Karen Meyerson, MSN, APRN, NP C, AE C
|
|
|
- Justin Stone
- 5 years ago
- Views:
Transcription


1 Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) June 2015 Karen Meyerson, MSN, APRN, NP C, AE C
2 Patient Education The goal of all patient education is to help patients take the actions needed to control their asthma or COPD.

3 Becoming COPD Prepared: A 4 STEP Approach
4 STEP: A Framework for COPD Care

5 Screening for COPD using a validated screening tool is an important step in identifying patients who may be at risk for COPD.


6 Top 5 Causes of Death COPD = 3rd Leading Cause of Death % Change, % 100% 80% 60% 40% 20% 0% -20% -40% -60% -80% -52% Heart disease Cancer Stroke COPD Accidents -3% -63% 103% -41% Jemal A, et al. JAMA. 2005; 294:
 are undiagnosed Most (70%) of patients with undiagnosed COPD are <65 years of age Percent With Undiagnosed COPD 30% Age 65 70%")
7 Under diagnosis of COPD in the United States Approximately 24 million adults have evidence of impaired lung function indicative of COPD Over 12.7 million people have been diagnosed with COPD Approximately half (50%) are undiagnosed Most (70%) of patients with undiagnosed COPD are <65 years of age Percent With Undiagnosed COPD 30% Age 65 70% <Age 65 Mannino DM, et al. MMWR Surveill Summ. 2002;51(1):1-13. Mannino DM, et al. Proc Am Thorac Soc. 2007;4(7): Pleis JR, et al. Vital Health Stat. 2006;132:1-153.
8 Significant Burden of COPD Why are approximately 50% of people with COPD undiagnosed? Patients typically seek medical attention at the moderate stage of COPD 81% of patients already had moderate to very severe COPD at initial spirometry confirmed diagnosis Each year due to COPD, there are approximately 16.3 million office visits 672,000 hospitalizations More than 22% of Medicare patients hospitalized for COPD were readmitted within 30 days of discharge; 36% of these readmissions were due to COPD
9 Why is Early Diagnosis of COPD Important? Lung damage starts early and is progressive Breathlessness occurs early, increases with severity, and is underestimated by patients Inactivity is common but must be carefully assessed by the health care provider Even patients with mild disease can have exacerbations Earlier intervention (i.e., smoking cessation) leaves patients with more lung function
10 Definition of COPD According to the ATS/ERS COPD Guidelines, COPD is a preventable and treatable disease state characterized by airflow limitation that is not fully reversible. The airflow limitation is usually progressive and is associated with an abnormal inflammatory response of the lungs to noxious particles or gases, primarily caused by cigarette smoking. Although COPD affects the lungs, it also produces significant systemic consequences. According to the GOLD guidelines, COPD is characterized by chronic inflammation throughout the airways
11 Definitions of Chronic Bronchitis and Emphysema Chronic bronchitis is clinically defined as chronic productive cough for 3 months in each of 2 successive years in a patient in whom other causes of productive chronic cough have been excluded Emphysema is defined as abnormal, permanent enlargement of the airspaces distal to the terminal bronchioles, accompanied by destruction of their walls, yet without obvious fibrosis

12 COPD Is a Multicomponent Disease 1 3 BRONCHOCONSTRICTION Tightness in the smooth muscle surrounding the airways in the lungs STRUCTURAL CHANGES Permanent damage to airways and alveoli INFLAMMATION Structural changes Narrowing of small airways Increase in inflammatory cells MUCOCILIARY DYSFUNCTION Excessive mucus production and decreased clearance Adapted. Illustration Copyright 2010 Nucleus Medical Art, All rights reserved Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) Accessed April 13, Agusti AG. Respir Med. 2005;99: Rodriguez-Roisin R. COPD. 2005;2:
13 Some Diagnostic Indicators for COPD Dyspnea Initially during exercise Progresses to occur with minimal exercise or at rest Chronic cough Intermittent early in disease process Occurring primarily in morning Persists throughout day with disease progression Sputum production Any pattern of chronic sputum production may indicate COPD History of exposure to risk factors Tobacco smoke Occupational dusts and chemicals Smoke from wood burning stoves and heating fuels


14 Who Is the COPD Patient? Perception3-5 Myth: COPD is a disease of the elderly1 Myth: COPD is a disease of men2 1. Tinkelman, et al. Am J Manag Care. 2003;9: Chapman KR. Clin Chest Med. 2004; 25: Rennard SI. New Engl J Med. 2004; 350: Kleinschmidt P. COPD and emphysema. Available at 5. Rennard SI. N Engl J Med. 2004;305: Netter illustrations, with permission from Icon Learning Systems, a division of MediMedia USA, Inc. All rights reserved.
15 COPD in Younger Patients and Women Is on the Rise Reality Reality: COPD afflicts the working age population. Reality: COPD is also a disease of women. Mannino, et al. MMWR. 2002;51(1)(6 suppl):1-13.


16 COPD Is Not a Man s Disease 65% Hypothetical Male Patient With COPD Symptoms Diagnosed as COPD by 65% of physicians Hypothetical Female Patient With COPD Symptoms Diagnosed as COPD by 49% of physicians 49% COPD symptoms in women were most commonly misdiagnosed as asthma. Chapman KR, et al. Chest. 2001;119(6):
17 Screening patients for COPD The COPD Alliance 1 recommends the utilization of a simple validated 2 questionnaire COPD Population Screener TM download at Persons at risk should be asked to complete the screener. 1 The COPD Alliance is composed of multidisciplinary societies, i.e., AANP, AAPA, ACCP, ACOFP, ACOI 2 Martinez FJ et al. COPD.2008;5(2):85-95


18
19 STEP Tools on COPD.org COPD Screener This validated COPD screening tool uses five questions to determine a patient s risk for COPD and the potential need for spirometry testing. The screener is available in English and Spanish Treatment room poster
20 Spirometry is a test that measures the amount of air a patient can breathe out and the amount of time it takes to do so. Spirometry can be administered by trained office staff in a primary care setting.
21 Diagnosis of COPD Diagnosis often does not occur until the disease has progressed significantly Lack of serious symptoms and poor recognition of clinical symptoms in early phase COPD is confirmed by performing a lung function test: post bronchodilator spirometry. Global Initiative for Chronic Obstructive Disease. Global strategy for the diagnosis, management, and prevention of COPD. Updated
22 Recommendations From the National Lung Health Education Program Primary care clinicians should perform an office spirometry test for the following patients: Patients 45 years old who report smoking (current smokers and those who recently quit) in order to detect COPD Patients with respiratory symptoms, such as chronic cough, sputum production, wheezing, or dyspnea on exertion Ferguson GT, et al. Chest. 2000;117(4):
23 Spirometry Is Essential for Diagnosing COPD If... Chronic symptoms = cough, sputum, and/or shortness of breath And... Exposure to risk factors = tobacco, occupational irritants, and/or indoor/outdoor pollution Then... Spirometry* to confirm COPD diagnosis FEV1/FVC <0.70 FEV1 determines staging *Additional testing: chest radiograph, echocardiogram, arterial blood gas, sputum analysis, CT scan. Global Initiative for Chronic Obstructive Disease. Global strategy for the diagnosis, management, and prevention of COPD. Updated
24 Barriers to Spirometry Use Overcoming barriers to spirometry use may lead to increased COPD diagnosis. Uncertainty about the impact of the test on outcome 1 Lack of training on spirometry use 1,2 Poor education on interpreting results 1,2 Time and logistical constraints 3 Reimbursement concerns 1 1. Kaminsky DA, et al. Respir Care. 2005;50(12): Díaz-Lobato, et al. Chest. 2004;126(5): Caramori, et al. Monaldi Arch Chest Dis. 2005;62:6-12.
25 Spirometry in Primary Care Clinical Value Confirms diagnosis and assesses severity of COPD Helps to differentiate asthma from COPD Helps to assess response to bronchodilator therapy The instrument is inexpensive, easy to maintain, and well reimbursed. Primary care clinicians can be trained to perform accurate interpretations. Yawn BP, et al. Chest. 2007;132(4):



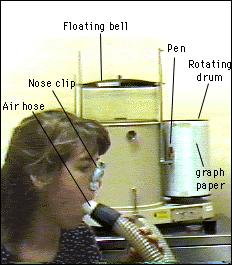
26 Old Spirometer NEW Portable Office Spirometers
27 Predicted Normal Values Affected by: Age Height Sex Ethnic Origin
28 Spirometric Diagnosis of COPD COPD is confirmed by post bronchodilator FEV 1 /FVC < 0.70 Post bronchodilator FEV 1 measured minutes after 2 to 4 puffs of a short acting bronchodilator
29 Flow Volume Loop Expiratory flow rate, L/sec Inspiratory flow rate, L/sec TLC FVC Maximum expiratory flow (PEF) Volume, L RV
30 Pharmacologic Therapy for Stable COPD All patients who are symptomatic merit a trial of drug treatment. Current long acting medications can Reduce symptoms Increase exercise capacity Reduce number and severity of exacerbations Improve health status Celli et al. Eur Respir J. 2004;23(6):
31 Smoking Abstinence: Slows Progression of COPD Lung Function FEV 1 (% Predicted) Susceptible smoker Disability Never smoked or not susceptible to smoke Smoked regularly and susceptible to its effects Stopped smoking at 45 y Stopped smoking at 65 y 0 Death Age (y) Fletcher C, et al. Br Med J. 1977;1(6077):
32 It is essential that you take the time to educate your patients about COPD, including symptoms, diagnosis, triggers of an exacerbation, and how to live better with the disease.
33 STEP Tools on COPD.org Flip Chart Developed by the AANP A Breath of Fresh Air enables clinicians to have a thorough dialogue with their patients about everything from adherence to nutrition. Video to show patients the proper use of all available inhalers.
34 Providing care and support to COPD patients is what clinicians strive to do at the highest levels and it is also the fourth STEP in becoming COPD Prepared.
35 Role of the Care Manager in COPD Care Managers may assist in identifying patients complaining of cough or shortness of breath who may be at risk for respiratory disorders Ask patients over 40 years of age who are current or ex smokers the following questions: Do you cough regularly? Do you cough up phlegm regularly? Do simple chores make you short of breath? Do you wheeze when you exert yourself, or at night? Do you get frequent colds that persist longer than those of other people you know? If patients answer yes to any of the questions, consider spirometric testing
36 Role of the Care Manager in COPD Promote education on COPD and self management techniques Counsel patients on the correct use of inhalers Care Managers should demonstrate the use of all newly prescribed devices and observe the patient s use of each device Question patients about their medication adherence in a nonjudgmental manner and take steps to resolve any reported problems
37 Role of the Care Manager in COPD Care Managers may assist patients in the prevention and management of COPD and COPD exacerbations by: Identifying and referring patients who may have COPD Educating patients on COPD and self management techniques Counseling patients on smoking cessation Recommending vaccinations Educating patients on signs/symptoms of COPD exacerbation Care Managers are well positioned to play a key role in many aspects of COPD management
38 Prevent COPD Exacerbations Defined as an acute change in a patient s baseline dyspnea, cough, and/or sputum beyond day to day variability, and sufficient to warrant a change in therapy The prevention of exacerbations is recognized as a goal in COPD disease state management Frequency of exacerbations contributes to a decline in lung function and significant worsening in quality of life
39 Prevent COPD Exacerbations Changes in the following that are beyond normal day to day variations, are acute in onset, and may warrant a change in regular medication: Baseline dyspnea (or breathlessness) Cough Sputum Increased breathlessness that may be accompanied by the following: Wheezing and chest tightness Increased cough and sputum Change of the color and/or tenacity of sputum Fever Tachycardia and tachypnea, malaise, insomnia, sleepiness, fatigue, depression, and confusion may accompany COPD exacerbations Decrease in exercise tolerance, fever, and/or new radiologic anomalies suggestive of pulmonary disease may be additional signs of COPD exacerbation
40 Prevent COPD Exacerbations Defined as an acute change in a patient s baseline dyspnea, cough, and/or sputum beyond day to day variability, and sufficient to warrant a change in therapy Evidence supports that exacerbations are acute inflammatory events superimposed on the chronic inflammation characteristic of COPD In a 12 month study, 77% of patients had at least 1 exacerbation Frequency of exacerbations contributes to a decline in lung function and significant worsening in quality of life The prevention of exacerbations is recognized as a goal in COPD disease state management

41 Help Patients Recognize and Treat Exacerbations Changes in signs and symptoms from baseline: Shortness of breath, even at rest More wheezing, coughing, mucus Mucus looks different Chest tightness Irritable, fatigued, no energy Fever Color changes Rapid breathing, heart rate
42 Tips for Reducing Exacerbations Wash hands often Avoid close contact with people who are ill Get a flu shot yearly and make sure pneumonia immunization is up to date Use your long term control medications daily Use antibiotics quickly for infections or sinus problems Follow the COPD Action Plan


43

44 Know When to Call the Doctor Shortness of breath or wheezing that does not resolve after using inhaler Change in color, smell, amount or thickness of mucus coughed up New or increased ankle swelling Awaken with shortness of breath > once/night Very tired and this lasts > than one/day Have a fever that lasts

45 Know When to go to the Hospital Confusion, slurring of speech or sleepiness during a serious lung infection Loss of alertness or two or more of: Increase in seriousness of symptoms, such as trouble breathing at rest Struggling to use your upper chest or neck muscles to try to breathe A large increase in how fast your heart is beating A large increase in how fast you are breathing Any severe shortness of breath or chest pain or any other severe symptom


46
47 COPD Assessment Test (CAT) I never cough I cough all the time I have no phlegm (mucus) in my chest at all My chest is completely full of phlegm (mucus) My chest does not feel tight at all My chest feels very tight When I walk up a hill or one flight of stairs I am not breathless I am very breathless I am confident leaving my home despite my lung condition I am not confident I sleep soundly I don t sleep soundly because of my lung condition I have lots of energy I have no energy at all * Range of CAT scores from Higher scores denote a more severe impact of COPD on a patient s life. The difference between stable and exacerbation patients was five units. No target score represents the best achievable outcome.
48 Role of the Care Manager in COPD Smoking cessation is the single most effective and cost effective intervention to reduce the risk of developing COPD and slow its progression Smoking cessation has the greatest capacity to influence the natural history of COPD. Health care providers should encourage all patients who smoke to quit. Additional benefits of smoking cessation: Lung function begins to improve in 2 weeks to 3 months after quitting Coughing and shortness of breath decreases in 1 9 months after quitting
49 Smoking Cessation: It s never too late to benefit lung function FEV 1 (L) Sustained Quitters Intermittent Quitters Continuous Smokers Year Loss of lung function over 11 years in the Lung Health Study. Anthonisen NR, Connett JE, Murray RP for the Lung Health Study Research Group. Smoking and Lung Function of Lung Health Study Participants after 11 Years. Am J Respir Crit Care Med. 2002;166:
50 Brief Strategies to Help the Patient Willing to Quit Smoking ASK ADVISE ASSESS ASSIST ARRANGE Systematically identify all tobacco users at every visit Strongly urge all tobacco users to quit Determine willingness to make a quit attempt Aid the patient in quitting Schedule follow up contact

51 Sustained Quitters Had Lowest Mortality P<.001 for trend Anthonisen NR, et al. Ann Intern Med. 2005;142(4):
52 Smoking Cessation Requires Multiple Attempts (8 on Average) Fiore MC, et al. Treating tobacco use and dependence: 2008 Update-Clincial Practice Guideline, US Department of Health and Human Services, 2008 John U, et al. Prev Med. 2004; 38(3):

53 Pharmacotherapy for Smoking Cessation All Smoking Cessation Therapies Have Significant Benefit All P<0.05 vs control NRT = Nicotine replacement therapy. Wu P, et al. BMC Public Health. 2006;6: Accessed

54 ACCP s Tobacco Dependence Treatment Toolkit A complete online resource for you and your patients Visit


55 COPD Education Topics Pulmonary rehabilitation Maintain proper nutritional status Conserve energy and control stress Control breathing Oxygen therapy Support groups Better Breathers Club
56 G O lobal Initiative for Chronic bstructive L D ung isease 2015 Global Initiative for Chronic Obstructive Lung Disease
57 Global Strategy for Diagnosis, Management and Prevention of COPD Definition of COPD COPD, a common preventable and treatable disease, is characterized by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases. Exacerbations and comorbidities contribute to the overall severity in individual patients Global Initiative for Chronic Obstructive Lung Disease
58 Global Strategy for Diagnosis, Management and Prevention of COPD Risk Factors for COPD Genes Exposure to particles Tobacco smoke Occupational dusts, organic and inorganic Indoor air pollution from heating and cooking with biomass in poorly ventilated dwellings Outdoor air pollution Lung growth and development Gender Age Respiratory infections Socioeconomic status Asthma/Bronchial hyperreactivity Chronic Bronchitis 2015 Global Initiative for Chronic Obstructive Lung Disease

59 Global Strategy for Diagnosis, Management and Prevention of COPD Risk Factors for COPD Genes Infections Socio-economic status Aging Populations 2015 Global Initiative for Chronic Obstructive Lung Disease
60 Global Strategy for Diagnosis, Management and Prevention of COPD Diagnosis and Assessment: Key Points A clinical diagnosis of COPD should be considered in any patient who has dyspnea, chronic cough or sputum production, and a history of exposure to risk factors for the disease. Spirometry is required to make the diagnosis; the presence of a post-bronchodilator FEV 1 /FVC < 0.70 confirms the presence of persistent airflow limitation and thus of COPD Global Initiative for Chronic Obstructive Lung Disease
61 Global Strategy for Diagnosis, Management and Prevention of COPD Diagnosis and Assessment: Key Points The goals of COPD assessment are to determine the severity of the disease, including the severity of airflow limitation, the impact on the patient s health status, and the risk of future events. Comorbidities occur frequently in COPD patients, and should be actively looked for and treated appropriately if present Global Initiative for Chronic Obstructive Lung Disease
62 Global Strategy for Diagnosis, Management and Prevention of COPD Diagnosis of COPD SYMPTOMS shortness of breath chronic cough sputum EXPOSURE TO RISK FACTORS tobacco occupation indoor/outdoor pollution SPIROMETRY: Required to establish diagnosis 2015 Global Initiative for Chronic Obstructive Lung Disease
63 Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of Airflow Limitation: Spirometry Spirometry should be performed after the administration of an adequate dose of a shortacting inhaled bronchodilator to minimize variability. A post-bronchodilator FEV 1 /FVC < 0.70 confirms the presence of airflow limitation. Where possible, values should be compared to age-related normal values to avoid over-diagnosis of COPD in the elderly Global Initiative for Chronic Obstructive Lung Disease
64 Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of COPD: Goals Determine the severity of the disease, its impact on the patient s health status and the risk of future events (for example exacerbations) to guide therapy. Consider the following aspects of the disease separately: current level of patient s symptoms severity of the spirometric abnormality frequency of exacerbations presence of comorbidities Global Initiative for Chronic Obstructive Lung Disease
65 Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of COPD Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Assess comorbidities 2015 Global Initiative for Chronic Obstructive Lung Disease
66 Global Strategy for Diagnosis, Management and Prevention of COPD Symptoms of COPD The characteristic symptoms of COPD are chronic and progressive dyspnea, cough, and sputum production that can be variable from day-to-day. Dyspnea: Progressive, persistent and characteristically worse with exercise. Chronic cough: May be intermittent and may be unproductive. Chronic sputum production: COPD patients commonly cough up sputum Global Initiative for Chronic Obstructive Lung Disease
67 Global Strategy for Diagnosis, Management and Prevention of COPD Assess symptoms Assess degree of airflow limitation using spirometry COPD Assessment Test (CAT) Assess risk of exacerbations Assess comorbidities Assessment of COPD or Clinical COPD Questionnaire (CCQ) or mmrc Breathlessness scale 2015 Global Initiative for Chronic Obstructive Lung Disease
68 Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of Symptoms COPD Assessment Test (CAT): An 8-item measure of health status impairment in COPD ( Clinical COPD Questionnaire (CCQ): Selfadministered questionnaire developed to measure clinical control in patients with COPD ( Global Initiative for Chronic Obstructive Lung Disease
69 Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of Symptoms Breathlessness Measurement using the Modified British Medical Research Council (mmrc) Questionnaire: Relates well to other measures of health status and predicts future mortality risk Global Initiative for Chronic Obstructive Lung Disease
70 Global Strategy for Diagnosis, Management and Prevention of COPD Modified MRC (mmrc)questionnaire 2015 Global Initiative for Chronic Obstructive Lung Disease
71 Global Strategy for Diagnosis, Management and Prevention of COPD Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Use spirometry for grading severity Assess comorbidities Assessment of COPD according to spirometry, using four grades split at 80%, 50% and 30% of predicted value 2015 Global Initiative for Chronic Obstructive Lung Disease
72 Global Strategy for Diagnosis, Management and Prevention of COPD Classification of Severity of Airflow Limitation in COPD* In patients with FEV 1 /FVC < 0.70: GOLD 1: Mild GOLD 2: Moderate GOLD 3: Severe GOLD 4: Very Severe FEV 1 > 80% predicted 50% < FEV 1 < 80% predicted 30% < FEV 1 < 50% predicted FEV 1 < 30% predicted *Based on Post-Bronchodilator FEV Global Initiative for Chronic Obstructive Lung Disease
73 Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of COPD Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Assess comorbidities Use history of exacerbations and spirometry. Two exacerbations or more within the last year or an FEV 1 < 50 % of predicted value are indicators of high risk. Hospitalization for a COPD exacerbation associated with increased risk of death Global Initiative for Chronic Obstructive Lung Disease
74 Global Strategy for Diagnosis, Management and Prevention of COPD Assess Risk of Exacerbations To assess risk of exacerbations use history of exacerbations and spirometry: Two or more exacerbations within the last year or an FEV 1 < 50 % of predicted value are indicators of high risk. One or more hospitalizations for COPD exacerbation should be considered high risk Global Initiative for Chronic Obstructive Lung Disease
75 Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Combine these assessments for the purpose of improving management of COPD 2015 Global Initiative for Chronic Obstructive Lung Disease
76 Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD Risk (GOLD Classification of Airflow Limitation)) (C) (A) (D) (B) 0 2 or >1 leading to hospital admission 1 (not leading to hospital admission) Risk (Exacerbation history) CAT < 10 Symptoms CAT >10 mmrc 0 1 mmrc >2 Breathlessness 2015 Global Initiative for Chronic Obstructive Lung Disease
77 Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD Assess symptoms first (C) (A) (D) (B) If CAT < 10 or mmrc 0-1: Less Symptoms/breathlessness (A or C) If CAT > 10 or mmrc > 2: More Symptoms/breathlessness (B or D) CAT < 10 CAT > 10 Symptoms mmrc 0 1 mmrc >2 Breathlessness 2015 Global Initiative for Chronic Obstructive Lung Disease
78 Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD Assess risk of exacerbations next Risk (GOLD Classification of Airflow Limitation) (C) (D) (A) (B) CAT < 10 CAT > 10 Symptoms 2 or >1 leading to hospital admission 1 (not leading to hospital admission) 0 Risk (Exacerbation history) If GOLD 3 or 4 or 2 exacerbations per year or > 1 leading to hospital admission: High Risk (C or D) If GOLD 1 or 2 and only 0 or 1 exacerbations per year (not leading to hospital admission): Low Risk (A or B) mmrc 0 1 mmrc > 2 Breathlessness 2015 Global Initiative for Chronic Obstructive Lung Disease
79 Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD Risk (GOLD Classification of Airflow Limitation)) (C) (A) (D) (B) 0 2 or >1 leading to hospital admission 1 (not leading to hospital admission) Risk (Exacerbation history) CAT < 10 Symptoms CAT >10 mmrc 0 1 mmrc >2 Breathlessness 2015 Global Initiative for Chronic Obstructive Lung Disease

80 Patient Characteristic Spirometric Classification A B C D Low Risk Less Symptoms Low Risk More Symptoms High Risk Less Symptoms High Risk More Symptoms Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment Exacerbations per year CAT mmrc GOLD < GOLD > 10 >2 GOLD 3-4 > 2 < GOLD 3-4 > 2 >10 of COPD When assessing risk, choose the highest risk according to GOLD grade or exacerbation history. One or more hospitalizations for COPD exacerbations should be considered high risk.) 2015 Global Initiative for Chronic Obstructive Lung Disease >2

81 Global Strategy for Diagnosis, Management and Prevention of COPD Assess COPD Comorbidities COPD patients are at increased risk for: Cardiovascular diseases Osteoporosis Respiratory infections Anxiety and Depression Diabetes Lung cancer Bronchiectasis These comorbid conditions may influence mortality and hospitalizations and should be looked for routinely, and treated appropriately Global Initiative for Chronic Obstructive Lung Disease
82 Global Strategy for Diagnosis, Management and Prevention of COPD Differential Diagnosis: COPD and Asthma COPD Onset in mid-life Symptoms slowly progressive Long smoking history ASTHMA Onset early in life (often childhood) Symptoms vary from day to day Symptoms worse at night/early morning Allergy, rhinitis, and/or eczema also present Family history of asthma 2015 Global Initiative for Chronic Obstructive Lung Disease
83 Global Strategy for Diagnosis, Management and Prevention of COPD Therapeutic Options: Key Points Appropriate pharmacologic therapy can reduce COPD symptoms, reduce the frequency and severity of exacerbations, and improve health status and exercise tolerance. None of the existing medications for COPD has been shown conclusively to modify the long-term decline in lung function. Influenza and pneumococcal vaccination should be offered depending on local guidelines Global Initiative for Chronic Obstructive Lung Disease
84 Beta 2 -agonists Global Strategy for Diagnosis, Management and Prevention of COPD Short-acting beta 2 -agonists Long-acting beta 2 -agonists Anticholinergics Short-acting anticholinergics Long-acting anticholinergics Therapeutic Options: COPD Medications Combination short-acting beta 2 -agonists + anticholinergic in one inhaler Combination long-acting beta 2 -agonist + anticholinergic in one inhaler Methylxanthines Inhaled corticosteroids Combination long-acting beta 2 -agonists + corticosteroids in one inhaler Systemic corticosteroids Phosphodiesterase-4 inhibitors 2015 Global Initiative for Chronic Obstructive Lung Disease
85 To be continued Webinar #6 COPD Medications Questions? Call: Visit:
Karen Meyerson, MSN, APRN, NP-C, AE-C Director, Commercial Care Management Priority Health
 Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) November 29, 2017 Karen Meyerson, MSN, APRN, NP-C, AE-C Director, Commercial Care Management Priority Health Top 5 Causes of Death
Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) November 29, 2017 Karen Meyerson, MSN, APRN, NP-C, AE-C Director, Commercial Care Management Priority Health Top 5 Causes of Death
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
UNDERSTANDING COPD MEDIA BACKGROUNDER
 UNDERSTANDING COPD MEDIA BACKGROUNDER What is COPD? Chronic Obstructive Pulmonary Disease (COPD) also called emphysema and/or chronic obstructive bronchitis* is a preventable lung disease caused by the
UNDERSTANDING COPD MEDIA BACKGROUNDER What is COPD? Chronic Obstructive Pulmonary Disease (COPD) also called emphysema and/or chronic obstructive bronchitis* is a preventable lung disease caused by the
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
People with asthma who smoke. The combination of asthma, a chronic airway disease, and smoking increases the risk of COPD even more.
 COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable
 THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
Anyone who smokes and/or has shortness of breath and sputum production could have COPD
 COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Management of Acute Exacerbations of COPD
 MiCMRC Educational Webinar Management of Acute Exacerbations of COPD August 22, 2018 MiCMRC Educational Webinar Management of Acute Exacerbations of COPD Expert Presenter: Catherine A. Meldrum PhD RN MS
MiCMRC Educational Webinar Management of Acute Exacerbations of COPD August 22, 2018 MiCMRC Educational Webinar Management of Acute Exacerbations of COPD Expert Presenter: Catherine A. Meldrum PhD RN MS
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
Life-long asthma and its relationship to COPD. Stephen T Holgate School of Medicine University of Southampton
 Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Living well with COPD
 This factsheet aims to show people with chronic obstructive pulmonary disease (COPD) and their friends and family how they can live a full life with this disease. What is COPD? COPD is a condition that
This factsheet aims to show people with chronic obstructive pulmonary disease (COPD) and their friends and family how they can live a full life with this disease. What is COPD? COPD is a condition that
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
CARE OF THE ADULT COPD PATIENT
 CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
Fact. Objectives 1/6/2016. Reducing Hospital Readmissions for Chronic Obstructive Pulmonary Disease (COPD)
") Reducing Hospital Readmissions for Chronic Obstructive Pulmonary Disease (COPD) Jin S. Oh, PharmD Larkin Community Hospital January 10, 2016 Fact COPD is the third leading cause of death in the United
Reducing Hospital Readmissions for Chronic Obstructive Pulmonary Disease (COPD) Jin S. Oh, PharmD Larkin Community Hospital January 10, 2016 Fact COPD is the third leading cause of death in the United
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Defining COPD. Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist
 Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
COPD in primary care: reminder and update
 COPD in primary care: reminder and update Managing COPD continues to be a major feature of primary care, particularly in practices with a high proportion of M ori and Pacific peoples. COPDX clinical practice
COPD in primary care: reminder and update Managing COPD continues to be a major feature of primary care, particularly in practices with a high proportion of M ori and Pacific peoples. COPDX clinical practice
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic Obstructive Pulmonary Disease (COPD).
.") Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
Overview of COPD INTRODUCTION
 Overview of COPD INTRODUCTION Chronic obstructive pulmonary disease (COPD) is a common lung disease that affects millions of people, and it is the fourth leading cause of death in the United States. It
Overview of COPD INTRODUCTION Chronic obstructive pulmonary disease (COPD) is a common lung disease that affects millions of people, and it is the fourth leading cause of death in the United States. It
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
American Thoracic Society (ATS) Perspective
 Perspective") National Surveillance System for Chronic Lung Disease (CLD): American Thoracic Society (ATS) Perspective Gerard J. Criner, M.D. Chronic Obstructive Pulmonary Disease (COPD) l Definition: Group of chronic
National Surveillance System for Chronic Lung Disease (CLD): American Thoracic Society (ATS) Perspective Gerard J. Criner, M.D. Chronic Obstructive Pulmonary Disease (COPD) l Definition: Group of chronic
Chronic obstructive pulmonary disease
 Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
COPD GOLD Guidelines & Barnet inhaler choices. Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust
 COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
Chronic Obstructive Pulmonary Disease
 Page 1 of 5 Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease (COPD) is an 'umbrella' term for people with chronic bronchitis, emphysema, or both. With COPD the airflow to the
Page 1 of 5 Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease (COPD) is an 'umbrella' term for people with chronic bronchitis, emphysema, or both. With COPD the airflow to the
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Presented by UIC College of Nursing
 Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long-acting inhalers and emergency use inhalers.
Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long-acting inhalers and emergency use inhalers.
Chronic Obstructive Pulmonary Disease 1/18/2018
 Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long acting inhalers and emergency use inhalers.
Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long acting inhalers and emergency use inhalers.
2017 GOLD Report. Is it worth its weight in GOLD??? CSHP-NB Fall Education Day September 30, 2017
 2017 GOLD Report Is it worth its weight in GOLD??? CSHP-NB Fall Education Day September 30, 2017 Lauren Munro; BSc(Pharm) Amanda Burns; BSc(Pharm) Pharmacy Residents The Moncton Hospital Objectives Explain
2017 GOLD Report Is it worth its weight in GOLD??? CSHP-NB Fall Education Day September 30, 2017 Lauren Munro; BSc(Pharm) Amanda Burns; BSc(Pharm) Pharmacy Residents The Moncton Hospital Objectives Explain
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015
 David CL Lam Department of Medicine University of Hong Kong October, 2015") Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Chronic Obstructive Pulmonary Disease
 Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
Disclosures. Chronic Obstructive Pulmonary Disease. Chronic Obstructive Pulmonary Disease (COPD)
") Chronic Obstructive Pulmonary Disease May 14, 2016 Orlando, FL COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United States. Alarmingly, COPD recently became
Chronic Obstructive Pulmonary Disease May 14, 2016 Orlando, FL COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United States. Alarmingly, COPD recently became
Chronic Obstructive Pulmonary Disease Guidelines and updates
 Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Objectives. Advances in Managing COPD Patients
 4:45 5:30pm Advances in Managing Patients SPEAKER Nicola Hanania, MD, FCCP, FRCP, FACP Presenter Disclosure Information The following relationships exist related to this presentation: Nicola Hanania, MD,
4:45 5:30pm Advances in Managing Patients SPEAKER Nicola Hanania, MD, FCCP, FRCP, FACP Presenter Disclosure Information The following relationships exist related to this presentation: Nicola Hanania, MD,
Provider Respiratory Inservice
 Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
9/22/2015 CONFLICT OF INTEREST OBJECTIVES. Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR
 Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR by Scott Cerreta, BS, RRT Director of Education www.copdfoundation.org scerreta@copdfoundation.org CONFLICT OF INTEREST
Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR by Scott Cerreta, BS, RRT Director of Education www.copdfoundation.org scerreta@copdfoundation.org CONFLICT OF INTEREST
Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR
 Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR by Scott Cerreta, BS, RRT Director of Education www.copdfoundation.org scerreta@copdfoundation.org CONFLICT OF INTEREST
Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR by Scott Cerreta, BS, RRT Director of Education www.copdfoundation.org scerreta@copdfoundation.org CONFLICT OF INTEREST
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
COPD/Asthma. Prudence Twigg, AGNP
 COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
GOLD UPDATE on COPD and the Importance of Accurate Dyspnea Evaluation
 GOLD UPDATE on COPD and the Importance of Accurate Dyspnea Evaluation George Anderson, PhD Sr. Medical Science Liaison MA-AZAP ML-4006-US-0212 Approved 11/16 Glob al Strategy for the Diagnosis, Management,
GOLD UPDATE on COPD and the Importance of Accurate Dyspnea Evaluation George Anderson, PhD Sr. Medical Science Liaison MA-AZAP ML-4006-US-0212 Approved 11/16 Glob al Strategy for the Diagnosis, Management,
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 CHRONIC OBSTRUCTIVE PULMONARY DISEASE DEFINITION Chronic obstructive pulmonary disease (COPD) is a common preventable and treatable disease characterized by airflow limitation that is usually progressive
CHRONIC OBSTRUCTIVE PULMONARY DISEASE DEFINITION Chronic obstructive pulmonary disease (COPD) is a common preventable and treatable disease characterized by airflow limitation that is usually progressive
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease CareOregon Pharmacy Abridged sample of presentation content Home Equipment Pathophysiology Exacerbations Guidelines Lifestyle Modification Medication Management Sample
Chronic Obstructive Pulmonary Disease CareOregon Pharmacy Abridged sample of presentation content Home Equipment Pathophysiology Exacerbations Guidelines Lifestyle Modification Medication Management Sample
COPD COPD. C - Chronic O - Obstructive P - Pulmonary D - Disease OBJECTIVES
 COPD C - Chronic O - Obstructive P - Pulmonary D - Disease 1 OBJECTIVES Following this presentation the participant should be able to demonstrate understanding of chronic lung disease by successful completion
COPD C - Chronic O - Obstructive P - Pulmonary D - Disease 1 OBJECTIVES Following this presentation the participant should be able to demonstrate understanding of chronic lung disease by successful completion
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide
 VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
Advances in Chronic Obstructive Pulmonary Disease
 Advances in Chronic Obstructive Pulmonary Disease By Dave C. Todd, MD; and Darcy D. Marciniuk, MD, FRCPC The case of Nina Nina, 64, presents to the clinic with a three- to fouryear history of progressive,
Advances in Chronic Obstructive Pulmonary Disease By Dave C. Todd, MD; and Darcy D. Marciniuk, MD, FRCPC The case of Nina Nina, 64, presents to the clinic with a three- to fouryear history of progressive,
COPD Treatable. Preventable.
 My COPD Action Plan Patient s Copy (Patient s Name) Date Canadian Respiratory COPD Treatable. Preventable. This is to tell me how I will take care of myself when I have a COPD flare-up. My goals are My
My COPD Action Plan Patient s Copy (Patient s Name) Date Canadian Respiratory COPD Treatable. Preventable. This is to tell me how I will take care of myself when I have a COPD flare-up. My goals are My
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
Conference Report. Chronic Obstructive Pulmonary Disease From a Payer and Provider Lens. Managed Care & Healthcare Communications, LLC
 AUTHOR Joseph Johnson, MD Chief Medical Officer Arizona Integrated Physicians PUBLISHING STAFF Senior Vice President, Clinical and Scientific Affairs Jeff Prescott, PharmD, RPh Clinical Projects Managers
AUTHOR Joseph Johnson, MD Chief Medical Officer Arizona Integrated Physicians PUBLISHING STAFF Senior Vice President, Clinical and Scientific Affairs Jeff Prescott, PharmD, RPh Clinical Projects Managers
Get Healthy Stay Healthy
 Asthma Management WHAT IS ASTHMA? Asthma causes swelling and inflammation in the breathing passages that lead to your lungs. When asthma flares up, the airways tighten and become narrower. This keeps the
Asthma Management WHAT IS ASTHMA? Asthma causes swelling and inflammation in the breathing passages that lead to your lungs. When asthma flares up, the airways tighten and become narrower. This keeps the
Course Handouts & Disclosure
 COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
COPD. The goals of COPD. about. you quit. If you. efforts to quit. Heart
 How Is COPD Treated? COPD has no cure yet. However, lifestyle changes and treatments can help you feel better, stay more active, and slow the progress of the disease. The goals of COPD treatment include:
How Is COPD Treated? COPD has no cure yet. However, lifestyle changes and treatments can help you feel better, stay more active, and slow the progress of the disease. The goals of COPD treatment include:
Fighting for Air, In Emphysema
 Fighting for Air, The Mechanism of Shortness of Breath In Emphysema Albert A. Rizzo, MD FCCP FACP Speaker, Nationwide Assembly of the American Lung Association & Section Chief Pulmonary/Critical Care Medicine
Fighting for Air, The Mechanism of Shortness of Breath In Emphysema Albert A. Rizzo, MD FCCP FACP Speaker, Nationwide Assembly of the American Lung Association & Section Chief Pulmonary/Critical Care Medicine
Asthma 2015: Establishing and Maintaining Control
 Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Chronic Obstructive Pulmonary Disease (COPD)
") Chronic Obstructive Pulmonary Disease (COPD) Health Promotion and Education Program Rev. 2014 2014, MMM Healthcare, Inc. - PMC Medicare Choice, Inc. Reproduction of this material is prohibited. MP-HEP-PPT-200-01-021914-E
Chronic Obstructive Pulmonary Disease (COPD) Health Promotion and Education Program Rev. 2014 2014, MMM Healthcare, Inc. - PMC Medicare Choice, Inc. Reproduction of this material is prohibited. MP-HEP-PPT-200-01-021914-E
COPD Management in LTC: Presented By: Jessica Denney RRT
 COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
written by Harvard Medical School COPD It Can Take Your Breath Away
 written by Harvard Medical School COPD It Can Take Your Breath Away www.patientedu.org What Is COPD? COPD stands for chronic obstructive pulmonary disease. There are 2 major diseases included in COPD:
written by Harvard Medical School COPD It Can Take Your Breath Away www.patientedu.org What Is COPD? COPD stands for chronic obstructive pulmonary disease. There are 2 major diseases included in COPD:
Asthma ASTHMA. Current Strategies for Asthma and COPD
 Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Known Allergies: Shellfish. Symptoms: abdominal pain, nausea, diarrhea, or vomiting. congestion, trouble breathing, or wheezing.
 CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
A Patient s Guide to Chronic Obstructive Pulmonary Disease (COPD)
") A Patient s Guide to Chronic Obstructive Pulmonary Disease (COPD) Table of Contents What is COPD? 2 How the Lungs Work 2 Lungs with Chronic Bronchitis 3 Lungs with Emphysema 4 Causes of COPD 4 COPD Symptoms
A Patient s Guide to Chronic Obstructive Pulmonary Disease (COPD) Table of Contents What is COPD? 2 How the Lungs Work 2 Lungs with Chronic Bronchitis 3 Lungs with Emphysema 4 Causes of COPD 4 COPD Symptoms
Integrated Cardiopulmonary Pharmacology Third Edition
 Integrated Cardiopulmonary Pharmacology Third Edition Chapter 13 Pharmacologic Management of Asthma, Chronic Bronchitis, and Emphysema Multimedia Directory Slide 7 Slide 12 Slide 60 COPD Video Passive
Integrated Cardiopulmonary Pharmacology Third Edition Chapter 13 Pharmacologic Management of Asthma, Chronic Bronchitis, and Emphysema Multimedia Directory Slide 7 Slide 12 Slide 60 COPD Video Passive
Curriculum Vitae. Head of Public Wing HCU - RSCM. Head of ICU Sari Asih Ciledug Hospital
 Curriculum Vitae Name : Dr. Ceva W. Pitoyo,SpPD,K-P,KIC,FINASIM POB / DOB : Jakarta, March 8th 1968 Education : o General Practitioner : FKUI 1993 o Internist : FKUI 2002 o Pulmonology Consultant : PAPDI-UI
Curriculum Vitae Name : Dr. Ceva W. Pitoyo,SpPD,K-P,KIC,FINASIM POB / DOB : Jakarta, March 8th 1968 Education : o General Practitioner : FKUI 1993 o Internist : FKUI 2002 o Pulmonology Consultant : PAPDI-UI
Cardiovascular and Respiratory Disorders
 Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
Bronchiectasis. What is bronchiectasis? What causes bronchiectasis?
 This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
Chronic Obstructive Pulmonary Disease, shortened to COPD, is an umbrella term for a group of conditions which cause long-term damage to the airways.
 10 Common QuESTIonS AbouT CoPD Chronic Obstructive Pulmonary Disease, shortened to COPD, is an umbrella term for a group of conditions which cause long-term damage to the airways. COPD includes: chronic
10 Common QuESTIonS AbouT CoPD Chronic Obstructive Pulmonary Disease, shortened to COPD, is an umbrella term for a group of conditions which cause long-term damage to the airways. COPD includes: chronic
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene
 Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
Healthy Lungs. Presented by: Brandi Bishop, RN and Patty Decker, RRT, RCP
 Healthy Lungs Presented by: Brandi Bishop, RN and Patty Decker, RRT, RCP Chronic Lower Respiratory Disease Chronic Lower Respiratory Disease includes 1. Chronic Obstructive Pulmonary Disease 2. Asthma
Healthy Lungs Presented by: Brandi Bishop, RN and Patty Decker, RRT, RCP Chronic Lower Respiratory Disease Chronic Lower Respiratory Disease includes 1. Chronic Obstructive Pulmonary Disease 2. Asthma
Function of the Respiratory System. Exchange CO2 (on expiration) for O2 (on inspiration)
 for O2 (on inspiration)") Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
MANAGING COPD AT HOME. Karla Schlichtmann, RRT
 MANAGING COPD AT HOME Karla Schlichtmann, RRT Chronic Obstructive Pulmonary Disease (COPD) is a progressive lung disease. WHAT IS COPD? The airways in your lungs become inflamed and thickens. This results
MANAGING COPD AT HOME Karla Schlichtmann, RRT Chronic Obstructive Pulmonary Disease (COPD) is a progressive lung disease. WHAT IS COPD? The airways in your lungs become inflamed and thickens. This results
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Chronic obstructive pulmonary disease: the management of adults with chronic obstructive pulmonary disease in primary and secondary
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Chronic obstructive pulmonary disease: the management of adults with chronic obstructive pulmonary disease in primary and secondary
MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C
 MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C Explain the importance of objective measures in the management of asthma Explain the different types of objective measures used in the management
MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C Explain the importance of objective measures in the management of asthma Explain the different types of objective measures used in the management
information Chronic Obstructive Pulmonary Disease - COPD (1 of 5) What is COPD? What is going on in my lungs? What are the symptoms of COPD?
 What is COPD? What is going on in my lungs? What are the symptoms of COPD?") information If you need this information in another language or medium (audio, large print, etc) please contact the Patient Advice and Liaison Service (PALS) on 0800 374 208 email: pal.service@ salisbury.nhs.uk.
information If you need this information in another language or medium (audio, large print, etc) please contact the Patient Advice and Liaison Service (PALS) on 0800 374 208 email: pal.service@ salisbury.nhs.uk.
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC
 KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC") Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Chronic Obstructive Pulmonary Disease (COPD) Measures Document
 Measures Document") Chronic Obstructive Pulmonary Disease (COPD) Measures Document COPD Version: 3 - covering patients discharged between 01/10/2017 and present. Programme Lead: Jo Higgins Clinical Lead: Dr Paul Albert Number
Chronic Obstructive Pulmonary Disease (COPD) Measures Document COPD Version: 3 - covering patients discharged between 01/10/2017 and present. Programme Lead: Jo Higgins Clinical Lead: Dr Paul Albert Number
A patient educational resource provided by Boehringer Ingelheim Pharmaceuticals, Inc.
 Boehringer Ingelheim Pharmaceuticals, Inc. has no ownership interest in any other organization that advertises or markets its disease management products and services. A patient educational resource provided
Boehringer Ingelheim Pharmaceuticals, Inc. has no ownership interest in any other organization that advertises or markets its disease management products and services. A patient educational resource provided
Treatment. Assessing the outcome of interventions Traditionally, the effects of interventions have been assessed by measuring changes in the FEV 1
 58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
The Respiratory System
 130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
Presented by the California Academy of Family Physicians 2013/California Academy of Family Physicians
 Family Medicine and Patient-Centered Asthma Care Presented by the California Academy of Family Physicians Faculty: Hobart Lee, MD Disclosures: Jeffrey Luther, MD, Program Director, Memorial Family Medicine
Family Medicine and Patient-Centered Asthma Care Presented by the California Academy of Family Physicians Faculty: Hobart Lee, MD Disclosures: Jeffrey Luther, MD, Program Director, Memorial Family Medicine
Reference Guide for Group Education
 A p l a n o f a c t i o n f o r l i f e Reference Guide for Group Education Session 5 Plan of Action: Part I Overview of the Plan of Action and Management of Respiratory Infections Plan of Action: Objectives
A p l a n o f a c t i o n f o r l i f e Reference Guide for Group Education Session 5 Plan of Action: Part I Overview of the Plan of Action and Management of Respiratory Infections Plan of Action: Objectives
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Clinical Practice Guideline: Asthma
 Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
AECOPD: Management and Prevention
 Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
CLINICAL PATHWAY. Acute Medicine. Chronic Obstructive Pulmonary Disease
 CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
UNDERSTANDING & MANAGING
 UNDERSTANDING & MANAGING YOUR CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD)* *Includes chronic bronchitis, emphysema, or both Boehringer Ingelheim Pharmaceuticals, Inc. has no ownership interest in any
UNDERSTANDING & MANAGING YOUR CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD)* *Includes chronic bronchitis, emphysema, or both Boehringer Ingelheim Pharmaceuticals, Inc. has no ownership interest in any
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016
 Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which