Shaping a Dynamic Future in Respiratory Practice. #DFResp
|
|
|
- Maximillian Burns
- 5 years ago
- Views:
Transcription

1 Shaping a Dynamic Future in Respiratory Practice #DFResp
2 Inhaled Therapy in COPD: Past, Present and Future Richard Russell Chest Physician West Hampshire Integrated Respiratory Service The views expressed in this presentation are those of the speaker and are not necessarily those of the meeting sponsors. This presentation may contain off-licence information. Please refer to the product SmPCs for the approved indication for use. UK/KOL/17/0008 Date of Preparation: February 2017
3 Disclosures: Who Boehringer Ingelheim GlaxoSmithKline Teva UK Limited AstraZeneca Pfizer Napp British Lung Foundation Editor at Int J COPD What Paid speaker Advisory boards Clinical trial investigator Travel support Support our patients! Increase our impact factor! I have no shares in pharmaceutical companies and do everything I can to hinder tobacco companies

4
5 ICS therapies in COPD, the past Numerous studies have looked at ICS therapies to improve outcomes in COPD - ISOLDE 1 - TORCH 2 - INSPIRE 3 - FORWARD 4 - BUD/FORM 5 1. Burge PS, et al. BMJ 2000 (FP vs Pla) 2. Calverley PM, et al. N Engl J Med 2007 (FP/Sal vs FP vs Sal vs Pla) 3. Wedzicha JA, et al. Am J Respir Crit Care Med 2008 (FP vs Pla) 4. Wedzicha JA, et al. Respir Med 2014 (BDP/FF vs FF) 5. Calverley PM, et al. ERJ 2003 (BUD/FORM vs BUD vs FORM vs Pla)
6 ICS monotherapy is more effective than placebo in stable COPD (ICS monotherapy is NOT licenced in COPD) Lung function Significant improvement of lung function vs placebo Use of ICS for > 6 months did not have a major effect on the rate of decline in FEV 1 (mean benefit of 5.80 ml/year with ICS over placebo, 95% CI: to 11.88, n=2333) Exacerbations Mortality Health status Reduced exacerbation rates (mean difference of exacerbations/patient/ year, 95% CI: to -0.14, n=2586) Increased risk of reported pneumonia No significant effects on mortality (OR: 0.98, 95% CI: 0.83 to 1.16, n=8390) Slowing of the rate of decline in QoL (improvement in SGRQ of 1.22 units/year, 95% CI: to -0.60, n=2507) Conclusions from a Cochrane systematic review of 55 primary studies published up to and including 2011 (n=16,154) Yang IA, et al. Cochrane Database Syst Rev 2012

7 Burge PS, et al. BMJ 2000
8 Rate of exacerbations vs placebo (%) ICS significantly reduces the rate of exacerbations needing medical intervention Szafranski 1 Calverley 2 Budesonide Formoterol 5 Budesonide Formoterol +3% 0-2% %* % * -20 *p<0.05 vs placebo -20 *p<0.05 vs placebo Fewer future attacks 1. Szafranski W, et al. Eur Respir J Calverley PM, et al. Eur Respir J 2003
9 mean exacerbation rate per patient per year Mean exacerbation rate per patient per year The risk of acute exacerbations in the TRISTAN study There were no differences between the three active treatment groups 1.5 TRISTAN Mahler and Hanania studies no significant differences between groups 0.00 Seretide Fluticasone Salmeterol placebo Seretide Fluticasone Salmeterol Placebo 1. Calverley PM, et al. Lancet 2003
10 Probability of death (%) The TORCH study: All-cause mortality at 3 years Placebo SALM FP SALM/FP Vertical bars are standard errors Number alive Time to death (weeks) Calverley PM, et al. N Engl J Med 2007
11 Mean number of exacerbations/year The TORCH study: Rate of moderate and severe exacerbations over 3 years * 0.93* *p<0.001 vs placebo Placebo SALM FP Treatment Calverley PM, et al. N Engl J Med 2007
12 Long-term inhaled steroids in COPD Trial n Duration Severity Outcome Copenhagen City years Mild No effect EUROSCOP years Mild No effect ISOLDE years Moderate No effect Lung Health years Moderate No effect 1 o outcome = decline in FEV 1 over 3 years Cochrane Review: >16,000 COPD patients - No FEV 1 decline - No mortality Yang IM, et al. 2012
13 What are we doing now? The present

14 Adapted from Gartlehner GG, et al. Ann Fam Med. 2006;4: Adapted COPD, from chronic Singh S, obstructive Loke YK. J COPD. pulmonary 2010;5: disease Potential Side Effects of COPD Therapy: ICS COPD: What is on our wish list? Unmet needs of patients with COPD Cataracts More effective diagnosis and primary prevention Better symptom control Rhinitis Fewer exacerbations Slowing of disease progression Sore throat Better life expectancy Increased bruising Unmet needs of the medical community Adverse effects on Optimising bone density/fracture disease prevention Increased intraocular pressure/glaucoma Oral Candidiasis Upper respiratory infection Less systemic disease secondary to COPD and fewer comorbidities Improving symptom control Pneumonia Preventing exacerbations and decreasing their clinical impact Preventing disease progression Reducing disease-related mortality Identifying systemic effects and comorbidities 1. Calverley PMA. Br J Pharmacol. 2008;155(4):
15 Modified version of the Fletcher and Peto graph showing the decline in FEV 1. FEV 1, forced expiratory volume in 1 second. Fletcher C, Peto R. BMJ 1977; 1: FEV 1 decline: The traditional view
16 FEV 1 (% predicted) FEV 1 decline: What is really going on? 100 Δ 40mL/yr GOLD 1 (mild) 80 Δ L/yr GOLD 2 (moderate) Δ 56 59mL/yr GOLD 3 (severe) Δ <35mL/yr GOLD 4 (very severe) Time since drug administration (hours) More recent analyses concluded that, in contrast with earlier findings, FEV 1 decline was fastest in the early stages of COPD, particularly in GOLD 2 disease FEV 1, forced expiratory volume in 1 second. Tantucci C, Modina D. Int J Chron Obstruct Pulmon Dis 2012; 7:
17 Affecting disease progression UPLIFT (subgroup) TORCH (subgroup) Real GOLD II FEV1 loss 61ml/year UPLIFT GOLD II loss 49ml/year UPLIFT GOLD III 38ml/year

18 Jenkins et al, Respiratory Research 2009; 10:59 TORCH study: FEV 1 loss
19 UPLIFT: GOLD II analysis n Tio ml/yr n Con ml/yr diff (CI) p Decamer et al. Lancet ,9696;
20 Decamer et al. Lancet ,9696; How do patients feel?

21 Decamer et al. Lancet ,9696; UPLIFT: GOLD II exacerbations


22 Paradigm of COPD management is shifting Global Initiative for Chronic Obstructive Lung Disease. Revised Available at:









23 High levels of off-guidelines ICS use worldwide* USA Western Europe South America Other 28% 47% 41% 24% Patients at GOLD Stage II with no history of exacerbations in the past year who were receiving ICS at baseline on enrolment *Data from 11 studies in 44 countries with a total of 9482 patients Yawn D, et al. Am J Resp Crit Care Med 2012;185:A2944 (Abstract).
24 So what are we doing now? It seems almost random: Population database study n=24,957-17% no treatment - 24% ICS - 26% ICS/LABA - 23% ICS, LABA, LAMA - 2% LAMA alone Irrespective of GOLD stage or GOLD group (A-D) Price D, et al. Int J Chron Obstruct Pulmon Dis 2014;9:

25 NICE Clinical Guidance (2010) When the 2010 guideline was being written, the available evidence for LABA plus LAMA combination therapy was relatively limited. As the NICE guidelines are purely evidence-based, the recommendation for LABA plus LAMA therapy is restricted in the 2010 guideline. Adapted from NICE. COPD pathway updated Sept (last accessed November 2014)
26 Expiratory flow limitation has systemic effects in COPD COPD Exacerbations Expiratory flow limitations Air trapping/ hyperinflation Breathlessness Deconditioning HRQoL Inactivity Reduced exercise capacity Disability Progression: decline in lung function Mortality Ferro TJ. Clinical Pulmonary Medicine 2005;12(4 Suppl):S13-S15; Decramer M. Eur Respir Rev 2006;15(99): COPD, chronic obstructive pulmonary disease; HRQoL, health-related quality of life
 Delays onset of dyspnoea when")
27 Bronchodilation and its consequences Relaxation of ASM Not the same as increased radius from reduction in oedema/cells Change in the degree/location of EFL Reduced static hyperinflation (EELV) Delays onset of dyspnoea when exercising

28 Beta-agonists and muscarinic antagonists


29 Anticholinergics HENBANE Deadly Nightshade






30 LAMA
31 Change from baseline in FEV 1 (L) Duration of action of tiotropium FEV 1 time profile (0-12 hours), test day Time after dose administration (hours) Tiotropium Respimat 5µg (n=187) Tiotropium Respimat 10µg (n=179) Tiotropium HandiHaler 18µg (n=186) Placebo (n=181) Van Noord DE, et al. Respir Med 2009;103:22-29.
32 Twice daily LAMA therapy
33 Trough FEV 1 (L) Effects of aclidinium on FEV 1 : ACCLAIM COPD trial results 1.5 Aclidinium 200µg Placebo p<0.05 p<0.001 p<0.001 p< p<0.001 p<0.001 p<0.001 p< ACCLAIM/ COPD I ACCLAIM/ COPD II ACCLAIM/ COPD I ACCLAIM/ COPD II ACCLAIM/ COPD I ACCLAIM/ COPD II ACCLAIM/ COPD I Week 4 Week 12 Week 28 Week 52 ACCLAIM/ COPD II Jones PW, et al. Respir Res 2011;12:55
34 Percent with moderate or severe exacerbations Effects of aclidinium on FEV 1 : ACCLAIM COPD trial results 45% 40% 35% 30% 25% 20% 15% 10% 5% 0% 26.60% Aclidinium ACCLAIM COPD I p= % Placebo 33.20% ACCLAIM COPD II p= % n=627 n=216 n=600 n=204 FEV 1, forced expiratory volume in 1 second Adapted from Jones PW, et al. Respir Res 2011;12:55
35 Long-term impact on health status Activity Tiotropium Control Symptoms Impact Troosters T, et al. Eur Respir J. 2010;36:65-73.


36 LABA
 Cote C et al.")
37 Formoterol has a significantly faster onset of action versus salmeterol (data presented after 28 days treatment) Cote C et al. Pulmonary Pharmacology & Therapeutics 2009; 22: 44 49
38 Trough FEV 1 (L) Indacaterol provided significant sustained improvement in trough FEV 1 over 26 weeks versus placebo and salmeterol Placebo Indacaterol 150µg o.d. Salmeterol 50µg b.i.d *** 1.42 *** 1.43 *** 1.39 *** 1.45 *** 1.36 *** ***p<0.001 vs placebo; p<0.001 vs salmeterol Data are LSM Day 2 Week 12 Week 26 Primary endpoint Kornmann et al. Eur Respir J 2011; Kornmann et al. ACCP 2009
39 Trough FEV 1 response, L FEV 1 AUC 0-3 response, L Olodaterol 5 and 10μg improve mean FEV 1 AUC 0-3h and trough FEV 1 responses over 48 weeks similarly Statistically significant at 12 weeks Studies.11/.12 Placebo Olodaterol 5µg Olodaterol 10µg Statistically significant at 24 weeks Studies.13/ Data on file. Studies ; ; Weeks Weeks Common baseline mean (standard error): Studies 11/12: (0.014); Studies 13/14: (0.011). Analysis with imputation (full analysis set). AUC0-3h, area under the plasma concentration time curve from 0 to 3 hours; FEV 1, forced expiratory volume in 1 second
40 LAMA/LABA
41 Short-acting 2-agonists versus anticholinergics D FEV 1 (%) Day 1 Day Ipratropium 36µg Salbutamol 200µg Both drugs combined Hours after test dose Combivent Study Group, Chest 1994; 105:1411
 55µg")


 340µg aclidinium 12µg")


42 Dual bronchodilators for COPD Anoro Ellipta (VIL/UMEC) 55µg umeclidinium 22µg vilanterol One inhalation Once daily Spiolto Respimat 2.5µg tiotropium 2.5µg olodaterol Two inhalations Once daily Duaklir Genuair (ACL/FORM) 340µg aclidinium 12µg formoterol One inhalation Twice daily Ultibro Breezhaler 50µg glycopyrronium 110µg indacaterol One inhalation Once daily SPCs accessed at [Accessed Jan 2016]
43 FEV 1 (L) 24-hour FEV 1 profile after six weeks of treatment significant improvements in lung function versus monotherapy and placebo T+O FDC 5/5µg AUC 0-3h 338mL Trough 207mL* 24-hour FEV1 profile Time since drug administration (hours) *Difference between T+O FDC 5/5µg and placebo Tiotropium 2.5μg Tiotropium 5μg Placebo Olodaterol 5μg Tiotropium+olodaterol FDC 2.5/5μg Tiotropium+olodaterol FDC 5/5μg Beeh KM et al. Pulm Pharmacol Ther 2015; DOI /j.pupt )

44 Change from baseline in pre-morning dose lung function (trough FEV 1 ) at Week 24: pooled data ACL/FORM significantly improved lung function pre-morning dose compared with aclidinium or formoterol

45 VIL/UMEC 55/22mcg improves lung function compared with TIO Primary endpoint: Trough FEV 1 at day 169 ZEP11711 DB DB Maleki-Yazdi MR, Kaelin T, Richard N, Zvarich M, Church A. Efficacy and safety of umeclidinium/vilanterol 62.5/25 mcg and tiotropium 18 mcg in COPD: results of a 24-week, randomized controlled trial. Respir Med. 2014;108(12): Decramer et al. Lancet Resp Med 2014 ; Vol 2 No. 6 pp
46 (L) VIVACITO: Adjusted mean IC, TLC, FRC and RV response (L) at 2:30 post-dose after six weeks treatment :30 hours after dosing Placebo Olo 5 Tio 2.5 Tio 5 T+O 2.5/5 T+O 5/5 IC * TLC * * * FRC * * RV FDC always superior over placebo. *Indicates additional superiority over at least one of the monotherapies. FDC, fixed-dose combination; FRC, functional residual capacity; IC, inspiratory capacity; L, litres; O/Olo, olodaterol; RV, residual volume; T/Tio, tiotropium; TLC, total lung capacity. 1. Beeh KM, et al. Pulm Pharmacol Ther 2015; May 6. pii: S (15) doi: /j.pupt

47 Rates of exacerbations at week 24: pooled data ACL/FORM was associated a statistically significant reduction of 29% in the rate of moderate or severe exacerbations AstraZeneca. Data on File: ABF/023/Jan15.
48 Probability of moderate/ severe exacerbation Exacerbations: Probability of moderate/severe exacerbations Tiotropium+olodaterol 2.5/5μg Tiotropium+olodaterol 5/5μg Tiotropium 2.5μg Olodaterol 5μg Tiotropium 5μg BI data on file. Studies /.6 combined dataset Test day Numbers at risk T+O 5/5 µg T+O 2.5/5 µg Tiotropium 5 µg Tiotropium 2.5 µg Olodaterol 5 µg

49
 Superiority margin Non-inferiority margin Per-protocol set (Primary analysis) 0.83 0.89 0.96 p=0.003 Modified intention-to-treat set (Supportive analysis) 0.82 0.88 0.94 p<0.")
50 FLAME is the first study to demonstrate superiority of indacaterol/glycopyrronium (Ultibro Breezhaler ) in exacerbation prevention versus SFC in COPD patients with 1 exacerbation in the preceding year Rate ratio (95% Cl) Superiority margin Non-inferiority margin Per-protocol set (Primary analysis) p=0.003 Modified intention-to-treat set (Supportive analysis) p< Favours IND/GLY Favours SFC Ultibro Breezhaler was non-inferior (primary endpoint) and superior to SFC for the rate of all (mild/moderate/severe) exacerbations over 52 weeks Wedzicha JA, et al. N Engl J Med 2016
51 Updated treatment algorithm in GOLD 2017
52 When should ICS be used in the management of COPD? The Future
53

54 EVIDENCE UNCERTAINTY EVIDENCE UNCERTAINTY UNCERTAINTY EVIDENCE UNCERTAINTY UNCERTAINTY EVIDENCE UNCERTAINTY
55 When should we use ICS in COPD? My view Disclaimer the views represented are those of the speaker and his appraisal of current evidence; they are likely to be biased and may not be the TRUTH Personal expert opinion Richard Russell
 Further exacerbation(s) LAMA + LABA + ICS LAMA + LABA Consider macrolide (in former smokers) Group D Persistent symptoms / further")
56 Group C Further exacerbation(s) LAMA + LABA LAMA GOLD recommendations for COPD treatment LABA + ICS Consider roflumilast if FEV 1 <50% pred. and patient has chronic bronchitis LAMA Further exacerbation(s) Further exacerbation(s) LAMA + LABA + ICS LAMA + LABA Consider macrolide (in former smokers) Group D Persistent symptoms / further exacerbation(s) LABA + ICS Group A Continue, stop or try alternative class of bronchodilator LAMA + LABA Group B Evaluate effect Persistent symptoms A bronchodilator A long-acting bronchodilator (LABA or LAMA) Preferred treatment In patients with a major discrepancy between the perceived level of symptoms and severity of airflow limitation, further evaluation is warranted Global Initiative for Chronic Obstructive Lung Disease, all rights reserved. Use is by express license from the owner. From the Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) Available from:
57 When should we use inhaled steroids in COPD? Consider use in GOLD groups C and D For patients with frequent exacerbations and poor lung function Do they help promote maximal bronchodilatation when added to LAMA/LABA? ICS can be withdrawn I make a positive decision to start ICS; it is NOT a default Personal expert opinion Richard Russell
58 Suissa S, et al. Thorax 2013 Pneumonia risk with ICS

59 Suissa S. Thorax Jun;68(6): doi: /thoraxjnl NNT and NNH for inhaled corticosteroids
60 Potential risks of ICS use Randomised controlled trial Observational study Systematic review Pneumonia Tuberculosis Bone fracture Skin thinning/easy bruising Cataract Diabetes No effect on fracture risk Oropharyngeal candidiasis Price D, et al. Prim Care Respir J 2013;22:92 100
61 New GOLD D: A treatable trait approach Several options are available if: Patient on LAMA/LABA Still exacerbating Poor lung function (<50%) 1. ICS: with eosinophils 2. Roflumilast: if chronic bronchitis and emphysema and BMI >23 3. Macrolide therapy: if not smoking (bronchiectasis, check microbiology) Role of therapeutic trial Non-eosinophilic Neutrophilic Personal expert opinion Richard Russell
62 The blood eosinophil count: reducing risk and ICS in COPD
63 Exacerbation rate INSPIRE 1 Blood eosinophils in COPD & ICS: reducing risk Randomised, double-blind, parallel-group, double-dummy study with either salmeterol/fluticasone propionate 50/500µg twice daily (n=658) or tiotropium bromide 18µg once daily (n=665) for 2 years Primary endpoint of health care utilisation exacerbation rate not different % diff p=0.006 SFC 50/500 Tio 18µg % diff p= n=263 n=287 n=371 n=348 EOS <2% EOS 2% 1. Wedzicha JA, et al. Am J Respir Crit Care Med Barnes N, et al. Am J Respir Crit Care Med 2015;191:A3975, poster 612

64 Blood eosinophils in COPD & ICS: reducing risk The effect of addition of fluticasone furoate (FF) to vilanterol (VI) HZC and HZC studies; safety and efficacy study 1 To determine if the combination of FF and VI is more protective than VI alone against COPD exacerbations; more AE, however, reanalysis by eos 2 42% diff 24% diff 32% diff 10% diff 1. Dransfield MT, et al. Lancet Respir Med Pascoe S, et al. Lancet Respir Med 2015

65 Blood eosinophils in COPD & ICS: reducing risk FORWARD Safety and efficacy of BDP/FORM vs FORM 1 Reduction in exacerbation rate in 3 rd and 4 th eosinophil quartile 2 1. Wedzicha JA, et al. Respir Med Siddiqui SH, et al. Am J Respir Crit Care Med 2015
66 Change from baseline pre-bronchodilator FEV 1 (ml) Blood eosinophils in COPD & ICS: reducing risk ISOLDE 1 Randomised, double-blind, parallel-group study with either fluticasone propionate 500µg twice daily (n=376) or placebo (n=375) for 3 years No difference in primary outcome of rate of FEV1 decline (ml/year), until analysed by Eos <2% 2% Difference=3.8mL/year p=0.616 Difference=37.7mL/year p= Treatment Placebo FP Burge PS, et al. BMJ Barnes N, et al. ATS 2015,p 613, AJRCCM 191, A Month
67 NEJM ICS (n=1243) ICS withdrawal (n=1242) Male, % Mean (SD) age, years 63.6 (8.6) 64.0 (8.4) Mean (SD) body mass index, kg/m (5.1) 25.2 (5.1) Current smoker, % Mean (SD) duration of COPD, years 7.8 (6.0) 8.0 (6.5) Lung function Mean (SD) post-dose screening FEV 1, L FEV 1 30 <50% (GOLD 3), n (%) FEV 1 <30% (GOLD 4), n (%) Mean (SD) baseline FEV 1, L* *After 6-week run-in on triple therapy 0.93 (0.29) 760 (61.1) 473 (38.1) 0.97 (0.36) 0.94 (0.30) 761 (61.3) 474 (38.2) 0.98 (0.36)

68 *p<0.05; **p<0.01. Watz et al., ATS 2016 Abstract 6944 Eosinophils and ICS
69 REAL-WORLD WISDOM sub-analysis: ICS withdrawal only EVIDENCE MONOTHERAPY COMBINATION WITHDRAWAL increased WISDOM the exacerbation subanalysis: rate in patients with the combination of raised eosinophil counts and frequent exacerbations HOME GUIDELINES SAFETY ALTERNATIVES ICS withdrawal only increased the exacerbation rate in patients with the combination of raised eosinophil counts and frequent exacerbations Patients, n Hazard ratio of exacerbations in patients with 300 or 400 cells/µl and <2 or 2 previous exacerbations HR 95% CI P-value Total 2441 Screening eosinophils , cells/µl < 2 exacerbations 2 exacerbations , , cells/µl < 2 exacerbations 2 exacerbations , , Favours ICS withdrawal Favours ICS Calverley PMA, et al. ERS 2016 oral presentation. Calverley PMA, et al. ERS 2016 oral presentation 63

70 WISDOM sub-analysis: Only a small subset of clearly identifiable patients may benefit from adding ICS to LAMA/LABA ICS may provide incremental benefit only in patients who meet 3 criteria 1. Severe/very severe COPD This is only 7% of the entire WISDOM study population 2. A history of 2 exacerbations/year 3. Blood eosinophil levels 300 cells/µl 1. Watz H, et al. Lancet Respir Med Calverley PMA, et al. ERS 2016 oral presentation
71 Differential treatment effect by blood eosinophil counts: anti IL-5Rα in eosinophilic COPD Change in FEV 1 (L) n= n=28 n=31 n=34 n=31 n=35 n= Blood eosinophil count (cell/µl) Brightling CE, et al. Lancet Respir Med 2014
72 Using the blood eosinophil count to guide ICS treatment in COPD The blood eosinophil count as a biomarker in COPD: - Relevant and valid Easily accessible Repeatable Identifies risk o Type and frequency of exacerbations o Mortality o Infection Personal expert opinion Richard Russell
73 Using the blood eosinophil count to guide ICS treatment in COPD The PBE: Predicts who can be taken off ICS (and who should not!) Predicts who should receive ICS - To reduce risk of exacerbation Predicts who will respond to new biological agents PBE, Percentage blood eosinophils Personal expert opinion Richard Russell
74 What about ACO? My view: - Truly try to diagnose asthma - Give steroids for a positive reason - Trial of treatment - Appropriate detailed testing Treatable trait approach will supersede labels Personal expert opinion Richard Russell

75 Choice is good Choice

76
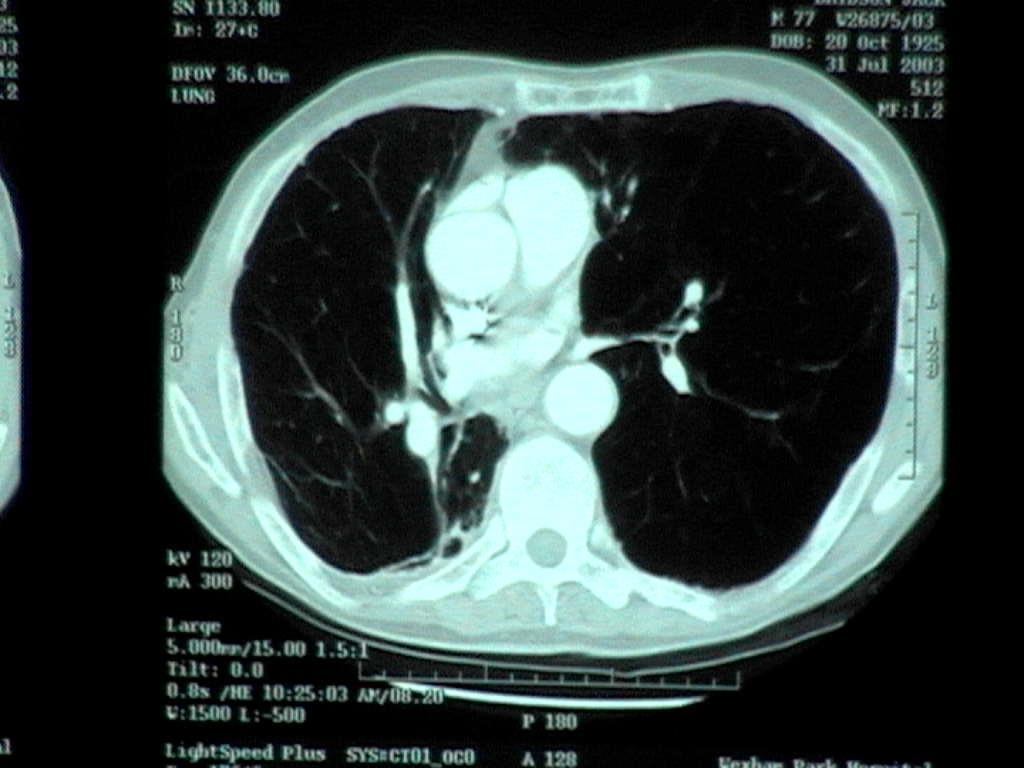
77 55-year-old man Ex-lorry driver Presented to GP with SOB Smoker 70 pack years GP worried by breathlessness and young age thus sent for specialist opinion

78 The CXR What is abnormal? A. Flat diaphragms B. Hyperlucency C. Consolidation D. Cardiomegaly Answers: 1. A,B,C,D 2. A,B 3. C 4. Normal CXR
79
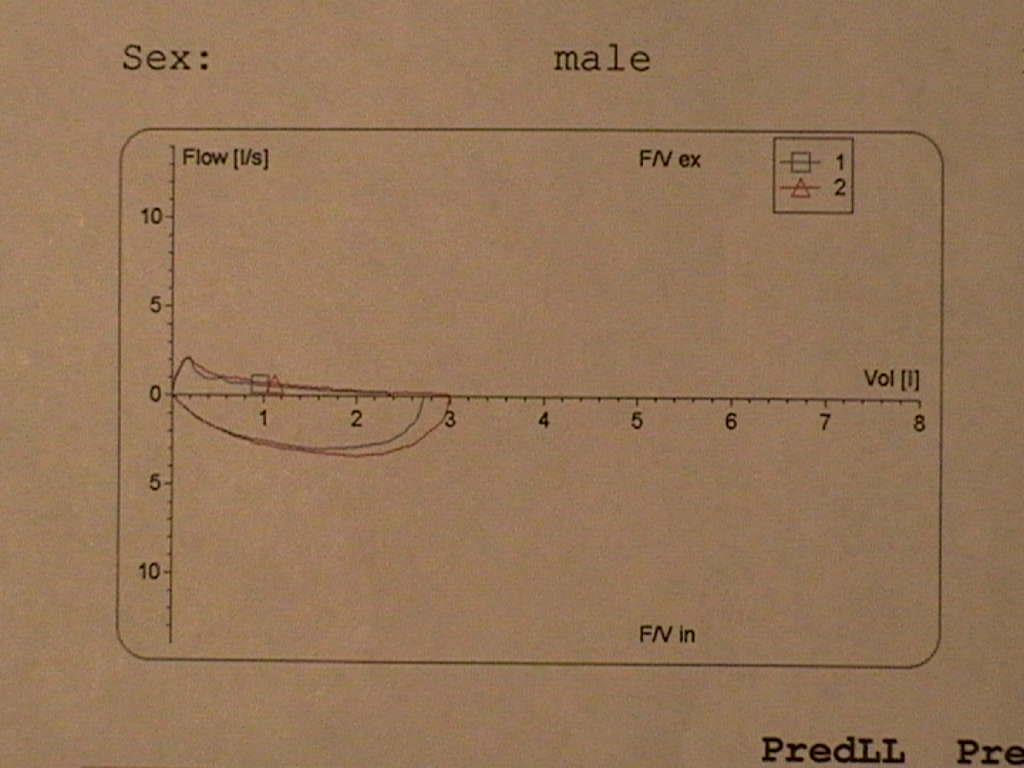
80 What will his spirometry show? 1. Fixed airway obstruction 2. Extra-thoracic obstruction 3. Restriction 4. Reversible airway obstruction
81
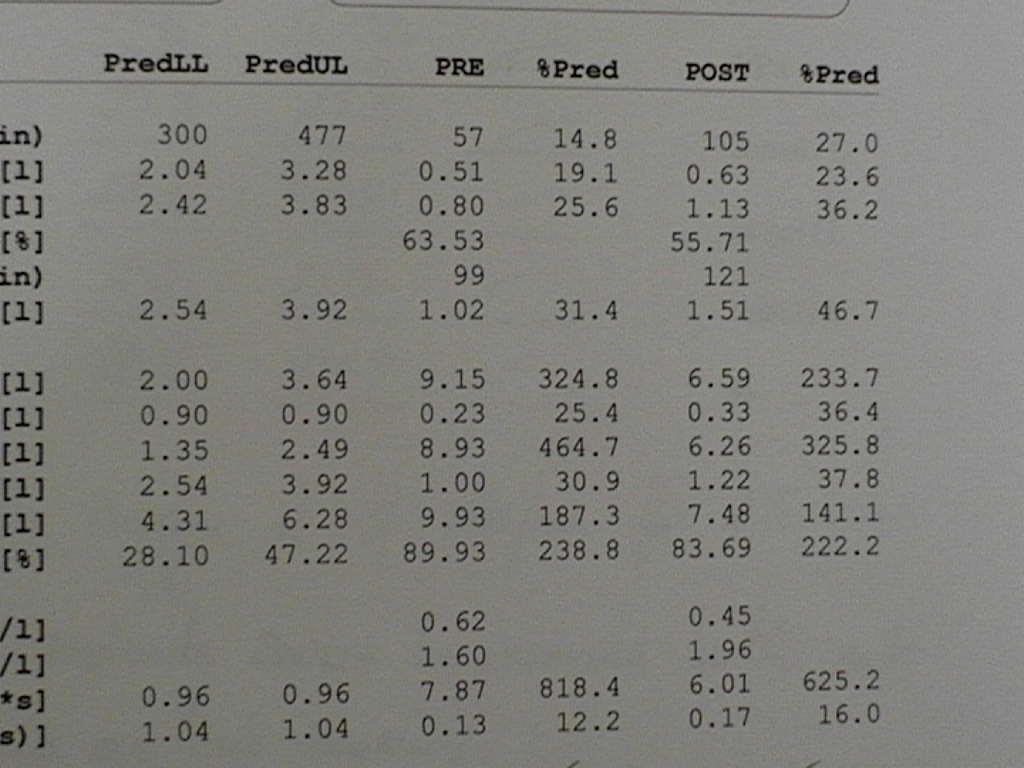
82
83 Diagnosis Severe emphysema Gas trapping Reversible hyperinflation
84 What are the treatment options? 1. Inhaled corticosteroids 2. Inhaled LABA 3. LAMA 4. LABA/LAMA combination 5. ICS/LABA 6. Lung volume reduction surgery
85 Management Check A1AT Eosinophil count Assess for LTOT Pulmonary rehabilitation Maximise therapy LABA/LAMA Consider LVRS/bullectomy/single lung transplantation
86 Progress Low eosinophils: Commenced on tiotropium/olodaterol therapy Completed pulmonary rehabilitation Maximised exercise tolerance Now runs Marathons!

87
88 How to treat COPD Diagnose early and stop smoking Bronchodilate to the maximum: - LAMA; LAMA/LABA Assess risk - Exacerbation - CVS Give inhaled steroids to the RIGHT patients (eos) Pulmonary rehabilitation for all
89

90
Shaping a Dynamic Future in Respiratory Practice. #DFResp
 Shaping a Dynamic Future in Respiratory Practice #DFResp www.dynamicfuture.co.uk Inhaled Therapy in COPD: Past, Present and Future Richard Russell Chest Physician West Hampshire Integrated Respiratory
Shaping a Dynamic Future in Respiratory Practice #DFResp www.dynamicfuture.co.uk Inhaled Therapy in COPD: Past, Present and Future Richard Russell Chest Physician West Hampshire Integrated Respiratory
Potential risks of ICS use
 Potential risks of ICS use Randomised controlled trial Observational study Systematic review Pneumonia Tuberculosis Bone fracture Skin thinning/easy bruising Cataract Diabetes No effect on fracture risk
Potential risks of ICS use Randomised controlled trial Observational study Systematic review Pneumonia Tuberculosis Bone fracture Skin thinning/easy bruising Cataract Diabetes No effect on fracture risk
Choosing an inhaler for COPD made simple. Dr Simon Hart Castle Hill Hospital
 Choosing an inhaler for COPD made simple Dr Simon Hart Castle Hill Hospital 1 Declaration of interests I have received speaker fees, sponsorship to attend conferences, and funding for research from companies
Choosing an inhaler for COPD made simple Dr Simon Hart Castle Hill Hospital 1 Declaration of interests I have received speaker fees, sponsorship to attend conferences, and funding for research from companies
รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น
 รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น COPD Guideline Changing concept in COPD management Evidences that we can offer COPD patients better life COPD Guidelines
รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น COPD Guideline Changing concept in COPD management Evidences that we can offer COPD patients better life COPD Guidelines
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university
 What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
Changing Landscapes in COPD New Zealand Respiratory Conference
 Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
COPD: Treatment Update Property of Presenter. Not for Reproduction. Barry Make, MD Professor of Medicine National Jewish Health
 COPD: Treatment Update Barry Make, MD Professor of Medicine National Jewish Health Disclosures Advisory board, consultant, multi-center trial, research funding, Data Safety Monitoring Board (DSMB), or
COPD: Treatment Update Barry Make, MD Professor of Medicine National Jewish Health Disclosures Advisory board, consultant, multi-center trial, research funding, Data Safety Monitoring Board (DSMB), or
Pharmacotherapy for COPD
 10/3/2017 Topics to be covered Pharmacotherapy for chronic treatment Pharmacotherapy for COPD Dr. W C Yu 3rd September 2017 Commonly used drugs Guidelines for their use Inhaled corticosteroids (ICS) in
10/3/2017 Topics to be covered Pharmacotherapy for chronic treatment Pharmacotherapy for COPD Dr. W C Yu 3rd September 2017 Commonly used drugs Guidelines for their use Inhaled corticosteroids (ICS) in
Treatment Responses. Ronald Dahl, Aarhus University Hospital, Denmark
 Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Optimum treatment for chronic obstructive pulmonary disease exacerbation prevention
 Commentary Page 1 of 5 Optimum treatment for chronic obstructive pulmonary disease exacerbation prevention Pradeep Karur, Dave Singh Centre for Respiratory Medicine and Allergy, Medicines Evaluation Unit,
Commentary Page 1 of 5 Optimum treatment for chronic obstructive pulmonary disease exacerbation prevention Pradeep Karur, Dave Singh Centre for Respiratory Medicine and Allergy, Medicines Evaluation Unit,
TORCH: Salmeterol and Fluticasone Propionate and Survival in COPD
 TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD)
") Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) Zahava Picado, PharmD PGY1 Pharmacy Practice Resident Central Texas Veterans Healthcare System Temple, TX October
Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) Zahava Picado, PharmD PGY1 Pharmacy Practice Resident Central Texas Veterans Healthcare System Temple, TX October
Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management. Colleen Sakon, PharmD BCPS September 27, 2018
 Management. Colleen Sakon, PharmD BCPS September 27, 2018") Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management Colleen Sakon, PharmD BCPS September 27, 2018 Disclosures I have no actual or potential conflicts of interest 2 Objectives Summarize
Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management Colleen Sakon, PharmD BCPS September 27, 2018 Disclosures I have no actual or potential conflicts of interest 2 Objectives Summarize
Surveillance report Published: 6 April 2016 nice.org.uk. NICE All rights reserved.
 Surveillance report 2016 Chronic obstructive pulmonary disease in over 16s: diagnosis and management (2010) NICE guideline CG101 Surveillance report Published: 6 April 2016 nice.org.uk NICE 2016. All rights
Surveillance report 2016 Chronic obstructive pulmonary disease in over 16s: diagnosis and management (2010) NICE guideline CG101 Surveillance report Published: 6 April 2016 nice.org.uk NICE 2016. All rights
Disease progression in COPD:
 Disease progression in COPD: What is it? How should it be measured? Can it be modified? Professor Paul Jones MD, PhD, FERS Emeritus Professor of Respiratory Medicine; St George s, University of London
Disease progression in COPD: What is it? How should it be measured? Can it be modified? Professor Paul Jones MD, PhD, FERS Emeritus Professor of Respiratory Medicine; St George s, University of London
Dr Stephen Child. General Physician Auckland. 14:20-14:40 Secondary Care Perspective
 Dr Stephen Child General Physician Auckland 14:20-14:40 Secondary Care Perspective Wheeze Witchery Stephen Child MD, FRACP, FRCPC General Physician Respiratory Interest Director of Clinical Training Auckland
Dr Stephen Child General Physician Auckland 14:20-14:40 Secondary Care Perspective Wheeze Witchery Stephen Child MD, FRACP, FRCPC General Physician Respiratory Interest Director of Clinical Training Auckland
Three better than 1 or 2?
 Three better than 1 or 2? DISCLOSURE Pam McLean-Veysey, Team Leader Drug Evaluation Unit DEU funded by the Drug Evaluation Alliance of NS. (DEANS). DEU prepares Drug Evaluation Reports for the Atlantic
Three better than 1 or 2? DISCLOSURE Pam McLean-Veysey, Team Leader Drug Evaluation Unit DEU funded by the Drug Evaluation Alliance of NS. (DEANS). DEU prepares Drug Evaluation Reports for the Atlantic
Three s Company - The role of triple therapy in chronic obstructive pulmonary
 Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) October 26 th, 2018 Zahava Picado, PharmD PGY1 Pharmacy Resident Central Texas Veterans Healthcare System Zahava.Picado@va.gov
Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) October 26 th, 2018 Zahava Picado, PharmD PGY1 Pharmacy Resident Central Texas Veterans Healthcare System Zahava.Picado@va.gov
umeclidinium/vilanterol, 55/22 micrograms, inhalation powder (Anoro ) SMC No. (978/14) GlaxoSmithKline
 SMC No. (978/14) GlaxoSmithKline") umeclidinium/vilanterol, 55/22 micrograms, inhalation powder (Anoro ) SMC No. (978/14) GlaxoSmithKline 04 July 2014 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
umeclidinium/vilanterol, 55/22 micrograms, inhalation powder (Anoro ) SMC No. (978/14) GlaxoSmithKline 04 July 2014 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
Advancing COPD treatment strategies with evidencebased. 17:15 19:15 Monday 11 September 2017 ERS 2017, Milan, Italy
 Advancing COPD treatment strategies with evidencebased approaches 17:15 19:15 Monday 11 September 2017 ERS 2017, Milan, Italy Increasing understanding of COPD and the effect on guideline evolution. GOLD
Advancing COPD treatment strategies with evidencebased approaches 17:15 19:15 Monday 11 September 2017 ERS 2017, Milan, Italy Increasing understanding of COPD and the effect on guideline evolution. GOLD
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015
 David CL Lam Department of Medicine University of Hong Kong October, 2015") Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
NEW OPTIONS FOR OPTIMAL BRONCHODILATION IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 NEW OPTIONS FOR OPTIMAL BRONCHODILATION IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE *Caroline Charles Scilink Medical Writing *Correspondence to scilink.mw@gmail.com Disclosure: Medical writing assistance
NEW OPTIONS FOR OPTIMAL BRONCHODILATION IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE *Caroline Charles Scilink Medical Writing *Correspondence to scilink.mw@gmail.com Disclosure: Medical writing assistance
Management of COPD Updates and Evidence
 Management of COPD Updates and Evidence Providence Alaska Medical Center PGY1 Pharmacy Practice Residents Ann-Chee Cheng, PharmD Kaite Kammers, PharmD http://www.fpnotebook.com/_media/lungxsgraybb962.gif
Management of COPD Updates and Evidence Providence Alaska Medical Center PGY1 Pharmacy Practice Residents Ann-Chee Cheng, PharmD Kaite Kammers, PharmD http://www.fpnotebook.com/_media/lungxsgraybb962.gif
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC
 KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC") Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
UPDATE IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 UPDATE IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE Radhika Shah, MD Erlanger Health System University of Tennessee College of Medicine Chattanooga Respiratory, Critical Care, and Sleep medicine No disclosures
UPDATE IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE Radhika Shah, MD Erlanger Health System University of Tennessee College of Medicine Chattanooga Respiratory, Critical Care, and Sleep medicine No disclosures
aclidinium 322 micrograms inhalation powder (Eklira Genuair ) SMC No. (810/12) Almirall S.A.
 SMC No. (810/12) Almirall S.A.") aclidinium 322 micrograms inhalation powder (Eklira Genuair ) SMC No. (810/12) Almirall S.A. 05 October 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and
aclidinium 322 micrograms inhalation powder (Eklira Genuair ) SMC No. (810/12) Almirall S.A. 05 October 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and
Defining COPD. Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist
 Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
COPD The New Epidemic. Peter Lin MD CCFP Director Primary Care Initiatives Canadian Heart Research Centre
 COPD The New Epidemic Peter Lin MD CCFP Director Primary Care Initiatives Canadian Heart Research Centre Conflict Disclosure Information Speaker: Dr. Peter Lin Title of Talk: COPD The New Epidemic Financial
COPD The New Epidemic Peter Lin MD CCFP Director Primary Care Initiatives Canadian Heart Research Centre Conflict Disclosure Information Speaker: Dr. Peter Lin Title of Talk: COPD The New Epidemic Financial
Design Treatment arms Duration Primary endpoint N. Indacaterol 150. Glycopyrronium 50, Tiotropium 18 (openlabel) Placebo. Placebo
 Placebo. Placebo") 1 S1 Table. Selected studies and methodology of the different clinical trials. Indacaterol/glycopyrronium Design Treatment arms Duration Primary endpoint N Bateman ED, et al. ERJ 2013 [1] SHINE Dahl R,
1 S1 Table. Selected studies and methodology of the different clinical trials. Indacaterol/glycopyrronium Design Treatment arms Duration Primary endpoint N Bateman ED, et al. ERJ 2013 [1] SHINE Dahl R,
Wirral COPD Prescribing Guidelines
 Wirral COPD Prescribing Guidelines (To be read in conjunction with the Wirral COPD Supplementary Information) STEP 1: Assess symptoms COPD Assessment Test (CAT) [Link for CAT-test Online] is a patient-completed
Wirral COPD Prescribing Guidelines (To be read in conjunction with the Wirral COPD Supplementary Information) STEP 1: Assess symptoms COPD Assessment Test (CAT) [Link for CAT-test Online] is a patient-completed
Adjunct Associate Professor Robert Young
 Adjunct Associate Professor Robert Young General Physician Auckland City Hospital 7:00-7:55 GlaxoSmithKline Breakfast Session - COPD New approaches in the management of COPD Dr Robert Young BMedSc MBChB
Adjunct Associate Professor Robert Young General Physician Auckland City Hospital 7:00-7:55 GlaxoSmithKline Breakfast Session - COPD New approaches in the management of COPD Dr Robert Young BMedSc MBChB
Test Your Inhaler Knowledge
 A Breath of Fresh Air: Updates in COPD Management Jennifer Austin Szwak, PharmD, BCPS, DPLA University of Chicago Medicine The speaker has nothing to disclose Abbreviations COPD: Chronic obstructive pulmonary
A Breath of Fresh Air: Updates in COPD Management Jennifer Austin Szwak, PharmD, BCPS, DPLA University of Chicago Medicine The speaker has nothing to disclose Abbreviations COPD: Chronic obstructive pulmonary
umeclidinium, 55 micrograms, powder for inhalation (Incruse ) SMC No. (1004/14) GlaxoSmithKline
 SMC No. (1004/14) GlaxoSmithKline") umeclidinium, 55 micrograms, powder for inhalation (Incruse ) SMC No. (1004/14) GlaxoSmithKline 07 November 2014 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
umeclidinium, 55 micrograms, powder for inhalation (Incruse ) SMC No. (1004/14) GlaxoSmithKline 07 November 2014 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
NHS Dumfries & Galloway Triple therapy in COPD patients over 16 years
 Title of Project: NHS Dumfries & Galloway Triple therapy in COPD patients over 16 years 1 Reason for the review Respiratory prescribing is long term and can be costly. Appropriate choice and use of inhaled
Title of Project: NHS Dumfries & Galloway Triple therapy in COPD patients over 16 years 1 Reason for the review Respiratory prescribing is long term and can be costly. Appropriate choice and use of inhaled
New Medicines Committee Briefing July Glycopyrronium bromide/indacaterol (Ultibro ) for maintenance treatment of adults with stable COPD
 for maintenance treatment of adults with stable COPD") Ultibro is to be reviewed for use within: New Medicines Committee Briefing July 2017 Glycopyrronium bromide/indacaterol (Ultibro ) for maintenance treatment of adults with stable COPD Summary: Primary
Ultibro is to be reviewed for use within: New Medicines Committee Briefing July 2017 Glycopyrronium bromide/indacaterol (Ultibro ) for maintenance treatment of adults with stable COPD Summary: Primary
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) TREATMENT GUIDELINES
 TREATMENT GUIDELINES") CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) TREATMENT GUIDELINES Document Description Document Type Service Application Version Guidelines All healthcare professionals(hcps) caring for patients with asthma
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) TREATMENT GUIDELINES Document Description Document Type Service Application Version Guidelines All healthcare professionals(hcps) caring for patients with asthma
Presenter Disclosure Information
 12:45 1:3 pm Improving Outcomes in COPD SPEAKER Michael Campos, MD Presenter Disclosure Information The following relationships exist related to this presentation: Michael Campos, MD: No financial relationships
12:45 1:3 pm Improving Outcomes in COPD SPEAKER Michael Campos, MD Presenter Disclosure Information The following relationships exist related to this presentation: Michael Campos, MD: No financial relationships
glycopyrronium 44 micrograms hard capsules of inhalation powder (Seebri Breezhaler ) SMC No. (829/12) Novartis Pharmaceuticals Ltd.
 SMC No. (829/12) Novartis Pharmaceuticals Ltd.") glycopyrronium 44 micrograms hard capsules of inhalation powder (Seebri Breezhaler ) SMC No. (829/12) Novartis Pharmaceuticals Ltd. 07 December 2012 The Scottish Medicines Consortium (SMC) has completed
glycopyrronium 44 micrograms hard capsules of inhalation powder (Seebri Breezhaler ) SMC No. (829/12) Novartis Pharmaceuticals Ltd. 07 December 2012 The Scottish Medicines Consortium (SMC) has completed
Medicines Management of Chronic Obstructive Pulmonary Disease (COPD)
") Medicines Management of Chronic Obstructive Pulmonary Disease (COPD) (Chronic & Acute) Guidelines for Primary Care Guideline Authors: Shaneez Dhanji (Wandsworth CCG) Samantha Prigmore (St George s Hospital)
Medicines Management of Chronic Obstructive Pulmonary Disease (COPD) (Chronic & Acute) Guidelines for Primary Care Guideline Authors: Shaneez Dhanji (Wandsworth CCG) Samantha Prigmore (St George s Hospital)
COPD EXACERBATIONS AND HOSPITAL ADMISSIONS HOW CAN WE PREVENT THEM? Wisia Wedzicha National Heart and Lung Institute, Imperial College London, UK
 COPD EXACERBATIONS AND HOSPITAL ADMISSIONS HOW CAN WE PREVENT THEM? Wisia Wedzicha National Heart and Lung Institute, Imperial College London, UK Presenter Disclosures Wisia Wedzicha All disclosures prior
COPD EXACERBATIONS AND HOSPITAL ADMISSIONS HOW CAN WE PREVENT THEM? Wisia Wedzicha National Heart and Lung Institute, Imperial College London, UK Presenter Disclosures Wisia Wedzicha All disclosures prior
If you require this document in another format such as Braille, large print, audio or another language please contact the Trusts Communications Team
 MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
GOLD 2017: cosa c è di nuovo
 GOLD 2017: cosa c è di nuovo Antonio Spanevello Università degli Studi dell Insubria, Varese Dipartimento di Medicina e Chirurgia Istituti Clinici Scientifici Maugeri, IRCCS, Tradate Dipartimento di Medicina
GOLD 2017: cosa c è di nuovo Antonio Spanevello Università degli Studi dell Insubria, Varese Dipartimento di Medicina e Chirurgia Istituti Clinici Scientifici Maugeri, IRCCS, Tradate Dipartimento di Medicina
COPD Importance of Symptoma3c Control. Dr James Calvert FRCP PhD MPH Respiratory Physician North Bristol NHS Trust
 COPD Importance of Symptoma3c Control Dr James Calvert FRCP PhD MPH Respiratory Physician North Bristol NHS Trust Introduc3on Symptoms and outcomes in COPD Right drug, right pabent using LAMA/LABA Drug
COPD Importance of Symptoma3c Control Dr James Calvert FRCP PhD MPH Respiratory Physician North Bristol NHS Trust Introduc3on Symptoms and outcomes in COPD Right drug, right pabent using LAMA/LABA Drug
COPD: Preventable and Treatable. Lecture Outline. Diagnosis of COPD. COPD: Defining Terms
 COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
NEWER BRONCHODILATORS. Dr R Lakshmi Narasimhan SR Pulmonary Medicine
 NEWER BRONCHODILATORS Dr R Lakshmi Narasimhan SR Pulmonary Medicine Topics to be covered Ultra LABA (+/-ICS) Newer LAMA LAMA + LABA Novel Bronchodilators Why the need for newer BD? OD dosing convenient
NEWER BRONCHODILATORS Dr R Lakshmi Narasimhan SR Pulmonary Medicine Topics to be covered Ultra LABA (+/-ICS) Newer LAMA LAMA + LABA Novel Bronchodilators Why the need for newer BD? OD dosing convenient
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Calverley P M A, Anzueto A R, Carter K, et
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Calverley P M A, Anzueto A R, Carter K, et
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Dr Stephen Child. Chief Medical Officer Southern Cross Health Society Auckland
 Dr Stephen Child Chief Medical Officer Southern Cross Health Society Auckland 7:00-7:55 GlaxoSmithKline Breakfast Session - Hot Topics in Airways Disease: COPD and Asthma Hot Topics in Airways Disease:
Dr Stephen Child Chief Medical Officer Southern Cross Health Society Auckland 7:00-7:55 GlaxoSmithKline Breakfast Session - Hot Topics in Airways Disease: COPD and Asthma Hot Topics in Airways Disease:
2017 GOLD Report. Is it worth its weight in GOLD??? CSHP-NB Fall Education Day September 30, 2017
 2017 GOLD Report Is it worth its weight in GOLD??? CSHP-NB Fall Education Day September 30, 2017 Lauren Munro; BSc(Pharm) Amanda Burns; BSc(Pharm) Pharmacy Residents The Moncton Hospital Objectives Explain
2017 GOLD Report Is it worth its weight in GOLD??? CSHP-NB Fall Education Day September 30, 2017 Lauren Munro; BSc(Pharm) Amanda Burns; BSc(Pharm) Pharmacy Residents The Moncton Hospital Objectives Explain
Evidence Summary to support COPD formulary decision making and guideline development
 Evidence Summary to support COPD formulary decision making and guideline development Prescribing and adverse event reporting information can be found on the final pages of this document. Anoro, and Ellipta
Evidence Summary to support COPD formulary decision making and guideline development Prescribing and adverse event reporting information can be found on the final pages of this document. Anoro, and Ellipta
Evidence Summary to support COPD formulary decision making and guideline development
 Evidence Summary to support COPD formulary decision making and guideline development Prescribing and adverse event reporting information can be found on the final page of this document. Trelegy and Ellipta
Evidence Summary to support COPD formulary decision making and guideline development Prescribing and adverse event reporting information can be found on the final page of this document. Trelegy and Ellipta
Address Comorbidities
 Greater Manchester COPD Management Plan Non-pharmacological management for ALL patients Smoking Cessation Annual Flu Vaccination Pulmonary Rehabilitation Increase daily activity Inhaler Technique Measure
Greater Manchester COPD Management Plan Non-pharmacological management for ALL patients Smoking Cessation Annual Flu Vaccination Pulmonary Rehabilitation Increase daily activity Inhaler Technique Measure
Chronic Obstructive Pulmonary Disease: What s New in Therapeutic Management?
 Chronic Obstructive Pulmonary Disease: What s New in Therapeutic Management? Sabrina Sherwood, PharmD PGY2 Internal Medicine Resident University of Utah Health September 29, 2018 Disclosures Relevant disclosures
Chronic Obstructive Pulmonary Disease: What s New in Therapeutic Management? Sabrina Sherwood, PharmD PGY2 Internal Medicine Resident University of Utah Health September 29, 2018 Disclosures Relevant disclosures
Class Update: Asthma / COPD Medications
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
COPD Therapeutic Update
 COPD Therapeutic Update The first ever NT patient.. Hubertus PA Jersmann MBBS, MD, PhD, FRACP, FThorSoc, AMA(M) Professor, School of Medicine, University of Adelaide Respiratory and Sleep Physician, Royal
COPD Therapeutic Update The first ever NT patient.. Hubertus PA Jersmann MBBS, MD, PhD, FRACP, FThorSoc, AMA(M) Professor, School of Medicine, University of Adelaide Respiratory and Sleep Physician, Royal
CHARM Guidelines for the diagnosis and
 \ CHARM Guidelines for the diagnosis and management of COPD City and Hackney CCG Homerton University Hospital NHS Foundation Trust Written by: Miss Hetal Dhruve, Specialist Pharmacist Respiratory Medicine,
\ CHARM Guidelines for the diagnosis and management of COPD City and Hackney CCG Homerton University Hospital NHS Foundation Trust Written by: Miss Hetal Dhruve, Specialist Pharmacist Respiratory Medicine,
SABA: VENTOLIN EVOHALER (SALBUTAMOL) SAMA: ATROVENT IPRATROPIUM. Offer LAMA (discontinue SAMA) OR LABA
 SAMA: ATROVENT IPRATROPIUM. Offer LAMA (discontinue SAMA) OR LABA") COPD GUIDELINES DIAGNOSIS >35 years of age Symptoms of cough, breathlessness, sputum, wheeze, Risk factor (SMOKING) Spirometry (post bronchodilator) FEV1/FVC = 0.7 ENCOURAGE PATIENTS TO BRING INHALERS
COPD GUIDELINES DIAGNOSIS >35 years of age Symptoms of cough, breathlessness, sputum, wheeze, Risk factor (SMOKING) Spirometry (post bronchodilator) FEV1/FVC = 0.7 ENCOURAGE PATIENTS TO BRING INHALERS
Turning Science into Real Life Roflumilast in Clinical Practice. Roland Buhl Pulmonary Department Mainz University Hospital
 Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
The Journal Club: COPD Exacerbations
 252 The Journal Club: COPD Exacerbations Chronic Obstructive Pulmonary Diseases: Journal of the COPD Foundation Journal Club The Journal Club: COPD Exacerbations Ron Balkissoon, MD, MSc, DIH, FRCPC 1 Abbreviations:
252 The Journal Club: COPD Exacerbations Chronic Obstructive Pulmonary Diseases: Journal of the COPD Foundation Journal Club The Journal Club: COPD Exacerbations Ron Balkissoon, MD, MSc, DIH, FRCPC 1 Abbreviations:
THE COPD PRESCRIBING TOOL
 THE COPD PRESCRIBING TOOL Revised edition, 2017 www.bpac.org.nz/copd CLASSIFICATION The COPD prescribing tool This tool provides pharmacological treatment options for patients with COPD based on their
THE COPD PRESCRIBING TOOL Revised edition, 2017 www.bpac.org.nz/copd CLASSIFICATION The COPD prescribing tool This tool provides pharmacological treatment options for patients with COPD based on their
11/27/18. Challenges in Pulmonary and Critical Care: COPD So Much is New! Faculty. Disclosures
 Challenges in Pulmonary and Critical Care: 2018 COPD So Much is New! 1 Faculty Anas Hadeh, MD, FCCP Director, Pulmonary and Critical Care Medicine Fellowship Program Affiliate Assistant Professor of Clinical
Challenges in Pulmonary and Critical Care: 2018 COPD So Much is New! 1 Faculty Anas Hadeh, MD, FCCP Director, Pulmonary and Critical Care Medicine Fellowship Program Affiliate Assistant Professor of Clinical
Controversies in Clinical Trials
 Controversies in Clinical Trials Christopher B Cooper, MD Professor of Medicine and Physiology David Geffen School of Medicine Medical Director, UCLA COPD Center Methodological issues discussed Pitfalls
Controversies in Clinical Trials Christopher B Cooper, MD Professor of Medicine and Physiology David Geffen School of Medicine Medical Director, UCLA COPD Center Methodological issues discussed Pitfalls
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
April 10 th, Bond Street, Toronto ON, M5B 1W8
 Comprehensive Research Plan: Inhaled long-acting muscarinic antagonists (LAMAs; long-acting anticholinergics) for the treatment of chronic obstructive pulmonary disease (COPD) April 10 th, 2014 30 Bond
Comprehensive Research Plan: Inhaled long-acting muscarinic antagonists (LAMAs; long-acting anticholinergics) for the treatment of chronic obstructive pulmonary disease (COPD) April 10 th, 2014 30 Bond
Model based longitudinal metaanalysis of FEV1 in COPD trials A tool for efficacy benchmarking
 Model based longitudinal metaanalysis of FEV1 in COPD trials A tool for efficacy benchmarking Julia Korell (1), Steven W. Martin (2), Mats O. Karlsson (1), Jakob Ribbing (1,3) (1) Uppsala University, Sweden
Model based longitudinal metaanalysis of FEV1 in COPD trials A tool for efficacy benchmarking Julia Korell (1), Steven W. Martin (2), Mats O. Karlsson (1), Jakob Ribbing (1,3) (1) Uppsala University, Sweden
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE
 BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE December 2014 Review date: December 2017 Bulletin 208 : Indacaterol + Glycopyrronium bromide 85/43 micrograms (Ultibro Breezhaler ) for the Treatment
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE December 2014 Review date: December 2017 Bulletin 208 : Indacaterol + Glycopyrronium bromide 85/43 micrograms (Ultibro Breezhaler ) for the Treatment
Blood Eosinophils and Response to Maintenance COPD Treatment: Data from the FLAME Trial. Online Data Supplement
 Blood Eosinophils and Response to Maintenance COPD Treatment: Data from the FLAME Trial Nicolas Roche, Kenneth R. Chapman, Claus F. Vogelmeier, Felix JF Herth, Chau Thach, Robert Fogel, Petter Olsson,
Blood Eosinophils and Response to Maintenance COPD Treatment: Data from the FLAME Trial Nicolas Roche, Kenneth R. Chapman, Claus F. Vogelmeier, Felix JF Herth, Chau Thach, Robert Fogel, Petter Olsson,
Research Review. Salmeterol/fluticasone propionate (Seretide ) in COPD. Extended listing for salmeterol/fluticasone propionate in COPD
 in COPD. Extended listing for salmeterol/fluticasone propionate in COPD") Research Review Salmeterol/fluticasone propionate (Seretide ) in COPD Extended listing for salmeterol/fluticasone propionate in COPD In New Zealand, salmeterol/fluticasone propionate (SFC) (Seretide )
Research Review Salmeterol/fluticasone propionate (Seretide ) in COPD Extended listing for salmeterol/fluticasone propionate in COPD In New Zealand, salmeterol/fluticasone propionate (SFC) (Seretide )
Lead team presentation: Roflumilast for treating chronic obstructive pulmonary disease [ID984]
![Lead team presentation: Roflumilast for treating chronic obstructive pulmonary disease [ID984]](/thumbs/85/91889043.jpg "Lead team presentation: Roflumilast for treating chronic obstructive pulmonary disease [ID984]") Lead team presentation: Roflumilast for treating chronic obstructive pulmonary disease [ID984] 1 st Appraisal Committee meeting Background & Clinical Effectiveness John McMurray 11 th January 2016 For
Lead team presentation: Roflumilast for treating chronic obstructive pulmonary disease [ID984] 1 st Appraisal Committee meeting Background & Clinical Effectiveness John McMurray 11 th January 2016 For
Curriculum Vitae. Head of Public Wing HCU - RSCM. Head of ICU Sari Asih Ciledug Hospital
 Curriculum Vitae Name : Dr. Ceva W. Pitoyo,SpPD,K-P,KIC,FINASIM POB / DOB : Jakarta, March 8th 1968 Education : o General Practitioner : FKUI 1993 o Internist : FKUI 2002 o Pulmonology Consultant : PAPDI-UI
Curriculum Vitae Name : Dr. Ceva W. Pitoyo,SpPD,K-P,KIC,FINASIM POB / DOB : Jakarta, March 8th 1968 Education : o General Practitioner : FKUI 1993 o Internist : FKUI 2002 o Pulmonology Consultant : PAPDI-UI
Journal of the COPD Foundation. Impact of the IMPACT Trial Ron Balkissoon, MD, MSc, DIH, FRCPC 1. Chronic Obstructive Pulmonary Diseases: Journal Club
 221 Journal Club: The IMPACT Trial Chronic Obstructive Pulmonary Diseases: Journal of the COPD Foundation Journal Club Impact of the IMPACT Trial Ron Balkissoon, MD, MSc, DIH, FRCPC 1 Abbreviations: Global
221 Journal Club: The IMPACT Trial Chronic Obstructive Pulmonary Diseases: Journal of the COPD Foundation Journal Club Impact of the IMPACT Trial Ron Balkissoon, MD, MSc, DIH, FRCPC 1 Abbreviations: Global
Chronic obstructive pulmonary disease (COPD) is characterized
 is characterized") DANIEL E. HILLEMAN, PharmD ABSTRACT OBJECTIVE: To review the role of long-acting bronchodilators in the treatment of chronic obstructive pulmonary disease (COPD), including the importance of treatment
DANIEL E. HILLEMAN, PharmD ABSTRACT OBJECTIVE: To review the role of long-acting bronchodilators in the treatment of chronic obstructive pulmonary disease (COPD), including the importance of treatment
Re-Submission. roflumilast, 500 microgram, film-coated tablet (Daxas ) SMC No 635/10 AstraZeneca UK Ltd. Published 11 September
 SMC No 635/10 AstraZeneca UK Ltd. Published 11 September") Re-Submission roflumilast, 500 microgram, film-coated tablet (Daxas ) SMC No 635/10 AstraZeneca UK Ltd 4 August 2017 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
Re-Submission roflumilast, 500 microgram, film-coated tablet (Daxas ) SMC No 635/10 AstraZeneca UK Ltd 4 August 2017 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
Aclidinium Bromide: Clinical Benefit in Patients with Moderate to Severe COPD
 Send Orders of Reprints at bspsaif@emirates.net.ae 150 The Open Respiratory Medicine Journal, 2012, 6, 150-154 Aclidinium Bromide: Clinical Benefit in Patients with Moderate to Severe COPD Charlotte Suppli
Send Orders of Reprints at bspsaif@emirates.net.ae 150 The Open Respiratory Medicine Journal, 2012, 6, 150-154 Aclidinium Bromide: Clinical Benefit in Patients with Moderate to Severe COPD Charlotte Suppli
Preventing clinically important deterioration with single-inhaler triple therapy in COPD
 ORIGINAL ARTICLE COPD Preventing clinically important deterioration with single-inhaler triple therapy in COPD Ian Naya 1, Chris Compton 1, Afisi S. Ismaila 2,3, Ruby Birk 4, Noushin Brealey 4, Maggie
ORIGINAL ARTICLE COPD Preventing clinically important deterioration with single-inhaler triple therapy in COPD Ian Naya 1, Chris Compton 1, Afisi S. Ismaila 2,3, Ruby Birk 4, Noushin Brealey 4, Maggie
Goals and Learning Objectives
 Small Airways (SAW) Symposium: Asthma Treatment Issues. New Bronchodilator for Asthma: A Patient Centric Approach for Treating Asthma Stephen P. Peters, MD, PhD, FAAAAI, FACP, FCCP, FCPP Thomas H. Davis
Small Airways (SAW) Symposium: Asthma Treatment Issues. New Bronchodilator for Asthma: A Patient Centric Approach for Treating Asthma Stephen P. Peters, MD, PhD, FAAAAI, FACP, FCCP, FCPP Thomas H. Davis
Blood eosinophil count: a biomarker of an important treatable trait in patients with airway disease
 EDITORIAL COPD Blood eosinophil count: a biomarker of an important treatable trait in patients with airway disease Ian D. Pavord 1 and Alvar Agusti 2 Affiliations: 1 Respiratory Medicine Unit, Nuffield
EDITORIAL COPD Blood eosinophil count: a biomarker of an important treatable trait in patients with airway disease Ian D. Pavord 1 and Alvar Agusti 2 Affiliations: 1 Respiratory Medicine Unit, Nuffield
HSN S FORMULARY ALTERNATIVES FOR STABLE COPD. Which drug comes with which device?
 HSN S FORMULARY ALTERNATIVES FOR STABLE COPD Which drug comes with which device? Long-Acting Bronchodilators LAMAs LABAs LONG ACTING MUSCARINIC ANTAGONISTS Blocks acetylcholine-mediated bronchoconstriction
HSN S FORMULARY ALTERNATIVES FOR STABLE COPD Which drug comes with which device? Long-Acting Bronchodilators LAMAs LABAs LONG ACTING MUSCARINIC ANTAGONISTS Blocks acetylcholine-mediated bronchoconstriction
Common Drug Review Pharmacoeconomic Review Report
 Common Drug Review Pharmacoeconomic Review Report January 2018 Drug umeclidinium bromide (Incruse Ellipta) Indication Listing request Dosage form(s) Manufacturer Indicated for long-term, once daily maintenance
Common Drug Review Pharmacoeconomic Review Report January 2018 Drug umeclidinium bromide (Incruse Ellipta) Indication Listing request Dosage form(s) Manufacturer Indicated for long-term, once daily maintenance
Nuovi farmaci in sviluppo per la BPCO
 PNEUMOLOGIA 2018 MILANO, 14 16 GIUGNO 2018 CENTRO CONGRESSI PALAZZO DELLE STELLINE Nuovi farmaci in sviluppo per la BPCO Leonardo M. Fabbri, MD, FERS Professor of Respiratory and Internal Medicine, University
PNEUMOLOGIA 2018 MILANO, 14 16 GIUGNO 2018 CENTRO CONGRESSI PALAZZO DELLE STELLINE Nuovi farmaci in sviluppo per la BPCO Leonardo M. Fabbri, MD, FERS Professor of Respiratory and Internal Medicine, University
COPD Update. Plus New and Improved Products for Inhaled Therapy. Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor
 COPD Update Plus New and Improved Products for Inhaled Therapy Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose concerning possible financial
COPD Update Plus New and Improved Products for Inhaled Therapy Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose concerning possible financial
COPD Medications Coverage Summary Non-Insured Health Benefits Coverage SABA Bricanyl turbuhaler Yes Yes
 COPD Medications Coverage Summary Drug Non-Insured Health Benefits Coverage SABA Bricanyl turbuhaler Yes Yes Ventolin MDI + generics Yes Yes Ventolin Diskus NO NO Yukon Pharmacare/Chronic Disease Program
COPD Medications Coverage Summary Drug Non-Insured Health Benefits Coverage SABA Bricanyl turbuhaler Yes Yes Ventolin MDI + generics Yes Yes Ventolin Diskus NO NO Yukon Pharmacare/Chronic Disease Program
Ultra LABAs in COPD. Puneet Saxena
 Ultra LABAs in COPD Puneet Saxena Changing the Natural History Smoking cessation LTOT LVRS in selected patients Pharmacotherapy? Anthonisen NR. The lung health study. JAMA. 1994 Nocturnal Oxygen Therapy
Ultra LABAs in COPD Puneet Saxena Changing the Natural History Smoking cessation LTOT LVRS in selected patients Pharmacotherapy? Anthonisen NR. The lung health study. JAMA. 1994 Nocturnal Oxygen Therapy
AWMSG SECRETARIAT ASSESSMENT REPORT. Glycopyrronium bromide (Seebri Breezhaler ) 44 micrograms inhalation powder as hard capsules
 44 micrograms inhalation powder as hard capsules") AWMSG SECRETARIAT ASSESSMENT REPORT Glycopyrronium bromide (Seebri Breezhaler ) 44 micrograms inhalation powder as hard capsules Reference number: 1455 FULL SUBMISSION This report has been prepared by
AWMSG SECRETARIAT ASSESSMENT REPORT Glycopyrronium bromide (Seebri Breezhaler ) 44 micrograms inhalation powder as hard capsules Reference number: 1455 FULL SUBMISSION This report has been prepared by
Original. Showa Univ J Med Sci 30 2, , June 2018
 Showa Univ J Med Sci 30 2, 159 174, June 2018 Original Efficacy and Safety of Long-acting Beta-2 Agonist and Long-acting Muscarinic Antagonist Combinations in Patients with Chronic Obstructive Pulmonary
Showa Univ J Med Sci 30 2, 159 174, June 2018 Original Efficacy and Safety of Long-acting Beta-2 Agonist and Long-acting Muscarinic Antagonist Combinations in Patients with Chronic Obstructive Pulmonary
Medicines Management Programme Inhaled Medicines for Chronic Obstructive Pulmonary Disease (COPD)
") Medicines Management Programme Inhaled Medicines for Chronic Obstructive Pulmonary Disease (COPD) Approved by Prof. Michael Barry, Clinical Lead, MMP. Date approved Version 1 July 2014 Date updated Version
Medicines Management Programme Inhaled Medicines for Chronic Obstructive Pulmonary Disease (COPD) Approved by Prof. Michael Barry, Clinical Lead, MMP. Date approved Version 1 July 2014 Date updated Version
What is COPD? COPD Pharmacotherapy. COPD Mortality Is Increasing
 COPD Pharmacotherapy Chronic Bronchitis What is COPD? 75% 17.5% Emphysema Laura C. Feemster, MD, MS Assistant Professor University of Washington Division of Pulmonary & Critical Care April 23,2015 COPD
COPD Pharmacotherapy Chronic Bronchitis What is COPD? 75% 17.5% Emphysema Laura C. Feemster, MD, MS Assistant Professor University of Washington Division of Pulmonary & Critical Care April 23,2015 COPD
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research
 Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data. The synopsis
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data. The synopsis
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE
 BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE Bulletin 218: September 2015 Review Date: September 2018 LAMA / LABA combination inhalers in COPD- Place in therapy review and choice of therapy JPC Recommendations:
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE Bulletin 218: September 2015 Review Date: September 2018 LAMA / LABA combination inhalers in COPD- Place in therapy review and choice of therapy JPC Recommendations:
Algorithm for the use of inhaled therapies in COPD Version 2 May 2017
 Algorithm for the use of inhaled therapies in COPD This document has been revised by the Berkshire West Respiratory Network to support clinicians in selecting the most appropriate, cost effective treatments
Algorithm for the use of inhaled therapies in COPD This document has been revised by the Berkshire West Respiratory Network to support clinicians in selecting the most appropriate, cost effective treatments
COPD is a significant cause of mortality
 RESPIRATORY CLINICAL FOCUS Comparing the range and costs of COPD treatments in primary care Practice nurses should familiarise themselves with the many products available for the management of chronic
RESPIRATORY CLINICAL FOCUS Comparing the range and costs of COPD treatments in primary care Practice nurses should familiarise themselves with the many products available for the management of chronic
Algorithm for the use of inhaled therapies in COPD
 Berkshire West Integrated Care System Representing Berkshire West Clinical Commisioning Group Royal Berkshire NHS Foundation Trust Berkshire Healthcare NHS Foundation Trust Berkshire West Primary Care
Berkshire West Integrated Care System Representing Berkshire West Clinical Commisioning Group Royal Berkshire NHS Foundation Trust Berkshire Healthcare NHS Foundation Trust Berkshire West Primary Care
Not available 100/6mcg 2 BD formoterol (Fostair MDI) 100/6mcg 33
 100/6mcg 33") COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP FLUTICASONE FUROATE/VILANTEROL COMBINATION INHALER - ASTHMA Policy agreed by Vale of York CCG (date) Drug, Treatment, Device name Fluticasone
COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP FLUTICASONE FUROATE/VILANTEROL COMBINATION INHALER - ASTHMA Policy agreed by Vale of York CCG (date) Drug, Treatment, Device name Fluticasone
COPD Robert Schilz DO, PhD Pulmonary, Critical Care and Sleep Medicine University Hospitals Case Medical Center
 COPD 2018 GOLD 2017 Report Global Initiative for Chronic Obstructive Lung D isease COPYRIGHTED MATERIAL- DO NOT COPY OR DISTRIBUTE GLOBAL STRATEGY FOR THE DIAGNOSIS, MANAGEMENT, AND PREVENTION OF CHRONIC
COPD 2018 GOLD 2017 Report Global Initiative for Chronic Obstructive Lung D isease COPYRIGHTED MATERIAL- DO NOT COPY OR DISTRIBUTE GLOBAL STRATEGY FOR THE DIAGNOSIS, MANAGEMENT, AND PREVENTION OF CHRONIC
Confronting the Challenges of COPD. What is New in The Approaches to Diagnosis, Treatment, and Patient Outcomes
 Confronting the Challenges of COPD What is New in The Approaches to Diagnosis, Treatment, and Patient Outcomes COPD Definition GOLD: Global Initiative for Chronic Obstructive Lung Disease Common, preventable,
Confronting the Challenges of COPD What is New in The Approaches to Diagnosis, Treatment, and Patient Outcomes COPD Definition GOLD: Global Initiative for Chronic Obstructive Lung Disease Common, preventable,
Addressing Undertreatment
 Objectives TOWARD BETTER COPD OUTCOMES The Critical Role of Primary Care for Early Diagnosis and Guideline-directed Management Keith Robinson, MD, MS, FCCP Pulmonary Physicians of South Florida, LLC Fusion
Objectives TOWARD BETTER COPD OUTCOMES The Critical Role of Primary Care for Early Diagnosis and Guideline-directed Management Keith Robinson, MD, MS, FCCP Pulmonary Physicians of South Florida, LLC Fusion
CDEC FINAL RECOMMENDATION
 CDEC FINAL RECOMMENDATION (FLUTICASONE FUROATE/VILANTEROL) (Breo Ellipta GlaxoSmithKline) Indication: Chronic Obstructive Pulmonary Disease Recommendation: The Canadian Drug Expert Committee (CDEC) recommends
CDEC FINAL RECOMMENDATION (FLUTICASONE FUROATE/VILANTEROL) (Breo Ellipta GlaxoSmithKline) Indication: Chronic Obstructive Pulmonary Disease Recommendation: The Canadian Drug Expert Committee (CDEC) recommends
AWMSG SECRETARIAT ASSESSMENT REPORT. Aclidinium bromide (Eklira Genuair ) 322 micrograms inhalation powder. Reference number: 938 FULL SUBMISSION
 322 micrograms inhalation powder. Reference number: 938 FULL SUBMISSION") AWMSG SECRETARIAT ASSESSMENT REPORT Aclidinium bromide (Eklira Genuair ) 322 micrograms inhalation powder Reference number: 938 FULL SUBMISSION This report has been prepared by the All Wales Therapeutics
AWMSG SECRETARIAT ASSESSMENT REPORT Aclidinium bromide (Eklira Genuair ) 322 micrograms inhalation powder Reference number: 938 FULL SUBMISSION This report has been prepared by the All Wales Therapeutics
Evidence Review for Prescribing Clinical Network
 Summary page Evidence Review for Prescribing Clinical Network Treatment: LABA/LAMA Combination devices in COPD Anoro Ellipta, Ultibro and Duaklir Genuair Prepared by: Noreen Devanney Topic Submitted by:
Summary page Evidence Review for Prescribing Clinical Network Treatment: LABA/LAMA Combination devices in COPD Anoro Ellipta, Ultibro and Duaklir Genuair Prepared by: Noreen Devanney Topic Submitted by: