Richard P Junghans, PhD, MD
|
|
|
- Philippa Paul
- 5 years ago
- Views:
Transcription
1 CANCER GENE THERAPY WITH DESIGNER T CELLS: TOXICITY VERSUS ACTIVITY Richard P Junghans, PhD, MD Director, Biotherapeutics Development Lab Associate Professor of Surgery and Medicine Boston University School of Medicine Chief, Division of Surgical Research Roger Williams Medical Center Providence, RI, USA No commercial relationships to disclose.

2 Anti- CEA Normal T cells Designer T cells IgTCR = Immunoglobulin-T cell receptor CIR = Chimeric immune receptor
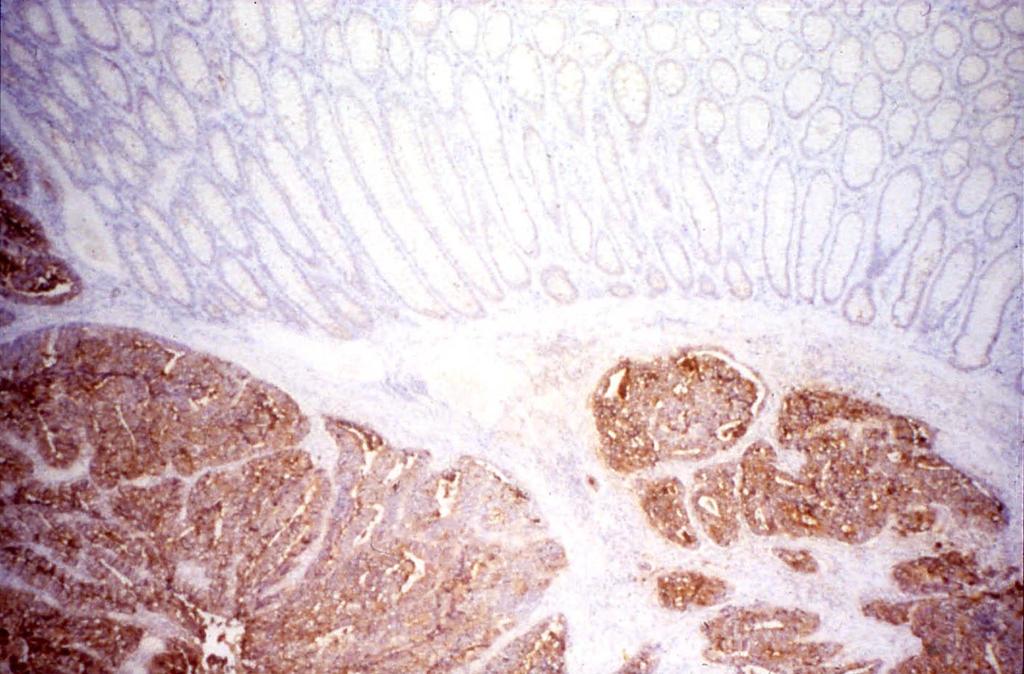
3 Carcinoembryonic antigen (CEA) o Expression High on tumor, low on normal Topological sequestration o High clinical relevance: On colorectal, breast, pancreas, lung, others More than 100,000 deaths/yr for CEA+ tumors
4
5 CLINICAL TRIAL Clinical Data: 1 st Generation Phase I Study of Anti-CEA Designer T Cells in Adenocarcinoma ( 1st generation ) FDA BB IND 7301

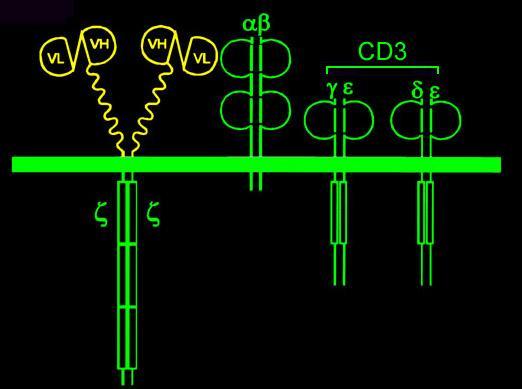
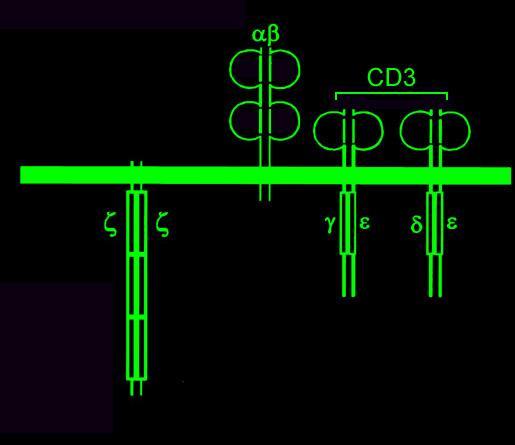
6 TCR Anti-Cancer T Cell Gene Therapy Gene-Modified TCR
7 Interventions o Phlebotomy/Apheresis o Isolate patient s peripheral blood mononuclear cells (PBMC) o Activate/transduce with IgTCR o Expand in IL2 o Harvest cells equal to dose; Infuse o Monitor for Toxicity/Response
8 Clinical Summary o Number of doses administered (24) o Patients treated (7): 5 colorectal, 2 breast o Doses sizes administered 1 x 10 9, 3 x 10 9, 1 x 10 10, 3 x 10 10, 1 x cells
9 Pharmacokinetics Rapid Systemic Loss
10 CEA (NG/ML) Response: Proof of Principle T Cells CEA Increasing pain Pain resolved Day of Treatment BUT! Time-Limited in Duration
11 Pharmacodynamics o Immunogenicity: None. 0/7 with plasma reactivity against designer T cells o IL2 arm: Systemically active. Positive for NK cell expansion, T cells stable
12 Toxicity o Probably related or Definitely related No grade III toxicity, one grade IV toxicity (grade II fever >> grade IV SVT) No delayed grade III, IV toxicity Positive for low grade fevers, mild GI symptoms (<grade III) Transient hypoxemia (O 2 sat<90%) with high T cell dose
13 (-) IL 2 Toxicity Name Sex Age Diagnosis Dose Fever (24h) Adverse Events (Grade III-IV) Relatedness MS Dose 1 (6/10/98) Dose 2 (6/24/98) Dose 3 (7/8/98) F 75 Colon Ca 1x10 9 3x10 9 1x F Bilirubin GI Bleed * Death * Possibly (temporal only) # Possibly (temporal only) # RH Dose 1 (7/13/99) Dose 2 (7/27/98) Dose 3 (8/10/98) Dose 4 (8/26/98) M 55 Rectal Ca 1x10 9 3x10 9 1x x F 101 F <101 F <101 F Anemia Possibly (temporal only) # DB Dose 1 (7/15/98) Dose 2 (7/29/98) Dose 3 (8/12/98) Dose 4 (8/26/98) M 54 Colon Ca 1x10 9 3x10 9 1x x F Rigors F Bilirubin (9/23/98;28 days) Possibly (temporal only) # HF Dose 1 (8/11/98) Dose 2 (8/25/98) Dose 3 (9/14/98) Dose 4 (10/14/98) Dose 5 (2/1/99) M 75 Colon Ca 1x x x x x A Flutter* A Flutter Death * (2/3/99) Possibly (temporal only) Possibly (temporal only) # GT Dose 1 (6/8/99) M 69 Rectal Ca 1x F SVT/Hypotension* Rigors Probably (to fever) (+) IL 2 Name Sex Age Diagnosis Dose Fever (24H) Adverse Events (Grade III-IV) Relatedness JD Dose 1 (9/23/98) Dose 2 (10/5/98) Dose 3 (10/19/98) Dose 4 (11/2/98) F 39 Breast CA 1x10 9 3x10 9 1x x F 102 F EM Dose 1 (11/4/98) Dose 2 (11/16/98) Dose 3 (11/30/98) F 47 Breast CA 1x10 9 3x10 9 1x F Bilirubin Death* Possibly (temporal only ) # Possibly (temporal only) # * Event generating SAE report # Current progression
14 Patient GT o 69M, rectal ca, baseline RBBB Febrile 103.8F (39.9C) within 6 hrs SVT, responsive to IV beta blockers blood pressure, 20 mm drop asymptomatic o blood cultures neg, cell cultures neg o expect it: >>immune response indicators recommend as pharmacodynamic measure o avoid predisposing cardiac conditions
15 Temperature Heart Rate GT Vital Signs Temperature Heart Rate :18 13:00 13:40 14:34 14:50 15:20 17:34 22:34 0:10 5:00 11:00 18:00 21:00 22:00 15:00 22:00 24:00:00 2:00 Time (Hour)
16 CEA (NG/ML) T Cells CEA Increasing pain Pain resolved Day of Treatment

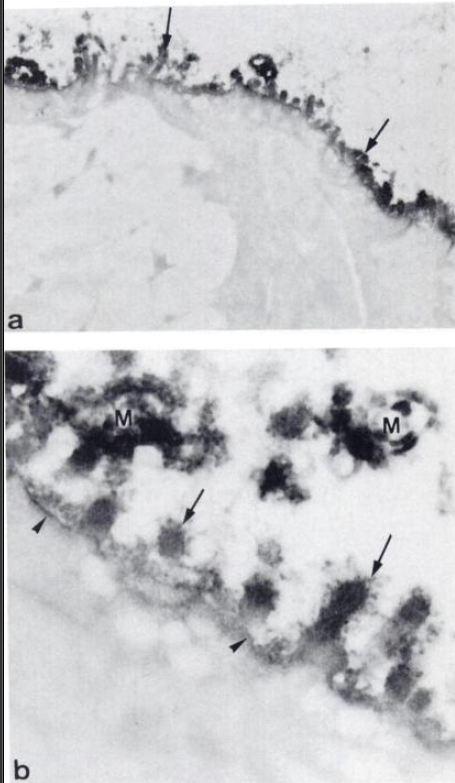
17 GVHD in bowel Apoptotic bodies at base of crypts

18 GT biopsy: no apoptotic bodies Conclude: cytokine syndrome
19 CEA targeting by TCR Parkhurst et al, ASGCT 2010 o Cloned murine TCR for HLA-A2 presented CEA peptide o TCR gene transfer (not CAR ~ 1 st gen), 3 subjects Lymphodepletion 2-4 x 10^8 cells 1-20% engraftment o Toxicity against bowel, all had grade 2/3 diarrhea T cell infiltration epithelial destruction o Some tumor partial response noted o However, concluded not safe to target CEA What is the difference???


20 MHC class I on enterocytes Topology MHC I: Primarily basal expression


21 CEA on enterocytes Antigen sequestration: CEA confined to microvilli
22 Lesson on Ag selection o What are normal tissues expressing? o What is topology of expression? Epithelial cancers Antigens Expression CEA Lumenal Class I Basal Her2 Basal CA IX Basal
23 Liver, etc Infuse Causes of Activity Loss? Tissues T T * Blood T #1 #2 T * Cancer
24 New Directions: Hypotheses o Tumor eradication would follow if EITHER #1. T cells persisted systemically [QUANTITY] ( bypass co-stimulation ) OR #2. T cells expanded intratumorally [QUALITY] ( provide co-stimulation )
25 Hypothesis 2: 2 nd Generation Provide co-stimulation Incorporate Signal 2 into designer T cells
26 Immunology 101
27 T Cell Activation Antigen Presenting Cell MHC B7 TCR CD T Cell o o o Gene expression - Cytokines (IL-2, 4, IFN-, etc) - Surface molecules (CD25, CD40L, etc) Cytotoxicity Proliferation
28 Designer T Cells First Generation o IgTCR chimeric immunoglobulin T cell receptor Tumor Cell Antigen Ig TCR 1 Modified T Cell CD28 MIPCEA Advantage: IgTCR provides Signal 1: adequate T cell cytotoxicity. Disadvantage: Lacking Signal 2, undergoes Activation-Induced Cell Death (AICD) after killing target cells. [HYPOTHESIS]
29 Signals o Signal 1: Activated: T cells kill tumor >> and die by AICD Resting: anergy o Signal 1+2: Activated: T cells kill tumor >> and proliferate Resting: activation, see above
30 1 st and 2 nd Gen Constructs IgTCR Ig28TCR ( Tandem ) VL VH VH VL VL VH VH VL Signal 1 Signal 1+2
31 2nd Gen T Cell Tumor-Induced Proliferation Expansion on MIP101 Expansion on MIPCEA 1.0E+07 CEA(-) 1.0E+07 CEA(+) 8.0E E E E+06 UnTd IgTCR Tandem 6.0E E+06 UnTd IgTCR Tandem 2.0E E E+00 Day 0 Day 3 Day 7 0.0E+00 Day 0 Day 3 Day 7 Day Day Emtage et al. Clin Cancer Res 2008
32 Adjuvant model: Superior in vivo Tumor Suppression by 2nd Gen T Cells Tumor size (mm ) 2 Tumor size (mm ) 300 MIP MIPCEA 250 CEA(-) 250 CEA(+) Untransduced IgTCR Tandem 200 2Untransduced IgTCR 150 Tandem Day post tumor cell injection Day post tumor cell injection
33 Phase Ia/Ib Trial of 2 nd Generation Anti-CEA Designer T Cells in Adenocarcinoma FDA BB IND 10791
34 Hypotheses o 2nd gen Signal 1+2 designer T cells will escape AICD and proliferate intratumorally o Expanding designer T cells in tumor will maintain anti-tumor activity until tumor elimination
35 -IL2 Pt # Cohort 1x10 9 1x x10 11 #1 #2 #3 #4 #5 #6 I II X X X T Cell Dose, Number of Cells X X X Phase Ia Safety Study Design #7 #8 #9 III X X X Any CEA+ cancer Funded by FDA Orphan Products Division
36 Summary 2 nd Generation CEA o 5 patients treated 1 st cohort completed 2 nd cohort in process o Safety, no SAEs (no new risks with 2 nd gen) o Responses one minor (brain and lung) one SD 12+ months o Continue in escalation o Need to assess value of IL2 supplementation
37 Hypothesis #1 T Cell Engraftment Auto-Transplant: Engraft designer T cells via lympho-expansive capacities of the body after lympho-depletion treatments (Bypass co-stimulation)
38
39 NMA Melanoma TILs Tumor Harvest Melanoma CD8+ TIL X Non-myeloablative (NMA) Conditioning Hematologic Recovery 6/13 major responses Tumor Response Dudley et al Science 2002;298:850
 Conditioning +IL2 low dose (outpatient) Hematologic Recovery CIR+ CD3+")
40 Prostate Cancer T Cell Harvest CIR+ Ex vivo gene therapy Anti-PSMA designer T cells Non-myeloablative (NMA) Conditioning +IL2 low dose (outpatient) Hematologic Recovery CIR+ CD3+ Tumor Response
41 Prostate Specific Membrane Antigen (PSMA) o Surface membrane glycoprotein 100,000 Daltons o Unrelated to PSA o Normal prostate epithelium and vasculature (reportedly on type II astrocytes?) o Elevated expression in metastatic lesions and hormone refractory disease o High clinical relevance: 28,000 deaths per year from PSMA+ prostate tumors o Antibody (3D8) from G. Murphy and A. Boynton

42 PSMA on prostate cancer



43 Normal tissue PSMA Tasch et al. Crit Rev Immunol 2001 Prostatic epithelium and vasculature Dispensable white gray And brain??!! Kinoshita et al. W J Surg 2006 Sacha et al. Neuroscience 2007
44 Thought: If DTC toxic against brain, then best to have a format that allows T cell suppression and escape T cell quantity: Can be controlled with infusion Engraftment with vast numbers hard to control But: No 1 st gen infused will be therapeutically successful T cell quality (potency): After remove steroid suppression: 1 st gen DTC won t reactivate 2 nd gen will Conclude: 1 st gen safe with engraftment (2 nd gen safe with infusion)
45 Phase I Study of Autologous Transplantation of Anti-PSMA Designer T Cells after NMA Conditioning in Prostate Cancer BB IND 12084
46 Treatment Schema Designer T cells modify T cells microbiologic testing NMA T cell infusion T cell collection G-CSF PSC collection chemotherapy start IL end IL2-21* -20* -16* Study Day Biopsy* CTX 60 mg/kg d-7, d-6 Fludarabine 25 mg/m2 d-5 to d-1
47 Phase I Study Enrollment Plan o T Cell Dose, Number of Cells o Pt # Cohort o #1 X o #2 I X o #3 X o #4 X o #5 X o #6 X o #7 X o #8 II X o #9 X o #10 X o #11 X o #12 X o (Bx) o #13 X o #14 III X o #15 X o #16 X o #17 X o #18 X omonitoring Safety Designer T cell persistence/expansion in blood In tumor Tumor response Funded in part by US Army
48 Counts per ul Counts per ul Peripheral Blood Recovery o Chemo d-8 to d-2 o T cells d0 o IL2 start d0-d28 o ANC=0 x5-8 d Recovery ANC> Pt #1 ANC and ALC over Time T cells days ANC ALC T cells days AC ALC
49 IL2 (pg/ml) IL2 via Continuous Infusion IL2 of JN IU/ml prescreen preinfusion post- 0 hr post 1 hr post 3 hr post 8 hr post 24 hr post 48 hr post-day 5 post-day 7 post-day 14 post-day 21 post-day 28 75,000 IU/kg/d ~ 3 MIU/m2/d

50 Engraftment 1.1% 2.5% Blood sample Day +14 #1 CIR+ CD3 61% #2 CIR+ 7.3% Dose CD3+
51 PSA PSA PSA Response 3.50 T cells Conditioning d-8 to d-2 T cells infused d0 Low dose IL2 d0 to d chemo Days T cells chemo Days
52 Summary Prostate o Five patients treated Safely administered; toxicity due to conditioning Neutropenic fevers, hospitalization for antibiotics Malaise, fatigue (IL2) 50 and 70% reduction in PSA in two subjects o More doses to follow in escalation 10^10 10^11 o Limitations??? 1st generation: signal 1 only, After resting, do not reactivate 2 nd generation in preclinical o Conclude: PSMA safe for DTC targeting
53 Considerations for Antigen Targeting o The target Normal tissues that express Essential/Dispensible? Topology of expression (epithelial) Unknowability is central to safety testing design Safety with Ab targeting no assurance for T cells o The method of targeting Potency: Co-stimulation, can reactivate after suppression Quantity: Infuse vs engraft Infusion allows control of patient exposures (DLI)
54 T cells homing in on target THE END
55 Table 1. Features of designer T cell versions On Contact with Antigen. CIR Activated T cells Resting T cells 1st gen Signal 1 killing, AICD anergy 2nd gen Signal 1+2 superactivation, killing, activation, killing, cytokines, proliferation cytokines, proliferation
56 Table 2. Features of T cell administration methods Conditioning Risk? In blood In tumor Cost* Infuse None No Transient Transient $5-10K Engraft Chemo, XRT Toxic Stable Sustained $60-100K *Clinical, non-manufacturing costs of patient treatment and monitoring. (Manufacturing ~$15K for 10^11 dose; less for lower doses.)
57 [ QUALITY ] Table 3. Options matrix for designer T cell Strategies (2x2) [ QUANTITY ] Administration method Infuse Engraft Designer 1st gen 1 2 T cell version 2nd gen is untested state Strategy 1 = 1 st gen infused Strategy 2 = 1 st gen engrafted Strategy 3 = 2 nd gen infused Strategy 4 = 2 nd gen engrafted
58 Table 4. Likely toxicity response of auto-reactive DTC to immune suppression on different Strategies On steroids Off steroids Comment 1 st gen only 1 st gen; 0 1 Suppress Suppressed don t reactivate 0 2 Suppress Suppressed don t reactivate 2 nd gen 2 nd gen reactivate; 0 3 Suppress Suppressed small numbers* 0 4 Suppress Autoimmune very large numbers *Known from BMT that dosage of allo-reactive T cells in donor lymphocyte infusions (DLI) critical to safety. Low dose controlled endogenous mechanisms (Treg, etc). High dose uncontrolled except with max suppress, lethal.
59 Safe paths of Strategy Escalation for exposures to designer T cells 1. Avoid maximum exposure for first-inhuman DTC tests for Ag (Strategy 4) 2. Once a Strategy safely tested for Ag, other Strategies safe for that Ag 3. But NOT all paths advisable (---) 0 is untested state Strategy 1 = 1 st gen infused Strategy 2 = 1 st gen engrafted Strategy 3 = 2 nd gen infused Strategy 4 = 2 nd gen engrafted
60 Optimal paths of Strategy Escalation for exposures to designer T cells All paths to 2 nd gen engrafted pass through 2 nd gen infused 1. Lower hazard 2. Lower cost 3. Better science: Test hypothesis of more signals to create effective immune response (without engraftment) NB: No 2 nd gen DTC has yet been tested by infusion to full doses with appropriate cytokine support; hypothesis of sufficiency OR deficiency still untested. 0 is untested state Strategy 1 = 1 st gen infused Strategy 2 = 1 st gen engrafted Strategy 3 = 2 nd gen infused Strategy 4 = 2 nd gen engrafted
61 Considerations for Antigen Targeting o The target Normal tissues that express Essential/Dispensible? Topology of expression (epithelial) Unknowability central to safety testing design Safety with Ab targeting no assurance for T cell o The method of targeting Co-stimulation, can reactivate after suppression Infuse vs engraft Infusion allows control of patient exposures (DLI)

62 T cells homing in on target THE END
63
DEVELOPMENT OF CELLULAR IMMUNOLOGY
 DEVELOPMENT OF CELLULAR IMMUNOLOGY 1880 s: Antibodies described (dominated studies of immunology until 1960 s) 1958: Journal of Immunology (137 papers) lymphocyte not listed in index Two papers on transfer
DEVELOPMENT OF CELLULAR IMMUNOLOGY 1880 s: Antibodies described (dominated studies of immunology until 1960 s) 1958: Journal of Immunology (137 papers) lymphocyte not listed in index Two papers on transfer
08/02/59. Tumor Immunotherapy. Development of Tumor Vaccines. Types of Tumor Vaccines. Immunotherapy w/ Cytokine Gene-Transfected Tumor Cells
 Tumor Immunotherapy Autologous virus Inactivation Inactivated virus Lymphopheresis Culture? Monocyte s Dendritic cells Immunization Autologous vaccine Development of Tumor Vaccines Types of Tumor Vaccines
Tumor Immunotherapy Autologous virus Inactivation Inactivated virus Lymphopheresis Culture? Monocyte s Dendritic cells Immunization Autologous vaccine Development of Tumor Vaccines Types of Tumor Vaccines
One Day BMT Course by Thai Society of Hematology. Management of Graft Failure and Relapsed Diseases
 One Day BMT Course by Thai Society of Hematology Management of Graft Failure and Relapsed Diseases Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital
One Day BMT Course by Thai Society of Hematology Management of Graft Failure and Relapsed Diseases Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital
The Immune System. Innate. Adaptive. - skin, mucosal barriers - complement - neutrophils, NK cells, mast cells, basophils, eosinophils
 Objectives - explain the rationale behind cellular adoptive immunotherapy - describe methods of improving cellular adoptive immunotherapy - identify mechanisms of tumor escape from cellular adoptive immunotherapy
Objectives - explain the rationale behind cellular adoptive immunotherapy - describe methods of improving cellular adoptive immunotherapy - identify mechanisms of tumor escape from cellular adoptive immunotherapy
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Chandran SS, Somerville RPT, Yang JC, et al.
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Chandran SS, Somerville RPT, Yang JC, et al.
The future of HSCT. John Barrett, MD, NHBLI, NIH Bethesda MD
 The future of HSCT John Barrett, MD, NHBLI, NIH Bethesda MD Transplants today Current approaches to improve SCT outcome Optimize stem cell dose and source BMT? PBSCT? Adjusting post transplant I/S to minimize
The future of HSCT John Barrett, MD, NHBLI, NIH Bethesda MD Transplants today Current approaches to improve SCT outcome Optimize stem cell dose and source BMT? PBSCT? Adjusting post transplant I/S to minimize
Cancer Immunotherapy. What is it? Immunotherapy Can Work! 4/15/09. Can the immune system be harnessed to fight cancer? T CD4 T CD28.
 Cancer Immunotherapy CANCER BIOLOGY April 15, 2009 Can the immune system be harnessed to fight cancer? Can the immune system see cancer? What is the best way to turn on the immune system to fight cancer?
Cancer Immunotherapy CANCER BIOLOGY April 15, 2009 Can the immune system be harnessed to fight cancer? Can the immune system see cancer? What is the best way to turn on the immune system to fight cancer?
ACTR (Antibody Coupled T-cell Receptor): A universal approach to T-cell therapy
: A universal approach to T-cell therapy") ACTR (Antibody Coupled T-cell Receptor): A universal approach to T-cell therapy European Medicines Agency Workshop on Scientific and Regulatory Challenges of Genetically Modified Cell-based Cancer Immunotherapy
ACTR (Antibody Coupled T-cell Receptor): A universal approach to T-cell therapy European Medicines Agency Workshop on Scientific and Regulatory Challenges of Genetically Modified Cell-based Cancer Immunotherapy
Immunology Lecture 4. Clinical Relevance of the Immune System
 Immunology Lecture 4 The Well Patient: How innate and adaptive immune responses maintain health - 13, pg 169-181, 191-195. Immune Deficiency - 15 Autoimmunity - 16 Transplantation - 17, pg 260-270 Tumor
Immunology Lecture 4 The Well Patient: How innate and adaptive immune responses maintain health - 13, pg 169-181, 191-195. Immune Deficiency - 15 Autoimmunity - 16 Transplantation - 17, pg 260-270 Tumor
Adoptive T Cell Therapy TILs & TCRs & CARs
 Adoptive T Cell Therapy TILs & TCRs & CARs Inge Marie Svane CCIT DENMARK Professor, MD Center for Cancer Immune Therapy Department of Oncology, Herlev Hospital Copenhagen University Denmark Therapeutic
Adoptive T Cell Therapy TILs & TCRs & CARs Inge Marie Svane CCIT DENMARK Professor, MD Center for Cancer Immune Therapy Department of Oncology, Herlev Hospital Copenhagen University Denmark Therapeutic
Advances in Adoptive Cellular Therapy of Cancer. Melanoma Bridge Meeting December 5, 2014
 Advances in Adoptive Cellular Therapy of Cancer Melanoma Bridge Meeting December 5, 2014 David Stroncek, MD Chief, Cell Processing Section, DTM, CC, NIH Bethesda, Maryland, USA Disclosures None Focus
Advances in Adoptive Cellular Therapy of Cancer Melanoma Bridge Meeting December 5, 2014 David Stroncek, MD Chief, Cell Processing Section, DTM, CC, NIH Bethesda, Maryland, USA Disclosures None Focus
An Overview of Blood and Marrow Transplantation
 An Overview of Blood and Marrow Transplantation October 24, 2009 Stephen Couban Department of Medicine Dalhousie University Objectives What are the types of blood and marrow transplantation? Who may benefit
An Overview of Blood and Marrow Transplantation October 24, 2009 Stephen Couban Department of Medicine Dalhousie University Objectives What are the types of blood and marrow transplantation? Who may benefit
Immunotherapy on the Horizon: Adoptive Cell Therapy
 Immunotherapy on the Horizon: Adoptive Cell Therapy Joseph I. Clark, MD, FACP Professor of Medicine Loyola University Chicago Stritch School of Medicine Maywood, IL June 23, 2016 Conflicts of Interest
Immunotherapy on the Horizon: Adoptive Cell Therapy Joseph I. Clark, MD, FACP Professor of Medicine Loyola University Chicago Stritch School of Medicine Maywood, IL June 23, 2016 Conflicts of Interest
Adoptive Cell Therapy: Treating Cancer
 Adoptive Cell Therapy: Treating Cancer with Genetically Engineered T Cells Steven A. Feldman, Ph.D. Surgery Branch National Cancer Institute NCT Conference Heidelberg, Germany September 24, 2013 Three
Adoptive Cell Therapy: Treating Cancer with Genetically Engineered T Cells Steven A. Feldman, Ph.D. Surgery Branch National Cancer Institute NCT Conference Heidelberg, Germany September 24, 2013 Three
Personalized medicine - cancer immunotherapy
 Personalized medicine - cancer immunotherapy Özcan Met, PhD Senior Staff Scientist, Cell Therapy Director Center for Cancer Immune Therapy Department of Hematology Department of Oncology University Hospital
Personalized medicine - cancer immunotherapy Özcan Met, PhD Senior Staff Scientist, Cell Therapy Director Center for Cancer Immune Therapy Department of Hematology Department of Oncology University Hospital
Darwinian selection and Newtonian physics wrapped up in systems biology
 Darwinian selection and Newtonian physics wrapped up in systems biology Concept published in 1957* by Macfarland Burnet (1960 Nobel Laureate for the theory of induced immune tolerance, leading to solid
Darwinian selection and Newtonian physics wrapped up in systems biology Concept published in 1957* by Macfarland Burnet (1960 Nobel Laureate for the theory of induced immune tolerance, leading to solid
IMMUNOTHERAPY FOR CANCER A NEW HORIZON. Ekaterini Boleti MD, PhD, FRCP Consultant in Medical Oncology Royal Free London NHS Foundation Trust
 IMMUNOTHERAPY FOR CANCER A NEW HORIZON Ekaterini Boleti MD, PhD, FRCP Consultant in Medical Oncology Royal Free London NHS Foundation Trust ASCO Names Advance of the Year: Cancer Immunotherapy No recent
IMMUNOTHERAPY FOR CANCER A NEW HORIZON Ekaterini Boleti MD, PhD, FRCP Consultant in Medical Oncology Royal Free London NHS Foundation Trust ASCO Names Advance of the Year: Cancer Immunotherapy No recent
CONTRACTING ORGANIZATION: Johns Hopkins University School of Medicine Baltimore, MD 21205
 AD Award Number: DAMD7---7 TITLE: Development of Artificial Antigen Presenting Cells for Prostate Cancer Immunotherapy PRINCIPAL INVESTIGATOR: Jonathan P. Schneck, M.D., Ph.D. Mathias Oelke, Ph.D. CONTRACTING
AD Award Number: DAMD7---7 TITLE: Development of Artificial Antigen Presenting Cells for Prostate Cancer Immunotherapy PRINCIPAL INVESTIGATOR: Jonathan P. Schneck, M.D., Ph.D. Mathias Oelke, Ph.D. CONTRACTING
Clinical: Ipilimumab (MDX-010) Update and Next Steps
 Update and Next Steps") Clinical: Ipilimumab (MDX-010) Update and Next Steps Geoffrey M. Nichol, M.D., M.B.A. Senior Vice President, Product Development Medarex, Inc. R&D Day December 9, 2005 Ipilimumab: New Class of Cancer Therapy
Clinical: Ipilimumab (MDX-010) Update and Next Steps Geoffrey M. Nichol, M.D., M.B.A. Senior Vice President, Product Development Medarex, Inc. R&D Day December 9, 2005 Ipilimumab: New Class of Cancer Therapy
A PHASE 1 STUDY OF TRC105 (ANTI- ADVANCED SOLID TUMORS
 ASCO 2011 Abstract Number: 3073 A PHASE 1 STUDY OF TRC105 (ANTI- CD105 ANTIBODY) IN PATIENTS WITH ADVANCED SOLID TUMORS J. W. Goldman, M. S. Gordon, H. Hurwitz, R. Pili, D. S. Mendelson, B. J. Adams, D.
ASCO 2011 Abstract Number: 3073 A PHASE 1 STUDY OF TRC105 (ANTI- CD105 ANTIBODY) IN PATIENTS WITH ADVANCED SOLID TUMORS J. W. Goldman, M. S. Gordon, H. Hurwitz, R. Pili, D. S. Mendelson, B. J. Adams, D.
Bone Marrow Transplantation and the Potential Role of Iomab-B
 Bone Marrow Transplantation and the Potential Role of Iomab-B Hillard M. Lazarus, MD, FACP Professor of Medicine, Director of Novel Cell Therapy Case Western Reserve University 1 Hematopoietic Cell Transplantation
Bone Marrow Transplantation and the Potential Role of Iomab-B Hillard M. Lazarus, MD, FACP Professor of Medicine, Director of Novel Cell Therapy Case Western Reserve University 1 Hematopoietic Cell Transplantation
Corporate Presentation
 Corporate Presentation June 2017 Forward-Looking Statements This presentation contains forward-looking statements reflecting management s current beliefs and expectations. These forward looking statements
Corporate Presentation June 2017 Forward-Looking Statements This presentation contains forward-looking statements reflecting management s current beliefs and expectations. These forward looking statements
Lecture 17: Vaccines (Therapeutic and Prophylactic Types)
") Lecture 17: Vaccines (Therapeutic and Prophylactic Types) Therapeutic vaccines Bacillus Calmette Guerin (BCG; TheraCys) Very old agent initially developed as vaccine for MTB. Uses: Superficial bladder
Lecture 17: Vaccines (Therapeutic and Prophylactic Types) Therapeutic vaccines Bacillus Calmette Guerin (BCG; TheraCys) Very old agent initially developed as vaccine for MTB. Uses: Superficial bladder
Immune Checkpoints. PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich
 Immune Checkpoints PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich Activation of T cells requires co-stimulation Science 3
Immune Checkpoints PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich Activation of T cells requires co-stimulation Science 3
Tumor Immunology. Wirsma Arif Harahap Surgical Oncology Consultant
 Tumor Immunology Wirsma Arif Harahap Surgical Oncology Consultant 1) Immune responses that develop to cancer cells 2) Escape of cancer cells 3) Therapies: clinical and experimental Cancer cells can be
Tumor Immunology Wirsma Arif Harahap Surgical Oncology Consultant 1) Immune responses that develop to cancer cells 2) Escape of cancer cells 3) Therapies: clinical and experimental Cancer cells can be
Oncolytic Viruses: Reovirus
 T S X : O N C N A S D A Q : O N C Y International Society for Biological Therapy of Cancer 2008 Oncology Biologics Development Primer Oncolytic Viruses: Reovirus REOLYSIN - mode of action REOLYSIN contains
T S X : O N C N A S D A Q : O N C Y International Society for Biological Therapy of Cancer 2008 Oncology Biologics Development Primer Oncolytic Viruses: Reovirus REOLYSIN - mode of action REOLYSIN contains
Neutrophil Recovery: The. Posttransplant Recovery. Bus11_1.ppt
 Neutrophil Recovery: The First Step in Posttransplant Recovery No conflicts of interest to disclose Bus11_1.ppt Blood is Made in the Bone Marrow Blood Stem Cell Pre-B White cells B Lymphocyte T Lymphocyte
Neutrophil Recovery: The First Step in Posttransplant Recovery No conflicts of interest to disclose Bus11_1.ppt Blood is Made in the Bone Marrow Blood Stem Cell Pre-B White cells B Lymphocyte T Lymphocyte
Introduction to Clinical Hematopoietic Cell Transplantation (HCT) George Chen, MD Thursday, May 03, 2018
 George Chen, MD Thursday, May 03, 2018") Introduction to Clinical Hematopoietic Cell Transplantation (HCT) George Chen, MD Thursday, May 03, 2018 The transfer of hematopoietic progenitor and stem cells for therapeutic purposes Hematopoietic Cell
Introduction to Clinical Hematopoietic Cell Transplantation (HCT) George Chen, MD Thursday, May 03, 2018 The transfer of hematopoietic progenitor and stem cells for therapeutic purposes Hematopoietic Cell
2/19/2018. The Immune System and Cancer. Fatal Melanoma Transferred in a Donated Kidney 16 years after Melanoma Surgery
 F141: Advanced Melanoma: Mechanisms of Immune Therapies beyond Checkpoint blockade Delphine J. Lee, MD, PhD Chief and Program Director, Dermatology, Harbor UCLA Medical Center Principal Investigator, Los
F141: Advanced Melanoma: Mechanisms of Immune Therapies beyond Checkpoint blockade Delphine J. Lee, MD, PhD Chief and Program Director, Dermatology, Harbor UCLA Medical Center Principal Investigator, Los
5/9/2018. Bone marrow failure diseases (aplastic anemia) can be cured by providing a source of new marrow
 can be cured by providing a source of new marrow") 5/9/2018 or Stem Cell Harvest Where we are now, and What s Coming AA MDS International Foundation Indianapolis IN Luke Akard MD May 19, 2018 Infusion Transplant Conditioning Treatment 2-7 days STEM CELL
5/9/2018 or Stem Cell Harvest Where we are now, and What s Coming AA MDS International Foundation Indianapolis IN Luke Akard MD May 19, 2018 Infusion Transplant Conditioning Treatment 2-7 days STEM CELL
Adoptive cell therapy and modulation of the tumour microenvironment: new insights from ASCO 2016
 Adoptive cell therapy and modulation of the tumour microenvironment: new insights from ASCO 2016 Leila Khoja 1,2 and Bishal Gyawali 3 1 Royal Free Hospital, Pond Street, London NW3 2QG, UK. 2 Astrazeneca
Adoptive cell therapy and modulation of the tumour microenvironment: new insights from ASCO 2016 Leila Khoja 1,2 and Bishal Gyawali 3 1 Royal Free Hospital, Pond Street, London NW3 2QG, UK. 2 Astrazeneca
Adoptive cell therapy using genetically modified antigen-presenting cells
 Adoptive cell therapy using genetically modified antigen-presenting cells Naoto Hirano Ontario Cancer Institute Princess Margaret Cancer Centre University of Toronto UofT-USP Oncology Conference November
Adoptive cell therapy using genetically modified antigen-presenting cells Naoto Hirano Ontario Cancer Institute Princess Margaret Cancer Centre University of Toronto UofT-USP Oncology Conference November
Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates
 Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates Christopher Turner, MD Vice President, Clinical Science 04 November 2016 Uveal Melanoma Celldex Pipeline CANDIDATE INDICATION Preclinical
Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates Christopher Turner, MD Vice President, Clinical Science 04 November 2016 Uveal Melanoma Celldex Pipeline CANDIDATE INDICATION Preclinical
The Role of Immunotherapy in Prostate Cancer: What s Trending?
 The Role of Immunotherapy in Prostate Cancer: What s Trending? Douglas G. McNeel, MD, PhD University of Wisconsin Carbone Cancer Center Madison, Wisconsin Prostate cancer rationale for immune therapies
The Role of Immunotherapy in Prostate Cancer: What s Trending? Douglas G. McNeel, MD, PhD University of Wisconsin Carbone Cancer Center Madison, Wisconsin Prostate cancer rationale for immune therapies
Minor H Antigen-Specific T Cells -The Black Box of the GVL Effect
 Minor H Antigen-Specific T Cells -The Black Box of the GVL Effect All Allogeneic Stem Cell Transplants Are Blind Doctor Donor Patient Genetic polymorphism gives rise to unique peptides in donor and recipient
Minor H Antigen-Specific T Cells -The Black Box of the GVL Effect All Allogeneic Stem Cell Transplants Are Blind Doctor Donor Patient Genetic polymorphism gives rise to unique peptides in donor and recipient
CBER Regulatory Considerations for Clinical Development of Immunotherapies in Oncology
 CBER Regulatory Considerations for Clinical Development of Immunotherapies in Oncology Peter Bross, MD Office of Cellular, Tissue and Gene Therapies, CBER FDA IOM Policy Issues in the Clinical Development
CBER Regulatory Considerations for Clinical Development of Immunotherapies in Oncology Peter Bross, MD Office of Cellular, Tissue and Gene Therapies, CBER FDA IOM Policy Issues in the Clinical Development
Tumor responses (patients responding/ patients treated)
") Table 1. ACT clinical trial tumor responses and toxicities. a Target antigen Cancer(s) Receptor type Tumor responses (patients responding/ patients treated) Immune-mediated toxicities (patients experiencing
Table 1. ACT clinical trial tumor responses and toxicities. a Target antigen Cancer(s) Receptor type Tumor responses (patients responding/ patients treated) Immune-mediated toxicities (patients experiencing
2/16/2018. The Immune System and Cancer. Fatal Melanoma Transferred in a Donated Kidney 16 years after Melanoma Surgery
 C007: Immunology of Melanoma: Mechanisms of Immune Therapies Delphine J. Lee, MD, PhD Chief and Program Director, Dermatology, Harbor UCLA Medical Center Principal Investigator, Los Angeles Biomedical
C007: Immunology of Melanoma: Mechanisms of Immune Therapies Delphine J. Lee, MD, PhD Chief and Program Director, Dermatology, Harbor UCLA Medical Center Principal Investigator, Los Angeles Biomedical
Vaccine Therapy for Cancer
 Vaccine Therapy for Cancer Lawrence N Shulman, MD Chief Medical Officer Senior Vice President for Medical Affairs Chief, Division of General Oncology Dana-Farber Cancer Institute Disclosures for Lawrence
Vaccine Therapy for Cancer Lawrence N Shulman, MD Chief Medical Officer Senior Vice President for Medical Affairs Chief, Division of General Oncology Dana-Farber Cancer Institute Disclosures for Lawrence
Management of Incurable Prostate Cancer in 2014
 Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
NIH Public Access Author Manuscript Science. Author manuscript; available in PMC 2008 March 12.
 NIH Public Access Author Manuscript Published in final edited form as: Science. 2006 October 6; 314(5796): 126 129. Cancer Regression in Patients After Transfer of Genetically Engineered Lymphocytes Richard
NIH Public Access Author Manuscript Published in final edited form as: Science. 2006 October 6; 314(5796): 126 129. Cancer Regression in Patients After Transfer of Genetically Engineered Lymphocytes Richard
T cell manipulation of the graft: Yes
 T cell manipulation of the graft: Yes J.H. Frederik Falkenburg Department of Hematology L M U C Allogeneic Hematopoietic Stem Cell Transplantation (SCT) for non-malignant disorders: no need for anti-tumor
T cell manipulation of the graft: Yes J.H. Frederik Falkenburg Department of Hematology L M U C Allogeneic Hematopoietic Stem Cell Transplantation (SCT) for non-malignant disorders: no need for anti-tumor
Basic Principles of Tumor Immunotherapy and Mechanisms of Tumor Immune Suppression. Bryon Johnson, PhD
 Basic Principles of Tumor Immunotherapy and Mechanisms of Tumor Immune Suppression Bryon Johnson, PhD Disclosures There will be discussion about the use of products for non-fda indications in this presentation.
Basic Principles of Tumor Immunotherapy and Mechanisms of Tumor Immune Suppression Bryon Johnson, PhD Disclosures There will be discussion about the use of products for non-fda indications in this presentation.
Exploiting tumour infiltrating lymphocytes (TILs) as a therapeutic strategy in epithelial ovarian cancer
 as a therapeutic strategy in epithelial ovarian cancer") Exploiting tumour infiltrating lymphocytes (TILs) as a therapeutic strategy in epithelial ovarian cancer G.L.Owens 1,2, V.Sheard 2, M.Price 1, D.E.Gilham 2, R.J.Edmondson 1 1 Gynaecological Oncology Research
Exploiting tumour infiltrating lymphocytes (TILs) as a therapeutic strategy in epithelial ovarian cancer G.L.Owens 1,2, V.Sheard 2, M.Price 1, D.E.Gilham 2, R.J.Edmondson 1 1 Gynaecological Oncology Research
An Introduction to Bone Marrow Transplant
 Introduction to Blood Cancers An Introduction to Bone Marrow Transplant Rushang Patel, MD, PhD, FACP Florida Hospital Medical Group S My RBC Plt Gran Polycythemia Vera Essential Thrombocythemia AML, CML,
Introduction to Blood Cancers An Introduction to Bone Marrow Transplant Rushang Patel, MD, PhD, FACP Florida Hospital Medical Group S My RBC Plt Gran Polycythemia Vera Essential Thrombocythemia AML, CML,
TITLE: Development of Antigen Presenting Cells for adoptive immunotherapy in prostate cancer
 AD Award Number: W8-XWH-5-- TITLE: Development of Antigen Presenting Cells for adoptive immunotherapy in prostate cancer PRINCIPAL INVESTIGATOR: Mathias Oelke, Ph.D. CONTRACTING ORGANIZATION: Johns Hopkins
AD Award Number: W8-XWH-5-- TITLE: Development of Antigen Presenting Cells for adoptive immunotherapy in prostate cancer PRINCIPAL INVESTIGATOR: Mathias Oelke, Ph.D. CONTRACTING ORGANIZATION: Johns Hopkins
CONTRACTING ORGANIZATION: Johns Hopkins University School of Medicine Baltimore, MD 21205
 AD Award Number: DAMD7---7 TITLE: Development of Artificial Antigen Presenting Cells for Prostate Cancer Immunotherapy PRINCIPAL INVESTIGATOR: Jonathan P. Schneck, M.D., Ph.D. Mathias Oelke, Ph.D. CONTRACTING
AD Award Number: DAMD7---7 TITLE: Development of Artificial Antigen Presenting Cells for Prostate Cancer Immunotherapy PRINCIPAL INVESTIGATOR: Jonathan P. Schneck, M.D., Ph.D. Mathias Oelke, Ph.D. CONTRACTING
Ex-Vivo heat shock protein 70-peptide-activated, autologous natural killer cells adoptive therapy: from the bench to the clinic
 Ex-Vivo heat shock protein 70-peptide-activated, autologous natural killer cells adoptive therapy: from the bench to the clinic isbtc 10-13 November 2005 Valeria Milani, MD, PhD Munich Agenda 1. NK ligands
Ex-Vivo heat shock protein 70-peptide-activated, autologous natural killer cells adoptive therapy: from the bench to the clinic isbtc 10-13 November 2005 Valeria Milani, MD, PhD Munich Agenda 1. NK ligands
Relapsed/Refractory Hodgkin Lymphoma
 Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma
 UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Supported by a grant from Supported by a grant from UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Jonathan W.
UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Supported by a grant from Supported by a grant from UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Jonathan W.
Immunotherapy of Prostate Cancer
 Immunotherapy of Prostate Cancer Robert E. Reiter MD MBA Bing Professor of Urologic Oncology Geffen School of Medicine at UCLA Costimulatory expression required for T cell activation Therapeutic Vaccines
Immunotherapy of Prostate Cancer Robert E. Reiter MD MBA Bing Professor of Urologic Oncology Geffen School of Medicine at UCLA Costimulatory expression required for T cell activation Therapeutic Vaccines
Immunotransplant for Mantle Cell Lymphoma: A phase I/II study demonstrating amplification of tumor-reactive T cells
 Immunotransplant for Mantle Cell Lymphoma: A phase I/II study demonstrating amplification of tumor-reactive T cells Joshua Brody MD Division of Oncology Stanford University Medical Center Presenter Disclosure
Immunotransplant for Mantle Cell Lymphoma: A phase I/II study demonstrating amplification of tumor-reactive T cells Joshua Brody MD Division of Oncology Stanford University Medical Center Presenter Disclosure
2019 ASCO-SITC. Nektar Therapeutics Investor & Analyst Call. March 1, 2019
 Nektar Therapeutics Investor & Analyst Call March 1, 2019 This presentation includes forward-looking statements regarding Nektar s proprietary drug candidates, the timing of the start and conclusion of
Nektar Therapeutics Investor & Analyst Call March 1, 2019 This presentation includes forward-looking statements regarding Nektar s proprietary drug candidates, the timing of the start and conclusion of
COURSE: Medical Microbiology, PAMB 650/720 - Fall 2008 Lecture 16
 COURSE: Medical Microbiology, PAMB 650/720 - Fall 2008 Lecture 16 Tumor Immunology M. Nagarkatti Teaching Objectives: Introduction to Cancer Immunology Know the antigens expressed by cancer cells Understand
COURSE: Medical Microbiology, PAMB 650/720 - Fall 2008 Lecture 16 Tumor Immunology M. Nagarkatti Teaching Objectives: Introduction to Cancer Immunology Know the antigens expressed by cancer cells Understand
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Tumors arise from accumulated genetic mutations. Tumor Immunology (Cancer)
") Tumor Immunology (Cancer) Tumors arise from accumulated genetic mutations Robert Beatty MCB150 Mutations Usually have >6 mutations in both activation/growth factors and tumor suppressor genes. Types of
Tumor Immunology (Cancer) Tumors arise from accumulated genetic mutations Robert Beatty MCB150 Mutations Usually have >6 mutations in both activation/growth factors and tumor suppressor genes. Types of
4100: Cellular Therapy Essential Data Follow-Up Form
 4100: Cellular Therapy Essential Data Follow-Up Form Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Event date: Visit: 100 day 6 months 1 year 2 years >2 years, Specify:
4100: Cellular Therapy Essential Data Follow-Up Form Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Event date: Visit: 100 day 6 months 1 year 2 years >2 years, Specify:
LAG-3: Validation Of Next Generation Checkpoint Pathways
 LAG-3: Validation Of Next Generation Checkpoint Pathways Frédéric Triebel, CO/CMO Immune Checkpoint Modulation & Combination Therapies April 13, 2016 London, UK. 1 AX:PRR; NADAQ:PBMD Notice: Forward Looking
LAG-3: Validation Of Next Generation Checkpoint Pathways Frédéric Triebel, CO/CMO Immune Checkpoint Modulation & Combination Therapies April 13, 2016 London, UK. 1 AX:PRR; NADAQ:PBMD Notice: Forward Looking
Determinants of Immunogenicity and Tolerance. Abul K. Abbas, MD Department of Pathology University of California San Francisco
 Determinants of Immunogenicity and Tolerance Abul K. Abbas, MD Department of Pathology University of California San Francisco EIP Symposium Feb 2016 Why do some people respond to therapeutic proteins?
Determinants of Immunogenicity and Tolerance Abul K. Abbas, MD Department of Pathology University of California San Francisco EIP Symposium Feb 2016 Why do some people respond to therapeutic proteins?
Focus on Immunotherapy as a Targeted Therapy. Brad Nelson, PhD BC Cancer, Victoria, Canada FPON, Oct
 Focus on Immunotherapy as a Targeted Therapy Brad Nelson, PhD BC Cancer, Victoria, Canada FPON, Oct 18 2018 Disclosures I have nothing to disclose that is relevant to this presentation. Immunology @ Deeley
Focus on Immunotherapy as a Targeted Therapy Brad Nelson, PhD BC Cancer, Victoria, Canada FPON, Oct 18 2018 Disclosures I have nothing to disclose that is relevant to this presentation. Immunology @ Deeley
Endogenous and Exogenous Vaccination in the Context of Immunologic Checkpoint Blockade
 Endogenous and Exogenous Vaccination in the Context of Immunologic Checkpoint Blockade Jedd Wolchok Ludwig Center for Cancer Immunotherapy Memorial Sloan-Kettering Cancer Center MEMORIAL SLOAN- KETTERING
Endogenous and Exogenous Vaccination in the Context of Immunologic Checkpoint Blockade Jedd Wolchok Ludwig Center for Cancer Immunotherapy Memorial Sloan-Kettering Cancer Center MEMORIAL SLOAN- KETTERING
Trends in Hematopoietic Cell Transplantation. AAMAC Patient Education Day Oct 2014
 Trends in Hematopoietic Cell Transplantation AAMAC Patient Education Day Oct 2014 Objectives Review the principles behind allogeneic stem cell transplantation Outline the process of transplant, some of
Trends in Hematopoietic Cell Transplantation AAMAC Patient Education Day Oct 2014 Objectives Review the principles behind allogeneic stem cell transplantation Outline the process of transplant, some of
Biological Therapies for Cancer: Questions and Answers
 Biological Therapies for Cancer: Questions and Answers Key Points Biological therapies use the body s immune system to fight cancer or to lessen the side effects that may be caused by some cancer treatments
Biological Therapies for Cancer: Questions and Answers Key Points Biological therapies use the body s immune system to fight cancer or to lessen the side effects that may be caused by some cancer treatments
Bioassays for Quality Control of Cell & Gene Therapy Products
 Bioassays for Quality Control of Cell & Gene Therapy Products Erik Rutjens, Cell & Gene Therapy, Novartis Pharma AG CASSS Bioassays, Silver Spring, March2015 CTL019 Introduction CARTs = Chimeric Antigen
Bioassays for Quality Control of Cell & Gene Therapy Products Erik Rutjens, Cell & Gene Therapy, Novartis Pharma AG CASSS Bioassays, Silver Spring, March2015 CTL019 Introduction CARTs = Chimeric Antigen
Immunology and Immunotherapy 101 for the Non-Immunologist
 Immunology and Immunotherapy 101 for the Non-Immunologist Stephen P. Schoenberger, Ph.D La Jolla Institute for Allergy and Immunology & UCSD Moores Cancer Center Disclosures Human Longevity Inc: Salary
Immunology and Immunotherapy 101 for the Non-Immunologist Stephen P. Schoenberger, Ph.D La Jolla Institute for Allergy and Immunology & UCSD Moores Cancer Center Disclosures Human Longevity Inc: Salary
TITLE: Development of Antigen Presenting Cells for adoptive immunotherapy in prostate cancer
 AD Award Number: W8XWH-5-- TITLE: Development of Antigen Presenting Cells for adoptive immunotherapy in prostate cancer PRINCIPAL INVESTIGATOR: Mathias Oelke Ph.D. CONTRACTING ORGANIZATION: Johns Hopkins
AD Award Number: W8XWH-5-- TITLE: Development of Antigen Presenting Cells for adoptive immunotherapy in prostate cancer PRINCIPAL INVESTIGATOR: Mathias Oelke Ph.D. CONTRACTING ORGANIZATION: Johns Hopkins
Exploring Immunotherapies: Beyond Checkpoint Inhibitors
 Exploring Immunotherapies: Beyond Checkpoint Inhibitors Authored by: Jennifer Dolan Fox, PhD VirtualScopics (Now part of BioTelemetry Research) jennifer_fox@virtualscopics.com +1 585 249 6231 Introduction
Exploring Immunotherapies: Beyond Checkpoint Inhibitors Authored by: Jennifer Dolan Fox, PhD VirtualScopics (Now part of BioTelemetry Research) jennifer_fox@virtualscopics.com +1 585 249 6231 Introduction
What s a Transplant? What s not?
 What s a Transplant? What s not? How to report the difference? Daniel Weisdorf MD University of Minnesota Anti-cancer effects of BMT or PBSCT [HSCT] Kill the cancer Save the patient Restore immunocompetence
What s a Transplant? What s not? How to report the difference? Daniel Weisdorf MD University of Minnesota Anti-cancer effects of BMT or PBSCT [HSCT] Kill the cancer Save the patient Restore immunocompetence
AE Toxicity Grading for Transplant Patients
 AE Toxicity Grading for Transplant Patients Marcie Tomblyn, MD, MS Associate Member Director, BMT Clinical Research Moffitt Cancer Center Objectives Why do we care????? Toxicity vs Adverse Event vs Serious
AE Toxicity Grading for Transplant Patients Marcie Tomblyn, MD, MS Associate Member Director, BMT Clinical Research Moffitt Cancer Center Objectives Why do we care????? Toxicity vs Adverse Event vs Serious
Transplantation - Challenges for the future. Dr Gordon Cook S t James s Institute of Oncology, Leeds Teaching Hospitals Trust
 Transplantation - Challenges for the future Dr Gordon Cook S t James s Institute of Oncology, Leeds Teaching Hospitals Trust Bone Marrow Transplantation Timeline, 1957-2006 Appelbaum F. N Engl J Med 2007;357:1472-1475
Transplantation - Challenges for the future Dr Gordon Cook S t James s Institute of Oncology, Leeds Teaching Hospitals Trust Bone Marrow Transplantation Timeline, 1957-2006 Appelbaum F. N Engl J Med 2007;357:1472-1475
Introduction to Immunology and the Immune System
 Introduction to Immunology and the Immune System Assistant professor Dr. Aida R. Al-Derzi M.B.Ch.B; M.Sc; FICM/Path Dept. of Microbiology/College of Medicine/Baghdad University Introduction to Immunology
Introduction to Immunology and the Immune System Assistant professor Dr. Aida R. Al-Derzi M.B.Ch.B; M.Sc; FICM/Path Dept. of Microbiology/College of Medicine/Baghdad University Introduction to Immunology
CAR-T. Subrena Powell RN, MSN, BMTCN
 CAR-T Subrena Powell RN, MSN, BMTCN Objectives Discuss the treatment timeline of a patient receiving CAR-T therapy Describe the side effects and management of symptoms of CAR-T therapy Treatment Schema
CAR-T Subrena Powell RN, MSN, BMTCN Objectives Discuss the treatment timeline of a patient receiving CAR-T therapy Describe the side effects and management of symptoms of CAR-T therapy Treatment Schema
Adoptive Cellular Therapy SITC Primer October 2012
 Adoptive Cellular Therapy SITC Primer October 2012 Cassian Yee MD Member Fred Hutchinson Cancer Research Center Program in Immunology Clinical Research Division Professor University of Washington Division
Adoptive Cellular Therapy SITC Primer October 2012 Cassian Yee MD Member Fred Hutchinson Cancer Research Center Program in Immunology Clinical Research Division Professor University of Washington Division
Bihong Zhao, M.D, Ph.D Department of Pathology
 Bihong Zhao, M.D, Ph.D Department of Pathology 04-28-2009 Is tumor self or non-self? How are tumor antigens generated? What are they? How does immune system respond? Introduction Tumor Antigens/Categories
Bihong Zhao, M.D, Ph.D Department of Pathology 04-28-2009 Is tumor self or non-self? How are tumor antigens generated? What are they? How does immune system respond? Introduction Tumor Antigens/Categories
Cancer Vaccines and Cytokines. Elizabeth A. Mittendorf, MD, PhD Assistant Professor Department of Surgical Oncology
 Cancer Vaccines and Cytokines Elizabeth A. Mittendorf, MD, PhD Assistant Professor Department of Surgical Oncology Disclosures I serve as the PI on a phase III trial sponsored by Galena BioPharma investigating
Cancer Vaccines and Cytokines Elizabeth A. Mittendorf, MD, PhD Assistant Professor Department of Surgical Oncology Disclosures I serve as the PI on a phase III trial sponsored by Galena BioPharma investigating
Tumor Markers Yesterday, Today & Tomorrow. Steven E. Zimmerman M.D. Vice President & Chief Medical Director
 Tumor Markers Yesterday, Today & Tomorrow Steven E. Zimmerman M.D. Vice President & Chief Medical Director Tumor Marker - Definition Substances produced by cancer cells or other cells in response to cancer
Tumor Markers Yesterday, Today & Tomorrow Steven E. Zimmerman M.D. Vice President & Chief Medical Director Tumor Marker - Definition Substances produced by cancer cells or other cells in response to cancer
LIGAND-INDUCIBLE, PROSTATE STEM CELL ANTIGEN (PSCA)-DIRECTED GoCAR-T CELLS IN ADVANCED SOLID TUMORS: PRELIMINARY RESULTS FROM A DOSE ESCALATION STUDY
-DIRECTED GoCAR-T CELLS IN ADVANCED SOLID TUMORS: PRELIMINARY RESULTS FROM A DOSE ESCALATION STUDY") LIGAND-INDUCIBLE, PROSTATE STEM CELL ANTIGEN (PSCA)-DIRECTED GoCAR-T CELLS IN ADVANCED SOLID TUMORS: PRELIMINARY RESULTS FROM A DOSE ESCALATION STUDY Carlos R. Becerra, 1 Pamela Hoof, 1 Scott Paulson,
LIGAND-INDUCIBLE, PROSTATE STEM CELL ANTIGEN (PSCA)-DIRECTED GoCAR-T CELLS IN ADVANCED SOLID TUMORS: PRELIMINARY RESULTS FROM A DOSE ESCALATION STUDY Carlos R. Becerra, 1 Pamela Hoof, 1 Scott Paulson,
Reduced-intensity Conditioning Transplantation
 Reduced-intensity Conditioning Transplantation Current Role and Future Prospect He Huang M.D., Ph.D. Bone Marrow Transplantation Center The First Affiliated Hospital Zhejiang University School of Medicine,
Reduced-intensity Conditioning Transplantation Current Role and Future Prospect He Huang M.D., Ph.D. Bone Marrow Transplantation Center The First Affiliated Hospital Zhejiang University School of Medicine,
S. No Topic Class No Date
 S. No Topic Class No Date 1 Introduction 2 3 4 5 6 7 Fundamentals of Immunology Definitions and basic terms Types of immunity Organs of immune system Cells of immune system Innate immunity PAMPs PRRs Phagocytosis
S. No Topic Class No Date 1 Introduction 2 3 4 5 6 7 Fundamentals of Immunology Definitions and basic terms Types of immunity Organs of immune system Cells of immune system Innate immunity PAMPs PRRs Phagocytosis
Cancer as a Complex Adaptive System: Cancer Progression, Evolutionary Dynamics and Implications for Treatment
 BIO 302: September 26, 2018 Cancer as a Complex Adaptive System: Cancer Progression, Evolutionary Dynamics and Implications for Treatment Dr. George Poste Chief Scientist, Complex Adaptive Systems Initiative
BIO 302: September 26, 2018 Cancer as a Complex Adaptive System: Cancer Progression, Evolutionary Dynamics and Implications for Treatment Dr. George Poste Chief Scientist, Complex Adaptive Systems Initiative
Refractory celiac disease (RCD) KASSEM BARADA LEBANESE SOCIETY OF GASTROENTEROLOGY NOVEMBER, 2014
 KASSEM BARADA LEBANESE SOCIETY OF GASTROENTEROLOGY NOVEMBER, 2014") Refractory celiac disease (RCD) KASSEM BARADA LEBANESE SOCIETY OF GASTROENTEROLOGY NOVEMBER, 2014 Case scenario (1) A 49 year woman presents with intermittent watery diarrhea and bloating of two years
Refractory celiac disease (RCD) KASSEM BARADA LEBANESE SOCIETY OF GASTROENTEROLOGY NOVEMBER, 2014 Case scenario (1) A 49 year woman presents with intermittent watery diarrhea and bloating of two years
Mucosal Immune System
 Exam Format 100 points - 60 pts mandatory; 40 points where 4, 10 point questions will be chosen Some open-ended questions, some short answer. Kuby question Cytokines Terminology How do cytokines achieve
Exam Format 100 points - 60 pts mandatory; 40 points where 4, 10 point questions will be chosen Some open-ended questions, some short answer. Kuby question Cytokines Terminology How do cytokines achieve
Clinical Translation of Immunotherapy using WT1 and CMV specific TCR Gene Transfer
 Clinical Translation of Immunotherapy using WT1 and CMV specific Gene Transfer Dr Emma C Morris Reader, Dept of Immunology, UCL Consultant Haematologist (BMT), UCLH and RFH ISCT, 2/5/211 Gene Transfer
Clinical Translation of Immunotherapy using WT1 and CMV specific Gene Transfer Dr Emma C Morris Reader, Dept of Immunology, UCL Consultant Haematologist (BMT), UCLH and RFH ISCT, 2/5/211 Gene Transfer
Restoring Immune Function of Tumor-Specific CD4 + T Cells during Recurrence of Melanoma
 Restoring Immune Function of Tumor-Specific CD4 + T Cells during Recurrence of Melanoma Goding SR et al. J Immunol 2013; 190:4899-4909 C. Nikolowsky Christian Doppler Laboratory for Cardiac and Thoracic
Restoring Immune Function of Tumor-Specific CD4 + T Cells during Recurrence of Melanoma Goding SR et al. J Immunol 2013; 190:4899-4909 C. Nikolowsky Christian Doppler Laboratory for Cardiac and Thoracic
Cellular Pathology of immunological disorders
 Cellular Pathology of immunological disorders SCBM344 Cellular and Molecular Pathology Witchuda Payuhakrit, Ph.D (Pathobiology) witchuda.pay@mahidol.ac.th Objectives Describe the etiology of immunological
Cellular Pathology of immunological disorders SCBM344 Cellular and Molecular Pathology Witchuda Payuhakrit, Ph.D (Pathobiology) witchuda.pay@mahidol.ac.th Objectives Describe the etiology of immunological
Mobilization & Pre-Transplant Conditioning Regimens
 Transplant Process & Pre-Transplant Conditioning Regimens (auto patients only) 30 days before BMT (allo donors) 5 days before BMT Conditioning (auto AND allo patients) Transplant A technique used to increase
Transplant Process & Pre-Transplant Conditioning Regimens (auto patients only) 30 days before BMT (allo donors) 5 days before BMT Conditioning (auto AND allo patients) Transplant A technique used to increase
Antigen Presentation and T Lymphocyte Activation. Abul K. Abbas UCSF. FOCiS
 1 Antigen Presentation and T Lymphocyte Activation Abul K. Abbas UCSF FOCiS 2 Lecture outline Dendritic cells and antigen presentation The role of the MHC T cell activation Costimulation, the B7:CD28 family
1 Antigen Presentation and T Lymphocyte Activation Abul K. Abbas UCSF FOCiS 2 Lecture outline Dendritic cells and antigen presentation The role of the MHC T cell activation Costimulation, the B7:CD28 family
Effective activity of cytokine-induced killer cells against autologous metastatic melanoma including cells with stemness features
 Effective activity of cytokine-induced killer cells against autologous metastatic melanoma including cells with stemness features Loretta Gammaitoni, Lidia Giraudo, Valeria Leuci, et al. Clin Cancer Res
Effective activity of cytokine-induced killer cells against autologous metastatic melanoma including cells with stemness features Loretta Gammaitoni, Lidia Giraudo, Valeria Leuci, et al. Clin Cancer Res
Melanoma Bridge Meeting
 Melanoma Bridge Meeting Improving Adoptive Immune Therapy with Genetically Engineered T cells David Stroncek, MD Chief, Cell Processing Section, DTM, CC, NIH 3 December 2015 Adoptive T Cell Therapy: Dose
Melanoma Bridge Meeting Improving Adoptive Immune Therapy with Genetically Engineered T cells David Stroncek, MD Chief, Cell Processing Section, DTM, CC, NIH 3 December 2015 Adoptive T Cell Therapy: Dose
TITLE: Development of Antigen Presenting Cells for adoptive immunotherapy in prostate cancer
 AD Award Number: W8-XWH-5-- TITLE: Development of Antigen Presenting Cells for adoptive immunotherapy in prostate cancer PRINCIPAL INVESTIGATOR: Mathias Oelke,. CONTRACTING ORGANIZATION: Johns Hopkins
AD Award Number: W8-XWH-5-- TITLE: Development of Antigen Presenting Cells for adoptive immunotherapy in prostate cancer PRINCIPAL INVESTIGATOR: Mathias Oelke,. CONTRACTING ORGANIZATION: Johns Hopkins
Umbilical Cord Blood-Derived T Regulatory Cells
 Umbilical Cord Blood-Derived T Regulatory Cells David H. McKenna, M.D. PACT Workshop - University of Pittsburgh May 5, 2008 Slide 1 Outline Overview of T regulatory (T R ) cells Potential for clinical
Umbilical Cord Blood-Derived T Regulatory Cells David H. McKenna, M.D. PACT Workshop - University of Pittsburgh May 5, 2008 Slide 1 Outline Overview of T regulatory (T R ) cells Potential for clinical
Immuno-Oncology Therapies and Precision Medicine: Personal Tumor-Specific Neoantigen Prediction by Machine Learning
 Immuno-Oncology Therapies and Precision Medicine: Personal Tumor-Specific Neoantigen Prediction by Machine Learning Yi-Hsiang Hsu, MD, SCD Sep 16, 2017 yihsianghsu@hsl.harvard.edu Director & Associate
Immuno-Oncology Therapies and Precision Medicine: Personal Tumor-Specific Neoantigen Prediction by Machine Learning Yi-Hsiang Hsu, MD, SCD Sep 16, 2017 yihsianghsu@hsl.harvard.edu Director & Associate
THE ROLE OF TBI IN STEM CELL TRANSPLANTATION. Dr. Biju George Professor Department of Haematology CMC Vellore
 THE ROLE OF TBI IN STEM CELL TRANSPLANTATION Dr. Biju George Professor Department of Haematology CMC Vellore Introduction Radiotherapy is the medical use of ionising radiation. TBI or Total Body Irradiation
THE ROLE OF TBI IN STEM CELL TRANSPLANTATION Dr. Biju George Professor Department of Haematology CMC Vellore Introduction Radiotherapy is the medical use of ionising radiation. TBI or Total Body Irradiation
COMPANY OVERVIEW January 2018
 COMPANY OVERVIEW January 2018 11 The Company Emerging leader in antigen-directed immunotherapies for cancer Artificial Immune Modulation (AIM TM ) Platform Core technology: artificial Antigen Presenting
COMPANY OVERVIEW January 2018 11 The Company Emerging leader in antigen-directed immunotherapies for cancer Artificial Immune Modulation (AIM TM ) Platform Core technology: artificial Antigen Presenting
Complications after HSCT. ICU Fellowship Training Radboudumc
 Complications after HSCT ICU Fellowship Training Radboudumc Type of HSCT HSCT Improved outcome due to better HLA matching, conditioning regimens, post transplant supportive care Over one-third have pulmonary
Complications after HSCT ICU Fellowship Training Radboudumc Type of HSCT HSCT Improved outcome due to better HLA matching, conditioning regimens, post transplant supportive care Over one-third have pulmonary
Self Tolerance and MHC Restriction. Dr. Issa Abu-Dayyeh
 Self Tolerance and MHC Restriction Dr. Issa Abu-Dayyeh How do we teach B and T cells not to recognise self antigens as dangerous? How do we restrict T cells to recognise only Ags presented on a self MHC
Self Tolerance and MHC Restriction Dr. Issa Abu-Dayyeh How do we teach B and T cells not to recognise self antigens as dangerous? How do we restrict T cells to recognise only Ags presented on a self MHC
CAR T-CELLS: ENGINEERING IMMUNE CELLS TO TREAT CANCER. Roman GALETTO, PhD 17 th Club Phase 1 Annual Meeting April 5 th Paris
 CAR T-CELLS: ENGINEERING IMMUNE CELLS TO TREAT CANCER Roman GALETTO, PhD 17 th Club Phase 1 Annual Meeting April 5 th 2018 - Paris Cellectis, 05-APR-2018 2 FORWARD-LOOKING STATEMENTS THIS PRESENTATION
CAR T-CELLS: ENGINEERING IMMUNE CELLS TO TREAT CANCER Roman GALETTO, PhD 17 th Club Phase 1 Annual Meeting April 5 th 2018 - Paris Cellectis, 05-APR-2018 2 FORWARD-LOOKING STATEMENTS THIS PRESENTATION
Artificial Antigen Presenting Cells as a Standardized Platform for Tumor Infiltrating Lymphocyte (TIL) expansion
 expansion") Artificial Antigen Presenting Cells as a Standardized Platform for Tumor Infiltrating Lymphocyte (TIL) expansion Concurrent Session 404: T cell Manufacturing and Potency 27 th Annual Meeting of the Society
Artificial Antigen Presenting Cells as a Standardized Platform for Tumor Infiltrating Lymphocyte (TIL) expansion Concurrent Session 404: T cell Manufacturing and Potency 27 th Annual Meeting of the Society
Phase 1 Trial of ALN-VSP in Cancers Involving the Liver. Annual Meeting of the Controlled Release Society August 2, 2011
 Phase 1 Trial of ALN-VSP in Cancers Involving the Liver Annual Meeting of the Controlled Release Society August 2, 2011 Agenda ALN-VSP: Background Phase 1 Trial Study Design Safety Data Tumor Response
Phase 1 Trial of ALN-VSP in Cancers Involving the Liver Annual Meeting of the Controlled Release Society August 2, 2011 Agenda ALN-VSP: Background Phase 1 Trial Study Design Safety Data Tumor Response
Designing clinical trials with BiTE antibody constructs by leveraging from nonclinical data. Benno Rattel Biologics Congress Berlin, 2015
 Designing clinical trials with BiTE antibody constructs by leveraging from nonclinical data Benno Rattel Biologics Congress Berlin, 215 1 BiTE Antibody Contructs are Designed to Function as a Bridge between
Designing clinical trials with BiTE antibody constructs by leveraging from nonclinical data Benno Rattel Biologics Congress Berlin, 215 1 BiTE Antibody Contructs are Designed to Function as a Bridge between