Proton- Radiotherapy: Overview of Clinical Indications
|
|
|
- Blaze Waters
- 5 years ago
- Views:
Transcription
1 Proton- Radiotherapy: Overview of Clinical Indications Eugen B. Hug (with emphasis on indications treated at PSI For comprehensive clinical reviews: ESTRO or PTCOG seminars) HUG 11/07
2 Complication Free Survival Complication-free Tumor Control
3 Complication free survival Complication-free Tumor Control
 Lomax, Phys. Med. Biol. 44:185-205, 1999 brainstem")
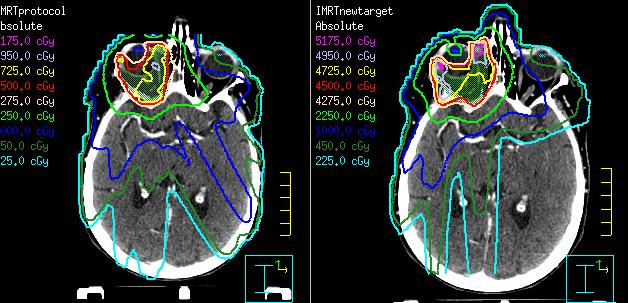
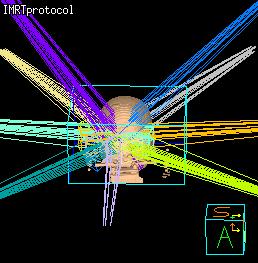
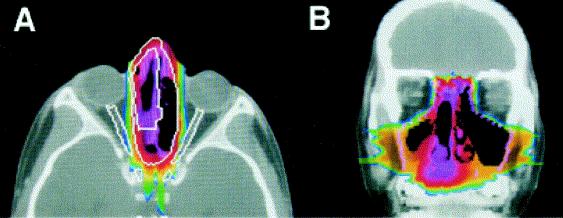
4 Proton-Radiotherapy for skull base tumors: 2 tumor (target volume) Lomax, Phys. Med. Biol. 44: , 1999 brainstem


5 Early clinical Phase: Proof of Safety and Efficacy 1973 Massachusetts General Hospital und Harvard Cyclotron, Boston und Cambridge, USA
6 Paradigm of proton therapy in the 70 s s and 80 s: Increase tumor dose = increase in local tumor control and Cure Early biologic models (Long-term outcomes data): eye tumors (uveal melanomas) skull base tumors paraspinale tumors of various histologies Unresectable sarcomas = excellent tumor models, but low incidence
7 Proton RT CPT Proton Radiation Therapy since the 70s and 80s the longest follow up data Uveal Melanomas Chordomas and Chondrosarcomas Skull Base and Paraspinal G. Goitein C. Ares C. Ares / E. Hug Sarcomas (occasional Pediatrics, Prostate-Ca) B. Timmermann


8 Tumors of the base of skull (examples) Primary skull base tumors: Chordoma, Chondrosarcoma Secondary infiltration from intracranial tumors: Meningioma Secondary infiltration from primary H&N tumors: Nasopharynx CA, Paranasale Sinus CA, Adenoid-cystic CA A.o. Nasopharynx Ca
9 Chordomas of the Base of Skull 5-year Local Control rates(%) Photons Romero 1993 Zorlu 2000 SRT Heidelb Protons MGH 1999 PSI 2007 LLUMC 1999 C-Ions GSI Dose [ Gy (RBE)]
10 Chordomas of the Base of Skull 5-year Local Control rates(%) Small Chordomas Chondrosarcomas High dose C-ions Photons Romero 1993 Zorlu 2000 SRT Heidelb Protons MGH 1999 PSI 2007 LLUMC 1999 C-Ions GSI Dose [ Gy (RBE)]
11 Proton Radiotherapy: - Results of the early clinical era- High-dose and/or hypofractionated therapy concepts increased tumor control compared to conventional photon RT by approx %.. and for the first time offered cures for selected, previously uncurable tumors (chondrosarcomas from 25-30% to 80% at 10 years) Examples: Skull Base Chordomas, Chondrosarcomas and adenoid Cystic Carcinomas, subgroups of Uveal Melanomas, Unresectable Sarcomas.

 2.")
12 Clinical Phase of the 90 s: Start of hospital-based Proton Radiotherapy Introduction of Gantry High-capacity patient treatments Additional clinical Indications: 1. Exploring high-frequeny diseases (prostate, lung) 2. New emphasis on Normal tissue sparing (pediatrics) Loma Linda, 1991

 (n =")
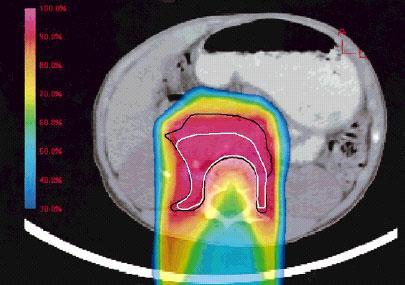
13 Protons for Prostate Ca: Multiple comparisons published Difference mainly in decreased Integral Dose Volume Comparison of Proton Therapy and Intensity-Modulated Radiotherapy for Prostate Cancer Vargas et al,ijrobp 2008, 70(3):744 Combined rectal dose volume curves for proton therapy and intensitymodulated radiotherapy (IMRT) (n = 20 plans)
14 Prostate Ca > Patients treated Loma Linda University Medical Center (Drs. Rossi, Slater ) 1255 patients treated between 10/91 and 12/97 Patients had no prior surgery or hormonal therapy CGE at CGE per fraction Follow-up mean 63 mos., median 62 mos. (range 1-132) Stage 1A/1B 1C 2A 2B 2C 3 Patients
15 Disease-free Survival (%) Prostate Cancer-LLUMC 10 YEAR Effect of Initial PSA on Disease-free Survival p = Years post Proton Radiation 90% < % 62% 43%
16 Treatment Morbidity RTOG Scale Grade 2 Grade 3 & 4 GI 3.5% 0 GU 5.4% 0.3% Total 9% 0.3%
17 Prospective, randomized trial: Comparison of Conventional-Dose vs High-Dose Conformal Radiation Therapy in Clinically Localized Adenocarcinoma of the Prostate: A randomized controlled trial Zietman AL et al. JAMA 2005; 294: patients enrolled 2 US academic institutions (LLUMC and HCL/MGH) Stage T1b through T2b prostate cancer Prostate-specific antigen (PSA) levels less than 15 ng/ml. Median PSA level was 6.3 ng/ml Median follow-up was 5.5 (range, ) years.

18 Randomized Trials: protons versus protons PROG 9509 T1b-2b prostate cancer PSA <15ng/ml r a n d o m i z a t i o n ACR/RTOG Proton boost 19.8 GyE Proton boost 28.8GyE 3-D conformal photons 50.4 Gy 3-D conformal photons 50.4 Gy Total prostate dose 70.2 GyE Total prostate dose 79.2 GyE
19 Zietman, A. L. et al. JAMA 2005;294: Freedom From Biochemical Failure (ASTRO Definition) Following Either Conventional-Dose (70.2 GyE) or High-Dose (79.2 GyE) Conformal Proton / Photon Radiation Therapy Copyright restrictions may apply.
20 Zietman, A. L. et al. CPT JAMA 2005;294: Acute and Late Genitourinary and Gastrointestinal (Rectal) Morbidity, by Assigned Radiation Therapy Dose and Toxicity Grade Authors conclusions: Men with clinically localized prostate cancer have a lower risk of biochemical failure if they receive high-dose rather than conventional-dose conformal radiation. This advantage was achieved without any associated increase in RTOG grade 3 acute or late urinary or rectal morbidity. Copyright restrictions may apply.
21 JAMA 2008: Correction Authors discovered incorrect coding in data base: Intended: biochem. failure = 3 successive PSA increases (ASTRO Def.) Coded: biochem. Failure = any 3 failures Result: higher # of pts. incorrectly coded as failures 79% 91% corrected 2008 incorrect 2005 Copyright restrictions may apply. JAMA 2008;299:
22 Randomized Trials: protons versus protons A Phase III Trial Employing Conformal Photons with Proton Boost in Early-stage Prostate Cancer: Conventional Dose (70.2 GyE) Compared to High-dose Irradiation (79.2 GyE): Long-term Update analysis of Proton Radiation Oncology Group (PROG)/American College of Radiology (ACR) Zietman AL, Rossi C, et al. IJROBP 2009, 75:3, S11 ASTRO Median follow-up: 8.9 years.
23 Zietman, A. L. et al. IJROBP 2009;75:3, S11 Freedom From Biochemical Failure (ASTRO Definition with backdating) Following Either Conventional-Dose (70.2 GyE) or High-Dose (79.2 GyE) Conformal Proton / Photon Radiation Therapy 70.2 vs GyE: 10-year BF rates (ASTRO) 35.3% vs % (p=0.0001) Low risk: 29% vs. 6.1% (p=0.0001) Intermed. Risk: 44.6 vs. 28.6% (p=0.06) No diff. in OS: 83.4 vs. 78.4% (p=0.45) No diff. in high Grade, late toxicity (> Gr. 3): overall 2.1% Higher toxicity, if Grade 2 included: (> Gr. 2): 29.4 vs. 39.4% (p=0.045) Authors conclusions: This RCT shows a long-term advantage in terms of freedom from biochemical failure for men with low and intermediate risk prostate cancer receiving high-dose vs. conventional dose conformal radiation delivered with mixed proton and photon beams. This advantage was achieved without any associated increase in Grade >3 late urinary or rectal morbidity.
 Similar rates of tumor control as had to be expected indications of decreasing rates of severe side effects for protons. approx.")
24 Status of Proton-Radiotherapy for Carcinoma of Prostate: Thus far a conservative approach Similar dose levels and fractionation regimen compared to modern photon RT (IMRT, IGRT, SBRT etc.) Similar rates of tumor control as had to be expected indications of decreasing rates of severe side effects for protons. approx. 50% of all patients treated world wide with Protons are treated for prostate CA
25 The conservative approach for Prostate Ca continues: New Protocol for early-stage Prostate Ca at LLUMC: 60 Gy (RBE) at 3 Gy / fract. Reduces treatment time from 45 frct. In 9 weeks (81 GyE at 1.8) to 20 frct. In 4 weeks
26 The conservative approach for prostate Ca continues unabated: New Protocol for early-stage Prostate Ca at LLUMC: 60 Gy (RBE) at 3 Gy / fract. Already done with photon-rt Primary goal reduce Tx-time time, economic concerns Very conservative hypofractionation compared to Cyberknife (King et al. IJROBP, 73(4), Gy x 5 = 36.25Gy) Where is the hypothesis-driven trial??
27 Proton Therapy for Malignancies of the Chest and Thorax: Breast-CA (Non-Small Cell) Lung CA Mesothelioma
28 Particle Therapy for Malignancies of the Chest and Thorax: Breast-CA CA: Partial Breast RT Whole Breast / Chestwall +/- regional LN RT (Non-Small Cell) Lung CA Mesothelioma
")




29 Partial Breast (accelerated) Irradiation: The goal: replace whole breast RT for low-risk breast Ca patients Interstitial Brachytherapy MammoSite



30 IMRT: Jagsi R, U. Michigan, IJROBP, in press Partial Breast (accelerated) Irradiation Helical Tomotherapy: Kainz K, Med. Coll. Wisconsin, IJROBP 74(1):275, 2009 Protons: Kozak K at MGH, IJROBP 65(5), 2006 plus intraoperative RT
31 Proton Therapy for Breast Ca: Accelerated Partial-Breast Proton Therapy: Initial MGH Experience Kozak, Taghian et al. IJROBP 66(3):691, 2006 Phase I/II trial. 20 women with T-1 breast Ca, neg. margins after lumpectomy PTV: lumpectomy cavity plus cm, minimum 5mm distance to surface/skin 32 Gy(RBE) total dose: 4 Gy (RBE) B.I.D. over 4 days 1-3 field arrangements overall, 1 field treated per day only Skin dose per field approached maximum dose, Single field per day = full 4 Gy skin dose. (MGH, passive scatttering ) Observation: Median F/U 12 months (8-22) increased acute toxicity: 80% moderate to severe skin color changes 22% severe moist desquamation
:691, 2006 Despite significant resolution of acute skin toxicities by 6 months, concerns persist Authors suggest: Multiple field arrangements, fields should not overlap at")
32 Accelerated Partial-Breast Proton Radiotherapy: Initial MGH Experience Kozak, Taghian et al. IJROBP 66(3):691, 2006 Despite significant resolution of acute skin toxicities by 6 months, concerns persist Authors suggest: Multiple field arrangements, fields should not overlap at skin, all fields treated per fraction Note: acute toxicity did not translate into early-late toxicity
33 Particle Therapy for Malignancies of the Chest and Thorax: Breast-CA CA: Partial Breast RT Whole Breast / Chestwall +/- regional LN RT (Non-Small Cell) Lung CA Mesothelioma

34 3D-CRT, IMRT, IMPT Comparison for local and locoregional breast RT (Ares for PSI, IJROBP Epub 2009) PTV1 scenario Whole Breast only Scenario #1: Whole breast 3D-CRT IMRT IMPT PTV2 scenario Whole Breast, MSC, LSC and AxIII Scenario #2: Whole breast, axillary LN, supraclav. LN 3D-CRT IMRT IMPT



35 PTV3 scenario Whole Breast, MSC, LSC, AxIII and IMC 3D-CRT IMRT IMPT Scenario #3: Whole breast, axillary LN, supraclav. LN IMC
36 Loco-regional RT (PTV-3) comparison Left lung V5 OAR s mean doses +/- SD Left lung V20 Right lung V5 Right lung V20 IMPT IMRT 3D-CRT Heart V5 Heart V22.5 Right breast mean Mean dose (%) +/- SD
37 Planned Pilot-Study at PSI: Proton Therapy for Breast Ca requiring locoregional Irradiation Eligibility criteria (draft version) female patients, non metastatic left-sided breast cancer with 4 positive axillary lymph nodes ( indication for inclusion of IMC nodes: internal quadrant tumors, or positive IMC uptake on lymphoscintigraphy or positive CT or PET-CT, or biopsy proven positive IMC nodes)
38 Particle Therapy for Malignancies of the Chest and Thorax: Breast-CA (Non-Small Cell) Lung CA Mesothelioma
, 2004 Proton radiotherapy only 68 patients, T1 (29 patients) and T2 (39 patients), NO,MO medically inoperable Non-small-cell Lung CA Dose: 51 cobalt Gray equivalent (CGE) in 10 fractions")
39 Proton-Radiotherapy for early Stage Lung Cancer Hypofractionated Proton Radiotherapy for Stage I Lung Cancer. Bush et al. Chest 126(4), 2004 Proton radiotherapy only 68 patients, T1 (29 patients) and T2 (39 patients), NO,MO medically inoperable Non-small-cell Lung CA Dose: 51 cobalt Gray equivalent (CGE) in 10 fractions over 2 weeks. Subsequently 60 CGE in 10 fractions. Median follow-up time 30 months Before PRT After PRT
, 2004 87% No symptomatic pneumonitis or late esophageal or cardiac toxicity 3-year local control: 74%; 3-year disease-specific survival: 72%")
40 Hypofractionated Proton Beam Radiotherapy for Stage I Lung Cancer. Bush et al. Chest 126(4), % No symptomatic pneumonitis or late esophageal or cardiac toxicity 3-year local control: 74%; 3-year disease-specific survival: 72% Local tumor control T1 vs T2 tumors = 87% vs 49% Trend toward improved survival.
 Present LLUMC- Protocol: 70 CGE / 10 frct. ( approx. 100 Gy at 2 Gy/frct)")
41 Effect of dose on Overall Survival: 3-year OS-rate 55% (60CGE) versus 27% (51 CGE) (p=0.03) Present LLUMC- Protocol: 70 CGE / 10 frct. ( approx. 100 Gy at 2 Gy/frct)
42 Studies on stage II and III NSCLC First Author STAGE II Year Txtype Pt. # Frct. dose (Gy) Frct. #: Total dose (Gy) % tumor < 3cm % medic. Inop. Median FU in months (range) Xia 2006 SBRT % 100% 27 (24-54) Salazar 2008 SBRT % 100% 38 (2-84) STAGE III Rowell 2004 CCR 1065 NR various NR NR various Auperin 2007 CCR 1205 NR various NR NR various Bush 1999 Proton Shioyam a % NR 14 (3-44) 2003 Proton % NR 30 (18-153)
43 Carbon-Ion Therapy for NSC-Lung Ca
44 Clinical Study on Carbon Beam Therapy for Stage I Non-Small Cell Lung Cancer (From: H. Tsjii, NIRs, Japan) Phase I/III (1994) 18 fr / 6 wks 47 pats Dose-escalation escalation 59.4GyE Phase I/II (1997) 9 fr / 3 wks 34 pts 68.4GyE Dose recommended 90GyE 72 GyE Phase (4/99-11/00) 9 fr / 3 wks 50 pats 72GyE Total 129 pats Phase I/II (12/00-11/03) 4 fr / 1 wk 79 pats 52.8GyE for stage IA 60.0GyE for stage IB Phase I/II (12/03 ~) Singledose 84 pats 28GyE
45 Local Control vs. Carbon Ion Dose for Different Fractionations in NSCLC 1.0 Local Control(%) Fr. 9 Fr GyE (TCP=0.95) 4 Fr. GyE 18 Fr. Patients data : 9 Fr. : 18 Fr. : 4 Fr.
46 Local Control in Single Fraction Treatment of Stage I NSCLC Total Dose Gy(RBE) No. 6mo. 12mo. 18mo. 24mo. 30mo. 36mo Currently, single fraction of 46GyE is being evaluated.
: 84.3% 2834GyE (n=67): 52.")
47 Local Control of Single Fraction C-ion RT(#0201) <34.0GyE vs. >36.0GyE P= GyE (n=105): 84.3% 2834GyE (n=67): 52.5% Months after RT



48 Single fraction 34GyE Pneumonitis appeared corresponding to the high dose area. From: Dr. Tsujii ESTRO Teaching course 2009
49 Particle Therapy for Malignancies of the Chest and Thorax: (Non-Small Cell) Lung CA present status a) Peripheral lung lesions: multiple modalities offer good local control (particles, SBRT, Cyberknife, Tomotherapy) area of great progress compared to standard EBRT. Local Control IA > 80%, lesser LC for IB.? Added benefit for particles? b) Central lung / mediastinum: remains a challenge for photons mainly due to V5-V20, MLD dose. Excellent opportunity for particles. c) The co-morbid patient: reduced lung function due to chronic lumonary disease (asthma, emphysema etc.) with little functional reserve to spare opportunity for particles Protons: evolving, essentially only few data, passive scattering only, active scanning technology presently not solved (except possibly by using anesthesia) Carbon Ions: very promising data, outstanding effort from NIRS, needs to be confirmed specifically toxicity profile
50 Particle Therapy for Malignancies of the Chest and Thorax: Breast-CA (Non-Small Cell) Lung CA Mesothelioma

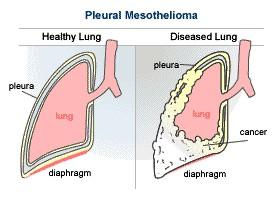


51 Asbestos From Asbestos to Mesothelioma Asbestos fibre From Asbestosis to chrysotile Mesothelioma
52 Standard Therapy for Mesothelioma: Trimodality Therapy / Triple Therapy Surgery (Extrapleural pneumonectomy) Chemotherapy Radiotherapy

")
53 Radiotherapy for Mesothelioma Conventional XRT (Plan from R. Cameron, UCLA, 2004) IMRT-Plan from MDAnderson CC)
54 Mesothelioma: high failure rate after triple-therapy CPT Comparison of Patterns of Failure After Extrapleural Pneumonectomy With or Without Adjuvant Therapy (Sugarbaker, 1997) Variable Sugarbaker 1997 Lung Cancer Study Group [1991] Cleveland Clinic [1994] Treatment EPP, CAP, RT EPP EPP or P, CT Median follow-up (mo) Not reported No. of patients evaluable for recurrence % of patients with recurrence 54% 76% 67% Recurrence site Recent series: approx. 30% Local % of all patients 35% 41% 56% % of recurrences 67% 54% 83% Abdomen % of all patients 26% 29% Not stated % of recurrences 50% 38% Contralateral thorax % of all patients 17% 29% Not stated % of recurrences 33% 38% Distant % of all patients 8% 35% 28% a % of recurrences 17% 46% 42% a


55 Mesothelioma: risk of contralateral lung damage by IMRT IJROBP / 13 patients developed FATAL pneumonitis after 54 Gy with IMRT



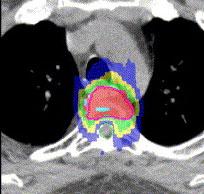
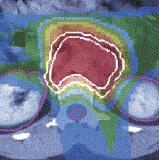
56 Mesothelioma: IMRT / Proton comparison U. Zürich / PSI collaboration Krayenbühl, Hartmann, Cziernik, Lomax (IJROBP submitted) IMRT Protons
57 Mesothelioma: IMRT / Proton comparison U. Zürich / PSI collaboration Krayenbühl, Hartmann, Cziernik, Lomax
58 Mesothelioma: IMRT / Proton comparison U. Zürich / PSI collaboration Krayenbühl, Hartmann, Cziernik, Lomax IMRT PT Mean difference p-value V95 (PTV1) [%] 96.0 ± 2,9 96,2 ± V105 (PTV1) [%] 4.8 ± ± V95 (PTV2) [%] 94,6 ± ± V105 (PTV2) [%] 36.1± ± IMRT PT Mean difference p-value D2 (spinal cord) [Gy] 15.1 ± 6, ± < 0,01 D2 (spinal cord) [Gy] 35.6 ± ± < 0,01 Dmean (ipsi. kidney) [Gy] 11,4 ± ± V15 (ipsi. Kidney) [%] 25.4 ± ± Dmean (heart) [Gy] 26,5 ± 6, ± < 0,01 V45 (heart) [%] 5.8 ± 2,0 2.3 ± Dmean (lung) [Gy] 9,6 ± ± < 0,01 V5 (lung) [%] 67.7 ± ± < 0,01 V13 (lung) [%] 24.1 ± ± V20 (lung) [%] 9.4 ± ±

59 2 legs of Proton Radiation Therapy High Dose Tumor application Reduction of low-dose volume of normal tissues
60 Orbital Rhabdomyosarcoma: Protons versus Photons Hein, Hug et al. IJROBP 62, 2005 Hug, et al. IJROBP, 47, 2000 Photons Protons

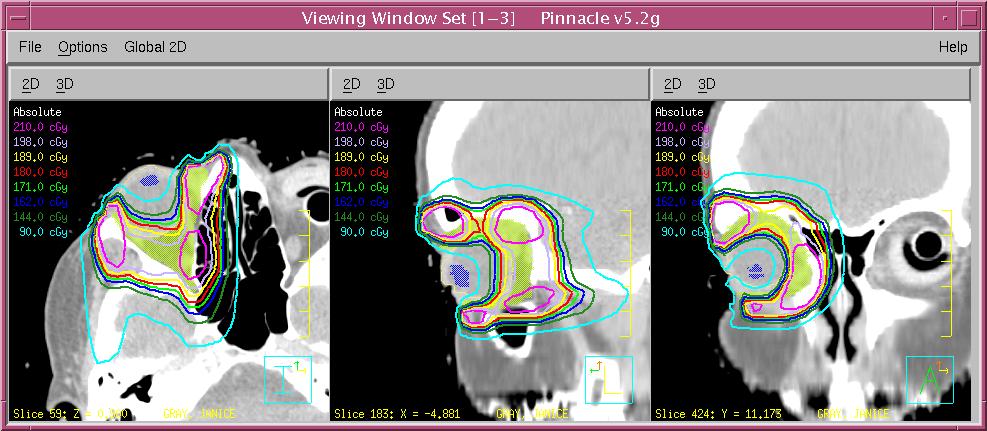
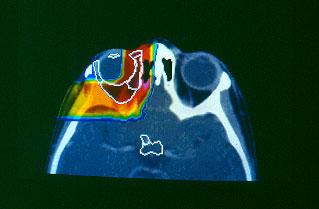
61 Orbitales Rhabdomyosarkom: Protonen versus Photonen Hein, Hug et al. IJROBP 62, 2005 Hug, et al. IJROBP, 47, 2000 Photonen Protonen
62 The Integral Dose Differential Comparative dose distributions for 9-field photon intensitymodulated photon (IMXT) and 3-field intensity-modulated protonradiation (IMPT) treatment plans for a patient with pelvic Ewing s sarcoma. IMXT IMPT (Courtesy of A.R. Smith and A.J. Lomax, in Delaney, Cancer Control, 2005) IMXT - IMPT
 treatment plans for a patient with pelvic Ewing s sarcoma. IMXT IMPT (Courtesy of A.R. Smith and A.J. Lomax, in Delaney, Cancer Control, 2005) IMXT - IMPT")
63 The Integral Dose Differential Comparative dose distributions for 9-field photon intensitymodulated photon (IMXT) and 3-field intensity-modulated protonradiation (IMPT) treatment plans for a patient with pelvic Ewing s sarcoma. IMXT IMPT (Courtesy of A.R. Smith and A.J. Lomax, in Delaney, Cancer Control, 2005) IMXT - IMPT

64 Pediatric Proton-- Radiotherapy
65 Protons for Pediatric Malignancies the accepted paradigm Reduction of the irradiated volume ( Integral Volume ) = Reduction of Late Effects Improved Quality of Life = Reduced risk of induction of Second Malignancy (Scanning Technologie )
66 Proton RT CPT Proton RT after >35 years and > patients treated no single disease entity ever treated with protons was later found unsuitable no publication has raised the issue of unexpected acute or late toxicity. (exception: Taghian et al., PBRT) The initial concept of physical dose distribution and biologic effectiveness has not been called into question by clinical results Proton-Radiotherapy has therefore successfully passed any reasonable requirements for treatment safety and feasibility.
67 Proton RT CPT Proton-RT: Status of Clinical Evidence Retrospective single-institution reports Prospective data accumulation Phase I and Phase II studies What about the evidence? What about randomized, prospective trials?
68 Level 1 Evidence for Proton Therapy (?) Randomized trial photons versus protons: Has not been done, EXCEPT: MGH/HCL Prostate trial: 67.2 Gy photons vs Gy protons/photons, T3 and T4 Randomized Trials: protons versus protons PROG 9509: Prostate CA, mixed photon/proton versus mixed photon/proton dose escalation: MGH + LBL+ LLUMC Chordoma and Chondrosarcoma Skull Base and C-spine randomized protocol (PROG) MGH/MEEI/HCL: Uveal Melanoma, dose de-escalation trial 70 vs. 50 Gy(RBE)
69 Proton RT CPT Proton RT Introduction of new radiotherapy technology has thus far never required randomized trials as long as safety and at least equivalency with prospect of superior outcomes have been demonstrated. (Examples: IMRT, Tomotherapy, Cyberknife)
70 The Confusing World of Precision- RT
71 The Confusing World of Precision- RT Clinical trial required Clinical trial required Clinical trial required




72 The Confusing World of Precision- RT Clinical trial required Clinical trial required Clinical trial required
73 ..more on trials and the ethics of trials on Wednesday THANK YOU!
Particle Radiation Therapy: CurrentStatus Indications -Results
 Particle Radiation Therapy: CurrentStatus Indications -Results Eugen B. Hug Center for Proton Therapy Paul Scherrer Institute and University of Zürich Switzerland Particle Radiation Therapy: Selection
Particle Radiation Therapy: CurrentStatus Indications -Results Eugen B. Hug Center for Proton Therapy Paul Scherrer Institute and University of Zürich Switzerland Particle Radiation Therapy: Selection
Proton Radiation Therapy for Osteosarcomas, Chondrogenic Tumors and Soft Tissue Sarcomas
 Proton Radiation Therapy for Osteosarcomas, Chondrogenic Tumors and Soft Tissue Sarcomas Eugen B. Hug Center for Proton Radiation Therapy Paul Scherrer Institute Is there a place for Proton/Particle Radiotherapy
Proton Radiation Therapy for Osteosarcomas, Chondrogenic Tumors and Soft Tissue Sarcomas Eugen B. Hug Center for Proton Radiation Therapy Paul Scherrer Institute Is there a place for Proton/Particle Radiotherapy
Proton Radiation Therapy for Osteosarcomas, Chondrogenic Tumors and Soft Tissue Sarcomas
 Proton Radiation Therapy for Osteosarcomas, Chondrogenic Tumors and Soft Tissue Sarcomas Eugen B. Hug Center for Proton Radiation Therapy Paul Scherrer Institute Histologies Osteogenic Tumors Osteogenic
Proton Radiation Therapy for Osteosarcomas, Chondrogenic Tumors and Soft Tissue Sarcomas Eugen B. Hug Center for Proton Radiation Therapy Paul Scherrer Institute Histologies Osteogenic Tumors Osteogenic
Future Directions in Prostate Cancer: The Case for Protons. John J. Coen, MD Helen & Harry Gray Cancer Center
 Future Directions in Prostate Cancer: The Case for Protons John J. Coen, MD Helen & Harry Gray Cancer Center November 14, 2012 Protons and prostate cancer Early proton experience at the MGH The case for
Future Directions in Prostate Cancer: The Case for Protons John J. Coen, MD Helen & Harry Gray Cancer Center November 14, 2012 Protons and prostate cancer Early proton experience at the MGH The case for
NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) BONE (Version , 03/28/18)
 BONE (Version , 03/28/18)") BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
Status of H 1 and C 12
 Status of H 1 and C 12 Herman Suit No Conflict of Interest 1 Goal of a New Treatment Modality Tumor Control Probability or No in Complication Rate 2 Truism No Advantage to: any Patient for any Radiation
Status of H 1 and C 12 Herman Suit No Conflict of Interest 1 Goal of a New Treatment Modality Tumor Control Probability or No in Complication Rate 2 Truism No Advantage to: any Patient for any Radiation
Proton- Radiotherapy:
 Proton- Radiotherapy: Future of Medical Indications and Treatment Concepts Eugen B. Hug and Ralf A. Schneider HUG 11/07 The emerging role of Proton Radiotherapy in the framework of modern Photon-RT 2000
Proton- Radiotherapy: Future of Medical Indications and Treatment Concepts Eugen B. Hug and Ralf A. Schneider HUG 11/07 The emerging role of Proton Radiotherapy in the framework of modern Photon-RT 2000
Carbon Ion Radiotherapy for Skull Base and Paracervical Chordomas
 Carbon Ion Radiotherapy for Skull Base and Paracervical Chordomas Azusa Hasegawa, Jun-etsu Mizoe and Hirohiko Tsujii Research Center Hospital for Charged Particle Therapy National Institute of Radiological
Carbon Ion Radiotherapy for Skull Base and Paracervical Chordomas Azusa Hasegawa, Jun-etsu Mizoe and Hirohiko Tsujii Research Center Hospital for Charged Particle Therapy National Institute of Radiological
Advances in external beam radiotherapy
 International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
Proton Radiotherapy for Skull Base and Para-spinal Tumors
 Proton Radiotherapy for Skull Base and Para-spinal Tumors Carmen Ares Primary tumors Tumors of the Skull Base - Chordomas, Chondrosarcomas Secondary infiltration or involvement by intracranial tumors -
Proton Radiotherapy for Skull Base and Para-spinal Tumors Carmen Ares Primary tumors Tumors of the Skull Base - Chordomas, Chondrosarcomas Secondary infiltration or involvement by intracranial tumors -
Proton-Radiotherapy for Tumors of the Skull Base: Indications, Advantages, Limitations
 Proton-Radiotherapy for Tumors of the Skull Base: Indications, Advantages, Limitations Eugen B. Hug, MD Director, Center for Proton-Radiotherapy, Paul Scherrer Institut, Villigen and Chair of Proton-Radiotherapy.
Proton-Radiotherapy for Tumors of the Skull Base: Indications, Advantages, Limitations Eugen B. Hug, MD Director, Center for Proton-Radiotherapy, Paul Scherrer Institut, Villigen and Chair of Proton-Radiotherapy.
HEAVY PARTICLE THERAPY
 HEAVY PARTICLE THERAPY DR. G.V. GIRI KIDWAI MEMORIAL INSTITUTE OF ONCOLOGY ICRO 2012 BHATINDA HEAVY PARTICLES USED IN A EFFORT TO IMPROVE TUMOR CONTROL, THAT DO NOT RESPOND TO PHOTONS OR ELECTRONS BETTER
HEAVY PARTICLE THERAPY DR. G.V. GIRI KIDWAI MEMORIAL INSTITUTE OF ONCOLOGY ICRO 2012 BHATINDA HEAVY PARTICLES USED IN A EFFORT TO IMPROVE TUMOR CONTROL, THAT DO NOT RESPOND TO PHOTONS OR ELECTRONS BETTER
Proton Therapy for tumors of the skull base - RESULTS. Eugen B. Hug, MD Medical Director, ProCure Proton Therapy Centers, NY
 Proton Therapy for tumors of the skull base - RESULTS Eugen B. Hug, MD Medical Director, ProCure Proton Therapy Centers, NY Petroclival Chondrosarcoma: 68 72 Gy(RBE) at 1.8 or 2.0 Gy(RBE) GTV: 70.2 Gy(RBE)
Proton Therapy for tumors of the skull base - RESULTS Eugen B. Hug, MD Medical Director, ProCure Proton Therapy Centers, NY Petroclival Chondrosarcoma: 68 72 Gy(RBE) at 1.8 or 2.0 Gy(RBE) GTV: 70.2 Gy(RBE)
Protons for Head and Neck Cancer. William M Mendenhall, M.D.
 Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Clinical Results of Carbon Ion Radiotherapy: The Heidelberg Experience
 Clinical Results of Carbon Ion Radiotherapy: The Heidelberg Experience Stephanie E. Combs, MD Department of Radiation Oncology University of Heidelberg, Germany Carbon ion RT at GSI Active beam delivery
Clinical Results of Carbon Ion Radiotherapy: The Heidelberg Experience Stephanie E. Combs, MD Department of Radiation Oncology University of Heidelberg, Germany Carbon ion RT at GSI Active beam delivery
Andrew K. Lee, MD, MPH Associate Professor Department tof fradiation Oncology M.D. Anderson Cancer Center
 Proton Therapy for Prostate Cancer Andrew K. Lee, MD, MPH Associate Professor Department tof fradiation Oncology M.D. Anderson Cancer Center Seungtaek Choi, MD Assistant Professor Department tof fradiation
Proton Therapy for Prostate Cancer Andrew K. Lee, MD, MPH Associate Professor Department tof fradiation Oncology M.D. Anderson Cancer Center Seungtaek Choi, MD Assistant Professor Department tof fradiation
Disclosures. Proton therapy advantages. Why are comparing therapies difficult? Proton Therapy for Low Risk Prostate Cancer
 Proton Therapy for Low Risk Prostate Cancer Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments Andrew K. Lee, MD, MPH Associate Professor
Proton Therapy for Low Risk Prostate Cancer Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments Andrew K. Lee, MD, MPH Associate Professor
Particle Therapy for Tumors of the Skull Base. Eugen B. Hug, MD Medical Director, ProCure Proton Therapy Centers, NY
 Particle Therapy for Tumors of the Skull Base Eugen B. Hug, MD Medical Director, ProCure Proton Therapy Centers, NY Particle Radiation Therapy for Tumors of the Skull Base Primary skull base tumors: Chordoma,
Particle Therapy for Tumors of the Skull Base Eugen B. Hug, MD Medical Director, ProCure Proton Therapy Centers, NY Particle Radiation Therapy for Tumors of the Skull Base Primary skull base tumors: Chordoma,
Clinical experience with TomoDirect System Tangential Mode
 Breast Cancer Clinical experience with TomoDirect System Tangential Mode European Institute of Oncology Milan, Italy Disclosure & Disclaimer An honorarium is provided by Accuray for this presentation The
Breast Cancer Clinical experience with TomoDirect System Tangential Mode European Institute of Oncology Milan, Italy Disclosure & Disclaimer An honorarium is provided by Accuray for this presentation The
Summary Talk of the Workshop
 Medical experience History of IBT 1954 1975 1976 1977 1982 1987 1992 Pituitary 1st He pt Treatment 1st C, Ne pt Eye treatment Phase-1 He Phase I-II Ne Phase I-II Ne & He 1st Comp Tx Plan 3D planning LBNL
Medical experience History of IBT 1954 1975 1976 1977 1982 1987 1992 Pituitary 1st He pt Treatment 1st C, Ne pt Eye treatment Phase-1 He Phase I-II Ne Phase I-II Ne & He 1st Comp Tx Plan 3D planning LBNL
Radiation Therapy 2013 The Role of Protons. Bob Gaston, D.O.
 Radiation Therapy 2013 The Role of Protons Bob Gaston, D.O. Disclosures Oklahoma ProCure Treatment Center Radiation Medicine Associates Goal of Radiation Therapy Increase the Therapeutic Ratio Therapeutic
Radiation Therapy 2013 The Role of Protons Bob Gaston, D.O. Disclosures Oklahoma ProCure Treatment Center Radiation Medicine Associates Goal of Radiation Therapy Increase the Therapeutic Ratio Therapeutic
Current Status and Future Medical Perspectives at MedAustron. U. Mock EBG MedAustron GmbH
 Current Status and Future Medical Perspectives at MedAustron U. Mock EBG MedAustron GmbH Cancer treatment facility Ion beam therapy with protons and carbon ions Research facility Medical physics Radiobiology
Current Status and Future Medical Perspectives at MedAustron U. Mock EBG MedAustron GmbH Cancer treatment facility Ion beam therapy with protons and carbon ions Research facility Medical physics Radiobiology
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING
 PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
Sacral Chordoma: The Loma Linda University Radiation Medicine Experience. Kevin Yiee MD, MPH Resident Physician
 Sacral Chordoma: The Loma Linda University Radiation Medicine Experience Kevin Yiee MD, MPH Resident Physician What is a chordoma? 1 st chordoma discovered in clivus by Virchow and Luschka 1856 Rare tumor
Sacral Chordoma: The Loma Linda University Radiation Medicine Experience Kevin Yiee MD, MPH Resident Physician What is a chordoma? 1 st chordoma discovered in clivus by Virchow and Luschka 1856 Rare tumor
Stereotactic radiotherapy
 Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
State of the Art Radiotherapy for Pediatric Tumors. Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center
 State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology
 The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
Questions may be submitted anytime during the presentation.
 Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Charged-Particle (Proton or Helium Ion) Radiotherapy for Neoplastic Conditions
 Radiotherapy for Neoplastic Conditions") Charged-Particle (Proton or Helium Ion) Radiotherapy for Neoplastic Conditions Policy Number: 8.01.10 Last Review: 11/2017 Origination: 11/2006 Next Review: 11/2018 Policy Blue Cross and Blue Shield of
Charged-Particle (Proton or Helium Ion) Radiotherapy for Neoplastic Conditions Policy Number: 8.01.10 Last Review: 11/2017 Origination: 11/2006 Next Review: 11/2018 Policy Blue Cross and Blue Shield of
Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT)
") Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT) The Institute for Clinical and Economic Review (ICER) has published appraisals on multiple management options for clinically-localized,
Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT) The Institute for Clinical and Economic Review (ICER) has published appraisals on multiple management options for clinically-localized,
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
The Rise, Fall, and Rise Again of Proton Therapy or Never count out a well-financed therapy
 The Rise, Fall, and Rise Again of Proton Therapy or Never count out a well-financed therapy Anthony Zietman MD Shipley Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School
The Rise, Fall, and Rise Again of Proton Therapy or Never count out a well-financed therapy Anthony Zietman MD Shipley Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School
Charged-Particle (Proton or Helium Ion) Radiotherapy for Neoplastic Conditions
 Radiotherapy for Neoplastic Conditions") Charged-Particle (Proton or Helium Ion) Radiotherapy for Neoplastic Conditions Policy Number: Original Effective Date: MM.05.005 07/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST
Charged-Particle (Proton or Helium Ion) Radiotherapy for Neoplastic Conditions Policy Number: Original Effective Date: MM.05.005 07/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy
 San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
Role of protons, heavy ions and BNCT in brain tumors
 Role of protons, heavy ions and BNCT in brain tumors Prof G K Rath Head, NCI (AIIMS-2) Chief, Dr. BRA IRCH, Professor Radiation Oncology All India Institute of Medical Sciences, New Delhi 1 Overview of
Role of protons, heavy ions and BNCT in brain tumors Prof G K Rath Head, NCI (AIIMS-2) Chief, Dr. BRA IRCH, Professor Radiation Oncology All India Institute of Medical Sciences, New Delhi 1 Overview of
Clinically Proven Metabolically-Guided TomoTherapy SM Treatments Advancing Cancer Care
 Clinically Proven Metabolically-Guided TomoTherapy SM Treatments Advancing Cancer Care Institution: San Raffaele Hospital Milan, Italy By Nadia Di Muzio, M.D., Radiotherapy Department (collaborators: Berardi
Clinically Proven Metabolically-Guided TomoTherapy SM Treatments Advancing Cancer Care Institution: San Raffaele Hospital Milan, Italy By Nadia Di Muzio, M.D., Radiotherapy Department (collaborators: Berardi
Particle (proton) Therapy Randomized trials vs. Prospective registry. Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology
 Therapy Randomized trials vs. Prospective registry. Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology") Particle (proton) Therapy Randomized trials vs. Prospective registry Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Should we do randomized trials? Are randomized trials needed
Particle (proton) Therapy Randomized trials vs. Prospective registry Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Should we do randomized trials? Are randomized trials needed
Effectiveness and Safety of Spot Scanning Proton Radiation Therapy for Skull Base Tumors: First Long Term Report of the PSI Experience
 Effectiveness and Safety of Spot Scanning Proton Radiation Therapy for Skull Base Tumors: First Long Term Report of the PSI Experience Carmen Ares, Antony J Lomax, Eugen B Hug, Alessandra Bolsi, Beate
Effectiveness and Safety of Spot Scanning Proton Radiation Therapy for Skull Base Tumors: First Long Term Report of the PSI Experience Carmen Ares, Antony J Lomax, Eugen B Hug, Alessandra Bolsi, Beate
Professor of Medicine. Division of General Internal Medicine. Department of Medicine. University of California San Francisco
 TITLE: Proton Therapy for Prostate Cancer AUTHOR: Judith Walsh, MD, MPH Professor of Medicine Division of General Internal Medicine Department of Medicine University of California San Francisco PUBLISHER:
TITLE: Proton Therapy for Prostate Cancer AUTHOR: Judith Walsh, MD, MPH Professor of Medicine Division of General Internal Medicine Department of Medicine University of California San Francisco PUBLISHER:
Radiation Technology, Hyogo Ion Beam Medical Center, Tatsuno, Hyogo, JAPAN
 Analysis of Visual Loss Due to Radiation- Induced Optic Neuropathy After Particle Therapy for Head and Neck and Skull Base Tumors Adjacent to Optic Nerves Y. Demizu 1, M. Murakami 1, D. Miyawaki 1, Y.
Analysis of Visual Loss Due to Radiation- Induced Optic Neuropathy After Particle Therapy for Head and Neck and Skull Base Tumors Adjacent to Optic Nerves Y. Demizu 1, M. Murakami 1, D. Miyawaki 1, Y.
Clinical Report for Wanjie Proton Therapy Center. Li Jiamin, MD Wanjie Proton Therapy Center
 Clinical Report for Wanjie Proton Therapy Center Li Jiamin, MD Wanjie Proton Therapy Center General Information Wanjie Proton Therapy Center was founded in June 2001 The first patient was treated in Dec.
Clinical Report for Wanjie Proton Therapy Center Li Jiamin, MD Wanjie Proton Therapy Center General Information Wanjie Proton Therapy Center was founded in June 2001 The first patient was treated in Dec.
SBRT in early stage NSCLC
 SBRT in early stage NSCLC Optimal technique and tumor dose Frank Zimmermann Clinic of Radiotherapy and Radiation Oncology University Hospital Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch Techniques
SBRT in early stage NSCLC Optimal technique and tumor dose Frank Zimmermann Clinic of Radiotherapy and Radiation Oncology University Hospital Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch Techniques
Charged-Particle (Proton or Helium Ion) Radiation Therapy. Original Policy Date
 Radiation Therapy. Original Policy Date") MP 8.01.08 Charged-Particle (Proton or Helium Ion) Radiation Therapy Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013
MP 8.01.08 Charged-Particle (Proton or Helium Ion) Radiation Therapy Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013
CyberKnife SBRT for Prostate Cancer
 CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
Clinical Aspects of Proton Therapy in Lung Cancer. Joe Y. Chang, MD, PhD Associate Professor
 Clinical Aspects of Proton Therapy in Lung Cancer Joe Y. Chang, MD, PhD Associate Professor Clinical Service Chief Thoracic Radiation Oncology Lung Cancer Basic Factors No. 1 cancer killer 161,840 patients
Clinical Aspects of Proton Therapy in Lung Cancer Joe Y. Chang, MD, PhD Associate Professor Clinical Service Chief Thoracic Radiation Oncology Lung Cancer Basic Factors No. 1 cancer killer 161,840 patients
RADIOTHERAPY IN BREAST CANCER :
 RADIOTHERAPY IN BREAST CANCER : PAST, PRESENT, FUTURE Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Cancer Institute Narayana Superspecialty Hospital Breast cancer is the classic paradigm
RADIOTHERAPY IN BREAST CANCER : PAST, PRESENT, FUTURE Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Cancer Institute Narayana Superspecialty Hospital Breast cancer is the classic paradigm
Treatment Planning for Breast Cancer: Contouring Targets. Julia White MD Professor
 Treatment Planning for Breast Cancer: Contouring Targets Julia White MD Professor Outline 1. RTOG Breast Cancer Atlas 2. Target development on Clinical Trials Whole Breast Irradiation 2-D Radiotherapy
Treatment Planning for Breast Cancer: Contouring Targets Julia White MD Professor Outline 1. RTOG Breast Cancer Atlas 2. Target development on Clinical Trials Whole Breast Irradiation 2-D Radiotherapy
Demands and Perspectives of Hadron Therapy
 Demands and Perspectives of Hadron Therapy Alexander Lin, M.D. Assistant Professor University of Pennsylvania Direction of Operations Roberts Proton Therapy Center Disclosures Teva Pharmaceuticals: Advisory
Demands and Perspectives of Hadron Therapy Alexander Lin, M.D. Assistant Professor University of Pennsylvania Direction of Operations Roberts Proton Therapy Center Disclosures Teva Pharmaceuticals: Advisory
MP Charged-Particle (Proton or Helium Ion) Radiotherapy for Neoplastic Conditions
 Radiotherapy for Neoplastic Conditions") Medical Policy BCBSA Ref. Policy: 8.01.10 Last Review: 07/25/2018 Effective Date: 07/25/2018 Section: Therapy Related Policies 6.01.10 Stereotactic Radiosurgery and Stereotactic Body Radiotherapy 8.01.46
Medical Policy BCBSA Ref. Policy: 8.01.10 Last Review: 07/25/2018 Effective Date: 07/25/2018 Section: Therapy Related Policies 6.01.10 Stereotactic Radiosurgery and Stereotactic Body Radiotherapy 8.01.46
External Beam Radiation Therapy for Low/Intermediate Risk Prostate Cancer
 External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
Where are we with radiotherapy for biliary tract cancers?
 Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Particle Therapy for CNS Tumors Anita Mahajan MD MD Anderson Cancer Center PTCOG, Shanghai June 10, 2014
 Particle Therapy for CNS Tumors Anita Mahajan MD MD Anderson Cancer Center PTCOG, Shanghai June 10, 2014 TCP/NTCP (%) The Potential for Protons in the CNS 10 0 Increase Tumor Control Increase TCP increased
Particle Therapy for CNS Tumors Anita Mahajan MD MD Anderson Cancer Center PTCOG, Shanghai June 10, 2014 TCP/NTCP (%) The Potential for Protons in the CNS 10 0 Increase Tumor Control Increase TCP increased
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES
 DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
Prostate Cancer. 3DCRT vs IMRT : Hasan Murshed
 Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
Page 1. Helical (Spiral) Tomotherapy. UW Helical Tomotherapy Unit. Helical (Spiral) Tomotherapy. MVCT of an Anesthetized Dog with a Sinus Tumor
 Tomotherapy. UW Helical Tomotherapy Unit. Helical (Spiral) Tomotherapy. MVCT of an Anesthetized Dog with a Sinus Tumor") Helical (Spiral) Tomotherapy Novel Clinical Applications of IMRT Linac Ring Gantry CT Detector X-Ray Fan Beam Binary Multileaf Collimator Binary MLC Leaves James S Welsh, MS, MD Department of Human Oncology
Helical (Spiral) Tomotherapy Novel Clinical Applications of IMRT Linac Ring Gantry CT Detector X-Ray Fan Beam Binary Multileaf Collimator Binary MLC Leaves James S Welsh, MS, MD Department of Human Oncology
Clinical Trials of Proton Therapy for Breast Cancer. Andrew L. Chang, MD 張維安 Study Chair
 Clinical Trials of Proton Therapy for Breast Cancer Andrew L. Chang, MD 張維安 Study Chair AndrewLChangMD@gmail.com Disclosure Proton Center Development Corporation Scripps San Diego Proton Therapy Center
Clinical Trials of Proton Therapy for Breast Cancer Andrew L. Chang, MD 張維安 Study Chair AndrewLChangMD@gmail.com Disclosure Proton Center Development Corporation Scripps San Diego Proton Therapy Center
ACR TXIT TM EXAM OUTLINE
 ACR TXIT TM EXAM OUTLINE Major Domain Sub-Domain 1 Statistics 1.1 Study design 1.2 Definitions of statistical terms 1.3 General interpretation & analysis 1.4 Survival curves 1.5 Specificity/sensitivity
ACR TXIT TM EXAM OUTLINE Major Domain Sub-Domain 1 Statistics 1.1 Study design 1.2 Definitions of statistical terms 1.3 General interpretation & analysis 1.4 Survival curves 1.5 Specificity/sensitivity
Tecniche Radioterapiche U. Ricardi
 Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
External Beam Radiotherapy for Prostate Cancer
 External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
Disclosures 5/13/2013. Principles and Practice of Radiation Oncology First Annual Cancer Rehabilitation Symposium May 31, 2013
 Principles and Practice of Radiation Oncology First Annual Cancer Rehabilitation Symposium May 31, 2013 Josh Yamada MD FRCPC Department of Radiation Oncology Memorial Sloan Kettering Cancer Center Disclosures
Principles and Practice of Radiation Oncology First Annual Cancer Rehabilitation Symposium May 31, 2013 Josh Yamada MD FRCPC Department of Radiation Oncology Memorial Sloan Kettering Cancer Center Disclosures
-Proton Beam Therapy in Paediatric Radiation Oncology -
 -Proton Beam Therapy in Paediatric Radiation Oncology - Beate Timmermann, M.D. West German Proton Therapy Centre Essen Germany Preview Survival Toxicity Why protons? (theoretically) Experiences so far
-Proton Beam Therapy in Paediatric Radiation Oncology - Beate Timmermann, M.D. West German Proton Therapy Centre Essen Germany Preview Survival Toxicity Why protons? (theoretically) Experiences so far
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy?
 Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
Hot topics in Radiation Oncology for the Primary Care Providers
 Hot topics in Radiation Oncology for the Primary Care Providers Steven Feigenberg, MD Professor Chief, Thoracic Oncology Vice Chair of Clinical Research April 19, 2018 Disclosures NONE 2 Early Stage Disease
Hot topics in Radiation Oncology for the Primary Care Providers Steven Feigenberg, MD Professor Chief, Thoracic Oncology Vice Chair of Clinical Research April 19, 2018 Disclosures NONE 2 Early Stage Disease
Radiotherapy Physics and Equipment
 Radiological Sciences Department Radiotherapy Physics and Equipment RAD 481 Lecture s Title: Introduction Dr. Mohammed EMAM Ph.D., Paris-Sud 11 University Vision :IMC aspires to be a leader in applied
Radiological Sciences Department Radiotherapy Physics and Equipment RAD 481 Lecture s Title: Introduction Dr. Mohammed EMAM Ph.D., Paris-Sud 11 University Vision :IMC aspires to be a leader in applied
The Current & Future State of Particle Therapy
 The Current & Future State of Particle Therapy The MD Anderson Proton Therapy Center- Houston Matthew Palmer, MBA, CMD Chief Operating Officer mpalmer@mdanderson.org The Challenge PlanIQ TM, Courtesy of
The Current & Future State of Particle Therapy The MD Anderson Proton Therapy Center- Houston Matthew Palmer, MBA, CMD Chief Operating Officer mpalmer@mdanderson.org The Challenge PlanIQ TM, Courtesy of
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部
 肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
and Strength of Recommendations
 ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
Disclosures. The Challenges Facing Proton Beam Therapy and Opportunities. Minesh P Mehta, MBChB, FASTRO
 Minesh P Mehta, MBChB, FASTRO The Challenges Facing Proton Beam Therapy and Opportunities Disclosures Consultant: Varian, IBA, Agenus, Remedy, Insys DSMB: Monteris Current as of October 2016 1 The Challenges
Minesh P Mehta, MBChB, FASTRO The Challenges Facing Proton Beam Therapy and Opportunities Disclosures Consultant: Varian, IBA, Agenus, Remedy, Insys DSMB: Monteris Current as of October 2016 1 The Challenges
Proton Therapy: Where Are We Now and Where Are We Going? Erin Davis MSN, CRNP, ACNP BC Lead Nurse Practitioner
 Proton Therapy: Where Are We Now and Where Are We Going? Erin Davis MSN, CRNP, ACNP BC Lead Nurse Practitioner Genevieve Hollis MSN, CRNP, ANP-BC, AOCN Oncology Nurse Practitioner Advanced Senior Lecturer-B
Proton Therapy: Where Are We Now and Where Are We Going? Erin Davis MSN, CRNP, ACNP BC Lead Nurse Practitioner Genevieve Hollis MSN, CRNP, ANP-BC, AOCN Oncology Nurse Practitioner Advanced Senior Lecturer-B
Current Status of Accelerated Partial Breast Irradiation. Julia White MD Professor, Radiation Oncology
 Current Status of Accelerated Partial Breast Irradiation Julia White MD Professor, Radiation Oncology I have no disclosures relative to the presented material Agenda ABPI Timeline APBI by Method Clinical
Current Status of Accelerated Partial Breast Irradiation Julia White MD Professor, Radiation Oncology I have no disclosures relative to the presented material Agenda ABPI Timeline APBI by Method Clinical
Charged-Particle (Proton) Radiotherapy
 Radiotherapy") Medical Policy Manual Medicine, Policy No. 49 Charged-Particle (Proton) Radiotherapy Next Review: June 2019 Last Review: October 2018 Effective: December 1, 2018 IMPORTANT REMINDER Medical Policies are
Medical Policy Manual Medicine, Policy No. 49 Charged-Particle (Proton) Radiotherapy Next Review: June 2019 Last Review: October 2018 Effective: December 1, 2018 IMPORTANT REMINDER Medical Policies are
PTCOG 46. Educational Workshop Session IV. Head & Neck CLINICAL. J. Mizoe (NIRS, Japan)
") PTCOG 46 Educational Workshop Session IV CLINICAL Head & Neck J. Mizoe (NIRS, Japan) Photon X-Ray γ-ray Fast Neutron Non-Charged Radiation Electron Proton Helium Light Ion Heavy Particle Carbon Neon Argon
PTCOG 46 Educational Workshop Session IV CLINICAL Head & Neck J. Mizoe (NIRS, Japan) Photon X-Ray γ-ray Fast Neutron Non-Charged Radiation Electron Proton Helium Light Ion Heavy Particle Carbon Neon Argon
Partial Breast Irradiation using adaptive MRgRT
 Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
Clinical Commissioning Policy Proposition: Proton Beam Therapy for Cancer of the Prostate
 Clinical Commissioning Policy Proposition: Proton Beam Therapy for Cancer of the Prostate Reference: NHS England B01X09 First published: March 2016 Prepared by NHS England Specialised Services Clinical
Clinical Commissioning Policy Proposition: Proton Beam Therapy for Cancer of the Prostate Reference: NHS England B01X09 First published: March 2016 Prepared by NHS England Specialised Services Clinical
Sarcoma and Radiation Therapy. Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington
 Sarcoma and Radiation Therapy Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington Objective: Helping you make informed decisions Introduction Process Radiation
Sarcoma and Radiation Therapy Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington Objective: Helping you make informed decisions Introduction Process Radiation
Particle Radiation Therapy Using Proton and Heavier Ion Beams Daniela Schulz-Ertner and Hirohiko Tsujii
 VOLUME 25 NUMBER 8 MARCH 10 2007 JOURNAL OF CLINICAL ONCOLOGY R E V I E W A R T I C L E Particle Radiation Therapy Using Proton and Heavier Ion Beams Daniela Schulz-Ertner and Hirohiko Tsujii From the
VOLUME 25 NUMBER 8 MARCH 10 2007 JOURNAL OF CLINICAL ONCOLOGY R E V I E W A R T I C L E Particle Radiation Therapy Using Proton and Heavier Ion Beams Daniela Schulz-Ertner and Hirohiko Tsujii From the
An Update on Radiation Therapy for Prostate Cancer
 An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
Radiotherapy physics & Equipments
 Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Protocol of Radiotherapy for Breast Cancer
 107 年 12 月修訂 Protocol of Radiotherapy for Breast Cancer Indication of radiotherapy Indications for Post-Mastectomy Radiotherapy (1) Axillary lymph node 4 positive (2) Axillary lymph node 1-3 positive:
107 年 12 月修訂 Protocol of Radiotherapy for Breast Cancer Indication of radiotherapy Indications for Post-Mastectomy Radiotherapy (1) Axillary lymph node 4 positive (2) Axillary lymph node 1-3 positive:
SRO Tutorial: Prostate Cancer Clinics
 SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
Combined modality treatment for N2 disease
 Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
Hypofractionated Radiotherapy for breast cancer: Updated evidence
 2 rd Bangladesh Breast Cancer Conference, Dhaka, December 2017 Hypofractionated Radiotherapy for breast cancer: Updated evidence Tabassum Wadasadawala Associate Professor of Radiation Oncology Tata Memorial
2 rd Bangladesh Breast Cancer Conference, Dhaka, December 2017 Hypofractionated Radiotherapy for breast cancer: Updated evidence Tabassum Wadasadawala Associate Professor of Radiation Oncology Tata Memorial
Potential benefits of intensity-modulated proton therapy in head and neck cancer van de Water, Tara Arpana
 University of Groningen Potential benefits of intensity-modulated proton therapy in head and neck cancer van de Water, Tara Arpana IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's
University of Groningen Potential benefits of intensity-modulated proton therapy in head and neck cancer van de Water, Tara Arpana IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: charged_particle_radiotherapy 3/12/96 5/2017 5/2018 5/2017 Description of Procedure or Service Charged-particle
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: charged_particle_radiotherapy 3/12/96 5/2017 5/2018 5/2017 Description of Procedure or Service Charged-particle
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Proton Therapy for Prostate Cancer. Andrew K. Lee, MD, MPH Director Proton Therapy Center
 Proton Therapy for Prostate Cancer Andrew K. Lee, MD, MPH Director Proton Therapy Center Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments
Proton Therapy for Prostate Cancer Andrew K. Lee, MD, MPH Director Proton Therapy Center Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments
PROTON BEAM RADIATION THERAPY
 PROTON BEAM RADIATION THERAPY UnitedHealthcare Commercial Medical Policy Policy Number: 2019T0132AA Effective Date: January 1, 2019 Instructions for Use Table of Contents Page COVERAGE RATIONALE... 1 DEFINITIONS...
PROTON BEAM RADIATION THERAPY UnitedHealthcare Commercial Medical Policy Policy Number: 2019T0132AA Effective Date: January 1, 2019 Instructions for Use Table of Contents Page COVERAGE RATIONALE... 1 DEFINITIONS...
2/14/09. Why Discuss this topic? Managing Local Recurrences after Radiation Failure. PROSTATE CANCER Second Treatment
 Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Hypofractionation in particle therapy. Marco Durante
 Hypofractionation in particle therapy Marco Durante 29.04.2014 Radiosurgery (SBRT): the new frontier in stereotactic imageguided radiotherapy Stage I (T1N0M0) NSCLC Oligometastases Hepatocellular carcinoma
Hypofractionation in particle therapy Marco Durante 29.04.2014 Radiosurgery (SBRT): the new frontier in stereotactic imageguided radiotherapy Stage I (T1N0M0) NSCLC Oligometastases Hepatocellular carcinoma
Dose escalation for NSCLC using conformal RT: 3D and IMRT. Hasan Murshed
 Dose escalation for NSCLC using conformal RT: 3D and IMRT. Hasan Murshed Take home message Preliminary data shows CRT technique in NSCLC allows dose escalation to an unprecedented level maintaining cancer
Dose escalation for NSCLC using conformal RT: 3D and IMRT. Hasan Murshed Take home message Preliminary data shows CRT technique in NSCLC allows dose escalation to an unprecedented level maintaining cancer
25 Years of Proton Radiation Therapy at PSI an Overview
 25 Years of Proton Radiation Therapy at PSI an Overview Gudrun Goitein for the Team of the Center for Proton Therapy Center for Proton Therapy Paul Scherrer Institut (www.psi.ch) 5232 Villigen PSI Switzerland
25 Years of Proton Radiation Therapy at PSI an Overview Gudrun Goitein for the Team of the Center for Proton Therapy Center for Proton Therapy Paul Scherrer Institut (www.psi.ch) 5232 Villigen PSI Switzerland
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
Therapy of Non-Operable early stage NSCLC
 SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
Clinical Proton Radiation Therapy Research at the Francis H. Burr Proton Therapy Center
 Technology in Cancer Research and Treatment ISSN 1533-0346 Volume 6, Number 4 Supplement, August 2007 Adenine Press (2007) Clinical Proton Radiation Therapy Research at the Francis H. Burr Proton Therapy
Technology in Cancer Research and Treatment ISSN 1533-0346 Volume 6, Number 4 Supplement, August 2007 Adenine Press (2007) Clinical Proton Radiation Therapy Research at the Francis H. Burr Proton Therapy
Systematic Review of Brachytherapy & Proton Beam Therapy for Low-Risk Prostate Cancer: Preliminary Findings
 Systematic Review of Brachytherapy & Proton Beam Therapy for Low-Risk Prostate Cancer: Preliminary Findings May 28, 2008 Dan Ollendorf, MPH, ARM Chief Review Officer Systematic Review Objectives To compare
Systematic Review of Brachytherapy & Proton Beam Therapy for Low-Risk Prostate Cancer: Preliminary Findings May 28, 2008 Dan Ollendorf, MPH, ARM Chief Review Officer Systematic Review Objectives To compare
Radiation Oncology MOC Study Guide
 Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
IEHP UM Subcommittee Approved Authorization Guidelines Proton Beam Radiation Therapy for Prostate Cancer
 Policy: The use of Proton Beam Therapy (PBT) in Prostate cancer has not been established as more effective than other forms of External Beam Radiation Therapies (EBRT s), such as Intensity Modulated Radiation
Policy: The use of Proton Beam Therapy (PBT) in Prostate cancer has not been established as more effective than other forms of External Beam Radiation Therapies (EBRT s), such as Intensity Modulated Radiation
Future of Radiation Therapy
 Future of Radiation Therapy JP Morgan Healthcare Conference January 12, 2016 Deepak Khuntia, MD, VP of Medical Affairs Patrick Kupelian, MD, VP of Clinical Affairs Cancer as a cause of death CANCER TREATMENT
Future of Radiation Therapy JP Morgan Healthcare Conference January 12, 2016 Deepak Khuntia, MD, VP of Medical Affairs Patrick Kupelian, MD, VP of Clinical Affairs Cancer as a cause of death CANCER TREATMENT
Proton or Photon RT for Retroperitoneal Sarcomas
 Principle Investigator Thomas F. DeLaney, M.D. Contact Additional Info Institution Thomas DeLaney, MD 617-726-6876 tdelaney@partners.org www.clinicaltrials.gov NCT01659203 Massachusetts General Hospital
Principle Investigator Thomas F. DeLaney, M.D. Contact Additional Info Institution Thomas DeLaney, MD 617-726-6876 tdelaney@partners.org www.clinicaltrials.gov NCT01659203 Massachusetts General Hospital