Brain metastases: changing visions
|
|
|
- Joella Phoebe Stokes
- 5 years ago
- Views:
Transcription

1 Brain metastases: changing visions Roberto Spiegelmann, MD Baiona, 2014 Head, Stereotactic Radiosurgery Unit Dept of Neurosurgery, Chaim Sheba Medical Center Tel Hashomer, Israel
2 The best current estimate is that brain metastases occur in at least 6% of all cancer patients. The proportion ranges from less than 1% in thyroid, liver, stomach, prostate, uterine or ovarian cancers, to 20% in lung cancer. Based on this estimate, metastatic brain tumors are thought to outnumber primary malignant brain tumors by at least three to one. Davis FG, Dolecek TA, McCarthy BJ, et al. Neuro-Oncology 2012;14(9):

:1781-8 Most common intracranial tumor Annual")
3 Other sources estimate that 24-45% of all cancer patients have brain metastases. Nussbaum ES, Djalilian HR, Cho KH, Hall WA. Cancer. 1996;78(8): Most common intracranial tumor Annual incidence 8.3/ Up to 50%will die as a direct result of them
4 Lung (50% of all metastases) Breast (most frequent source in women) Melanoma (40-60% of melanoma patients develop brain mets) Colon Kidney
5 Median Survival 1 month with no therapy 2 months with steroids 11 months with all we have
6 Surgery Radiosurgery Whole Brain RT
7 Surgery Immediate relief of site-related deficit fast resolution of edema
8 surgery large lesion with brain shift unknown diagnosis/accessible lesion obstruction of CSF pathways severe edema with neuro deficit
9 Surgery Technically straightforward: Clear delimitation from normal brain tissue Accessibility Stereotaxis/Neuronavigation minimize access trauma


10 Surgical limitations > 50% of patients are not candidates for surgery: tumor inaccessibility Tumor multiplicity extensive systemic disease
11 tissue manipulation scarring functional deterioration neural muscular-skeletal


12 Surgery Infection Bleeding Seeding
13 radiosurgery

14 Israel, 1993
15 Radiosurgery Troublesome definition of tumor control



16 Recurrence vs Radiation injury Confusion between both continues to compromise result assessment
17 Clinical Neurosurgery Volume 57, 2010
18

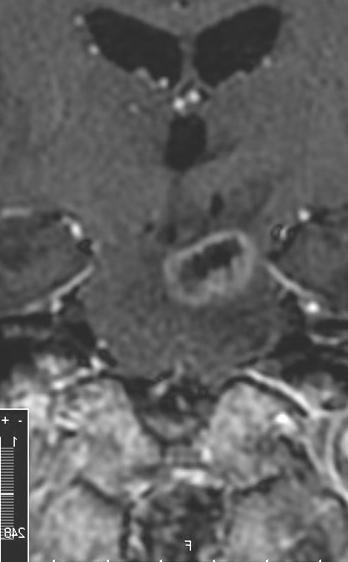
19 Recidive or radiation injury?
 rigid/elastic co-registration and intensity-variation")

20 Delayed Contrast Extravasation MRI Treatment Response Assessment Maps (TRAMs) Method a) 2 series of T1-MRI: 2 & 75 min post contrast injection b) rigid/elastic co-registration and intensity-variation corrections c) early (2 min) images subtracted from late (75 min) images 75 min Gd 2 min Gd TRAM Blue = tumor tissue, efficient Gd clearance at 75 min Red = non tumor tissue, Gd accumulation at 75 min 2 0

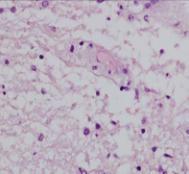
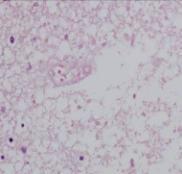
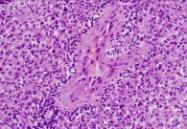
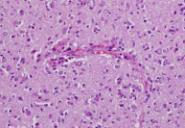
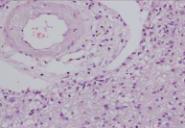
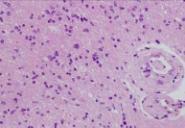
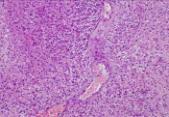
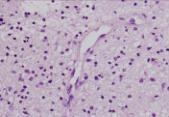
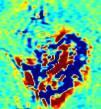
21 Delayed Contrast Extravasation MRI: The Rationale A B C Blue/tumor: Morphologically, the vessel lumens are undamaged resulting in efficient contrast clearance D E F G H I Red/non-tumoral: Morphologically, vessels present significantly damaged lumens resulting in Gd accumulation 2 1


22 Delayed Contrast Extravasation MRI: Histological Validation Red = non-tumoral tissues: Blue = morphologically active tumor: validated by 44 histological samples 2
23 Surgery or radiosurgery?
24 radiosurgery deficit reversed by steroids asymptomatic mets
25 WBRT The classic approach to patients with multiple foci
26 Whole Brain Radiation Hair loss Acute mental effects Delayed diffuse brain cell injury Marginal effect upon frequent tumors: melanoma Renal Cells Carcinoma
27 Dose/efficacy Clinical situation Cure radiosensitive tumors (germinoma, lymphoma) Required dose 24 to 36 Gy 90% chance of controlling microscopic cancer 45 to 55 Gy 90% chance of curing a 1-cm squamous cancer 66 Gy A 1-cm lesion requires 66 Gy for local control.
28 In a series of lung cancer patients with brain mets surviving more than 1 year, 36 of 37 treated with WBRT had leukoencephalopathy compared with Only 1 of 31 who had radiosurgery alone Monaco EA, Faraji AH, Berkowitz O, et al, Cancer. 2013:
29 Hippocampal sparing
30 WBRT Not curative MMSE deterioration in long term less incidence of new brain disease in the short term New disease generates MMSE deterioration
31 WBRT can only affect contemporary overt or occult disease
32 Mix and Match Surgery + Radiosurgery Surgery + WBRT Radiosurgery + WBRT
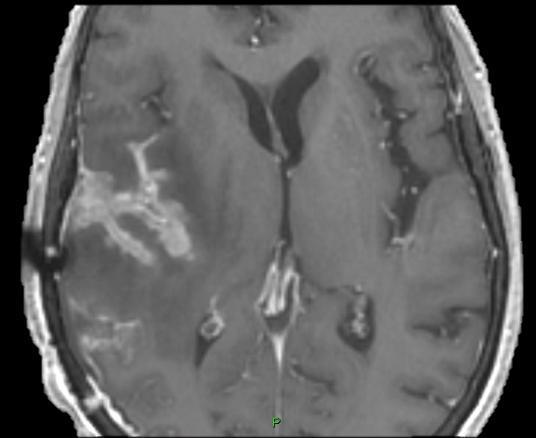
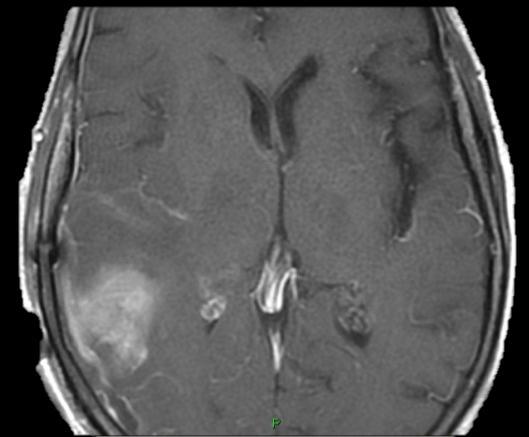
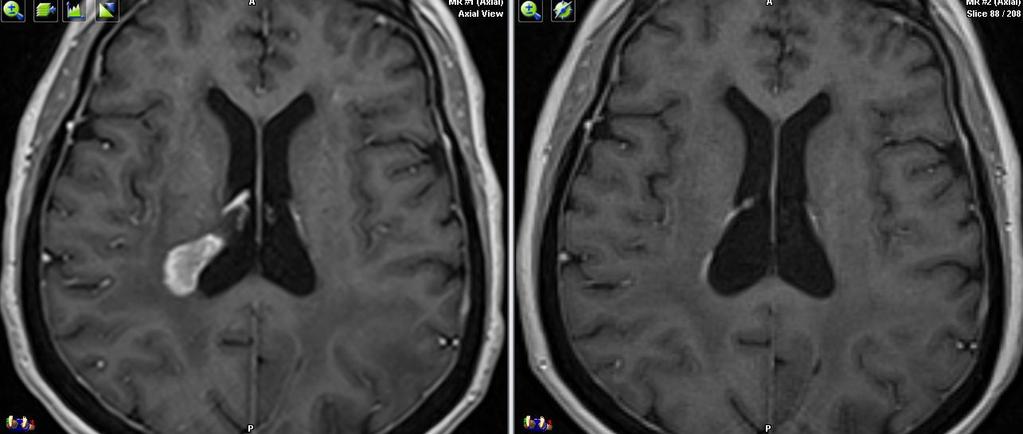
33 Strange bed partners Radiosurgery in tumor bed after Surgery Is it worth?
34
35
36
37
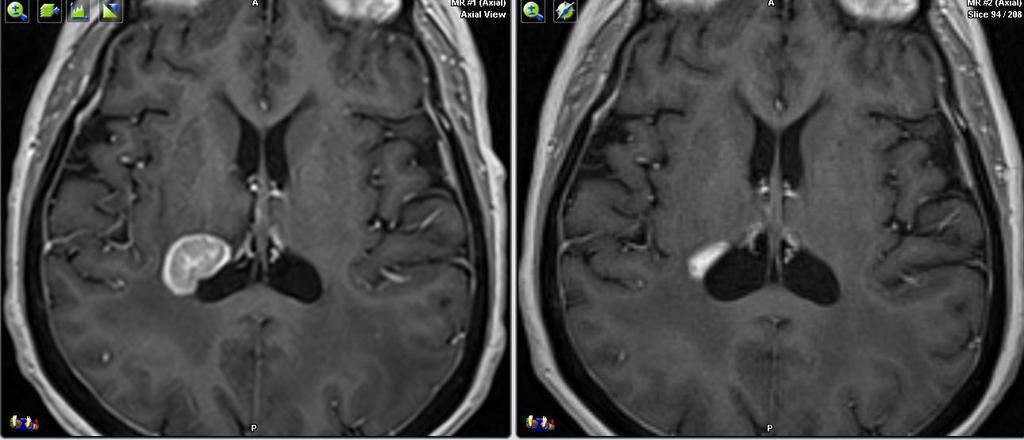
38 Radiosurgery after Surgery Where is the residual tumor in the tumor bed?
39 Radiosurgery after Surgery When residual is obvious
")
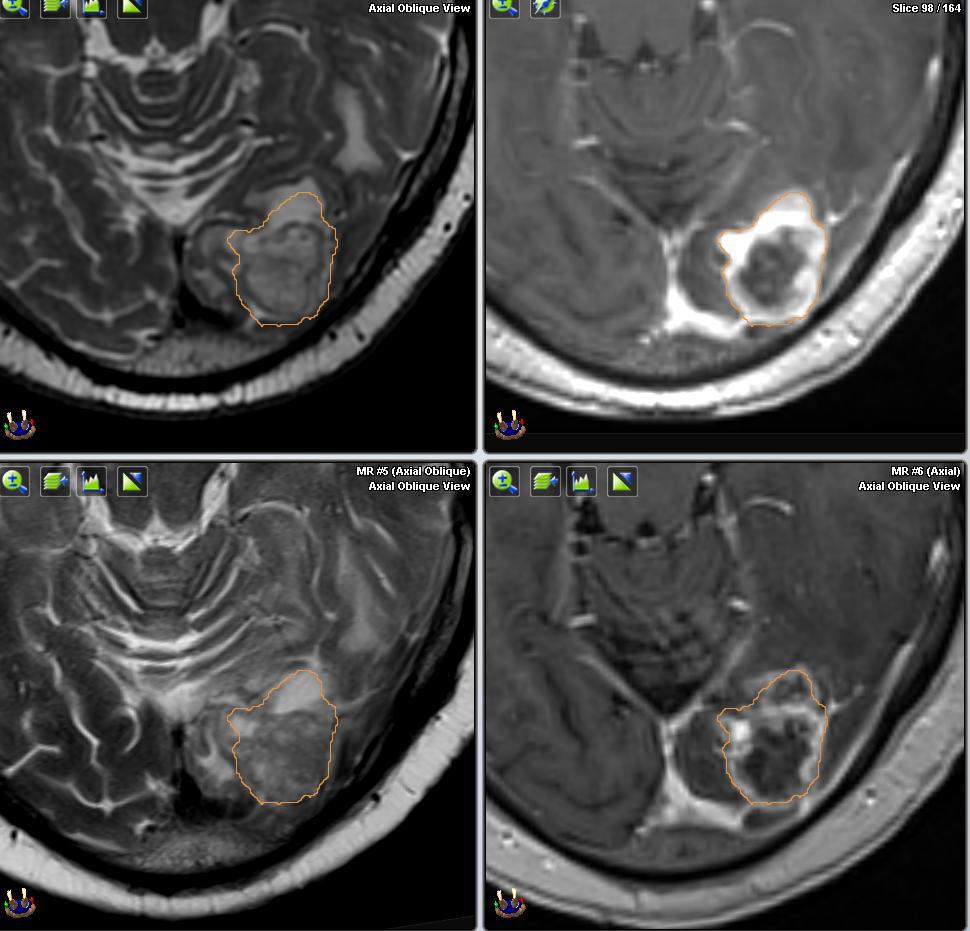
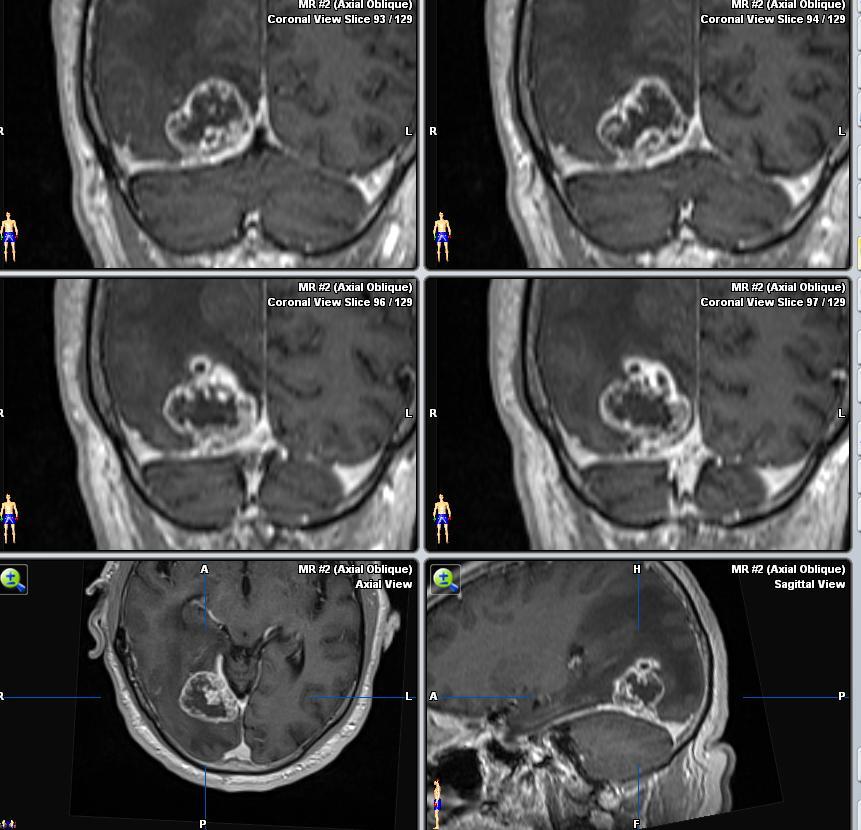
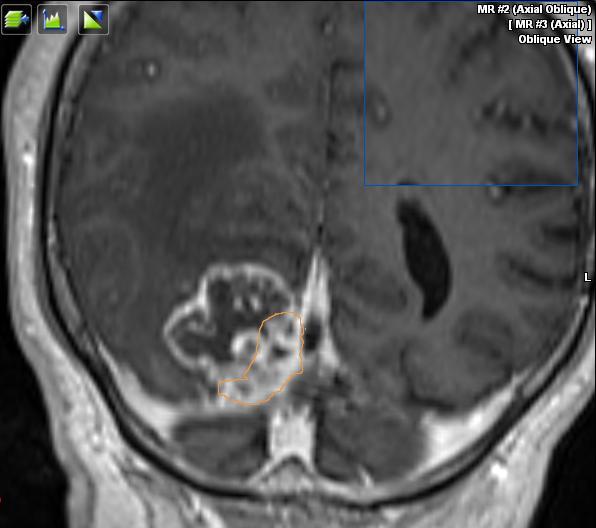
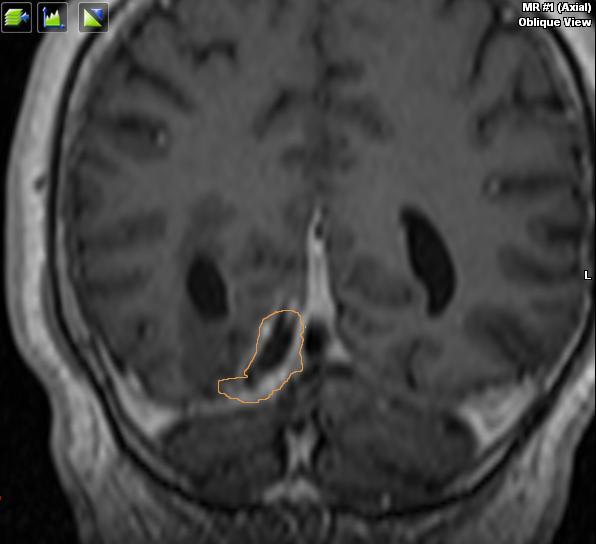
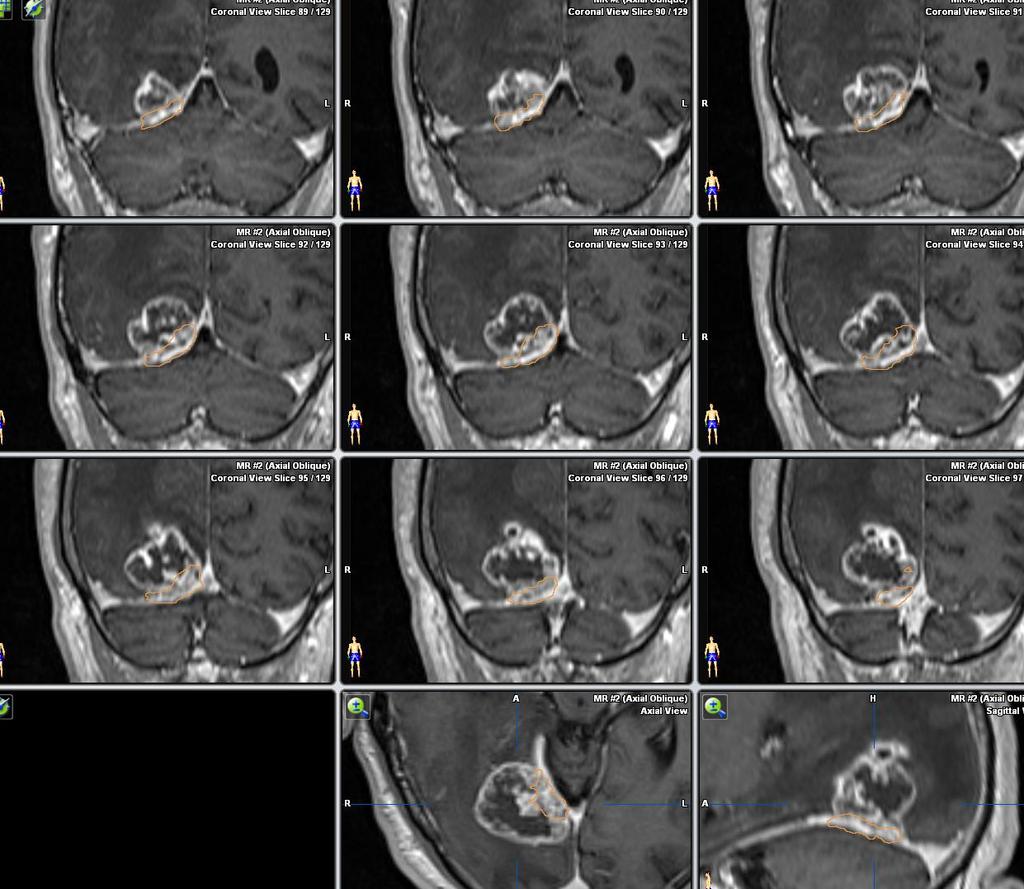
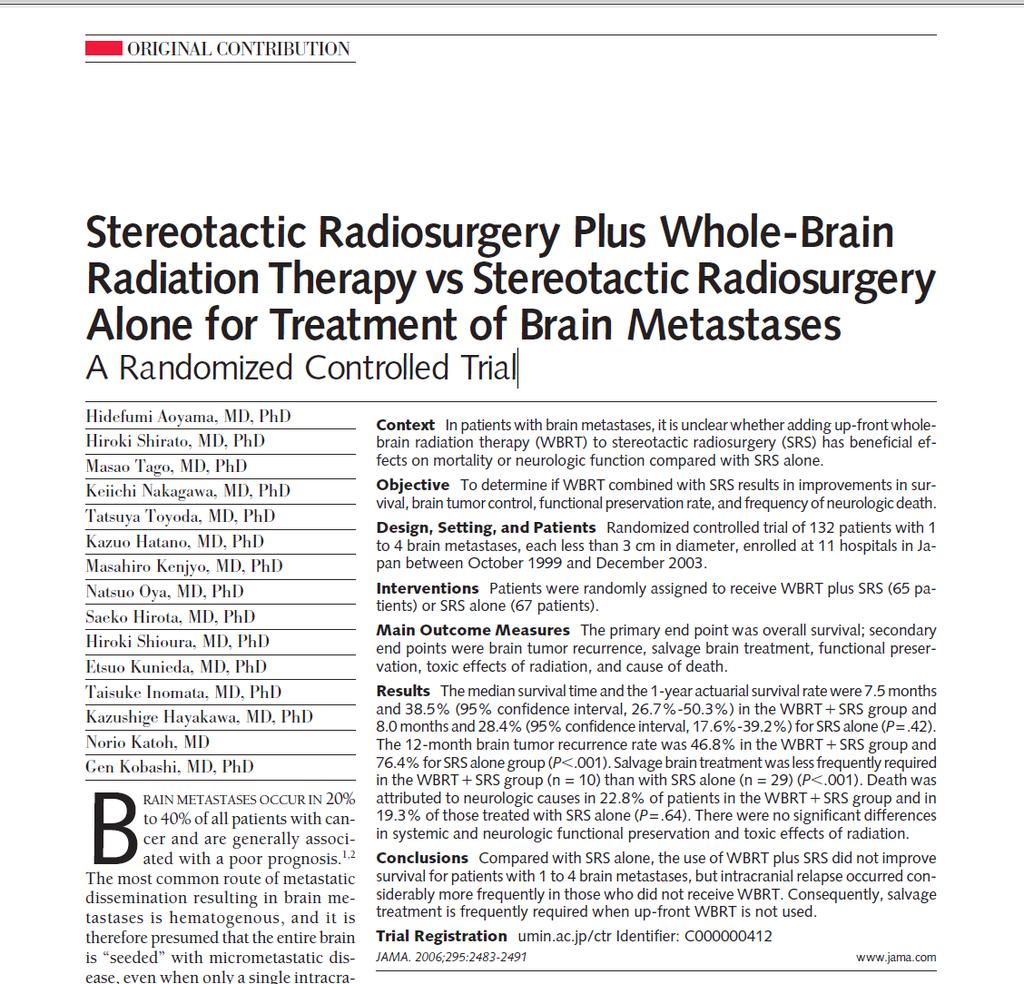
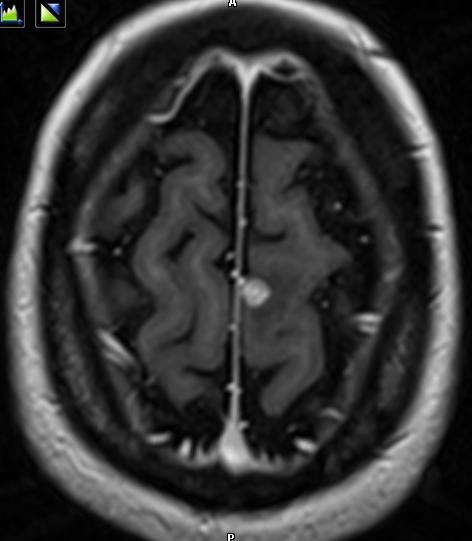
40 Cystic metastasis A cystic metastasis in eloquent brain is a major challenge for total (oncological) removal
41 Cystic metastases are tricky collapse once opened thin layer of tumor cells difficult to remove without poking the surrounding tissue When in eloquent area, this may result in functional damage/residual tumor islands left behind
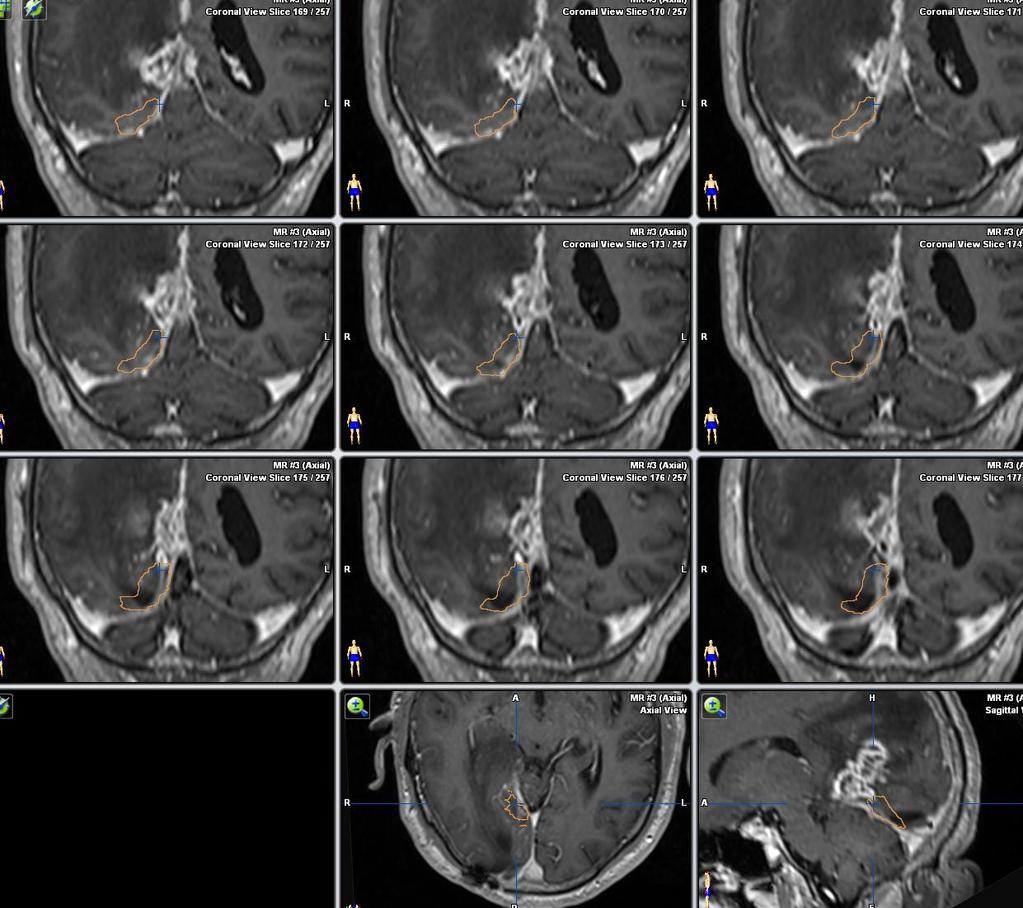
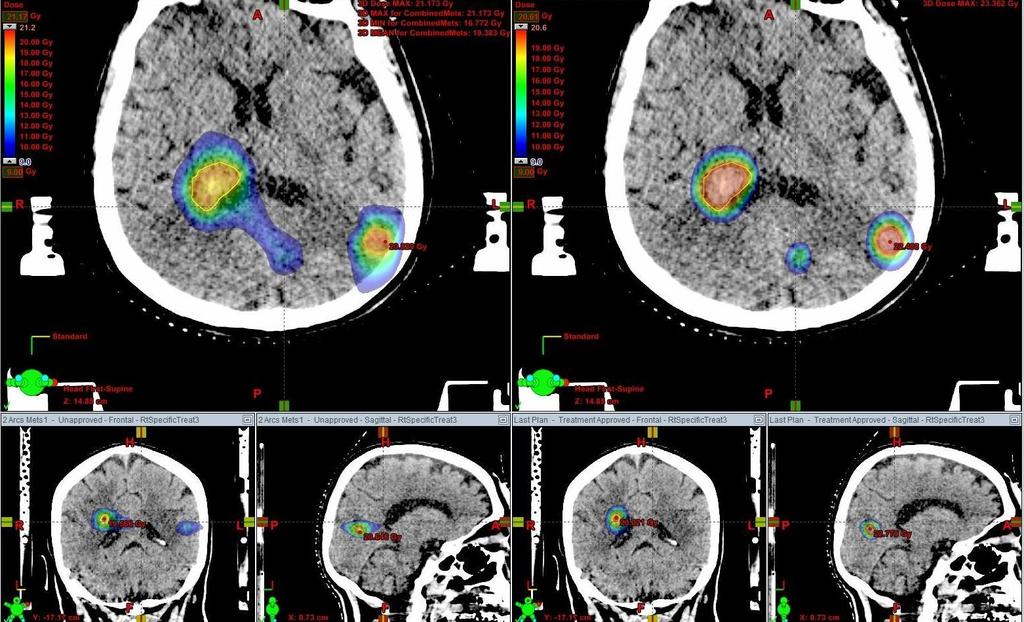
42 Radiosurgery for cystic mets irradiating water large area of irradiation: high comp risk
43 combine Drain the cyst Irradiate residual tumor



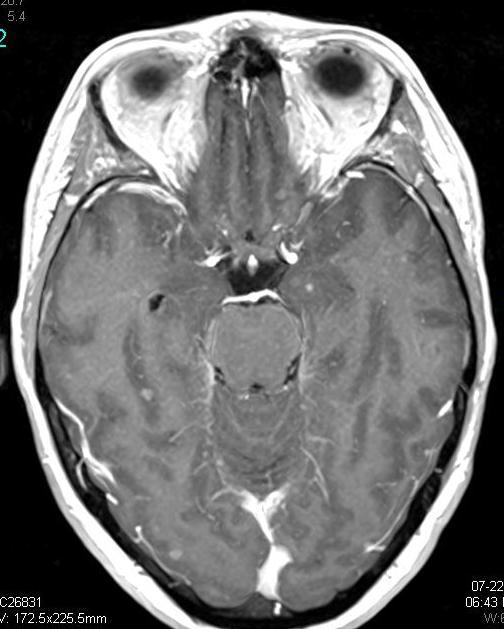
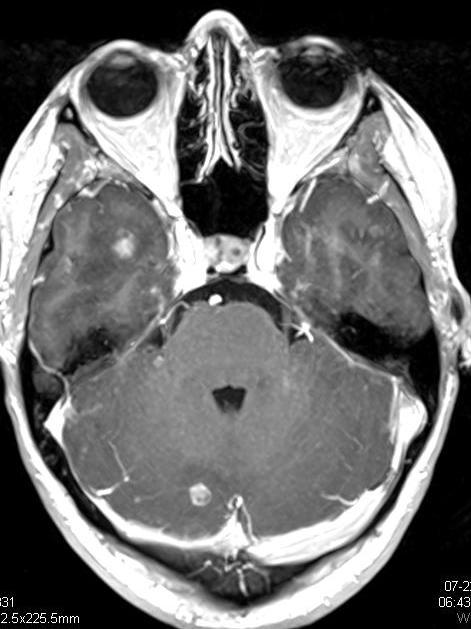
44 At presentation 62 y old. NSCCa lung Left hemiparesis Focal seizures Post Ommaya aspiration 18 months post radiosurgery

45 05/01/ /01/ /05/2009
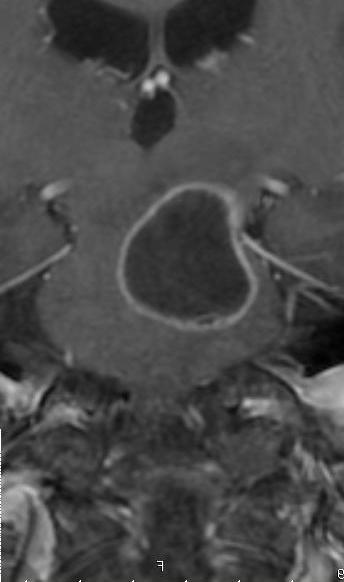
46 05/01/ /05/2009
47 Radiosurgery and whole brain radiation
48 Local Control with SRS Boost Study WBRT + SRS P value When RTOG 71% 82%.01 1yr Tufts 87% 91% NS? Pittsburgh 8% 100% yr
49
50 Relapse After Radiosurgery Recurrence RS without RT (67) RS + RT (65) Relative Risk P-value Local bed 30% 14% 1.2 <.0001 Distant brain 52% 18% 1.7 <.0001 Note: Local failure at 1 year, distant brain failure at 6 months Withholding WBRT significantly increases relapse in the brain and locally. Aoyama, JAMA 2006
51 troublesome definitions Local tumor progression was defined as a radiographic increase of 25% or more in the size of a metastatic lesion If an MRI result showed central or heterogeneous low intensity and if the lesion size decreased on serial studies, brain necrosis was scored
52 ends meet Death was attributed to neurologic causes in 22.8% in the WBRT/SRS group and in 19.3% in the SRS-alone group The median survival time was 7.5 months with WBRT/SRS and 8.0 months with SRS alone.
53 take home Although surgery and SRS are both focal treatments, SRS is less invasive and may be repeated more often than surgical intervention early detection of a brain recurrence and early salvage brain treatment may prevent neurologic deterioration and neurologic death, even when WBRT is not included in the initial treatment.
54 SRS alone without upfront WBRT was associated with increased brain tumor recurrence; however, it did not result in worsened neurologic function or increased risk of neurologic death. Therefore, SRS alone could be a treatment option, provided that frequent monitoring of brain tumor status is conducted
55 The main reason we still do it is that RS for multiple simultaneous foci is cumbersome, lengthy, and costly
56 Masaaki Yamamoto, et al, Lancet Oncol 2014; 15: We aimed to examine whether stereotactic radiosurgery without whole-brain radiotherapy (WBRT) as the initial treatment for patients with five to ten brain metastases is non-inferior to that for patients with two to four brain metastases in terms of overall survival. Standard stereotactic radiosurgery procedures were used in all patients; tumor volumes smaller than 4 ml were irradiated with 22 Gy at the lesion periphery and those that were 4 10 ml with 20 Gy. The primary endpoint was overall survival, for which the non-inferiority margin for the comparison of outcomes in patients with two to four brain metastases with those of patients with fi ve to ten brain metastases was set as the value of the upper 95% CI for a hazard ratio (HR) of 1 30, and all data were analysed by intention to treat. The study was finalised on Dec 31, 2012, for analysis of the primary endpoint; however, monitoring of stereotactic radiosurgery-induced complications and neurocognitive function assessment will continue for the censored subset until the end of2014. We enrolled 1194 eligible patients between March 1, 2009, and Feb 15, Median overall survival after stereotactic radiosurgery was 13 9 months [95% CI ] in the 455 patients with one tumor, 10 8 months [ ] in the 531 patients with two to four tumors, and 10 8 months [ ] in the 208 patients with five to ten tumors. Overall survival did not differ between the patients with two to four tumors and those with five to ten (HR 0 97, 95% CI [less than non-inferiority margin], p=0 78; pnon-inferiority<0 0001). Stereotactic radiosurgeryinduced adverse events occurred in 101 (8%) patients; nine (2%) patients with one tumor had one or more grade 3 4 event compared with 13 (2%) patients with two to four tumors and six (3%) patients with five to ten tumors.
57 The proportion of patients who had one or more treatment-related adverse event of any grade did not differ significantly between the two groups of patients with multiple tumors (50 [9%] patients with two to four tumors vs 18 [9%] with five to ten; p=0 89). Four patients died, mainly of complications relating to stereotactic radiosurgery (two with one tumor and one each in the other two groups). Our results suggest that stereotactic radiosurgery without WBRT in patients with five to ten brain metastases is non-inferior to that in patients with two to four brain metastases. Considering the minimal invasiveness of stereotactic radiosurgery and the fewer side-effects than with WBRT, stereotactic radiosurgery might be a suitable alternative for patients with up to ten brain metastases.
58 Baschnagel AM, Meyer KD, Chen PY, et al. J Neurosurg. 2013: patients with 1 to 14 brain metastases initially managed with radiosurgery alone. The 1-year local control rate was 92%, and the median time to distant brain failure was 8 months. Total tumor volume was a better predictor of overall survival than number of brain metastases and a better predictor of distant brain failure and even local brain tumor control..
59 Instead of WBRT Follow up closely Increase imaging diagnostic power Salvage radiosurgery for new mets
60 need Better tools for multiple metastases radiosurgery

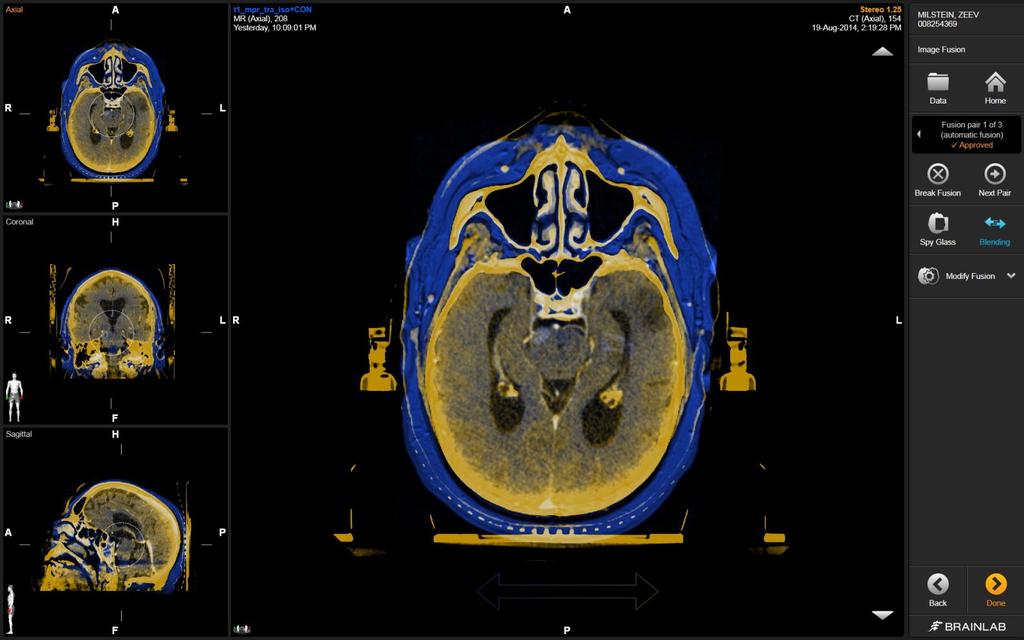
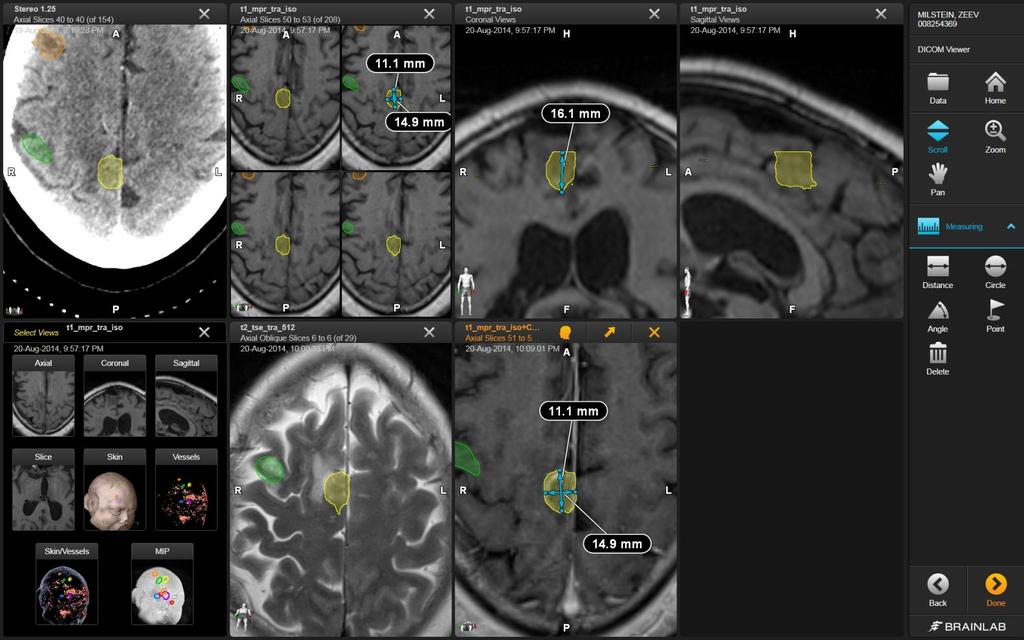
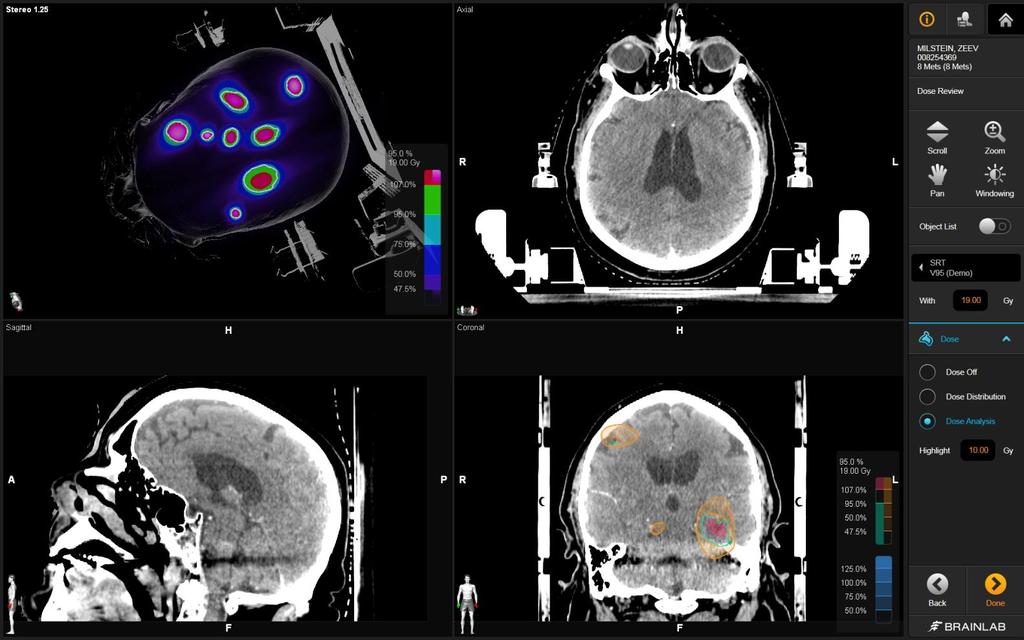
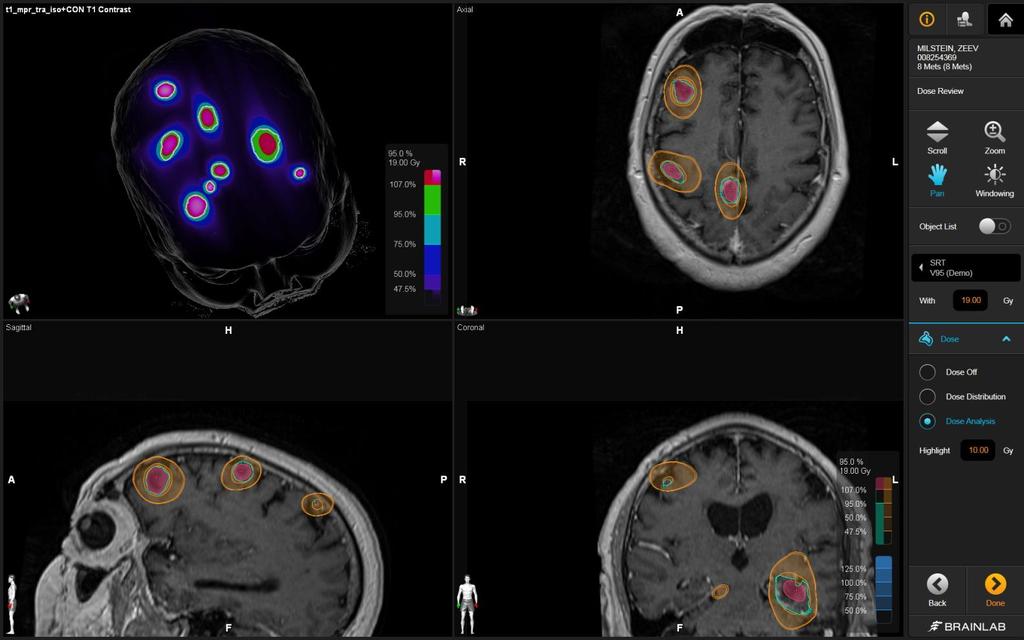
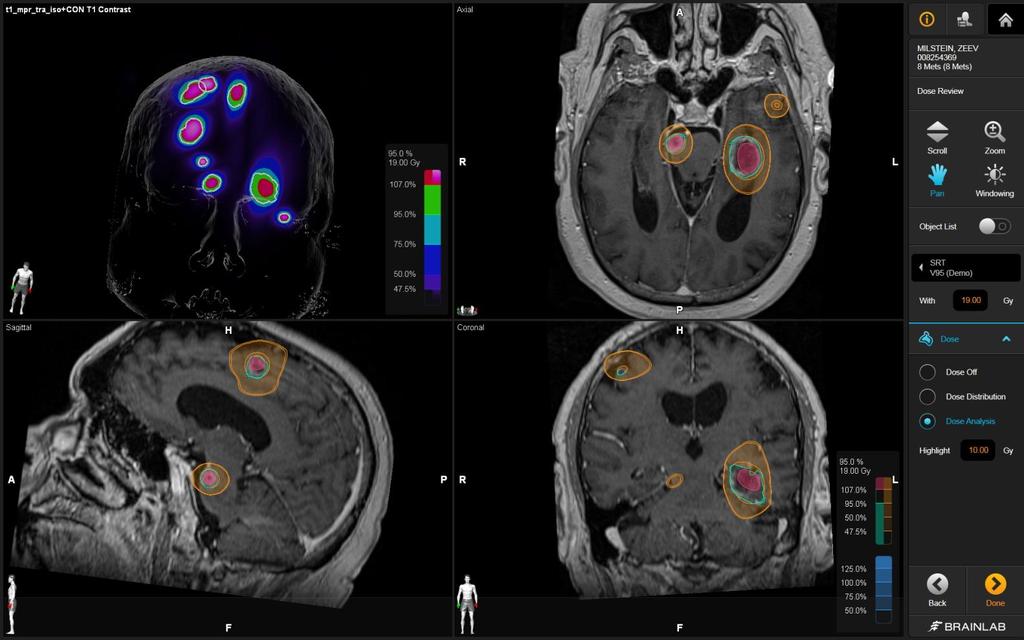
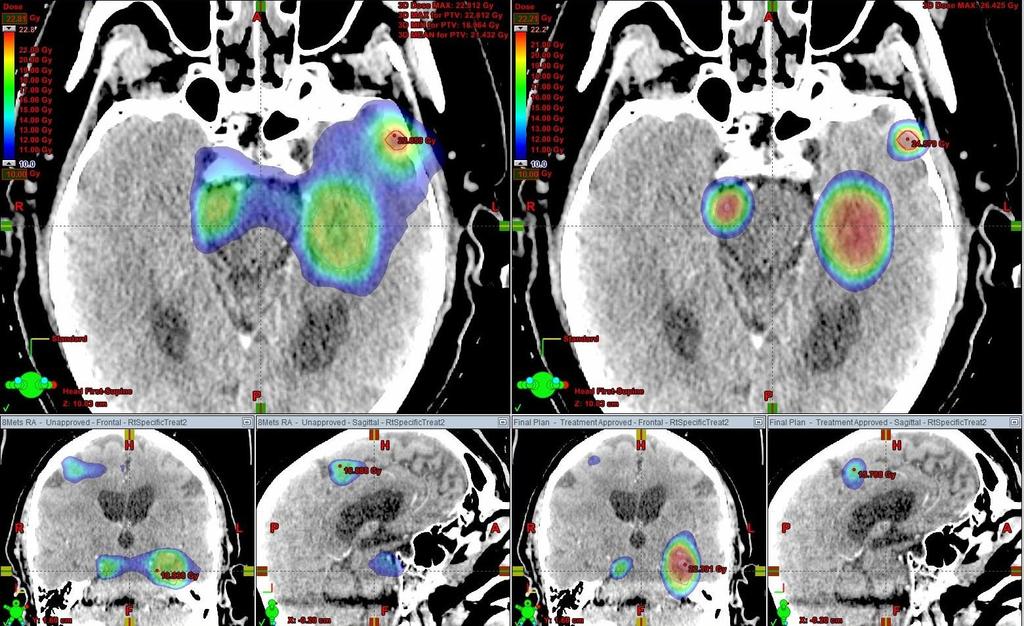
61 Multiple Mets Treament Module

62 Brainlab multiple mets module Image-based non stereotactic (CT with mask, no stereo localizer)
63
64
65

66
67
68
69
70
71 8 mets Planning time: 20 Total treatment time: 20 Total beam-on time: 6
72 So far 5 patients 8 mets 5 mets 4 mets (2) 3 mets No acute toxicity
73
74
75
76 ra mbmm
77 ra mbmm
78 Relative Volume (%) 4 Mets 22 Gy Brain Metastases vs. RapidArc 100 Brain RA Rt occipital RA Fronto Polar RA 80 Lt Parietal RA Lt Cerebellar RA Brain 60 Rt Occipital Fronto Polar Lt Parietal 40 Lt Cerebellar Dose (Gy)
79 A requiem for whole brain radiotherapy?
80 Radiosurgery for multiple brain mets Logistical and technical barriers are down Strong rationale Cost efficient Effective
Minesh Mehta, Northwestern University. Chicago, IL
 * Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
* Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms. Overall Clinical Significance 8/3/13
 Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Selecting the Optimal Treatment for Brain Metastases
 Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015
 Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015 Most common brain tumor, affecting 8.5-15% of cancer patients. Treatment options: Whole brain radiation
Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015 Most common brain tumor, affecting 8.5-15% of cancer patients. Treatment options: Whole brain radiation
Optimal Management of Isolated HER2+ve Brain Metastases
 Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey
 Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Management of Brain Metastases Dr. Luis Souhami Professor Department of Radiation Oncology University,
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Management of Brain Metastases Dr. Luis Souhami Professor Department of Radiation Oncology University,
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Is it cost-effective to treat brain metastasis with advanced technology?
 Is it cost-effective to treat brain metastasis with advanced technology? Cost-effectiveness analysis of whole brain RT, stereotactic radiosurgery and craniotomy in HA setting Lam, Tai-Chung, Choi CW Horace,
Is it cost-effective to treat brain metastasis with advanced technology? Cost-effectiveness analysis of whole brain RT, stereotactic radiosurgery and craniotomy in HA setting Lam, Tai-Chung, Choi CW Horace,
We have previously reported good clinical results
 J Neurosurg 113:48 52, 2010 Gamma Knife surgery as sole treatment for multiple brain metastases: 2-center retrospective review of 1508 cases meeting the inclusion criteria of the JLGK0901 multi-institutional
J Neurosurg 113:48 52, 2010 Gamma Knife surgery as sole treatment for multiple brain metastases: 2-center retrospective review of 1508 cases meeting the inclusion criteria of the JLGK0901 multi-institutional
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia
 for Brain Metastasis in Nova Scotia") A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia Gaurav Bahl, Karl Tennessen, Ashraf Mahmoud-Ahmed, Dorianne Rheaume, Ian Fleetwood,
A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia Gaurav Bahl, Karl Tennessen, Ashraf Mahmoud-Ahmed, Dorianne Rheaume, Ian Fleetwood,
Place of tumor bed radiosurgery and focal radiotherapy following resec7on of brain metastases: A new paradigm Lucyna Kepka
 Place of tumor bed radiosurgery and focal radiotherapy following resec7on of brain metastases: A new paradigm Lucyna Kepka Department of Radia7on Oncology; M. Sklodowska- Curie Memorial Cancer Center and
Place of tumor bed radiosurgery and focal radiotherapy following resec7on of brain metastases: A new paradigm Lucyna Kepka Department of Radia7on Oncology; M. Sklodowska- Curie Memorial Cancer Center and
Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen?
 Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Hong Kong Hospital Authority Convention 2018
 Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Treating Multiple. Brain Metastases (BM)
") ESTRO 36 5-9 May 2017, Vienna Austria, Accuray Symposium Treating Multiple Brain Metastases (BM) with CyberKnife System Frederic Dhermain MD PhD, Radiation Oncologist Gustave Roussy University Hospital,
ESTRO 36 5-9 May 2017, Vienna Austria, Accuray Symposium Treating Multiple Brain Metastases (BM) with CyberKnife System Frederic Dhermain MD PhD, Radiation Oncologist Gustave Roussy University Hospital,
ARROCase Brain Metastases
 ARROCase Brain Metastases Colin Hill*, Daniel M. Trifiletti*, Timothy N. Showalter*, Jason P. Sheehan Radiation Oncology* and Neurosurgery University of Virginia Charlottesville, VA Case: HPI 64 year old
ARROCase Brain Metastases Colin Hill*, Daniel M. Trifiletti*, Timothy N. Showalter*, Jason P. Sheehan Radiation Oncology* and Neurosurgery University of Virginia Charlottesville, VA Case: HPI 64 year old
Radiotherapy and Brain Metastases. Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem
 Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
Palliative radiotherapy in lung cancer
 New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
Surgery for recurrent brain metastases
 Surgery for recurrent brain metastases Pr Philippe METELLUS Neurosurgeon, Clairval Hospital Center, Marseille 8th Annual Brain Metastases Research and Emerging Therapy Conference September 21st, 2018 Conflict
Surgery for recurrent brain metastases Pr Philippe METELLUS Neurosurgeon, Clairval Hospital Center, Marseille 8th Annual Brain Metastases Research and Emerging Therapy Conference September 21st, 2018 Conflict
Evidence Based Medicine for Gamma Knife Radiosurgery. Metastatic Disease GAMMA KNIFE SURGERY
 GAMMA KNIFE SURGERY Metastatic Disease Evidence Based Medicine for Gamma Knife Radiosurgery Photos courtesy of Jean Régis, Timone University Hospital, Marseille, France Brain Metastases The first report
GAMMA KNIFE SURGERY Metastatic Disease Evidence Based Medicine for Gamma Knife Radiosurgery Photos courtesy of Jean Régis, Timone University Hospital, Marseille, France Brain Metastases The first report
State of the Art Radiotherapy for Pediatric Tumors. Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center
 State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
Management of single brain metastasis: a practice guideline
 PRACTICE GUIDELINE SERIES Management of single brain metastasis: a practice guideline A. Mintz MD,* J. Perry MD, K. Spithoff BHSc, A. Chambers MA, and N. Laperriere MD on behalf of the Neuro-oncology Disease
PRACTICE GUIDELINE SERIES Management of single brain metastasis: a practice guideline A. Mintz MD,* J. Perry MD, K. Spithoff BHSc, A. Chambers MA, and N. Laperriere MD on behalf of the Neuro-oncology Disease
Neurosurgical Management of Brain Tumours. Nicholas Little Neurosurgeon RNSH
 Neurosurgical Management of Brain Tumours Nicholas Little Neurosurgeon RNSH General Most common tumours are metastatic 10x more common than primary Incidence of primary neoplasms is 20 per 100000 per year
Neurosurgical Management of Brain Tumours Nicholas Little Neurosurgeon RNSH General Most common tumours are metastatic 10x more common than primary Incidence of primary neoplasms is 20 per 100000 per year
Update on management of metastatic brain disease. Peter Hoskin Mount Vernon Cancer Centre Northwood UK
 Update on management of metastatic brain disease Peter Hoskin Mount Vernon Cancer Centre Northwood UK Incidence 15-30% of patients with solid tumours will develop brain metastases Most common primary sites
Update on management of metastatic brain disease Peter Hoskin Mount Vernon Cancer Centre Northwood UK Incidence 15-30% of patients with solid tumours will develop brain metastases Most common primary sites
Where are we with radiotherapy for biliary tract cancers?
 Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Update on Pediatric Brain Tumors
 Update on Pediatric Brain Tumors David I. Sandberg, M.D. Director of Pediatric Neurosurgery & Associate Professor Dr. Marnie Rose Professorship in Pediatric Neurosurgery Pre-talk Questions for Audience
Update on Pediatric Brain Tumors David I. Sandberg, M.D. Director of Pediatric Neurosurgery & Associate Professor Dr. Marnie Rose Professorship in Pediatric Neurosurgery Pre-talk Questions for Audience
Outline. WBRT field. Brain Metastases. Whole Brain RT Prophylactic WBRT Stereotactic radiosurgery (SRS) 1 fraction Stereotactic frame
 1 fraction Stereotactic frame") Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
CONTINUING PROFESSIONAL DEVELOPMENT
 23/09/15 POSTGRADUATE SCHOOL OF MEDICINE BRAIN METASTASES Prof M Brada and Dr John Green MDSC156/199: Acute Clinical Oncology A MEMBER OF THE RUSSELL GROUP CONTINUING PROFESSIONAL DEVELOPMENT Brain Metastases
23/09/15 POSTGRADUATE SCHOOL OF MEDICINE BRAIN METASTASES Prof M Brada and Dr John Green MDSC156/199: Acute Clinical Oncology A MEMBER OF THE RUSSELL GROUP CONTINUING PROFESSIONAL DEVELOPMENT Brain Metastases
Overview: Immunotherapy in CNS Metastases
 Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
When is local surgery indicated in metastatic breast cancer?
 When is local surgery indicated in metastatic breast cancer? NICOLA ROCHE THE ROYAL MARSDEN HOSPITAL IBCS 2018 Stage at diagnosis 2014 Survival with Stage IV breast cancer Hypothesis Surgical removal of
When is local surgery indicated in metastatic breast cancer? NICOLA ROCHE THE ROYAL MARSDEN HOSPITAL IBCS 2018 Stage at diagnosis 2014 Survival with Stage IV breast cancer Hypothesis Surgical removal of
Protocolos de consenso: MTS Cerebrales Resumen ASTRO. Javier Aristu y Germán Valtueña Servicio Oncología Rad. Depart.
 Protocolos de consenso: MTS Cerebrales Resumen ASTRO Javier Aristu y Germán Valtueña Servicio Oncología Rad. Depart. ASTRO 2013 Brain met SRS Abstracts 97. Comparative Effectiveness of SRS versus WBRT
Protocolos de consenso: MTS Cerebrales Resumen ASTRO Javier Aristu y Germán Valtueña Servicio Oncología Rad. Depart. ASTRO 2013 Brain met SRS Abstracts 97. Comparative Effectiveness of SRS versus WBRT
Survival and Intracranial Control of Patients With 5 or More Brain Metastases Treated With Gamma Knife Stereotactic Radiosurgery
 ORIGINAL ARTICLE Survival and Intracranial Control of Patients With 5 or More Brain Metastases Treated With Gamma Knife Stereotactic Radiosurgery Ann C. Raldow, BS,* Veronica L. Chiang, MD,w Jonathan P.
ORIGINAL ARTICLE Survival and Intracranial Control of Patients With 5 or More Brain Metastases Treated With Gamma Knife Stereotactic Radiosurgery Ann C. Raldow, BS,* Veronica L. Chiang, MD,w Jonathan P.
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING
 PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
Clinical Case Conference
 Clinical Case Conference Palliative radiation therapy for bone metastasis Jeff Burkeen, MD, PGY2 7/20/2015 1 Overview Epidemiology Pathophysiology Common presentations and symptoms Imaging Surgery Radiation
Clinical Case Conference Palliative radiation therapy for bone metastasis Jeff Burkeen, MD, PGY2 7/20/2015 1 Overview Epidemiology Pathophysiology Common presentations and symptoms Imaging Surgery Radiation
PET IMAGING (POSITRON EMISSION TOMOGRAPY) FACT SHEET
 FACT SHEET") Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Prophylactic Cranial Irradiation and Thoracic Radiotherapy in Extensive Stage Small-Cell Lung Cancer
 Prophylactic Cranial Irradiation and Thoracic Radiotherapy in Extensive Stage Small-Cell Lung Cancer Dr Neil Bayman Consultant Clinical Oncology ESMO-Christie Preceptorship Programme in Lung Cancer, March
Prophylactic Cranial Irradiation and Thoracic Radiotherapy in Extensive Stage Small-Cell Lung Cancer Dr Neil Bayman Consultant Clinical Oncology ESMO-Christie Preceptorship Programme in Lung Cancer, March
The use of surgery in the elderly. for management of metastatic epidural spinal cord compression
 The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care
 Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland
Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland
Cerebel trial Any impact on the clinical practice? Antonio Frassoldati Oncologia Clinica - Ferrara
 Cerebel trial Any impact on the clinical practice? Antonio Frassoldati Oncologia Clinica - Ferrara CNS metastases in HER2+ BC The proportion of patients with HER2+ advanced breast cancer who have CNS metastases
Cerebel trial Any impact on the clinical practice? Antonio Frassoldati Oncologia Clinica - Ferrara CNS metastases in HER2+ BC The proportion of patients with HER2+ advanced breast cancer who have CNS metastases
Laser Interstitial Thermal Therapy (LITT) in Neuro-Oncology. Tim Lucas, MD, PhD Neurosurgery
 in Neuro-Oncology. Tim Lucas, MD, PhD Neurosurgery") Laser Interstitial Thermal Therapy (LITT) in Neuro-Oncology Tim Lucas, MD, PhD Neurosurgery Timothy.Lucas@uphs.upenn.edu 2016 Laser Interstitial Thermal Therapy (LITT) in Neuro-Oncology Tim Lucas, MD,
Laser Interstitial Thermal Therapy (LITT) in Neuro-Oncology Tim Lucas, MD, PhD Neurosurgery Timothy.Lucas@uphs.upenn.edu 2016 Laser Interstitial Thermal Therapy (LITT) in Neuro-Oncology Tim Lucas, MD,
Metastasi cerebrali La Radioterapia: tecnica, frazionamento, radiosensibilizzanti
 Metastasi cerebrali La Radioterapia: tecnica, frazionamento, radiosensibilizzanti Brain Metastases Radiation Therapy of multiple brain metastases Is treatment appropriate? - Survival - QoL Brain Metastases
Metastasi cerebrali La Radioterapia: tecnica, frazionamento, radiosensibilizzanti Brain Metastases Radiation Therapy of multiple brain metastases Is treatment appropriate? - Survival - QoL Brain Metastases
Brain metastases and meningitis carcinomatosa: Prof. Rafal Dziadziuszko Medical University of Gdańsk, Poland
 Brain metastases and meningitis carcinomatosa: a palliative situation? Prof. Rafal Dziadziuszko Medical University of Gdańsk, Poland SAMO, Lucerne, February 1-2, 2013 Treatment options for NSCLC patients
Brain metastases and meningitis carcinomatosa: a palliative situation? Prof. Rafal Dziadziuszko Medical University of Gdańsk, Poland SAMO, Lucerne, February 1-2, 2013 Treatment options for NSCLC patients
Selected radiosurgery cases from the Rotating Gamma Institute Debrecen, Hungary
 Selected radiosurgery cases from the Rotating Gamma Institute Debrecen, Hungary László Bognár M.D., Ph.D., József G. Dobai M.D., Gábor Csiky and Imre Fedorcsák M.D., Ph.D. Department of Neurosurgery, Medical
Selected radiosurgery cases from the Rotating Gamma Institute Debrecen, Hungary László Bognár M.D., Ph.D., József G. Dobai M.D., Gábor Csiky and Imre Fedorcsák M.D., Ph.D. Department of Neurosurgery, Medical
Dr Eddie Mee. Neurosurgeon Auckland City Hospital, Ascot Integrated Hospital, MercyAscot Hospitals, Auckland
 Dr Eddie Mee Neurosurgeon Auckland City Hospital, Ascot Integrated Hospital, MercyAscot Hospitals, Auckland 16:30-17:25 WS #48: Current Management of Brain Bleeds and Tumours 17:35-18:30 WS #58: Current
Dr Eddie Mee Neurosurgeon Auckland City Hospital, Ascot Integrated Hospital, MercyAscot Hospitals, Auckland 16:30-17:25 WS #48: Current Management of Brain Bleeds and Tumours 17:35-18:30 WS #58: Current
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2
 Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Cost-effectiveness of stereotactic radiosurgery versus whole brain radiation therapy for up to 10 brain metastases
 Cost-effectiveness of stereotactic radiosurgery versus whole brain radiation therapy for up to 10 brain metastases Nataniel H. Lester-Coll, MD, Arie P. Dosoretz, MD, MBA, Maxwell S. Laurans, MD, Veronica
Cost-effectiveness of stereotactic radiosurgery versus whole brain radiation therapy for up to 10 brain metastases Nataniel H. Lester-Coll, MD, Arie P. Dosoretz, MD, MBA, Maxwell S. Laurans, MD, Veronica
Hypofractionated RT in Cervix Cancer. Anuja Jhingran, MD
 Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Gamma Knife Radiosurgery A tool for treating intracranial conditions. CNSA Annual Congress 2016 Radiation Oncology Pre-congress Workshop
 Gamma Knife Radiosurgery A tool for treating intracranial conditions CNSA Annual Congress 2016 Radiation Oncology Pre-congress Workshop ANGELA McBEAN Gamma Knife CNC State-wide Care Coordinator Gamma Knife
Gamma Knife Radiosurgery A tool for treating intracranial conditions CNSA Annual Congress 2016 Radiation Oncology Pre-congress Workshop ANGELA McBEAN Gamma Knife CNC State-wide Care Coordinator Gamma Knife
Outcomes after Reirradiation for Brain Metastases
 Original Article PROGRESS in MEDICAL PHYSICS Vol. 26, No. 3, September, 2015 http://dx.doi.org/10.14316/pmp.2015.26.3.137 Outcomes after Reirradiation for Brain Metastases Jesang Yu, Ji Hoon Choi, Sun
Original Article PROGRESS in MEDICAL PHYSICS Vol. 26, No. 3, September, 2015 http://dx.doi.org/10.14316/pmp.2015.26.3.137 Outcomes after Reirradiation for Brain Metastases Jesang Yu, Ji Hoon Choi, Sun
PSA nadir post LDR Brachytherapy and early Salvage Therapy. Dr Duncan McLaren UK & Ireland Users Group Meeting 2016
 PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
Treatment of Recurrent Brain Metastases
 Treatment of Recurrent Brain Metastases Penny K. Sneed, M.D. Dept. of Radiation Oncology University of California San Francisco Background Brain metastases occur in 8.5-15% of cancer pts in population-
Treatment of Recurrent Brain Metastases Penny K. Sneed, M.D. Dept. of Radiation Oncology University of California San Francisco Background Brain metastases occur in 8.5-15% of cancer pts in population-
Life after ARUBA: Management of Unruptured Brain Arteriovenous Malformations (AVMs)
") Life after ARUBA: Management of Unruptured Brain Arteriovenous Malformations (AVMs) Eric L. Zager, MD University of Pennsylvania Department of Neurosurgery No Disclosures Brain AVMs Incidence ~1 in 100,000
Life after ARUBA: Management of Unruptured Brain Arteriovenous Malformations (AVMs) Eric L. Zager, MD University of Pennsylvania Department of Neurosurgery No Disclosures Brain AVMs Incidence ~1 in 100,000
Radiation Therapy for Soft Tissue Sarcomas
 Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
CME. Special Article. Received 27 October 2011; revised 9 December 2011; accepted 15 December Practical Radiation Oncology (2012) 2,
 2,") Practical Radiation Oncology (2012) 2, 210 225 CME www.practicalradonc.org Special Article Radiotherapeutic and surgical management for newly diagnosed brain metastasis(es): An American Society for Radiation
Practical Radiation Oncology (2012) 2, 210 225 CME www.practicalradonc.org Special Article Radiotherapeutic and surgical management for newly diagnosed brain metastasis(es): An American Society for Radiation
Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps?
 Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps? Michael J Zelefsky, M.D. Professor of Radiation Oncology Chief Brachytherapy Service Department of Radiation Oncology
Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps? Michael J Zelefsky, M.D. Professor of Radiation Oncology Chief Brachytherapy Service Department of Radiation Oncology
Radiotherapy of Brain Metastases and Carcinomatous Meningitis
 Universitätsspital Basel Radiotherapy of Brain Metastases and Carcinomatous Meningitis Dr. J. Winkler 16.01.2009 1 in 4 cancer patients develop brain metastases In 1/3-1/2 of these patients brain metastasis
Universitätsspital Basel Radiotherapy of Brain Metastases and Carcinomatous Meningitis Dr. J. Winkler 16.01.2009 1 in 4 cancer patients develop brain metastases In 1/3-1/2 of these patients brain metastasis
Role of Prophylactic Cranial Irradiation in Small Cell Lung Cancer
 Role of Prophylactic Cranial Irradiation in Small Cell Lung Cancer Kazi S. Manir MD,DNB,ECMO,PDCR Clinical Tutor Department of Radiotherapy R. G. Kar Medical College and Hospital, Kolkata SCLC 15% of lung
Role of Prophylactic Cranial Irradiation in Small Cell Lung Cancer Kazi S. Manir MD,DNB,ECMO,PDCR Clinical Tutor Department of Radiotherapy R. G. Kar Medical College and Hospital, Kolkata SCLC 15% of lung
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
The Four R s. Repair Reoxygenation Repopulation Redistribution. The Radiobiology of Small Fraction Numbers. The Radiobiology of Small Fraction Numbers
 The Radiobiology of Small Fraction Numbers David J. Brenner, PhD, DSc Center for Radiological Research Columbia University Medical Center djb3@columbia.edu The Radiobiology of Small Fraction Numbers 1.
The Radiobiology of Small Fraction Numbers David J. Brenner, PhD, DSc Center for Radiological Research Columbia University Medical Center djb3@columbia.edu The Radiobiology of Small Fraction Numbers 1.
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Otolaryngologist s Perspective of Stereotactic Radiosurgery
 Otolaryngologist s Perspective of Stereotactic Radiosurgery Douglas E. Mattox, M.D. 25 th Alexandria International Combined ORL Conference April 18-20, 2007 Acoustic Neuroma Benign tumor of the schwann
Otolaryngologist s Perspective of Stereotactic Radiosurgery Douglas E. Mattox, M.D. 25 th Alexandria International Combined ORL Conference April 18-20, 2007 Acoustic Neuroma Benign tumor of the schwann
11/27/2017. Modern Treatment of Meningiomas. Disclosures. Modern is Better? No disclosures relevant to this presentation
 Modern Treatment of Meningiomas Michael A. Vogelbaum MD, PhD Professor of Neurosurgery Cleveland Clinic Disclosures No disclosures relevant to this presentation IP and royalties related to drug and device
Modern Treatment of Meningiomas Michael A. Vogelbaum MD, PhD Professor of Neurosurgery Cleveland Clinic Disclosures No disclosures relevant to this presentation IP and royalties related to drug and device
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
SUCCESSFUL TREATMENT OF METASTATIC BRAIN TUMOR BY CYBERKNIFE: A CASE REPORT
 SUCCESSFUL TREATMENT OF METASTATIC BRAIN TUMOR BY CYBERKNIFE: A CASE REPORT Cheng-Ta Hsieh, 1 Cheng-Fu Chang, 1 Ming-Ying Liu, 1 Li-Ping Chang, 2 Dueng-Yuan Hueng, 3 Steven D. Chang, 4 and Da-Tong Ju 1
SUCCESSFUL TREATMENT OF METASTATIC BRAIN TUMOR BY CYBERKNIFE: A CASE REPORT Cheng-Ta Hsieh, 1 Cheng-Fu Chang, 1 Ming-Ying Liu, 1 Li-Ping Chang, 2 Dueng-Yuan Hueng, 3 Steven D. Chang, 4 and Da-Tong Ju 1
Management of Brain Metastases Sanjiv S. Agarwala, MD
 Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
The Role of Radiotherapy in Metastatic Breast Cancer. Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health
 The Role of Radiotherapy in Metastatic Breast Cancer Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health Indications for Palliative Pain Control Radiation Bone
The Role of Radiotherapy in Metastatic Breast Cancer Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health Indications for Palliative Pain Control Radiation Bone
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy
 San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
Disclosures. Overview 8/3/2016. SRS: Cranial and Spine
 SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
ORIGINAL ARTICLE. Annals of Oncology 28: , 2017 doi: /annonc/mdx332 Published online 27 June 2017
 Annals of Oncology 28: 2588 2594, 217 doi:1.193/annonc/mdx332 Published online 27 June 217 ORIGINAL ARTICLE Whole brain radiotherapy after stereotactic radiosurgery or surgical resection among patients
Annals of Oncology 28: 2588 2594, 217 doi:1.193/annonc/mdx332 Published online 27 June 217 ORIGINAL ARTICLE Whole brain radiotherapy after stereotactic radiosurgery or surgical resection among patients
Disclosures. Neurological Manifestations of Von Hippel Lindau Syndrome. Objectives. Overview. None No conflicts of interest
 Neurological Manifestations of Von Hippel Lindau Syndrome ARNOLD B. ETAME MD, PhD NEURO-ONCOLOGY/NEUROSURGERY Moffitt Cancer Center Disclosures None No conflicts of interest VHL Alliance Annual Family
Neurological Manifestations of Von Hippel Lindau Syndrome ARNOLD B. ETAME MD, PhD NEURO-ONCOLOGY/NEUROSURGERY Moffitt Cancer Center Disclosures None No conflicts of interest VHL Alliance Annual Family
Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased
 Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased analysis Roel Schlijper Fellow Radiation Oncology BC Cancer, Prince George Disclosures No conflicts
Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased analysis Roel Schlijper Fellow Radiation Oncology BC Cancer, Prince George Disclosures No conflicts
RESEARCH HUMAN CLINICAL STUDIES
 TOPIC RESEARCH HUMAN CLINICAL STUDIES RESEARCH HUMAN CLINICAL STUDIES Radiosurgery to the Surgical Cavity as Adjuvant Therapy for Resected Brain Metastasis Jared R. Robbins, MD* Samuel Ryu, MD* Steven
TOPIC RESEARCH HUMAN CLINICAL STUDIES RESEARCH HUMAN CLINICAL STUDIES Radiosurgery to the Surgical Cavity as Adjuvant Therapy for Resected Brain Metastasis Jared R. Robbins, MD* Samuel Ryu, MD* Steven
Intracranial AT RT / radiotherapy. Therapeutic dilemma / radiotherapy
 Therapeutic dilemma / radiotherapy Agressive tumour, poor outcome Past treatments based on MB concepts (RT CSA) MB Overall survival Mean age : 6.52 years n=36, 5 year 75% 1. Tumour occurs in the very young
Therapeutic dilemma / radiotherapy Agressive tumour, poor outcome Past treatments based on MB concepts (RT CSA) MB Overall survival Mean age : 6.52 years n=36, 5 year 75% 1. Tumour occurs in the very young
Impact of Targeted/Immunotherapy on Gamma Knife Radiosurgery
 Impact of Targeted/Immunotherapy on Gamma Knife Radiosurgery Veronica Chiang, MD Yale University Department of Neurosurgery IGKRF Scientific Session University of Pennsylvania, Philadelphia June 23-24,
Impact of Targeted/Immunotherapy on Gamma Knife Radiosurgery Veronica Chiang, MD Yale University Department of Neurosurgery IGKRF Scientific Session University of Pennsylvania, Philadelphia June 23-24,
Neurosurgery Review. Mudit Sharma, MD May 16 th, 2008
 Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
SBRT for lung metastases: Case report
 SBRT for lung metastases: Case report Guillermo de Velasco MD, PhD University Hospital 12 de Octubre @H12O_GUCancer @g_develasco Case report 71 years old man Smoker DM 2005 Right radical nephrectomy Histology:
SBRT for lung metastases: Case report Guillermo de Velasco MD, PhD University Hospital 12 de Octubre @H12O_GUCancer @g_develasco Case report 71 years old man Smoker DM 2005 Right radical nephrectomy Histology:
Therapy of Non-Operable early stage NSCLC
 SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
SURGICAL MANAGEMENT OF BRAIN TUMORS
 SURGICAL MANAGEMENT OF BRAIN TUMORS LIGIA TATARANU, MD, Ph D NEUROSURGICAL CLINIC, BAGDASAR ARSENI CLINICAL HOSPITAL BUCHAREST, ROMANIA SURGICAL INDICATIONS CONFIRMING HISTOLOGIC DIAGNOSIS REDUCING TUMOR
SURGICAL MANAGEMENT OF BRAIN TUMORS LIGIA TATARANU, MD, Ph D NEUROSURGICAL CLINIC, BAGDASAR ARSENI CLINICAL HOSPITAL BUCHAREST, ROMANIA SURGICAL INDICATIONS CONFIRMING HISTOLOGIC DIAGNOSIS REDUCING TUMOR
Neurological Change after Gamma Knife Radiosurgery for Brain Metastases Involving the Motor Cortex
 ORIGINAL ARTICLE Brain Tumor Res Treat 2016;4(2):111-115 / pissn 2288-2405 / eissn 2288-2413 http://dx.doi.org/10.14791/btrt.2016.4.2.111 Neurological Change after Gamma Knife Radiosurgery for Brain Metastases
ORIGINAL ARTICLE Brain Tumor Res Treat 2016;4(2):111-115 / pissn 2288-2405 / eissn 2288-2413 http://dx.doi.org/10.14791/btrt.2016.4.2.111 Neurological Change after Gamma Knife Radiosurgery for Brain Metastases
Brain Tumor Treatment
 Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Radiotherapy in feline and canine head and neck cancer
 Bettina Kandel Like surgery radiotherapy is usually a localized type of treatment. Today it is more readily available for the treatment of cancer in companion animals and many clients are well informed
Bettina Kandel Like surgery radiotherapy is usually a localized type of treatment. Today it is more readily available for the treatment of cancer in companion animals and many clients are well informed
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
CUrative Radiotherapy to the primary tumor vs. best supportive care in patients with initially metastatic Cervical carcinoma (CURE-C trial)
") CUrative Radiotherapy to the primary tumor vs. best supportive care in patients with initially metastatic Cervical carcinoma (CURE-C trial) EORTC ROG-GCG-QLG Study coordinator Igor Sirák, M.D., Ph.D Department
CUrative Radiotherapy to the primary tumor vs. best supportive care in patients with initially metastatic Cervical carcinoma (CURE-C trial) EORTC ROG-GCG-QLG Study coordinator Igor Sirák, M.D., Ph.D Department
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer
 Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
New modalities in the salvage of recurrent nasopharyngeal carcinoma
 New modalities in the salvage of recurrent nasopharyngeal carcinoma Dr Jeeve Kanagalingam FRCS Eng (ORL-HNS) Department of Otorhinolaryngology Tan Tock Seng Hospital SINGAPORE Nasopharyngeal carcinoma
New modalities in the salvage of recurrent nasopharyngeal carcinoma Dr Jeeve Kanagalingam FRCS Eng (ORL-HNS) Department of Otorhinolaryngology Tan Tock Seng Hospital SINGAPORE Nasopharyngeal carcinoma
Treatment of Brain Metastases
 1 Treatment of Brain Metastases An Overview and Pending Research Questions To Answer Olav E. Yri, MD, PhD www.ntnu.no/prc European Palliative Care Research Centre (PRC) The brain metastases diagnosis Outline
1 Treatment of Brain Metastases An Overview and Pending Research Questions To Answer Olav E. Yri, MD, PhD www.ntnu.no/prc European Palliative Care Research Centre (PRC) The brain metastases diagnosis Outline
Immunotherapy for the Treatment of Brain Metastases
 Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases Lawrence G. Lum, MD, DSc Karmanos Cancer Institute and Wayne State University Advances in Cancer Immunotherapy
Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases Lawrence G. Lum, MD, DSc Karmanos Cancer Institute and Wayne State University Advances in Cancer Immunotherapy
Laryngeal Preservation Using Radiation Therapy. Chemotherapy and Organ Preservation
 1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
Brain mets under I.O.
 Brain mets under I.O. Bernard Escudier Gustave Roussy, Villejuif, France Disclosure Honorarium received from BMS, Novartis, Pfizer, Bayer, Roche, Exelixis, Ipsen, Eisai, Calithera Travel Grant from BMS,
Brain mets under I.O. Bernard Escudier Gustave Roussy, Villejuif, France Disclosure Honorarium received from BMS, Novartis, Pfizer, Bayer, Roche, Exelixis, Ipsen, Eisai, Calithera Travel Grant from BMS,
Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases
 Immunotherapy for the Treatment of Brain Metastases") Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases Geoffrey T. Gibney, MD Georgetown-Lombardi Comprehensive Cancer Center Medstar-Georgetown University Hospital
Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases Geoffrey T. Gibney, MD Georgetown-Lombardi Comprehensive Cancer Center Medstar-Georgetown University Hospital
Stereotactic Radiosurgery. Extracranial Stereotactic Radiosurgery. Linear accelerators. Basic technique. Indications of SRS
 Stereotactic Radiosurgery Extracranial Stereotactic Radiosurgery Annette Quinn, MSN, RN Program Manager, University of Pittsburgh Medical Center Using stereotactic techniques, give a lethal dose of ionizing
Stereotactic Radiosurgery Extracranial Stereotactic Radiosurgery Annette Quinn, MSN, RN Program Manager, University of Pittsburgh Medical Center Using stereotactic techniques, give a lethal dose of ionizing
Hypofractionated Radiotherapy for breast cancer: Updated evidence
 2 rd Bangladesh Breast Cancer Conference, Dhaka, December 2017 Hypofractionated Radiotherapy for breast cancer: Updated evidence Tabassum Wadasadawala Associate Professor of Radiation Oncology Tata Memorial
2 rd Bangladesh Breast Cancer Conference, Dhaka, December 2017 Hypofractionated Radiotherapy for breast cancer: Updated evidence Tabassum Wadasadawala Associate Professor of Radiation Oncology Tata Memorial
Use of radiation to kill diseased cells. Cancer is the disease that is almost always treated when using radiation.
 Radiation Therapy Use of radiation to kill diseased cells. Cancer is the disease that is almost always treated when using radiation. One person in three will develop some form of cancer in their lifetime.
Radiation Therapy Use of radiation to kill diseased cells. Cancer is the disease that is almost always treated when using radiation. One person in three will develop some form of cancer in their lifetime.
CNS SESSION 3/8/ th Multidisciplinary Management of Cancers: A Case based Approach
 CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
JAMA. 2006;295:
 ORIGINAL CONTRIBUTION Stereotactic Radiosurgery Plus Whole-Brain Radiation Therapy vs Stereotactic Radiosurgery Alone for Treatment of Brain Metastases A Randomized Controlled Trial Hidefumi Aoyama, MD,
ORIGINAL CONTRIBUTION Stereotactic Radiosurgery Plus Whole-Brain Radiation Therapy vs Stereotactic Radiosurgery Alone for Treatment of Brain Metastases A Randomized Controlled Trial Hidefumi Aoyama, MD,
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our