UPDATES IN THE SURGICAL PATHOLOGY OF LUNG CANCER. Four Ps of Pulmonary Cytopathology: Procedural, Predictive, Personalized and Participatory
|
|
|
- Morgan Lane
- 6 years ago
- Views:
Transcription
1 UPDATES IN THE SURGICAL PATHOLOGY OF LUNG CANCER Four Ps of Pulmonary Cytopathology: Procedural, Predictive, Personalized and Participatory American Society of Cytopathology Companion Society Symposia United States and Canadian Academy of Pathology (USCAP) Sunday, March 18, 2012 Vancouver, BC William Travis, M.D. Department of Pathology Memorial Sloan Kettering Cancer Center New York, NY
2 Travis WD Lung Cancer Surgical Pathology Update Worldwide, lung cancer is the most common cause of major cancer mortality in men and the second most common in women. 1 Recent therapeutic advances have led to a revolution in the lung cancer field in discovering therapeutically tractable oncogene dependency, that have major implications for patient evaluation and approach to diagnosis. The recently published IASLC/ATS/ERS Classification of Lung Adenocarcinoma addresses these issues. 2 This classification was developed based on an evidence-based approach by an international multidisciplinary panel including pathologists, oncologists/respiratory physicians, radiologists, molecular biologists, and thoracic surgeons. 2 Multiple new approaches are outlined that will have a major influence on clinical practice for pathologists as well as the entire multidisciplinary team caring for patients with lung cancer. Since 70% of patients with lung cancer present with advanced stage disease, 2 their diagnosis is usually established based on small biopsies, cytology specimens or both, and the primary therapy is chemotherapy; the remaining patients usually have resectable lesions and surgery is the primary treatment. To address all types of patients with lung cancer, there are two major components to the classification based on the type of specimen: 1) small biopsies and cytology (Table 1) or 2) resection (Table 2). Because previous WHO classifications did not provide specific criteria and terminology for pathologic diagnosis of lung cancer in small biopsies and cytology, 2 this new classification is more clinically relevant as it addresses these small specimens and addresses molecular testing. In recent years, three therapeutic advances for advanced NSCLC have made accurate histologic diagnosis a critical step for developing an individualized approach to management. The first, relates to tyrosine kinase inhibitors as first line therapy in patients with advanced lung adenocarcinoma with EGFR mutations. 3 For this reason, in the new classification EGFR mutation testing is recommended for advanced lung cancer patients with a histologic diagnosis of adenocarcinoma. Second, patients with adenocarcinoma or NSCLC, not otherwise specified (NSCLC-NOS) are more responsive to pemetrexed than those squamous cell carcinoma. 4 Third, squamous cell carcinoma is associated with life threatening hemorrhage in patients treated with bevacizumab; therefore, this drug is contraindicated in lung cancer patients with this histology. 5 So a pathologic diagnosis of adenocarcinoma or squamous cell carcinoma will determine patient eligibility for EGFR mutation testing and for specific therapies. In all of these clinical trials the pathologic diagnoses were based on light microscopy with or without mucin stains but not on the basis of immunohistochemical stains. 3-5 Other emerging genetic advances hold future promise for molecular targeted therapies such as 1) crizotinib which appears to be effective in adenocarcinoma patients with EML4-ALK translocations 6 and 2) the recent discoveries of FGFR1 amplification and DDR2 mutations in squamous cell carcinoma, 7;8 which may render patients exquisitely sensitive to FGFR inhibition and dasatinib respectively. CLASSIFICATION BASED ON SMALL BIOPSIES AND CYTOLOGY Given the need to individualize lung cancer therapy based on the histologic type of lung cancer and molecular status, the pathologist s role and approach to lung cancer diagnosis in small biopsies and cytology have been affected substantially. 9 2
3 Travis WD Lung Cancer Surgical Pathology Update The need to classify non-small cell carcinoma (NSCLC) further to distinguish squamous cell carcinoma from adenocarcinoma has not existed until recently so the frequency of NSCLC-not otherwise specified (NOS) has been increasing up to 20-40%. 10 Pathologists now need to make an effort to make a more specific diagnosis using special stains. 11;12 Tumors that show morphologic squamous or adenocarcinoma differentiation can be classified as squamous cell carcinoma or adenocarcinoma, respectively. However, for those tumors that lack clear differentiation by morphology and would be classified as NSCLC-NOS in the past, now need to be evaluated by immunohistochemistry. The recommendation is to use a single adenocarcinoma marker such as TTF-1 and a single squamous marker such as the recently described p40 antibody. 13 Intensive investigation of other adenocarcinoma (napsin-a) and squamous (p63, CK5/6) immunohistochemical markers are ongoing. 2;13;14 Cytology is a powerful tool for subclassifying lung cancers in the separation of adenocarcinoma versus squamous cell carcinoma with high diagnostic accuracy that can exceed 90%. 15 If a NSCLC-NOS by light microscopy shows a staining pattern that clearly points to adenocarcinoma (TTF-1 positive, p40 negative), the tumor can be classified as NSCLC, favor adenocarcinoma (Table 1). If such a tumor stains with a squamous pattern (p40 positive, TTF-1 negative), then it can be called NSCLC, favor squamous cell carcinoma. If the tumor does not show clear differentiation by immunohistochemistry, it should remain classified as NSCLC-NOS. These terms and criteria will help track the former NOS tumors that are being reclassified with the addition of special stains for future clinical trials as the current trial data are based on light microscopic diagnoses without special stains. Advanced stage tumors classified as adenocarcinoma, NSCLC, favor adenocarcinoma or NSCLC-NOS should be tested for EGFR mutation; mutation positive patients are eligible for tyrosine kinase inhibitor therapy. If there is no EGFR mutation, recent data suggest these patients are candidates for EML4-ALK fusion testing, and if this testing is positive, these patients may benefit from the FDA-approved drug crizotinib, 6 and if negative these patients are eligible for pemetrexed or bevacizumab based chemotherapeutic regimens. In the new classification, a limited use of special stains is recommended for NSCLC-NOS by light microscopy to try further classifying these tumors. Minimizing special stains is helpful to maximize the amount of tissue available for molecular testing. 2 A new responsibility for pathologists, in addition to making a correct diagnosis is to manage these small biopsies and cytology specimens strategically so there is sufficient tissue preserved for molecular studies. A new emphasis is placed on the need for a multidisciplinary approach to lung cancer diagnosis. One of the central proposals in this classification is that each institution should have a comprehensive strategy that addresses how to obtain these small specimens, how to process them in the pathology laboratory, how to preserve material for molecular testing, sending specimens to the molecular laboratory for expedited testing and the reporting the results in a pathology report. It may be useful to have a multidisciplinary committee to develop this strategy and to monitor issues in an ongoing fashion. CLASSIFICATION BASED ON RESECTION SPECIMENS 3
4 Travis WD Lung Cancer Surgical Pathology Update Major changes are also recommended for adenocarcinomas diagnosed in resection specimens (Table 2): 2 1) the term bronchioloalveolar carcinoma (BAC) should not be used anymore, because tumors previously classified as BAC are represented by five different tumors in this classification; 2), for solitary tumors measuring 3cm, new concepts of adenocarcinoma in situ (AIS) and minimally invasive adenocarcinoma (MIA) have been introduced for lesions that have no invasion or 5mm invasion, respectively; these patients should have 100% or near 100% disease free survival (DFS); 3) for invasive adenocarcinomas, comprehensive histologic subtyping is recommended for evaluation with classification according to the predominant subtype; 4) micropapillary adenocarcinoma is proposed as a new subtype with a poor prognosis; 5) the term lepidic replaces BAC for tumors with a predominant component formerly called non-mucinous BAC, and the term lepidic predominant adenocarcinoma (LPA) is recommended along with discontinuing the term mixed subtype ; and 6) invasive mucinous adenocarcinoma (IMA) is the term used to replace those formerly classified as mucinous BAC. IMA are strongly correlated with KRAS mutation. EGFR mutations are reported to be associated with AIS, LPA, papillary and micropapillary patterns and EML4-ALK translocations with acinar, cribriform and signet ring patterns. 2;16 The classification stratifies resected tumors into prognostically significant histologic subtypes with excellent (AIS and MIA), intermediate (lepidic, acinar and papillary) and poor prognosis (solid, micropapillary, invasive mucinous and colloid) In summary this classification outlines many new approaches in lung cancer diagnosis that underscore the importance of histology and genetics in individualizing treatment for patients with lung cancer. Evidence-based recommendations are made that will transform the clinical practice of all physicians involved with lung cancer diagnosis. Acknowledgements: I would like to acknowledge the contributions of all the IASLC/ATS/ERS panel members who contributed to this work and were co-authors of the article published in primary article in the Journal of Thoracic Oncology, especially Dr. Elisabeth Brambilla who contributed to development of this document. 4
5 Travis WD Lung Cancer Surgical Pathology Update TABLE 1: IASLC/ATS/ERS CLASSIFICATION FOR SMALL BIOPSIES/CYTOLOGY 2004 WHO Classification Morphology/Stains IASLC/ATS/ERS Terminology ADENOCARCINOMA Mixed subtype Acinar Papillary Solid Bronchioloalveolar carcinoma, nonmucinous Bronchioloalveolar carcinoma, mucinous No 2004 WHO counterpart most will be solid adenocarcinomas Morphologic adenocarcinoma patterns clearly present Morphologic adenocarcinoma patterns not present (supported by special stains, i.e. +TTF-1) Adenocarcinoma, describe identifiable patterns present (including micropapillary pattern not included in 2004 WHO classification) Adenocarcinoma with lepidic pattern (if pure, add note: an invasive component cannot be excluded) Mucinous adenocarcinoma (describe patterns present) Non-small cell carcinoma, favor adenocarcinoma SQUAMOUS CELL CARCINOMA No 2004 WHO counterpart LARGE CELL CARCINOMA Morphologic squamous cell patterns clearly present Morphologic squamous cell patterns not present (supported by stains i.e. +p40) No clear adenocarcinoma, squamous or neuroendocrine morphology or staining pattern Squamous cell carcinoma Non-small cell carcinoma, favor squamous cell carcinoma Non-small cell carcinoma, not otherwise specified (NOS) Modified from reference 2 NSCLC-NOS pattern can be seen not only in large cell carcinomas but also when the solid poorly differentiated component of adenocarcinomas or squamous cell carcinomas are sampled but do not express immunohistochemical markers or mucin 5
6 Travis WD Lung Cancer Surgical Pathology Update TABLE 2: IASLC/ATS/ERS CLASSIFICATION OF LUNG ADENOCARCINOMA IN RESECTION SPECIMENS PREINVASIVE LESIONS Atypical adenomatous hyperplasia Adenocarcinoma in situ ( 3 cm formerly BAC) - nonmucinous - mucinous - mixed mucinous/non-mucinous MINIMALLY INVASIVE ADENOCARCINOMA ( 3 cm lepidic predominant tumor with 5 mm invasion) -nonmucinous -mucinous - mixed mucinous/non-mucinous INVASIVE ADENOCARCINOMA Lepidic predominant (formerly non-mucinous BAC pattern, with >5 mm invasion) Acinar predominant Papillary predominant Micropapillary predominant Solid predominant with mucin production VARIANTS OF INVASIVE ADENOCARCINOMA Invasive mucinous adenocarcinoma (formerly mucinous BAC) Colloid Fetal (low and high grade) Enteric From reference 2 6
7 Travis WD Lung Cancer Surgical Pathology Update Reference List (1) Jemal A, Center MM, DeSantis C, Ward EM. Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiol Biomarkers Prev 2010;19: (2) Travis WD, Brambilla E, Noguchi M et al. The New IASLC/ATS/ERS International Multidisciplinary Lung Adenocarcinoma Classification. J Thoracic Oncol 2011;6: (3) Mok TS, Wu YL, Thongprasert S et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med 2009;361: (4) Scagliotti GV, Parikh P, von PJ et al. Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-small-cell lung cancer. J Clin Oncol 2008;26: (5) Johnson DH, Fehrenbacher L, Novotny WF et al. Randomized phase II trial comparing bevacizumab plus carboplatin and paclitaxel with carboplatin and paclitaxel alone in previously untreated locally advanced or metastatic non-smallcell lung cancer. J Clin Oncol 2004;22: (6) Kwak EL, Bang YJ, Camidge DR et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N Engl J Med 2010;363: (7) Dutt A, Ramos AH, Hammerman PS et al. Inhibitor-Sensitive FGFR1 Amplification in Human Non-Small Cell Lung Cancer. PLoS ONE 2011;6:e (8) Hammerman PS, Sos ML, Ramos AH et al. Mutations in the DDR2 Kinase Gene Identify a Novel Therapeutic Target in Squamous Cell Lung Cancer. Cancer Discov 2011;1: (9) Travis WD, Brambilla E, Van SP et al. Paradigm shifts in lung cancer as defined in the new IASLC/ATS/ERS lung adenocarcinoma classification. Eur Respir J 2011;38: (10) Ou SH, Zell JA. Carcinoma NOS is a Common Histologic Diagnosis and is Increasing in Proportion Among Non-small Cell Lung Cancer Histologies. J Thorac Oncol 2009;4: (11) Travis WD, Rekhtman N. Pathological diagnosis and classification of lung cancer in small biopsies and cytology: strategic management of tissue for molecular testing. Semin Respir Crit Care Med 2011;32: (12) Travis WD, Rekhtman N, Riley GJ et al. Pathologic diagnosis of advanced lung cancer based on small biopsies and cytology: a paradigm shift. J Thorac Oncol 2010;5:
8 Travis WD Lung Cancer Surgical Pathology Update (13) Bishop JA, Teruya-Feldstein J, Westra WH, Pelosi G, Travis WD, Rekhtman N. p40 (DeltaNp63) is superior to p63 for the diagnosis of pulmonary squamous cell carcinoma. Mod Pathol (14) Rekhtman N, Ang DC, Sima CS, Travis WD, Moreira AL. Immunohistochemical algorithm for differentiation of lung adenocarcinoma and squamous cell carcinoma based on large series of whole-tissue sections with validation in small specimens. Mod Pathol 2011;24: (15) Rekhtman N, Brandt SM, Sigel CS et al. Suitability of Thoracic Cytology for New Therapeutic Paradigms in Non-Small Cell Lung Carcinoma: High Accuracy of Tumor Subtyping and Feasibility of EGFR and KRAS Molecular Testing. Journal of Thoracic Oncology 2011;6: (16) McLeer-Florin A, Moro-Sibilot D, Melis A et al. Dual IHC and FISH Testing for ALK Gene Rearrangement in Lung Adenocarcinomas in a Routine Practice: A French Study. J Thorac Oncol (17) Yoshizawa A, Motoi N, Riely GJ et al. Impact of proposed IASLC/ATS/ERS classification of lung adenocarcinoma: prognostic subgroups and implications for further revision of staging based on analysis of 514 stage I cases. Mod Pathol 2011;24: (18) Russell PA, Wainer Z, Wright GM, Daniels M, Conron M, Williams RA. Does lung adenocarcinoma subtype predict patient survival?: A clinicopathologic study based on the new International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society international multidisciplinary lung adenocarcinoma classification. J Thorac Oncol 2011;6: (19) Warth A, Muley T, Meister M et al. Back to the Roots: The Novel Histologic IASLC/ATS/ERS Classification System of Invasive Pulmonary Adenocarcinoma is a Stage-Independent Predictor of Survival. J Clin Oncol 2011;In press. 8
9 UPDATES IN THE SURGICAL PATHOLOGY OF LUNG CANCER Four Ps of Pulmonary Cytopathology: Procedural, Predictive, Personalized and Participatory American Society of Cytopathology, USCAP Vancouver, BC; March 18, 2012 William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY
10 RATIONALE FOR NEW ADENOCARCINOMA CLASSIFICATION Lung cancer most frequent cause major cancer incidence/mortality worldwide Adenocarcinoma the most common histologic subtype Widely divergent clinical, radiologic, molecular & pathologic spectrum Bronchioloalveolar carcinoma (BAC) confusing used many different ways despite 99/04 WHO; mucinous/nonmucinous Rapid evolving molecular advances (EGFR)
11 IASLC/ATS/ERS ADENOCARCINOMA CLASSIFCATION: MULTIDISCIPLINARY APPROACH Prior WHO classifications: by pathologists Due to remarkable advances in past 10 yrs: oncology, molecular, radiology, surgery: need for integrated multidisciplinary approach International Association for the Study of Lung Cancer (IASLC); American Thoracic Society (ATS), European Respiratory Society (ERS) Panel: Pathologists, Oncologists, Radiologists, Molecular Biologists, Surgeons

12 Courtesy of Marc Ladanyi, MSKCC


13 Journal of Thoracic Oncology 6(2): , 2011
14 Personalized Therapy For Lung Cancer Patients is Driven by Histology and Genetics Predictive of response EGFR mutation (adenoca) EGFR TKI s Adenoca or NSCLC-NOS pemetrexed EML4-ALK translocation (adenoca)- crizotinib Predictive of toxicity Bevacizumab contraindicated in lifethreatening hemorrhage in squamous carcinoma
15 Results in EGFR mutation positive and negative patients ( All Asian, 94% Never Smokers) EGFR mutation positive EGFR mutation negative Probability of progression-free survival At risk : Gefitinib C / P Gefitinib (n=132) Carboplatin / paclitaxel (n=129) HR (95% CI) = 0.48 (0.36, 0.64) p< No. events gefitinib: 97 No. events Chemo: Months Probability of progression-free survival Gefitinib (n=91) Carboplatin / paclitaxel (n=85) HR (95% CI) = 2.85 (2.05, 3.98) p< No. events gefitinib: 88 No. events Chemo: Months Gefitinib CR/PR Rate 71% CBP/PTX CR/PR Rate 47% Mok N Engl J Med 361: , 2009 Gefitinib CR/PR Rate 1% CBP/PTX CR/PR Rate 24%
16 First Line TKI Therapy in EGFR Mutated NSCLC Study N Treatmen t Arm Control Arm Stage Median PFS Media n OS Indication Study Type Mok T N Engl J Med 361:947, 2009 IPASS 1217 Gefitinib Carboplatin/ Pactilaxel IIIB/IV 5.7 vs 5.8 mo (HR for EGFR mutated pts 0.48; HR for nmutated pts 2.84) 18.6 vs 17.3 months (P = NS) Firstline Randomize d Phase III Mitsudomi T Lancet Oncol 11:121, 2010 WJTOG (M+) Gefitinib Cisplatin, Docetaxel IIIB/IV 9.2 vs 6.3 mo (P < 0.001) First-line Randomize d Phase III Maemondo M N Engl J Med 362:2380, (M+) Gefitinib Carboplatin, Paclitaxel IIIB/IV 10.8 vs 5.4 mo (HR 0.3, P < ) 30.5 vs 23.6 months (P = NS) First-line Randomize d Phase III Zhou C Lancet Oncol 12:735, 2011 Optimal 165 (M+) Erlotinib Carboplatin/ Gemciatbine IIIB/IV 13.6 vs 4.6 mo (HR 0.16, P < ) First-line Randomize d Phase III Rosell R J Clin Oncol 29: Suppl (M+) Erlotinib Platinumbased chemothera IIIB/IV 9.4 vs 5.2 mo (HR, 0.42, P < ) 22.9 vs 18.8 months First-line Randomize d Phase III
17 CLINICAL RECOMMENDATION In patients with advanced lung adenocarcinoma we recommend testing for EGFR mutation (strong recommendation, moderate quality evidence). Remarks: This is a strong recommendation because potential benefits clearly outweigh harms. This recommendation assumes that correct classification by EGFR mutation status is associated with important benefit based upon randomized phase 3 clinical trials of EGFR TKI therapy which demonstrate a predictive benefit for response rate and progression-free survival, but not overall survival, as well as subset analyses of multiple additional studies. Travis WD et al; JTO 6: , 2011
18 PEMETREXED IS MORE EFFECTIVE IN ADCA AND LARGE CELL CA THAN SQUAMOUS CA 100 Scagliotti G et al JCO 26: , 2008 Patients Randomized to Pemetrexed Percent Surviving 50 Squamous: Median = 6.2 Non-squamous: Median = 9.2 Overall Survival p=0.001 Prog Free Survival (not shown) p= Overall Survival (months)

19 CRIZOTINIB ALK INHIBITON IN NSCLC Kwak EL et al; NEJM 2010; 363:1693
20 Initial Therapy of Advanced Adenoca or NSCLC-NOS Adenocarcinoma Large cell ca NSCLC-NOS EGFR Mutation Exon 19 del Exon 21 L858R, L861X Exon 18 G719A/S Neg EGFR mut Pos EML4-ALK Neg EGFR mut Neg EML4-ALK Unknown EGFR Mutation & ALK Status Erlotinib/Gefitinib ± Pem/Bev/Cis Crizotinib Pemetrexed Bevacizumab Cisplatin Modified from Mark Kris, Chief, Thoracic Oncology, MSKCC
21 Molecular Characteristics Used to Select Patients for Protocols at MSK EGFR EGFR + T790M KRAS MET Amplification EML4-ALK BRAF, MEK HER2 PIK3CA PF Erlotinib (Adjuvant) BIBW Cetuximab Ridaforolimus GI-4000 (G12C,V,D) (Adjuvant) Crizotinib Crizotinib Zelboraf (vemurafenib) Selumetinib (AZ6244) GSK PF GSK Courtesy of Mark Kris, Chief, Thoracic Oncology, MSKCC
22 P. S. Hammerman, et a: Cancer. Cancer Discov 1:78-89, NCI TCGA The Cancer Genome Atlas Preliminary Analysis 150 Squamous Ca Gene Event type Frequency FGFR1 Amplification 20-25% FGFR2 Mutation 5% PIK3CA Mutation 9% PTEN Mutation/Deletion 18% CCND1 Amplification 8% CDKN2A Deletion/mutation 45% PDGFRA Amplification/mutation 9% EGFR Amplification 10% MCL1 Amplification 10% DDR2 Mutation 4% ERBB2 Amplification 2% Hammerman P, JTO 2011; 6: S2, S39 Possible therapeutic target identified in 63% of Squamous cell ca Targets need to be validated in pre-clinical models P. S. Hammerman, et al: DDR2. Cancer Discov 1:78-89, J. Weiss, et a; FGFR1. Sci.Transl.Med. 2 (62):62ra93, 2010 FGFR1/2, PIK3CA and DDR2 inhibitor trials are planned or ongoing
23 LUNG ADENOCARCINOMA CLASSIFICATION IN SMALL BIOPSY AND CYTOLOGY SPECIMENS Because this was never addressed by WHO, by necessity other histologies needed to be addressed


24 NON-SMALL CELL LUNG CANCER: 70% PRESENT IN ADVANCED STAGE
25 SMALL BIOPSY/CYTOLOGY LUNG CANCER DIAGNOSIS: IN USA OVER 130,000 CASES IN : ACS estimates for USA: 221,130 Lung Cancers Sigel RA et al: CA Cancer J Clin 2011:61:epub 85% NSCLC = 187,961 (15% SCLC) 70% Advanced Stage = 131,572 Unresectable: Diagnosed by small biopsies/cytology


26 PHASE III STUDY COMPARING CISPLATIN PLUS GEMCITABINE WITH CISPLATIN & PEMETREXED IN ADVANCED NSCLC Scagliotti G, et al: JCO 26: , 2008


27 PHASE III STUDY COMPARING CISPLATIN PLUS GEMCITABINE WITH CISPLATIN & PEMETREXED IN ADVANCED NSCLC Scagliotti G, et al: JCO 26: , 2008

28 SPECIAL STAINS ARE INTRODUCED TO CLASSIFY NSCLC-NOS FURTHER Travis WD et al; JTO 6: , 2011
:244-485,")
29 SMALL BIOPSY AND CYTOLOGY IASLC/ATS/ERS SPECIFIC TERMINOLOGY RECOMMENDED FOR LUNG CANCER DIAGNOSES Journal of Thoracic Oncology 6(2): , 2011
30 IASLC/ATS/ERS TERMINOLOGY FOR SMALL BIOPSIES AND CYTOLOGY 2004 WHO CLASSIFICATION 2011 IASLC/ATS/ERS CLASSIFICATION ADENOCARCINOMA Mixed subtype Acinar Papillary Solid Bronchioloalveolar No 2004 WHO counterpart most will be solid adenocarcinomas SQUAMOUS CELL CARCINOMA Papillary Clear cell Small cell Basaloid No 2004 WHO counterpart LARGE CELL CARCINOMA J Thoracic Oncol: 6: , 2011 Morphologic adenocarcinoma patterns clearly present: Adenocarcinoma, describe identifiable patterns present (including micropapillary pattern not included in 2004 WHO classification) Morphologic adenocarcinoma patterns not present (supported by special stains): Non-small cell carcinoma, favor adenocarcinoma Morphologic squamous cell patterns clearly present: Squamous cell carcinoma Morphologic squamous cell patterns not present (supported by stains): Non-small cell carcinoma, favor squamous cell carcinoma Non-small cell carcinoma, not otherwise specified (NOS)
31 IMMUNOHISTOCHEMICAL MARKERS ADENOCARCINOMA (ONE MARKER) TTF-1 (best), Napsin, PE-10 SQUAMOUS CARCINOMA (ONE MARKER) p40 (best), p63, CK5/6, 34βE12 Desmocolin-3 (need more testing) Cocktails nuclear/cytoplasmic antibodies Adenoca TTF-1/Napsin Squamous p63/ck5/6
32 p40 antibody (5-17, Calbiochem, 1:2000)


33 NSCLC-NOS BY LIGHT MICROSCOPY


34 NSCLC FAVOR ADENOCARCINOMA TTF-1 P63


35 NSCLC FAVOR ADENOCARCINOMA TOUCH PREP CYTOLOGY
36 NSCLC-NOS, FAVOR ADENOCARCINOMA CONFIRMED BY MOLECULAR EGFR mutation - negative Exon 19 deletion Exon 21 L858R mutation KRAS mutation - positive G12V Results favor adenocarcinoma

37 CYTOLOGY IS A POWERFUL TOOL FOR CLASSIFYING NSCLC J Thoracic Oncol 6:451-8, 2011
38 NSCLC DIAGNOSED BY LIGHT MICROSCOPY IN SMALL BIOPSIES/CYTOLOGY SQUAMOUS CELL CARCINOMA NSCLC-NOS 20-30% 20-40% HISTORICALLY NSCLC-NOS HAS BEEN ENCOURAGED BECAUSE THERE WAS NO REASON TO CLASSIFY THESE TUMORS FURTHER ADENO- CARCINOMA 40-50% AS A RESULT 20-40% OF NSCLC IN SMALL BIOPSIES/CYTOLOGY ARE CURRENTLY BEING DIAGNOSED AS NSCLC-NOS
39 LIGHT MICROSCOPY SQUAMOUS CELL CARCINOMA 20-30% FORMER NSCLC- NOS:20-40% OF NSCLC NEW CLASSIFI- CATION NSCLC, FAVOR SQUAMOUS CELL CARCINOMA NSCLC-NOS ADENO- CARCINOMA 20-40% 40-50% NSCLC-NOS <5% NSCLC, FAVOR ADENO- CARCINOMA METASTASIS OR OTHER TUMOR
40 LIGHT MICROSCOPY SQUAMOUS CELL CARCINOMA 20-30% FORMER NSCLC- NOS:20-40% OF NSCLC NEW CLASSIFI- CATION NSCLC-NOS 20-40% ADENO- CARCINOMA 40-50% NSCLC-NOS Goal <5%
41 NEED TO DISCRIMINATE BETWEEN DIAGNOSES BASED ON LIGHT MICROSCOPY VS LM & IHC The only validation of histology for EGFR mutation/tki s, Pemetrexed and Bevacizumab is by light microscopy alone The use of IHC for diagnosis is not validated in clinical trials
42 EGFR MUTATION SPECIFIC ANTIBODIES (Cell Signaling) Exon 19 deletion All 20 cases with 15-bp deletion were MS Ab positive (sensitivity 100%, specificity 99%) 35 other than the common 15bp deletion 49% stained positively (sensitivity 74%) EGFR L858R mutation 17/18 cases were positive with MS Ab (sensitivity 95%, specificity 99%); better if use 2+/3+ for positive Brevet M et al: J Mol Diagn 12: , 2010

43 EGFR EXON 21 L858R MUTATION SPECIFIC AB Brevet M et al: J Mol Diagn 12: , 2010

44 EGFR EXON 19 DELETION MUTATION SPECIFIC AB Brevet M et al: J Mol Diagn 12: , 2010
45 TISSUE MANAGEMENT Each group of thoracic physicians (clinicians, radiologists, surgeons, pathologists, molecular biologists) must develop a strategy to manage tissues Obtaining biopsies or cytology samples Optimal processing by laboratories/pathologists for diagnosis AND molecular studies Pathologists should be the leader of this
46 KEY PRINCIPLES Minimize diagnostic stains to maximize tissue for molecular studies Molecular testing is reliable on FFPE tissues even very small samples Unstained slides (n=10-15) provide adequate DNA if sufficient tumor Cytology fluids (i.e. pleural) cytospin and make cell block (for IHC/molecular)



47 PERSONALIZED MEDICINE IN ADVANCED LUNG CANCER PATIENTS IS DRIVEN BY HISTOLOGY AND GENETICS
48 LUNG ADENOCARCINOMA CLASSIFICATION IN RESECTION SPECIMENS
49 OLD BAC CONCEPT FIVE PLACES IN NEW CLASSIFICATION 1. Adenocarcinoma in situ (AIS) which can be nonmucinous and rarely mucinous 2. Minimally invasive adenocarcinoma 3. Invasive adenocarcinoma with predominant nonmucinous lepidic pattern 4. Invasive adenocarcinoma with less than predominant nonmucinous lepidic pattern (probably most formerly clinically advanced adenocarcinomas with BAC pattern) 5. Mucinous adenocarcinoma with lepidic pattern
50 IASLC/ATS/ERS ADENOCARCINOMA PREINVASIVE LESIONS CLASSIFICATION ATYPICAL ADENOMATOUS HYPERPLASIA ADENOCARCINOMA IN SITU ( 3 cm, formerly BAC pattern) non-mucinous mucinous MINIMALLY INVASIVE ADENOCARCINOMA ( 3 cm, a lepidic predominant tumor with 5mm invasion) INVASIVE ADENOCARCINOMA Size should be specified. AIS and MIA should be completely sampled histologically

51 ATYPICAL ADENOMATOUS HYPERPLASIA


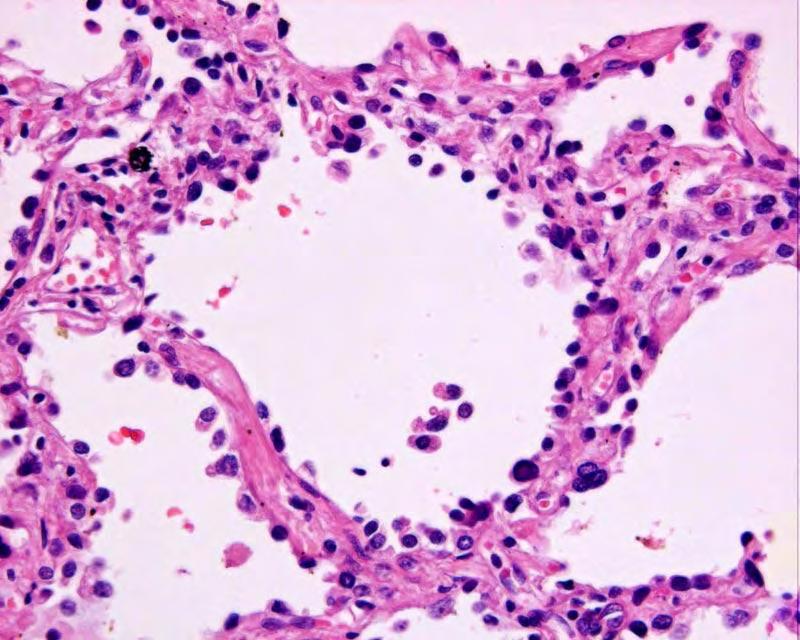
52 ADENOCARCINOMA IN SITU NONMUCINOUS


53 ADENOCARCINOMA IN SITU NONMUCINOUS
54 IASLC/ATS/ERS ADENOCARCINOMA PREINVASIVE LESIONS CLASSIFICATION ATYPICAL ADENOMATOUS HYPERPLASIA ADENOCARCINOMA IN SITU ( 3 cm, formerly BAC pattern) non-mucinous mucinous MINIMALLY INVASIVE ADENOCARCINOMA ( 3 cm, a lepidic predominant tumor with 5mm invasion) INVASIVE ADENOCARCINOMA Size should be specified. AIS and MIA should be completely sampled histologically



55 MINIMALLY INVASIVE ADENOCA NONMUCINOUS

56 MINIMALLY INVASIVE ADENOCA NONMUCINOUS
57 IASLC/ATS/ERS ADENOCARCINOMA CLASSIFICATION INVASIVE ADENOCARCINOMA Lepidic pattern predominant (formerly nonmucinous BAC pattern) Acinar pattern predominant Papillary pattern predominant Micropapillary pattern, predominant Solid pattern predominant (Comprehensive histologic subtyping: semiquantitative assessment of patterns in 5-10% increments)



58 LEPIDIC PREDOMINANT


59 ACINAR PAPILLARY



60 MICRO- PAPILLARY SOLID WITH MUCIN DPAS STAIN


61 INVASIVE MUCINOUS ADENOCARCINOMA


62 INVASIVE MUCINOUS ADENOCARCINOMA Frequent KRAS mutations
 5 Year RFS % AIS (1) 100 MIA (8) 100 Lepidic NM (29) 90 Papillary (143) 83 Acinar (232) 85 Inv Mucinous Ad (13) 76 Solid")
63 STAGE I ADENOCARCINOMA (N=514) RECURRENCE-FREE SURVIVAL (RFS) BY IASLC HISTOLOGIC TYPE AIS, MIA Lepidic, Papillary & Acinar Predominant Micropapillary & Solid Predominant Colloid, Mucinous Ad P=0.003 Yoshizawa, A et al; Modern Pathology 24: , 2011 Histologic Type (N) 5 Year RFS % AIS (1) 100 MIA (8) 100 Lepidic NM (29) 90 Papillary (143) 83 Acinar (232) 85 Inv Mucinous Ad (13) 76 Solid (67) 71 Micropapillary (12) 64 Colloid (9) 71



 Nitadori")
64 MICROPAPILLARY ADCA IS AN INDEPENDENT PREDICTOR OF RECURRENCE IN LIMITED RESECTIONS (</=2CM) Nitadori J & Adusumilli P, et al JTO 6: S564, 2011
65 COMBINED ARCHITECTURAL AND MITOTIC GRADING Kadota K et al (in preparation)


66 Tumor Size Difficult to Appreciate Grossly If Lepidic Growth



67 CASE 1: 68F, Multiple, bilateral GGN Dx: Adenocarcinoma with lepidic pattern
68 CASE 1: 68F, Multiple, bilateral GGN PATHOLOGY Dx: Adenocarcinoma with lepidic pattern PATHOLOGY DIFFERENTIAL DIAGNOSIS Adenocarcinoma in situ Minimally invasive adenocarcinoma Adenocarcinoma with lepidic pattern Lepidic predominant Invasive predominant


69 CASE 1: 68F, Multiple, bilateral GGN
70 CASE 1: 68F, Multiple, bilateral GGN RADIOLOGIC PATHOLOGIC CORRELATION Most likely diagnosis: Adenocarcinoma in situ Minimally invasive adenocarcinoma Less likely diagnosis Adenocarcinoma with lepidic pattern Lepidic predominant Invasive predominant

71 CASE 2: 73F, Left Lung Mass Adenocarcinoma with lepidic pattern

72 CASE 2: 73F, Left Lung Mass Adenocarcinoma with lepidic pattern possible focus of invasion
73 CASE 2: 73F, Left Lung Mass PATHOLOGY Dx: Adenocarcinoma with lepidic pattern focus suspicious for invasion PATHOLOGY DIFFERENTIAL DIAGNOSIS Adenocarcinoma in situ Minimally invasive adenocarcinoma Adenocarcinoma with lepidic pattern Lepidic predominant Invasive predominant


74 CASE 2: 73F, Left Lung Mass Part Solid Nodule
75 CASE 2: 73F, Left Lung Mass RADIOLOGIC PATHOLOGIC CORRELATION Most likely diagnosis: Adenocarcinoma with lepidic pattern Invasive predominant Lepidic predominant Less likely diagnosis Adenocarcinoma in situ Minimally invasive adenocarcinoma
HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY
 HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY 7 TH Annual New York Lung Cancer Symposium Saturday, November 10, 2012 William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering
HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY 7 TH Annual New York Lung Cancer Symposium Saturday, November 10, 2012 William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering
THE IASLC/ERS/ATS ADENOCARCINOMA CLASSIFICATION RATIONALE AND STRENGTHS
 THE IASLC/ERS/ATS ADENOCARCINOMA CLASSIFICATION RATIONALE AND STRENGTHS PULMONARY PATHOLOGY SOCIETY USCAP, BALTIMORE, March 2, 2013 William D. Travis, M.D. Dept of Pathology, Memorial Sloan-Kettering Cancer
THE IASLC/ERS/ATS ADENOCARCINOMA CLASSIFICATION RATIONALE AND STRENGTHS PULMONARY PATHOLOGY SOCIETY USCAP, BALTIMORE, March 2, 2013 William D. Travis, M.D. Dept of Pathology, Memorial Sloan-Kettering Cancer
Disclosure of Relevant Financial Relationships NON-SMALL CELL LUNG CANCER: 70% PRESENT IN ADVANCED STAGE
 MORPHOLOGY AND MOLECULAR TESTING IN NON-SMALL CELL OF LUNG NEW FRONTIEIRS IN CYTOPATHOLOGY PRACTICE American Society for Cytopathology San Antonio, Texas Sunday March 5, 2017 Disclosure of Relevant Financial
MORPHOLOGY AND MOLECULAR TESTING IN NON-SMALL CELL OF LUNG NEW FRONTIEIRS IN CYTOPATHOLOGY PRACTICE American Society for Cytopathology San Antonio, Texas Sunday March 5, 2017 Disclosure of Relevant Financial
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Non-Small Cell Lung Carcinoma - Myers
 Role of Routine Histology and Special Testing in Managing Patients with Non- Small Cell Lung Carcinoma Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of
Role of Routine Histology and Special Testing in Managing Patients with Non- Small Cell Lung Carcinoma Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach
 The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
Steering Committee. Waiting on photo. Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD.
 Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Disclosures Genomic testing in lung cancer
 Disclosures Genomic testing in lung cancer No disclosures Objectives Understand how FISH and NGS provide complementary data for the evaluation of lung cancer Recognize the challenges of performing testing
Disclosures Genomic testing in lung cancer No disclosures Objectives Understand how FISH and NGS provide complementary data for the evaluation of lung cancer Recognize the challenges of performing testing
LUNG CANCER. pathology & molecular biology. Izidor Kern University Clinic Golnik, Slovenia
 LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
The new international multidisciplinary lung adenocarcinoma
 Eur Respir J 2011; 38: 239 243 DOI: 10.1183/09031936.00026711 CopyrightßERS 2011 EDITORIAL Paradigm shifts in lung cancer as defined in the new IASLC/ATS/ERS lung adenocarcinoma classification W.D. Travis*,"",
Eur Respir J 2011; 38: 239 243 DOI: 10.1183/09031936.00026711 CopyrightßERS 2011 EDITORIAL Paradigm shifts in lung cancer as defined in the new IASLC/ATS/ERS lung adenocarcinoma classification W.D. Travis*,"",
Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination
 National Quality Strategy Domain: Communication and Care Coordination") Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Lung Neoplasia II Resection specimens Pathobasic. Lukas Bubendorf Pathology
 Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD. Mount Carrigain 2/4/17
 Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD Mount Carrigain 2/4/17 Histology Adenocarcinoma: Mixed subtype, acinar, papillary, solid, micropapillary, lepidic
Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD Mount Carrigain 2/4/17 Histology Adenocarcinoma: Mixed subtype, acinar, papillary, solid, micropapillary, lepidic
Molecular Targets in Lung Cancer
 Molecular Targets in Lung Cancer Robert Ramirez, DO, FACP Thoracic and Neuroendocrine Oncology November 18 th, 2016 Disclosures Consulting and speaker fees for Ipsen Pharmaceuticals, AstraZeneca and Merck
Molecular Targets in Lung Cancer Robert Ramirez, DO, FACP Thoracic and Neuroendocrine Oncology November 18 th, 2016 Disclosures Consulting and speaker fees for Ipsen Pharmaceuticals, AstraZeneca and Merck
Classification of non-small cell lung carcinomas (NSCLC)
") Classification of non-small cell lung carcinomas (NSCLC) 1. NordiQC Conference on Standardization in Applied Immunohistochemistry 4-7 June 2013 Birgit Guldhammer Skov, MD. DMeSci, Dept. Of Pathology, Rigshospitalet,
Classification of non-small cell lung carcinomas (NSCLC) 1. NordiQC Conference on Standardization in Applied Immunohistochemistry 4-7 June 2013 Birgit Guldhammer Skov, MD. DMeSci, Dept. Of Pathology, Rigshospitalet,
Molecular Testing in Lung Cancer
 Molecular Testing in Lung Cancer Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in lung cancer Source: Khono et al, Trans
Molecular Testing in Lung Cancer Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in lung cancer Source: Khono et al, Trans
Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination
 National Quality Strategy Domain: Communication and Care Coordination") Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE:
Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE:
International association for the study of lung cancer/american thoracic society/european respiratory
 International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. William Travis, Elisabeth
International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. William Travis, Elisabeth
Personalized Medicine: Lung Biopsy and Tumor
 Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Elizabeth H. Moore, MD Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Genomic testing has resulted in a paradigm shift in the
Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Elizabeth H. Moore, MD Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Genomic testing has resulted in a paradigm shift in the
Ground Glass Opacities
 Ground Glass Opacities A pathologist s perspective Marie-Christine Aubry, M.D. Professor of Pathology Mayo Clinic Objectives Discuss the proposed new pathologic classification of adenocarcinoma with historical
Ground Glass Opacities A pathologist s perspective Marie-Christine Aubry, M.D. Professor of Pathology Mayo Clinic Objectives Discuss the proposed new pathologic classification of adenocarcinoma with historical
2 nd line Therapy and Beyond NSCLC. Alan Sandler, M.D. Oregon Health & Science University
 2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
The lung adenocarcinoma guidelines: what to be considered by surgeons
 Review Article The lung adenocarcinoma guidelines: what to be considered by surgeons Rodrigo A. S. Sardenberg 1, Evandro Sobroza Mello 1, Riad N. Younes 2 1 Hospital Alemão Oswaldo Cruz, São Paulo, Brazil;
Review Article The lung adenocarcinoma guidelines: what to be considered by surgeons Rodrigo A. S. Sardenberg 1, Evandro Sobroza Mello 1, Riad N. Younes 2 1 Hospital Alemão Oswaldo Cruz, São Paulo, Brazil;
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Impact of immunostaining of pulmonary and mediastinal cytology
 Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
8/22/2016. Major risk factors for the development of lung cancer are: Outline
 Carcinomas of the Lung: Changes in Staging, Adenocarcinoma Classification and Genetics Grace Y. Lin, M.D., Ph.D. Outline Background Staging of Lung Cancer: Review of the 2010 7 th Edition of the AJCC Cancer
Carcinomas of the Lung: Changes in Staging, Adenocarcinoma Classification and Genetics Grace Y. Lin, M.D., Ph.D. Outline Background Staging of Lung Cancer: Review of the 2010 7 th Edition of the AJCC Cancer
Lung cancer is now a major cause of death in developed
 Original Article New IASLC/ATS/ERS Classification and Invasive Tumor Size are Predictive of Disease Recurrence in Stage I Lung Adenocarcinoma Naoki Yanagawa, MD, PhD,* Satoshi Shiono, MD, PhD, Masami Abiko,
Original Article New IASLC/ATS/ERS Classification and Invasive Tumor Size are Predictive of Disease Recurrence in Stage I Lung Adenocarcinoma Naoki Yanagawa, MD, PhD,* Satoshi Shiono, MD, PhD, Masami Abiko,
and management of lung cancer Maureen F. Zakowski, M.D. Memorial Sloan-Kettering Cancer Center
 The new role of cytology in the diagnosis and management of lung cancer Maureen F. Zakowski, M.D. Memorial Sloan-Kettering Cancer Center Outline Role of cytology in the diagnosis of lung cancer Non-small
The new role of cytology in the diagnosis and management of lung cancer Maureen F. Zakowski, M.D. Memorial Sloan-Kettering Cancer Center Outline Role of cytology in the diagnosis of lung cancer Non-small
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer.
 Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Biomarkers of Response to EGFR-TKIs EORTC-NCI-ASCO Meeting on Molecular Markers in Cancer November 17, 2007
 Biomarkers of Response to EGFR-TKIs EORTC-NCI-ASCO Meeting on Molecular Markers in Cancer November 17, 2007 Bruce E. Johnson, MD Dana-Farber Cancer Institute, Brigham and Women s Hospital, and Harvard
Biomarkers of Response to EGFR-TKIs EORTC-NCI-ASCO Meeting on Molecular Markers in Cancer November 17, 2007 Bruce E. Johnson, MD Dana-Farber Cancer Institute, Brigham and Women s Hospital, and Harvard
Histology: Its Influence on Therapeutic Decision Making
 Histology: Its Influence on Therapeutic Decision Making Mark A. Socinski, MD Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology Co-Director, UPMC
Histology: Its Influence on Therapeutic Decision Making Mark A. Socinski, MD Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology Co-Director, UPMC
Slide 1. Slide 2. Slide 3. Individualized Therapy in Lung Cancer : Where are we in 2011? Notable Advances in Cancer Research in the last 2 years
 Slide 1 Individualized Therapy in Lung Cancer : Where are we in 2011? Giorgio V. Scagliotti University of Torino Department of Clinical & Biological Sciences giorgio.scagliotti@unito.it Slide 2 Notable
Slide 1 Individualized Therapy in Lung Cancer : Where are we in 2011? Giorgio V. Scagliotti University of Torino Department of Clinical & Biological Sciences giorgio.scagliotti@unito.it Slide 2 Notable
Minor Components of Micropapillary and Solid Subtypes in Lung Adenocarcinoma are Predictors of Lymph Node Metastasis and Poor Prognosis
 Ann Surg Oncol (2016) 23:2099 2105 DOI 10.1245/s10434-015-5043-9 ORIGINAL ARTICLE THORACIC ONCOLOGY Minor Components of Micropapillary and Solid Subtypes in Lung Adenocarcinoma are Predictors of Lymph
Ann Surg Oncol (2016) 23:2099 2105 DOI 10.1245/s10434-015-5043-9 ORIGINAL ARTICLE THORACIC ONCOLOGY Minor Components of Micropapillary and Solid Subtypes in Lung Adenocarcinoma are Predictors of Lymph
MOLECULAR PREDICTIVE MARKERS OF LUNG CARCINOMA: KFSH&RC EXPERIENCE
 25 th IAP-Arab Division Conference 07-09 November 2013, Amman, Jordan MOLECULAR PREDICTIVE MARKERS OF LUNG CARCINOMA: KFSH&RC EXPERIENCE Fouad Al Dayel, MD, FRCPA, FRCPath Professor and Chairman Department
25 th IAP-Arab Division Conference 07-09 November 2013, Amman, Jordan MOLECULAR PREDICTIVE MARKERS OF LUNG CARCINOMA: KFSH&RC EXPERIENCE Fouad Al Dayel, MD, FRCPA, FRCPath Professor and Chairman Department
Steering Committee. Waiting on photo. Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD.
 Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Steering Committee. Waiting on photo. Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD.
 Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Changing demographics of smoking and its effects during therapy
 Changing demographics of smoking and its effects during therapy Egbert F. Smit MD PhD. Dept. Pulmonary Diseases, Vrije Universiteit Medical Centre, Amsterdam, The Netherlands Smoking prevalence adults
Changing demographics of smoking and its effects during therapy Egbert F. Smit MD PhD. Dept. Pulmonary Diseases, Vrije Universiteit Medical Centre, Amsterdam, The Netherlands Smoking prevalence adults
Pulmonary adenocarcinoma: implications of the recent advances in molecular biology, treatment and the IASLC/ATS/ERS classification
 Review Article Pulmonary adenocarcinoma: implications of the recent advances in molecular biology, treatment and the IASLC/ATS/ERS classification Swaroop Revannasiddaiah 1, Priyanka Thakur 2, Bhaskar Bhardwaj
Review Article Pulmonary adenocarcinoma: implications of the recent advances in molecular biology, treatment and the IASLC/ATS/ERS classification Swaroop Revannasiddaiah 1, Priyanka Thakur 2, Bhaskar Bhardwaj
The Evolving Role of Molecular Markers in Managing Non-Small Cell Lung Cancer
 The Evolving Role of Molecular Markers in Managing Non-Small Cell Lung Cancer Nathan A. Pennell, M.D., Ph.D. Assistant Professor Solid Tumor Oncology Cleveland Clinic Taussig Cancer Institute www.cancergrace.org
The Evolving Role of Molecular Markers in Managing Non-Small Cell Lung Cancer Nathan A. Pennell, M.D., Ph.D. Assistant Professor Solid Tumor Oncology Cleveland Clinic Taussig Cancer Institute www.cancergrace.org
Joachim Aerts Erasmus MC Rotterdam, Netherlands. Drawing the map: molecular characterization of NSCLC
 Joachim Aerts Erasmus MC Rotterdam, Netherlands Drawing the map: molecular characterization of NSCLC Disclosures Honoraria for advisory board/consultancy/speakers fee Eli Lilly Roche Boehringer Ingelheim
Joachim Aerts Erasmus MC Rotterdam, Netherlands Drawing the map: molecular characterization of NSCLC Disclosures Honoraria for advisory board/consultancy/speakers fee Eli Lilly Roche Boehringer Ingelheim
Lung cancer is the leading cause of cancer-related
 Original Articles Correlation of Mutation Status With Predominant Histologic Subtype of Adenocarcinoma According to the New Lung Adenocarcinoma Classification of the International Association for the Study
Original Articles Correlation of Mutation Status With Predominant Histologic Subtype of Adenocarcinoma According to the New Lung Adenocarcinoma Classification of the International Association for the Study
EGFR. Pathway and biomarkers. Alex Soltermann
 EGFR Pathway and biomarkers Alex Soltermann EGFR = HER1 signaling pathway EGFR Cheng Mod Pathol 2012 Chromosome 7p11.2, spans 200kb, 28 exons, 464 aa, 170 kda protein 2 Signal transduction pathways controlled
EGFR Pathway and biomarkers Alex Soltermann EGFR = HER1 signaling pathway EGFR Cheng Mod Pathol 2012 Chromosome 7p11.2, spans 200kb, 28 exons, 464 aa, 170 kda protein 2 Signal transduction pathways controlled
Update on 2015 WHO Classification of Lung Adenocarcinoma 1/3/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
7/6/2015. Cancer Related Deaths: United States. Management of NSCLC TODAY. Emerging mutations as predictive biomarkers in lung cancer: Overview
 Emerging mutations as predictive biomarkers in lung cancer: Overview Kirtee Raparia, MD Assistant Professor of Pathology Cancer Related Deaths: United States Men Lung and bronchus 28% Prostate 10% Colon
Emerging mutations as predictive biomarkers in lung cancer: Overview Kirtee Raparia, MD Assistant Professor of Pathology Cancer Related Deaths: United States Men Lung and bronchus 28% Prostate 10% Colon
Individualized therapy in lung cancer Where are we in 2012?
 UNIVERSITY OF OF TORINO DEPARTMENT OF ONCOLOGY Individualized therapy in lung cancer Where are we in 2012? Giorgio V. Scagliotti University of Torino Professor of Medical Oncology Department of Oncology
UNIVERSITY OF OF TORINO DEPARTMENT OF ONCOLOGY Individualized therapy in lung cancer Where are we in 2012? Giorgio V. Scagliotti University of Torino Professor of Medical Oncology Department of Oncology
Extensive immunohistochemistry was performed on this case, in the referring community /district hospital. This showed the following results:
 Case 1 The New Classification Helped Keith Kerr Clinical history This 75 year old female patient presented with an increasing cough and some vague symptoms of pain over the left lower chest wall. She is
Case 1 The New Classification Helped Keith Kerr Clinical history This 75 year old female patient presented with an increasing cough and some vague symptoms of pain over the left lower chest wall. She is
IASLC 2011/WHO 2015 CLASSIFICATION OF LUNG ADENOCARCINOMAS
 Serban Negoita Dylan Holt Marsha Dunn IASLC 2011/WHO 2015 CLASSIFICATION OF LUNG ADENOCARCINOMAS DEMOGRAPHIC PATTERNS, TRENDS, AND IMPLICATIONS FOR CANCER SURVEILLANCE Outline Relevance of lung adenocarcinoma
Serban Negoita Dylan Holt Marsha Dunn IASLC 2011/WHO 2015 CLASSIFICATION OF LUNG ADENOCARCINOMAS DEMOGRAPHIC PATTERNS, TRENDS, AND IMPLICATIONS FOR CANCER SURVEILLANCE Outline Relevance of lung adenocarcinoma
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Treatment of EGFR mutant advanced NSCLC
 Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and Manchester University Hospital Manchester, UK Outline Data on first-line Overcoming T790M mutation
Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and Manchester University Hospital Manchester, UK Outline Data on first-line Overcoming T790M mutation
Histopathology of NSCLC, IHC markers and ptnm classification
 ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
Difficult Diagnoses and Controversial Entities in Neoplastic Lung
 Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Management Strategies for Lung Cancer Sensitive or Resistant to EGRF Inhibitors
 Management Strategies for Lung Cancer Sensitive or Resistant to EGRF Inhibitors Conor E. Steuer, MD Assistant Professor The Winship Cancer Institute of Emory University July 27, 2017 1 Lung Cancer One
Management Strategies for Lung Cancer Sensitive or Resistant to EGRF Inhibitors Conor E. Steuer, MD Assistant Professor The Winship Cancer Institute of Emory University July 27, 2017 1 Lung Cancer One
Management of advanced non small cell lung cancer
 Management of advanced non small cell lung cancer Jean-Paul Sculier Intensive Care & Thoracic Oncology Institut Jules Bordet Université Libre de Bruxelles (ULB) www.pneumocancero.com Declaration No conflict
Management of advanced non small cell lung cancer Jean-Paul Sculier Intensive Care & Thoracic Oncology Institut Jules Bordet Université Libre de Bruxelles (ULB) www.pneumocancero.com Declaration No conflict
Selection of systemic therapy in Advanced NSCLC based on biological factors. State of the Art
 Selection of systemic therapy in Advanced NSCLC based on biological factors State of the Art Giorgio V. Scagliotti University of Torino Department of Clinical & Biological Sciences giorgio.scagliotti@unito.it
Selection of systemic therapy in Advanced NSCLC based on biological factors State of the Art Giorgio V. Scagliotti University of Torino Department of Clinical & Biological Sciences giorgio.scagliotti@unito.it
Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis
 19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
Evolution of Pathology
 1 Traditional pathology Molecular pathology 2 Evolution of Pathology Gross Pathology Cellular Pathology Morphologic Pathology Molecular/Predictive Pathology Antonio Benivieni (1443-1502): First autopsy
1 Traditional pathology Molecular pathology 2 Evolution of Pathology Gross Pathology Cellular Pathology Morphologic Pathology Molecular/Predictive Pathology Antonio Benivieni (1443-1502): First autopsy
Exploring Personalized Therapy for First Line Treatment of Advanced Non-Small Cell Lung Cancer (NSCLC)
") Exploring Personalized Therapy for First Line Treatment of Advanced Non-Small Cell Lung Cancer (NSCLC) Suresh S. Ramalingam, MD Director of Thoracic Oncology Associate Professor Emory University Atlanta,
Exploring Personalized Therapy for First Line Treatment of Advanced Non-Small Cell Lung Cancer (NSCLC) Suresh S. Ramalingam, MD Director of Thoracic Oncology Associate Professor Emory University Atlanta,
Molecular Diagnosis of Lung Cancer
 Molecular Diagnosis of Lung Cancer Lucian R. Chirieac, M.D. Assistant Professor of Pathology Harvard Medical School Staff Pathologist, Department of Pathology Brigham and Women's Hospital 75 Francis Street
Molecular Diagnosis of Lung Cancer Lucian R. Chirieac, M.D. Assistant Professor of Pathology Harvard Medical School Staff Pathologist, Department of Pathology Brigham and Women's Hospital 75 Francis Street
Frequency of Epidermal Growth Factor Mutation Status and Its Effect on Outcome of Patients with Adenocarcinoma of the Lung
 Journal of Cancer Therapy, 2014, 5, 1012-1020 Published Online September 2014 in SciRes. http://www.scirp.org/journal/jct http://dx.doi.org/10.4236/jct.2014.511106 Frequency of Epidermal Growth Factor
Journal of Cancer Therapy, 2014, 5, 1012-1020 Published Online September 2014 in SciRes. http://www.scirp.org/journal/jct http://dx.doi.org/10.4236/jct.2014.511106 Frequency of Epidermal Growth Factor
Prudence Anne Russell 1,2, Gavin Michael Wright 3,4
 Editorial Page 1 of 7 Predominant histologic subtype in lung adenocarcinoma predicts benefit from adjuvant chemotherapy in completely resected patients: discovery of a holy grail? Prudence Anne Russell
Editorial Page 1 of 7 Predominant histologic subtype in lung adenocarcinoma predicts benefit from adjuvant chemotherapy in completely resected patients: discovery of a holy grail? Prudence Anne Russell
Frequencies of actionable mutations and survival in variants of invasive adenocarcinoma of lung
 Original Article Frequencies of actionable mutations and survival in variants of invasive adenocarcinoma of lung Zhengbo Song 1,2 *, Tangfeng Lv 1 *, Yiping Zhang 2, Yong Song 1 1 Department of Respiratory
Original Article Frequencies of actionable mutations and survival in variants of invasive adenocarcinoma of lung Zhengbo Song 1,2 *, Tangfeng Lv 1 *, Yiping Zhang 2, Yong Song 1 1 Department of Respiratory
3/23/2017. Disclosure of Relevant Financial Relationships. Pathologic Staging Updates in Lung Cancer T STAGE OUTLINE SURVIVAL ACCORDING TO SIZE ONLY
 Pathologic Staging Updates in Lung Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Pathologic Staging Updates in Lung Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Mutation and prognostic analyses of PIK3CA in patients with completely resected lung adenocarcinoma
 Cancer Medicine ORIGINAL RESEARCH Open Access Mutation and prognostic analyses of PIK3CA in patients with completely resected lung adenocarcinoma Zhengbo Song 1,2, Xinmin Yu 1 & Yiping Zhang 1,2 1 Department
Cancer Medicine ORIGINAL RESEARCH Open Access Mutation and prognostic analyses of PIK3CA in patients with completely resected lung adenocarcinoma Zhengbo Song 1,2, Xinmin Yu 1 & Yiping Zhang 1,2 1 Department
The ABCs of BAC: Bronchioloalveolar Carcinoma
 The ABCs of BAC: Bronchioloalveolar Carcinoma Howard (Jack) West, MD Medical Oncologist Medical Director, Thoracic Oncology Program Swedish Cancer Institute Seattle, WA March, 2009 President & CEO GRACE
The ABCs of BAC: Bronchioloalveolar Carcinoma Howard (Jack) West, MD Medical Oncologist Medical Director, Thoracic Oncology Program Swedish Cancer Institute Seattle, WA March, 2009 President & CEO GRACE
Lung Cancer Case. Since the patient was symptomatic, a targeted panel was sent. ALK FISH returned in 2 days and was positive.
 Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Histology in the Decision-making Process
 Histology in the Decision-making Process Giorgio V. Scagliotti University of Torino Department of Clinical & Biological Sciences giorgio.scagliotti@unito.it Lung Cancer Four Main Histological Subtypes
Histology in the Decision-making Process Giorgio V. Scagliotti University of Torino Department of Clinical & Biological Sciences giorgio.scagliotti@unito.it Lung Cancer Four Main Histological Subtypes
Lung Cancer Epidemiology. AJCC Staging 6 th edition
 Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP
 What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma
 Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Systemic therapy for Non-Small Cell Lung Cancer in 2013 (What you should know)
") Systemic therapy for Non-Small Cell Lung Cancer in 2013 (What you should know) นายแพทย ช ยย ทธ ย ทธ เจร ญธรรม หน วยมะเร งว ทยา ภาคว ชาอาย ร อาย รศาสตร Inter-hospitol Conference, 16 th March 2013 Systemic
Systemic therapy for Non-Small Cell Lung Cancer in 2013 (What you should know) นายแพทย ช ยย ทธ ย ทธ เจร ญธรรม หน วยมะเร งว ทยา ภาคว ชาอาย ร อาย รศาสตร Inter-hospitol Conference, 16 th March 2013 Systemic
Lihong Ma 1 *, Zhengbo Song 2 *, Yong Song 1, Yiping Zhang 2. Original Article
 Original Article MET overexpression coexisting with epidermal growth factor receptor mutation influence clinical efficacy of EGFR-tyrosine kinase inhibitors in lung adenocarcinoma patients Lihong Ma 1
Original Article MET overexpression coexisting with epidermal growth factor receptor mutation influence clinical efficacy of EGFR-tyrosine kinase inhibitors in lung adenocarcinoma patients Lihong Ma 1
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS
 LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC. Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy
 PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy Prognostic versus predictive Prognostic: In presence of the biomarker patient outcome
PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy Prognostic versus predictive Prognostic: In presence of the biomarker patient outcome
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? VEGF Is the Only Angiogenic Factor Present Throughout the Tumor Life Cycle
 Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Corporate Medical Policy
 Corporate Medical Policy Molecular Analysis for Targeted Therapy for Non-Small Cell Lung File Name: Origination: Last CAP Review: Next CAP Review: Last Review: molecular_analysis_for_targeted_therapy_for_non_small_cell_lung_cancer
Corporate Medical Policy Molecular Analysis for Targeted Therapy for Non-Small Cell Lung File Name: Origination: Last CAP Review: Next CAP Review: Last Review: molecular_analysis_for_targeted_therapy_for_non_small_cell_lung_cancer
Personalized Medicine for Advanced NSCLC in East Asia
 Personalized Medicine for Advanced NSCLC in East Asia - Update treatment strategy for NSCLC based on Japanese clinical practice guideline - Masahiro Tsuboi, M.D., Ph.D. Associate-professor, School of Medicine,
Personalized Medicine for Advanced NSCLC in East Asia - Update treatment strategy for NSCLC based on Japanese clinical practice guideline - Masahiro Tsuboi, M.D., Ph.D. Associate-professor, School of Medicine,
Treatment of EGFR mutant advanced NSCLC
 Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Data on first-line Overcoming T790M
Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Data on first-line Overcoming T790M
Surgical pathology of early stage non-small cell lung carcinoma
 Review Article Page 1 of 8 Surgical pathology of early stage non-small cell lung carcinoma Mary Beth Beasley 1, Francine R. Dembitzer 1, Raja M. Flores 2 1 Department of Pathology, 2 Department of Thoracic
Review Article Page 1 of 8 Surgical pathology of early stage non-small cell lung carcinoma Mary Beth Beasley 1, Francine R. Dembitzer 1, Raja M. Flores 2 1 Department of Pathology, 2 Department of Thoracic
NSCLC: Terapia medica nella fase avanzata. Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza
 NSCLC: Terapia medica nella fase avanzata Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza First-line Second-line Third-line Not approved CT AND SILENT APPROVAL Docetaxel 1999 Paclitaxel Gemcitabine
NSCLC: Terapia medica nella fase avanzata Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza First-line Second-line Third-line Not approved CT AND SILENT APPROVAL Docetaxel 1999 Paclitaxel Gemcitabine
Medical Treatment of Advanced Lung Cancer
 Medical Treatment of Advanced Lung Cancer Oncology for Scientists April 26, 2018 Edwin Yau, MD., Ph.D. Assistant Professor of Oncology Department of Medicine Department of Cancer Genetics and Genomics
Medical Treatment of Advanced Lung Cancer Oncology for Scientists April 26, 2018 Edwin Yau, MD., Ph.D. Assistant Professor of Oncology Department of Medicine Department of Cancer Genetics and Genomics
Osamu Tetsu, MD, PhD Associate Professor Department of Otolaryngology-Head and Neck Surgery School of Medicine, University of California, San
 Osamu Tetsu, MD, PhD Associate Professor Department of Otolaryngology-Head and Neck Surgery School of Medicine, University of California, San Francisco Lung Cancer Classification Pathological Classification
Osamu Tetsu, MD, PhD Associate Professor Department of Otolaryngology-Head and Neck Surgery School of Medicine, University of California, San Francisco Lung Cancer Classification Pathological Classification
Molecular Diagnostics in Lung Cancer
 Molecular Diagnostics in Lung Cancer Mutations in lung carcinomas and their impact on diagnosis and treatment With special thanks to: Barbara Chaitin, MD Medical Director, Esoteric Services AmeriPath Orlando,
Molecular Diagnostics in Lung Cancer Mutations in lung carcinomas and their impact on diagnosis and treatment With special thanks to: Barbara Chaitin, MD Medical Director, Esoteric Services AmeriPath Orlando,
Utility of small biopsies for diagnosis of lung nodules: doing more with less
 & 2012 USCAP, Inc. All rights reserved 0893-3952/12 $32.00 S43 Utility of small biopsies for diagnosis of lung nodules: doing more with less Sanjay Mukhopadhyay Department of Pathology, State University
& 2012 USCAP, Inc. All rights reserved 0893-3952/12 $32.00 S43 Utility of small biopsies for diagnosis of lung nodules: doing more with less Sanjay Mukhopadhyay Department of Pathology, State University
State of the Art Treatment of Lung Cancer Ravi Salgia, MD, PhD
 State of the Art Treatment of Lung Cancer Ravi Salgia, MD, PhD Professor and Chair Arthur & Rosalie Kaplan Chair Medical Oncology and Therapeutics Research Nothing to disclose DISCLOSURE Objectives Lung
State of the Art Treatment of Lung Cancer Ravi Salgia, MD, PhD Professor and Chair Arthur & Rosalie Kaplan Chair Medical Oncology and Therapeutics Research Nothing to disclose DISCLOSURE Objectives Lung
Optimum Sequencing of EGFR targeted therapy in NSCLC. Dr. Sema SEZGİN GÖKSU Akdeniz Univercity, Antalya, Turkey
 Optimum Sequencing of EGFR targeted therapy in NSCLC Dr. Sema SEZGİN GÖKSU Akdeniz Univercity, Antalya, Turkey Lung cancer NSCLC SCLC adeno squamous EGFR ALK ROS1 BRAF HER2 KRAS EGFR Transl Lung Cancer
Optimum Sequencing of EGFR targeted therapy in NSCLC Dr. Sema SEZGİN GÖKSU Akdeniz Univercity, Antalya, Turkey Lung cancer NSCLC SCLC adeno squamous EGFR ALK ROS1 BRAF HER2 KRAS EGFR Transl Lung Cancer
Slide 1. Slide 2. Slide 3. Disclosures. Personalized Medicine for Advanced NSCLC in East Asia. No conflicts related to this presentation
 Slide 1 12 th International Lung Cancer Conference Personalized Medicine for Advanced NSCLC in East Asia Masahiro Tsuboi, M.D., Ph.D. Group Chair, Lung Cancer Surgical Study Group in Japan Clinical Oncology
Slide 1 12 th International Lung Cancer Conference Personalized Medicine for Advanced NSCLC in East Asia Masahiro Tsuboi, M.D., Ph.D. Group Chair, Lung Cancer Surgical Study Group in Japan Clinical Oncology
Next Generation Sequencing in Clinical Practice: Impact on Therapeutic Decision Making
 Next Generation Sequencing in Clinical Practice: Impact on Therapeutic Decision Making November 20, 2014 Capturing Value in Next Generation Sequencing Symposium Douglas Johnson MD, MSCI Vanderbilt-Ingram
Next Generation Sequencing in Clinical Practice: Impact on Therapeutic Decision Making November 20, 2014 Capturing Value in Next Generation Sequencing Symposium Douglas Johnson MD, MSCI Vanderbilt-Ingram
Do You Think Like the Experts? Refining the Management of Advanced NSCLC With ALK Rearrangement. Reference Slides Introduction
 Do You Think Like the Experts? Refining the Management of Advanced NSCLC With ALK Rearrangement Reference Slides Introduction EML4-ALK Fusion Oncogene Key Driver in 3% to 7% NSCLC Inversion or Translocation
Do You Think Like the Experts? Refining the Management of Advanced NSCLC With ALK Rearrangement Reference Slides Introduction EML4-ALK Fusion Oncogene Key Driver in 3% to 7% NSCLC Inversion or Translocation
Personalized Medicine in Oncology and the Implication for Clinical Development
 THE POWER OFx Experts. Experienc e. Execution. Personalized Medicine in Oncology and the Implication for Clinical Development Jamal Gasmi MD, PhD, Medical Director, Medpace Introduction The notable success
THE POWER OFx Experts. Experienc e. Execution. Personalized Medicine in Oncology and the Implication for Clinical Development Jamal Gasmi MD, PhD, Medical Director, Medpace Introduction The notable success
Targeted Therapies for Advanced NSCLC
 Targeted Therapies for Advanced NSCLC Current Clinical Developments Friday, June 3, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016 ASCO Annual Meeting
Targeted Therapies for Advanced NSCLC Current Clinical Developments Friday, June 3, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016 ASCO Annual Meeting
Introduction: Overview of Current Status of Lung Cancer Predictive Biomarkers
 Introduction: Overview of Current Status of Lung Cancer Predictive Biomarkers Program 7:15 7:40 Translocations as predictive biomarkers in lung cancer: Overview Mari Mino Kenudson, MD 7:40 8:05 Translocation
Introduction: Overview of Current Status of Lung Cancer Predictive Biomarkers Program 7:15 7:40 Translocations as predictive biomarkers in lung cancer: Overview Mari Mino Kenudson, MD 7:40 8:05 Translocation
K-Ras signalling in NSCLC
 Targeting the Ras-Raf-Mek-Erk pathway Egbert F. Smit MD PhD Dept. Pulmonary Diseases Vrije Universiteit VU Medical Centre Amsterdam, The Netherlands K-Ras signalling in NSCLC Sun et al. Nature Rev. Cancer
Targeting the Ras-Raf-Mek-Erk pathway Egbert F. Smit MD PhD Dept. Pulmonary Diseases Vrije Universiteit VU Medical Centre Amsterdam, The Netherlands K-Ras signalling in NSCLC Sun et al. Nature Rev. Cancer
Research Article Prognostic Implication of Predominant Histologic Subtypes of Lymph Node Metastases in Surgically Resected Lung Adenocarcinoma
 BioMed Research International, Article ID 64568, 6 pages http://dx.doi.org/.55/24/64568 Research Article Prognostic Implication of Predominant Histologic Subtypes of Lymph Node Metastases in Surgically
BioMed Research International, Article ID 64568, 6 pages http://dx.doi.org/.55/24/64568 Research Article Prognostic Implication of Predominant Histologic Subtypes of Lymph Node Metastases in Surgically
Page: 1 of 27. Molecular Analysis for Targeted Therapy of Non-Small-Cell Lung Cancer
 Last Review Status/Date: December 2014 Page: 1 of 27 Non-Small-Cell Lung Cancer Description Over half of patients with non-small-cell lung cancer (NSCLC) present with advanced and therefore incurable disease,
Last Review Status/Date: December 2014 Page: 1 of 27 Non-Small-Cell Lung Cancer Description Over half of patients with non-small-cell lung cancer (NSCLC) present with advanced and therefore incurable disease,
Role of molecular studies in the diagnosis of lung adenocarcinoma
 & 2012 USCAP, Inc. All rights reserved 0893-3952/12 $32.00 S11 Role of molecular studies in the diagnosis of lung adenocarcinoma Samuel A Yousem Department of Pathology, University of Pittsburgh Medical
& 2012 USCAP, Inc. All rights reserved 0893-3952/12 $32.00 S11 Role of molecular studies in the diagnosis of lung adenocarcinoma Samuel A Yousem Department of Pathology, University of Pittsburgh Medical
EGFR Tyrosine Kinase Inhibitors Prolong Overall Survival in EGFR Mutated Non-Small-Cell Lung Cancer Patients with Postsurgical Recurrence
 102 Journal of Cancer Research Updates, 2012, 1, 102-107 EGFR Tyrosine Kinase Inhibitors Prolong Overall Survival in EGFR Mutated Non-Small-Cell Lung Cancer Patients with Postsurgical Recurrence Kenichi
102 Journal of Cancer Research Updates, 2012, 1, 102-107 EGFR Tyrosine Kinase Inhibitors Prolong Overall Survival in EGFR Mutated Non-Small-Cell Lung Cancer Patients with Postsurgical Recurrence Kenichi
Supplementary Online Content
 Supplementary Online Content Kris MG, Johnson BE, Berry LD, et al. Using Multiplexed Assays of Oncogenic Drivers in Lung Cancers to Select Targeted Drugs. JAMA. doi:10.1001/jama.2014.3741 etable 1. Trials
Supplementary Online Content Kris MG, Johnson BE, Berry LD, et al. Using Multiplexed Assays of Oncogenic Drivers in Lung Cancers to Select Targeted Drugs. JAMA. doi:10.1001/jama.2014.3741 etable 1. Trials
Additional clinical features of this patient include:
 *Not an actual patient. Challenge your knowledge of biomarker testing in advanced NSCLC. Consider this case study of disease progression following chemotherapy, with insightful commentary from Dr Edward
*Not an actual patient. Challenge your knowledge of biomarker testing in advanced NSCLC. Consider this case study of disease progression following chemotherapy, with insightful commentary from Dr Edward
Targeted Therapy for NSCLC: EGFR and ALK Fadlo R. Khuri, MD
 EGFR and ALK Fadlo R. Khuri, MD President, American University of Beirut Professor of Medicine July 26, 2018 A great year end! Targeted Therapy for NSCLC: Evolving Landscape of Lung Adenocarcinoma NSCLC
EGFR and ALK Fadlo R. Khuri, MD President, American University of Beirut Professor of Medicine July 26, 2018 A great year end! Targeted Therapy for NSCLC: Evolving Landscape of Lung Adenocarcinoma NSCLC