Practice Guideline for the Treatment of Patients With Major Depressive Disorder: American Psychiatric Association
|
|
|
- Regina Victoria Taylor
- 5 years ago
- Views:
Transcription
1 Practice Guideline for the Treatment of Patients With Major Depressive Disorder: American Psychiatric Association Our clinical advisor adds updated advice on electroconvulsive therapy, transcranial magnetic stimulation, lithium, light therapy, sleep hygiene, and more Summary Recommendation Created by Andrea Gundlach, PharmD, MPH, and Karis Dampier Knight, MD, FAPA

2 1 First of all, here are the major changes since the last time this guideline was published: Use clinician- or patient-administered rating scales: Rating scales can assess the type, frequency, and magnitude of psychiatric symptoms to tailor the treatment plan to individual patient needs Strengthening of maintenance treatment recommendation: After the continuation phase of depression, maintenance treatment should be considered, especially for patients with risk factors for recurrence Aerobic exercise or resistance training: Mood symptoms may improve with aerobic exercise or resistance training, particularly in older adults and patients with co-occurring medical problems Electroconvulsive therapy (ECT) for treatment-resistant depression: Options for treatment-resis tant depression include ECT, monoamine oxidase inhibitors, transcranial magnetic stimulation ( TMS), and vagus nerve stimulation In our clinical advisor s view, ECT is appropriate for using in these special cases: o Severe psychotic depression with severe suicidality, catatonia, or not eating so that remission can occur as soon as possible o TMS now has much stronger evidence of effectiveness for treatment-resistant depression, including catatonia Acute-Phase Treatment For acute phase treatment, focus on remission of the depressive episode, achieving full return to baseline functioning, addressing co-occurring psychiatric disorders, such as substance abuse, and base treatment on MDD severity. Our clinical advisor believes it is also crucial to address other medical comorbidities
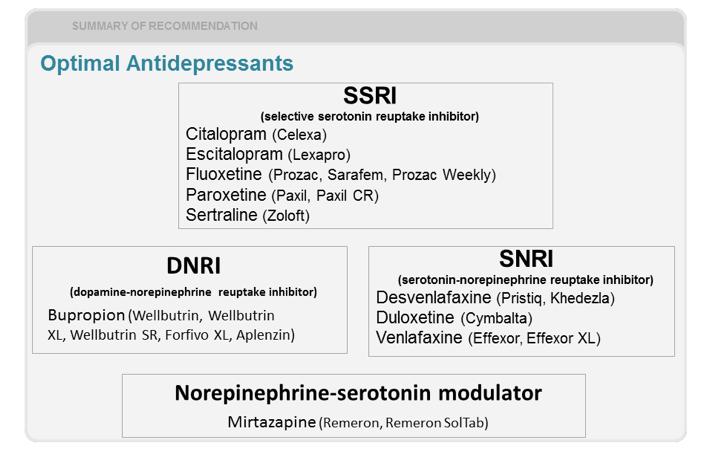
3 2 When assessing suicide risk, look for: Presence of suicidal or homicidal ideation, intent, or plans History and seriousness of previous attempts Access to means for suicide and lethality potential Presence of severe anxiety, panic attacks, agitation, and/or impulsivity Presence of psychotic symptoms, such as command hallucinations or poor reality testing Presence of alcohol or other substance use Family history of or recent exposure to suicide Absence of protective factors According to our clinical advisor, for patients with suicidal tendencies, lithium is the best option. Consider it when the patient has a strong family history of suicide, history of persistent suicidal ideation, or multiple attempts at suicide. Selecting Antidepressants Generally, antidepressants are similar between and within drug classes in terms of effectiveness. Consider patient factors relative to antidepressant characteristics. Patient factors include patient preference, prior response, and comorbidities. Antidepressant characteristics include efficacy, safety, potential drug interactions, duration of effect, and cost. The best first-choice treatment for most patients are selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), mirtazapine, and bupropion. Two complementary and alternative agents S-adenosylmethionine (SAM-e) and St John s wort (SJW) have modest evidence for efficacy. Note, however, that SJW causes frequent drug interactions. Additionally, aerobic exercise or resistance training may improve mood symptoms, especially in older adults with comorbidities. Regular exercise may also reduce the prevalence of depressive symptoms in the general population. Our clinical advisor believes that light therapy can also be considered. Treatments to Avoid Avoid first-line treatment with nonselective monoamine oxidase inhibitors (MAOIs). Dietary restrictions and potential drug interactions relegate which medications to use in patients unresponsive to other treatments. Also avoid using tricyclic antidepressants (TCAs). Most antidepressants are better tolerated than are TCAs.
4 3
: SSRI/serotonin 5-HT3 receptor antagonist/serotonin 5-HT1A receptor agonist Levomilnacipran (Fetzima): Isomer of milnacipran (SNRI) Treatment Monitoring Titrate antidepressants based on")
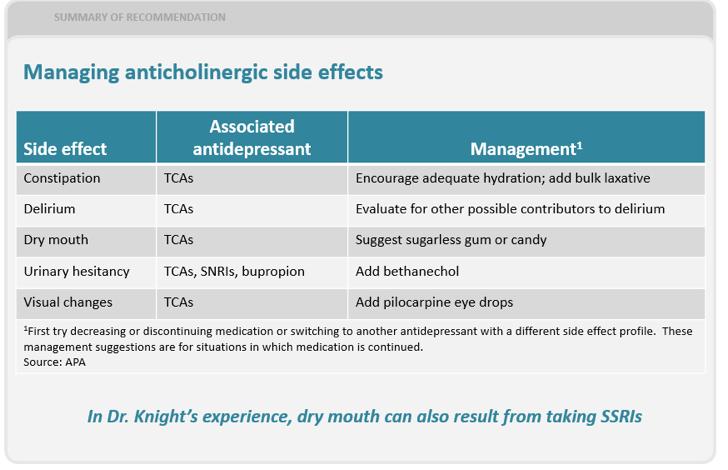
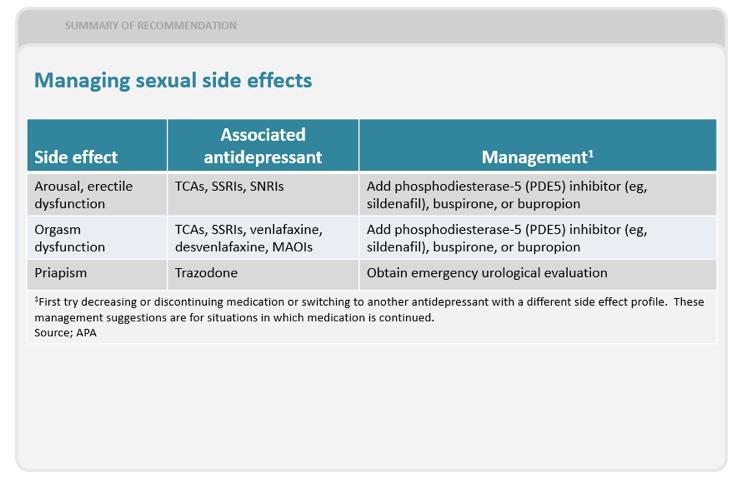
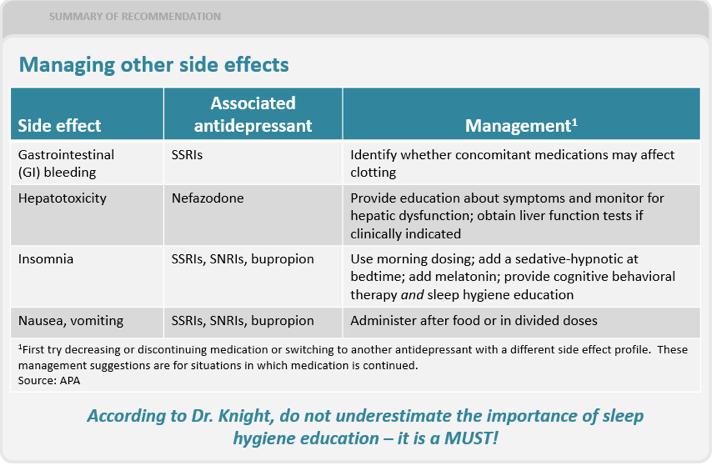
5 4 Keep in mind that the following antidepressants were approved and marketed after guideline publication: Vilazodone (Viibryd): SSRI/partial serotonin 5-HT1A receptor agonist Vortioxetine (Trintellix): SSRI/serotonin 5-HT3 receptor antagonist/serotonin 5-HT1A receptor agonist Levomilnacipran (Fetzima): Isomer of milnacipran (SNRI) Treatment Monitoring Titrate antidepressants based on the patient s age, treatment setting, comorbidities, concurrent pharmacotherapy, and adverse events. When adverse events occur, lower the dose or switch treatments. Additionally, assess psychiatric symptoms for type, frequency, and magnitude. The following charts provide an in-depth look at managing potential adverse reactions:

6 5

7 6

8 7
9 8 Treatment Response Incomplete response is associated with poor functional outcomes. If improvement does not occur in 4 to 8 weeks, reconsider diagnosis, assess adverse effects and adherence to treatment, review comorbidities and psychosocial factors, adjust treatment plan, and consider consultation. Continuation Phase The continuation phase takes place in the 4 to 9 months after acute-phase treatment, usually with the same dose of antidepressant. During this phase, use a clinician- or patient-administered rating scale to assess treatment and tailor the treatment plan. It is essential to assess symptoms, side effects, adherence, and functional status. Depression-focused psychotherapy is recommended. Evidence suggests that cognitive behavioral therapy (CBT) is the best option. Continue pharmacotherapy in patients who respond to an acute course of ECT. Best evidence is to use lithium and nortriptyline. Alternatively, continue ECT in patients who responded to an acute ECT course, particularly if medication or psychotherapy does not maintain remission. Maintenance Phase Maintenance phase treatment should progress from continuation phase treatment in patients with 3 or more prior major depressive episodes or chronic depressive disorder. Consider maintenance treatment in patients with additional risk factors for recurrence, including presence of residual symptoms, ongoing psychosocial stressors, early age at onset, and family history of mood disorders. Continue medication at full therapeutic dosage. If necessary, continue psychotherapy with less frequent sessions. According to our clinical advisor: Often psychotherapy sessions and other psychosocial interventions (such as yoga, exercise, and partic ipation in support groups) are increased as medication is tapered CBT should include problem-solving therapy, behavioral activation therapy, and interpersonal therapy to, among other things, address social support issues Maintenance phase treatment may be required indefinitely, particularly in patients with chronic and recurrent MDD. Factors that play into duration are: Patient preference Type of treatment used Adverse effects Comorbid conditions Frequency and severity of previous depressive episodes, including psychosis and suicide risk Persistence of depressive symptoms after recovery Discontinuing Treatment Antidepressants should be tapered. Taper should occur over at least several weeks. Advise patients not to stop medications abruptly. To reduce the risk of discontinuation syndrome, taper slowly and temporarily switch to a longer half-life antidepressant. Warn patients about possibility of relapse and monitor for several months after discontinuation.
10 9 About the authors Dr Gundlach is a pharmacist at Stone Springs Hospital Center in Dulles, VA, and a medical writer. Dr Knight is CEO of Magnolia Family Psychiatry and TMS Center in Decatur, AL Citation: Gelenberg AJ, Freeman MP, Markowitz JC, et al. American Psychiatric Association Practice Guideline for the Treatment of Patients With Major Depressive Disorder, Third Edition. Am J Psychiatry. 2010;167(suppl):1-152.
Diagnosis & Management of Major Depression: A Review of What s Old and New. Cerrone Cohen, MD
 Diagnosis & Management of Major Depression: A Review of What s Old and New Cerrone Cohen, MD Why You re Treating So Much Mental Health 59% of Psychiatrists Are Over the Age of 55 AAMC 2014 Physician specialty
Diagnosis & Management of Major Depression: A Review of What s Old and New Cerrone Cohen, MD Why You re Treating So Much Mental Health 59% of Psychiatrists Are Over the Age of 55 AAMC 2014 Physician specialty
TREATING MAJOR DEPRESSIVE DISORDER
 TREATING MAJOR DEPRESSIVE DISORDER A Quick Reference Guide Based on Practice Guideline for the Treatment of Patients With Major Depressive Disorder, Second Edition, originally published in April 2000.
TREATING MAJOR DEPRESSIVE DISORDER A Quick Reference Guide Based on Practice Guideline for the Treatment of Patients With Major Depressive Disorder, Second Edition, originally published in April 2000.
Bipolar Disorder Clinical Practice Guideline Summary for Primary Care
 Bipolar Disorder Clinical Practice Guideline Summary for Primary Care DIAGNOSIS AND CLINICAL ASSESSMENT Bipolar Disorder is categorized by extreme mood cycling; manifested by periods of euphoria, grandiosity,
Bipolar Disorder Clinical Practice Guideline Summary for Primary Care DIAGNOSIS AND CLINICAL ASSESSMENT Bipolar Disorder is categorized by extreme mood cycling; manifested by periods of euphoria, grandiosity,
Objectives. Objectives. A practice review. 02-Nov-16 MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS
 MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS Jon-Paul Khoo What is treatment resistance really? Database review 328 consecutive non-remitted MDD patients referred for private
MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS Jon-Paul Khoo What is treatment resistance really? Database review 328 consecutive non-remitted MDD patients referred for private
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia
 Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
Joel V. Oberstar, M.D. 1
 Diagnosis and Treatment of Depressive Disorders in Children and Adolescents Joel V. Oberstar, M.D. CEO & Chief Medical Officer Adjunct Assistant Professor of Psychiatry University of Minnesota Medical
Diagnosis and Treatment of Depressive Disorders in Children and Adolescents Joel V. Oberstar, M.D. CEO & Chief Medical Officer Adjunct Assistant Professor of Psychiatry University of Minnesota Medical
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
Treatment-resistant depression in primary care
 Treatment-resistant depression in primary care Interprofessional CME, October 2017 Brian J. Mickey, MD, PhD Associate Professor School of Medicine Department of Psychiatry Disclosures Speakers bureau:
Treatment-resistant depression in primary care Interprofessional CME, October 2017 Brian J. Mickey, MD, PhD Associate Professor School of Medicine Department of Psychiatry Disclosures Speakers bureau:
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
Psychiatry curbside: Answers to a primary care doctor s top mental health questions
 Psychiatry curbside: Answers to a primary care doctor s top mental health questions April 27, 2018 Laurel Ralston, DO Psychiatrist, Taussig Cancer Institute Objectives Review current diagnostic and prescribing
Psychiatry curbside: Answers to a primary care doctor s top mental health questions April 27, 2018 Laurel Ralston, DO Psychiatrist, Taussig Cancer Institute Objectives Review current diagnostic and prescribing
Treatment Options for Bipolar Disorder Contents
 Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Summary of guideline for the. treatment of depression RANZCP CLINICAL PRACTICE GUIDELINES ASSESSMENT
 RANZCP CLINICAL PRACTICE GUIDELINES Summary of guideline for the RANZCP CLINICAL PRACTICE GUIDELINES treatment of depression Pete M. Ellis, Ian B. Hickie and Don A. R. Smith for the RANZCP Clinical Practice
RANZCP CLINICAL PRACTICE GUIDELINES Summary of guideline for the RANZCP CLINICAL PRACTICE GUIDELINES treatment of depression Pete M. Ellis, Ian B. Hickie and Don A. R. Smith for the RANZCP Clinical Practice
Guidelines MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD)
") MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
KEY MESSAGES. It is often under-recognised and 30-50% of MDD cases in primary care and medical settings are not detected.
 KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
Depression. University of Illinois at Chicago College of Nursing
 Depression University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this session, participants will be better able to: 1. Recognize depression, its symptoms and behaviors
Depression University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this session, participants will be better able to: 1. Recognize depression, its symptoms and behaviors
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 5. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 5. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
Major Depression and Anxiety in Adolescents and Adults
 Major Depression and Anxiety in Adolescents and Adults Miggie Greenberg, M.D. Associate Professor of Psychiatry St. Louis University School of Medicine greenbml@slu.edu *NO DISCLOSURES* OBJECTIVES * Recognize
Major Depression and Anxiety in Adolescents and Adults Miggie Greenberg, M.D. Associate Professor of Psychiatry St. Louis University School of Medicine greenbml@slu.edu *NO DISCLOSURES* OBJECTIVES * Recognize
Consultant Pharmacist Approach to Major Depressive Disorder
 Consultant Pharmacist Approach to Major Depressive Disorder ALAN OBRINGER RPH, CPH, CGP PRESIDENT/OWNER GUARDIAN PHARMACY OF ORLANDO Objectives What is Depression? Discuss the epidemiology of depression
Consultant Pharmacist Approach to Major Depressive Disorder ALAN OBRINGER RPH, CPH, CGP PRESIDENT/OWNER GUARDIAN PHARMACY OF ORLANDO Objectives What is Depression? Discuss the epidemiology of depression
Consultant Pharmacist Approach to Major Depressive Disorder ALAN OBRINGER RPH, CPH, CGP PRESIDENT/OWNER GUARDIAN PHARMACY OF ORLANDO
 Consultant Pharmacist Approach to Major Depressive Disorder ALAN OBRINGER RPH, CPH, CGP PRESIDENT/OWNER GUARDIAN PHARMACY OF ORLANDO Objectives What is Depression? Discuss the epidemiology of depression
Consultant Pharmacist Approach to Major Depressive Disorder ALAN OBRINGER RPH, CPH, CGP PRESIDENT/OWNER GUARDIAN PHARMACY OF ORLANDO Objectives What is Depression? Discuss the epidemiology of depression
Where to from Here? Evidence-Based Strategies for Treatment of Refractory Depression
 Where to from Here? Evidence-Based Strategies for Treatment of Refractory Depression Michael D. Jibson, MD, PhD Professor of Psychiatry University of Michigan Major Depression #1 WHO cause of disability
Where to from Here? Evidence-Based Strategies for Treatment of Refractory Depression Michael D. Jibson, MD, PhD Professor of Psychiatry University of Michigan Major Depression #1 WHO cause of disability
DSM-5 Criteria: Major Depressive Disorder
 DSM-5 Criteria: Major Depressive Disorder Box 3. Major Depressive Episode: DSM-5 Diagnosis: Major Depressive Disorder Five (or more) of the following symptoms have been present during the same 2-week period
DSM-5 Criteria: Major Depressive Disorder Box 3. Major Depressive Episode: DSM-5 Diagnosis: Major Depressive Disorder Five (or more) of the following symptoms have been present during the same 2-week period
Suicide Risk and Melancholic Features of Major Depressive Disorder: A Diagnostic Imperative
 Suicide Risk and Melancholic Features of Major Depressive Disorder: A Diagnostic Imperative Robert I. Simon, M.D.* Suicide risk is increased in patients with Major Depressive Disorder with Melancholic
Suicide Risk and Melancholic Features of Major Depressive Disorder: A Diagnostic Imperative Robert I. Simon, M.D.* Suicide risk is increased in patients with Major Depressive Disorder with Melancholic
Clinical Perspective on Conducting TRD Studies. Hans Eriksson, M.D., Ph.D., M.B.A. Chief Medical Specialist, H. Lundbeck A/S Valby, Denmark
 Clinical Perspective on Conducting TRD Studies Hans Eriksson, M.D., Ph.D., M.B.A. Chief Medical Specialist, H. Lundbeck A/S Valby, Denmark Overview of Presentation Treatment-Resistant Depression (TRD)
Clinical Perspective on Conducting TRD Studies Hans Eriksson, M.D., Ph.D., M.B.A. Chief Medical Specialist, H. Lundbeck A/S Valby, Denmark Overview of Presentation Treatment-Resistant Depression (TRD)
Some newer, investigational approaches to treating refractory major depression are being used.
 CREATED EXCLUSIVELY FOR FINANCIAL PROFESSIONALS Rx FOR SUCCESS Depression and Anxiety Disorders Mood and anxiety disorders are common, and the mortality risk is due primarily to suicide, cardiovascular
CREATED EXCLUSIVELY FOR FINANCIAL PROFESSIONALS Rx FOR SUCCESS Depression and Anxiety Disorders Mood and anxiety disorders are common, and the mortality risk is due primarily to suicide, cardiovascular
MOLINA HEALTHCARE CLINICAL PRACTICE GUIDELINES: Treatment of Patients with Major Depressive Disorder
 MOLINA HEALTHCARE CLINICAL PRACTICE GUIDELINES: Treatment of Patients with Major Depressive Disorder Molina Healthcare has adopted the Treatment of Patients with Major Depressive Disorder Clinical Practice
MOLINA HEALTHCARE CLINICAL PRACTICE GUIDELINES: Treatment of Patients with Major Depressive Disorder Molina Healthcare has adopted the Treatment of Patients with Major Depressive Disorder Clinical Practice
Best Practices in Prescribing Benzodiazepines. Michael Carlisle, DO Medical Director University Hospitals Geauga Medical Center
 Best Practices in Prescribing Benzodiazepines Michael Carlisle, DO Medical Director University Hospitals Geauga Medical Center Objectives To review current practice guidelines in benzodiazepine prescribing
Best Practices in Prescribing Benzodiazepines Michael Carlisle, DO Medical Director University Hospitals Geauga Medical Center Objectives To review current practice guidelines in benzodiazepine prescribing
Depressive and Bipolar Disorders
 Depressive and Bipolar Disorders Symptoms Associated with Depressive and Bipolar Disorders Characteristics of mood symptoms Affects a person s well being, school, work, or social functioning Continues
Depressive and Bipolar Disorders Symptoms Associated with Depressive and Bipolar Disorders Characteristics of mood symptoms Affects a person s well being, school, work, or social functioning Continues
Depression in adults: treatment and management
 1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
(levomilnacipran) extended-release capsules
 extended-release capsules") MEDICATION GUIDE FETZIMA (fet-zee-muh) (levomilnacipran) extended-release capsules Read this Medication Guide before you start taking FETZIMA and each time you get a refill. There may be new information.
MEDICATION GUIDE FETZIMA (fet-zee-muh) (levomilnacipran) extended-release capsules Read this Medication Guide before you start taking FETZIMA and each time you get a refill. There may be new information.
Mental Health Practice Support
 Initial Screening and Triage for Follow-up HEALTH TEAM Depression is suspected: Perform two-question screen 1,2 (box 1)* Review risk factors 1-3 (box 2) Diagnose and characterize MDE with clinical interview:
Initial Screening and Triage for Follow-up HEALTH TEAM Depression is suspected: Perform two-question screen 1,2 (box 1)* Review risk factors 1-3 (box 2) Diagnose and characterize MDE with clinical interview:
Antidepressant Medication Therapy in Primary Care July 25, 2013
 New York State Collaborative Care Initiative Antidepressant Medication Therapy in Primary Care July 25, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
New York State Collaborative Care Initiative Antidepressant Medication Therapy in Primary Care July 25, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
Objectives. DSM-V Changes: Elimination of Multiaxial Diagnostic System
 Conflicts of Interest I have no conflicts to disclose. 2014 Updates to the Updates in Pharmacotherapy Webinar Psychiatry Updates for Pharmacotherapy Specialists Jacintha S. Cauffield, Pharm.D., BCPS Associate
Conflicts of Interest I have no conflicts to disclose. 2014 Updates to the Updates in Pharmacotherapy Webinar Psychiatry Updates for Pharmacotherapy Specialists Jacintha S. Cauffield, Pharm.D., BCPS Associate
Appendix C: Algorithms. Algorithm C-1: Enhanced Screening Algorithm
 Appendix C: Algorithms Algorithm C-1: Enhanced Screening Algorithm PCC Depression Screening Neg Annual Screening Pos CPRS Alert to Team Enhanced Screening Via Telephone Unable To Contact Telephone Introduction
Appendix C: Algorithms Algorithm C-1: Enhanced Screening Algorithm PCC Depression Screening Neg Annual Screening Pos CPRS Alert to Team Enhanced Screening Via Telephone Unable To Contact Telephone Introduction
MAJOR DEPRESSION CLINICAL PRACTICE GUIDELINE
 MAJOR DEPRESSION CLINICAL PRACTICE GUIDELINE Reviewed and Updated by the Behvioral Health Subcommittee 7/20/2017 Topic Purpose Access Assessment 7/2017 Recommendations SummaCare Health Plan bases its Clinical
MAJOR DEPRESSION CLINICAL PRACTICE GUIDELINE Reviewed and Updated by the Behvioral Health Subcommittee 7/20/2017 Topic Purpose Access Assessment 7/2017 Recommendations SummaCare Health Plan bases its Clinical
Daniel Suzuki, MD Adjunct Clinical Associate Professor of Psychiatry, USC Keck School of Medicine Clinical Adjunct Professor/Faculty, Graduate School
 Daniel Suzuki, MD Adjunct Clinical Associate Professor of Psychiatry, USC Keck School of Medicine Clinical Adjunct Professor/Faculty, Graduate School of Psychology, Fuller Theological Seminary Medical
Daniel Suzuki, MD Adjunct Clinical Associate Professor of Psychiatry, USC Keck School of Medicine Clinical Adjunct Professor/Faculty, Graduate School of Psychology, Fuller Theological Seminary Medical
Wellbutrin/Wellbutrin-SR/ Wellbutrin-XL (bupropion)
") Wellbutrin/Wellbutrin-SR/ Wellbutrin-XL (bupropion) Generic name: Bupropion Available strengths: 75 mg, 100 mg immediate-release tablets; 100 mg, 150 mg, 200 mg sustained-release tablets (Wellbutrin-SR);
Wellbutrin/Wellbutrin-SR/ Wellbutrin-XL (bupropion) Generic name: Bupropion Available strengths: 75 mg, 100 mg immediate-release tablets; 100 mg, 150 mg, 200 mg sustained-release tablets (Wellbutrin-SR);
Treatment of Major Depressive Disorder
 Treatment of Major Depressive Disorder Sarah Mullowney, MD PGY3 Psychiatry Resident, University of Utah Paula Gibbs, MD Medical Director of 5 West at UUMC Clerkship Director MS III Psychiatric Rotation
Treatment of Major Depressive Disorder Sarah Mullowney, MD PGY3 Psychiatry Resident, University of Utah Paula Gibbs, MD Medical Director of 5 West at UUMC Clerkship Director MS III Psychiatric Rotation
BRIEF SUMMARY CONTENT
 Page 1 of 17 Brief Summary GUIDELINE TITLE Depression. The treatment and management of depression in adults. BIBLIOGRAPHIC SOURCE(S) National Collaborating Centre for Mental Health. Depression. The treatment
Page 1 of 17 Brief Summary GUIDELINE TITLE Depression. The treatment and management of depression in adults. BIBLIOGRAPHIC SOURCE(S) National Collaborating Centre for Mental Health. Depression. The treatment
Depression in Pregnancy
 TREATING THE MOTHER PROTECTING THE UNBORN A MOTHERISK Educational Program The content of this program reflects the expression of a consensus on emerging clinical and scientific advances as of the date
TREATING THE MOTHER PROTECTING THE UNBORN A MOTHERISK Educational Program The content of this program reflects the expression of a consensus on emerging clinical and scientific advances as of the date
Depression major depressive disorder. Some terms: Major Depressive Disorder: Major Depressive Disorder:
 Depression major depressive disorder Oldest recognized disorder: melancholia It is a positive and active anguish, a sort of psychical neuralgia wholly unknown to normal life. - William James "I am now
Depression major depressive disorder Oldest recognized disorder: melancholia It is a positive and active anguish, a sort of psychical neuralgia wholly unknown to normal life. - William James "I am now
Drugs for Emotional and Mood Disorders Chapter 16
 Drugs for Emotional and Mood Disorders Chapter 16 NCLEX-RN Review Question 1 Choices Please note Question #1 at the end of Ch 16 pg 202 & Key pg 805 answer is #4 1. Psychomotor symptoms 2. Tachycardia,
Drugs for Emotional and Mood Disorders Chapter 16 NCLEX-RN Review Question 1 Choices Please note Question #1 at the end of Ch 16 pg 202 & Key pg 805 answer is #4 1. Psychomotor symptoms 2. Tachycardia,
Antidepressant Selection in Primary Care
 Antidepressant Selection in Primary Care R E B E C C A D. L E W I S, D O O O A S U M M E R C M E B R A N S O N, M O 1 5 A U G U S T 2 0 1 5 Objectives Understand the epidemiology of depression. Recognize
Antidepressant Selection in Primary Care R E B E C C A D. L E W I S, D O O O A S U M M E R C M E B R A N S O N, M O 1 5 A U G U S T 2 0 1 5 Objectives Understand the epidemiology of depression. Recognize
Antidepressants. Dr Malek Zihlif
 Antidepressants The optimal use of antidepressant required a clear understanding of their mechanism of action, pharmacokinetics, potential drug interaction and the deferential diagnosis of psychiatric
Antidepressants The optimal use of antidepressant required a clear understanding of their mechanism of action, pharmacokinetics, potential drug interaction and the deferential diagnosis of psychiatric
Guilt Suicidality. Depression Co-Occurs with Medical Illness The rate of major depression among those with medical illness is significant.
 1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
Depression & Anxiety in Adolescents
 Depression & Anxiety in Adolescents Objectives 1) Review diagnosis of anxiety and depression in adolescents 2) Provide overview of evidence-based treatment options 3) Increase provider comfort level with
Depression & Anxiety in Adolescents Objectives 1) Review diagnosis of anxiety and depression in adolescents 2) Provide overview of evidence-based treatment options 3) Increase provider comfort level with
Pamelor (nortriptyline)
") Generic name: Nortriptyline Available strengths: 10 mg, 25 mg, 50 mg, 75 mg capsules; 10 mg/5 ml oral solution Available in generic: Yes Drug class: Tricyclic antidepressant General Information Pamelor
Generic name: Nortriptyline Available strengths: 10 mg, 25 mg, 50 mg, 75 mg capsules; 10 mg/5 ml oral solution Available in generic: Yes Drug class: Tricyclic antidepressant General Information Pamelor
Norpramin (desipramine)
") Generic name: Desipramine Available strengths: 10 mg, 25 mg, 50 mg, 75 mg, 100 mg, 150 mg tablets Available in generic: Yes Drug class: Tricyclic antidepressant General Information Norpramin (desipramine)
Generic name: Desipramine Available strengths: 10 mg, 25 mg, 50 mg, 75 mg, 100 mg, 150 mg tablets Available in generic: Yes Drug class: Tricyclic antidepressant General Information Norpramin (desipramine)
Depressive, Bipolar and Related Disorders
 Depressive, Bipolar and Related Disorders Robert Kelly, MD Assistant Professor of Psychiatry Weill Cornell Medical College White Plains, New York Lecture available at www.robertkelly.us Financial Conflicts
Depressive, Bipolar and Related Disorders Robert Kelly, MD Assistant Professor of Psychiatry Weill Cornell Medical College White Plains, New York Lecture available at www.robertkelly.us Financial Conflicts
Manual of Clinical Psychopharmacology
 Manual of Clinical Psychopharmacology Fourth Edition Alan F. Schatzberg, M.D. Kenneth T. Norris, Jr., Professor and Chairman, Department of Psychiatry and Behavioral Sciences, Stanford University School
Manual of Clinical Psychopharmacology Fourth Edition Alan F. Schatzberg, M.D. Kenneth T. Norris, Jr., Professor and Chairman, Department of Psychiatry and Behavioral Sciences, Stanford University School
Mood Disorders.
 Mood Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Mood Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
DISEASES AND DISORDERS
 DISEASES AND DISORDERS 13. The mood (affective) disorders 99 14. The psychotic disorders: schizophrenia 105 15. The anxiety and somatoform disorders 111 16. Dementia and delirium 117 17. Alcohol and substance-related
DISEASES AND DISORDERS 13. The mood (affective) disorders 99 14. The psychotic disorders: schizophrenia 105 15. The anxiety and somatoform disorders 111 16. Dementia and delirium 117 17. Alcohol and substance-related
Effective Date: 5/28/2014 Version: 2.0 (Revised: 10/12/2015) Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017)
 Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017)") Protocol Title: Depression & Generalized Anxiety Disorder Effective Date: 5/28/2014 Version: 2.0 (Revised: 10/12/2015) Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017) Group
Protocol Title: Depression & Generalized Anxiety Disorder Effective Date: 5/28/2014 Version: 2.0 (Revised: 10/12/2015) Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017) Group
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abuse alcohol, aggression and, 52 53 substance, aggression and, 52 54 ACE. See Aid to Capacity Evaluation (ACE). AEDs. See Antiepileptic
Index Note: Page numbers of article titles are in boldface type. A Abuse alcohol, aggression and, 52 53 substance, aggression and, 52 54 ACE. See Aid to Capacity Evaluation (ACE). AEDs. See Antiepileptic
A Basic Approach to Mood and Anxiety Disorders in the Elderly
 A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
10 INDEX Acknowledgements, i
 INDEX 10 INDEX Acknowledgements, i Acute Care, Admissions to, 3.83 Discharge Planning, 3.86 Involuntary Admission Criteria, 3.84 List of Designated Provincial and Regional Mental Health Facilities, 3.83
INDEX 10 INDEX Acknowledgements, i Acute Care, Admissions to, 3.83 Discharge Planning, 3.86 Involuntary Admission Criteria, 3.84 List of Designated Provincial and Regional Mental Health Facilities, 3.83
Depressive Disorders A clinical overview. Dr. Scott Yarosh, Medical Director, Behavioral Health
 Depressive Disorders A clinical overview Dr. Scott Yarosh, Medical Director, Behavioral Health Depressive Disorders What is depression? Complex series of conditions Physical component Emotional component
Depressive Disorders A clinical overview Dr. Scott Yarosh, Medical Director, Behavioral Health Depressive Disorders What is depression? Complex series of conditions Physical component Emotional component
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults
 Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Taking Care: Child and Youth Mental Health TREATMENT OPTIONS
 Taking Care: Child and Youth Mental Health TREATMENT OPTIONS Open Learning Agency 2004 TREATMENT OPTIONS With appropriate treatment, more than 80% of people with depression get full relief from their symptoms
Taking Care: Child and Youth Mental Health TREATMENT OPTIONS Open Learning Agency 2004 TREATMENT OPTIONS With appropriate treatment, more than 80% of people with depression get full relief from their symptoms
Pharmacists in Medication Adherence in Psychiatric Patients
 Pharmacists in Medication Adherence in Psychiatric Patients Mamta Parikh, PharmD, BCPS, BCPP Assistant Professor, Clinical and Administrative Sciences Notre Dame of Maryland University School of Pharmacy
Pharmacists in Medication Adherence in Psychiatric Patients Mamta Parikh, PharmD, BCPS, BCPP Assistant Professor, Clinical and Administrative Sciences Notre Dame of Maryland University School of Pharmacy
Mentoring Session: Participant Cases
 Handout for the Neuroscience Education Institute (NEI) online activity: Mentoring Session: Participant Cases The Case: 55-year-old patient with depression and anxiety The Question: What to do when antidepressants
Handout for the Neuroscience Education Institute (NEI) online activity: Mentoring Session: Participant Cases The Case: 55-year-old patient with depression and anxiety The Question: What to do when antidepressants
Obsessive-Compulsive Disorder Clinical Practice Guideline Summary for Primary Care
 Obsessive-Compulsive Disorder Clinical Practice Guideline Summary for Primary Care CLINICAL ASSESSMENT AND DIAGNOSIS (ADULTS) Obsessive-Compulsive Disorder (OCD) is categorized by recurrent obsessions,
Obsessive-Compulsive Disorder Clinical Practice Guideline Summary for Primary Care CLINICAL ASSESSMENT AND DIAGNOSIS (ADULTS) Obsessive-Compulsive Disorder (OCD) is categorized by recurrent obsessions,
Children s Hospital Of Wisconsin
 Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Elavil (amitriptyline)
") Generic name: Amitriptyline Available strengths: 10 mg, 25 mg, 50 mg, 75 mg, 100 mg, 150 mg tablets; 10 mg/ml injection Available in generic: Yes Drug class: Tricyclic antidepressant General Information
Generic name: Amitriptyline Available strengths: 10 mg, 25 mg, 50 mg, 75 mg, 100 mg, 150 mg tablets; 10 mg/ml injection Available in generic: Yes Drug class: Tricyclic antidepressant General Information
Treatment of Psychological Disorders
 Chapter 11 Treatment of Psychological Disorders McGraw-Hill 2010 The McGraw-Hill Companies, Inc. All rights reserved. Psychotherapy: Psychodynamic, Behavioral, and Cognitive Approaches Learning Outcomes
Chapter 11 Treatment of Psychological Disorders McGraw-Hill 2010 The McGraw-Hill Companies, Inc. All rights reserved. Psychotherapy: Psychodynamic, Behavioral, and Cognitive Approaches Learning Outcomes
Adult Depression - Clinical Practice Guideline
 1 Adult Depression - Clinical Practice Guideline 05/2018 Diagnosis and Screening Diagnostic criteria o Please refer to Attachment A Screening o The United States Preventative Services Task Force (USPSTF)
1 Adult Depression - Clinical Practice Guideline 05/2018 Diagnosis and Screening Diagnostic criteria o Please refer to Attachment A Screening o The United States Preventative Services Task Force (USPSTF)
The Role of the Family Physician in Managing Depression
 Middle East Journal of Family Medicine, 2004; Vol. 2 (2) The Role of the Family Physician in Managing Depression 1-Homoud F. Al-Zuabi, BSc.MBBCh.RCGP. Head of Ferdous Health Center Farwania Primary Health
Middle East Journal of Family Medicine, 2004; Vol. 2 (2) The Role of the Family Physician in Managing Depression 1-Homoud F. Al-Zuabi, BSc.MBBCh.RCGP. Head of Ferdous Health Center Farwania Primary Health
Managing Late Life Depression
 Managing Late Life Depression Maria I. Lapid, M.D, Professor of Psychiatry Program Director, Geriatric Psychiatry Fellowship Simon Kung, M.D. Associate Professor of Psychiatry Medical Director, Mood Disorders
Managing Late Life Depression Maria I. Lapid, M.D, Professor of Psychiatry Program Director, Geriatric Psychiatry Fellowship Simon Kung, M.D. Associate Professor of Psychiatry Medical Director, Mood Disorders
Vilazodone New Option for Depression
 Human Journals Review Article November 2018 Vol.:13, Issue:4 All rights are reserved by Jisha Vijayan et al. Vilazodone New Option for Depression Keywords: Vilazodone, Safety, Efficacy, Major Depressive
Human Journals Review Article November 2018 Vol.:13, Issue:4 All rights are reserved by Jisha Vijayan et al. Vilazodone New Option for Depression Keywords: Vilazodone, Safety, Efficacy, Major Depressive
9/24/2012. Amer M Burhan, MBChB, FRCP(C)
") Depression and Dementia Amer M Burhan MBChB, FRCPC Head of CAMH Memory Clinic, Toronto Geriatric Neuropsychiatrist Assistant Prof Psychiatry at U of T Objectives Discuss the prevalence and impact of depression
Depression and Dementia Amer M Burhan MBChB, FRCPC Head of CAMH Memory Clinic, Toronto Geriatric Neuropsychiatrist Assistant Prof Psychiatry at U of T Objectives Discuss the prevalence and impact of depression
9/20/2011. Integrated Care for Depression & Anxiety: Psychotropic Medication Management for PCPs. Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Clinical Policy: Levomilnacipran (Fetzima) Reference Number: HIM.PA.125 Effective Date: Last Review Date: 11.18
 Reference Number: HIM.PA.125 Effective Date: Last Review Date: 11.18") Clinical Policy: (Fetzima) Reference Number: HIM.PA.125 Effective Date: 12.01.17 Last Review Date: 11.18 Line of Business: HIM Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Fetzima) Reference Number: HIM.PA.125 Effective Date: 12.01.17 Last Review Date: 11.18 Line of Business: HIM Revision Log See Important Reminder at the end of this policy for important
Doctor Discussion Guide
 Doctor Discussion Guide What should I tell my doctor? Talking to your doctor about depression doesn t have to be as hard as you may think. These simple tips can help you gather information and prepare
Doctor Discussion Guide What should I tell my doctor? Talking to your doctor about depression doesn t have to be as hard as you may think. These simple tips can help you gather information and prepare
Chapter 6 Mood Disorders and Suicide An Overview of Mood Disorders
 Page 1 Extremes in Normal Mood Chapter 6 Mood Disorders and Suicide An Overview of Mood Disorders Nature of depression Nature of mania and hypomania Types of DSM-IV Depressive Disorders Major depressive
Page 1 Extremes in Normal Mood Chapter 6 Mood Disorders and Suicide An Overview of Mood Disorders Nature of depression Nature of mania and hypomania Types of DSM-IV Depressive Disorders Major depressive
PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES
 PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES Table of Contents Print TABLE OF CONTENTS Drug Page Number Anafranil... 2 Asendin... 4 Celexa... 4 Cymbalta... 6 Desyrel... 8 Effexor...10 Elavil...14
PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES Table of Contents Print TABLE OF CONTENTS Drug Page Number Anafranil... 2 Asendin... 4 Celexa... 4 Cymbalta... 6 Desyrel... 8 Effexor...10 Elavil...14
Pediatrics Grand Rounds 5 March University of Texas Health Science Center at San Antonio I-1
 Diagnosis and Treatment of Depression in Children and Adolescents Steven R. Pliszka, M.D. Professor and Vice Chair Chief, Division of Child and Adolescent Psychiatry Department of Psychiatry The Disclosures
Diagnosis and Treatment of Depression in Children and Adolescents Steven R. Pliszka, M.D. Professor and Vice Chair Chief, Division of Child and Adolescent Psychiatry Department of Psychiatry The Disclosures
Which statement applies to you?
 Beyond Burnout: a Case based Approach to Managing Depression & Preventing Suicide Erika E. Tillery, PharmD, BCPP, BCGP Associate Professor of Pharmacy Practice, Presbyterian College School of Pharmacy
Beyond Burnout: a Case based Approach to Managing Depression & Preventing Suicide Erika E. Tillery, PharmD, BCPP, BCGP Associate Professor of Pharmacy Practice, Presbyterian College School of Pharmacy
Clinical Guideline for the Management of Bipolar Disorder in Adults
 Clinical Guideline for the Management of Bipolar Disorder in Adults Goal: To improve the quality of life of adults with bipolar disorder Identification and Treatment of Bipolar Disorder Criteria for Diagnosis:
Clinical Guideline for the Management of Bipolar Disorder in Adults Goal: To improve the quality of life of adults with bipolar disorder Identification and Treatment of Bipolar Disorder Criteria for Diagnosis:
This initial discovery led to the creation of two classes of first generation antidepressants:
 Antidepressants - TCAs, MAOIs, SSRIs & SNRIs First generation antidepressants TCAs and MAOIs The discovery of antidepressants could be described as a lucky accident. During the 1950s, while carrying out
Antidepressants - TCAs, MAOIs, SSRIs & SNRIs First generation antidepressants TCAs and MAOIs The discovery of antidepressants could be described as a lucky accident. During the 1950s, while carrying out
Drugs, Society and Behavior
 SOCI 270 Drugs, Society and Behavior Spring 2016 Professor Kurt Reymers, Ph.D. Chapter 8 Medication for Mental Disorders 1. Mental Disorders: a. The Medical Model Model: symptoms diagnosis determination
SOCI 270 Drugs, Society and Behavior Spring 2016 Professor Kurt Reymers, Ph.D. Chapter 8 Medication for Mental Disorders 1. Mental Disorders: a. The Medical Model Model: symptoms diagnosis determination
Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90
 Depression in adults: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Depression in adults: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Antidepressant Selection in Primary Care
 Antidepressant Selection in Primary Care Rebecca D. Lewis, DO OOA Summer CME Oklahoma City, OK 6 August 2017 Objectives Understand the epidemiology of depression. Recognize factors to help choose antidepressants.
Antidepressant Selection in Primary Care Rebecca D. Lewis, DO OOA Summer CME Oklahoma City, OK 6 August 2017 Objectives Understand the epidemiology of depression. Recognize factors to help choose antidepressants.
VA/DoD Clinical Practice Guideline for Management of Post Traumatic Stress. Core Module
 VA/DoD Clinical Practice Guideline for Management of Post Traumatic Stress Core Module Module A Acute Stress Continue Treatment for ASD Treatment for ACUTE Stress Disorder Module B PTSD Continue Treatment
VA/DoD Clinical Practice Guideline for Management of Post Traumatic Stress Core Module Module A Acute Stress Continue Treatment for ASD Treatment for ACUTE Stress Disorder Module B PTSD Continue Treatment
Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg91
 Depression in adults with a chronic physical health problem: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg91 NICE 2018. All rights reserved. Subject to
Depression in adults with a chronic physical health problem: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg91 NICE 2018. All rights reserved. Subject to
5 COMMON QUESTIONS WHEN TREATING DEPRESSION
 5 COMMON QUESTIONS WHEN TREATING DEPRESSION Do Antidepressants Increase the Possibility of Suicide? Will I Accidentally Induce Mania if I Prescribe an SSRI? Are Depression Medications Safe and Effective
5 COMMON QUESTIONS WHEN TREATING DEPRESSION Do Antidepressants Increase the Possibility of Suicide? Will I Accidentally Induce Mania if I Prescribe an SSRI? Are Depression Medications Safe and Effective
Psychotic and Mood Disorders
 Psychotic and Mood Disorders د ر ا ر با ی کلاس د یاران سال اول روا پ ز ش ی وه روا پ ز ش ی دا ه ع وم زپ ش ی ا ان 93/6/16 2 Symptoms Mood Anxious Psychotic Non-specific Depressed mood Anxiety/Worry Delusion
Psychotic and Mood Disorders د ر ا ر با ی کلاس د یاران سال اول روا پ ز ش ی وه روا پ ز ش ی دا ه ع وم زپ ش ی ا ان 93/6/16 2 Symptoms Mood Anxious Psychotic Non-specific Depressed mood Anxiety/Worry Delusion
Neurobiology of Depression
 Chapter 1 Neurobiology of Depression Depression can affect every aspect of life. A patient undergoing a major depressive episode who receives treatment with any antidepressant will often experience symptomatic
Chapter 1 Neurobiology of Depression Depression can affect every aspect of life. A patient undergoing a major depressive episode who receives treatment with any antidepressant will often experience symptomatic
Depression and Anxiety. What is Depression? What is Depression? By Christopher Okiishi, MD Spring Not just being sad A syndrome of symptoms
 Depression and Anxiety By Christopher Okiishi, MD Spring 2016 What is Depression? Not just being sad A syndrome of symptoms Depressed mood Sleep disturbance Decreased interest in usual activities (anhedonia)
Depression and Anxiety By Christopher Okiishi, MD Spring 2016 What is Depression? Not just being sad A syndrome of symptoms Depressed mood Sleep disturbance Decreased interest in usual activities (anhedonia)
Depression: management of depression in primary and secondary care
 Issue date: December 2004, with amendments April 2007 Quick reference guide (amended) Depression: management of depression in primary and secondary care Amendment of recommendations concerning venlafaxine:
Issue date: December 2004, with amendments April 2007 Quick reference guide (amended) Depression: management of depression in primary and secondary care Amendment of recommendations concerning venlafaxine:
CME. Pharmacotherapy of Depression in Older Adults. Introduction. Major Depression
 CME Pharmacotherapy of Depression in Older Adults This CME learning activity is available at www.geriatricsandaging.ca/cme_page.htm. Participating physicians are entitled to one () MAINPRO-M credit by
CME Pharmacotherapy of Depression in Older Adults This CME learning activity is available at www.geriatricsandaging.ca/cme_page.htm. Participating physicians are entitled to one () MAINPRO-M credit by
Resident Rotation: Collaborative Care Consultation Psychiatry
 Resident Rotation: Collaborative Care Consultation Psychiatry Anna Ratzliff, MD, PhD Ramanpreet Toor, MD James Basinski, MD With contributions from: Jürgen Unützer, MD, MPH, MA Jennifer Sexton, MD, Catherine
Resident Rotation: Collaborative Care Consultation Psychiatry Anna Ratzliff, MD, PhD Ramanpreet Toor, MD James Basinski, MD With contributions from: Jürgen Unützer, MD, MPH, MA Jennifer Sexton, MD, Catherine
The Pharmacist's Role in Major Depressive Disorder: Optimizing Care. Welcome We will begin shortly.
 The Pharmacist's Role in Major Depressive Disorder: Optimizing Care Welcome We will begin shortly. The Canadian Pharmacists Association is pleased to be partnering with Pfizer to highlight the role of
The Pharmacist's Role in Major Depressive Disorder: Optimizing Care Welcome We will begin shortly. The Canadian Pharmacists Association is pleased to be partnering with Pfizer to highlight the role of
Abnormal Mood 6 Mania 9 Hypomania 15 The Syndrome of Depression 17 Mixed States 25
 Contents Preface Part I SYMPTOMS, SYNDROMES, AND DIAGNOSIS 1 1. Normal and Abnormal Mood 5 Abnormal Mood 6 Mania 9 Hypomania 15 The Syndrome of Depression 17 Mixed States 25 2. The Diagnosis of Bipolar
Contents Preface Part I SYMPTOMS, SYNDROMES, AND DIAGNOSIS 1 1. Normal and Abnormal Mood 5 Abnormal Mood 6 Mania 9 Hypomania 15 The Syndrome of Depression 17 Mixed States 25 2. The Diagnosis of Bipolar
Learning Objectives. Faculty. Why Treat Depression in Primary Care. A Real Case. Presenter Disclosure Information
 2:15 3:30 pm Major Depressive Disorder: Improving Models for Care in the Primary Care Setting Presenter Disclosure Information The following relationships exist related to this presentation: Thomas Heinrich,
2:15 3:30 pm Major Depressive Disorder: Improving Models for Care in the Primary Care Setting Presenter Disclosure Information The following relationships exist related to this presentation: Thomas Heinrich,
Chapter 7 - Mood Disorders
 Chapter 7 - Mood Disorders I. DEPRESSION A. Description Symptoms: 5+ constant over 2 weeks - sadness/depressed mood - guilt/remorse/worthlessness - suicidal thoughts - anhedonia (lack of pleasure) - fatigue/lethargy
Chapter 7 - Mood Disorders I. DEPRESSION A. Description Symptoms: 5+ constant over 2 weeks - sadness/depressed mood - guilt/remorse/worthlessness - suicidal thoughts - anhedonia (lack of pleasure) - fatigue/lethargy
How to treat depression with medication: Some rules of thumb
 How to treat depression with medication: Some rules of thumb R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon. Consultant Psychiatrist Regional
How to treat depression with medication: Some rules of thumb R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon. Consultant Psychiatrist Regional
Depression After Traumatic Brain Injury (TBI)
") Depression After Traumatic Brain Injury (TBI) A resource for individuals with traumatic brain injury and their supporters This presentation is based on TBI Model Systems research and was developed with
Depression After Traumatic Brain Injury (TBI) A resource for individuals with traumatic brain injury and their supporters This presentation is based on TBI Model Systems research and was developed with
GREATER MANCHESTER INTERFACE PRESCRIBING GROUP
 GREATER MANCHESTER INTERFACE PRESCRIBING GROUP On behalf of the GREATER MANCHESTER MEDICINES MANAGEMENT GROUP SHARED CARE GUIDELINE FOR THE PRESCRIBING OF SELECTIVE SEROTONIN REUPTAKE INHIBITORS (SSRIs)
GREATER MANCHESTER INTERFACE PRESCRIBING GROUP On behalf of the GREATER MANCHESTER MEDICINES MANAGEMENT GROUP SHARED CARE GUIDELINE FOR THE PRESCRIBING OF SELECTIVE SEROTONIN REUPTAKE INHIBITORS (SSRIs)
Mending the Mind: treatment of the severely mentally ill
 Mending the Mind: treatment of the severely mentally ill First, the bad news Mental Illness Prevalence: putting things in perspective --More than 54 million Americans have a mental disorder in any given
Mending the Mind: treatment of the severely mentally ill First, the bad news Mental Illness Prevalence: putting things in perspective --More than 54 million Americans have a mental disorder in any given
Volume 4; Number 5 May 2010
 Volume 4; Number 5 May 2010 CLINICAL GUIDELINES FOR ANTIDEPRESSANT USE IN PRIMARY AND SECONDARY CARE Lincolnshire Partnership Foundation Trust in conjunction with Lincolnshire PACEF have recently updated
Volume 4; Number 5 May 2010 CLINICAL GUIDELINES FOR ANTIDEPRESSANT USE IN PRIMARY AND SECONDARY CARE Lincolnshire Partnership Foundation Trust in conjunction with Lincolnshire PACEF have recently updated