Metastasi cerebrali La Radioterapia: tecnica, frazionamento, radiosensibilizzanti
|
|
|
- Meghan Stevens
- 5 years ago
- Views:
Transcription


1 Metastasi cerebrali La Radioterapia: tecnica, frazionamento, radiosensibilizzanti

2 Brain Metastases Radiation Therapy of multiple brain metastases Is treatment appropriate? - Survival - QoL
3 Brain Metastases Survival by RPA prognostic class Gaspar et al,1997
4 Multiple Brain Metastases Patients with brain metastases Supportive Care Palliative RT and Supportive Care
5 WBI for Multiple Brain Metastases No data regarding - Tumor response - Intracranial WBI plus Progression-free supportive care* duration - Quality of life - Toxicity Median Survival 14 wks Improvement in PS 61% p value not stated Supportive care* * Oral prednisone Median Survival 10 wks Improvement in PS 63% Horton, 1971
6 Multiple Brain Metastases Whole Brain Radiotherapy
7 Brain metastases and Radiotherapy Randomized trials Patients with brain metastases Whole brain radiotherapy Schedule A Schedule B
8
9 Royal College of Radiologists Brain metastases trial WBI 30 Gy/10fr Patients with symptomatic brain metastases 544 pts (533 eligible) WBI 12 Gy/2fr Priestman et al., Clin.Oncol, 1996
10 Royal College brain metastases trial Characteristics of the 533 eligible patients The two treatment groups were well balanced with respect to patients characteristics Priestman et al., Clin.Oncol, 1996
11 Royal College brain metastases trial Analysis of the survival curves showed a marginal advantage for ten fractions (p = 0.04). The 3-month and 6-month survival rates were 42% and 17% respectively for the two fractions treatment and 48% and 25 % respectively for the tenfractions regimen Priestman et al., Clin.Oncol, 1996
12 Royal College brain metastases trial Analysis of prognostic factors for survival age (p=0.008) site of the primary tumour (p=0.002) extent of cerebral disease (p = 0.008) dosage of dexamethasone at the time of entry into the trial (p = 0.001) WHO performance status (p<0.0001) Priestman et al., Clin.Oncol, 1996
13 Royal College brain metastases trial Survival by prognostic groups Grouping the patients into 'good risk' (three or four favourable factors), 'intermediate risk' (two favourable, two unfavourable factors), 'three poor', or 'four poor' factors revealed significant differences in survival (p<0.0001) Priestman et al., Clin.Oncol, 1996
14 These results suggest that any increase in survival due to longer radiotherapy treatment is confined to good prognosis patients, but, for the majority, there is no advantage and the value of radiotherapy for these patients relates purely to the possibility of control or relief of distressing symptoms. Priestman et al., Clin.Oncol, 1996
15 A retrospective analysis of 164 pts treated with a standard regimen of 30 Gy/10fr was performed to find factors correlating with the local results To compare 39 pts treated with a total dose of Gy with patients treated with the standard regimen 30 Gy/10fr
16 Response to radiotherapy and survival for brain metastases Median survival 6 mo in the CR group Median survival 4 mo in the PR group Median survival 2.4 mo in the SD group
17 Relation between local result and total dose of RT for brain metastases The retrospective analysis showed a dependence of the local result after RT on two parameters: - diameter of brain mets - tumor histology (SCLC and adenoca more radiosensitive than squamous cell carcinoma) The Local Response (CR or PR) was 48%-52% after 30 Gy 77% after Gy (p 0.05) Survival was not significantly different
18
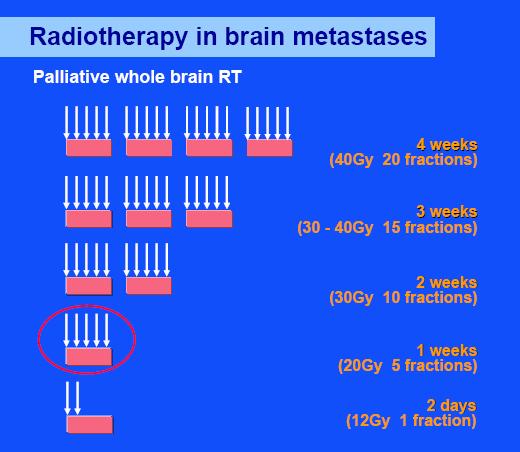
19 RTOG brain metastases trials Patients with brain metastases WBI 20 Gy in 5 fractions 1 week 30 Gy in 10 fractions 30 Gy in 15 fractions 37.5 Gy in 15 fractions 40 Gy in 15 fractions 40 Gy in 20 fractions 4 weeks
20 WBI for Multiple Brain Metastases - WBI is the conventional treatment for most patients with brain mets (except radioresistant tumors, i.e. melanoma) - No specific dose or radiation schedule has been found to be superior (from 20 Gy over 1 week to 50 Gy over 5 weeks) Typical radiation schedule: 30 Gy/10 fr or 37.5 Gy/15 fr (RTOG) - Some risk (>10%) of significant neurocognitive impairment and radiologic findings in long-term survivors (> 9 months) Potentially safer schedules in patients with a likelihood of surviving more than 9 months



21 Good RT technique also for palliation Technical considerations: Modern conventional CNS RT: - conformal - conventional fraction size
22 To evaluate the potential benefits of CT simulation in WBI comparing field-shaping based on 3D CT simulation to conventional 2D simulation.
 as in conventional simulation")

23 Role of CT simulation in WBI CT head scans were obtained from 20 patients. Conventional 2D planning was obtained by drawing the block contours on digitally reconstructed radiographs (DRR) as in conventional simulation 3D-planning was obtained by contouring target volume on the CT slices. To assess the adequacy of margins, the minimal distance from the field edge to the contoured organ was measured for both planning situations at six sites (the subfrontal region (midline), both ocular lenses, both temporal lobes, and the medulla) Portal design in WBI by conventional simulation 3D block shaping in 3D-planning
24 RESULTS In conventional planning using DRR - major geographic mismatches (< -3 mm) occurred in the subfrontal region - minor mismatches (-3 to 0 mm) predominantly occurred in the contralateral lens (21%), ipsilateral lens (10%), and subfrontal region (9%). - close margins (0 5 mm) were most frequently noted at the contralateral lens (49%), ipsilateral lens (35%), and the subfrontal region (28%). In 3D planning - mismatches were not found. - close margins were inevitable at the ipsilateral lens (5%), subfrontal region (30%), and contralateral lens (70%).
25 CT simulation in WBI is significantly superior to conventional simulation with respect to complete coverage of the target volume and protection of the eye lenses
26 Multiple Brain Metastases Whole Brain Radiotherapy Can we improve the efficacy of RT?
27 Improvement of therapeutic index by radiosensitization (shift of TCP curve to the left) TCP or NTCP 1 0,9 0,8 0,7 0,6 0,5 0,4 0,3 0,2 0,1 0 TCP= Tumor Control Probability NTCP=Normal Tissue Complication Probability Dose (Gy)
28 Randomized studies of WBI with radiosensitizers Study Study arms N. of pts (eval) Overall Median Survival Overall Surv at 6 months Response Rates De Angelis. Eyre Komarnicky Phillips 30 Gy/10fr+lonidamine 30 Gy/10fr 30 Gy/10fr+metronidazole 30 Gy/10fr 30Gy/6fr+misonidazole 30Gy/6fr 30Gy/10fr+misonidazole 30 Gy/10fr 37.5Gy/15fr+BrdUrd 37.5Gy/15fr 31(19) 27 (20) (57) (54) 220 (196) 216 (200) 211 (190) 212 (193) No significant difference 35 (34) 37 (36) NR % 55% 27% 24% 63% of 22pts 50% of 24pts
")
29 NSCLC Brain (RTOG 0320) Solitary or oligometastases (1-3) R A N D WBI + SRS WBI + SRS + temozolomide WBI + SRS + erlotinib Stratifications: - PS: 0/1 v 2 - Extracranial status: controlled vs active Targeted N = To detect a 50% improvement in median survival (5.8 to 8.7 months)
30 New radiosensitizing agents in brain mets: Motexafin Gadolinium Porphyrin-like macrocyclic compounds Motexafin gadolinium is selectively taken up and retained in tumor cells to a greater degree than in normal tissues Inside the tumor cell, it generates reactive oxygen species and oxidizes various intracellular reducing metabolites, inhibiting systems that normally protect cells against oxidative stress (inhibition of DNA repair, lower threshold for apoptosis)
31 Radiosensitizing agents in brain mets: Motexafin Gadolinium Study Patients Comments Carde, 2001 Mehta, 2003 Phase I-II trial; WBI 30 Gy+Motexafin from 0.3 to 8.4 mg/kg/d x 10; 39 phase I and 22 phase II pts Phase III trial; WBI 30 Gy ± Motexafin; 5.5 mg/kg/d x 10 Well balanced arms; 401 pts Selective MR localization seen; drug well tolerated; Median Survival 4.7 months Median Survival 5.2 vs 4.9 months; Median Time to neurologic progression improved for NSCLC
32 Randomized Phase III Trial of Motexafin Gadolinium for Patients with Brain Metastases 401 pts WBI R A N D O M I Z A T I O N Motexafin gadolinium Control arm Mehta,2003
33 Randomized Phase III Trial of Motexafin Gadolinium for Patients with Brain Metastases Overall the study was negative, with no benefit in either end points..but Motexafin Gadolinium plus WBI significantly prolonged time to neurologic progression in NSCLC patients The benefit of motexafin gadolinium was also evident on several secondary end points, including deaths from CNS causes in lung cancer pts (52% vs 36%; p.037) and improved memory and executive function in lung cancer pts ( p.062) relative to whole brain alone Adverse events were mild to moderate and manageable (Skin and urine discoloration the most common adverse events) Phase III trial in NSCLC ongoing
34 Influence of Tissue Oxygenation on Radiosensitivity

35 Efaproxiral (RSR13) Well defined mechanism of Action Synthetic allosteric modifier of hemoglobin Decreases Hb affinity for O 2, increasing diffusion of O 2 to tissues No cytotoxic activity In vivo studies show reduction of hypoxic fraction in tumors after efaproxiral administration Increases tumor oxygenation during radiation therapy Need not penetrate tumor tissue for activity Need not cross blood brain barrier Rapid action and short half-life
36 Radiosensitizing agents in brain mets: Efaproxiral (RSR 13) Study Patients Comments Shaw, 2003 Suh, 2003 Phase II trial; WBI 30 Gy with 100 mg/kg efaproxiral; 69 pts Phase III trial; WBI 30 Gy ± efaproxiral 100 mg/kg/die; 538 pts Median Survival 6.4 months; Grade 3-4 toxicities were hypoxia 10%, headache 10%, anemia 4% Median survival 5.3 months vs 4.5; improved survival in breast cancer subset
37 Phase III study of Efaproxiral as an adjunct to whole-brain Radiation therapy for brain Metastases 538 pts WBI R A N D O M I Z A T I O N Efaproxiral Control arm J.H. Suh,2003
38 Phase III Trial: WBRT +/- RSR patients enrolled WBRT and Supplemental O2 +/- RSR-13 No survival advantage: 5.3 vs 4.5 mo (p=0.17) In subset of 111 pts with breast cancer: Control (n=52): 4.6 mo RSR-13 (n=59): 8.7 mo Pts with metastatic breast cancer to the brain also sustained a statistically significant increase in RR A confirmatory phase III trial is underway
39 The ENRICH Study ENRICH..defined ENhancing Whole Brain Radiation Therapy In Patients with Breast Cancer and Hypoxic Brain Metastases
40 The ENRICH Study Objectives: - Determine the effect of efaproxiral on primary and secondary endpoints in women with brain metastases from breast cancer receiving standard WBRT with supplemental oxygen - Assess the safety of efaproxiral End points: Primary: - Survival Secondary: - Response rate in the brain at 3 months - KPS and neurologic signs and symptoms Mehta,2003
41 The ENRICH Study 360 eligible patients receiving a 2-week (10 fractions) course of WBRT (30.0 Gy/3.0 Gy fractions per day) with or without efaproxiral Patients are randomized 1:1 to: Treatment Arm A: WBRT with efaproxiral (via a central venous access device) plus supplemental oxygen Treatment Arm B: WBRT with supplemental oxygen, without a placebo
42 Efaproxiral Administration Repeat for 10 days Outpatient clinic If Spo 2 90% Monitor and release Oxygen tapered off Radiation is administered O 2 and pulse oximeter initiated 5 <30 30 Efaproxiral administered Transfer for radiation treatment 30-minute window If Spo 2 90%
43 Exclusion Criteria Active concurrent malignancy (except nonmelanoma skin cancer or in situ carcinoma of the cervix). If there is a history of prior malignancy, the patient must be disease-free for 5 years. The patient is a candidate for surgical resection and/or stereotactic radiosurgery as initial therapy for brain metastases. Planned concurrent systemic (cytotoxic and/or cytostatic) treatment for breast cancer and/or extracranial metastases during WBRT, with the exception of trastuzumab, hormonal, and/or corticosteroid therapy. Prior treatment for brain metastases (including external beam radiation therapy, brachytherapy, stereotactic radiosurgery, surgery, chemotherapy, and treatments with investigational drugs, biologics, or devices). Presence of leptomeningeal metastases.
44 Study Status Patient enrollment completed in August 2006, with a total of 368 patients enrolled at 78 medical centers Final analysis expected to occur in mid-2007
45 WBI and chemical modifiers of Radiation Therapy ( Radiosensitizers( Radiosensitizers ) Improvement of tumor response is a worthwhile aim in this population Regression of brain mets after WBI correlates with improved neurocognitive function and QoL (Level Ib) Radiosensitizers are not primary disease-specific


46 Solitary Brain Metastases Oncological Management Options
47 Randomized studies of WBI plus SRS vs WBI alone in oligo (< 3) brain metastases RTOG-9508: Phase III Trial Enrollment: 1/96-6/01: N = 333 (2 pts excluded) Arm 1: WBRT (37.5 Gy) + SRS: N = 164 Arm 2: WBRT (37.5 Gy) alone: N = 167 Stratification < 2 cm 24 Gy cm 18 Gy cm 15 Gy 1. Number of brain metastases (1 vs 2-3) 2. Extracranial mets (none vs present) Andrews DW, et al. Lancet % & 24% of 1 & 2-3 brain met pts randomized to RS did not receive it
48 Randomized studies of WBI plus SRS vs WBI in oligo brain metastases RTOG-9508: Subset Analysis Survival Analyses WBRT & SRS WBRT p-value Overall 6.5 mo 5.7 mo Solitary brain met. 6.5 mo. 4.9 mo mets & Age < mo. 8.3 mo mets & NSCLC 5.9 mo. 3.9 mo mets & RPA Class mo. 9.6 mo. 0.05
49 Role of Adjuvant WBI Surgery (46) Surgery + WBI (49) Recurrence: local 46% 10% p<.001 in brain 37% 14% p<.01 Time to recurrence: in brain (median) 26 wks 220 wks Neurologic death 44% 14% p =.003 Survival (median) 43 wks 48 wks p =.39 Patchell,, 1998
50 SRS No Survival difference (8.0 vs 7.5 mesi; p=ns) 132 pts with up four mets R A N D SRS+WBI Better intracranial desease control (23.6% vs 53.2%; p<0.001) No difference in neurocognitive outcome
51 Neurological Functional Preservation Rate (RPA class < 2) PROBABILITY (%) WBI+SRS SRS alone Rate at 1 year WBI+SRS: 70% SRS alone: 71% P= Months Aoyama, ASCO 2004
52
53 WBI and NCF/QOL - WBRT is bad and should be delayed because that prevents neurocognitive deterioration and maintains quality of life - Maybe so, probably not, because recurrence is worse for the brain
54 WBI and NCF/QOL Dementia after WBI of brain metastases Risk factors - Treatment volume - Fraction size >2 Gy - Total dose: less important than fraction size - Concurrent chemotherapy: possible - Age: elderly patients (> 60 yrs) at higher risk
55 Percentage Patients Impaired at Presentation Brain mets patients have high rates of Motor Function baseline deficits Memory Executive Function N=401 Impairment = Z Fluency Memory 0 Peg D Peg ND Recall Delay Trail B COWA Delay COWA Recog Meyers CA, et al. J Clin Oncol Recog
56 RTOG 91-04: Neurocognitive Outcome 445 patients accrued to RTOG CF: 3.0 Gy QD to 30.0 Gy 445 patients Randomization AH: 1.6 Gy BID to 54.4 Gy 359 patients had Mini-Mental Status Examinations (MMSE) performed before WBRT; and at 2 and 3 months
57 Tumor Control and MMSE Change Uncontrolled tumor is bad for the brain. At 2 months Avg Change At 3 months Avg Change Brain Mets (N=91) in MMSE (N=23) in MMSE Controlled 91% % -0.5 Uncontrolled 9% % -6.3 P=0.02 Regine, WF et al. IJROBP, 2001
58 WBI and NCF/QOL What have we learned? Radiation is not nearly as bad as the tumor is!!
59 Is It Rational to Withhold Whole Brain Radiotherapy?

60 EORTC No radiotherapy versus whole brain radiotherapy for 1 to 3 brain metastases from solid tumor after surgical resection or radiosurgery: a randomized Phase III trial
61 Role of WBI as prophylactic therapy
62 Meta-analysis analysis of PCI in SCLC Overall survival Brain metastases Auperin A NEJM 1999
63 Results of the meta-analysis analysis of PCI in SCLC in complete remission Treatment group No. of pts Control group Relative risk (95% CI) P value 3-yr rate in the control group Absolute benefit at 3 yr OS ( ) % +5.4% DFS ( ) < % +8.8% Brain metastases ( ) < % -25.3% Auperin NEJM 1999
64 SCLC and Radiation therapy PCI - The role of PCI now seems quite clearly indicated - Dose, fractionation and timing require further clarification (PCI EULINT-EORTC EORTC trial, 25 Gy in 10 fr vs 36 Gy in 18 fr) - Concerns on serious neurotoxicity mainly related to old hypofractionated schedules (prospective NCF evaluation as a part of prospective trials)
65 NSCLC and Radiation therapy PCI - Brain mets are a relative common event in radically treated NSCLC patients - PCI may reduce the incidence of brain mets, but there is no evidence of a survival benefit - No data regarding whether radiotherapy regimen is superior, and the effect of PCI on QoL - RTOG 0214, randomized trial, is ongoing Carolan, 2005
66 Prophylactic Cranial Irradiation in the treatment of locally advanced NSCLC Study pts PCI dose Primary treatment CNS failure (Obs vs PCI) P value Cox et al Gy RT alone 13% vs 6% Russell et al Gy RT alone 19% vs 9% Umsawasdi et al Gy CT and RT or CT,RT, and surgery 27% vs 4% Significantly lower risk for developing brain mets with PCI, but no difference in survival Phase III randomized trial RTOG 0214
67 Conclusions - Disease oriented studies in brain metastases - Identification of patients at higher risk of developing brain mets (epidemiological studies,, gene expression profiling) - RT, with or without chemo, is still the treatment of choice for pts needing a palliation of neurological symptoms
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Management of Brain Metastases Dr. Luis Souhami Professor Department of Radiation Oncology University,
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Management of Brain Metastases Dr. Luis Souhami Professor Department of Radiation Oncology University,
Minesh Mehta, Northwestern University. Chicago, IL
 * Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
* Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms. Overall Clinical Significance 8/3/13
 Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen?
 Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Optimal Management of Isolated HER2+ve Brain Metastases
 Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Palliative radiotherapy in lung cancer
 New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
Update on Limited Small Cell Lung Cancer. Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver
 Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Role of Prophylactic Cranial Irradiation in Small Cell Lung Cancer
 Role of Prophylactic Cranial Irradiation in Small Cell Lung Cancer Kazi S. Manir MD,DNB,ECMO,PDCR Clinical Tutor Department of Radiotherapy R. G. Kar Medical College and Hospital, Kolkata SCLC 15% of lung
Role of Prophylactic Cranial Irradiation in Small Cell Lung Cancer Kazi S. Manir MD,DNB,ECMO,PDCR Clinical Tutor Department of Radiotherapy R. G. Kar Medical College and Hospital, Kolkata SCLC 15% of lung
Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey
 Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Brain metastases and meningitis carcinomatosa: Prof. Rafal Dziadziuszko Medical University of Gdańsk, Poland
 Brain metastases and meningitis carcinomatosa: a palliative situation? Prof. Rafal Dziadziuszko Medical University of Gdańsk, Poland SAMO, Lucerne, February 1-2, 2013 Treatment options for NSCLC patients
Brain metastases and meningitis carcinomatosa: a palliative situation? Prof. Rafal Dziadziuszko Medical University of Gdańsk, Poland SAMO, Lucerne, February 1-2, 2013 Treatment options for NSCLC patients
ES-SCLC Joint Case Conference. Anthony Paravati Adam Yock
 ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia
 for Brain Metastasis in Nova Scotia") A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia Gaurav Bahl, Karl Tennessen, Ashraf Mahmoud-Ahmed, Dorianne Rheaume, Ian Fleetwood,
A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia Gaurav Bahl, Karl Tennessen, Ashraf Mahmoud-Ahmed, Dorianne Rheaume, Ian Fleetwood,
VINCENT KHOO. 8 th EIKCS Symposium: May 2013
 8 th EIKCS Symposium: May 2013 VINCENT KHOO Royal Marsden NHS Foundation Trust & Institute of Cancer Research St George s Hospital & University of London Austin Health & University of Melbourne Disclosures
8 th EIKCS Symposium: May 2013 VINCENT KHOO Royal Marsden NHS Foundation Trust & Institute of Cancer Research St George s Hospital & University of London Austin Health & University of Melbourne Disclosures
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy
 San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
Radiotherapy and Brain Metastases. Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem
 Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
Prophylactic Cranial Irradiation and Thoracic Radiotherapy in Extensive Stage Small-Cell Lung Cancer
 Prophylactic Cranial Irradiation and Thoracic Radiotherapy in Extensive Stage Small-Cell Lung Cancer Dr Neil Bayman Consultant Clinical Oncology ESMO-Christie Preceptorship Programme in Lung Cancer, March
Prophylactic Cranial Irradiation and Thoracic Radiotherapy in Extensive Stage Small-Cell Lung Cancer Dr Neil Bayman Consultant Clinical Oncology ESMO-Christie Preceptorship Programme in Lung Cancer, March
Update on management of metastatic brain disease. Peter Hoskin Mount Vernon Cancer Centre Northwood UK
 Update on management of metastatic brain disease Peter Hoskin Mount Vernon Cancer Centre Northwood UK Incidence 15-30% of patients with solid tumours will develop brain metastases Most common primary sites
Update on management of metastatic brain disease Peter Hoskin Mount Vernon Cancer Centre Northwood UK Incidence 15-30% of patients with solid tumours will develop brain metastases Most common primary sites
Outline. WBRT field. Brain Metastases. Whole Brain RT Prophylactic WBRT Stereotactic radiosurgery (SRS) 1 fraction Stereotactic frame
 1 fraction Stereotactic frame") Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Place of tumor bed radiosurgery and focal radiotherapy following resec7on of brain metastases: A new paradigm Lucyna Kepka
 Place of tumor bed radiosurgery and focal radiotherapy following resec7on of brain metastases: A new paradigm Lucyna Kepka Department of Radia7on Oncology; M. Sklodowska- Curie Memorial Cancer Center and
Place of tumor bed radiosurgery and focal radiotherapy following resec7on of brain metastases: A new paradigm Lucyna Kepka Department of Radia7on Oncology; M. Sklodowska- Curie Memorial Cancer Center and
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
Radiation Therapy in SCLC. What is New? Prof. Dr. Hoda Abdel Baky El Bakry Cairo Cancer Institute Radiation Oncology Department
 Radiation Therapy in SCLC What is New? Prof. Dr. Hoda Abdel Baky El Bakry Cairo Cancer Institute Radiation Oncology Department Background Overview Small Cell Lung cancer constitute about 15 % of all newly
Radiation Therapy in SCLC What is New? Prof. Dr. Hoda Abdel Baky El Bakry Cairo Cancer Institute Radiation Oncology Department Background Overview Small Cell Lung cancer constitute about 15 % of all newly
Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We
 Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We Edward Garon, MD, MS Associate Professor Director- Thoracic Oncology Program David
Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We Edward Garon, MD, MS Associate Professor Director- Thoracic Oncology Program David
Selecting the Optimal Treatment for Brain Metastases
 Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
Management of Brain Metastases Sanjiv S. Agarwala, MD
 Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Cécile Le Péchoux Department of Radiation Oncology, Institut Gustave Roussy, Villejuif France Amsterdam 2010
 Prophylactic Cranial Irradiation in Lung Cancer Cécile Le Péchoux Department of Radiation Oncology, Institut Gustave Roussy, Villejuif France Amsterdam 2010 Prophylactic cranial irradiation PCI was introduced
Prophylactic Cranial Irradiation in Lung Cancer Cécile Le Péchoux Department of Radiation Oncology, Institut Gustave Roussy, Villejuif France Amsterdam 2010 Prophylactic cranial irradiation PCI was introduced
Hong Kong Hospital Authority Convention 2018
 Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
ARROCase Brain Metastases
 ARROCase Brain Metastases Colin Hill*, Daniel M. Trifiletti*, Timothy N. Showalter*, Jason P. Sheehan Radiation Oncology* and Neurosurgery University of Virginia Charlottesville, VA Case: HPI 64 year old
ARROCase Brain Metastases Colin Hill*, Daniel M. Trifiletti*, Timothy N. Showalter*, Jason P. Sheehan Radiation Oncology* and Neurosurgery University of Virginia Charlottesville, VA Case: HPI 64 year old
Treatment of Recurrent Brain Metastases
 Treatment of Recurrent Brain Metastases Penny K. Sneed, M.D. Dept. of Radiation Oncology University of California San Francisco Background Brain metastases occur in 8.5-15% of cancer pts in population-
Treatment of Recurrent Brain Metastases Penny K. Sneed, M.D. Dept. of Radiation Oncology University of California San Francisco Background Brain metastases occur in 8.5-15% of cancer pts in population-
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS
 UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
Radiotherapy for Brain Metastases
 Radiotherapy for Brain Metastases Robert B. Den, MD a, David W. Andrews, MD b, * KEYWORDS Brain metastases Treatment approaches SRS WBRT The optimal treatment of brain metastases remains controversial.
Radiotherapy for Brain Metastases Robert B. Den, MD a, David W. Andrews, MD b, * KEYWORDS Brain metastases Treatment approaches SRS WBRT The optimal treatment of brain metastases remains controversial.
Management of single brain metastasis: a practice guideline
 PRACTICE GUIDELINE SERIES Management of single brain metastasis: a practice guideline A. Mintz MD,* J. Perry MD, K. Spithoff BHSc, A. Chambers MA, and N. Laperriere MD on behalf of the Neuro-oncology Disease
PRACTICE GUIDELINE SERIES Management of single brain metastasis: a practice guideline A. Mintz MD,* J. Perry MD, K. Spithoff BHSc, A. Chambers MA, and N. Laperriere MD on behalf of the Neuro-oncology Disease
Hypofractionated RT in Cervix Cancer. Anuja Jhingran, MD
 Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Where are we with radiotherapy for biliary tract cancers?
 Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
RTOG Lung Cancer Committee 2012 Clinical Trial Update. Wally Curran RTOG Group Chairman
 RTOG Lung Cancer Committee 2012 Clinical Trial Update Wally Curran RTOG Group Chairman 1 RTOG Lung Committee: Active Trials Small Cell Lung Cancer Limited Stage (Intergroup Trial) Extensive Stage (RTOG
RTOG Lung Cancer Committee 2012 Clinical Trial Update Wally Curran RTOG Group Chairman 1 RTOG Lung Committee: Active Trials Small Cell Lung Cancer Limited Stage (Intergroup Trial) Extensive Stage (RTOG
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部
 肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased
 Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased analysis Roel Schlijper Fellow Radiation Oncology BC Cancer, Prince George Disclosures No conflicts
Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased analysis Roel Schlijper Fellow Radiation Oncology BC Cancer, Prince George Disclosures No conflicts
Current Approaches for Limited Small Cell Lung Cancer. Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver
 Current Approaches for Limited Small Cell Lung Cancer Laurie Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Can we improve or personalize treatment? Limited Histology/molecular
Current Approaches for Limited Small Cell Lung Cancer Laurie Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Can we improve or personalize treatment? Limited Histology/molecular
Overview: Immunotherapy in CNS Metastases
 Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
CME. Special Article. Received 27 October 2011; revised 9 December 2011; accepted 15 December Practical Radiation Oncology (2012) 2,
 2,") Practical Radiation Oncology (2012) 2, 210 225 CME www.practicalradonc.org Special Article Radiotherapeutic and surgical management for newly diagnosed brain metastasis(es): An American Society for Radiation
Practical Radiation Oncology (2012) 2, 210 225 CME www.practicalradonc.org Special Article Radiotherapeutic and surgical management for newly diagnosed brain metastasis(es): An American Society for Radiation
Cerebel trial Any impact on the clinical practice? Antonio Frassoldati Oncologia Clinica - Ferrara
 Cerebel trial Any impact on the clinical practice? Antonio Frassoldati Oncologia Clinica - Ferrara CNS metastases in HER2+ BC The proportion of patients with HER2+ advanced breast cancer who have CNS metastases
Cerebel trial Any impact on the clinical practice? Antonio Frassoldati Oncologia Clinica - Ferrara CNS metastases in HER2+ BC The proportion of patients with HER2+ advanced breast cancer who have CNS metastases
Treating Brain Metastases in the Changing World of Oncology: Matthew Ewend, MD Kay and Van Weatherspoon Professor Chair, Department of Neurosurgery
 Treating Brain Metastases in the Changing World of Oncology: Matthew Ewend, MD Kay and Van Weatherspoon Professor Chair, Department of Neurosurgery Disclosures Consultant: None Stock Holdings: None Paid
Treating Brain Metastases in the Changing World of Oncology: Matthew Ewend, MD Kay and Van Weatherspoon Professor Chair, Department of Neurosurgery Disclosures Consultant: None Stock Holdings: None Paid
Quality of life in brain metastases radiation trials: a literature review
 RADIATION ONCOLOGY Quality of life in brain metastases radiation trials: a literature review J. Wong,* A. Hird,* A. Kirou Mauro,* J. Napolskikh BSc,* and E. Chow MBBS* ABSTRACT Background An estimated
RADIATION ONCOLOGY Quality of life in brain metastases radiation trials: a literature review J. Wong,* A. Hird,* A. Kirou Mauro,* J. Napolskikh BSc,* and E. Chow MBBS* ABSTRACT Background An estimated
CNS Metastases in Breast Cancer
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer CNS Metastases in Breast Cancer CNS Metastases in Breast Cancer Version 2006: Maass / Junkermann Version 2007 2009: Bischoff
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer CNS Metastases in Breast Cancer CNS Metastases in Breast Cancer Version 2006: Maass / Junkermann Version 2007 2009: Bischoff
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care
 Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland
Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland
GCIG Rare Tumour Brainstorming Day
 GCIG Rare Tumour Brainstorming Day Relatively (Not So) Rare Tumours Adenocarcinoma of Cervix Keiichi Fujiwara, Ros Glasspool Benedicte Votan, Jim Paul Aim of the Day To develop at least one clinical trial
GCIG Rare Tumour Brainstorming Day Relatively (Not So) Rare Tumours Adenocarcinoma of Cervix Keiichi Fujiwara, Ros Glasspool Benedicte Votan, Jim Paul Aim of the Day To develop at least one clinical trial
Benefits of Radiation Therapy in the Palliative Cancer Patient
 Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
Place de la radiothérapie dans les CBPC métastatiques
 Place de la radiothérapie dans les CBPC métastatiques Cecile Le Péchoux, 12 ème Biennale Monégasque de Cancérologie, 2016 IOT Institut d Oncologie Thoracique CBPC metastatique Rapid doubling time, early
Place de la radiothérapie dans les CBPC métastatiques Cecile Le Péchoux, 12 ème Biennale Monégasque de Cancérologie, 2016 IOT Institut d Oncologie Thoracique CBPC metastatique Rapid doubling time, early
Survival and Intracranial Control of Patients With 5 or More Brain Metastases Treated With Gamma Knife Stereotactic Radiosurgery
 ORIGINAL ARTICLE Survival and Intracranial Control of Patients With 5 or More Brain Metastases Treated With Gamma Knife Stereotactic Radiosurgery Ann C. Raldow, BS,* Veronica L. Chiang, MD,w Jonathan P.
ORIGINAL ARTICLE Survival and Intracranial Control of Patients With 5 or More Brain Metastases Treated With Gamma Knife Stereotactic Radiosurgery Ann C. Raldow, BS,* Veronica L. Chiang, MD,w Jonathan P.
Multiple Brain Metastases EVIDENCE TABLE
 . Posner JB. Management of brain metastases. Rev Neurol (Paris). 992;48(6-7):477-487. 2. Wen PY, Black PM, Loeffler JS. Metastatic brain cancer. In: DeVita VT, Hellman S, Rosenberg SA, eds. Cancer, principles
. Posner JB. Management of brain metastases. Rev Neurol (Paris). 992;48(6-7):477-487. 2. Wen PY, Black PM, Loeffler JS. Metastatic brain cancer. In: DeVita VT, Hellman S, Rosenberg SA, eds. Cancer, principles
Timing of targeted therapy in patients with low volume mrcc. Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital
 1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
Radiotherapy of Brain Metastases and Carcinomatous Meningitis
 Universitätsspital Basel Radiotherapy of Brain Metastases and Carcinomatous Meningitis Dr. J. Winkler 16.01.2009 1 in 4 cancer patients develop brain metastases In 1/3-1/2 of these patients brain metastasis
Universitätsspital Basel Radiotherapy of Brain Metastases and Carcinomatous Meningitis Dr. J. Winkler 16.01.2009 1 in 4 cancer patients develop brain metastases In 1/3-1/2 of these patients brain metastasis
Two Cycles of Chemoradiation: 2 Cycles is Enough. Concurrent Chemotherapy / RT Regimens
 1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
Laboratory data from the 1970s first showed that malignant melanoma
 2265 Survival by Radiation Therapy Oncology Group Recursive Partitioning Analysis Class and Treatment Modality in Patients with Brain Metastases from Malignant Melanoma A Retrospective Study Jeffrey C.
2265 Survival by Radiation Therapy Oncology Group Recursive Partitioning Analysis Class and Treatment Modality in Patients with Brain Metastases from Malignant Melanoma A Retrospective Study Jeffrey C.
CALGB Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer
 CALGB 30610 Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer Jeffrey A. Bogart Department of Radiation Oncology Upstate Medical University Syracuse, NY Small Cell Lung Cancer Estimated 33,000
CALGB 30610 Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer Jeffrey A. Bogart Department of Radiation Oncology Upstate Medical University Syracuse, NY Small Cell Lung Cancer Estimated 33,000
Standard care plan for Prophylactic Cranial Irradiation for Limited Stage (stage I-III) Small Cell Lung Cancer (25Gy in 10 fractions) References
 Small Cell Lung Cancer (25Gy in 10 fractions) References") CHEMOTHERAPY CARE PLAN Document Title: Document Type: Subject: Approved by: Prophylactic Cranial Irradiation for Limited-stage Small Cell Lung Cancer (20Gy in 5 fractions) Clinical Guideline Standard Care
CHEMOTHERAPY CARE PLAN Document Title: Document Type: Subject: Approved by: Prophylactic Cranial Irradiation for Limited-stage Small Cell Lung Cancer (20Gy in 5 fractions) Clinical Guideline Standard Care
Is it cost-effective to treat brain metastasis with advanced technology?
 Is it cost-effective to treat brain metastasis with advanced technology? Cost-effectiveness analysis of whole brain RT, stereotactic radiosurgery and craniotomy in HA setting Lam, Tai-Chung, Choi CW Horace,
Is it cost-effective to treat brain metastasis with advanced technology? Cost-effectiveness analysis of whole brain RT, stereotactic radiosurgery and craniotomy in HA setting Lam, Tai-Chung, Choi CW Horace,
Radiotherapy symptoms control in bone mets. Francesco Cellini GemelliART. Ernesto Maranzano,MD. Session 5: Symptoms management
 Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015
 Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015 Most common brain tumor, affecting 8.5-15% of cancer patients. Treatment options: Whole brain radiation
Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015 Most common brain tumor, affecting 8.5-15% of cancer patients. Treatment options: Whole brain radiation
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Some Seminal Studies. Chemotherapy Alone is Inadequate. Bladder Cancer Role of Radiation in Bladder Sparing. Primary Radiation for Bladder Cancer
 Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Treatment of Brain Metastases
 1 Treatment of Brain Metastases An Overview and Pending Research Questions To Answer Olav E. Yri, MD, PhD www.ntnu.no/prc European Palliative Care Research Centre (PRC) The brain metastases diagnosis Outline
1 Treatment of Brain Metastases An Overview and Pending Research Questions To Answer Olav E. Yri, MD, PhD www.ntnu.no/prc European Palliative Care Research Centre (PRC) The brain metastases diagnosis Outline
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Radiation and DCIS. The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging
 Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Brain metastases: changing visions
 Brain metastases: changing visions Roberto Spiegelmann, MD Baiona, 2014 Head, Stereotactic Radiosurgery Unit Dept of Neurosurgery, Chaim Sheba Medical Center Tel Hashomer, Israel The best current estimate
Brain metastases: changing visions Roberto Spiegelmann, MD Baiona, 2014 Head, Stereotactic Radiosurgery Unit Dept of Neurosurgery, Chaim Sheba Medical Center Tel Hashomer, Israel The best current estimate
Jefferson Digital Commons. Thomas Jefferson University. Mark E Linskey Department of Neurosurgery, University of California-Irvine Medical Center
 Thomas Jefferson University Jefferson Digital Commons Department of Neurosurgery Faculty Papers Department of Neurosurgery 1-1-2010 The role of stereotactic radiosurgery in the management of patients with
Thomas Jefferson University Jefferson Digital Commons Department of Neurosurgery Faculty Papers Department of Neurosurgery 1-1-2010 The role of stereotactic radiosurgery in the management of patients with
Brain metastases are detected in approximately 20%
 COUNTERPOINTS Current Controversies in Hematology and Oncology Should All Patients With SCLC Receive Prophylactic Cranial Irradiation If They Have Responded to Treatment? Brain metastases are common in
COUNTERPOINTS Current Controversies in Hematology and Oncology Should All Patients With SCLC Receive Prophylactic Cranial Irradiation If They Have Responded to Treatment? Brain metastases are common in
SYNOPSIS PROTOCOL N UC-0107/1602
 SYNOPSIS PROTOCOL N UC-0107/1602 A) TRIAL IDENTIFICATION SPONSOR PROTOCOL CODE NUMBER: UC-0107/1602 VERSION (NR & DATE): 0.1, MARCH 2016 TRIAL TITLE: Extracranial Stereotactic Body Radiation Therapy (SBRT)
SYNOPSIS PROTOCOL N UC-0107/1602 A) TRIAL IDENTIFICATION SPONSOR PROTOCOL CODE NUMBER: UC-0107/1602 VERSION (NR & DATE): 0.1, MARCH 2016 TRIAL TITLE: Extracranial Stereotactic Body Radiation Therapy (SBRT)
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
LUNG CANCER. Agnieszka Słowik, MD. Department of Oncology, University Hospital in Cracow Jagiellonian University
 LUNG CANCER Agnieszka Słowik, MD Department of Oncology, University Hospital in Cracow Jagiellonian University Epidemiology Most common malignancy worldwide Place of lung cancer among other malignancies
LUNG CANCER Agnieszka Słowik, MD Department of Oncology, University Hospital in Cracow Jagiellonian University Epidemiology Most common malignancy worldwide Place of lung cancer among other malignancies
Innova&ve Trial Concepts for Brain Metastases. Minesh P Mehta, MD, FASTRO Professor, University of Maryland
 Innova&ve Trial Concepts for Brain Metastases Minesh P Mehta, MD, FASTRO Professor, University of Maryland Historic Trial Design A common theme has been to design an all inclusive trial that includes Most
Innova&ve Trial Concepts for Brain Metastases Minesh P Mehta, MD, FASTRO Professor, University of Maryland Historic Trial Design A common theme has been to design an all inclusive trial that includes Most
Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases
 Immunotherapy for the Treatment of Brain Metastases") Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases Geoffrey T. Gibney, MD Georgetown-Lombardi Comprehensive Cancer Center Medstar-Georgetown University Hospital
Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases Geoffrey T. Gibney, MD Georgetown-Lombardi Comprehensive Cancer Center Medstar-Georgetown University Hospital
Advances in Radiation Therapy
 Advances in Radiation Therapy 2017 Recent Advances in Oncology Michelle Alonso-Basanta, MD PhD Helene Blum Assistant Professor Associate Chief of Clinical Operations Director of Quality Assurance Chief,
Advances in Radiation Therapy 2017 Recent Advances in Oncology Michelle Alonso-Basanta, MD PhD Helene Blum Assistant Professor Associate Chief of Clinical Operations Director of Quality Assurance Chief,
SBRT for lung metastases: Case report
 SBRT for lung metastases: Case report Guillermo de Velasco MD, PhD University Hospital 12 de Octubre @H12O_GUCancer @g_develasco Case report 71 years old man Smoker DM 2005 Right radical nephrectomy Histology:
SBRT for lung metastases: Case report Guillermo de Velasco MD, PhD University Hospital 12 de Octubre @H12O_GUCancer @g_develasco Case report 71 years old man Smoker DM 2005 Right radical nephrectomy Histology:
Heterogeneity of N2 disease
 Locally Advanced NSCLC Surgery? No. Ramaswamy Govindan M.D Co-Director, Section of Medical Oncology Alvin J Siteman Cancer Center at Washington University School of Medicine St. Louis, Missouri Heterogeneity
Locally Advanced NSCLC Surgery? No. Ramaswamy Govindan M.D Co-Director, Section of Medical Oncology Alvin J Siteman Cancer Center at Washington University School of Medicine St. Louis, Missouri Heterogeneity
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
The use of surgery in the elderly. for management of metastatic epidural spinal cord compression
 The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Adjuvant Radiotherapy for completely resected NSCLC
 Adjuvant Radiotherapy for completely resected NSCLC ESMO Preceptorship on lung Cancer Manchester February 2017 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique Local
Adjuvant Radiotherapy for completely resected NSCLC ESMO Preceptorship on lung Cancer Manchester February 2017 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique Local
Outcomes after Reirradiation for Brain Metastases
 Original Article PROGRESS in MEDICAL PHYSICS Vol. 26, No. 3, September, 2015 http://dx.doi.org/10.14316/pmp.2015.26.3.137 Outcomes after Reirradiation for Brain Metastases Jesang Yu, Ji Hoon Choi, Sun
Original Article PROGRESS in MEDICAL PHYSICS Vol. 26, No. 3, September, 2015 http://dx.doi.org/10.14316/pmp.2015.26.3.137 Outcomes after Reirradiation for Brain Metastases Jesang Yu, Ji Hoon Choi, Sun
Sergio Bracarda MD. Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy
 San Donato Hospital Arezzo, Italy") Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view. Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium
 HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
ORIGINAL ARTICLE Quality of Life and Symptoms Control in Brain Metastasis After Palliative Whole Brain Radiotherapy Using Two Different Protocols
 ORIGINAL ARTICLE Quality of Life and Symptoms Control in Brain Metastasis After Palliative Whole Brain Radiotherapy Using Two Different Protocols Muhammad Sohail Akhtar 1, Farzana Kousar 3, Shahab Fatmi
ORIGINAL ARTICLE Quality of Life and Symptoms Control in Brain Metastasis After Palliative Whole Brain Radiotherapy Using Two Different Protocols Muhammad Sohail Akhtar 1, Farzana Kousar 3, Shahab Fatmi
Treating Multiple. Brain Metastases (BM)
") ESTRO 36 5-9 May 2017, Vienna Austria, Accuray Symposium Treating Multiple Brain Metastases (BM) with CyberKnife System Frederic Dhermain MD PhD, Radiation Oncologist Gustave Roussy University Hospital,
ESTRO 36 5-9 May 2017, Vienna Austria, Accuray Symposium Treating Multiple Brain Metastases (BM) with CyberKnife System Frederic Dhermain MD PhD, Radiation Oncologist Gustave Roussy University Hospital,
Oligometastatic Disease
 Oligometastatic Disease Fact or Fantasy? Jennifer R Bellon MD, FASTRO Dana-Farber Cancer Institute Harvard Medical School Alexander V Louie MD PhD, FRCPC London Health Sciences Center Western University
Oligometastatic Disease Fact or Fantasy? Jennifer R Bellon MD, FASTRO Dana-Farber Cancer Institute Harvard Medical School Alexander V Louie MD PhD, FRCPC London Health Sciences Center Western University
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Oncological Management of Brain Tumours. Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013
 Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
Adjuvant Chemotherapy
 State-of-the-art: standard of care for resectable NSCLC Adjuvant Chemotherapy JY DOUILLARD MD PhD Professor of Medical Oncology Integrated Centers of Oncology R Gauducheau University of Nantes France Adjuvant
State-of-the-art: standard of care for resectable NSCLC Adjuvant Chemotherapy JY DOUILLARD MD PhD Professor of Medical Oncology Integrated Centers of Oncology R Gauducheau University of Nantes France Adjuvant
Radioterapia no Tratamento dos Gliomas de Baixo Grau
 Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
BRAIN METS IN 2018: ANY CLOSER TO THE END OF A LONG AND WINDING ROAD?
 BRAIN METS IN 2018: ANY CLOSER TO THE END OF A LONG AND WINDING ROAD? M.J. van den Bent The Brain Tumor Center at Erasmus MC Cancer Center Rotterdam, the Netherlands Molecular targets in primary cancers
BRAIN METS IN 2018: ANY CLOSER TO THE END OF A LONG AND WINDING ROAD? M.J. van den Bent The Brain Tumor Center at Erasmus MC Cancer Center Rotterdam, the Netherlands Molecular targets in primary cancers
Combined modality treatment for N2 disease
 Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
ESRA KAYTAN SAĞLAM, MD Istanbul University Oncology Institute
 USE OF RADIOSENSITIZERS IN ONCOLOGY ESRA KAYTAN SAĞLAM, MD Istanbul University Oncology Institute According to cell type: Radiosensitive tumors (embryojenic tumors, lymphomas) Moderate sensitives (Squamous
USE OF RADIOSENSITIZERS IN ONCOLOGY ESRA KAYTAN SAĞLAM, MD Istanbul University Oncology Institute According to cell type: Radiosensitive tumors (embryojenic tumors, lymphomas) Moderate sensitives (Squamous
Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology
 Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology Abdominal SBRT: Clinical Aspects Rationales for liver and pancreas SBRT
Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology Abdominal SBRT: Clinical Aspects Rationales for liver and pancreas SBRT
NRG ONCOLOGY NRG-CC003
 NRG ONCOLOGY NRG-CC003 A Randomized Phase II/III Trial of Prophylactic Cranial Irradiation with or without Hippocampal Avoidance for Small Cell Lung Cancer SCHEMA Histologic proof or unequivocal cytologic
NRG ONCOLOGY NRG-CC003 A Randomized Phase II/III Trial of Prophylactic Cranial Irradiation with or without Hippocampal Avoidance for Small Cell Lung Cancer SCHEMA Histologic proof or unequivocal cytologic
Clinical Study on Prognostic Factors and Nursing of Breast Cancer with Brain Metastases
 Clinical Study on Prognostic Factors and Nursing of Breast Cancer with Brain Metastases Ying Zhou 1#, Kefang Zhong 1#, Fang Zhou* 2 ABSTRACT This paper aims to explore the clinical features and prognostic
Clinical Study on Prognostic Factors and Nursing of Breast Cancer with Brain Metastases Ying Zhou 1#, Kefang Zhong 1#, Fang Zhou* 2 ABSTRACT This paper aims to explore the clinical features and prognostic
Protocolos de consenso: MTS Cerebrales Resumen ASTRO. Javier Aristu y Germán Valtueña Servicio Oncología Rad. Depart.
 Protocolos de consenso: MTS Cerebrales Resumen ASTRO Javier Aristu y Germán Valtueña Servicio Oncología Rad. Depart. ASTRO 2013 Brain met SRS Abstracts 97. Comparative Effectiveness of SRS versus WBRT
Protocolos de consenso: MTS Cerebrales Resumen ASTRO Javier Aristu y Germán Valtueña Servicio Oncología Rad. Depart. ASTRO 2013 Brain met SRS Abstracts 97. Comparative Effectiveness of SRS versus WBRT