Advancing Care Through Teamwork
|
|
|
- James Hardy
- 5 years ago
- Views:
Transcription
1 Advancing Care Through Teamwork How Medical Physicists and Medical Doctors Can Work Together to Create Change. Jonathan Feddock, MD University of Kentucky Department of Radiation Medicine
2 Disclosures Clinical Educator and Consultant to Isoray Medical, INC. Consultant to Radiadyne, LLC
3 Objectives Review epidemiology of Gynecologic Cancers including treatment Discuss the role of complex brachytherapy procedures Discuss Permanent Interstitial Brachytherapy (PIB) Describe the team process for adapting new therapies using PIB as an example Discuss initial isotope selection for PIB Applicability and selection of patients for PIB Review our personal experience with Cesium-131 PIB Curative treatment of recurrent disease Integration of PIB into initial therapy for complex cases Suggest how to incorporate new modalities into your current brachytherapy program



4 Kentucky what do we do well?



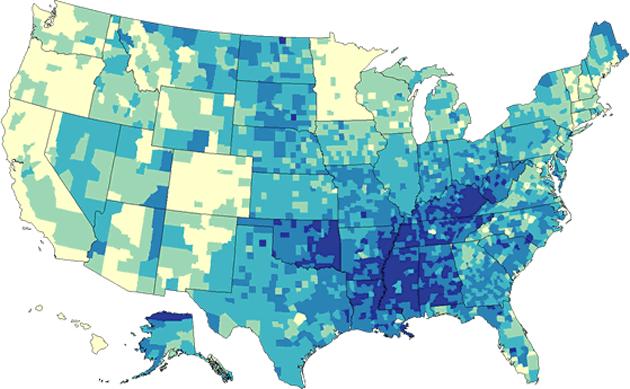
5 Kentucky what do we also do well? Smoking Physical Inactivity Lung Cancer Cancer Mortality

6 Risk Factors for Gynecologic Cancers Ovarian Cancer familial and sporadic cancers Uterine Cancer obesity Cervical Cancer, Vaginal Cancer, & Vulvar Cancer Human papilloma virus (HPV)
7 Gynecologic Cancer Treatment Uterine Cancer Early stage = surgery then external radiation ± brachy Advanced stage = surgery then external radiation + brachy Cervical Cancer Early stage = surgery then external radiation ± brachy Advanced stage = external radiation + brachy Vaginal Cancer Early stage = surgery then external radiation ± brachy Advanced stage = external radiation + brachy Vulvar Cancer Early stage = surgery then external radiation ± brachy Advanced stage = external radiation + brachy
8 Improvements in Gynecologic Cancer Treatment in last 20yrs Addition of chemotherapy to pelvic radiation therapy results in 5% improvement in overall survival for Cervical Cancer Transition from low dose rate (LDR) brachytherapy to high dose rate (HDR) brachytherapy resulting in improved patient quality of life (QOL), reduced exposure to radiation staff, and reduce cost for care Use of Intensity Modulated Radiation Therapy (IMRT) for post-operative gynecologic cancers resulting in significant reduction in acute and late GI toxicities Advent of image-guided brachytherapy


9 Image Guided Brachytherapy Improved delineation of gross disease and target volumes Improved identification of organs at risk Ability to identify changes between brachytherapy fractions and optimize treatments accordingly
10 Brachytherapy is Imperative! Most important component of radiation therapy for gynecologic cancers Superior survival outcomes seen with use of brachytherapy in cervical cancer and vaginal cancer Benefits cannot be replaced with advanced techniques such as Intensity modulated radiation therapy (IMRT) or stereotactic body radiotherapy (SBRT) Omission of brachytherapy has been associated with as much as a 30% decrease in cancer-specific survival Despite the proven benefits, there has been a consistent decline in brachytherapy utilization since 1998 Orton A, Boothe D, Williams N, Buchmiller T, Huang YJ, Suneja G, Poppe M, Gaffney D. Gynecolol Oncol. (2016) June; 141 (3):
11
12 Question #1 In a recent Surveillance, Epidemiology, and End Results (SEER) registry trial by Orton et al., what was the benefit observed with the use of brachytherapy in women with any stage of primary vaginal cancer? a) The use of brachytherapy significantly reduces the risk of death from vaginal cancer regardless of the stage of tumor b) Brachytherapy can be replaced by advanced radiation techniques such as SBRT, IMRT, etc. c) Brachytherapy only benefits women with larger tumors d) None of the above are TRUE.
13 Question #1 In a recent Surveillance, Epidemiology, and End Results (SEER) registry trial by Orton et al., what was the benefit observed with the use of brachytherapy in women with any stage of primary vaginal cancer? a) The use of brachytherapy significantly reduces the risk of death from vaginal cancer regardless of the stage of tumor b) Brachytherapy can be replaced by advanced radiation techniques such as SBRT, IMRT, etc. c) Brachytherapy only benefits women with larger tumors d) None of the above are TRUE. Reference: Orton A, Boothe D, Williams N, Buchmiller T, Huang YJ, Suneja G, Poppe M, Gaffney D. Gynecolol Oncol. (2016) June; 141 (3):
14 Common Barriers to Performing Brachytherapy Physician training and experience Facility expenses, equipment, and maintenance Appropriate physics support Medical knowledge Patient health and performance Tumor related Increased utilization of other radiation techniques: IMRT, SBRT
15 Brachytherapy Options Radiation Oncologist s Comfort Zones (most Radiation Oncologists) HDR Vaginal Cylinders Tandem & Ovoids Tandem & Ring Interstitial Implants LDR PIB
16 Question #2 Which of the following are common reasons that the utilization of brachytherapy has declined in recent years? a) Increased utilization of non-invasive radiation techniques such as SBRT and IMRT b) Inadequate training of Radiation Oncology residents in brachytherapy techniques and skills c) Facility limitations and cost for purchasing and maintaining brachytherapy equipment d) All of the above are cited reasons for the declining use of brachytherapy.
17 Question #2 Which of the following are common reasons that the utilization of brachytherapy has declined in recent years? a) Increased utilization of non-invasive radiation techniques such as SBRT and IMRT b) Inadequate training of Radiation Oncology residents in brachytherapy techniques and skills c) Facility limitations and cost for purchasing and maintaining brachytherapy equipment d) All of the above are cited reasons for the declining use of brachytherapy. Reference: Gill BS, Lin JF, Krivak TC, et al. National Cancer Data Base analysis of radiation therapy consolidation modality for cervical cancer: the impact of new technological advancements. Int J Radiat Oncol Biol Phys 2014 Dec 1;90(5):
18 My 1 st Medical Event for Brachytherapy October 8, :08 am
19 The Problem = Complex Interstitial Implants Awful procedure for patients Morbid concept Long process Many variables capable of going wrong: LDR no routine re-imaging to assess for needle migration HDR able to re-optimize plans in the event of migration, but ability to readjust needles is somewhat limited Complex Interstitial Implants are necessary in certain situations 1 : Bulky tumors not adequately covered by intracavitary techinques Large tumor size Involvement of the lower vagina, urethra, and/or rectovaginal septum 1. Viswanathan et al. Brachytherapy; 2012; 11:

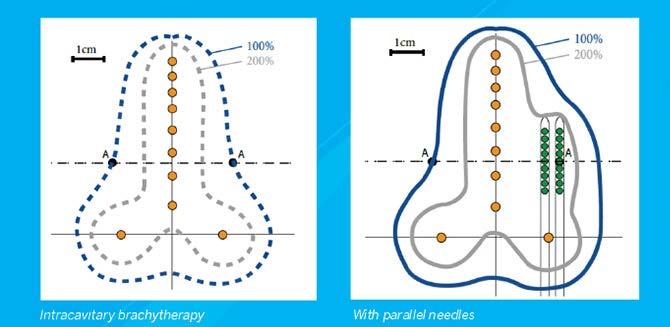
20 Hybrid Applicators a partial solution
21 Question #3 What are the common clinical indications where an interstitial implant should be considered for women with gynecologic cancers? a) Large tumor size b) Involvement of the lower vagina and/or urethra c) Inability to appropriately cover a tumor using intracavitary techniques d) All of the above are indications for interstitial brachytherapy
22 Question #3 What are the common clinical indications where an interstitial implant should be considered for women with gynecologic cancers? a) Large tumor size b) Involvement of the lower vagina and/or urethra c) Inability to appropriately cover a tumor using intracavitary techniques d) All of the above are indications for interstitial brachytherapy Reference: Viswanathan AN, Thomadsen BC. American Brachytherapy Society cervical cancer recommendations, American Brachytherapy Society consensus guidelines for locally advanced carcinoma of the cervix. Part I: general principles. Brachytherapy. 2012;11:33-46.


23 The Manchester System of Brachytherapy Non-uniform placement of sources to create a uniform dose distribution.


24 Single outpatient procedure 55 Gy to 5mm Curative
25 Permanent Interstitial Brachytherapy Ideal strategy for treating small volume disease High cumulative radiation dose Tightly conformal volumes Reduced toxicity compared to external RT Single application that can be done as an outpatient
26 What really makes PIB appealing? Single treatment capable of delivering curative doses (> 50 Gy) Ability to generate very tight dose distribution No hospitalization required Need for indwelling applicators for a few days was not necessary Relatively straightforward regarding resources Hand-calculations or using existing software (Prowess, Variseed, etc.) Low toxicity rates and high curative potential
27 Initial Experience with Interstitial Re-irradiation (IRI) using Au permanent seed implants (5 Au-198, 2 Pd-103) 6 temporary implants (LDR Ir-192, SNIT) Mean and median implanted volumes: 14.3, 12 cc 9/13 (69%) had CR 6/14 (46%) NED months later Median f/u = 58 months Only 1 possible complication: R-V fistula 22 months following SNIT, in presence of recurrent dz Randall ME, Evans L, Greven KM, et al. Gyn Oncol (1993) 48:
28 IRI Favorable Prognostic Factors Cervical and vaginal > endometrial Squamous > adenocarcinoma Smaller tumor volumes Higher RT doses (> 50 Gy) Permanent implants > temporary (SNIT) Vaginal wall/suburethra > vaginal cuff Longer disease-free intervals Randall ME, Evans L, Greven KM, et al. Interstitial Reirradiation for Recurrent Gynecologic Malignancies: Results and Analysis of Prognostic Factors. Gyn Oncol (1993) 48:
29 UK Experience with Permanent Isotopes in Gynecologic Cancers 30 year experience with permanent Au 198, particularly in gynecologic cancers (Randall) No known experience to evaluate the safety/efficacy of Cs 131 in gynecologic malignancies Hypothesized Cs 131 efficacy would be at least equivalent to Au 198 with the added benefit of lower radiation exposure for occupationally exposed personnel in 2010 Based on 6+ years of experience, UK is exclusively utilizing Cs 131 for permanent interstitial brachytherapy for gynecologic malignancies
30 Brachytherapy Isotopes Isotope Half-Life Mean Energy Au days KeV Cs days 30.4 KeV Pd days 20.8 KeV I days 28 KeV Au-198 dosing is essentially equivalent to External Beam radiation therapy dosing e.g. 50 Gy EBRT = 50 Gy Au-198 =
 translates into adequate dose distribution with better radiation safety* Relative equivalence to Au 198 facilitating clinical")
31 Favorable properties of Cesium-131 Short ½ life translates into high initial dose rate (9.7 days vs. 2.7 days for Au-198) Lower energy (30.4 KeV vs 411 KeV for Au-198) translates into adequate dose distribution with better radiation safety* Relative equivalence to Au 198 facilitating clinical dosing/conversions
32 UK Dosimetric Modeling Studies for 131 Cs Multiple Monte Carlo simulations to evaluate optimal distribution of activity Essentially comparing Quimby vs Manchester rules Goal of adequate coverage and homogeneity of dose distribution. Determined that optimal planning was based on Paterson-Parker (Manchester) rules for permanent implants (uneven distribution of activity to create more homogeneity) To determine doses, used BED formalism to estimate, then adopted correction factor (compared to Au 198 ) based on clinical experience = 1.1 Luo W, Molloy J, Aryal P, Feddock J, Randall M. Med Phys. (2014), 41 (2).
33 UK Initial Experience using Cs patients treated with a total of 17 Cs-131 permanent implants 10 implants for recurrent gynecologic cancers 7 implants for definitive treatment, and used as a boost Included spectrum of gynecologic sites and pathologies for primary and recurrent cancers Wooten CE, Randall ME, Feddock J. Gyn Oncol 2014;
34 UK Initial Experience using Cs-131 Actuarial local control at 12 months = 84.4% Two local failures occurred 5 and 7 months after the implant One patient was able to gain local control through re-implantation The second received a dose of 44 Gy to largest implant area of 17.5 cm 3 Probability of tumor control correlated most closely with Doses > 45 Gy and Small Tumor Size Wooten CE, Randall ME, Feddock J. Gyn Oncol 2014.
35 Question #4 What prescription dose for permanent interstitial brachytherapy using Au-198 or Cs-131 appears to be a threshold for controlling gross disease? a) 25 Gy b) 35 Gy c) 45 Gy d) 55 Gy e) 65 Gy
36 Question #4 What prescription dose for permanent interstitial brachytherapy using Au-198 or Cs-131 appears to be a threshold for controlling gross disease? a) 25 Gy b) 35 Gy c) 45 Gy d) 55 Gy e) 65 Gy References: Randall ME, Evans L, Greven KM, McCunniff AJ, Doline RM. Interstitial reirradiation for recurrent gynecologic malignancies: results and analysis of prognostic factors. Gynecologic oncology. 1993;48: Wooten CE, Randall M, Edwards J, et al. Implementation and early clinical results utilizing Cs-131 permanent interstitial implants for gynecologic malignancies. Gynecol Oncol. 2014; 133 (2):

37 Updated UK Experience for Re-Irradiation 61 PIB implants performed for re-irradiation of a pelvic malignancy Median F/U 14.6 months Median time to failure was not reached for 1 st attempt at salvage Median time to failure was more than 8 months for 2 nd attempt at salvage Feddock et al. Int. Radiat Oncol Biol Phys. (2017) EPUB.

38 Orthogonal Radiographs of an Interstitial Au- 198 Implant of a Vaginal Cuff Recurrence

39 Reconstructed 50 Gy Dose Cloud
40 Improving Workflow
41 Migration to CT Planning PIB Or at least CT post-planning
42 Why not use our experience with small volume PIB to revamp Complex Interstitial Implants?
43 Why use PIB with Cs-131 in definitive therapy? Template-guided interstitial implants are not ideal* Prolonged bedrest Hospitalization Patient limitations Practice limitations Intracavitary techniques are often not acceptable Hybrid applicators are not always available and have limitations Conventional interstitial techniques can be overkill Relative ease of calculating dose (multiply EBRT dose X 1.1) Radiobiologic benefits of low dose rate brachytherapy is suggested to result in lower rates of late toxicity
 What about HDR?")
44 Interstitial Implants = Torture (well some are ) Typical LDR Implant 2-3 days bedrest Epidural pain pump Inability to appropriately use the bathroom Risks for: Deep venous thrombosis Pneumonia Urinary Tract Infections We Can Do Better Long term patients have post-traumatic stress disorder (PTSD) What about HDR? Same overall process, but without isolation Multiple fractions Ability to optimize dwell positions, so better plans
45 Potential Risks of Permanent Template Guided Implants High risk to patient if needles placed inappropriately Once you put radiation in, you can t take it back Very high reliance on image-guided therapy Due to decay characteristics of Cs-131 compared to Ir-192 in certain cases, more needles may be required to generate equivalent plans Strands migrate according to location to the pelvic diaphgram
46 How did the first PIB Syed Happen? Patient with recurrent endometrial cancer despite chemotherapy and previous radiation x2 Medically unfit to undergo a multiple day implant Lived in another state so unable to undergo multiple fractions Extensive discussion and planning with brachytherapy physicist Graph paper Prowess Hand calcs Proposed workflow (next slide)
47 Revised Workflow for Cesium-131 Template-Guided Implants 1. All needle positions pre-planned 2. Patient enters the procedure suite 3. Exam performed and template sutured to perineum 4. Needles advanced based on pre-planned arrangement and distances obtained from diagnostic imaging 5. Once all needles have been placed, patient awakens from anesthesia 6. Transfer patient to the CT simulator 7. Needles adjusted and unsheathed incrementally using CT 8. Patient completes recovery and is discharged home

48 1 st PIB Syed
49 What did we learn from our first PIB Syed? 1. The Procedure room and CT simulator doesn t fit a lot of people 2. Needle insertion is not perfect and not as accurate as what you plan 3. Some patients awake from anesthesia quite rapidly 4. After recovering for 5-10min, patients can only really tolerate a few needle adjustments, and with small increments 5. When placing 15+ needles its really hard to look at axial or sagittal CT slices, and pick out the exact 3 needles and run and adjust it and be correct 6. Plan ahead the an artificial hip is going to make needle identification difficult
50 First 5 Patients Treated with a Permanent Template-Guided Interstitial Implant Cesium-131 PIB performed as salvage re-irradiation without any other treatment 3 Vaginal Recurrences of Endometrial Cancer with Side Wall Extension 2 Vulvar Recurrences with extension into the Vagina & PSW A total of 40 needles were placed: Patients 1 & 2 utilized stranded sources Patients 3-5 utilized a combination of stranded & unstranded sources Overall Results: Well tolerated - No significant acute toxicities 4/5 patients were discharged to home within 3 hours of Cs-131 Syed 1 st patient admitted for 23hr observation nothing happened Strand/seed positions were re-evaluated 2-3 weeks later with a repeat CT Feddock et al. Brachytherapy. (2017)

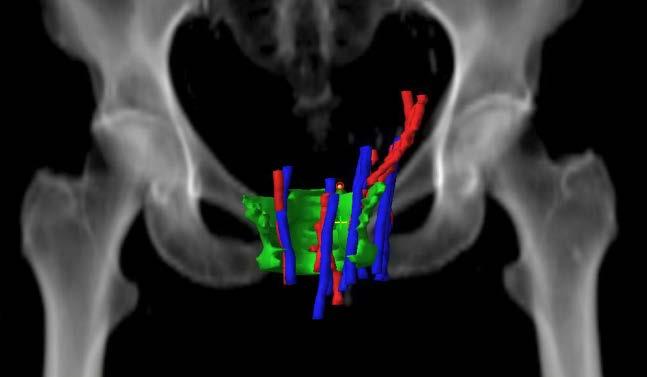
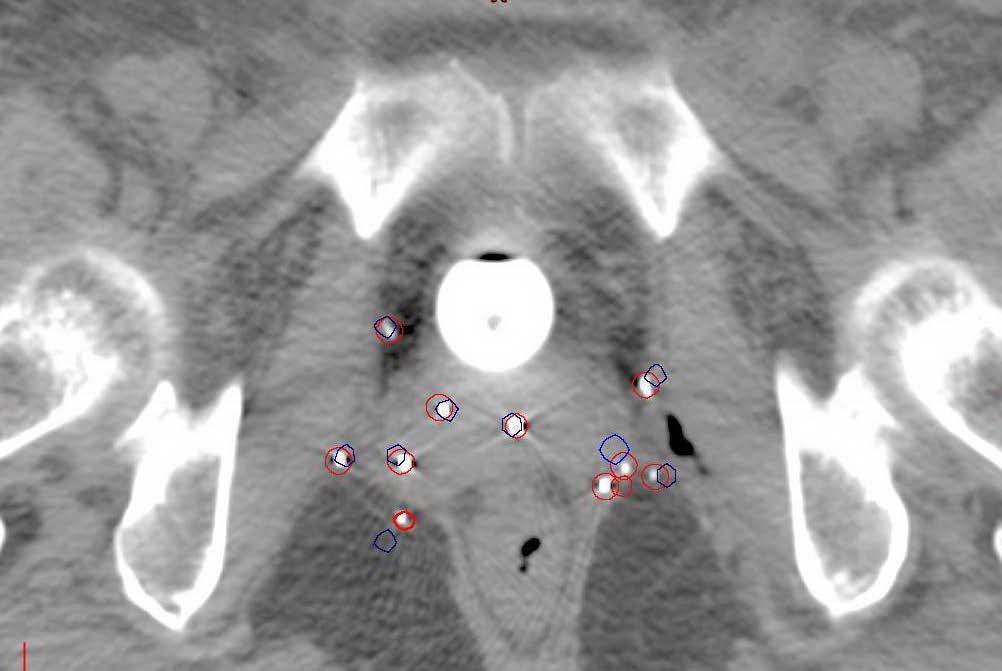
51 A Strand Migration B
52 Making changes and improving the process 1. Structured templates for needle positions 2. Input coordinates for needle positions into Eclipse Brachyvision and all interstitial plans are now pre-planned Able to use CT or MRI Improved needle placement and spacing Revise our active lengths according to organs at risk Gain a better insight into the source strengths and dose 3. Incorporation of Image-guidance combinations of ultrasound, fluoroscopy, and CT 4. Manipulation of existing equipment

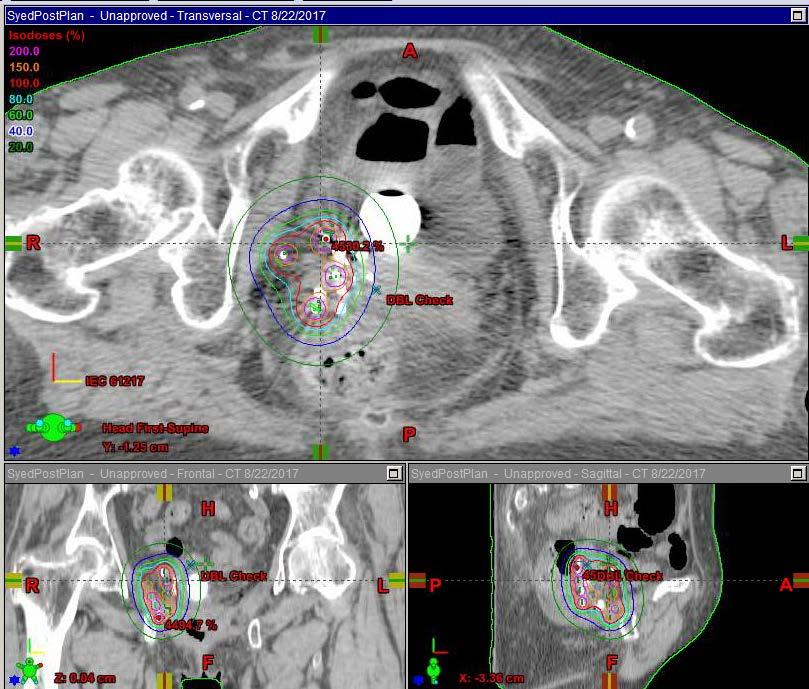
53 Pre-Plan Actual Implant
54 Revised Workflow for Cesium-131 Template-Guided Implants 1. Modify the template prior to procedure to enable use of trans-rectal ultrasound 2. Patient enters the procedure suite 3. Exam performed, TRUS positioned, and template sutured to perineum 4. Needles advanced based on pre-planned arrangement and distances obtained from diagnostic imaging under direct-ultrasound guidance 5. Needles adjusted and unsheathed visually using ultrasound; template removed 6. Patient awakes from conscious sedation 7. Transferred to CT Simulator for confirmatory imaging 8. Patient completes recovery and is discharged home
55 UK PIB Syed Experience Since 2014, more than n=32 permanent interstitial procedures have been performed with at least 6 months follow-up Median PTV volume: 36.4 cm 3 ( cm 3 ) Average source strength: 1.8 u/seed Median # Needles: 8 (5-21) Median Active Length: 5cm (3-11cm) Control rate 77% Only 2 patients have experienced a grade 2+ toxicity as a result of the permanent implant Only one patient has been admitted for an overnight hospital stay (#1) Manuscript in progress
56 Question #5 What makes permanent interstitial brachytherapy an ideal treatment approach in cases where re-irradiation is necessary? a) A curative dose of radiation can be delivered in a single procedure and limited to only the area of interest b) Treatment can be delivered between multiple fractions thereby minimizing toxicity c) The delivery of radiation using low dose rate techniques may potentially reduce the rate of late toxicities d) A and B are correct e) All of the above are correct
57 Question #5 What makes permanent interstitial brachytherapy an ideal treatment approach in cases where re-irradiation is necessary? a) A curative dose of radiation can be delivered in a single procedure and limited to only the area of interest b) Treatment can be delivered between multiple fractions thereby minimizing toxicity c) The delivery of radiation using low dose rate techniques may potentially reduce the rate of late toxicities d) A and B are correct e) All of the above are correct Reference: Wooten CE, Randall M, Edwards J, et al. Implementation and early clinical results utilizing Cs-131 permanent interstitial implants for gynecologic malignancies. Gynecol Oncol. 2014; 133 (2):
58 Final Thoughts Regarding PIB Another tool in the shed Cs-131 dose characteristics very appealing Relatively easy, Clinical brachytherapy procedure Capable of delivering therapeutic doses in a single implant Low Cost Multiple different treatment applications & potential
59 How did this work? Hard-headed physician Right patient population Hard-working and very smart physicists One perfectionist One quiet and extremely diligent at doing long, complex equations One determined to make the process more straightforward, reproducible, and accurate Supportive staff
60 Special Thanks Marcus Randall, MD Prakash Aryal, PhD Wei Luo, PhD Dennis Cheek, PhD Dave Lockhart Penny Ross, RN Laura Reichel, RN
Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w
 Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w Quality assurance Classical implant systems w Manchester
Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w Quality assurance Classical implant systems w Manchester
Brachytherapy Planning and Quality Assurance
 Brachytherapy Planning and Quality Assurance Classical implant systems Most common clinical applications and modern dosimetry methods Quality assurance Classical implant systems Manchester (Paterson-Parker)
Brachytherapy Planning and Quality Assurance Classical implant systems Most common clinical applications and modern dosimetry methods Quality assurance Classical implant systems Manchester (Paterson-Parker)
 https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
Interstitial Brachytherapy. Low dose rate brachytherapy. Brachytherapy alone cures some cervical cancer. Learning Objectives
 Interstitial Learning Objectives To discuss practical aspects of selection and insertion techniques for interstitial brachytherapy and their relation to clinical trials Akila Viswanathan, MD MPH Johns
Interstitial Learning Objectives To discuss practical aspects of selection and insertion techniques for interstitial brachytherapy and their relation to clinical trials Akila Viswanathan, MD MPH Johns
Definitions. Brachytherapy in treatment of cancer. Implantation Techniques and Methods of Dose Specifications. Importance of Brachytherapy in GYN
 Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
GYNECOLOGIC CANCER and RADIATION THERAPY. Jon Anders M.D. Radiation Oncology
 GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
Venezia Advanced Gynecological Applicator Reaching beyond
 Venezia Advanced Gynecological Applicator Reaching beyond Advanced Gynecological Applicator Venezia is FDA cleared and CE marked, but is not available in all markets. 1 Helping clinicians improve patients
Venezia Advanced Gynecological Applicator Reaching beyond Advanced Gynecological Applicator Venezia is FDA cleared and CE marked, but is not available in all markets. 1 Helping clinicians improve patients
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป
 ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
Patterns of Care in Patients with Cervical Cancer:
 Patterns of Care in Patients with Cervical Cancer: Power and Pitfalls of Claims-Based Analysis Grace Smith, MD, PhD, MPH Resident, PGY-5 Department of Radiation Oncology, MD Anderson Cancer Center Acknowledgments
Patterns of Care in Patients with Cervical Cancer: Power and Pitfalls of Claims-Based Analysis Grace Smith, MD, PhD, MPH Resident, PGY-5 Department of Radiation Oncology, MD Anderson Cancer Center Acknowledgments
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer
 for Gynaecological Cancer") Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
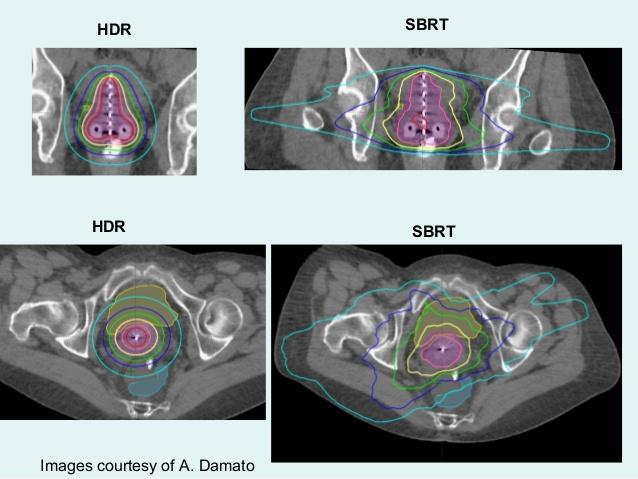
HDR vs. LDR Is One Better Than The Other?
 HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
Basics of Cervix Cancer Brachytherapy
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Cancer Brachytherapy David Gaffney MDPhD, FASTRO, FACR University of Utah Huntsman Cancer Institute Incidence Cervix: 445,000
Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Cancer Brachytherapy David Gaffney MDPhD, FASTRO, FACR University of Utah Huntsman Cancer Institute Incidence Cervix: 445,000
Regulatory Guidelines and Computational Methods for Safe Release of Radioactive Patients II. Brachytherapy
 Regulatory Guidelines and Computational Methods for Safe Release of Radioactive Patients II. Brachytherapy Firas Mourtada, Ph.D., DABR Chief of Clinical Physics Helen F. Graham Cancer Center Christiana
Regulatory Guidelines and Computational Methods for Safe Release of Radioactive Patients II. Brachytherapy Firas Mourtada, Ph.D., DABR Chief of Clinical Physics Helen F. Graham Cancer Center Christiana
Radiotherapy physics & Equipments
 Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Trina Lynd, M.S. Medical Physicist Lifefirst Imaging & Oncology Cullman, AL Tri-State Alabama, Louisiana and Mississippi Spring 2016 Meeting April
 Trina Lynd, M.S. Medical Physicist Lifefirst Imaging & Oncology Cullman, AL Tri-State Alabama, Louisiana and Mississippi Spring 2016 Meeting April 17, 2016 Discuss permanent prostate brachytherapy and
Trina Lynd, M.S. Medical Physicist Lifefirst Imaging & Oncology Cullman, AL Tri-State Alabama, Louisiana and Mississippi Spring 2016 Meeting April 17, 2016 Discuss permanent prostate brachytherapy and
HDR Brachytherapy I: Overview of Clinical Application and QA. Disclosures. Learning Objectives 7/23/2014. Consultant, Varian Medical Systems
 HDR Brachytherapy I: Overview of Clinical Application and QA Timothy Showalter, MD Associate Professor tns3b@virginia.edu Disclosures Consultant, Varian Medical Systems Learning Objectives To understand
HDR Brachytherapy I: Overview of Clinical Application and QA Timothy Showalter, MD Associate Professor tns3b@virginia.edu Disclosures Consultant, Varian Medical Systems Learning Objectives To understand
DOSIMETRIC OPTIONS AND POSSIBILITIES OF PROSTATE LDR BRACHYTHERAPY WITH PERMANENT I-125 IMPLANTS
 DOSIMETRIC OPTIONS AND POSSIBILITIES OF PROSTATE LDR BRACHYTHERAPY WITH PERMANENT I-125 IMPLANTS Andrius IVANAUSKAS*, Eduardas ALEKNAVIČIUS*, Arvydas BURNECKIS*, Albert MILLER *Institute of Oncology Vilnius
DOSIMETRIC OPTIONS AND POSSIBILITIES OF PROSTATE LDR BRACHYTHERAPY WITH PERMANENT I-125 IMPLANTS Andrius IVANAUSKAS*, Eduardas ALEKNAVIČIUS*, Arvydas BURNECKIS*, Albert MILLER *Institute of Oncology Vilnius
Brachytherapy. What is brachytherapy and how is it used?
 Scan for mobile link. Brachytherapy Brachytherapy places radioactive sources inside the patient on a temporary or permanent basis to damage cancer cells DNA and destroy their ability to divide and grow.
Scan for mobile link. Brachytherapy Brachytherapy places radioactive sources inside the patient on a temporary or permanent basis to damage cancer cells DNA and destroy their ability to divide and grow.
Brachytherapy an Overview
 Brachytherapy an Overview Yakov Pipman, D Sc North Shore LIJ Health System Monterrey, Nov30-Dec1, 2007 Brachytherapy A procedure in therapeutic radiology that involves the irradiation of a target with
Brachytherapy an Overview Yakov Pipman, D Sc North Shore LIJ Health System Monterrey, Nov30-Dec1, 2007 Brachytherapy A procedure in therapeutic radiology that involves the irradiation of a target with
MRI Guided GYN Brachytherapy: Clinical Considerations
 MRI Guided GYN Brachytherapy: Clinical Considerations AAPM Junzo Chino MD Duke Radiation Oncology 8/8/2013 Disclosures none Learning Objectives Historical Context: Film based Brachytherapy Advantages of
MRI Guided GYN Brachytherapy: Clinical Considerations AAPM Junzo Chino MD Duke Radiation Oncology 8/8/2013 Disclosures none Learning Objectives Historical Context: Film based Brachytherapy Advantages of
2015 Radiology Coding Survival Guide
 2015 Radiology Coding Survival Guide Chapter 31: Clinical Brachytherapy (77750-77799) Clinical brachytherapy involves applying radioelements into or around a treatment field. CPT guidelines clarify that
2015 Radiology Coding Survival Guide Chapter 31: Clinical Brachytherapy (77750-77799) Clinical brachytherapy involves applying radioelements into or around a treatment field. CPT guidelines clarify that
PROSTATE CANCER BRACHYTHERAPY. Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College
 PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
Patient Safety Focused QA. LDR Brachytherapy Vrinda Narayana
 Patient Safety Focused QA LDR Brachytherapy Vrinda Narayana D < 2 Gy/h Old LDR Brachytherapy? Ra-226; Cs-137; Ir-192 New Gynecological; interstitial Pd-103; I-125; Cs-131 Prostate implants Eye plaques
Patient Safety Focused QA LDR Brachytherapy Vrinda Narayana D < 2 Gy/h Old LDR Brachytherapy? Ra-226; Cs-137; Ir-192 New Gynecological; interstitial Pd-103; I-125; Cs-131 Prostate implants Eye plaques
3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER
 SAUDI JOURNAL OF OBSTETRICS AND GYNECOLOGY VOLUME 11 NO. 2 1430 H - 2009 G 3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER DR YASIR BAHADUR 1, DR CAMELIA CONSTANTINESCU 2,
SAUDI JOURNAL OF OBSTETRICS AND GYNECOLOGY VOLUME 11 NO. 2 1430 H - 2009 G 3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER DR YASIR BAHADUR 1, DR CAMELIA CONSTANTINESCU 2,
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer
 Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
Image based Brachytherapy- HDR applications in Gynecological Tumors
 Image based Brachytherapy- HDR applications in Gynecological Tumors Yakov Pipman, D. Sc. North Shore LIJ Health System Sites amenable to treatment with HDR Brachytherapy GYN Breast Prostate Head and Neck
Image based Brachytherapy- HDR applications in Gynecological Tumors Yakov Pipman, D. Sc. North Shore LIJ Health System Sites amenable to treatment with HDR Brachytherapy GYN Breast Prostate Head and Neck
Varian Acuity BrachyTherapy Suite One Room Integrated Image-Guided Brachytherapy
 Varian Acuity BrachyTherapy Suite One Room Integrated Image-Guided Brachytherapy The Acuity BrachyTherapy Suite Integrating Imaging, Planning, and Treatment in a Single Room Each component draws on the
Varian Acuity BrachyTherapy Suite One Room Integrated Image-Guided Brachytherapy The Acuity BrachyTherapy Suite Integrating Imaging, Planning, and Treatment in a Single Room Each component draws on the
FEE RULES RADIATION ONCOLOGY FEE SCHEDULE CONTENTS
 Tel: +27-21-9494060 Fax: +27-21-9494112 E-mail: leon.gouws@cancercare.co.za FEE RULES RADIATION ONCOLOGY FEE SCHEDULE CONTENTS 1. EXTERNAL BEAM RADIATION... 2 2. PLANNING OF TREATMENT... 2 3. DELIVERY
Tel: +27-21-9494060 Fax: +27-21-9494112 E-mail: leon.gouws@cancercare.co.za FEE RULES RADIATION ONCOLOGY FEE SCHEDULE CONTENTS 1. EXTERNAL BEAM RADIATION... 2 2. PLANNING OF TREATMENT... 2 3. DELIVERY
INTRODUCTION PATIENT. J. Radiat. Res., 52, (2011)
") J. Radiat. Res., 52, 54 58 (2011) Regular Paper Intracavitary Combined with CT-guided Interstitial Brachytherapy for Locally Advanced Uterine Cervical Cancer: Introduction of the Technique and a Case Presentation
J. Radiat. Res., 52, 54 58 (2011) Regular Paper Intracavitary Combined with CT-guided Interstitial Brachytherapy for Locally Advanced Uterine Cervical Cancer: Introduction of the Technique and a Case Presentation
Basics of Cervix Brachytherapy. William Small, Jr., MD Professor and Chairman Loyola University Chicago
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Brachytherapy William Small, Jr., MD Professor and Chairman Loyola University Chicago Cervix Cancer Education Symposium, January
Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Brachytherapy William Small, Jr., MD Professor and Chairman Loyola University Chicago Cervix Cancer Education Symposium, January
Radiation Therapy for Prostate Cancer. Resident Dept of Urology General Surgery Grand Round November 24, 2008
 Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Brachytherapy The use of radioactive sources in close proximity to the target area for radiotherapy
 Brachytherapy The use of radioactive sources in close proximity to the target area for radiotherapy Interstitial Seven 192-Ir wires Interstitial implant for breast radiotherapy Intracavitary Three 137-Cs
Brachytherapy The use of radioactive sources in close proximity to the target area for radiotherapy Interstitial Seven 192-Ir wires Interstitial implant for breast radiotherapy Intracavitary Three 137-Cs
Limitations. General Clinical Applications of Brachytherapy Physics. Learning Objectives. Conflicts of Interest. University of Wisconsin - Madison
 General Clinical Applications of Brachytherapy Physics Bruce Thomadsen Limitations Due to file size limitations for this handout, many of the figures have had to be removed. I apologize for the lack of
General Clinical Applications of Brachytherapy Physics Bruce Thomadsen Limitations Due to file size limitations for this handout, many of the figures have had to be removed. I apologize for the lack of
How ICD-10 Affects Radiation Oncology. Presented by, Lashelle Bolton CPC, COC, CPC-I, CPMA
 How ICD-10 Affects Radiation Oncology Presented by, Lashelle Bolton CPC, COC, CPC-I, CPMA ICD-10 ICD-10-CM has added new challenges to the radiation oncology specialty. Approximately 220 ICD-9-CM codes
How ICD-10 Affects Radiation Oncology Presented by, Lashelle Bolton CPC, COC, CPC-I, CPMA ICD-10 ICD-10-CM has added new challenges to the radiation oncology specialty. Approximately 220 ICD-9-CM codes
The New ICRU/GEC ESTRO Report in Clinical Practice. Disclosures
 The New ICRU/GEC ESTRO Report in Clinical Practice Christian Kirisits, MSc, PhD; Richard Pötter, MD Medical University of Vienna, Vienna, Austria On behalf of the Committee: B. Erickson, C. Haie Meder,
The New ICRU/GEC ESTRO Report in Clinical Practice Christian Kirisits, MSc, PhD; Richard Pötter, MD Medical University of Vienna, Vienna, Austria On behalf of the Committee: B. Erickson, C. Haie Meder,
MR-Guided Brachytherapy
 MR-Guided Brachytherapy Joann I. Prisciandaro, Ph.D. The Department of Radiation Oncology University of Michigan Outline Traditional 2D technique for brachytherapy treatment planning Transition to MR-guided
MR-Guided Brachytherapy Joann I. Prisciandaro, Ph.D. The Department of Radiation Oncology University of Michigan Outline Traditional 2D technique for brachytherapy treatment planning Transition to MR-guided
Outline - MRI - CT - US. - Combinations of imaging modalities for treatment planning
 Imaging Outline - MRI - CT - US - Combinations of imaging modalities for treatment planning Imaging Part 1: MRI MRI for cervical cancer high soft tissue contrast multiplanar imaging MRI anatomy: the normal
Imaging Outline - MRI - CT - US - Combinations of imaging modalities for treatment planning Imaging Part 1: MRI MRI for cervical cancer high soft tissue contrast multiplanar imaging MRI anatomy: the normal
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy
 Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
Comparison of rectal and bladder ICRU point doses to the GEC ESTRO volumetric doses in Cervix cancer
 Comparison of rectal and bladder ICRU point doses to the GEC ESTRO volumetric doses in Cervix cancer Poster No.: RO-0049 Congress: RANZCR FRO 202 Type: Authors: Scientific Exhibit G. Govindarajulu, A.
Comparison of rectal and bladder ICRU point doses to the GEC ESTRO volumetric doses in Cervix cancer Poster No.: RO-0049 Congress: RANZCR FRO 202 Type: Authors: Scientific Exhibit G. Govindarajulu, A.
Challenging Cases in Cervical Cancer: Parametrial Boosting. Beth Erickson, MD, FACR, FASTRO Medical College Wisconsin
 Challenging Cases in Cervical Cancer: Parametrial Boosting Beth Erickson, MD, FACR, FASTRO Medical College Wisconsin Disclosure Chart Rounds participant No COI Learning Objectives Discuss the challenges
Challenging Cases in Cervical Cancer: Parametrial Boosting Beth Erickson, MD, FACR, FASTRO Medical College Wisconsin Disclosure Chart Rounds participant No COI Learning Objectives Discuss the challenges
Advances in Treatment of Cancer by Brachytherapy in Kenya, in Particular, Prostate Cancer
 Research Article imedpub Journals www.imedpub.com Journal Of Medical Physics And Applied Sciences ISSN 2574-285X DOI: 1.21767/2574-285X.12 Advances in Treatment of Cancer by Brachytherapy in Kenya, in
Research Article imedpub Journals www.imedpub.com Journal Of Medical Physics And Applied Sciences ISSN 2574-285X DOI: 1.21767/2574-285X.12 Advances in Treatment of Cancer by Brachytherapy in Kenya, in
Advances in Gynecologic Brachytherapy
 Advances in Gynecologic Brachytherapy Anuj V Peddada, M.D. Director Department of Radiation Oncology Penrose Cancer Center Colorado Springs, CO USA Brachytherapy Issues in Gyn/onc Cervix Endometrial Rational
Advances in Gynecologic Brachytherapy Anuj V Peddada, M.D. Director Department of Radiation Oncology Penrose Cancer Center Colorado Springs, CO USA Brachytherapy Issues in Gyn/onc Cervix Endometrial Rational
Enterprise Interest None
 Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring)
") Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
Brachytherapy in Africa
 Brachytherapy in Africa Deanine Halliman PhD Sr. Director Medical Affairs Elekta Brachytherapy Burden of cervical cancer in Africa est. 2012 incidence per 100,000 women Bouassa M, et al. Cervical cancer
Brachytherapy in Africa Deanine Halliman PhD Sr. Director Medical Affairs Elekta Brachytherapy Burden of cervical cancer in Africa est. 2012 incidence per 100,000 women Bouassa M, et al. Cervical cancer
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer?
 Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas Dept. of Medical Physics & Engineering, Strahlenklinik, Klinikum Offenbach GmbH 63069 Offenbach, Germany
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas Dept. of Medical Physics & Engineering, Strahlenklinik, Klinikum Offenbach GmbH 63069 Offenbach, Germany
Prostate Cancer Treatment
 Scan for mobile link. Prostate Cancer Treatment Prostate cancer overview Prostate cancer is the most common form of cancer in American men, most prevalent in men over age 65 and fairly common in men 50-64
Scan for mobile link. Prostate Cancer Treatment Prostate cancer overview Prostate cancer is the most common form of cancer in American men, most prevalent in men over age 65 and fairly common in men 50-64
Johannes C. Athanasios Dimopoulos
 BrachyNext Symposium Miami Beach, USA, May 30 31, 2014 Imaging Modalities: Current Challenges and Future Directions Johannes C. Athanasios Dimopoulos Imaging Modalities: Current Challenges and Future Directions
BrachyNext Symposium Miami Beach, USA, May 30 31, 2014 Imaging Modalities: Current Challenges and Future Directions Johannes C. Athanasios Dimopoulos Imaging Modalities: Current Challenges and Future Directions
Cervical Cancer Treatment
 Scan for mobile link. Cervical Cancer Treatment Cervical cancer overview Cervical cancer occurs in the cervix, the part of the female reproductive system that connects the vagina and uterus. Almost all
Scan for mobile link. Cervical Cancer Treatment Cervical cancer overview Cervical cancer occurs in the cervix, the part of the female reproductive system that connects the vagina and uterus. Almost all
The Role of Radiation in the Management of Gynecologic Cancers. Scott Glaser, MD
 The Role of Radiation in the Management of Gynecologic Cancers Scott Glaser, MD Nothing to disclose DISCLOSURE Outline The role of radiation in: Endometrial Cancer Adjuvant Medically inoperable Cervical
The Role of Radiation in the Management of Gynecologic Cancers Scott Glaser, MD Nothing to disclose DISCLOSURE Outline The role of radiation in: Endometrial Cancer Adjuvant Medically inoperable Cervical
External Beam Radiotherapy for Prostate Cancer
 External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
Pulsed Dose Rate for GYN Brachytherapy
 Pulsed Dose Rate for GYN Brachytherapy Firas Mourtada,, Ph.D. Department of Radiation Physics Dose equivalency to LDR Brief Introduction Radiobiology Dose Distribution: Radial dose function Source anisotropy
Pulsed Dose Rate for GYN Brachytherapy Firas Mourtada,, Ph.D. Department of Radiation Physics Dose equivalency to LDR Brief Introduction Radiobiology Dose Distribution: Radial dose function Source anisotropy
HDR Brachytherapy: Results and Future Studies in Monotherapy
 HDR Brachytherapy: Results and Future Studies in Monotherapy Nikolaos Zamboglou and Nikolaos Tselis Strahlenklinik Klinikum Offenbach - Germany Prostate Brachytherapy UK & Ireland Conference 2013 Comparison
HDR Brachytherapy: Results and Future Studies in Monotherapy Nikolaos Zamboglou and Nikolaos Tselis Strahlenklinik Klinikum Offenbach - Germany Prostate Brachytherapy UK & Ireland Conference 2013 Comparison
Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej. The role of brachytherapy in recurrent. oral cavity
 Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej The role of brachytherapy in recurrent tumours of the tongue and fundus of the oral cavity Janusz Skowronek, MD, PhD, Ass. Prof.
Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej The role of brachytherapy in recurrent tumours of the tongue and fundus of the oral cavity Janusz Skowronek, MD, PhD, Ass. Prof.
BRACHYTHERAPY IN HORSES
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk BRACHYTHERAPY IN HORSES Author : DAVID DONALDSON Categories : Vets Date : June 16, 2014 DAVID DONALDSON BVSc(Hons), DipECVO,
Vet Times The website for the veterinary profession https://www.vettimes.co.uk BRACHYTHERAPY IN HORSES Author : DAVID DONALDSON Categories : Vets Date : June 16, 2014 DAVID DONALDSON BVSc(Hons), DipECVO,
LDR Monotherapy vs. HDR Monotherapy
 Abstract No. 1234 LDR Monotherapy vs. HDR Monotherapy Is it time for LDR to retire? Gerard Morton 2 LDR Seed Brachytherapy First 2000 LDR patients from BCCA Low and Intermediate Risk LDR Implant Morris
Abstract No. 1234 LDR Monotherapy vs. HDR Monotherapy Is it time for LDR to retire? Gerard Morton 2 LDR Seed Brachytherapy First 2000 LDR patients from BCCA Low and Intermediate Risk LDR Implant Morris
Who Should Know Radiation Oncology Coding?
 Why Should We Learn Radiation Oncology Coding? Terry Wu, Ph.D. Chief Physicist Radiation Oncology Department Willis-Knighton Cancer Center Who Should Know Radiation Oncology Coding? Radiation Oncologist
Why Should We Learn Radiation Oncology Coding? Terry Wu, Ph.D. Chief Physicist Radiation Oncology Department Willis-Knighton Cancer Center Who Should Know Radiation Oncology Coding? Radiation Oncologist
University Medical Center Utrecht The Netherlands
 University Medical Center Utrecht The Netherlands Metha Maenhout, MD: PHD student Maaike Koelink: Specialist RTT Wilfred de Vries: Physicist Assistant MED-00005 [00] UMC Utrecht Radiotherapy Department
University Medical Center Utrecht The Netherlands Metha Maenhout, MD: PHD student Maaike Koelink: Specialist RTT Wilfred de Vries: Physicist Assistant MED-00005 [00] UMC Utrecht Radiotherapy Department
2/14/09. Why Discuss this topic? Managing Local Recurrences after Radiation Failure. PROSTATE CANCER Second Treatment
 Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Image guided brachytherapy in cervical cancer Clinical Aspects
 Image guided brachytherapy in cervical cancer Clinical Aspects Richard Pötter MD Department of Radiation Oncology, Medical University of Vienna, Austria ICARO-2, IAEA, Vienna, June, 22, 2017 Outline Tumor
Image guided brachytherapy in cervical cancer Clinical Aspects Richard Pötter MD Department of Radiation Oncology, Medical University of Vienna, Austria ICARO-2, IAEA, Vienna, June, 22, 2017 Outline Tumor
Basic Fundamentals & Tricks of the Trade for Intracavitary Radiotherapy for Cervix Cancer. Paula A. Berner, B.S., CMD, FAAMD
 Basic Fundamentals & Tricks of the Trade for Intracavitary Radiotherapy for Cervix Cancer Paula A. Berner, B.S., CMD, FAAMD Conflicts of Interest None to disclose Equipment Philips Healthcare, USA Nucletron
Basic Fundamentals & Tricks of the Trade for Intracavitary Radiotherapy for Cervix Cancer Paula A. Berner, B.S., CMD, FAAMD Conflicts of Interest None to disclose Equipment Philips Healthcare, USA Nucletron
Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer
 Techniques in Head and Neck Cancer") 1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
National System for Incident Reporting in Radiation Therapy (NSIR-RT) Taxonomy
 Taxonomy") Canadian Partnership for Quality Radiotherapy (CPQR) National System for Incident Reporting in Radiation Therapy (NSIR-RT) National System for Incident Reporting in Radiation Therapy (NSIR-RT) Taxonomy
Canadian Partnership for Quality Radiotherapy (CPQR) National System for Incident Reporting in Radiation Therapy (NSIR-RT) National System for Incident Reporting in Radiation Therapy (NSIR-RT) Taxonomy
Partial Breast Irradiation using adaptive MRgRT
 Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
20 Prostate Cancer Dan Ash
 20 Prostate Cancer Dan Ash 1 Introduction Prostate cancer is a disease of ageing men for which the aetiology remains unknown. The incidence rises up to 30 to 40% in men over 80. The symptoms of localised
20 Prostate Cancer Dan Ash 1 Introduction Prostate cancer is a disease of ageing men for which the aetiology remains unknown. The incidence rises up to 30 to 40% in men over 80. The symptoms of localised
ARROCase: Locally Advanced Endometrial Cancer
 ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
EORTC Member Facility Questionnaire
 Page 1 of 9 EORTC Member Facility Questionnaire I. Administrative Data Name of person submitting this questionnaire Email address Function Phone Institution Address City Post code Country EORTC No Enter
Page 1 of 9 EORTC Member Facility Questionnaire I. Administrative Data Name of person submitting this questionnaire Email address Function Phone Institution Address City Post code Country EORTC No Enter
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments
 Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
Disclosure SBRT. SBRT for Spinal Metastases 5/2/2010. No conflicts of interest. Overview
 Stereotactic Body Radiotherapy (SBRT) for Recurrent Spine Tumors Arjun Sahgal M.D., F.R.C.P.C. Assistant Professor Princess Margaret Hospital Sunnybrook Health Sciences Center University of Toronto Department
Stereotactic Body Radiotherapy (SBRT) for Recurrent Spine Tumors Arjun Sahgal M.D., F.R.C.P.C. Assistant Professor Princess Margaret Hospital Sunnybrook Health Sciences Center University of Toronto Department
Corporate Medical Policy
 Corporate Medical Policy Intensity Modulated Radiation Therapy (IMRT) of Abdomen and File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_abdomen_and_pelvis
Corporate Medical Policy Intensity Modulated Radiation Therapy (IMRT) of Abdomen and File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_abdomen_and_pelvis
Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases
 Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases CASE STUDY Institution: Odette Cancer Centre Location: Sunnybrook
Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases CASE STUDY Institution: Odette Cancer Centre Location: Sunnybrook
EMBRACE- Studien Analysen und Perspektiven
 EMBRACE- Studien Analysen und Perspektiven Alina Sturdza EMBRACE study group Outline Historical development of GEC ESTRO Gyn Group Historical development of the MRI compatible applicators Presentation
EMBRACE- Studien Analysen und Perspektiven Alina Sturdza EMBRACE study group Outline Historical development of GEC ESTRO Gyn Group Historical development of the MRI compatible applicators Presentation
The Canadian National System for Incident Reporting in Radiation Treatment (NSIR-RT) Taxonomy March 11, 2015
 Taxonomy March 11, 2015") The Canadian National System for Incident Reporting in Radiation Treatment (NSIR-RT) Taxonomy March 11, 2015 Taxonomy Data Category Number Description Data Fields and Menu Choices 1. Impact 1.1 Incident
The Canadian National System for Incident Reporting in Radiation Treatment (NSIR-RT) Taxonomy March 11, 2015 Taxonomy Data Category Number Description Data Fields and Menu Choices 1. Impact 1.1 Incident
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer?
 Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas 1,3, Natasa Milickovic 1, Nikolaos Zamboglou 2 1 Dept. of Medical Physics & Engineering, 2 Strahlenklinik,
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas 1,3, Natasa Milickovic 1, Nikolaos Zamboglou 2 1 Dept. of Medical Physics & Engineering, 2 Strahlenklinik,
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia
 Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Prostate Cancer. What is prostate cancer?
 Scan for mobile link. Prostate Cancer Prostate cancer is a tumor of the prostate gland, which is located in front of the rectum and below the bladder. Your doctor may perform a physical exam, prostate-specific
Scan for mobile link. Prostate Cancer Prostate cancer is a tumor of the prostate gland, which is located in front of the rectum and below the bladder. Your doctor may perform a physical exam, prostate-specific
BRACHYTHERAPY FOR PROSTATE CANCER. Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital
, FRANZCR Radiation Oncologist, The Canberra Hospital") BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
High-Dose-Rate Orthogonal Intracavitary Brachytherapy with 9 Gy/Fraction in Locally Advanced Cervical Cancer: Is it Feasible??
 DOI 10.1007/s13224-015-0812-8 ORIGINAL ARTICLE High-Dose-Rate Orthogonal Intracavitary Brachytherapy with 9 Gy/Fraction in Locally Advanced Cervical Cancer: Is it Feasible?? Saptarshi Ghosh 1 Pamidimukalabramhananda
DOI 10.1007/s13224-015-0812-8 ORIGINAL ARTICLE High-Dose-Rate Orthogonal Intracavitary Brachytherapy with 9 Gy/Fraction in Locally Advanced Cervical Cancer: Is it Feasible?? Saptarshi Ghosh 1 Pamidimukalabramhananda
NIA MAGELLAN HEALTH RADIATION ONCOLOGY CODING STANDARD. Dosimetry Planning
 NIA MAGELLAN HEALTH RADIATION ONCOLOGY CODING STANDARD Dosimetry Planning CPT Codes: 77295, 77300, 77301, 77306, 77307, 77321, 77316, 77317, 77318, 77331, 77399 Original Date: April, 2011 Last Reviewed
NIA MAGELLAN HEALTH RADIATION ONCOLOGY CODING STANDARD Dosimetry Planning CPT Codes: 77295, 77300, 77301, 77306, 77307, 77321, 77316, 77317, 77318, 77331, 77399 Original Date: April, 2011 Last Reviewed
3D CONFORMATIONAL INTERSTITIAL BRACHYTHERAPY PLANNING FOR SOFT TISSUE SARCOMA
 3D CONFORMATIONAL INTERSTITIAL BRACHYTHERAPY PLANNING FOR SOFT TISSUE SARCOMA Alina TĂNASE 1,3, M. DUMITRACHE 2,3, O. FLOREA 1 1 Emergency Central Military Hospital Dr. Carol Davila Bucharest, Romania,
3D CONFORMATIONAL INTERSTITIAL BRACHYTHERAPY PLANNING FOR SOFT TISSUE SARCOMA Alina TĂNASE 1,3, M. DUMITRACHE 2,3, O. FLOREA 1 1 Emergency Central Military Hospital Dr. Carol Davila Bucharest, Romania,
HDR Applicators and Dosimetry*
 HDR Applicators and Dosimetry* Jason Rownd, MS Medical College of Wisconsin *with a too much radiobiology Objectives Review the radiobiology of brachytherapy-linear quadratic model. Understand how to convert
HDR Applicators and Dosimetry* Jason Rownd, MS Medical College of Wisconsin *with a too much radiobiology Objectives Review the radiobiology of brachytherapy-linear quadratic model. Understand how to convert
Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology
 Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology The head and neck cancer service provides training in the diagnosis, management, treatment, and follow-up care of head
Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology The head and neck cancer service provides training in the diagnosis, management, treatment, and follow-up care of head
Salvage HDR Brachytherapy. Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK
 Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
MRI in Cervix and Endometrial Cancer
 28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
Course Directors: Teaching Staff: Guest Lecturers: Local Organiser: ESTRO coordinator: Melissa Vanderijst, project manager (BE)
") ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Prague, Czech Republic 22-26 October 2017 Course Directors: Richard
ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Prague, Czech Republic 22-26 October 2017 Course Directors: Richard
A SIMPLE METHOD OF OBTAINING EQUIVALENT DOSES FOR USE IN HDR BRACHYTHERAPY
 PII S0360-3016(99)00330-2 Int. J. Radiation Oncology Biol. Phys., Vol. 46, No. 2, pp. 507 513, 2000 Copyright 2000 Elsevier Science Inc. Printed in the USA. All rights reserved 0360-3016/00/$ see front
PII S0360-3016(99)00330-2 Int. J. Radiation Oncology Biol. Phys., Vol. 46, No. 2, pp. 507 513, 2000 Copyright 2000 Elsevier Science Inc. Printed in the USA. All rights reserved 0360-3016/00/$ see front
MEDICAL POLICY SUBJECT: BRACHYTHERAPY OR RADIOACTIVE SEED IMPLANTATION FOR PROSTATE CANCER
 MEDICAL POLICY SUBJECT: BRACHYTHERAPY OR PAGE: 1 OF: 6 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy
MEDICAL POLICY SUBJECT: BRACHYTHERAPY OR PAGE: 1 OF: 6 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy
Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT)
") Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT) The Institute for Clinical and Economic Review (ICER) has published appraisals on multiple management options for clinically-localized,
Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT) The Institute for Clinical and Economic Review (ICER) has published appraisals on multiple management options for clinically-localized,
Dose-Volume Histogram Analysis in Point A-based Dose Prescription of High-dose-rate Brachytherapy for Cervical Carcinoma
 Showa Univ J Med Sci 30 2, 227 235, June 2018 Original Dose-Volume Histogram Analysis in Point A-based Dose Prescription of High-dose-rate Brachytherapy for Cervical Carcinoma Rei KOBAYASHI 1, Yoshikazu
Showa Univ J Med Sci 30 2, 227 235, June 2018 Original Dose-Volume Histogram Analysis in Point A-based Dose Prescription of High-dose-rate Brachytherapy for Cervical Carcinoma Rei KOBAYASHI 1, Yoshikazu
CT Guided Contouring: Challenges and Pitfalls
 CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
SYSTEMS IN BRACHYTHERAPY. Alfredo Polo MD, PhD Division of Human Health International Atomic Energy Agency
 SYSTEMS IN BRACHYTHERAPY Alfredo Polo MD, PhD Division of Human Health International Atomic Energy Agency SYSTEMS IN BRACHYTHERAPY: WHAT IS IN A NAME? SYSTEMS FOR DOSE PRESCRIPTION IN BRACHYTHERAPY: GENERAL
SYSTEMS IN BRACHYTHERAPY Alfredo Polo MD, PhD Division of Human Health International Atomic Energy Agency SYSTEMS IN BRACHYTHERAPY: WHAT IS IN A NAME? SYSTEMS FOR DOSE PRESCRIPTION IN BRACHYTHERAPY: GENERAL
High-Dose Rate Temporary Prostate Brachytherapy. Original Policy Date
 MP 8.01.15 High-Dose Rate Temporary Prostate Brachytherapy Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return
MP 8.01.15 High-Dose Rate Temporary Prostate Brachytherapy Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return
Stereotactic MR-guided adaptive radiation therapy (SMART) for locally advanced pancreatic tumors
 for locally advanced pancreatic tumors") Stereotactic MR-guided adaptive radiation therapy (SMART) for locally advanced pancreatic tumors Anna Bruynzeel, Radiation Oncologist VU University Medical Center, Amsterdam, The Netherlands Current standard
Stereotactic MR-guided adaptive radiation therapy (SMART) for locally advanced pancreatic tumors Anna Bruynzeel, Radiation Oncologist VU University Medical Center, Amsterdam, The Netherlands Current standard
Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK
 Lead Group Log Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK Cervical Cancer treatment Treatment planning should be made on a multidisciplinary
Lead Group Log Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK Cervical Cancer treatment Treatment planning should be made on a multidisciplinary
Ovarian Cancer Survival. Ovarian Cancer Follow-up. Ovarian Cancer Treatment. Management of Recurrent Ovarian Carcinoma. 15,520 cancer deaths
 Management of Recurrent Ovarian Carcinoma Lee-may Chen, M.D. Department of Obstetrics, Gynecology, & Reproductive Sciences UCSF Comprehensive Cancer Center Ovarian Cancer Survival United States, 28: 1
Management of Recurrent Ovarian Carcinoma Lee-may Chen, M.D. Department of Obstetrics, Gynecology, & Reproductive Sciences UCSF Comprehensive Cancer Center Ovarian Cancer Survival United States, 28: 1
High dose-rate tandem and ovoid brachytherapy in cervical cancer: dosimetric predictors of adverse events
 Romano et al. Radiation Oncology (2018) 13:129 https://doi.org/10.1186/s13014-018-1074-2 RESEARCH Open Access High dose-rate tandem and ovoid brachytherapy in cervical cancer: dosimetric predictors of
Romano et al. Radiation Oncology (2018) 13:129 https://doi.org/10.1186/s13014-018-1074-2 RESEARCH Open Access High dose-rate tandem and ovoid brachytherapy in cervical cancer: dosimetric predictors of
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer
 A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
HYPERTHERMIA in CERVIX and VAGINA CANCER. J. van der Zee
 HYPERTHERMIA in CERVIX and VAGINA CANCER J. van der Zee ESTRO 2006 Deep hyperthermia in Rotterdam HYPERTHERMIA in CERVIX and VAGINA CANCER ESTRO 2006 Hyperthermia and radiotherapy in primary advanced cervix
HYPERTHERMIA in CERVIX and VAGINA CANCER J. van der Zee ESTRO 2006 Deep hyperthermia in Rotterdam HYPERTHERMIA in CERVIX and VAGINA CANCER ESTRO 2006 Hyperthermia and radiotherapy in primary advanced cervix