11.1 The Respiratory System pages 346-350 1. Distinguish between A. ventilation:
Biology 12 Name: Respiratory System Per: Date: Chapter 11 The Respiratory System Complete using BC Biology 12, page 342-371 11.1 The Respiratory System pages 346-350 1. Distinguish between A. ventilation:
3/10/15. Summary. Anatomy Larynx. Anatomy Trachea
 Summary Anatomy Brachycephalic Airway Syndrome (BCAS) Crisis Anatomy Larynx Anatomy Trachea Tracheal rings are incomplete, C-shaped cartilage with the dorsal membrane being completed by tracheal muscle
Summary Anatomy Brachycephalic Airway Syndrome (BCAS) Crisis Anatomy Larynx Anatomy Trachea Tracheal rings are incomplete, C-shaped cartilage with the dorsal membrane being completed by tracheal muscle
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery. By: Lillian Han
 Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
BRONCHIOLITIS PEDIATRIC
 DEFINITION Bronchiolitis is typically defined as the first episode of wheezing in infants < 24 months of age. It is a viral illness of the lower respiratory tract that causes tachypnea, bronchospasm, and
DEFINITION Bronchiolitis is typically defined as the first episode of wheezing in infants < 24 months of age. It is a viral illness of the lower respiratory tract that causes tachypnea, bronchospasm, and
Respiratory Emergencies
 Respiratory Emergencies Chapter 24 Respiratory Emergencies Introduction Breathing should be effortless, and individuals should exhibit respiratory rates and tidal volumes appropriate for their ages (normally
Respiratory Emergencies Chapter 24 Respiratory Emergencies Introduction Breathing should be effortless, and individuals should exhibit respiratory rates and tidal volumes appropriate for their ages (normally
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Pulmonary
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Pulmonary 1. GOAL: Diagnose and manage patients with asthma. 2. GOAL: Understand the role of the pediatrician in preventing
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Pulmonary 1. GOAL: Diagnose and manage patients with asthma. 2. GOAL: Understand the role of the pediatrician in preventing
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Acute Cough. These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Acute Cough. These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio
McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis. Optional #2 2017
 McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis Optional #2 2017 The tones go out at 3 am for a child with difficulty breathing. As it is a kid
McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis Optional #2 2017 The tones go out at 3 am for a child with difficulty breathing. As it is a kid
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
The Throat. Image source:
 The Throat Anatomy Image source: http://anatomyforlayla.blogspot.co.za/2007/04/blog-post.html The Throat consists of three parts: 1. The Nasopharynx is the upper part of the throat and it is situated behind
The Throat Anatomy Image source: http://anatomyforlayla.blogspot.co.za/2007/04/blog-post.html The Throat consists of three parts: 1. The Nasopharynx is the upper part of the throat and it is situated behind
Upper and Lower Respiratory Tract Disorders
 F.A. Davis: Advantage Upper and Lower Respiratory Tract Disorders (11.16.15) Page 1 Upper and Lower Respiratory Tract Disorders The respiratory system is an interconnected network of organs, tissues, and
F.A. Davis: Advantage Upper and Lower Respiratory Tract Disorders (11.16.15) Page 1 Upper and Lower Respiratory Tract Disorders The respiratory system is an interconnected network of organs, tissues, and
It s Monday! July 28, 2014
 It s Monday! July 28, 2014 Prep Question The mother of a 6-year-old girl reports during a health supervision visit that her daughter has nighttime wetting and occasional daytime accidents with urgency.
It s Monday! July 28, 2014 Prep Question The mother of a 6-year-old girl reports during a health supervision visit that her daughter has nighttime wetting and occasional daytime accidents with urgency.
Pediatric Assessment Triangle
 Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
Chapter 10 The Respiratory System
 Chapter 10 The Respiratory System Biology 2201 Why do we breathe? Cells carry out the reactions of cellular respiration in order to produce ATP. ATP is used by the cells for energy. All organisms need
Chapter 10 The Respiratory System Biology 2201 Why do we breathe? Cells carry out the reactions of cellular respiration in order to produce ATP. ATP is used by the cells for energy. All organisms need
Glossary of Asthma Terms
 HealthyKidsExpress@bjc.org Asthma Words to Know Developed in partnership with Health Literacy Missouri Airways (Bronchi, Bronchial Tubes): The tubes in the lungs that let air in and out of the body. Airway
HealthyKidsExpress@bjc.org Asthma Words to Know Developed in partnership with Health Literacy Missouri Airways (Bronchi, Bronchial Tubes): The tubes in the lungs that let air in and out of the body. Airway
Asthma Care in the Emergency Department Clinical Practice Guideline
 Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely
Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Evaluation of Stridor. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Evaluation of Stridor. These podcasts are designed to give medical students an overview of key topics in pediatrics.
Your Virtual Health Partner. Respiratory Distress in the Pediatric Patient: Think quick and calmly
 Your Virtual Health Partner Respiratory Distress in the Pediatric Patient: Think quick and calmly Are kids really so different? You be the judge Children are not small adults Children are still growing
Your Virtual Health Partner Respiratory Distress in the Pediatric Patient: Think quick and calmly Are kids really so different? You be the judge Children are not small adults Children are still growing
The Respiratory System
 BIOLOGY OF HUMANS Concepts, Applications, and Issues Fifth Edition Judith Goodenough Betty McGuire 14 The Respiratory System Lecture Presentation Anne Gasc Hawaii Pacific University and University of Hawaii
BIOLOGY OF HUMANS Concepts, Applications, and Issues Fifth Edition Judith Goodenough Betty McGuire 14 The Respiratory System Lecture Presentation Anne Gasc Hawaii Pacific University and University of Hawaii
PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT
 PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT Dr started to talk about his specialty at the hospital which is (ICU-Pulmonary-Internal Medicine). Pulmonary medical branch is a subspecialty of internal medicine.
PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT Dr started to talk about his specialty at the hospital which is (ICU-Pulmonary-Internal Medicine). Pulmonary medical branch is a subspecialty of internal medicine.
BJ Coopes, MD Medical Director, Pediatric Critical Care, Inpatient Pediatrics
 BJ Coopes, MD Medical Director, Pediatric Critical Care, Inpatient Pediatrics The BIG Question: Sick or Not Sick? Signs of Respiratory Distress Tachypnea Tachycardia Retractions Accessory muscles Head
BJ Coopes, MD Medical Director, Pediatric Critical Care, Inpatient Pediatrics The BIG Question: Sick or Not Sick? Signs of Respiratory Distress Tachypnea Tachycardia Retractions Accessory muscles Head
PEDIATRIC RESPIRATORY SYNCYTIAL VIRUS (RSV) ALL THAT WHEEZES IS NOT ASTHMA
 ALL THAT WHEEZES IS NOT ASTHMA") PEDIATRIC RESPIRATORY SYNCYTIAL VIRUS (RSV) ALL THAT WHEEZES IS NOT ASTHMA Season changes here in Ohio can send the census numbers in our local P.I.C.U. s, N.I.C.U. s and Emergency Rooms through the roof.
PEDIATRIC RESPIRATORY SYNCYTIAL VIRUS (RSV) ALL THAT WHEEZES IS NOT ASTHMA Season changes here in Ohio can send the census numbers in our local P.I.C.U. s, N.I.C.U. s and Emergency Rooms through the roof.
Chronic obstructive pulmonary disease
 Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?