Management of Liver Metastasis from Colorectal Carcinoma. Aisha White, M.D. SUNY Downstate Division of Transplantation
|
|
|
- Denis Andrews
- 6 years ago
- Views:
Transcription
1 Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation
2

3

4

5

6

7

8
9
10 Management of Colorectal Liver Metastasis
11 Epidemiology 25% of patients diagnosed with colorectal carcinoma will have liver metastasis at presentation. Another 50% of patients will have recurrent disease develop within the liver. 85% of tumor recurrences are detected within 2.5 years after resection of the primary colorectal CA and the remaining 15% are detected within the next 2.5 years.
12 History The earliest hepatic procedures were performed almost exclusively for trauma The earliest resection for tumor was by Langenbuch in By the 1940s a more aggressive operative approach was being taken in the treatment of patients with colorectal carcinoma metastatic to the liver.
13 Scientific Basis for Resection of Colorectal Liver Metastasis Hematogenous metastases from primary colorectal cancer develop in a step-wise fashion. In most patients, the primary tumor disseminates to local lymph nodes, to the liver, or to peritoneal surfaces. This is considered a metachronous or step-wise progression of the malignant process. Only in a minority of patients is there synchronous spread of the malignancy from the primary site to systemic sites.
14 Natural History of Colorectal Liver Metastasis Death of colorectal cancer is often a result of liver metastasis. Surgical resection of distant metastasis can produce long-term survival and cure in some patients.
15 Natural History of Colorectal Liver Metastasis continued A retrospective study by Wilson et al. (Arch Surg 1976; 111: ) looking at the survival of patients with potentially resectable colorectal liver mets left untreated reported a 0% 5-year survival for patients untreated compared with a 28% 5-year survival for patients whose liver mets were resected.
16 Natural History of Colorectal Liver Metastasis continued A retrospective study by Wanebo et al. (Am J Surg 1978; 135: 81-85) found that patients with an untreated single liver metastasis had a median survival of 19 months, with no patient surviving 5 years, while patients with a resected single liver metastasis had a median survival of 36 months with 25% of patients surviving 5 years.
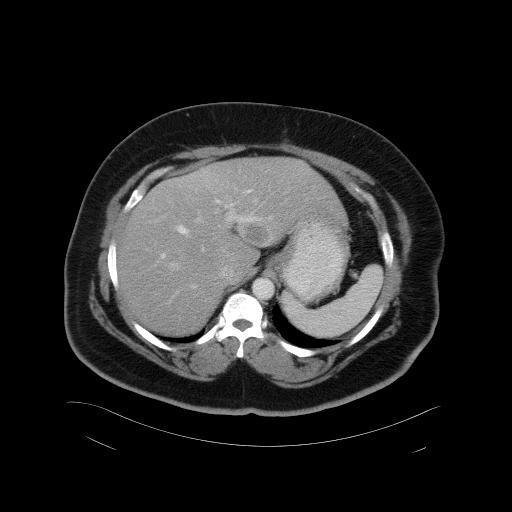
17 Diagnosis of Liver Metastasis The most common symptoms of hepatic metastatic disease are pain, ascites, jaundice, palpable mass, weight loss, anorexia, fever, and vague GI complaints. Many patients are diagnosed through routine radiologic studies or elevations in the CEA level, which prompt further investigation.
18 Prognostic Variables for Liver Metastasis Age >70 Primary tumor stage Primary tumor location (colon > rectum) Clinical presentation of metastasis (signs/symptoms, lab abnormalities) Synchronous metastasis Size of metastatic lesion(s) Extent of liver involvement
19 Prognostic Variables for Liver Metastasis continued Interval between primary diagnosis and appearance of metachronous metastasis (diagnostic interval 1 year) Multiple metastases Presence of satellite lesions Presence of extrahepatic disease
20 Pre-op Work-up for Candidates for Resection of Metastasis Detailed history and physical Labs including CBC and LFTs CXR CT or MRI of abdomen/pelvis Colonoscopy (if none within 6 months) PET scan
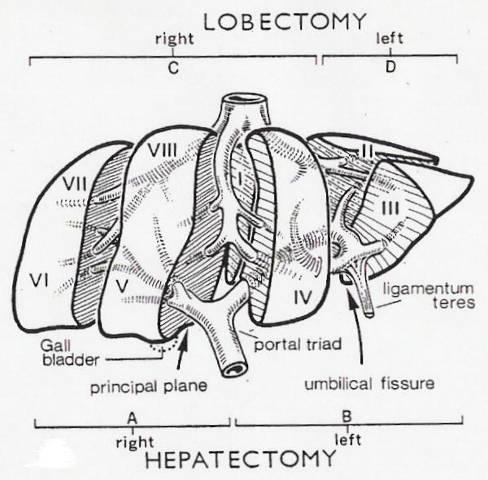
21 Liver Anatomy- Morphological The liver is divided by the umbilical fissure and falciform ligament into two lobes- the right lobe (which is larger) and the left lobe. The right lobe is comprised of two accessory lobes which are individualized by well-defined fissures.

22
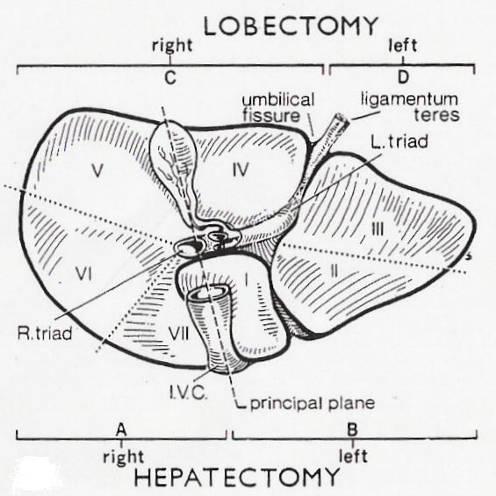
23 Liver Anatomy- Functional This description was initiated by Cantlie in It was later followed by the works of McIndoe & Counseller (1927), Hjörstjö (1931), Ton That Tung (1939), Goldsmith & Woodburne (1957), and Couinaud (1957). This description of hepatic segmentation is based upon the distribution of the portal pedicles and the location of the hepatic veins.
24
25
26
27 Hepatic Resections There are 3 types of hepatic resection: 1. Anatomic Resections a. R Hepatectomy b. L Hepatectomy c. R Lobectomy (R Trisegmentectomy) d. L Lobectomy (L Lateral Segmentectomy) e. Extended L Hepatectomy (L Trisegmentectomy) f. Transverse Hepatectomy
28 Hepatic Resections continued 2. Nonanatomic Resections 3. Enucleation Procedures

29
30 Contraindications to Major Resection for Metastases Total hepatic involvement Advanced cirrhosis Jaundice (except from extrinsic hepatic ductal obstruction) Vena Cava or main Portal Vein invasion Extrahepatic tumor involvement (except lung)
31 Complications of Surgery Operative Mortality ranges from 0-7% Hemorrhage Sepsis Liver Failure Morbidity ranges from 22-39% Hemorrhage (1-3%) Biliary leak or fistula (4%) Liver failure (3-8%)
32 Complications of Surgery continued Perihepatic abscess (2-10%) Pneumonia (5-22%) Symptomatic pleural effusion (5-10%) Pulmonary embolism (1%)
33 Prehepatectomy Predictors of Survival and Nonrecurrence
34 Tanaka et al World J Surg 2004; 28: Retrospective Study of 144 patients between who underwent potentially curative hepatic resection for colorectal liver metastases. The study looked at identifying factors that influence overall survival and recurrence in the remnant liver. The study sought to demonstrate that metastatic tumor doubling time is the most important prehepatectomy predictor of survival and nonrecurrence of hepatic colorectal metastasis.
35 Tanaka et al continued Univariate Analysis of Influence of Tumor-Related Variables on Survival After Hepatectomy Overall Survival (%) p value 3Y 5Y Concomitant extrahepatic disease present <0.01 absent Distribution unilobar <0.05 bilobar Size (mm) < < >
36 Tanaka et al continued Univariate Analysis of Influence of Tumor-Related Variables on Survival After Hepatectomy Overall Survival (%) p value 3Y 5Y Doubling time 45 days <0.05 >45 days p53 expression positive <0.05 negative
37 Tanaka et al continued Multivariate Analysis of Prognostic Factors Adjusted relative risk p value Maximum size (mm) Doubling time >45 days p53 expression negative
38 Tanaka et al continued Univariate Analysis of Risk Factors for Remnant Liver Recurrence Disease-Free Survival (%) p value 1Y 3Y 5Y Primary lesion site colon <0.01 rectum Lymph node mets present <0.05 absent Vascular permeation present <0.05 absent Liver metastases synchronous <0.05 metachronous
39 Tanaka et al continued Univariate Analysis of Risk Factors for Remnant Liver Recurrence Disease-Free Survival (%) p value 1Y 3Y 5Y Distribution unilobar <0.01 bilobar Vascular invasion present <0.05 absent Doubling time 45 days <0.05 >45 days p53 expression positive <0.05 negative
40 Tanaka et al continued Multivariate Analysis of Risk Factors for Remnant Liver Recurrence Adjusted relative risk p value Doubling time >45 days
41 Tanaka et al continued World J Surg 2004; 28: Conclusions Patients with doubling times >45 days had relatively few liver recurrences. Moreover, when there was a recurrence, the patient was a candidate for repeat hepatectomy. Prophylactic chemotherapy and highly sensitive follow-up testing might improve the prognosis for patients with a short doubling time.
42 Timing of Hepatectomy- Simultaneous vs. Delayed
43 Tanaka et al Surgery 2004; 136(3): Retrospective study of 39 consecutive patients with synchronous colorectal liver metastases who underwent curative simultaneous 1-stage hepatectomy and resection of colorectal primary. 91 patients with colorectal CA and synchronous liver mets were evaluated as candidates for simultaneous resection. Simultaneous resections were performed in patients with a relatively small number of liver neoplasms considered to be completely removed by a relatively simple hepatectomy procedure.
44 Tanaka et al continued Surgery 2004; 136(3): Liver resection was contraindicated at the time of primary operation in 50 patients for the following reasons: poor performance status (4), massive neoplasm (2), unfavorably located neoplasm (2), multicentricity (6), and multiple, bilobar metastases (36). Intraoperatively, the following criteria for simultaneous liver resection were applied: Primary colorectal neoplasm resectable with a negative margin Absence of uncontrollable extrahepatic disease Ability to resect all liver neoplasms with negative margins
45 Tanaka et al continued Surgery 2004; 136(3): Overall cumulative survival rates 1Y 3Y 5Y simultaneous resection 86% 68% 53% metachronous resection 83% 47% 47% Disease-free survival rates 1Y 3Y 5Y simultaneous resection 64% 20% 16% metachronous resection 51% 35% 28%
46 Tanaka et al continued Surgery 2004; 136(3): Variables influencing survival after simulataneous resection of colon & liver lesions (univariate analysis): histologic features of primary (well to mod diff) p<0.01 age (<70) p<0.05 No variables affected survival after metachronous resection
47 Tanaka et al continued Surgery 2004; 136(3): Potential disadvantages of synchronous resection: Intraoperative contamination of the cut liver surface may be more likely Postoperative anastomotic leakage may be favored by impairment of liver function Occult micrometastatic lesions may remain unresected, leading to higher recurrence rates
48 Tanaka et al continued Surgery 2004; 136(3): Conclusion- Simultaneous colorectal and hepatic resections are not recommended for the following: Patients who require resection of more than 1 hepatic section to remove liver metastases Patients 70 years of age or older Patients with poorly differentiated or mucinous adenocarcinoma as the primary lesion
49 Role of Rescue Surgery for Unresectable Liver Metastases
50 René et al. Ann Surg 2004; 240(4): Prospective study of 1439 patients with colorectal liver metastases managed between 1988 and (77%), initially unresectable, were treated by chemotherapy and 335 (23%), resectable, were treated by primary liver resection. Among 1104 unresectable patients, 138 good responders (12.5%) underwent secondary hepatic resection after an average of 10 courses of chemotherapy. (95 patients had a 50% or more decrease in total tumor size.)
51 René et al. continued Ann Surg 2004; 240(4): Combined techniques to achieve resectability Preop portal embolization in 12 patients (9%) RFA or cryosurgery in 20 patients (14%) Two-stage hepatectomy in 15 patients (11%) Most liver resections were nonanatomic or mixed (anatomic & nonanatomic) procedures (69%) The majority of resections were potentially curative (93%)
52 René et al. continued Ann Surg 2004; 240(4): Conclusions Modern chemotherapy allows 12.5% of patients with unresectable colorectal liver metastases to be rescued by liver surgery. Despite a high recurrence rate, 5 year survival is 33%.
53 Options for Palliation
54 Radiofrequency Ablation (RFA) RF thermal ablation works by converting RF waves into heat. A high-frequency alternating current ( khz) passes from an uninsulated electrode tip into the surrounding tissues and causes ionic vibration. The ionic vibration causes frictional heating of the tissues surrounding the electrode. The goal of RFA is to achieve local temperatures that make tissue destruction occur. Tissue heating also drives
55 RFA continued extra- and intracellular water out of the tissue and results in further destruction due to coagulative necrosis. Studies have shown that hyperthermia can also cause accelerated emigration of peripheral blood mononuclear cells, activation of effect cells, secretion of cytokines, and increased induction of apoptosis.
56 RFA continued The abundant portal venous blood flow present in normal hepatic parenchyma acts as a heat pump, which makes the creation of thermal injury in normal liver more difficult than in liver tumors. RFA has been found to be safer and better tolerated than other ablative techniques, such as cryotherapy, lasar ablation, and microwave ablation, and is described as having a 0% mortality rate. It is also associated with fewer local recurrence.
57 Complications of RFA Symptomatic pleural effusion Fever Pain Hemorrhage Subcutaneous hematoma Subcapsular liver hematoma Ventricular fibrillation Skin burn (in percutaneous procedures)
58 Complications of RFA continued Diaphragmatic necrosis Hepatic abscess Hepatic artery injuries Bile duct injuries Renal failure Liver failure Coagulopathy
59 Cryotherapy Hepatic cryotherapy involves the freezing and thawing of liver tumors by means of a cryoprobe inserted into the tumors. During freeze/thaw cycles, intracellular and extracellular ice formation occurs in an area termed the iceball, leading to tumor destruction. This procedure is done through an abdominal incision and cannot be done percutaneously like RFA.
60 Complications of Cryotherapy Hemorrhage of cracking frozen liver Bile collection Biliary fistula Pleural effusion Liver abscess Thrombocytopenia Myoglobinuria
61 Complications of Cryotherapy continued Arrhythmia Acute renal failure Cryoshock due to multi-organ failure with DIC Mortality rates range from 0-8% (overall mortality rate of 1.6%)
62 Hepatic Artery Chemotherapy The rationale for hepatic artery catheter chemotherapy is based on the fact that liver metastases over 1 cm derive most of their blood supply from the hepatic artery. The other rationale is the high first pass hepatic extraction of the drug used for this approach. Both factors cause high local drug concentrations with reduced systemic toxicity and allow higher dosages compared with intravenous treatment.
63 Hepatic Artery Chemotherapy continued 5-FU and fluorodeoxyuride (FUDR) are the chemotherapy agents usually used for this route of administration One British study reported a response rate of 43% in the intra-arterial group compared with 9% in the systemic chemotherapy group. Another study reported longer survival in the intra-arterial group compared with the systemic group (405 days vs. 226 days).
64 Immunotherapy Immunotherapy is mainly used in advanced diseases which have failed to respond to conventional therapy. Levamisole, a nonspecific immune stimulant, has been used in adjunctive treatment with 5-FU as an immune modulator. Some clinical trials have also shown that monoclonal antibody 17-1A is effective in increasing survival following resection of Dukes C primary colorectal tumors.
65 Radiotherapy Traditional external beam irradiation has found little place in the management of liver tumors because of the particularly radiosensitive nature of normal liver tissue, which limits the total dosage to Gy. Selective internal radiation therapy (SIRT) is a new modality that may be valuable in colorectal liver metastases that are not suitable to resection, RFA, or cryotherapy.
66 Selective Internal Radiation Therapy (SIRT) SIRT is a technique that allows high average doses of radiation ( Gy) to liver tumors with minimal serious effects on the non-tumorous liver. The treatment entails delivery of usually a single dose of Yttrium microspheres into the hepatic artery which, by virtue of almost exclusive arterial supply to liver tumors compared with the predominant portal supply to normal liver, results in selective tumor uptake and irradiation.
67 Conclusions Indications for resection of colorectal liver metastasis continue to broaden. Minimally invasive surgical techniques allow resection and palliation to be available to more patients. New technologies for palliation continue to emerge and become refined.
68
Current Treatment of Colorectal Metastases. Dr. Thavanathan Surgical Grand Rounds February 1, 2005
 Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
Management of Colorectal Liver Metastases
 Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options
 State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
Colon Cancer Liver Metastases: Liver-Directed Therapy
 Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
RF Ablation: indication, technique and imaging follow-up
 RF Ablation: indication, technique and imaging follow-up Trongtum Tongdee, M.D. Radiology Department, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand Objective Basic knowledge
RF Ablation: indication, technique and imaging follow-up Trongtum Tongdee, M.D. Radiology Department, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand Objective Basic knowledge
Multiple Primary Quiz
 Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Interventional Radiology in Liver Cancer. Nakarin Inmutto MD
 Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases
 Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases Thomas J. Vogl, B. Panahi, N. Nour-Eldin I D I R: Institute of Diagnostic and Interventional Radiology Goethe University Frankfurt,
Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases Thomas J. Vogl, B. Panahi, N. Nour-Eldin I D I R: Institute of Diagnostic and Interventional Radiology Goethe University Frankfurt,
HEPATIC METASTASES. We can state 3 types of metastases depending on their treatment options:
 HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
MANAGEMENT OF COLORECTAL METASTASES. Robert Warren, MD. The Postgraduate Course in General Surgery March 22, /22/2011
 MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Radiofrequency Ablation of Liver Tumors
 Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
Colorectal Liver Metastases Metachronous
 Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
Structured Follow-Up after Colorectal Cancer Resection: Overrated. R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007
 Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Management of Stage IV Colorectal Cancer: Expanding the Horizon
 Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
General summary GENERAL SUMMARY
 General summary GENERAL SUMMARY In Chapter 2.1 the long-term results and prognostic factors of radiofrequency ablation (RFA) for unresectable colorectal liver metastases (CRLM) in a single center with
General summary GENERAL SUMMARY In Chapter 2.1 the long-term results and prognostic factors of radiofrequency ablation (RFA) for unresectable colorectal liver metastases (CRLM) in a single center with
Trattamento chirurgico delle lesioni epatiche secondarie difficili. Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica
 Trattamento chirurgico delle lesioni epatiche secondarie difficili Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica What does it mean difficult lesions? Diagnosis Treatment Small size Unfit
Trattamento chirurgico delle lesioni epatiche secondarie difficili Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica What does it mean difficult lesions? Diagnosis Treatment Small size Unfit
Embolotherapy for Cholangiocarcinoma: 2016 Update
 Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
Metastatic Liver Cancer
 4 Metastatic Liver Cancer ANDREW J. SMITH, MD, FRCSC RONALD P. DEMATTEO, MD YUMAN FONG, MD, FACS LESLIE H. BLUMGART, MD, FACS, FRCS (ENG, EDIN, GLAS) The management of hepatic metastases has become more
4 Metastatic Liver Cancer ANDREW J. SMITH, MD, FRCSC RONALD P. DEMATTEO, MD YUMAN FONG, MD, FACS LESLIE H. BLUMGART, MD, FACS, FRCS (ENG, EDIN, GLAS) The management of hepatic metastases has become more
LIVER SURGERY 2. Case 1. Med 5 Refresher Course (Surgery) 2013/14. Dr Sunny Cheung
 2013/14. Dr Sunny Cheung") LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
Ruolo della interventistica per le secondarietà epatiche e di altre sedi
 Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
The Surgical Management of Colorectal Metastases
 11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
Management of colorectal cancer liver metastases
 Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Treatment of Colorectal Liver Metastases State of the Art
 Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Pre-operative assessment of patients for cytoreduction and HIPEC
 Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Liver metastases: treatment planning. PJ Valette
 Liver metastases: treatment planning PJ Valette Liver metastases removal December 2010 April 2011 : after chemotherapy June 2011 : after resection of left lobe mets & portal embol. Sept 2011 : 1 year after
Liver metastases: treatment planning PJ Valette Liver metastases removal December 2010 April 2011 : after chemotherapy June 2011 : after resection of left lobe mets & portal embol. Sept 2011 : 1 year after
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy
 Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
RFA of Tumors of the Lung: How and Why. Radiofrequency Ablation. Radiofrequency Ablation. RFA of pulmonary metastases. Radiofrequency Ablation of Lung
 RFA of Tumors of the Lung: How and Why Radiofrequency Ablation of Lung Ernest Scalzetti MD SUNY Upstate Medical University Syracuse NY FDA WARNING: Off-label use of a medical device Radiofrequency Ablation
RFA of Tumors of the Lung: How and Why Radiofrequency Ablation of Lung Ernest Scalzetti MD SUNY Upstate Medical University Syracuse NY FDA WARNING: Off-label use of a medical device Radiofrequency Ablation
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview
 Overview") Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Management of Cholangiocarcinoma. Roseanna Lee, MD PGY-5 Kings County Hospital
 Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Corporate Medical Policy
 Corporate Medical Policy Cryosurgical Ablation of Primary or Metastatic Liver Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: cryosurgical_ablation_of_primary_or_metastatic_liver_tumors
Corporate Medical Policy Cryosurgical Ablation of Primary or Metastatic Liver Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: cryosurgical_ablation_of_primary_or_metastatic_liver_tumors
pitfall Table 1 4 disorientation pitfall pitfall Table 1 Tel:
 11 687 692 2002 pitfall 1078 29 17 9 1 2 3 dislocation outflow block 11 1 2 3 9 1 2 3 4 disorientation pitfall 11 687 692 2002 Tel: 075-751-3606 606-8507 54 2001 8 27 2002 10 31 29 4 pitfall 16 1078 Table
11 687 692 2002 pitfall 1078 29 17 9 1 2 3 dislocation outflow block 11 1 2 3 9 1 2 3 4 disorientation pitfall 11 687 692 2002 Tel: 075-751-3606 606-8507 54 2001 8 27 2002 10 31 29 4 pitfall 16 1078 Table
RADIOFREQUENCY ABLATION
 RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
PET IMAGING (POSITRON EMISSION TOMOGRAPY) FACT SHEET
 FACT SHEET") Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
ONCOLOGIC PERCUTANEOUS INTERVENTION: 2015 UPDATE HANH VU NGHIEM, MD OAKLAND UNIVERSITY WILLIAM BEAUMONT SCHOOL OF MEDICINE
 ONCOLOGIC PERCUTANEOUS INTERVENTION: 2015 UPDATE HANH VU NGHIEM, MD OAKLAND UNIVERSITY WILLIAM BEAUMONT SCHOOL OF MEDICINE ONCOLOGIC PERCUTANEOUS IMAGE GUIDED TUMOR ABLATION Evolving, growing and increasingly
ONCOLOGIC PERCUTANEOUS INTERVENTION: 2015 UPDATE HANH VU NGHIEM, MD OAKLAND UNIVERSITY WILLIAM BEAUMONT SCHOOL OF MEDICINE ONCOLOGIC PERCUTANEOUS IMAGE GUIDED TUMOR ABLATION Evolving, growing and increasingly
Liver surgery, acute GI tract bleeding
 Semmelweis University, Faculty of Medicine, 1 st Department of Surgery Liver surgery, acute GI tract bleeding Oszkár HAHN M.D. LIVER CYST US, CT, MRI Parasite (ELISA, eosinophil, anaphylaxy) Echinococcus
Semmelweis University, Faculty of Medicine, 1 st Department of Surgery Liver surgery, acute GI tract bleeding Oszkár HAHN M.D. LIVER CYST US, CT, MRI Parasite (ELISA, eosinophil, anaphylaxy) Echinococcus
Management of Rare Liver Tumours
 Gian Luca Grazi Hepato-Biliary-Pancreatic Surgery National Cancer Institute Regina Elena Rome Fibrolamellar Carcinoma Mixed Hepato Cholangiocellular Carcinoma Hepatoblastoma Carcinosarcoma Primary Hepatic
Gian Luca Grazi Hepato-Biliary-Pancreatic Surgery National Cancer Institute Regina Elena Rome Fibrolamellar Carcinoma Mixed Hepato Cholangiocellular Carcinoma Hepatoblastoma Carcinosarcoma Primary Hepatic
How to deal with synchronous primary and liver metastases
 How to deal with synchronous primary and liver metastases Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB) Department of Surgery.
How to deal with synchronous primary and liver metastases Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB) Department of Surgery.
Locoregional Treatments for HCC Applications in Transplant Candidates. Locoregional Treatments for HCC Applications in Transplant Candidates
 Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page
 Vol.69(1), Page") The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
How to integrate surgery in the treatment of patients with liver-only metastatic disease
 How to integrate surgery in the treatment of patients with liver-only metastatic disease Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB)
How to integrate surgery in the treatment of patients with liver-only metastatic disease Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB)
Staging Colorectal Cancer
 Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Synchronous Hepatic Cryotherapy and Resection
 HPB Surgery, 2000, Vol. 11, pp. 379-382 Reprints available directly from the publisher Photocopying permitted by license only (C) 2000 OPA (Overseas Publishers Association) N.V. Published by license under
HPB Surgery, 2000, Vol. 11, pp. 379-382 Reprints available directly from the publisher Photocopying permitted by license only (C) 2000 OPA (Overseas Publishers Association) N.V. Published by license under
Hepatobiliary Malignancies Retrospective Study at Truman Medical Center
 Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
LiverGroup.org. Case Report Form (CRF) for STAGED procedures
 for STAGED procedures") Case Report Form (CRF) for STAGED procedures Patient Characteristics Case number * Age * ( 18)y Gender * Male Female Race * Caucasian Asian African Other If other race, please specify Height * cm Weight
Case Report Form (CRF) for STAGED procedures Patient Characteristics Case number * Age * ( 18)y Gender * Male Female Race * Caucasian Asian African Other If other race, please specify Height * cm Weight
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Liver surgery for colorectal liver metastases. Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham
 Liver surgery for colorectal liver metastases Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham Introduction: what do we do? UHB Liver Unit: Liver resections
Liver surgery for colorectal liver metastases Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham Introduction: what do we do? UHB Liver Unit: Liver resections
Intraductal papillary neoplasms in the bile ducts
 Intraductal papillary neoplasms in the bile ducts Seok Hwa Youn Myunghee Yoon Dong Hoon Shin Kosin University Gospel Hospital Department of general surgery Hepato-biliary-pancreatic division Introduction
Intraductal papillary neoplasms in the bile ducts Seok Hwa Youn Myunghee Yoon Dong Hoon Shin Kosin University Gospel Hospital Department of general surgery Hepato-biliary-pancreatic division Introduction
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers
 Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers Ching-Wei D. Tzeng, M.D. Assistant Professor Surgical Oncology University of Kentucky Markey Cancer Center Affiliate Network
Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers Ching-Wei D. Tzeng, M.D. Assistant Professor Surgical Oncology University of Kentucky Markey Cancer Center Affiliate Network
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
Nicolae Bacalbasa Carol Davila University Of Medicine and Pharmacy
 Nicolae Bacalbasa Carol Davila University Of Medicine and Pharmacy Approximately 5% to 10% of breast cancers are metastatic at diagnosis (1) 50% of breast cancer patients will develop distant metastases
Nicolae Bacalbasa Carol Davila University Of Medicine and Pharmacy Approximately 5% to 10% of breast cancers are metastatic at diagnosis (1) 50% of breast cancer patients will develop distant metastases
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms
 Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Case Report In Situ Split of the Liver When Portal Venous Embolization Fails to Induce Hypertrophy: A Report of Two Cases
 Case Reports in Surgery Volume 2013, Article ID 238675, 4 pages http://dx.doi.org/10.1155/2013/238675 Case Report In Situ Split of the Liver When Portal Venous Embolization Fails to Induce Hypertrophy:
Case Reports in Surgery Volume 2013, Article ID 238675, 4 pages http://dx.doi.org/10.1155/2013/238675 Case Report In Situ Split of the Liver When Portal Venous Embolization Fails to Induce Hypertrophy:
Dr Adam Bartlett. General Surgeon Senior Lecturer University of Auckland Auckland City Hospital
 Dr Adam Bartlett General Surgeon Senior Lecturer University of Auckland Auckland City Hospital 11:05-11:15 Hepatic Metastectomy is Associated with Improved Survival Where is everyone? Hepatic Metastectomy
Dr Adam Bartlett General Surgeon Senior Lecturer University of Auckland Auckland City Hospital 11:05-11:15 Hepatic Metastectomy is Associated with Improved Survival Where is everyone? Hepatic Metastectomy
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Liver Tumors. Patient Education. Treatment options 8 4A. About the Liver. Surgical Specialties
 Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
Chirurgie beim oligo-metastatischen NSCLC
 24. Ärzte-Fortbildungskurs in Klinischer Onkologie 20.-22. Februar 2014, Kantonsspital St. Gallen Chirurgie beim oligo-metastatischen NSCLC Prof. Dr. med. Walter Weder Klinikdirektor Thoraxchirurgie, UniversitätsSpital
24. Ärzte-Fortbildungskurs in Klinischer Onkologie 20.-22. Februar 2014, Kantonsspital St. Gallen Chirurgie beim oligo-metastatischen NSCLC Prof. Dr. med. Walter Weder Klinikdirektor Thoraxchirurgie, UniversitätsSpital
Regional Therapy for Metastatic Neuroendocrine Tumors. Janette Durham, MD Professor of Radiology University of Colorado School of Medicine
 Regional Therapy for Metastatic Neuroendocrine Tumors Janette Durham, MD Professor of Radiology University of Colorado School of Medicine Introduce regional therapy for mnet Arterial therapies Injection
Regional Therapy for Metastatic Neuroendocrine Tumors Janette Durham, MD Professor of Radiology University of Colorado School of Medicine Introduce regional therapy for mnet Arterial therapies Injection
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines
 Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Radiofrequency ablation combined with conventional radiotherapy: a treatment option for patients with medically inoperable lung cancer
 Radiofrequency ablation combined with conventional radiotherapy: a treatment option for patients with medically inoperable lung cancer Poster No.: C-0654 Congress: ECR 2011 Type: Scientific Paper Authors:
Radiofrequency ablation combined with conventional radiotherapy: a treatment option for patients with medically inoperable lung cancer Poster No.: C-0654 Congress: ECR 2011 Type: Scientific Paper Authors:
Liver Tumors. Prof. Dr. Ahmed El - Samongy
 Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Cholangiocarcinoma (Bile Duct Cancer)
") Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Published: Address correspondence to Vidal-Jove Joan:
 Oncothermia Journal 7:111-114 (2013) Complete responses after hyperthermic ablation by ultrasound guided high intensity focused ultrasound (USgHIFU) plus cystemic chemotherapy (SC) for locally advanced
Oncothermia Journal 7:111-114 (2013) Complete responses after hyperthermic ablation by ultrasound guided high intensity focused ultrasound (USgHIFU) plus cystemic chemotherapy (SC) for locally advanced
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5 Contents 5. Assessment & Management of Liver Metastases 42 5.1. Metachronous
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5 Contents 5. Assessment & Management of Liver Metastases 42 5.1. Metachronous
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
SECONDARIES: A PRELIMINARY REPORT
 HPB Surgery, 1990, Vol. 2, pp. 69-72 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORTS
HPB Surgery, 1990, Vol. 2, pp. 69-72 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORTS
TIMOTHY M. PAWLIK, RICHARD D. SCHULICK, MICHAEL A. CHOTI
 The Oncologist Hepatobiliary Expanding Criteria for Resectability of Colorectal Liver Metastases TIMOTHY M. PAWLIK,RICHARD D. SCHULICK,MICHAEL A. CHOTI Department of Surgery, Johns Hopkins University School
The Oncologist Hepatobiliary Expanding Criteria for Resectability of Colorectal Liver Metastases TIMOTHY M. PAWLIK,RICHARD D. SCHULICK,MICHAEL A. CHOTI Department of Surgery, Johns Hopkins University School
Cholangiocarcinoma. GI Practice Guideline. Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist)
 Barbara Fisher, MD, FRCPC (Radiation Oncologist)") Cholangiocarcinoma GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: October 2006 This guideline is a statement of consensus
Cholangiocarcinoma GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: October 2006 This guideline is a statement of consensus
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Percutaneous Radiofrequency Ablation of Lung Malignant Tumours: Survival, disease progression and complication rates
 Percutaneous Radiofrequency Ablation of Lung Malignant Tumours: Survival, disease progression and complication rates Poster No.: C-2576 Congress: ECR 2012 Type: Authors: Keywords: DOI: Scientific Exhibit
Percutaneous Radiofrequency Ablation of Lung Malignant Tumours: Survival, disease progression and complication rates Poster No.: C-2576 Congress: ECR 2012 Type: Authors: Keywords: DOI: Scientific Exhibit
LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE METASTASES
 LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE COLORECTAL CANCER LIVER METASTASES Jaime R. Merchan, MD, MMSc Associate Professor of Medicine Division of Hematology-Oncology University of Miami
LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE COLORECTAL CANCER LIVER METASTASES Jaime R. Merchan, MD, MMSc Associate Professor of Medicine Division of Hematology-Oncology University of Miami
Radioembolization with Lipiodol for the Treatment of Hepatocellular Carcinoma and Liver Metastases
 Radioembolization with Lipiodol for the Treatment of Hepatocellular Carcinoma and Liver Metastases Pr Francesco Giammarile CHLS Lyon Faculté de Lyon Sud «Aut tace aut loquere meliora silentio» Malignant
Radioembolization with Lipiodol for the Treatment of Hepatocellular Carcinoma and Liver Metastases Pr Francesco Giammarile CHLS Lyon Faculté de Lyon Sud «Aut tace aut loquere meliora silentio» Malignant
Tumor incidence varies significantly, depending on geographical location.
 Hepatocellular carcinoma is the 5 th most common malignancy worldwide with male-to-female ratio 5:1 in Asia 2:1 in the United States Tumor incidence varies significantly, depending on geographical location.
Hepatocellular carcinoma is the 5 th most common malignancy worldwide with male-to-female ratio 5:1 in Asia 2:1 in the United States Tumor incidence varies significantly, depending on geographical location.
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases
 Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
NAACCR Webinar Series 1
 Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Therapeutic Value of Radiofrequency Ablation of Hepatic Malignant Tumors
 Therapeutic Value of Radiofrequency Ablation of Hepatic Malignant Tumors Student: Shazia Hussain, V-01 Supervisor: Trond Buanes (Ullevål universitetssykehus) Universitetet i Oslo Det medisinske fakultet
Therapeutic Value of Radiofrequency Ablation of Hepatic Malignant Tumors Student: Shazia Hussain, V-01 Supervisor: Trond Buanes (Ullevål universitetssykehus) Universitetet i Oslo Det medisinske fakultet
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging
 Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Outcome following hepatic resection of metastatic renal tumors: the Paul Brousse Hospital experience
 HPB, 2006; 8: 100/105 REVIEW ARTICLE Outcome following hepatic resection of metastatic renal tumors: the Paul Brousse Hospital experience THOMAS A. ALOIA, RENÉ ADAM, DANIEL AZOULAY, HENRI BISMUTH & DENIS
HPB, 2006; 8: 100/105 REVIEW ARTICLE Outcome following hepatic resection of metastatic renal tumors: the Paul Brousse Hospital experience THOMAS A. ALOIA, RENÉ ADAM, DANIEL AZOULAY, HENRI BISMUTH & DENIS
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age. Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010
 Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D.
 Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
Hepatocellular Carcinoma: A major global health problem. David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center
 Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Aggressive surgery in the multimodality treatment of liver metastases from colorectal cancer
 Journal of BUON 12: 209-213, 2007 2007 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Aggressive surgery in the multimodality treatment of liver metastases from colorectal cancer N.
Journal of BUON 12: 209-213, 2007 2007 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Aggressive surgery in the multimodality treatment of liver metastases from colorectal cancer N.
Workup of a Solid Liver Lesion
 Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD
 UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
NEUROENDOCRINE CARCINOID TUMORS PANCREATIC NEUROENDOCRINE TUMORS
 University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
Locoregional Therapy for Hepatoma
 Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery
 Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation I: Patient ER 74 y/o male with A1A
Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation I: Patient ER 74 y/o male with A1A
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Cancer is a group of more than 100 different diseases that are characterized by uncontrolled cellular growth,
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Cancer is a group of more than 100 different diseases that are characterized by uncontrolled cellular growth,
EASL-EORTC Guidelines
 Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening