Regional Therapy for Metastatic Neuroendocrine Tumors. Janette Durham, MD Professor of Radiology University of Colorado School of Medicine
|
|
|
- Clyde Randall Hubbard
- 5 years ago
- Views:
Transcription
1 Regional Therapy for Metastatic Neuroendocrine Tumors Janette Durham, MD Professor of Radiology University of Colorado School of Medicine
2 Introduce regional therapy for mnet Arterial therapies Injection of particles into the hepatic artery to block the oxygen supply with addition of chemotherapeutic or radiation source Trans-arterial embolization (TAE) Trans-arterial chemoembolization (TACE) Conventional chemoembolization (ctace) Drug-eluting bead embolization (DEB-TACE) Trans-arterial radioembolization with Y90 (TARE) Ablation therapy Place needle probe directly into tumor to heat, freeze, or poison tumor cells
3 Interventional Radiologist Member of a multi-disciplinary cancer team Image guided therapy (minimally invasive surgery) Supportive therapy Biopsies Central venous access Fluid drainage paracentesis /thoracentesis Enteral feeding Non-operative management of post operative complications Non-surgical palliative cancer therapy
4 Disclosure NET tumors are rare 5.25 per 100,000 with prevalence of 100,000 in US. (2014)* Evidence for regional therapy is limited to small retrospective single institutional reviews Tumor location - pnet vs. carcinoid (foregut, midgut, hindgut) was not initially considered Tumor biology including tumor staging, proliferation index (Ki67,MIB-1), angioinvasion, and mitoses typically not considered Castellano. Cancer Chemother Pharmacol 2014.
5 Background Curative liver resection feasible in 10% of patients with liver metastasis 73% 4-Y survival Regional therapy has a role in the treatment of metastatic disease to liver that is not amenable to surgery for anatomic or clinical reasons, when liver involvement is dominant Anatomic considerations Multiple lesions Bilobar disease
6 Indication 1. Management of hormone symptoms refractory to somatostatin analogues 2. Disease progression 3. Mass symptoms from large tumors or extensive tumor burden-pain, abdominal distention, early satiety Treatment of early disease remains controversial due to the indolent nature of the disease
7 Patient selection Clinical considerations Good performance status ECOG < 2.0 Adequate liver reserve Bilirubin mg/dl Normal (correctable) coagulation profile
8 Contraindications Liver insufficiency or obstructive jaundice Involvement of > 50% of liver Renal insufficiency Biliary-enteric anastomosis Significant portal vein thrombosis Reduction in cardiac ejection fraction <50%
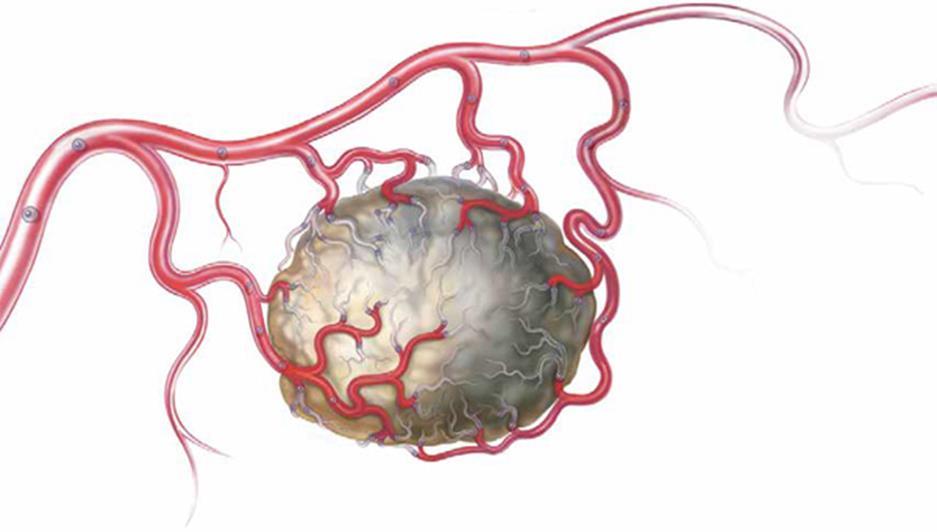
9 Mechanism of intra-arterial therapy Dual blood supply to the liver Dominant low oxygen portal circulation - 80% High oxygen hepatic arterial circulation - 20% NET lesions are hypervascular and fed from the hepatic artery Delivery of agent into hepatic arterial circulation at level dictated by anatomic distribution of lesions High concentration of agent near the tumor with low concentration escaping to the systemic circulation
10
11


12

13 Trans-arterial embolization (TAE) micron spherical embolic particles introduced to block high oxygen blood supply to tumors causing tumor necrosis. Embolization to stasis of arterial vasculature of hemiliver vs. segment Perfusion to uninvolved liver is maintained by the portal vein permitting selective targeting of tumor 2-3 sessions separated by 4-6 weeks Repeatable until vasculature does not support therapy.

14
15 Factors affecting morbidity, mortality, and 30 day survival 320 consecutive procedures in 137 patients ( ) mean OS 43 months (similar for carcinoid and pnet) OS 82,57,35M 1,3,5Y Factors negatively effecting OS Urgent HAE for symptom management > 50% tumor involvement Extrahepatic mets Additive effect with OS of 86 m cw 8.5 m if all three factors present Factors negatively effecting 30 day mortality Urgent therapy Male Sofocleous. JVIR 2014:25:22
16 Conventional trans-arterial chemoembolization (ctace) Chemotherapy mixed with a carrier (Lipiodol) injected into the hepatic artery. Distributed by blood flow, concentrating drug in tumors 5:1. Chemotherapy delivered in high concentration enhances coagulative tumor necrosis Followed by particle embolization to cause ischemic necrosis. Hypoxia further enhances effect of drug. 2-3 sessions separate by 6-8 weeks Repeatable until vasculature does not support therapy or cumulative drug limit reached.

17
18
19
20 Drug-eluting bead trans-arterial chemoembolization (DEB-TACE) Chemotherapy loaded on to bead Beads carry drug to peritumoral capillary bed Drug slowly elutes off beads over days creating highly concentrated prolonged exposure to drug

21 LC Beads Drug delivery system comprising biocompatible, non resorable hydrogel beads loaded with anthracyclin derivatives Higher tumor concentrations and lower systemic concentrations of doxorubicin compared to ctace Better tolerated permitting repeat procedures in shorter intervals. Concern about biliary injuries
22 Results Response in 52-86% patients with duration of response often longer than 12 months Complete symptomatic response in 70% Survival 36M favoring carcinoid over pnet (Hur) 123 patients - 33M vs 23M favoring carcinoid over pnet(gupta) 103 patients 7Y when sunitinib, everolimus, and somatostatin analogs added (debarre) Hur. JVIR 2013;24 Gupta.Cancer 2005;104 debarre.eurj Endo 2014;e
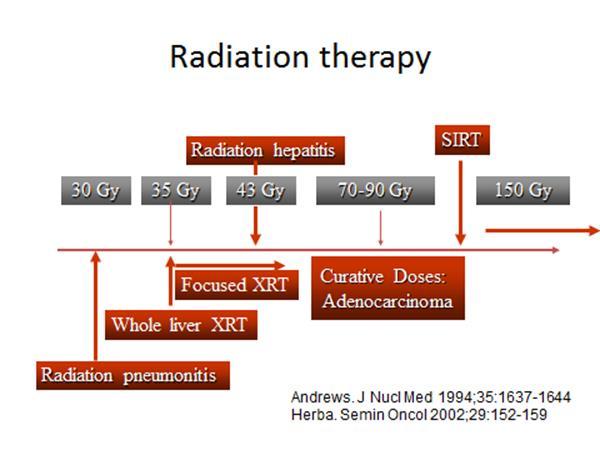
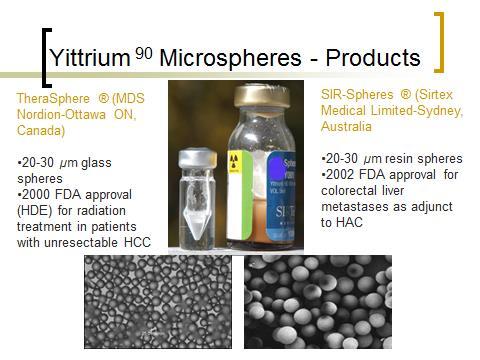
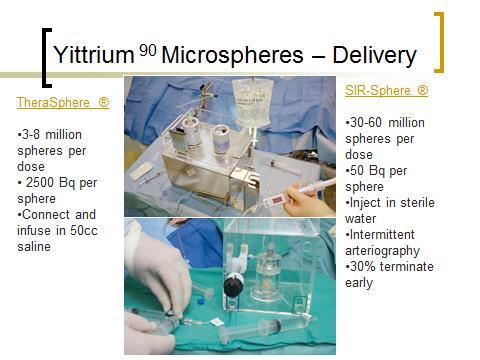
23 Transarterial radioembolization (TARE) micron resin or glass beads loaded with Yttrium 90 injected into peritumoral capillary bed Targeted doses of 120 Gy or greater to tumor
24
25 Yttrium 90 Microspheres β particle emitter (.936 MeV) as it decays to stable zirconium-90 Maximum penetration < 10mm (mean < 2.5 mm) Half life of 64 hrs, mean life of 3.85 days 94% of radiation delivered in 11 days Tumor to non-tumor uptake may triple the absorbed dose in tumor Classified as brachytherapy devices Regulated by the US Nuclear Regulatory Commission
26
27
28 Results 40 patients treated with TheraSphere Median dose 113 Gy CR 20%; PR43% (EASL) Time to response was 4.9M OS 72.5,62.5,45% at 1,2,3 Y Memon.Int J Radiat Oncol Biol Phys 2012;83
29 Pre procedure management Octreotide prior to procedure added to monthly maintainace dose? Hold angiogenic inhibitors Sutent, Everolimus Hydration Antibiotics Prophylactic single dose When biliary intervention or enteric anastomosis prolonged administration Single dose steroids Anti-emetics for nausea Sedation


30

31



32
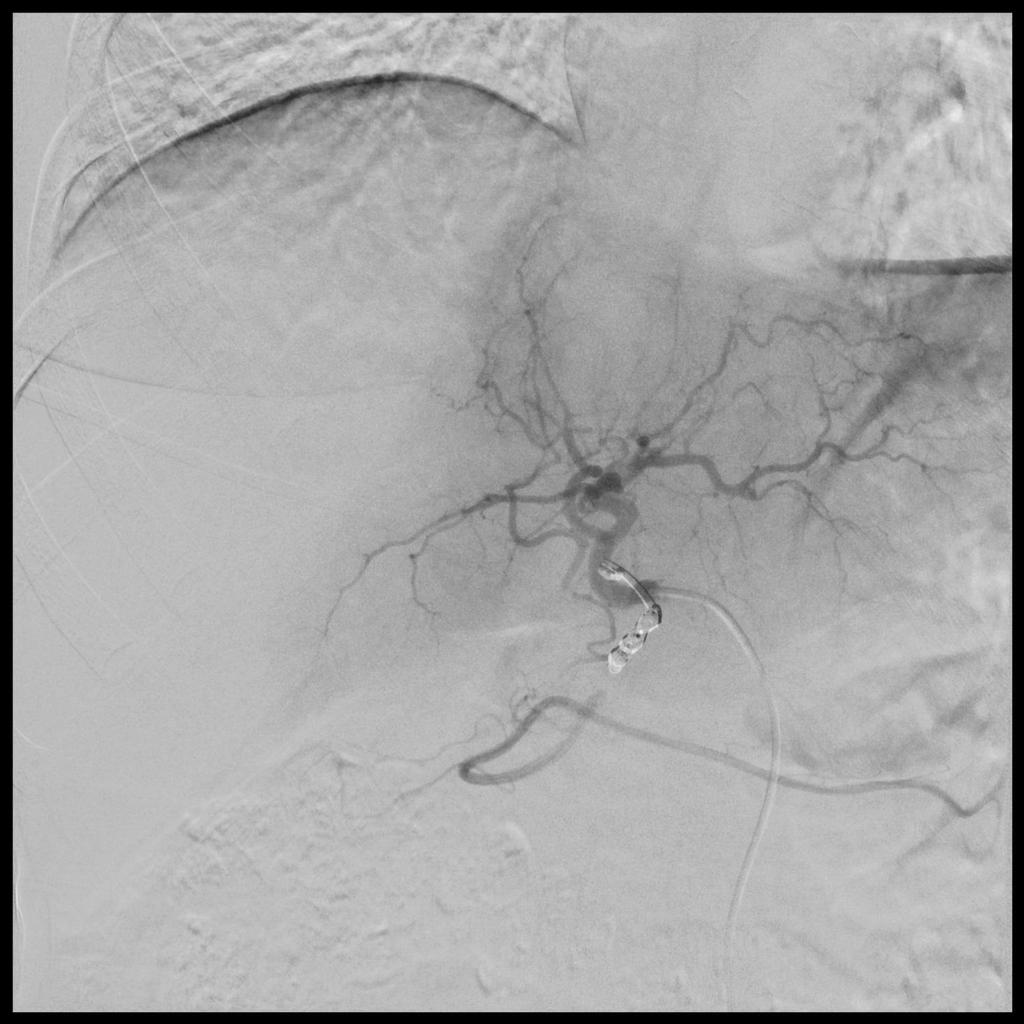
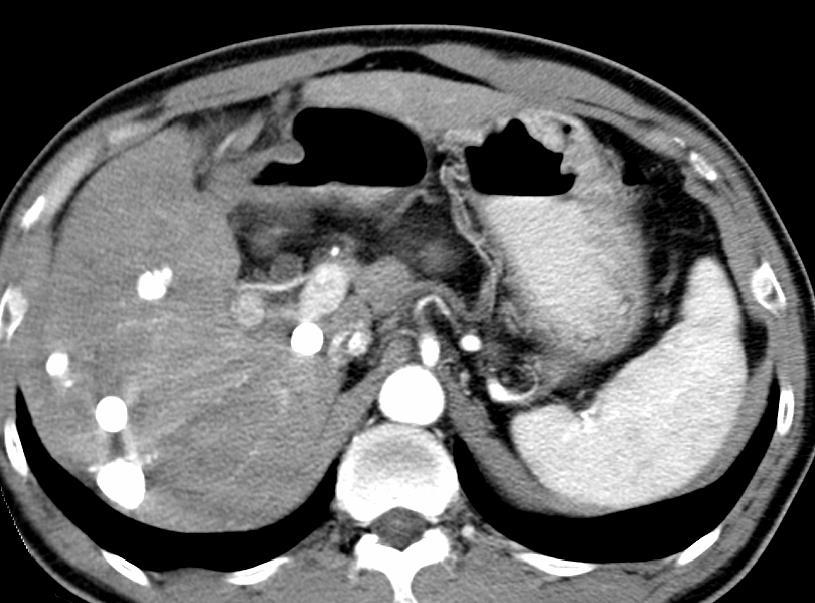
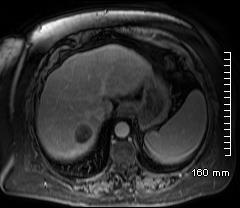
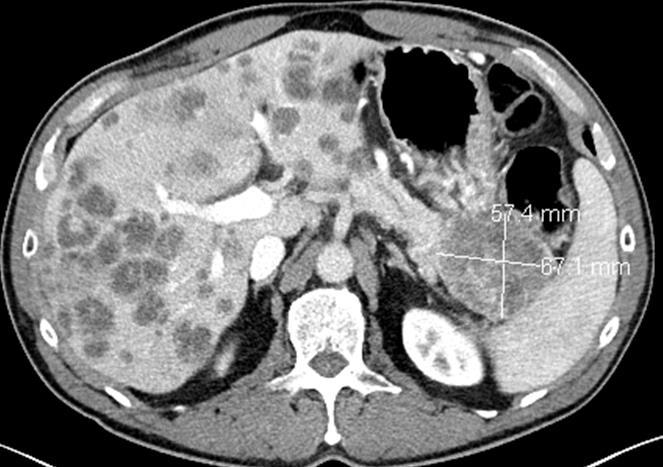
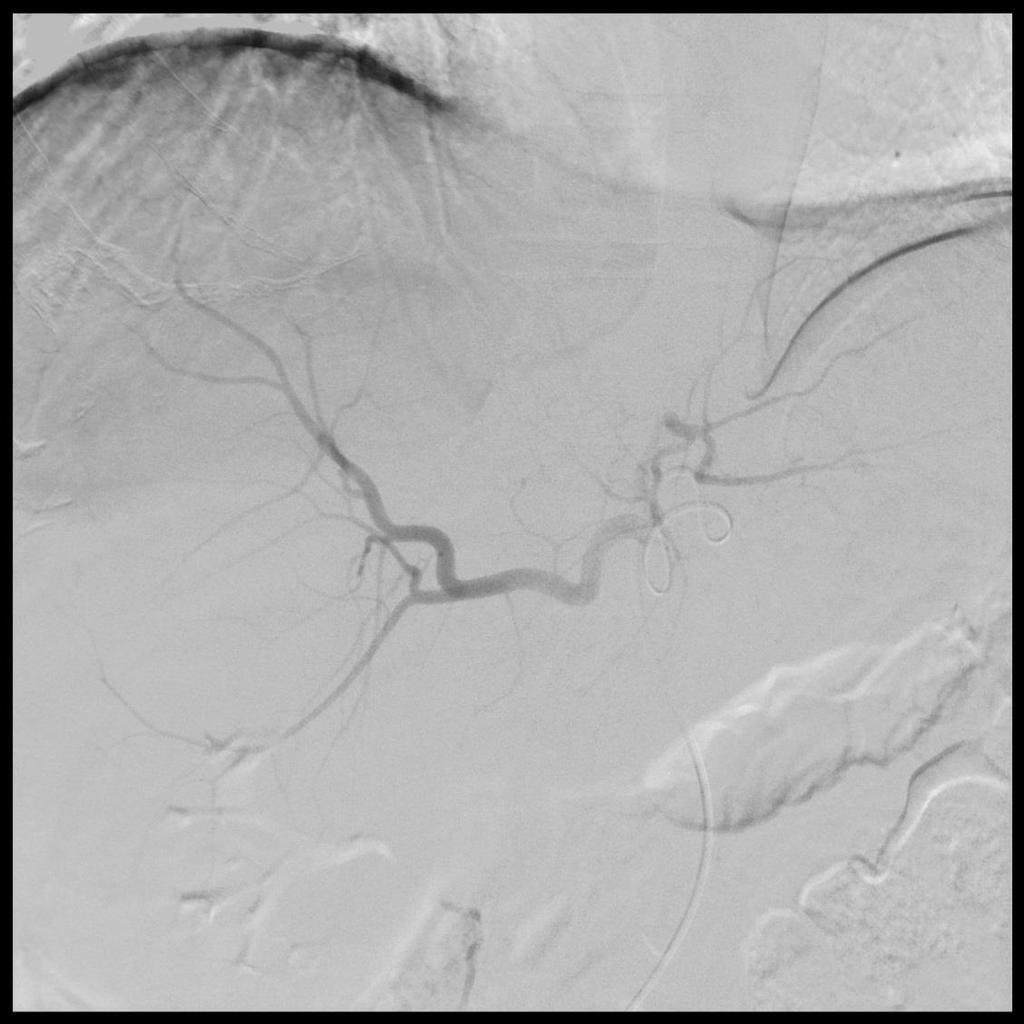
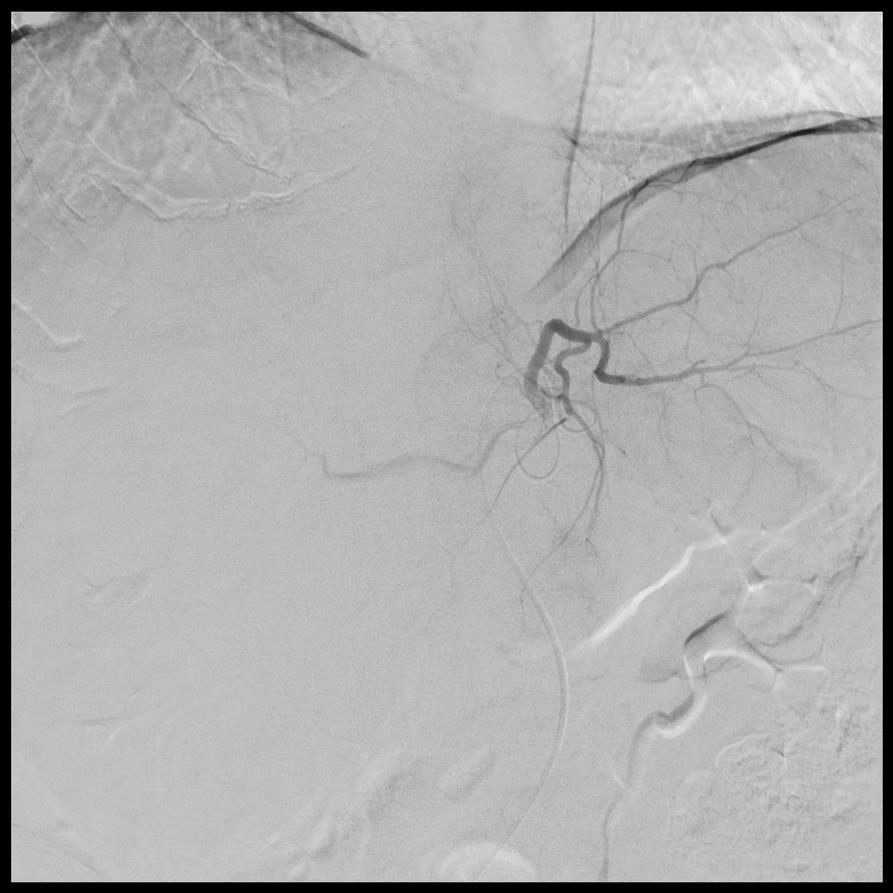
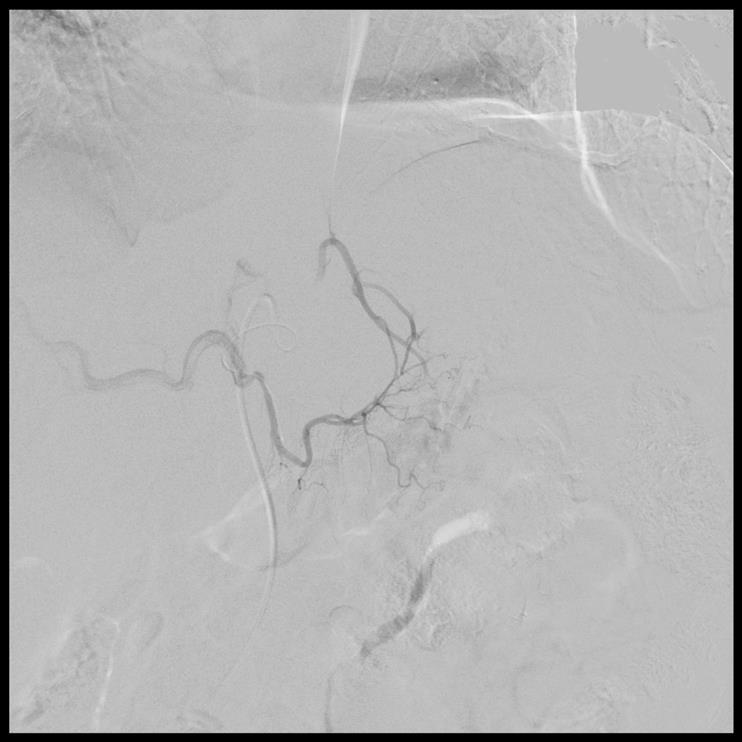
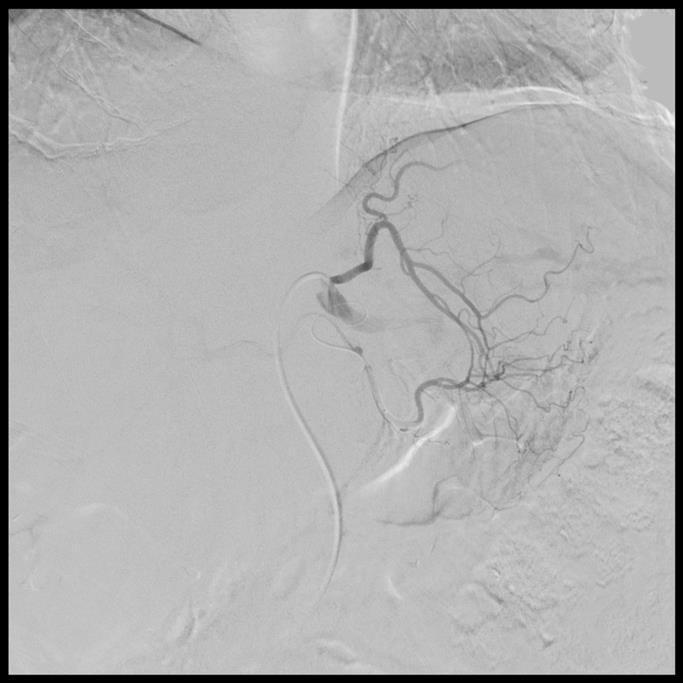
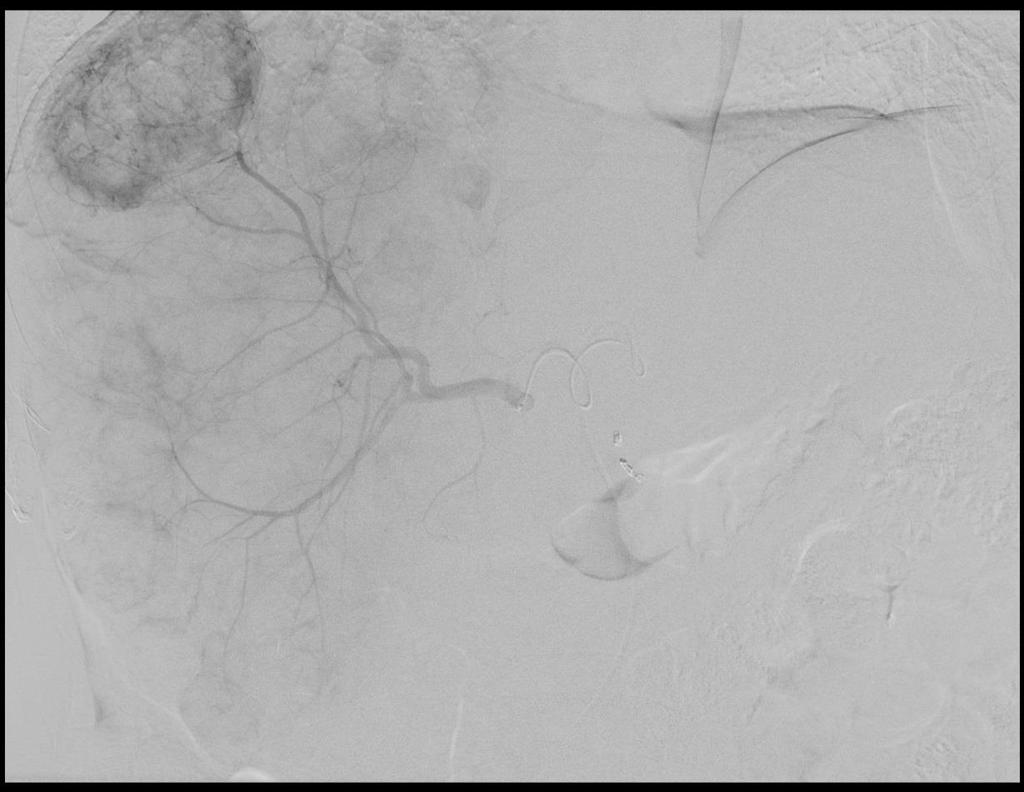
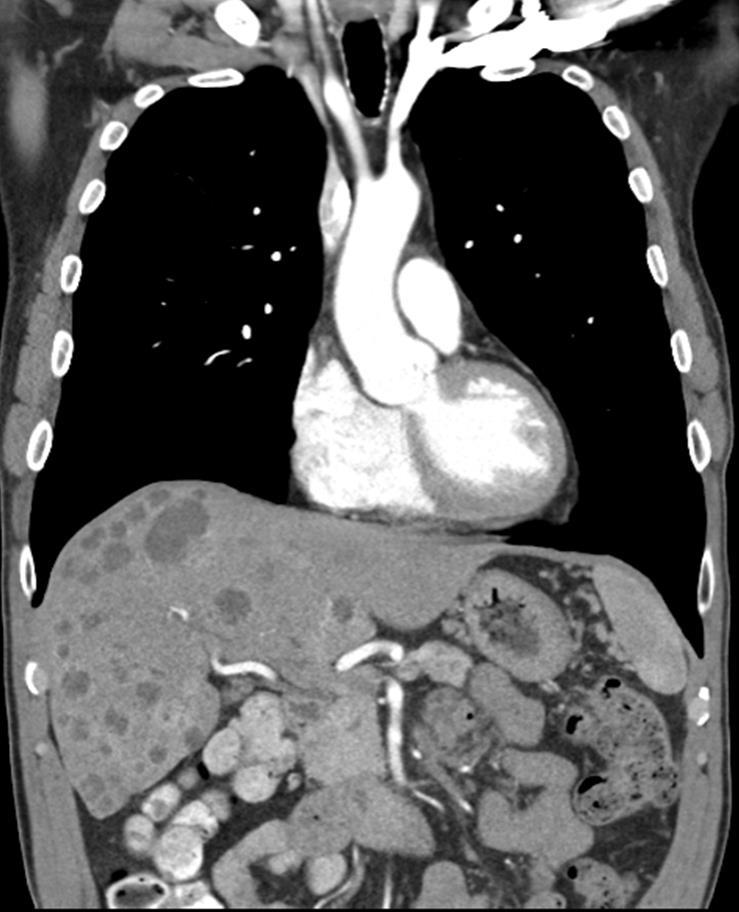
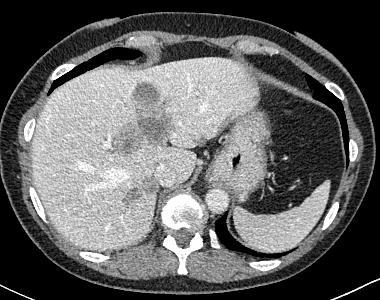
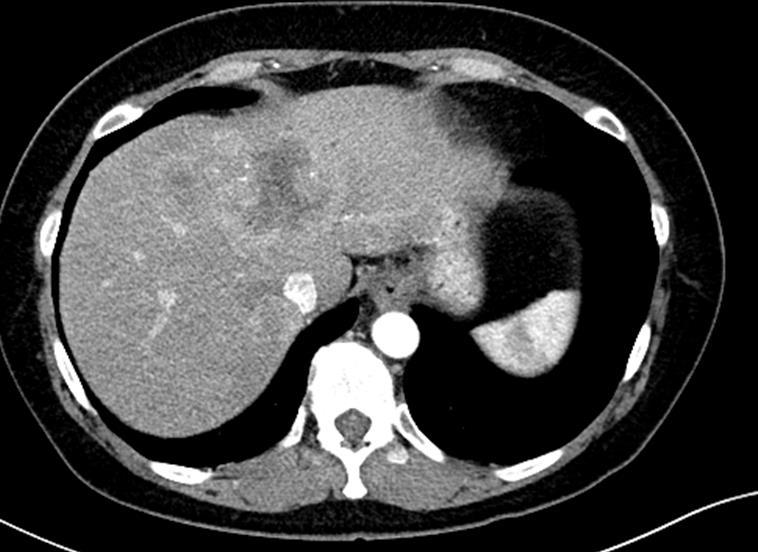
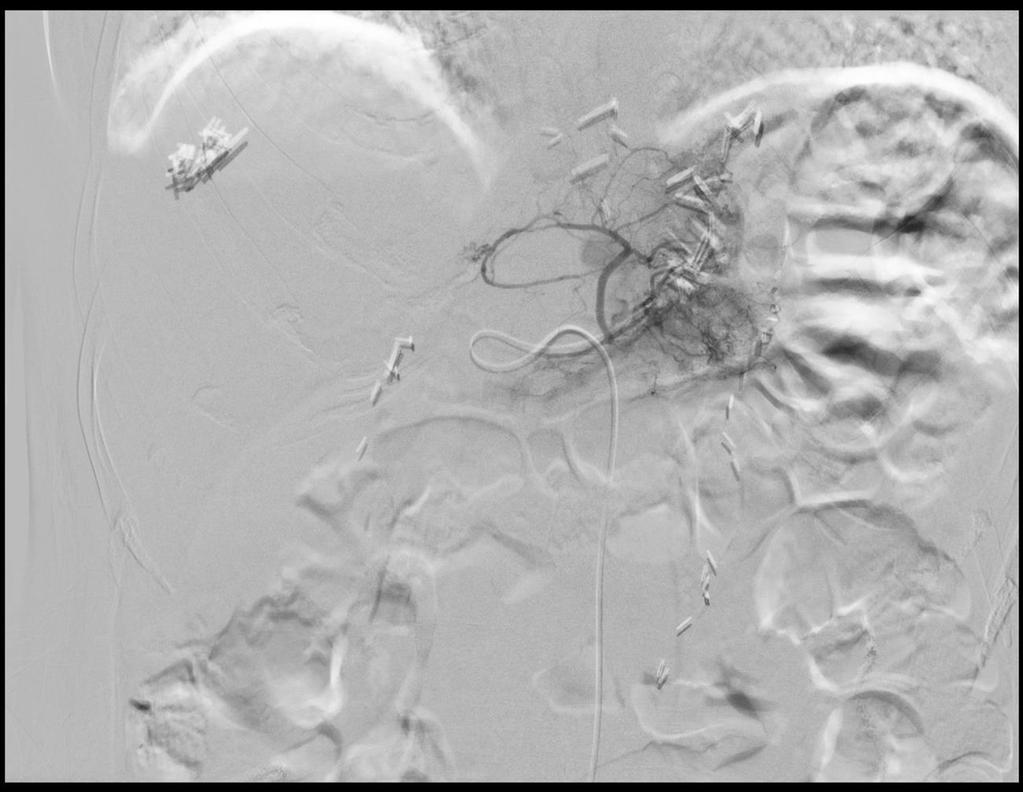
33 Case 1 58 yo M with non-resected pnet with progression of liver mets ECOG 0 Bilirubin.9 Alb 3.9

34

35

36
37
38

39
40
41

42

43

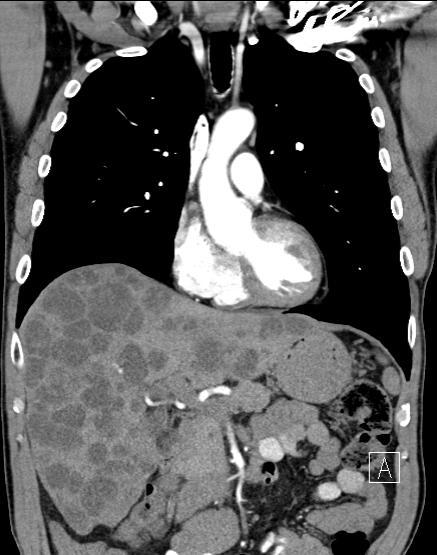
44 7 M Baseline 7 months later


45
46
47
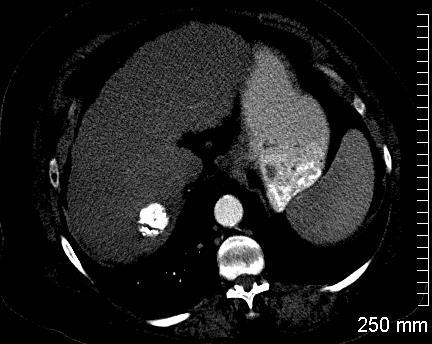
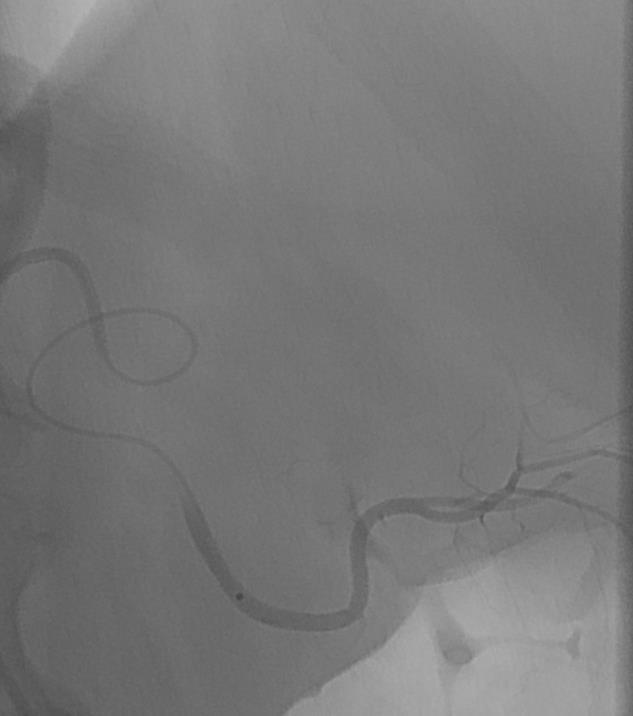
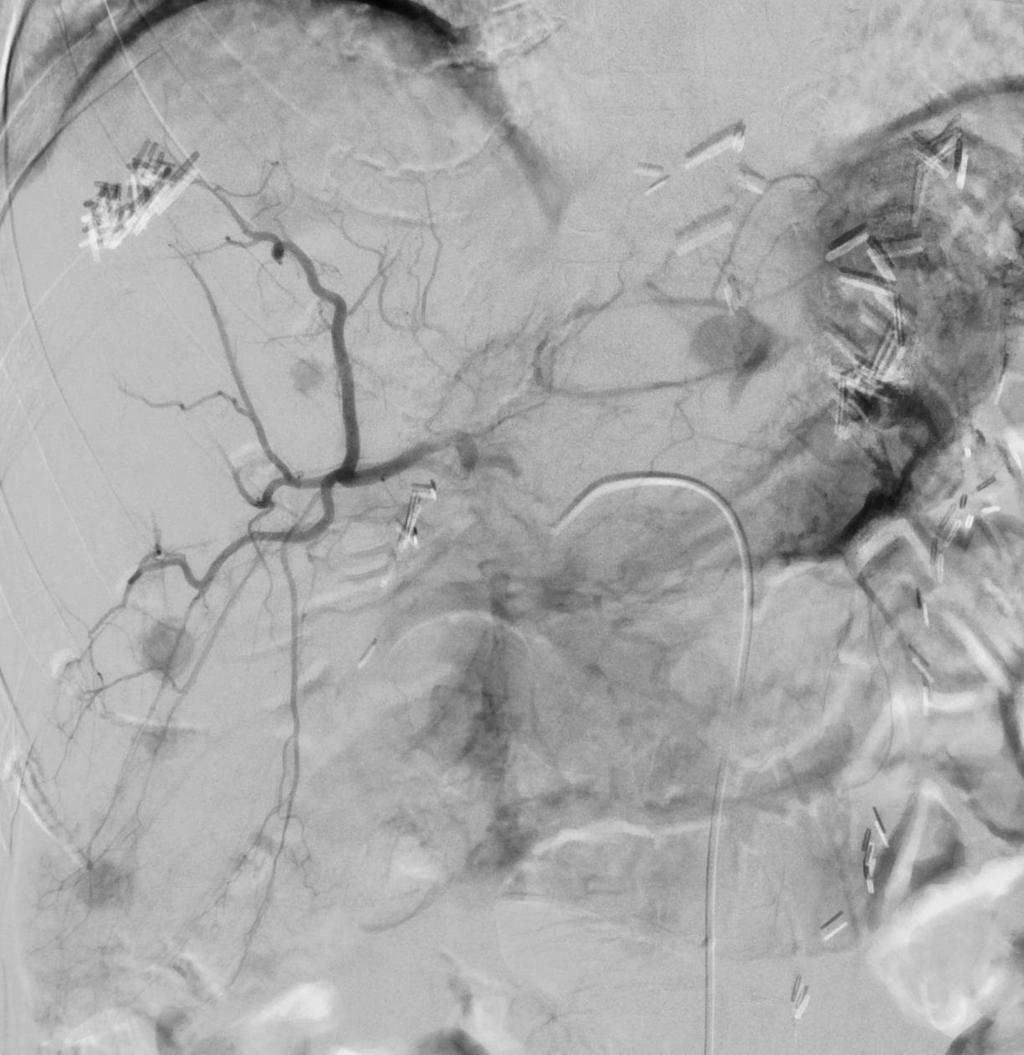
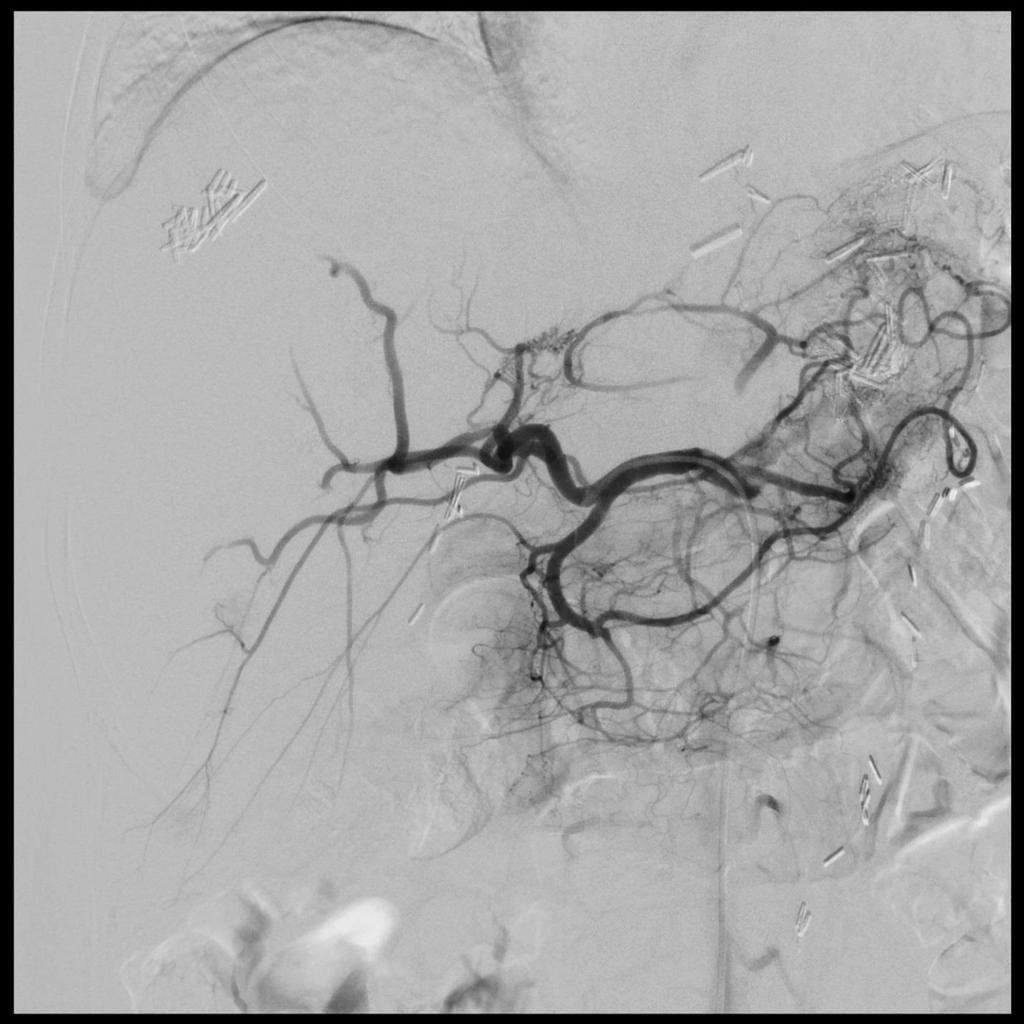
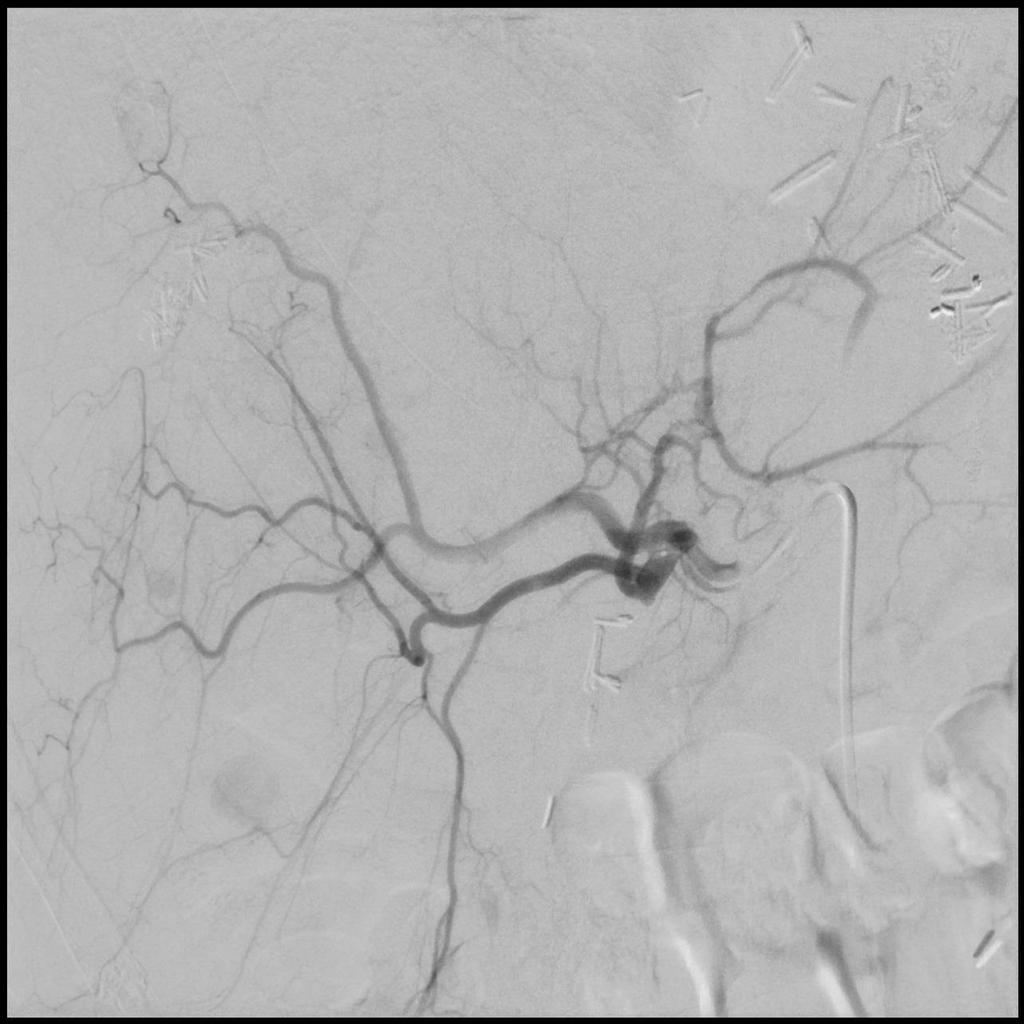
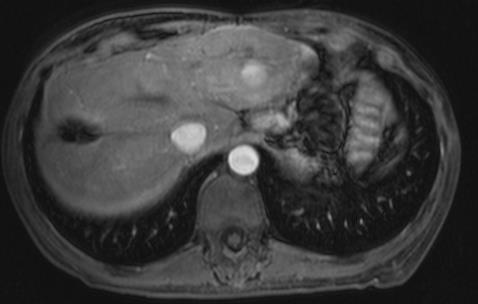
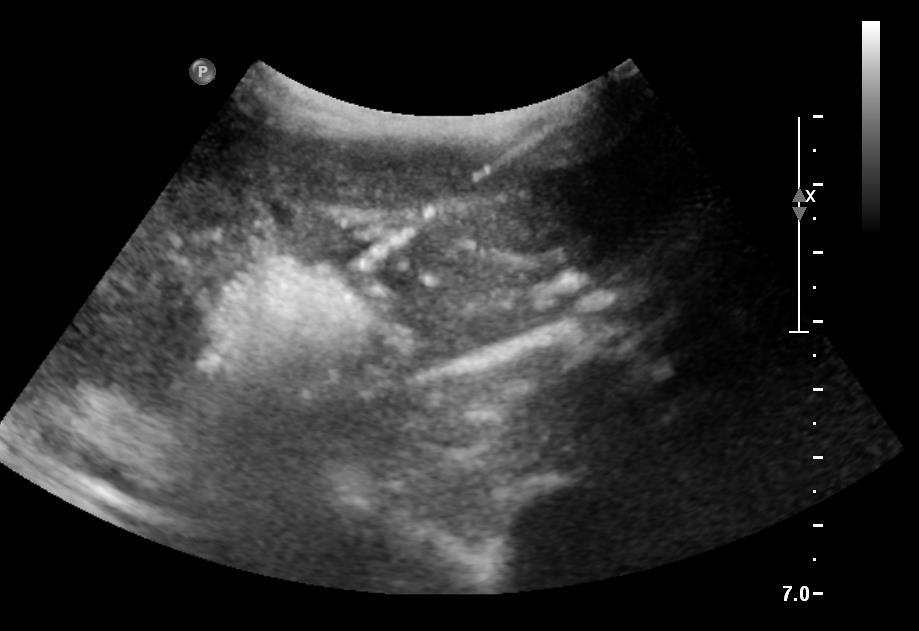
48 Case 2 50 F with resected pnet and history of prior gastric surgery. Progression of liver mets 7 months post operatively. ECOG 0 Normal liver function No hormonal symptoms

49
50
51

52
53
54 1) TAE ANTERIOR RIGHT LOBE 2) TAE POSTERIOR RIGHT LOBE 3) ABLATION SINGLE LESION LEFT LOBE
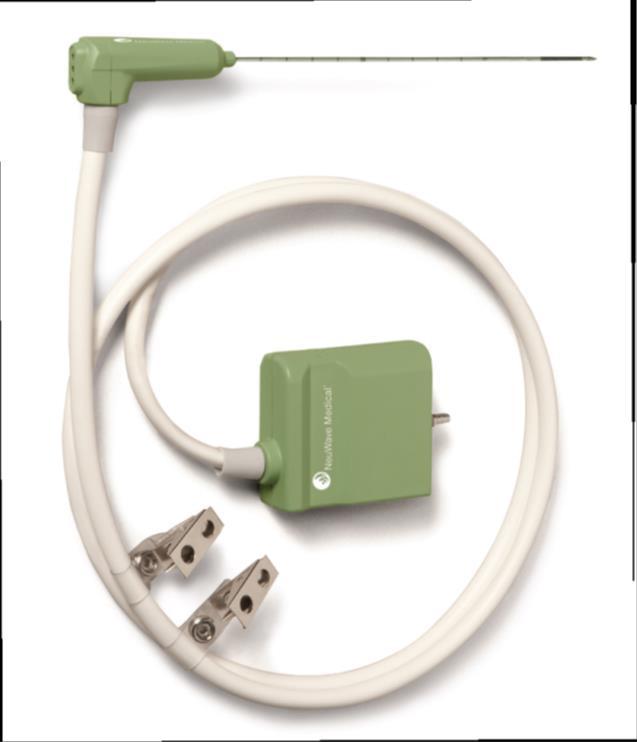
55 Ablation therapy PEI-percutaneous ethanol injection RFA-radiofrequency ablation frictional heating resulting from RF current Microwave- excitation of water molecules IRE Irreversible electroporation - non thermal ablation with electric current (some promise in the pancreas)
56 Microwave Electromagnetic radiation More efficient energy deposition Desiccation and charring not limiting Faster heating, higher temperatures, larger ablation volumes, shorter ablation times Less susceptibility to heat sink Maybe safer around bile ducts Easier to use no grounding pads, easier to run machine

57
58

59
60 Ablation Laparoscopic, at time of surgery vs. percutaneous 1 lesion < 5 cm or up to 3 lesions <3 cm (8cm total) Location-liver, lung, bone
61 Contraindications Close to structures of hilum- bile ducts Close to large vessels Close to the gut Subcapsular
62 Ablation complications General anesthesia Overnight admission for pain control Morbidity 7 %; mortality < 1% Bleeding requiring transfusion 1% Liver abscess 1% Higher risk if biliary enteric anastomosis Tract seeding 1-3% Gervais. JVIR 2009;20.
63 Trans-arterial complications Sedation complications Arteriography complications Contrast induced renal failure transient Vascular access injury Access hematoma Prolonged PES and severe dehydration Transient hyperbilirubinemia Liver fibrosis
64 Post embolization syndrome (PES) 2 week course of pain, nausea, low grade fever, fatigue, leukocytosis Control Hydration Anti-emetics Pain medication Narcotics Anti-inflammatories Steroids
65 Unusual complications Alopecia Acute carcinoid crisis Renal failure - permanent Contrast induced renal failure Tumor necrosis Dehydration Liver abscess Infection rare unless biliary tree compromised Radiation induced liver disease (RILD)
66 What therapy when? Differences in these therapy have not been evaluated head to head Response rates felt to be about 50% for all intraarterial therapies Approved therapies Newer beads are FDA approved for hyper vascular lesions TARE approved for primary liver cancers and CRC metastasis Perhaps chemo does not add much particularly for carcinoid tumors Perhaps more biliary complications after DEB bead use Perhaps easier PES course after Y90
67 What therapy when? Anatomy is critical to decision making Pre-operative high-quality, 3 phase CT liver imaging important for best decisions Because of the indolent nature of NET all therapies have a role Due to less post embolization syndrome following Y90 I choose this therapy to start in patients with Large disease burden But Cumulative radiation exposure limits repetition TAE over TACE to avoid exposure to drug therapy that may not provide additional benefit unless single lesion is being targeted where cumulative injury may be beneficial When limited disease ablation may be the most efficient
Locoregional Treatments for HCC Applications in Transplant Candidates. Locoregional Treatments for HCC Applications in Transplant Candidates
 Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Locoregional Therapy for Hepatoma
 Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Liver Directed Therapy for Hepatocellular Carcinoma
 Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer
Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer
Hepatocellular Carcinoma: A major global health problem. David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center
 Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Ruolo della interventistica per le secondarietà epatiche e di altre sedi
 Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Interventional Radiology in Liver Cancer. Nakarin Inmutto MD
 Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Hepatic metastases of neuroendocrine tumors: treatment options and outcomes of local patients treated with radioembolization
 Hepatic metastases of neuroendocrine tumors: treatment options and outcomes of local patients treated with radioembolization JP King PGY2 May 22, 2015 Neuroendocrine Tumor (NET) WHO Classification Location
Hepatic metastases of neuroendocrine tumors: treatment options and outcomes of local patients treated with radioembolization JP King PGY2 May 22, 2015 Neuroendocrine Tumor (NET) WHO Classification Location
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Management of Colorectal Liver Metastases
 Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD
 UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Embolotherapy for Cholangiocarcinoma: 2016 Update
 Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
COMPARING Y90 DEVICES
 COMPARING Y90 DEVICES William S Rilling MD, FSIR Professor of Radiology and Surgery Director, Vascular and Interventional Radiology Medical College of Wisconsin DISCLOSURES Research support : Siemens,
COMPARING Y90 DEVICES William S Rilling MD, FSIR Professor of Radiology and Surgery Director, Vascular and Interventional Radiology Medical College of Wisconsin DISCLOSURES Research support : Siemens,
treatment options for primary liver malignancies and metastatic disease
 State of the art treatment options for primary liver malignancies and metastatic disease Peter Huppert Prof. of Radiology and Neuroradiology Klinikum Darmstadt Certified Vascular and Oncologic Center Disclosure
State of the art treatment options for primary liver malignancies and metastatic disease Peter Huppert Prof. of Radiology and Neuroradiology Klinikum Darmstadt Certified Vascular and Oncologic Center Disclosure
LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE METASTASES
 LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE COLORECTAL CANCER LIVER METASTASES Jaime R. Merchan, MD, MMSc Associate Professor of Medicine Division of Hematology-Oncology University of Miami
LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE COLORECTAL CANCER LIVER METASTASES Jaime R. Merchan, MD, MMSc Associate Professor of Medicine Division of Hematology-Oncology University of Miami
HCC Imaging and Advances in Locoregional Therapy. David S. Kirsch MD Ochsner Clinic Foundation
 HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC?
 WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Corporate Medical Policy
 Corporate Medical Policy Cryosurgical Ablation of Primary or Metastatic Liver Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: cryosurgical_ablation_of_primary_or_metastatic_liver_tumors
Corporate Medical Policy Cryosurgical Ablation of Primary or Metastatic Liver Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: cryosurgical_ablation_of_primary_or_metastatic_liver_tumors
Current Treatment of Colorectal Metastases. Dr. Thavanathan Surgical Grand Rounds February 1, 2005
 Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page
 Vol.69(1), Page") The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
SIRT in the Management of Metastatic Neuroendocrine Tumors
 SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases
 Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases Thomas J. Vogl, B. Panahi, N. Nour-Eldin I D I R: Institute of Diagnostic and Interventional Radiology Goethe University Frankfurt,
Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases Thomas J. Vogl, B. Panahi, N. Nour-Eldin I D I R: Institute of Diagnostic and Interventional Radiology Goethe University Frankfurt,
Liver Tumors. Patient Education. Treatment options 8 4A. About the Liver. Surgical Specialties
 Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
Guidelines for SIRT in HCC An Evolution
 Guidelines for SIRT in HCC An Evolution 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore The challenge of HCC Surgery is potentially curative in early
Guidelines for SIRT in HCC An Evolution 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore The challenge of HCC Surgery is potentially curative in early
Intra-arterial Therapy in Management of HCC: ctace, DEB-TACE, and Y90 Radioembolization
 Intra-arterial Therapy in Management of HCC: ctace, DEB-TACE, and Y90 Radioembolization Department of Radiology, National Cancer Center In Joon Lee Contents Conventional TACE Role of TACE in management
Intra-arterial Therapy in Management of HCC: ctace, DEB-TACE, and Y90 Radioembolization Department of Radiology, National Cancer Center In Joon Lee Contents Conventional TACE Role of TACE in management
New Energy Sources for Local Ablation Therapy. Jeong Kyong Lee, MD Ewha Womans University
 New Energy Sources for Local Ablation Therapy Jeong Kyong Lee, MD Ewha Womans University New Energy Sources for Local Ablation Therapy Microwave Ablation Irreversible Electroporation Cryoablation Microwave
New Energy Sources for Local Ablation Therapy Jeong Kyong Lee, MD Ewha Womans University New Energy Sources for Local Ablation Therapy Microwave Ablation Irreversible Electroporation Cryoablation Microwave
INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES. Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí
 INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí STRATEGIES FOR CRLM LIVER METASTASES Extended indications Resectable
INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí STRATEGIES FOR CRLM LIVER METASTASES Extended indications Resectable
100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days
 94% of radiation delivered within 11 days") 100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days TheraSphere [US package insert]. Surrey, UK: Biocompatibles UK Ltd,
100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days TheraSphere [US package insert]. Surrey, UK: Biocompatibles UK Ltd,
SIRT Dosimetry: Sometimes Less Is More
 SIRT Dosimetry: Sometimes Less Is More Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director, Radiation Oncology,
SIRT Dosimetry: Sometimes Less Is More Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director, Radiation Oncology,
SELECTIVE INTERNAL RADIATION THERAPY FOR TREATMENT OF LIVER CANCER
 SELECTIVE INTERNAL RADIATION THERAPY FOR TREATMENT OF LIVER CANCER SIR-Spheres*: A New Treatment Option for Non-Resectable Liver Tumors Treatment Overview SIRT: Selective Internal Radiation Therapy Concept
SELECTIVE INTERNAL RADIATION THERAPY FOR TREATMENT OF LIVER CANCER SIR-Spheres*: A New Treatment Option for Non-Resectable Liver Tumors Treatment Overview SIRT: Selective Internal Radiation Therapy Concept
State-of-the-art minimally invasive interventions for liver tumors
 William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD State-of-the-art minimally invasive interventions for liver tumors William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD
William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD State-of-the-art minimally invasive interventions for liver tumors William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD
Hepatocellular Carcinoma. Markus Heim Basel
 Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Treatment of Hepatocellular Carcinoma. Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center
 Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
SIRT in Neuroendocrine Tumors
 SIRT in Neuroendocrine Tumors Marnix G.E.H. Lam, MD PhD Professor of Nuclear Medicine AVL Amsterdam UMC Utrecht ENETS Center of Excellence, The Netherlands Disclosure of speaker s interests Consultant
SIRT in Neuroendocrine Tumors Marnix G.E.H. Lam, MD PhD Professor of Nuclear Medicine AVL Amsterdam UMC Utrecht ENETS Center of Excellence, The Netherlands Disclosure of speaker s interests Consultant
8/1/2017. Disclosures. Outline. SAM Imaging Education Course 90Y-Microsphere Therapy: Emerging Trends and Future Directions
 SAM Imaging Education Course Y-Microsphere Therapy: Emerging Trends and Future Directions Matt Vanderhoek, PhD Henry Ford Health System, Detroit, MI Vanessa Gates, MS Northwestern University, Chicago,
SAM Imaging Education Course Y-Microsphere Therapy: Emerging Trends and Future Directions Matt Vanderhoek, PhD Henry Ford Health System, Detroit, MI Vanessa Gates, MS Northwestern University, Chicago,
EASL-EORTC Guidelines
 Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Surveillance for Hepatocellular Carcinoma
 Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Radiofrequency Ablation of Liver Tumors
 Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC
 Dr Apoorva Gogna MBBS FRCR FAMS Consultant Interventional Radiology Center Department of Diagnostic Radiology SingaporeGeneral Hospital MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC CASE HISTORY
Dr Apoorva Gogna MBBS FRCR FAMS Consultant Interventional Radiology Center Department of Diagnostic Radiology SingaporeGeneral Hospital MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC CASE HISTORY
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
NAACCR Webinar Series 1
 Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Update on the Management of Neuroendocrine Hepatic Metastases
 Review Articles Update on the Management of Neuroendocrine Hepatic Metastases David C. Madoff, MD, Sanjay Gupta, MD, Kamran Ahrar, MD, Ravi Murthy, MD, and James C. Yao, MD Neuroendocrine tumors (NETs)
Review Articles Update on the Management of Neuroendocrine Hepatic Metastases David C. Madoff, MD, Sanjay Gupta, MD, Kamran Ahrar, MD, Ravi Murthy, MD, and James C. Yao, MD Neuroendocrine tumors (NETs)
Transarterial Chemoembolisation (TACE) with Drug-Eluting Beads
 with Drug-Eluting Beads") Transarterial Chemoembolisation (TACE) with Drug-Eluting Beads A minimally invasive treatment for liver cancer Provided as an educational service by Biocompatibles UK Ltd, a BTG International group company
Transarterial Chemoembolisation (TACE) with Drug-Eluting Beads A minimally invasive treatment for liver cancer Provided as an educational service by Biocompatibles UK Ltd, a BTG International group company
Tips and tricks. Camillo Aliberti, Massimo Tilli
 Tips and tricks Camillo Aliberti, Massimo Tilli Unit of Oncological Diagnostic and Interventional Radiology, Delta Hospital AUSL Ferrara, Ferrara Italy camy.ali@libero.it mtilli72@libero.it Intra-arterial
Tips and tricks Camillo Aliberti, Massimo Tilli Unit of Oncological Diagnostic and Interventional Radiology, Delta Hospital AUSL Ferrara, Ferrara Italy camy.ali@libero.it mtilli72@libero.it Intra-arterial
Management of Liver Metastasis from Colorectal Carcinoma. Aisha White, M.D. SUNY Downstate Division of Transplantation
 Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Transarterial Chemoembolization in Neuroendocrine Liver Metastasis
 Transarterial Chemoembolization in Neuroendocrine Liver Metastasis Ricardo D. Garcia-Monaco, MD, PhD, FSIR; Andres Alejandro Kohan, MD From Vascular and Interventional Radiology, Department of Radiology,
Transarterial Chemoembolization in Neuroendocrine Liver Metastasis Ricardo D. Garcia-Monaco, MD, PhD, FSIR; Andres Alejandro Kohan, MD From Vascular and Interventional Radiology, Department of Radiology,
Prior Authorization Review Panel MCO Policy Submission
 Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Radioembolization of the Liver. Michael Meuse, M.D. Vascular and Interventional Radiology
 Radioembolization of the Liver Michael Meuse, M.D. Vascular and Interventional Radiology Brachytherapy Principle Radiation is accepted as a standard treatment option for liver cancer Radiation will break
Radioembolization of the Liver Michael Meuse, M.D. Vascular and Interventional Radiology Brachytherapy Principle Radiation is accepted as a standard treatment option for liver cancer Radiation will break
Molecular Imaging Guided Therapy: The Perfect Storm. David M Schuster, MD Emory University Department of Radiology Atlanta, GA
 Molecular Imaging Guided Therapy: The Perfect Storm David M Schuster, MD Emory University Department of Radiology Atlanta, GA Talk can be found at radiology.emory.edu Let s start with a case 74 year
Molecular Imaging Guided Therapy: The Perfect Storm David M Schuster, MD Emory University Department of Radiology Atlanta, GA Talk can be found at radiology.emory.edu Let s start with a case 74 year
HCC RADIOLOGIC DIAGNOSIS
 UCSF Transplant 2010 THE BEFORE AND AFTER HEPATOCELLULAR CARCINOMA MANAGEMENT Francis Yao, M.D. Professor of Clinical Medicine and Surgery Medical Director, Liver Transplantation University of California,
UCSF Transplant 2010 THE BEFORE AND AFTER HEPATOCELLULAR CARCINOMA MANAGEMENT Francis Yao, M.D. Professor of Clinical Medicine and Surgery Medical Director, Liver Transplantation University of California,
Liver 6/5/14. Collecting Cancer Data: Liver NAACCR Webinar Series. June 5, 2014
 Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Liver Cancer: Diagnosis and Treatment Options
 Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
MEDICAL MANAGEMENT OF METASTATIC GEP-NET
 MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
A) PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS
 PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines
 Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS
 UnitedHealthcare Oxford Clinical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: CANCER 036.11 T2 Effective Date: May 1, 2018 Table of Contents Page INSTRUCTIONS
UnitedHealthcare Oxford Clinical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: CANCER 036.11 T2 Effective Date: May 1, 2018 Table of Contents Page INSTRUCTIONS
The Role of Interventional Radiology in Cancer and Palliative Care. David T. Wang, D.O.
 The Role of Interventional Radiology in Cancer and Palliative Care David T. Wang, D.O. Disclosures None Objectives Give an overview of the role Interventional Radiology can play in Cancer and Palliative
The Role of Interventional Radiology in Cancer and Palliative Care David T. Wang, D.O. Disclosures None Objectives Give an overview of the role Interventional Radiology can play in Cancer and Palliative
Radioembolization for Primary and Metastatic Tumors of the Liver
 Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2018 Origination: 8/2006 Next Review: 8/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue
Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2018 Origination: 8/2006 Next Review: 8/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue
Paul Martin MD FACG. University of Miami
 Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Disclosures. Fees for Non CME/CE services received. agents: Bayer Healthcare. CT guided HDR Brachytherapy in Oligometastases
 CT guided HDR Brachytherapy in Oligometastases Jens Ricke Radiology and Nuclear medicine University of Magdeburg Disclosures Fees for Non CME/CE services received directlyfrom a commercial interest or
CT guided HDR Brachytherapy in Oligometastases Jens Ricke Radiology and Nuclear medicine University of Magdeburg Disclosures Fees for Non CME/CE services received directlyfrom a commercial interest or
HEPATIC METASTASES. We can state 3 types of metastases depending on their treatment options:
 HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS
 UnitedHealthcare Commercial Medical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: 2018T0445O Effective Date: February 1, 2018 Table of Contents Page INSTRUCTIONS
UnitedHealthcare Commercial Medical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: 2018T0445O Effective Date: February 1, 2018 Table of Contents Page INSTRUCTIONS
Hepatocellular carcinoma: Intra-arterial treatments
 Hepatocellular carcinoma: Intra-arterial treatments Irene Bargellini U.O. Radiologia Interventistica Azienda Ospedaliero Universitaria Pisana IRENE BARGELLINI,MD UO RADIOLOGIA INTERVENTISTICA, AZIENDA
Hepatocellular carcinoma: Intra-arterial treatments Irene Bargellini U.O. Radiologia Interventistica Azienda Ospedaliero Universitaria Pisana IRENE BARGELLINI,MD UO RADIOLOGIA INTERVENTISTICA, AZIENDA
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of selective internal radiation therapy for primary liver cancer Selective internal
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of selective internal radiation therapy for primary liver cancer Selective internal
Surgical Metabolism Section, Surgery Branch, NCI, Bethesda, MD Division of Surgical Oncology, University of Maryland, Baltimore, MD
 High Dose Intra-Arterial Melphalan Delivered via Percutaneous Hepatic Perfusion (PHP) for Patients with Unresectable Hepatic Metastases from Primary Neuroendocrine Tumors. James F. Pingpank, Richard E.
High Dose Intra-Arterial Melphalan Delivered via Percutaneous Hepatic Perfusion (PHP) for Patients with Unresectable Hepatic Metastases from Primary Neuroendocrine Tumors. James F. Pingpank, Richard E.
RFA of Tumors of the Lung: How and Why. Radiofrequency Ablation. Radiofrequency Ablation. RFA of pulmonary metastases. Radiofrequency Ablation of Lung
 RFA of Tumors of the Lung: How and Why Radiofrequency Ablation of Lung Ernest Scalzetti MD SUNY Upstate Medical University Syracuse NY FDA WARNING: Off-label use of a medical device Radiofrequency Ablation
RFA of Tumors of the Lung: How and Why Radiofrequency Ablation of Lung Ernest Scalzetti MD SUNY Upstate Medical University Syracuse NY FDA WARNING: Off-label use of a medical device Radiofrequency Ablation
RF Ablation: indication, technique and imaging follow-up
 RF Ablation: indication, technique and imaging follow-up Trongtum Tongdee, M.D. Radiology Department, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand Objective Basic knowledge
RF Ablation: indication, technique and imaging follow-up Trongtum Tongdee, M.D. Radiology Department, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand Objective Basic knowledge
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
Hepatobiliary Malignancies Retrospective Study at Truman Medical Center
 Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Percutaneous Ultrasound-guided Radiofrequency Ablation of Colorectal Liver Metastases
 Chin J Radiol 2005; 30: 153-158 153 Percutaneous Ultrasound-guided Radiofrequency Ablation of Colorectal Liver Metastases YI-YOU CHIOU YI-HONG CHOU JEN-HUEY CHIANG HSIN-KAI WANG CHENG-YEN CHANG Department
Chin J Radiol 2005; 30: 153-158 153 Percutaneous Ultrasound-guided Radiofrequency Ablation of Colorectal Liver Metastases YI-YOU CHIOU YI-HONG CHOU JEN-HUEY CHIANG HSIN-KAI WANG CHENG-YEN CHANG Department
Radioembolization for Primary and Metastatic Tumors of the Liver
 Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2017 Origination: 8/2006 Next Review: 8/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue
Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2017 Origination: 8/2006 Next Review: 8/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue
RADIATION SEGMENTECTOMY. Robert J Lewandowski, MD
 RADIATION SEGMENTECTOMY Robert J Lewandowski, MD Robert Lewandowski, M.D. Consultant/Advisory Board: Cook Medical, LLC, Arsenal, BTG International, Boston Scientific Corp., ABK Reference Unlabeled/Unapproved
RADIATION SEGMENTECTOMY Robert J Lewandowski, MD Robert Lewandowski, M.D. Consultant/Advisory Board: Cook Medical, LLC, Arsenal, BTG International, Boston Scientific Corp., ABK Reference Unlabeled/Unapproved
Trans-arterial radioembolisation (TARE) of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis?
 of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis?") Trans-arterial radioembolisation (TARE) of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis? Poster No.: C-1634 Congress: ECR 2014 Type: Authors: Keywords: DOI:
Trans-arterial radioembolisation (TARE) of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis? Poster No.: C-1634 Congress: ECR 2014 Type: Authors: Keywords: DOI:
The Role of Interventional Radiology (Locoregional
 The Role of Interventional Radiology (Locoregional therapies) in HCC Richard Owen MB, MRCP, FRCR Interventional Radiology, Associate Professor University of Alberta Aldo Montana-Loza MD, FRCPC Hepatology
The Role of Interventional Radiology (Locoregional therapies) in HCC Richard Owen MB, MRCP, FRCR Interventional Radiology, Associate Professor University of Alberta Aldo Montana-Loza MD, FRCPC Hepatology
Unmet needs in intermediate HCC. Korea University Guro Hospital Ji Hoon Kim
 Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Interventional Radiologic Treatment of Hepatocellular Carcinoma
 Interventional Radiologic Treatment of Hepatocellular Carcinoma Fatih Boyvat Abstract The current treatment modalities for patients with hepatocellular carcinoma are discussed in this review. Hepatocellular
Interventional Radiologic Treatment of Hepatocellular Carcinoma Fatih Boyvat Abstract The current treatment modalities for patients with hepatocellular carcinoma are discussed in this review. Hepatocellular
Description. Section: Therapy Effective Date: July 15, 2014 Subsection: Therapy Original Policy Date: June 7, 2012 Subject: Page: 1 of 23
 Last Review Status/Date: June 2014 Page: 1 of 23 Description Radioembolization (RE), referred to as selective internal radiation therapy or SIRT in older literature, is the intra-arterial delivery of small
Last Review Status/Date: June 2014 Page: 1 of 23 Description Radioembolization (RE), referred to as selective internal radiation therapy or SIRT in older literature, is the intra-arterial delivery of small
Disclosures. I am on the Onyx speaker bureau I am a paid consultant to. Boston Scientific CeloNova Cook MDS Nordion Sirtex
 Disclosures I am on the Onyx speaker bureau I am a paid consultant to Boston Scientific CeloNova Cook MDS Nordion Sirtex Comparing Y90 Devices Matthew S. Johnson MD, FSIR Indiana University School of Medicine
Disclosures I am on the Onyx speaker bureau I am a paid consultant to Boston Scientific CeloNova Cook MDS Nordion Sirtex Comparing Y90 Devices Matthew S. Johnson MD, FSIR Indiana University School of Medicine
Index. C Cancer, Carcinoid syndrome, 413. D DCIS. See Ductal carcinoma in situ (DCIS) DEB-TACE. See Drug eluting beads-tace (DEB-TACE)
 DEB-TACE. See Drug eluting beads-tace (DEB-TACE)") Index A Ablation, 179 199, 843 853 devices, 179, 199 liver tumors, 527 techniques, 516 Ablative radiation therapy, 456 Accelerated partial breast, 894, 896 898 Adaptive radiation therapy, 586, 598, 602
Index A Ablation, 179 199, 843 853 devices, 179, 199 liver tumors, 527 techniques, 516 Ablative radiation therapy, 456 Accelerated partial breast, 894, 896 898 Adaptive radiation therapy, 586, 598, 602
Disclosure. Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report:
 Disclosure Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report: Consulting Employment in industry Stockholder of a healthcare company Owner of a healthcare company
Disclosure Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report: Consulting Employment in industry Stockholder of a healthcare company Owner of a healthcare company
Use of Irreversible Electroporation in Unresectable Pancreatic Cancer. Robert C. G. Martin, II, MD, PhD, FACS
 Use of Irreversible Electroporation in Unresectable Pancreatic Cancer Robert C. G. Martin, II, MD, PhD, FACS University of Louisville Division of Surgical Oncology, James Graham Brown Cancer Center, Department
Use of Irreversible Electroporation in Unresectable Pancreatic Cancer Robert C. G. Martin, II, MD, PhD, FACS University of Louisville Division of Surgical Oncology, James Graham Brown Cancer Center, Department
SIRT for Intermediate and Advanced HCC
 Pamplona, junio de 2008 SIRT for Intermediate and Advanced HCC Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain 90 Y-RE MRI SPECT FUSION 90 Y-RE = Yttrium-90 radioembolization Sangro
Pamplona, junio de 2008 SIRT for Intermediate and Advanced HCC Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain 90 Y-RE MRI SPECT FUSION 90 Y-RE = Yttrium-90 radioembolization Sangro
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
December 12 th 2017 CM) INTERVENTIONAL ONCOLOGY 09:00 REGISTRATION
 INTERVENTIONAL ONCOLOGY 09:00 REGISTRATION") December 12 th 2017 09:00 REGISTRATION 09:30 10:30 LYMPHONODES AND ADRENAL METASTASES Lymphonodes metastases clinical assessment Lymphonodes metastases imaging assessment and percutaneous treatments Adrenal
December 12 th 2017 09:00 REGISTRATION 09:30 10:30 LYMPHONODES AND ADRENAL METASTASES Lymphonodes metastases clinical assessment Lymphonodes metastases imaging assessment and percutaneous treatments Adrenal
DC Bead Chemoembolisation for the Treatment of Primary [DEBDOX ] and Secondary [DEBIRI ] Liver Cancer Review of Published Clinical Data
![DC Bead Chemoembolisation for the Treatment of Primary [DEBDOX ] and Secondary [DEBIRI ] Liver Cancer Review of Published Clinical Data](/thumbs/78/77499894.jpg "DC Bead Chemoembolisation for the Treatment of Primary [DEBDOX ] and Secondary [DEBIRI ] Liver Cancer Review of Published Clinical Data") DC Bead Chemoembolisation for the Treatment of Primary [DEBDOX ] and Secondary [DEBIRI ] Liver Cancer Review of Published Clinical Data Professor Thomas J Vogl Goethe University Hospital Frankfurt-am-Main,
DC Bead Chemoembolisation for the Treatment of Primary [DEBDOX ] and Secondary [DEBIRI ] Liver Cancer Review of Published Clinical Data Professor Thomas J Vogl Goethe University Hospital Frankfurt-am-Main,
How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung
 How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung End points in research for solid cancers Overall survival (OS) The most ideal one, but requires long follow-up duration
How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung End points in research for solid cancers Overall survival (OS) The most ideal one, but requires long follow-up duration
1/13/2014 Ries et al (eds). At: 2
. At: 2") 1/13/2014 1 1/13/2014 Ries et al (eds). At: http://seer.cancer.gov/csr/1975_2002 2 1/13/2014 Coldwell et al, General Selection Criteria of Patients for Radioembolization of Liver Tumors AJCO 2010 3 1/13/2014
1/13/2014 1 1/13/2014 Ries et al (eds). At: http://seer.cancer.gov/csr/1975_2002 2 1/13/2014 Coldwell et al, General Selection Criteria of Patients for Radioembolization of Liver Tumors AJCO 2010 3 1/13/2014
Phase II Study of Chemoembolization with Drug-eluting Beads in Patients with Hepatic. Neuroendocrine Metastases: Interim Analysis
 Phase II Study of Chemoembolization with Drug-eluting Beads in Patients with Hepatic Neuroendocrine Metastases: Interim Analysis Original research Advances in knowledge: 1. The incidence of biloma and
Phase II Study of Chemoembolization with Drug-eluting Beads in Patients with Hepatic Neuroendocrine Metastases: Interim Analysis Original research Advances in knowledge: 1. The incidence of biloma and
Clinical Commissioning Policy Proposition:
 Clinical Commissioning Policy Proposition: Chemosaturation for liver metastases from ocular melanomas Reference: NHS England A02X05/01 Information Reader Box (IRB) to be inserted on inside front cover
Clinical Commissioning Policy Proposition: Chemosaturation for liver metastases from ocular melanomas Reference: NHS England A02X05/01 Information Reader Box (IRB) to be inserted on inside front cover
Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery
 Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation I: Patient ER 74 y/o male with A1A
Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation I: Patient ER 74 y/o male with A1A
NYU School of Medicine Department of Radiology Rotation-Specific House Staff Evaluation
 Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
EPIDEMIOLOGY. Long established risk factors for CCA: hepatobiliaryflukes, PSC, biliary tract cysts, epatolithiasis.
 EPIDEMIOLOGY Intrahepatic cholangiocarcinoma(icc) is the second most common (15%) primary liver cancer after hepatocellular carcinoma (HCC), with a rate of about 2.1/100,000 people per year in western
EPIDEMIOLOGY Intrahepatic cholangiocarcinoma(icc) is the second most common (15%) primary liver cancer after hepatocellular carcinoma (HCC), with a rate of about 2.1/100,000 people per year in western
Role of loco-regional treatment in the medical and surgical management strategy of metastatic colorectal cancer
 Role of loco-regional treatment in the medical and surgical management strategy of metastatic colorectal cancer M Ducreux, MD, PhD Gustave Roussy Villejuif, FRANCE M Ducreux is a consultant to Biocompatibles
Role of loco-regional treatment in the medical and surgical management strategy of metastatic colorectal cancer M Ducreux, MD, PhD Gustave Roussy Villejuif, FRANCE M Ducreux is a consultant to Biocompatibles
Radioembolization for Primary and Metastatic Tumors of the Liver
 Page: 1 of 28 Last Review Status/Date: September 2015 Description Radioembolization (RE), also referred to as selective internal radiotherapy (SIRT), is the intra-arterial delivery of small beads (microspheres)
Page: 1 of 28 Last Review Status/Date: September 2015 Description Radioembolization (RE), also referred to as selective internal radiotherapy (SIRT), is the intra-arterial delivery of small beads (microspheres)
PRIOR AUTHORIZATION Prior authorization is required for BlueCHiP for Medicare members and recommended for Commercial products.
 Medical Coverage Policy Radioembolization for Primary and Metastatic Tumors of the Liver EFFECTIVE DATE: 10 06 2009 POLICY LAST UPDATED: 08 02 2016 OVERVIEW Radioembolization (RE), referred to as selective
Medical Coverage Policy Radioembolization for Primary and Metastatic Tumors of the Liver EFFECTIVE DATE: 10 06 2009 POLICY LAST UPDATED: 08 02 2016 OVERVIEW Radioembolization (RE), referred to as selective
DEB-TACE vs Conventional TACE in Intermediate HCC: Best Candidates for DEB-TACE?
 DEB-TACE vs Conventional TACE in Intermediate HCC: Best Candidates for DEB-TACE? Ho Jong Chun, MD., PhD Seoul St. Mary s Hospital, The Catholic University of Korea Why Drug-eluting Beads? Clear Rationale
DEB-TACE vs Conventional TACE in Intermediate HCC: Best Candidates for DEB-TACE? Ho Jong Chun, MD., PhD Seoul St. Mary s Hospital, The Catholic University of Korea Why Drug-eluting Beads? Clear Rationale
Radioembolization (Y90)
") Scan for mobile link. Radioembolization (Y90) Radioembolization is a minimally invasive procedure that combines embolization and radiation therapy to treat liver cancer. Tiny glass or resin beads filled
Scan for mobile link. Radioembolization (Y90) Radioembolization is a minimally invasive procedure that combines embolization and radiation therapy to treat liver cancer. Tiny glass or resin beads filled