Depression Pharmacology. PHPP 517 (IT-III) Fall 2011
|
|
|
- Joel Fletcher
- 5 years ago
- Views:
Transcription
1 Depression Pharmacology PHPP 517 (IT-III) Fall 2011
2 Depression
3 Symptoms of Depression Emotional symptoms Physical symptoms Cognitive symptoms Psychomotor symptoms
4 Depression Pharmacology Loss of brain tissue due to neuronal cell death in white matter (Cortico-limbic areas) cortical cortical limbic areas DR LC VTA

5 Depression Pharmacology Monoamine Hypothesis of Depression Monoamines: Reduced 5-HT (DR) levels NE (LC) DA (VTA) Depressed mood Anhedonia Fatigue Difficulty concentrating Changes in weight Sleep disorders cortical cortical limbic areas DR LC VTA
6 Depression Pharmacology Monoamine Hypothesis of Depression Pharmacological Evidence: Reserpine (antihypertensive) Imipramine (antipsychotic) Iproniazid (anti-tuberculosis) 5-HT, NE, DA 5-HT, NE 5-HT, NE, DA Mood depression (in subset of patients) Mood improvement (in depressed patients) Dopamine Norepinephrine VMAT Reserpine VMAT Reserpine DA DA DA NE NE NE monoamines empty MAO Reuptake Transporter monoamines
7 Depression Pathophysiology INCREASED expression of presynaptic 2 receptors G i coupled (inhibitory) DECREASE monoamine release
8 Depression Pathophysiology INCREASED expression of presynaptic 5-HT receptors G i coupled (inhibitory) DECREASE monoamine release
9 Depression Pathophysiology TrkB BDNF Autophosphorylation on five different Tyr residues PIP2 + PI3K Bone-Derived Neurotrophic Factor: growth factor protein that regulates neuronal differentiation and survival PIP3 + AKT + Energy Metabolism Cell Proliferation Transcription/Translation (new gene expression) Cell Survival Cell Migration
10 Depression Pathophysiology AKT - GSK3 + Cell Death - Gene Expression New gene expression is essential for synaptic plasticity

11 Depression Pathophysiology TrkB BDNF Bone-Derived Neurotrophic Factor: growth factor protein that regulates neuronal differentiation and survival Autophosphorylation on five different Tyr residues PIP2 + PLC DAG IP3 Calcium signaling + PKC + Neuronal differentiation Cell Migration
12 Stress-induced depression Chronic stress increase glucocorticoids Disruption of BDNF expression (camp-creb signaling)

13 Depression Pharmacology HPA axis Hypothesis of Depression The Hypothalamic-pituitaryadrenal axis may also play a role in depression. ~50% of patients with depression have increased levels of cortisol
14 Depression Pharmacology HPA axis Hypothesis of Depression Hypothalamus CRH release Anterior pituitary ACTH release Adrenal cortex Cortisol Periphery
15 Depression Pharmacology Stress Cortisol elevated Increase glutamate Increase Calcium signaling Calcium-dependent death enzymes Neuronal cell death
16 Treatment objectives To reduce the symptoms of acute depression Help the patient to function at a level comparable to that before the onset of illness Prevent relapse/future episodes of depression
17 Three phases of treatment Acute phase: 6-10 weeks Attenuate symptoms or remission Continuation phase: 4-9 months after remission is achieved Eliminate residual symptoms Prevent relapse Maintenance phase: months Prevent relapse
18 Non-pharmacological therapy Psychotherapy: Electroconvulsive therapy (ECT): For certain, severe neural disorders If want a quick response, patient has history of poor response to antidepressants but good response to ECT, and patient prefers ECT Light therapy: Effective against seasonal affective disorder
19 Pharmacologic therapy
20 Drug targets for treatment of Inhibit monoamine reuptake transporters Block inhibitory presynaptic receptors Inhibit monoamine oxidases Objective: Increase the concentration of monoamines and their duration in the synaptic cleft Increase monoamine neurotransmission depressive disorders
21 Antidepressant drugs Serotonin reuptake inhibitors (SSRI) Serotonin-norepinephrine reuptake inhibitors (SNRI) Tricyclic antidepressants (TCA) Monoamine oxidase inhibitors (MAOI) Others: Aminoketone Triazolopyradines Tetracyclic antidepressants
22 Depression Pharmacology Drugs used to treat depression Pharmaceutical approaches to increase monoamine activity Inhibit the reuptake of monoamines from the synapse DA DAT NE NET 5-HT SERT Reuptake inhibitors (RI): DRI: Dopamine RI NRI: Norepinephrine RI SSRI: Selective serotonin RI DA NE 5-HT Also... SNRI: Serotonin-norepinephrine RI NDRI: Norepinephrine-dopamine RI SNRDI: Serotonin-norepinephrine-dopamine RI
23 Serotonin selective reuptake inhibitors (SSRI) Generally chosen as first-line antidepressants These compounds are structurally unrelated. NC O O HN CH 3 O O CH 2 CH 2 CH 2 N(CH 3 ) 2 HBr Paroxetine CH 2 Citalopram S-citalopram F N Cl F 3 C C CH 2 CH 2 CH 2 CH 2 O CH 3 N Fluvoxamine O CH 2 CH 2 NH 2 Cl Sertraline O Fluoxetine H C CH 2 CH 2 N CH 3 H Celexa Package Insert, Forest Laboratories, Inc. Physicians Desk Reference
24 Serotonin selective reuptake inhibitors (SSRI) Selectively inhibits serotonin reuptake inhibitors Generally chosen as first-line antidepressant Improved tolerability safety (overdose)
25 Depression SSRIs SSRIs approved in US Fluoxetine (1987) - Prozac Sertraline (1991) - Zoloft Paroxetine (1992) - Paxil Fluvoxamine (1994) - Luvox Citalopram (1998) - Celexa Escitalopram (2002) - Lexapro
26 Depression Pharmacology SSRIs Relative affinities of SSRIs K i (for reuptake transporters) SERT NET ratio Fluoxetine LOWEST affinity, selectivity Sertraline Paroxetine HIGHEST affinity Fluvoxamine Citalopram HIGHEST selectivity
27 Serotonin-norepinephrine reuptake inhibitors (SNRI) Venlafaxine Desvenlafaxine Duloxetine
28 Serotonin-norepinephrine reuptake inhibitors (SNRI) Venlafaxine, Desvenlafaxine, Duloxetine Have both serotonin and norepinephrine reuptake inhibitory properties Inhibition of 5-HT or NE may vary depending on the dose or may be comparable across all doses
29 Depression Pharmacology SNRI Venlafaxine (1993) - Effexor - Wyeth (Pfizer) Duloxetine (2004) - Cymbalta - Lilly Desvenlafaxine (2008) - Pristiq - Wyeth (Pfizer) Milnacipran (2009) - Savella - Cypress
30 Depression Pharmacology TCA Mechanism(s) of action 1 Primary mechanism Reuptake inhibitors: SNRI: Serotonin-Norepinephrine reuptake inhibitors...but profile varies NET > SERT desipramine nortriptyline protriptyline SERT > NET amitriptyline clomipramine* imipramine trimipramine NE NE NET 5-HT 5-HT SERT NE and 5-HT eventually cause changes in receptor populations (basis of drug efficacy) *clomipramine: SERT>>NET
31 Tricyclic antidepressants (TCA) Amitriptyline clomipramine doxepin imipramine Desipramine Nortriptyline Blocks serotonin and norepinephrine reuptake But also affects other receptor systems
32 Depression Pharmacology Tricyclics (TCA) Example: Most tricyclic antidepressants antagonize: Sodium channels Calcium channels Potassium channels
33 Depression Pharmacology MAOI Pharmaceutical approaches to increase monoamine activity Inhibit the enzymatic removal of monoamines NE, DA, 5-HT NE, DA MAO COMT Inactive metabolites MAO inhibitors (MAOI) Iproniazid discovered in 1950 s (as TB drug) But it causes hepatic failure! COMT inhibitors Tried in the 1990 s with MIXED RESULTS Not used clinically
34 Monoamine oxidase inhibitors (MAOI) Phenelzine Selegiline Tranylcypromine Inhibits monoamine oxidase enzymes Increase concentrations of NE, DA and 5-HT Isoform specific Affects other receptor systems monoamines MAO
35 Two isoforms of MAO NE, DA, 5-HT Depression Pharmacology MAOI Substrate specificity profile DA Expression profile MAO-A MAO-B MAO-A: CNS (neurons, glia, synaptic clefts) Peripheral (liver, GI tract) MAO-B: CNS (neurons, glia, synaptic clefts) Peripheral (platelets) Nonspecific and MAO-A specific: Depression, Anxiety MAO-B specific: Parkinson s disease
36 Other antidepressants Triazolopyridines: Trazodone, nefazodone 5-HT2 antagonists and 5-HT reuptake inhibitors Aminoketones: Bupropion Norepinephrine and dopamine reuptake inhibitor Tetracyclics: Mirtazapine Central presynaptic α2-adrenergic autoreceptor and heteroceptor antagonist Inhibits 5-HT2,3 receptors and histamine receptors
37 Depression Pharmacology Others Bupropion (1985) - Wellbutrin NDRI (no effects on 5-HT) Trazodone (1981) - Desyrel (now, Oleptro ) Nefazodone (1994) - Serzone Various (mechanisms unclear) SSRI 5-HT 1A antagonism 5-HT 2A antagonism 1 antagonism 2 antagonism
38 Receptors affected by antidepressants
39 Classical Neurotransmitters: Summary Neurotransmitter Receptor Exitatory or Inhibitory Coupling or Ion ACh machr 1,3,5 Excitatory G q (PLC) ACh machr 2,4 Inhibitory G i (AC, K + ) ACh nachr Excitatory Na +, Ca 2+ DA D 1,5 Excitatory G s (AC) DA D 2,3,4 Inhibitory G i (AC, K + ) 5-HT 5-HT 4,6,7 Excitatory G s (AC) 5-HT 5-HT 2A, 2C Excitatory G q (PLC) 5-HT 5-HT 3 Excitatory Na + 5-HT 5-HT 1A, 1D Inhibitory G i (AC, K + )
40 Classical Neurotransmitters: Summary Neurotransmitter Receptor Exitatory or Inhibitory Coupling or Ion Histamine H 1 Excitatory G s (AC) Histamine H 3 Inhibitory G i (AC, K + ) Glu NMDA Excitatory Na +, Ca 2+ Glu AMPA Excitatory Na + Glu mglur I Excitatory G q (PLC) Glu mglur II,III Inhibitory G i (AC, K + ) GABA GABA A Inhibitory Cl - GABA GABA B Inhibitory G i (AC, K + ) Gly GlyR Inhibitory Cl -
41 Side effects
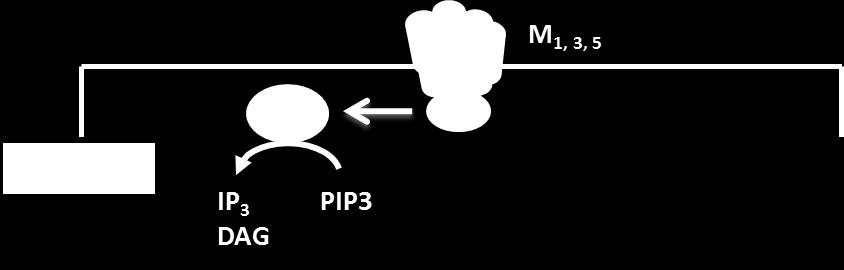

42 Anticholinergic effects Muscarinic ACh receptor regulation


43 Histamine (H1) Blockade Sedation and drowsiness Weight gain Hypotension
44 Orthostatic reflex effects 1 -Adrenergic Receptor Adrenergic receptor regulation Vasodilation Decreased peripheral resistance 1 PLC G q Excitatory IP 3 DAG PIP3
45 Seizures Dose dependent Increase susceptibility: In patients with history of head trauma In patients who had CNS tumor In bulimics and anemic patients (prone to electrolyte imbalance)
46
47 Depression Pharmacology SSRIs and SNRIs SSRI and SNRI Adverse Effects SSRIs and SNRIs DO NOT cause same side effects as TCAs example: fluoxetine vs. desipramine K i (nm) SERT NET H M SSRI and SNRI do NOT cause sedation orthostatic hypotension tachycardia anticholinergic effects* *(paroxetine is mildly anticholinergic)
48 Depression Pharmacology SSRIs and SNRIs SSRI and SNRI Adverse Effects Sexual dysfunction Serotonin Syndrome CNS excitation agitation insomnia anxiety Enteric excitation GI upset nausea
49 Depression Pharmacology TCA Mechanism(s) of action Receptor binding: Antagonism of various receptors (high affinity examples) 1 (amitriptyline, doxepin, trimipramine) H 1 (amitriptyline, doxepin, trimipramine) M 1 (amitriptyline, clomipramine) 5-HT 2 (amitriptyline, doxepin) - may explain clinical benefit Explains side effects: Orthostatic hypotension Tachycardia (supine and postural) Sedation Weight gain Anticholinergic (dry mouth, constipation, etc.)

50 Depression Pharmacology TCA
51 Depression Pharmacology TCA TCAs block sodium and other membrane ion channels. The influx of sodium is the major event responsible for the zero phase of depolarisation in cardiac muscle and Purkinje fibres. As the degree of Na+ channel block increases with use, the QRS width will increase with increasing heart rates.
52 Depression Pharmacology TCA Other cardiac channel effects include reversible inhibition of the outward potassium channels responsible for repolarisation giving a mechanism for QT prolongation and arrhythmia generation TCAs demonstrate a dose dependent direct depressant effect on myocardial contractility that is independent of impaired conduction alter mitochondrial function and uncouple oxidative phosphorylation
53 Depression Pharmacology TCA Other adverse effects Delirium Toxicity caused by M 1 and H 1 blockade Confusion, disorientation caused by high drug levels Dose dependent (at blood levels > 300 ng/ml) Occurs at lower levels in patients with dementia Seizure risk dose-dependent e.g. Clomipramine
54 Depression Pharmacology TCA Other adverse effects Amoxapine metabolized to 7-hydroxy metabolite with neuroleptic (D 2 antipsychotic) activity Thus can cause neuroleptic malignant syndrome (rare) and tardive dyskinesia - rare but worth remembering Imipramine and desipramine have been reported to cause acute hepatitis (potentially fatal) QT prolongation TCAs have been reported to increase QT intervals, potentially cause fatal AV block (but no Boxed warnings or recalls)
55 Antidepressants: targets and side effect profile reuptake antagonism anticholinergic Orthostatic conduction Generic name Trade name Norepinephrine Serotonin Effects Sedation hypotension seizures abnormalities 5HT reuptake inh citalopram Celexa 0 (++++) 0 (+) 0 (++) 0 escitalopram Lexapro 0 (++++) fluoxetine Prozac 0 (+++) (++) 0 fluvoxamine Luvox 0 (++++) (++) 0 paroxetine Paxil 0 (++++) (+) (+) 0 (++) 0 sertraline Zoloft 0 (++++) (++) 0 5HT/NE reuptake inh venlafaxine Effexor (++++) (++++) (+) (+) 0 (++) (+) desvenlafaxine Pristiq (++++) (++++) (+) (+) 0 (++) (+) duloxetine Cymbalta (++++) (++++) (+) 0 (+) 0 0 Aminoketone bupropion Wellbutrin (+) 0 (+) 0 0 (++++) (+) Triazolopyradines nefazodone Serzone 0 (++) 0 (+++) (+++) (++) (+) trazodone Desyrel 0 (++) 0 (++++) (+++) (++) (+) Tetracyclic mirtazapine Remeron 0 0 (+) (++) (++) 0 (+) Tricyclics tertiary amines amitriptyline Elavil (++) (++++) (++++) (++++) (+++) (+++) (+++) clomipramine Anafranil (++) (+++) (++++) (++++) (++) (++++) (+++) doxepin Sinequan (++) (++) (+++) (++++) (++) (+++) (++) imipramine Tofranil (++++) (+++) (+++) (+++) (++++) (+++) (+++) secondary amines desipramine Norpramin (++++) (+) (++) (++) (++) (++) (++) nortriptyline Pamelor (+++) (++) (++) (++) (+) (++) (++) Monoamine oxidase in phenelzine Nardil (++) (++) (+) (++) (++) (+) selegeline Emsam (+) (++) 0 0 tranylcypromine Parnate (++) (+) (+) (+) (++) (+) (+)
56 Pharmacokinetics of antidepressants
57 SSRI SSRI have half life of approximately 1-2 days, up to 7 days for Citalopram Reaches steady state in 3-6 days, up to days with Fluoxetine Subject to first pass metabolism SSRI Citalopram Fluoxetine Fluvoxamine Paroxetine Sertraline CYP enzyme metabolism 2C19 mediates initial step, then 2D6 2D6 partially responsible not known 2D6 principal P450 3A3/4 responsible for demethylation
58 SSRI Pharmacokinetics Routes: All ORAL Depression Pharmacology SSRIs Absorption: Generally well absorbed (small intestine) Affected by food? ONLY sertraline (slower absorption, more complete) Distribution: Lipophilic HIGH V d (10-40 L/kg) Highly protein bound (75-99%) High bioavailability 80-95%, except for Paroxetine and Sertraline
59 Depression Pharmacology SSRIs SSRI Pharmacokinetics Half-lives: Varies, most about hours Metabolism: Two SSRIs form active metabolites (via CYP2C9, CYP2C19) P450 fluoxetine norfluoxetine (equally active) sertraline N-desmethylsertraline (active) Similar metabolites from other SSRIs are mostly inactive: citalopram N-desmethylcitalopram (DCT, 10% active)
60 SSRI Drug interactions Depression Pharmacology SSRIs Interactions occur with other classes of antidepressants MAOI serotonin syndrome TCA potentiation of side effects CYP1A2 Inhibitors Fluvoxamine 1A2 Substrates Some TCAs Clozapine Olanzapine Caffeine CYP2C19 Inhibitors Fluvoxamine 2C19 Substrates Some TCAs Proton pump inhibitors Diazepam Phenobarbital CYP2D6 Inhibitors Fluoxetine Paroxetine 2D6 Substrates Some TCAs Some antipsychotics blockers Antiarrhythmics Opioids
61 SNRI Venlafaxine is well absorbed after oral admin. Subject to first-pass metabolism producing desvenlafaxine (active metabolite) Has half life of 4hours Metabolized by CYP2D6 Desvenlafaxine has half life of 8 hours Desvenlafaxine is metabolized by CYP3A4 CYP2D6 Venlafaxine Desvenlafaxine (active) 10% bioavailable 80% bioavailable
62 Depression Pharmacology SNRIs SNRI Pharmacokinetics Less protein binding than TCAs or SSRIs ONLY 10-30% bound (except duloxetine, 90% to albumin) Lower V d than TCAs or SSRIs (3-10 L/kg)
63 Depression Pharmacology SNRIs SNRI Metabolism SNRI Drug Interactions Interactions occur with other classes of antidepressants MAOI serotonin syndrome TCA potentiation of side effects Duloxetine + alcohol abuse hepatitis (contraindicated)
64 Depression Pharmacology TCAs Well absorbed after oral administration Reach plasma concentrations within 2-6 hours Extensively bound to plasma proteins (63-97%) Active metabolites Metabolized by CYP2D6, CYP2C19, CYP1A2, CYP3A4
65 Depression Pharmacology MAOIs Pharmacokinetic parameters not well defined Half lives, distribution, metabolism, excretion not well known Half lives of little interest because these are irreversible MAO inhibitors Selegiline is metabolized to methamphetamine and levoamphetamine May account for some of the clinical effects
66 Pharmacokinetics of other antidepressants
67 Tetracyclic antidepressant Mirtazapine is rapidly absorbed after oral administration Subject to first-pass metabolism Bioavailability about 50% Half life of hours Reach steady state levels after 4-9 days Metabolized by four or more CYP enzymes Metabolites have no activity
68 Triazolopyradines: nefazodone Rapidly absorbed after oral administration Subject to first-pass metabolism Metabolized to produce active metabolite (m-cpp) Metabolized by CYP2D6 Half life is 2-4 hours Metabolites have longer half lives
69 Triazolopyradines: trazodone Rapidly absorbed after oral administration Subject to first-pass metabolism More than 90% is bound to plasma protein Metabolized by CYP2D6 Has active metabolite (m-cpp) Has a half life of 4-14 hours
70 Depression Pharmacology Trazodone and Nefazodone Metabolism Trazodone CYP3A4 Nefazodone m-chlorophenylpiperazine (M-CPP) illicit drug (psychoactive - anxiogenic) Serotonin AGONIST at many different receptors
71 Depression Pharmacology Bupropion Rapidly absorbed after oral administration Subject to first pass metabolism Metabolized by CYP2D6 and CYP2B6 Half life of 14 hours Bupropion Bupropion is a CYP2D6 Inhibitor Hydroxybupropion (ACTIVE) 2D6 Substrates Some TCAs Some antipsychotics blockers Antiarrhythmics Opioids
72 Summary: Pharmacokinetics of antidepressants t1/2 time to peak [plasma] %pl. prot binding %bioavail cl.imp.metab. hep enz r.o.ad. 5HT reuptake inh citalopram 33h 2-4h 80 >80 CYP3A4, CYP2C19 oral escitalopram 27-32h 5h CYP3A4, CYP2C20 oral fluoxetine 4-6days 4-8h norfluoxetine CYP2D6 oral fluvoxamine 15-26h 2-8h oral paroxetine 24-31h 5-7h 95 CYP2D6 oral sertraline 27h 6-8h CYP2B6, CYP2D6, CYP2C9, CYP2C19, CYCP3A4 oral 5HT/NE reuptake inh venlafaxine 5h 2h O-desmethylvenlafaxine CYP2D6 oral desvenlafaxine 11h 7.5h CYP3A4 oral duloxetine 12h 6h CYP2D6, CYP1A2 oral Aminoketone bupropion 10-21h 3h hydroxybupropion CYP2B6, CYP2D6 oral threhydrobupropion erythrohydrobupropion Triazolopyradines nefazodone 2-4h 1h meta-chlorophenylpiperazine oral trazodone 6-11h 1-2h 92 meta-chlorophenylpiperazine CYP3A4 oral Tetracyclic mirtazapine 20-40h 2h CYP2D6, CYP3A4 oral Tricyclics oral tertiary amines amitriptyline 9-46h 1-5h nortriptyline CYP2C19, CYP1A2, CYP2D6 oral clomipramine 20-24h 2-6h desmethylclomipramine CYP1A2 oral, IM, IV doxepin 8-36h 1-4h desmethyldoxepin oral, IM, IV imipramine 6-34h 1.5-3h desipramine oral secondary amines desipramine 11-46h 3-6h hydroxydesipramine oral nortriptyline 16-88h 3-12h hydroxynortriptyline CYP2D6 oral
73 Discussion
BRIEF ANTIDEPRESSANT OVERVIEW. Casey Gallimore, Pharm.D., M.S.
 BRIEF ANTIDEPRESSANT OVERVIEW Casey Gallimore, Pharm.D., M.S. Antidepressant Medication Classes First Generation Tricyclic Antidepressants (TCAs) Monoamine Oxidase Inhibitors (MAOIs) Second Generation
BRIEF ANTIDEPRESSANT OVERVIEW Casey Gallimore, Pharm.D., M.S. Antidepressant Medication Classes First Generation Tricyclic Antidepressants (TCAs) Monoamine Oxidase Inhibitors (MAOIs) Second Generation
PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES
 PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES Table of Contents Print TABLE OF CONTENTS Drug Page Number Anafranil... 2 Asendin... 4 Celexa... 4 Cymbalta... 6 Desyrel... 8 Effexor...10 Elavil...14
PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES Table of Contents Print TABLE OF CONTENTS Drug Page Number Anafranil... 2 Asendin... 4 Celexa... 4 Cymbalta... 6 Desyrel... 8 Effexor...10 Elavil...14
Psychobiology Handout
 Nsg 85A / Psychiatric Page 1 of 7 Psychobiology Handout STRUCTURE AND FUNCTION OF THE BRAIN Psychiatric illness and the treatment of psychiatric illness alter brain functioning. Some examples of this are
Nsg 85A / Psychiatric Page 1 of 7 Psychobiology Handout STRUCTURE AND FUNCTION OF THE BRAIN Psychiatric illness and the treatment of psychiatric illness alter brain functioning. Some examples of this are
Antidepressant Medication Strategies We ve Come a Long Way or Have We? Who Writes Prescriptions for Psychotropic Medications. Biological Psychiatry
 Antidepressant Medication Strategies We ve Come a Long Way or Have We? Joe Wegmann, PD, LCSW The PharmaTherapist Joe@ThePharmaTherapist.com 504.587.9798 www.pharmatherapist.com Are you receiving our free
Antidepressant Medication Strategies We ve Come a Long Way or Have We? Joe Wegmann, PD, LCSW The PharmaTherapist Joe@ThePharmaTherapist.com 504.587.9798 www.pharmatherapist.com Are you receiving our free
PHARMACODYNAMICS OF ANTIDEPRESSANTS MOOD STABILIZING AGENTS ANXIOLYTICS SEDATIVE-HYPNOTICS
 PHARMACODYNAMICS OF ANTIDEPRESSANTS MOOD STABILIZING AGENTS ANXIOLYTICS SEDATIVE-HYPNOTICS Yogesh Dwivedi, Ph.D. Assistant Professor of Psychiatry and Pharmacology Psychiatric Institute Department of Psychiatry
PHARMACODYNAMICS OF ANTIDEPRESSANTS MOOD STABILIZING AGENTS ANXIOLYTICS SEDATIVE-HYPNOTICS Yogesh Dwivedi, Ph.D. Assistant Professor of Psychiatry and Pharmacology Psychiatric Institute Department of Psychiatry
TREATMENT OF DEPRESSION IN LATE LIFE. Robert Kohn, MD
 TREATMENT OF DEPRESSION IN LATE LIFE Robert Kohn, MD WHY TREAT ELDERLY PERSONS Major depression is not a normal part of aging The rates are lower than younger cohorts The prevalence rates are still high
TREATMENT OF DEPRESSION IN LATE LIFE Robert Kohn, MD WHY TREAT ELDERLY PERSONS Major depression is not a normal part of aging The rates are lower than younger cohorts The prevalence rates are still high
Optimal Use of Antidepressants: Focusing on SNRI, NDRI and SSRE
 Optimal Use of Antidepressants: Focusing on SNRI, NDRI and SSRE Chan-Hyung Kim, MD Severance Mental Health Hospital Institute of Behavioral Science in Medicine Diagnostic Criteria Pyramid Etiologic Pathophysiologic
Optimal Use of Antidepressants: Focusing on SNRI, NDRI and SSRE Chan-Hyung Kim, MD Severance Mental Health Hospital Institute of Behavioral Science in Medicine Diagnostic Criteria Pyramid Etiologic Pathophysiologic
BELBUCA (buprenorphine buccal film)
") RATIONALE FOR INCLUSION IN PA PROGRAM Background Belbuca is indicated for the management of chronic pain severe enough to require daily, aroundthe-clock, long-acting opioid treatment for which alternative
RATIONALE FOR INCLUSION IN PA PROGRAM Background Belbuca is indicated for the management of chronic pain severe enough to require daily, aroundthe-clock, long-acting opioid treatment for which alternative
Diagnosis & Management of Major Depression: A Review of What s Old and New. Cerrone Cohen, MD
 Diagnosis & Management of Major Depression: A Review of What s Old and New Cerrone Cohen, MD Why You re Treating So Much Mental Health 59% of Psychiatrists Are Over the Age of 55 AAMC 2014 Physician specialty
Diagnosis & Management of Major Depression: A Review of What s Old and New Cerrone Cohen, MD Why You re Treating So Much Mental Health 59% of Psychiatrists Are Over the Age of 55 AAMC 2014 Physician specialty
3. Atypical antidepressants
 3. Atypical antidepressants Bupropion, mirtazapine, nefazodone & trazodone. Mixed group that act at several different sites. Bupropion Acts as a weak dopamine & NE reuptake inhibitor. Has short half-life.
3. Atypical antidepressants Bupropion, mirtazapine, nefazodone & trazodone. Mixed group that act at several different sites. Bupropion Acts as a weak dopamine & NE reuptake inhibitor. Has short half-life.
OXYCODONE IR (oxycodone)
") RATIONALE FOR INCLUSION IN PA PROGRAM Background Oxycodone hydrochloride, a pure opioid agonist, is used in the treatment of moderate to severe pain (1-2). The precise mechanism of action is unknown; however,
RATIONALE FOR INCLUSION IN PA PROGRAM Background Oxycodone hydrochloride, a pure opioid agonist, is used in the treatment of moderate to severe pain (1-2). The precise mechanism of action is unknown; however,
90 dosage units per 90 days OR. Extended-release Formulations Ultram ER 90 dosage units per 90 days OR
 Pre - PA Allowance 12 years of age or older Quantity Immediate-release Formulation Ultracet 720 dosage units per 90 days OR Ultram 720 dosage units per 90 days Extended-release Formulations Ultram ER 90
Pre - PA Allowance 12 years of age or older Quantity Immediate-release Formulation Ultracet 720 dosage units per 90 days OR Ultram 720 dosage units per 90 days Extended-release Formulations Ultram ER 90
RATIONALE FOR INCLUSION IN PA PROGRAM
 RATIONALE FOR INCLUSION IN PA PROGRAM Background Tramadol is a centrally acting synthetic opioid analgesic used to treat moderate to moderately severe chronic pain in adults. Along from analgesia, tramadol
RATIONALE FOR INCLUSION IN PA PROGRAM Background Tramadol is a centrally acting synthetic opioid analgesic used to treat moderate to moderately severe chronic pain in adults. Along from analgesia, tramadol
Xartemis XR (oxycodone / acetaminophen extended release)
") RATIONALE FOR INCLUSION IN PA PROGRAM Background Xartemis XR is a combination of oxycodone and acetaminophen in a dosage formulation to deliver both immediate pain relief, in less than an hour, and extended-release
RATIONALE FOR INCLUSION IN PA PROGRAM Background Xartemis XR is a combination of oxycodone and acetaminophen in a dosage formulation to deliver both immediate pain relief, in less than an hour, and extended-release
Duragesic Patch (fentanyl patch) Prior authorization is not required if prescribed by an oncologist
 Prior authorization is not required if prescribed by an oncologist") Pre - PA Allowance Quantity 30 patches every 90 days Prior-Approval Requirements Prior authorization is not required if prescribed by an oncologist Age 2 years of age or older Diagnosis Patient must have
Pre - PA Allowance Quantity 30 patches every 90 days Prior-Approval Requirements Prior authorization is not required if prescribed by an oncologist Age 2 years of age or older Diagnosis Patient must have
Treating Depression in Adults
 Treating Depression in Adults By Deborah Christensen, Ph.D., M.S.C.P. Depressive Disorders represent a broad and heterogeneous group of commonly diagnosed psychological disorders. The DSM adequately describes
Treating Depression in Adults By Deborah Christensen, Ph.D., M.S.C.P. Depressive Disorders represent a broad and heterogeneous group of commonly diagnosed psychological disorders. The DSM adequately describes
Antidepressants and Sedatives. David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School
 Antidepressants and Sedatives David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School Depression A frequent problem, affecting up to 5% of the population Common presentations
Antidepressants and Sedatives David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School Depression A frequent problem, affecting up to 5% of the population Common presentations
Introduction to Drug Treatment
 Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
HYSINGLA ER (hydrocodone bitartrate) Prior authorization is not required if prescribed by an oncologist.
 Prior authorization is not required if prescribed by an oncologist.") Pre - PA Allowance None Prior authorization is not required if prescribed by an oncologist. Prior-Approval Requirements Age 18 years of age or older Diagnosis Patient must have the following: 1. Pain,
Pre - PA Allowance None Prior authorization is not required if prescribed by an oncologist. Prior-Approval Requirements Age 18 years of age or older Diagnosis Patient must have the following: 1. Pain,
RATIONALE FOR INCLUSION IN PA PROGRAM
 RATIONALE FOR INCLUSION IN PA PROGRAM Background hydromorphone (Exalgo, Dilaudid) and oxymorphone (Opana and Opana ER) are Schedule II narcotics prescribed to treat moderate to severe pain. Morphine produces
RATIONALE FOR INCLUSION IN PA PROGRAM Background hydromorphone (Exalgo, Dilaudid) and oxymorphone (Opana and Opana ER) are Schedule II narcotics prescribed to treat moderate to severe pain. Morphine produces
Prepared by: Elizabeth Vicens-Fernandez, LMHC, Ph.D.
 Prepared by: Elizabeth Vicens-Fernandez, LMHC, Ph.D. Sources: National Institute of Mental Health (NIMH), the National Alliance on Mental Illness (NAMI), and from the American Psychological Association
Prepared by: Elizabeth Vicens-Fernandez, LMHC, Ph.D. Sources: National Institute of Mental Health (NIMH), the National Alliance on Mental Illness (NAMI), and from the American Psychological Association
MORPHINE IR DRUG CLASS Morphine IR, Dilaudid IR (hydromorphone), Opana IR (oxymorphone)
, Opana IR (oxymorphone)") Pre - PA Allowance Tablets & Suppositories Morphine sulfate tablets Morphine sulfate suppositories Oxymorphone tablets Hydromorphone tablets Hydromorphone suppositories 360 tablets per 90 days OR 360 suppositories
Pre - PA Allowance Tablets & Suppositories Morphine sulfate tablets Morphine sulfate suppositories Oxymorphone tablets Hydromorphone tablets Hydromorphone suppositories 360 tablets per 90 days OR 360 suppositories
Pre - PA Allowance. Prior-Approval Requirements LEVORPHANOL TARTRATE. None
 Pre - PA Allowance None Prior-Approval Requirements Prior authorization is not required if prescribed by an oncologist and/or the member has paid pharmacy claims for an oncology medication(s) in the past
Pre - PA Allowance None Prior-Approval Requirements Prior authorization is not required if prescribed by an oncologist and/or the member has paid pharmacy claims for an oncology medication(s) in the past
Anti-Depressant Medications
 Anti-Depressant Medications A Introduction: This topic may be a little bit underestimated here in Jordan, while in western countries it has more significance. The function of anti-depressants is to change
Anti-Depressant Medications A Introduction: This topic may be a little bit underestimated here in Jordan, while in western countries it has more significance. The function of anti-depressants is to change
Affective or Mood Disorders. Dr. Alia Shatanawi March 12, 2018
 Affective or Mood Disorders Dr. Alia Shatanawi March 12, 2018 Affective or Mood Disorders Reactive Depression. Secondary: Medical Neurological Drugs Major (Endogenous) Depression = Unipolar: Depressed
Affective or Mood Disorders Dr. Alia Shatanawi March 12, 2018 Affective or Mood Disorders Reactive Depression. Secondary: Medical Neurological Drugs Major (Endogenous) Depression = Unipolar: Depressed
Treatment of Major Depressive Disorder
 Treatment of Major Depressive Disorder Sarah Mullowney, MD PGY3 Psychiatry Resident, University of Utah Paula Gibbs, MD Medical Director of 5 West at UUMC Clerkship Director MS III Psychiatric Rotation
Treatment of Major Depressive Disorder Sarah Mullowney, MD PGY3 Psychiatry Resident, University of Utah Paula Gibbs, MD Medical Director of 5 West at UUMC Clerkship Director MS III Psychiatric Rotation
Linda Sobeski Farho, PharmD, BCPS Assistant Professor, Pharmacy Practice UNMC College of Pharmacy Critical Issues in Geriatrics June 24, 2010
 Pharmacologic Treatment of Depression Linda Sobeski Farho, PharmD, BCPS Assistant Professor, Pharmacy Practice UNMC College of Pharmacy Critical Issues in Geriatrics June 24, 2010 1 Disclosure I have no
Pharmacologic Treatment of Depression Linda Sobeski Farho, PharmD, BCPS Assistant Professor, Pharmacy Practice UNMC College of Pharmacy Critical Issues in Geriatrics June 24, 2010 1 Disclosure I have no
Medications and Children Disorders
 Mental Health Comprehensive Services Providing Family Stability and Developing Life Coping Skills Medications and Children Disorders Psychiatric medications can be an effective part of the treatment for
Mental Health Comprehensive Services Providing Family Stability and Developing Life Coping Skills Medications and Children Disorders Psychiatric medications can be an effective part of the treatment for
Psychopharmacological Management of Depressive and Anxiety Disorders
 Psychopharmacological Management of Depressive and Anxiety Disorders Waseem Ahmed, M.D Medical Director: Population Health and Dallas County Correctional System Email: waseem.ahmed@phhs.org Tel: 214-653-2927
Psychopharmacological Management of Depressive and Anxiety Disorders Waseem Ahmed, M.D Medical Director: Population Health and Dallas County Correctional System Email: waseem.ahmed@phhs.org Tel: 214-653-2927
Common Antidepressant Medications for Adults
 (and Citalopram (Celexa) Escitalopram (Lexapro) Fluoxetine (Prozac) Fluoxetine Weekly (Prozac Weekly) 20 in AM w/ food (10 mg in elderly or those w/ panic disorder) 20 40 40 (If age >60yo, max 20) 10 10
(and Citalopram (Celexa) Escitalopram (Lexapro) Fluoxetine (Prozac) Fluoxetine Weekly (Prozac Weekly) 20 in AM w/ food (10 mg in elderly or those w/ panic disorder) 20 40 40 (If age >60yo, max 20) 10 10
RATIONALE FOR INCLUSION IN PA PROGRAM
 RATIONALE FOR INCLUSION IN PA PROGRAM Background Methadone hydrochloride is a long-acting opioid agonist at mu-opioid receptors that is used to manage pain that requires long-term, daily opioid treatment
RATIONALE FOR INCLUSION IN PA PROGRAM Background Methadone hydrochloride is a long-acting opioid agonist at mu-opioid receptors that is used to manage pain that requires long-term, daily opioid treatment
The Context: Why is this so important to treat?
 Depression for PG1s Ian A. Cook, M.D. UCLA Department of Psychiatry Laboratory of Brain, Behavior, and Pharmacology Semel Institute for Neuroscience & Human Behavior DepressionLA.com PsychiatryGuidelines.com
Depression for PG1s Ian A. Cook, M.D. UCLA Department of Psychiatry Laboratory of Brain, Behavior, and Pharmacology Semel Institute for Neuroscience & Human Behavior DepressionLA.com PsychiatryGuidelines.com
Antidepressants Choosing the Right One
 Antidepressants Choosing the Right One Dr Lim Boon Leng Consultant Psychiatrist Dr BL Lim Centre For Psychological Wellness #09-09, Gleneagles Medical Centre, 6 Napier Rd, S258499 www.psywellness.com.sg
Antidepressants Choosing the Right One Dr Lim Boon Leng Consultant Psychiatrist Dr BL Lim Centre For Psychological Wellness #09-09, Gleneagles Medical Centre, 6 Napier Rd, S258499 www.psywellness.com.sg
Study Guidelines for Quiz #1
 Annex to Section J Page 1 Study Guidelines for Quiz #1 Theory and Principles of Psychopharmacology, Classifications and Neurotransmitters, Anxiolytics/Antianxiety/Minor Tranquilizers, Stimulants, Nursing
Annex to Section J Page 1 Study Guidelines for Quiz #1 Theory and Principles of Psychopharmacology, Classifications and Neurotransmitters, Anxiolytics/Antianxiety/Minor Tranquilizers, Stimulants, Nursing
Drugs Used in Mood Disorders
 33 Drugs Used in Mood Disorders Herbert E. Ward and Albert J. Azzaro DRUG LIST GENERIC NAME PAGE GENERIC NAME PAGE Amitriptyline 389 Amoxapine 389 Bupropion 388 Carbamazepine 395 Citalopram 388 Clomipramine
33 Drugs Used in Mood Disorders Herbert E. Ward and Albert J. Azzaro DRUG LIST GENERIC NAME PAGE GENERIC NAME PAGE Amitriptyline 389 Amoxapine 389 Bupropion 388 Carbamazepine 395 Citalopram 388 Clomipramine
Major Depressive Disorder
 Major Depressive Disorder HEDIS Measures And Clinical Practice Guidelines Jennifer Highley, PMHNP-BC Behavioral Health West Point Healthcare Effectiveness Data and Information Set (HEDIS) Performance measures
Major Depressive Disorder HEDIS Measures And Clinical Practice Guidelines Jennifer Highley, PMHNP-BC Behavioral Health West Point Healthcare Effectiveness Data and Information Set (HEDIS) Performance measures
Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Treatment of Depression in the Primary Care Office
 Treatment of Depression in the Primary Care Office Paul E.A. Glaser, MD, PhD Departments of Psychiatry, Pediatrics and Anatomy & Neurobiology University of Kentucky November 5, 2010 Disclosures of Potential
Treatment of Depression in the Primary Care Office Paul E.A. Glaser, MD, PhD Departments of Psychiatry, Pediatrics and Anatomy & Neurobiology University of Kentucky November 5, 2010 Disclosures of Potential
9/20/2011. Integrated Care for Depression & Anxiety: Psychotropic Medication Management for PCPs. Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Drugs for Emotional and Mood Disorders Chapter 16
 Drugs for Emotional and Mood Disorders Chapter 16 NCLEX-RN Review Question 1 Choices Please note Question #1 at the end of Ch 16 pg 202 & Key pg 805 answer is #4 1. Psychomotor symptoms 2. Tachycardia,
Drugs for Emotional and Mood Disorders Chapter 16 NCLEX-RN Review Question 1 Choices Please note Question #1 at the end of Ch 16 pg 202 & Key pg 805 answer is #4 1. Psychomotor symptoms 2. Tachycardia,
Depression. There are several forms of depression (depressive disorders). Major depressive disorder and dysthymic disorder are the most common.
. Major depressive disorder and dysthymic disorder are the most common.") Depression Depression is a state of low mood and aversion to activity that can affect a person's thoughts, behavior, feelings and sense of well-being. People with depressed mood can feel sad, anxious,
Depression Depression is a state of low mood and aversion to activity that can affect a person's thoughts, behavior, feelings and sense of well-being. People with depressed mood can feel sad, anxious,
Primary Care Management of Depression. John Briles, MD, Medical Director October 11, 2017
 John Briles, MD, Medical Director October 11, 2017 Molina Healthcare of Michigan uses a HEDIS measure for Antidepressant Medication Management (AMM) to measure how well treating providers (PCPs) appropriately
John Briles, MD, Medical Director October 11, 2017 Molina Healthcare of Michigan uses a HEDIS measure for Antidepressant Medication Management (AMM) to measure how well treating providers (PCPs) appropriately
Levorphanol. Levorphanol Tartrate. Description
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.59 Subject: Levorphanol Page: 1 of 8 Last Review Date: March 17, 2017 Levorphanol Description Levorphanol
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.59 Subject: Levorphanol Page: 1 of 8 Last Review Date: March 17, 2017 Levorphanol Description Levorphanol
Drugs, Sleep & Wakefulness. Brian Koo Reena Mehra MD MS Kingman Strohl MD
 Drugs, Sleep & Wakefulness Brian Koo Reena Mehra MD MS Kingman Strohl MD Things To Keep In Mind Many drugs effect sleep either causing insomnia or sedation Disruption of sleep and wakefulness may not be
Drugs, Sleep & Wakefulness Brian Koo Reena Mehra MD MS Kingman Strohl MD Things To Keep In Mind Many drugs effect sleep either causing insomnia or sedation Disruption of sleep and wakefulness may not be
Butrans (buprenorphine patch) Description. Section: Prescription Drugs Effective Date: October 1, 2017
 Description. Section: Prescription Drugs Effective Date: October 1, 2017") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Butrans Page: 1 of 9 Last Review Date: September 15, 2017 Butrans (buprenorphine patch) Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Butrans Page: 1 of 9 Last Review Date: September 15, 2017 Butrans (buprenorphine patch) Description
ANTIDEPRESSANTS IN USE IN CLINICAL PRACTICE
 Medicinska naklada - Zagreb, Croatia Conference paper ANTIDEPRESSANTS IN USE IN CLINICAL PRACTICE Mark Agius 1 & Hannah Bonnici 2 1 Clare College, University of Cambridge, Cambridge, UK 2 Hospital Pharmacy
Medicinska naklada - Zagreb, Croatia Conference paper ANTIDEPRESSANTS IN USE IN CLINICAL PRACTICE Mark Agius 1 & Hannah Bonnici 2 1 Clare College, University of Cambridge, Cambridge, UK 2 Hospital Pharmacy
The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders What are functional GI disorders?
 The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders Christine B. Dalton, PA-C Douglas A. Drossman, MD and Kellie Bunn, PA-C What are functional GI
The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders Christine B. Dalton, PA-C Douglas A. Drossman, MD and Kellie Bunn, PA-C What are functional GI
Review of Psychotrophic Medications. (An approved North Carolina Division of Health Services Regulation Continuing Education Course)
") Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
10/27/09! Psychopharmacology 101 for the LADC! Disclosures! Lecture outline! Structural divisions of the nervous system!
 Disclosures! Psychopharmacology 101 for the LADC! David A. Frenz, M.D.! Mental Health & Addiction Services! St. Josephʼs Hospital! I am employed by the HealthEast Care System! I do not have any financial
Disclosures! Psychopharmacology 101 for the LADC! David A. Frenz, M.D.! Mental Health & Addiction Services! St. Josephʼs Hospital! I am employed by the HealthEast Care System! I do not have any financial
Nucynta IR. Nucynta IR (tapentadol immediate-release) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Nucynta IR Page: 1 of 9 Last Review Date: December 8, 2017 Nucynta IR Description Nucynta IR (tapentadol
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Nucynta IR Page: 1 of 9 Last Review Date: December 8, 2017 Nucynta IR Description Nucynta IR (tapentadol
Belbuca (buprenorphine buccal film) Belbuca (buprenorphine buccal film) Description
 Belbuca (buprenorphine buccal film) Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Belbuca Page: 1 of 9 Last Review Date: September 15, 2017 Belbuca (buprenorphine buccal film)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Belbuca Page: 1 of 9 Last Review Date: September 15, 2017 Belbuca (buprenorphine buccal film)
Levorphanol. Levorphanol Tartrate. Description
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.59 Subject: Levorphanol Page: 1 of 8 Last Review Date: March 16, 2018 Levorphanol Description Levorphanol
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.59 Subject: Levorphanol Page: 1 of 8 Last Review Date: March 16, 2018 Levorphanol Description Levorphanol
Treat mood, cognition, and behavioral disturbances associated with psychological disorders. Most are not used recreationally or abused
 Psychiatric Drugs Psychiatric Drugs Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally or abused Benzodiazepines
Psychiatric Drugs Psychiatric Drugs Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally or abused Benzodiazepines
WESTMEAD PRIMARY EXAM GROUP PSYCHOTROPIC MEDICATIONS
 WESTMEAD PRIMARY EXAM GROUP PSYCHOTROPIC MEDICATIONS DOPAMINE HYPOTHESIS Excessive limbic dopamine is hypothesised to cause psychosis Many antipsychotics inhibit dopamine 2 receptors in mesolimbic and
WESTMEAD PRIMARY EXAM GROUP PSYCHOTROPIC MEDICATIONS DOPAMINE HYPOTHESIS Excessive limbic dopamine is hypothesised to cause psychosis Many antipsychotics inhibit dopamine 2 receptors in mesolimbic and
Depression Update. Disclosure. Outline 1/28/2018. David Justice, MD FAPA Director of Behavioral Health Sumter Family Health Center
 Depression Update David Justice, MD FAPA Director of Behavioral Health Sumter Family Health Center Disclosure No significant relationships to disclose Outline Overview of depression Standard treatment
Depression Update David Justice, MD FAPA Director of Behavioral Health Sumter Family Health Center Disclosure No significant relationships to disclose Outline Overview of depression Standard treatment
Belbuca (buprenorphine buccal film) Description. Section: Prescription Drugs Effective Date: October 1, 2016
 Description. Section: Prescription Drugs Effective Date: October 1, 2016") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Belbuca Page: 1 of 9 Last Review Date: September 15, 2016 Belbuca (buprenorphine buccal film)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Belbuca Page: 1 of 9 Last Review Date: September 15, 2016 Belbuca (buprenorphine buccal film)
Quick Guide to Common Antidepressants-Adults
 Quick Guide to Common Antidepressants-Adults Medication Therapeutic Range (mg/day) Initial Suggested Serotonin Reuptake Inhibitors (SSRIs) All available as generic FLUOXETINE (Prozac) CITALOPRAM (Celexa
Quick Guide to Common Antidepressants-Adults Medication Therapeutic Range (mg/day) Initial Suggested Serotonin Reuptake Inhibitors (SSRIs) All available as generic FLUOXETINE (Prozac) CITALOPRAM (Celexa
Psychiatry curbside: Answers to a primary care doctor s top mental health questions
 Psychiatry curbside: Answers to a primary care doctor s top mental health questions April 27, 2018 Laurel Ralston, DO Psychiatrist, Taussig Cancer Institute Objectives Review current diagnostic and prescribing
Psychiatry curbside: Answers to a primary care doctor s top mental health questions April 27, 2018 Laurel Ralston, DO Psychiatrist, Taussig Cancer Institute Objectives Review current diagnostic and prescribing
Depression and Anxiety. What is Depression? What is Depression? By Christopher Okiishi, MD Spring Not just being sad A syndrome of symptoms
 Depression and Anxiety By Christopher Okiishi, MD Spring 2016 What is Depression? Not just being sad A syndrome of symptoms Depressed mood Sleep disturbance Decreased interest in usual activities (anhedonia)
Depression and Anxiety By Christopher Okiishi, MD Spring 2016 What is Depression? Not just being sad A syndrome of symptoms Depressed mood Sleep disturbance Decreased interest in usual activities (anhedonia)
Guilt Suicidality. Depression Co-Occurs with Medical Illness The rate of major depression among those with medical illness is significant.
 1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
Demerol (meperidine oral tablet, oral solution), Meperitab (oral tablet)
, Meperitab (oral tablet)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Meperidine Page: 1 of 7 Last Review Date: September 15, 2017 Meperidine Description Demerol (meperidine
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Meperidine Page: 1 of 7 Last Review Date: September 15, 2017 Meperidine Description Demerol (meperidine
PSYCHIATRIC DRUGS. Mr. D.Raju, M.pharm, Lecturer
 PSYCHIATRIC DRUGS Mr. D.Raju, M.pharm, Lecturer PSYCHIATRIC DRUGS Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally
PSYCHIATRIC DRUGS Mr. D.Raju, M.pharm, Lecturer PSYCHIATRIC DRUGS Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally
Anti- Depressants, Mood Stabilizers: What Works Best For Bipolar Disorder? Date: March 30, 2007 Source: NIH/National Institute of.
 30-3-2007 Anti- Depressants, Mood Stabilizers: What Works Best For Bipolar Disorder? Date: March 30, 2007 Source: NIH/National Institute of. 30-3-2018 C. Psychiatric drugs: controlled trial demonstrated
30-3-2007 Anti- Depressants, Mood Stabilizers: What Works Best For Bipolar Disorder? Date: March 30, 2007 Source: NIH/National Institute of. 30-3-2018 C. Psychiatric drugs: controlled trial demonstrated
A Brief Overview of Psychiatric Pharmacotherapy. Joel V. Oberstar, M.D. Chief Executive Officer
 A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
Nortriptyline vs amitriptyline in elderly
 Nortriptyline vs amitriptyline in elderly Amitriptyline (Elavil ) vs other antidepressants - comparative analysis amitriptyline vs divalproate, amitriptyline vs trazodone. Learn what other patients are
Nortriptyline vs amitriptyline in elderly Amitriptyline (Elavil ) vs other antidepressants - comparative analysis amitriptyline vs divalproate, amitriptyline vs trazodone. Learn what other patients are
Study Guide Unit 3 Psych 2022, Fall 2003
 Psychological Disorders: General Study Guide Unit 3 Psych 2022, Fall 2003 1. What are psychological disorders? 2. What was the main treatment for some psychological disorders prior to the 1950 s? 3. What
Psychological Disorders: General Study Guide Unit 3 Psych 2022, Fall 2003 1. What are psychological disorders? 2. What was the main treatment for some psychological disorders prior to the 1950 s? 3. What
Hysingla ER. Hysingla ER (hydrocodone bitartrate) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.38 Subject: Hysingla ER Page: 1 of 9 Last Review Date: September 15, 2017 Hysingla ER Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.38 Subject: Hysingla ER Page: 1 of 9 Last Review Date: September 15, 2017 Hysingla ER Description
Antidepressants. BMF 83 - Antidepressants
 Antidepressants BMF 83 - Antidepressants Depression is a common psychiatric disorder impacting millions of people worldwide. It is caused by an imbalance of chemicals in the brain, namely serotonin and
Antidepressants BMF 83 - Antidepressants Depression is a common psychiatric disorder impacting millions of people worldwide. It is caused by an imbalance of chemicals in the brain, namely serotonin and
Realities of Depression in Primary Care Setting
 Realities of Depression in Primary Care Setting Jaroslava Salman, MD Department of Supportive Care Medicine Division of Psychiatry Click to edit Master Presentation Date August 4 th 2018 Disclosure I have
Realities of Depression in Primary Care Setting Jaroslava Salman, MD Department of Supportive Care Medicine Division of Psychiatry Click to edit Master Presentation Date August 4 th 2018 Disclosure I have
Duragesic patch. Duragesic patch (fentanyl patch) Description
 Description") 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.31 Subject: Duragesic patch Page: 1 of 9 Last Review Date: September 15, 2017 Duragesic patch Description Duragesic patch (fentanyl
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.31 Subject: Duragesic patch Page: 1 of 9 Last Review Date: September 15, 2017 Duragesic patch Description Duragesic patch (fentanyl
Antidepressant Pharmacology An Overview
 Figure 1. Antidepressant Pharmacology An Overview Source: NEJM 2005;353:1819-34 Figure 2. 1 Figure 3: Antidepressant Pharmacology pictures: Weak inhibition Bupropion NOTE: CYP enzymes noted are those inhibited
Figure 1. Antidepressant Pharmacology An Overview Source: NEJM 2005;353:1819-34 Figure 2. 1 Figure 3: Antidepressant Pharmacology pictures: Weak inhibition Bupropion NOTE: CYP enzymes noted are those inhibited
Antidepressants. Dr Malek Zihlif
 Antidepressants The optimal use of antidepressant required a clear understanding of their mechanism of action, pharmacokinetics, potential drug interaction and the deferential diagnosis of psychiatric
Antidepressants The optimal use of antidepressant required a clear understanding of their mechanism of action, pharmacokinetics, potential drug interaction and the deferential diagnosis of psychiatric
Antidepressant Selection in Primary Care
 Antidepressant Selection in Primary Care Rebecca D. Lewis, DO OOA Summer CME Oklahoma City, OK 6 August 2017 Objectives Understand the epidemiology of depression. Recognize factors to help choose antidepressants.
Antidepressant Selection in Primary Care Rebecca D. Lewis, DO OOA Summer CME Oklahoma City, OK 6 August 2017 Objectives Understand the epidemiology of depression. Recognize factors to help choose antidepressants.
Antidepressants. NEPHAR 305 Pharmaceutical Chemistry I. Assist.Prof.Dr. Banu Keşanlı
 Antidepressants EPHAR 305 Pharmaceutical Chemistry I Assist.Prof.Dr. Banu Keşanlı 1 Antidepressants What is depression? Depression is not a disease per se, but a clinical disorder that is manifested by
Antidepressants EPHAR 305 Pharmaceutical Chemistry I Assist.Prof.Dr. Banu Keşanlı 1 Antidepressants What is depression? Depression is not a disease per se, but a clinical disorder that is manifested by
DRUGS THAT ACT IN THE CNS
 DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
Duragesic patch. Duragesic patch (fentanyl patch) Description
 Description") 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.31 Section: Prescription Drugs Effective Date: April1, 2017 Subject: Duragesic patch Page: 1 of 10 Last Review Date: March
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.31 Section: Prescription Drugs Effective Date: April1, 2017 Subject: Duragesic patch Page: 1 of 10 Last Review Date: March
Embeda. Embeda (morphine sulfate and naltrexone hydrochloride) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.39 Subject: Embeda Page: 1 of 8 Last Review Date: September 15, 2017 Embeda Description Embeda (morphine
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.39 Subject: Embeda Page: 1 of 8 Last Review Date: September 15, 2017 Embeda Description Embeda (morphine
The Context: Why is this so important to treat?
 ER Management of Depression for PGY1s Ian A. Cook, M.D. Director, UCLA Depression Research Program UCLA Department of Psychiatry Laboratory of Brain, Behavior, and Pharmacology Semel Institute for Neuroscience
ER Management of Depression for PGY1s Ian A. Cook, M.D. Director, UCLA Depression Research Program UCLA Department of Psychiatry Laboratory of Brain, Behavior, and Pharmacology Semel Institute for Neuroscience
Management of SSRI Induced Sexual Dysfunction. Serotonin Reuptake Inhibitors*
 Management of SSRI Induced Sexual Dysfunction John J. Miller, M.D. Medical Director, Center for Health and WellBeing Exeter, NH Serotonin Reuptake Inhibitors* fluoxetine clomipramine sertraline paroxetine
Management of SSRI Induced Sexual Dysfunction John J. Miller, M.D. Medical Director, Center for Health and WellBeing Exeter, NH Serotonin Reuptake Inhibitors* fluoxetine clomipramine sertraline paroxetine
Depression. University of Illinois at Chicago College of Nursing
 Depression University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this session, participants will be better able to: 1. Recognize depression, its symptoms and behaviors
Depression University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this session, participants will be better able to: 1. Recognize depression, its symptoms and behaviors
Partners in Care Quick Reference Cards
 Partners in Care Quick Reference Cards Supported by the Agency for Healthcare Research and Quality MR-1198/8-AHRQ R This project was funded by the Agency for Healthcare Research and Quality (AHRQ), formerly
Partners in Care Quick Reference Cards Supported by the Agency for Healthcare Research and Quality MR-1198/8-AHRQ R This project was funded by the Agency for Healthcare Research and Quality (AHRQ), formerly
Depression in Pregnancy
 TREATING THE MOTHER PROTECTING THE UNBORN A MOTHERISK Educational Program The content of this program reflects the expression of a consensus on emerging clinical and scientific advances as of the date
TREATING THE MOTHER PROTECTING THE UNBORN A MOTHERISK Educational Program The content of this program reflects the expression of a consensus on emerging clinical and scientific advances as of the date
Guide to Psychiatric Medications for Children and Adolescents
 Guide to Psychiatric Medications for Children and Adolescents by Glenn S. Hirsch, M.D. The following guide includes most of the medications used to treat child and adolescent mental disorders. It lists
Guide to Psychiatric Medications for Children and Adolescents by Glenn S. Hirsch, M.D. The following guide includes most of the medications used to treat child and adolescent mental disorders. It lists
Ruby Williams, M.D. Drugs, Alcohol and Sleep February 24, 2018
 Ruby Williams, M.D. Drugs, Alcohol and Sleep February 24, 2018 Objectives Describe pharmacology of commonly prescribed drugs for stimulants and hypnotics Brief review of common drugs that affect sleep
Ruby Williams, M.D. Drugs, Alcohol and Sleep February 24, 2018 Objectives Describe pharmacology of commonly prescribed drugs for stimulants and hypnotics Brief review of common drugs that affect sleep
Children s Hospital Of Wisconsin
 Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Appendix: Psychotropic Medication Reference Tables
 Appendix: Psychotropic Medication Reference Tables How to Use these Tables These reference tables are designed to provide clinic staff with specific medication related criteria for the Polypharmacy, Cardiometabolic
Appendix: Psychotropic Medication Reference Tables How to Use these Tables These reference tables are designed to provide clinic staff with specific medication related criteria for the Polypharmacy, Cardiometabolic
MAJOR DEPRESSION CLINICAL PRACTICE GUIDELINE
 MAJOR DEPRESSION CLINICAL PRACTICE GUIDELINE Reviewed and Updated by the Behvioral Health Subcommittee 7/20/2017 Topic Purpose Access Assessment 7/2017 Recommendations SummaCare Health Plan bases its Clinical
MAJOR DEPRESSION CLINICAL PRACTICE GUIDELINE Reviewed and Updated by the Behvioral Health Subcommittee 7/20/2017 Topic Purpose Access Assessment 7/2017 Recommendations SummaCare Health Plan bases its Clinical
Overview and Update on Current Psychopharmacological Medications, Including New Medications in Clinical Trials
 SPEAKER NOTES Overview and Update on Current Psychopharmacological Medications, Including New Medications in Clinical Trials Summarized by Thomas T. Thomas New psychotropic medications are coming on the
SPEAKER NOTES Overview and Update on Current Psychopharmacological Medications, Including New Medications in Clinical Trials Summarized by Thomas T. Thomas New psychotropic medications are coming on the
Treatment of Neuropathic Pain: What Does the Evidence Say? or Just the Facts Ma am
 Treatment of Neuropathic Pain: What Does the Evidence Say? or Just the Facts Ma am Tim R Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy Cleveland Clinic Akron General Center for Family
Treatment of Neuropathic Pain: What Does the Evidence Say? or Just the Facts Ma am Tim R Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy Cleveland Clinic Akron General Center for Family
Psycho-pharmacologic Therapy. Objectives
 Psycho-pharmacologic Therapy for Functional Bowel Disorders John J. Hutchings, M.D. Assistant Professor of Medicine and Psychiatry Louisiana i State t University it School of Medicine i Department of Medicine
Psycho-pharmacologic Therapy for Functional Bowel Disorders John J. Hutchings, M.D. Assistant Professor of Medicine and Psychiatry Louisiana i State t University it School of Medicine i Department of Medicine
Major Depressive Disorder: Diagnosis, Treatment & Impact on Rural Communities
 Page 1 Major Depressive Disorder: Diagnosis, Treatment & Impact on Rural Communities Elizabeth Montagnese, M.D. Adult, Child and Adolescent Psychiatrist This program has been supported by an educational
Page 1 Major Depressive Disorder: Diagnosis, Treatment & Impact on Rural Communities Elizabeth Montagnese, M.D. Adult, Child and Adolescent Psychiatrist This program has been supported by an educational
John J. Miller, M.D. October 2, 2015
 Pharmacokinetic and Pharmacodynamic Differences Among Antidepressants October 2, 2015 John J. Miller, M.D. Medical Director, Brain Health Staff Psychiatrist, Seacoast Mental Health Center Consulting Psychiatrist,
Pharmacokinetic and Pharmacodynamic Differences Among Antidepressants October 2, 2015 John J. Miller, M.D. Medical Director, Brain Health Staff Psychiatrist, Seacoast Mental Health Center Consulting Psychiatrist,
Mental Health Nursing: Mood Disorders. By Mary B. Knutson, RN, MS, FCP
 Mental Health Nursing: Mood Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Mood Prolonged emotional state that influences the person s whole personality and life functioning Adaptive Functions
Mental Health Nursing: Mood Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Mood Prolonged emotional state that influences the person s whole personality and life functioning Adaptive Functions
Dual Diagnosis: Substance Abuse and Mental Illness
 Dual Diagnosis: Substance Abuse and Mental Illness and a review of the major PSYCHIATRIC MEDICINES Mark Stanford, Ph.D. Santa Clara Valley Health & Hospital System Department of Alcohol & Drug Services
Dual Diagnosis: Substance Abuse and Mental Illness and a review of the major PSYCHIATRIC MEDICINES Mark Stanford, Ph.D. Santa Clara Valley Health & Hospital System Department of Alcohol & Drug Services
Morphine IR Hydromorphone IR Oxymorphone IR. Morphine IR, Dilaudid IR (hydromorphone), Opana IR (oxymorphone),
, Opana IR (oxymorphone),") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.33 Subject: Morphine IR Drug Class Page: 1 of 11 Last Review Date: December 8, 2017 Morphine IR Hydromorphone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.33 Subject: Morphine IR Drug Class Page: 1 of 11 Last Review Date: December 8, 2017 Morphine IR Hydromorphone
Change Your Brain, Change Your Life. The Breakthrough Program for Conquering Anxiety, Depression, Obsessiveness, Anger, and Impulsiveness
 Change Your Brain, Change Your Life The Breakthrough Program for Conquering Anxiety, Depression, Obsessiveness, Anger, and Impulsiveness Daniel G Amen Three Rivers Press New York Appendix Medication 1.
Change Your Brain, Change Your Life The Breakthrough Program for Conquering Anxiety, Depression, Obsessiveness, Anger, and Impulsiveness Daniel G Amen Three Rivers Press New York Appendix Medication 1.
Duragesic patch. Duragesic patch (fentanyl patch) Description. Section: Prescription Drugs Effective Date: January 1, 2019
 Description. Section: Prescription Drugs Effective Date: January 1, 2019") 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Duragesic patch Page: 1 of 9 Last Review Date: November 30, 2018 Duragesic patch Description Duragesic patch (fentanyl
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Duragesic patch Page: 1 of 9 Last Review Date: November 30, 2018 Duragesic patch Description Duragesic patch (fentanyl
ANTI-DEPRESSANT MEDICATIONS
 ANTI-DEPRESSANT MEDICATIONS This information is not intended to be a substitute for medical advice. It s purpose is solely informative. If your client or yourself are taking antidepressants, do not change
ANTI-DEPRESSANT MEDICATIONS This information is not intended to be a substitute for medical advice. It s purpose is solely informative. If your client or yourself are taking antidepressants, do not change
Depression major depressive disorder. Some terms: Major Depressive Disorder: Major Depressive Disorder:
 Depression major depressive disorder Oldest recognized disorder: melancholia It is a positive and active anguish, a sort of psychical neuralgia wholly unknown to normal life. - William James "I am now
Depression major depressive disorder Oldest recognized disorder: melancholia It is a positive and active anguish, a sort of psychical neuralgia wholly unknown to normal life. - William James "I am now