Luminal A and B Where are we? (or lost in translation?)
|
|
|
- Kelly Doyle
- 6 years ago
- Views:
Transcription
1 Luminal A and B Where are we? (or lost in translation?) Emiel J. Rutgers The Netherlands Cancer Institute Antoni Van Leeuwenhoek Hospital Amsterdam
 The Netherlands Cancer Institute Antoni Van Leeuwenhoek Hospital")
2 How to determine adjuvant or neoadjuvant treatment for Luminal A or Luminal B cancers? (as a surgeon) The Netherlands Cancer Institute Antoni Van Leeuwenhoek Hospital Amsterdam
3 Disclosures No financial interest in a pharmaceutical or diagnostic company Not a member of speakers bureau or advisory board I m a surgical oncologist/breast cancer specialist with specific interest in translational research


4 And some about us The Netherlands Cancer Institute
5 The clinical issue The prognosis of the patient. What is Luminal A? What is Luminal B? Or how to distinguish Luminal A vs B How to treat pts with Luminal A vs Luminal B cancers? Should treatment for Luminal A cancers be different from Luminal B cancers Or. Is it simpler? - ER strong +ve & low risk: HT? - ER +ve plus risk factor: HT + chemotherapy?
6 Where it all started.
7 Molecular ( intrinsic ) subtypes Specimens from 65 tumors from 42 patients Perou et al., Nature (2000) 406:747

8 Molecular ( intrinsic ) subtypes Sørlie et al., PNAS (2003) 100:8418

9 Immunohistochemistry ( surrogate subtypes ) IHC ER PR HER2 lum A Surrogate subtype lum B HER2 Basal

10 Molecular Subtypes provide insight on which therapies to select (St. Gallen, May 2011)


11 Classification of breast cancer Potentials, limitations, challenges
12 The clinical issue. Think step by step Step 1: The very low risk cancer: is chemotherapy indicated anyway? Step 2: Is ER+ve really ER +ve? (or: do you trust your specimen work up system?) Step 3: If ER +ve is reliably proven, and there is some risk of relapse: adjuvant anti estrogen treatment Step 4: What are the factors that justify adjuvant chemotherapy (luminal A > B)
13 The clinical issue. Think step by step Step 1: Is prognosis so good that survival advantage of adjuvant chemotherapy outweighs the disadvantages & serious late side effects?
14 Clinical determinate cases High Risk Low Risk ER negative Lymph Node positive HER2 positive Grade III Larger tumor size ER positive Lymph Node negative HER2 negative Grade I Small tumor size Half of our patients are somewhere in between! What to do?
15 Interobserver agreement morphology and IHC Kappa statistics local vs. central assessment Tumor type 0.56 Grade 0.50 ER 0.85 PR 0.72 HER Degree of agreement: slight fair moderate substantial (almost) perfect Bueno-de Mesquita et al.; Annals Oncol. (2010) 21: 40-44
16 Is determinate always determinate? Some examples Small cancers good prognosis? Grade 1 good prognosis? There is an important and reproducible discordance between clinical-pathological risk estimates compared to newer techniques by tumor profiling
17 MammaPrint and Tumorsize T1c BCSS mm Tumors 99% 92% Good signature (n=441) 88% 72% Poor signature (n=384) Log rank p<0.001 HR at 10 yrs: 4.42 (95% CI ); p<0.001 Log rank p = 0,036 T1c tumors derived from pooled database of all MammaPrint validation studies (all, n=1696) Mook et al, Ann Surg Oncol, 2010
18 HR 3.9 ( ) p=0.05
 were classified as good prognosis and 866 (53%)")

19 MammaPrint adds to grading of breast cancer 764 of 1630 patients (47%) were classified as good prognosis and 866 (53%) as poor prognosis by MammaPrint Histological grading was centrally reviewed for all patients MammaPrint high risk MammaPrint low risk
20 DDFS N -ve Survival Functions MammaPrint censored 1-censored

21 DDFS N-ve Survival Functions MammaPrint censored 1-censored
 HIGH N(%) Total 70-gene risk LOW 2586 (40) 1436 (22) 4022 (62) HIGH 678 (10) 1827 (28) 2505 (38)")

22 Patient risk allocation Clin-path risk and 70- gene risk at enrollment Clinical-pathological risk LOW N(%) HIGH N(%) Total 70-gene risk LOW 2586 (40) 1436 (22) 4022 (62) HIGH 678 (10) 1827 (28) 2505 (38) Total 3264 (50)* 3263 (50)* N=6527 Discordant cases ( = 32%) match protocol hypothesis The absolute difference between C-HIGH / G-LOW and C-LOW / G-HIGH is 11.6% *The split is coincidental
 (142 pat) Int Risk (RS 18-30) (154 pat) 37.8% (48.9%, 26.8%) (85 pat) 20.5% (30.4%, 10.5%) (69 pat) High Risk (RS 31) (178 pat) 31.3% (40.9%, 21.8%) (99 pat) 29.7% (40.2%, 19.")
23 Oncotype DX and low risk B-14 Data NSABP Untreated Population Treated Population Breast Cancer Mortality (95%CI, 355 pat) (85%CI) (290) Low Risk (RS<18) (313 pat) 14.1% (19.5%, 8.64%) (171 pat) 6.9% (11.2%, 2.5%) (142 pat) Int Risk (RS 18-30) (154 pat) 37.8% (48.9%, 26.8%) (85 pat) 20.5% (30.4%, 10.5%) (69 pat) High Risk (RS 31) (178 pat) 31.3% (40.9%, 21.8%) (99 pat) 29.7% (40.2%, 19.3%) (79 pat)

24 70-Gene signature (MammaPrint) prospectively predicts prognosis of patients with nodenegative breast cancer: 5 year follow-up of the RASTER study S.C. Linn, C.A. Drukker, V.P. Retèl, J.M. Bueno-de-Mesquita, W.H. van Harten, H. van Tinteren, J. Wesseling, L.J. van t Veer, E.J.T. Rutgers, M.J. van de Vijver
25 5-year distant recurrence-free interval MammaPrint AOL 15% CT 18% CT 81% CT 75% CT low risk: 97 % high risk: 91.7 % p=0.03 low risk: 96.7 % high risk: 93.4 % p=ns

26 Linn, Rutgers, Drukker, et al., EBCC 2012 MammaPrint in observational prospective trial RASTER study, 5-year DDFS of 427 patients according to 70GPS or AOL 5YR DDFS 5YR DDFS 89.8% 92.4% 96.1% 70 pts no AST: DDFS 100% 94.4% 70-gene signature Adjuvant Online
27 Discordant cases who received no AST n=70 n=88 60 mos mlow-clow 95.0% (95%CI ) 60 mos mlow-chigh 100% (95%CI )
28 Discordant cases who received no AST or endocrine therapy only n=94 n=92 60 mos mlow-clow 94.1% (95%CI ) 60 mos mlow-chigh 97.8% (95%CI )
29 Role of Ki-67 RFS luminal A vs. B based on Ki-67 Cheang et al., JNCI (2009) 101:
30
31 Mitch Dowsett (Mr. Ki-67): Ki-67 may identify luminal class with a cut-off level of 13.25% proposed to distinguish poorer prognosis luminal B cancers from luminal A Lack of between laboratory standards limiting application as a surrogate marker Standardized methodologies for Ki-67 are lacking ASCO Tumor Marker Guidelines Committee: clinical utility of Ki-67 insufficient to recommend routine use for prognostic purposes In 2011, the International Ki-67 in Breast Cancer Working Group published recommendations for Ki-67 assessment in breast cancer Sheri & Dowsett, Ann. Oncol. (2012) 23:
32
33 The clinical issue. Think step by step Step 1: Is prognosis so good that survival advantage of adjuvant chemotherapy outweighs the disadvantages & serious late side effects? Can we select those patients? My conclusion: on the basis of standard clinical-pathological data only a few. Ki-67 is of limited help, only in the extremes You need to add extra information on the molecular tumor biology of the primary to be able to select a larger proportion (40% vs 10% of early node negative ER +ve breast cancers)
34 The clinical issue. Think step by step Step 2: Is ER +ve really ER +ve? Or: - How reliable is your ER IHC scoring? - Where is the cut-off?

35 Stages of IHC testing Preanalytic Analytic Postanalytic Transport Secretary support Tissue, type, and dimension Decalcification Preparation Fixation Time, Type, Volume Section Thickness Storage & Drying Antigen retrieval Primary antibody Clone Dilution Buffer Time Temperature Manual vs. Automated Development Visualization Sensitivity Specificity Interpretation Localization Cut-off Quantification Reporting Secretary support! Control Internal External Quality assessment
36 The perfect test is non-existent No 100% sensitivity No 100% specificity
37 ER-status based on IHC, mrna, and signature (n=456 FNAs) mrna signature Iwamoto et al., J. Clin. Oncol. (2012) 30:
38 IHC and mrna ER-status and OS IHC mrna Iwamoto et al., J. Clin. Oncol. (2012) 30:
39 Viale et al., J. Clin. Oncol. (2007) 25: DFS and ER-status in BIG 1-98 trial P < 0.001

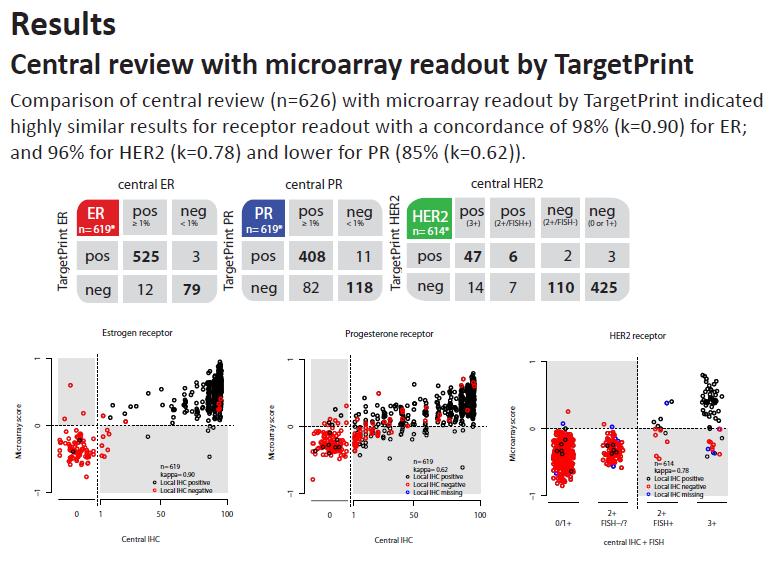
40 TargetPrint as second opinion B. Viale et al. (2011) ASCO
41
 ASCO")
42 J. Wesseling et al. (2011) ASCO

43 Reliable second opinion
44 The clinical issue. Think step by step Step 2: Is ER +ve really ER +ve? My conclusion (for debate): Have your ER testing done by standard operational procedures, including quality control programs in sufficient case load labs. IHC is good Threshold: like ASCO-CAP guidelines: >1% consider anti ER therapy
45 The clinical issue. Think step by step (the most easy one) Step 3: If ER +ve is reliably proven, and there is some risk of relapse Adjuvant anti-estrogen treatments: effect is proven - At least 5 years - Premenopausal: tamoxifen +/- ovarion ablation - Postmenopausal at least 2-3 years AI (+ tamoxifen) or AI only - In higher risk: extended to 7 (10?) years
46
47
48
49 Step 3: If ER +ve is reliably proven, and there is some risk of relapse My conclusions: Adjuvant anti-estrogen treatments: effect is proven - At least 5 years - Premenopausal: tamoxifen +/- ovarion ablation(role await SOFT trial results) - Postmenopausal at least 2-3 years AI (+ tamoxifen) or AI only - In higher risk: extended to 7 (10?) years: see upcoming ATLAS trial results!
50 The clinical issue. Think step by step (the most difficult one) Step 4: What are the factors that justify adjuvant chemotherapy (luminal A > B) Is every luminal A a luminal A? What makes luminal B a luminal B? What is the effect of chemotherapy: different for luminal A or B?

51 What are Intrinsic Molecular Subtypes? Molecular subtypes show which pathway drives cancer growth. Luminal it is the estrogen pathway ERB2 it is the HER2 pathway Basal it is neither one of them There is approx 20% discordance between molecular subtypes and subtyping with IHC (Perou 2011) Red = Up-regulation Green = Down-regulation
52 Is molecular subtyping useful in fine tuning your treatment decisions? First some supportive data

53 Response to neo-adjuvant chemotherapy in molecular subgroups 53
54 PcR and 5yr follow-up of neoadjuvant patients confirms the very response to chemotherapy of Luminal Low Risk patients. PcR rates confirm that there is a benefit of chemotherapy in Luminal High Risk patients. PcR rates in Basal & HER2 are high stressing the importance of identifying the subtype in these two groups. 3% 11 % 56 % 50 %

55 Molecular Subtyping Signature 80-gene signature Profiles Basal, Luminal and HER2 subtypes

56 ASCO
57 Key Findings: 5 year survival data suggests that a combination of MammaPrint and BluePrint more accurately identifies Luminal, Basal and ERB2 subtypes compared to IHC % % 73 % 94% 77% 78% 77% 69%

58 Key Findings: 42% of patients that were classified as HER 2+ by IHC/ Fish were reclassified as Luminal s with Blue Print Luminal A s have a 5yr DMFS of 94%. If significant comorbidites exist is it worth considering withholding Herceptin from Luminal A patients?
59 Is molecular subtyping useful in fine tuning your treatment decisions? Than some sobering data.

60 Concordance single sample predictors (SSP) Weigelt et al., Lancet Oncology (2010) 11: 229
61 Concordance SSP algorithms Weigelt et al., Lancet Oncology (2010) 11: 229
 Lips et al.")
62 Concordance molecular vs. IHC subtyping (n=560) Lips et al., submitted

63 ASCO
64 HER2+ and ER+ are often BP Luminal If you have patients with co-morbidities that you are concerned about treating with Herceptin, is there a subset of patients that you can withhold this drug? Large group of clinical HER2+ cases that are BluePrint Luminal type (46%). Indicating the tumor s expression of the Luminal profile to be dominate over the expression of the HER2+ profile. These patients may have a lower response to trastuzumab (von Minckwitz et al, 2012)
65 Even the best KI67 assessment shows 30% discordance with MammaPrint Ki67 is assumed to be a fairly reliable measure of proliferation. Ki67 is utilized as a biomarker for chemotherapy The concordance between MammaPrint and centrally assessed Ki67 in Luminal-type patients is 71%, with a k score of 0.35 (95% CI ). The relatively high discordance with MammaPrint indicates that Ki67 and MammaPrint cannot reliably substitute for each other. MammaPrint has a higher hazard ratio than KI67 and is a better indictor for prognosis
66 Key Findings: 20% of the Basal is IHC ER+ These patients might take Endocrine therapy without effect Of the BluePrint Basal cases, 20% are not pathological Basal (16% Luminal, 4% HER2+ Of the 16% Luminal cases, the majority (80% are IHC ER/PR borderline ( 1% and 10%)
67 Are clinico-pathological data useful in fine tuning your treatment decisions towards adjuvant chemotherapy? Then the basic & confusing data.
68 68
69
70
71
72 Value of molecular subtyping and prediction to effect of chemotherapy Classification often dependent of method used Despite differences in gene lists, outcome similar Most signatures discriminate based on ER-status and proliferative activity Prognostic value restricted to ER-positive tumors Subclassification ER-positive breast cancer in luminal A and luminal B is arbitrary, based on proliferation Expression signatures are complementary to standard clinico-pathological parameters Weigelt et al., Nature Reviews Clinical Oncology (2011)
73 Predictive profiles fail Even the best arrays unable to give a sufficient signal at low expression of very relevant genes Subtle, non detectable changes in level of expression can make the difference Expression profiling unable to pick up resistance mechanisms if such a mechanism is only present in a proportion of the tumors Tumors are heterogeneous, RNA bulk analysis will not help Borst & Wessels, Cell Cycle (2011) 9: 4836
74 Integration of tumor features is essential Adequate morphological diagnosis Robust and reliable IHC-panel ER, PR, HER2, (Ki-67) Gene signature has additional value for a substantial subgroup Requires for all disciplines sufficient volume and expertise
75 The clinical issue. Think step by step (the most difficult one) Step 4: What are the factors that justify adjuvant chemotherapy (luminal A > B) My conlusions (for debate) Is every luminal A a luminal A? No, there are some high risk cancers between them What makes luminal B a luminal B? The proliferation/propensity to disseminate: you need extra information because you do not see it sufficiently on standard pathology/ihc (Ki 67: to much differences in quality, to many in betweens, not proven to be
76 The clinical issue. Think step by step (the most difficult one) Step 4: What are the factors that justify adjuvant chemotherapy (luminal A > B) My conlusions (for debate) What is the effect of chemotherapy: different for luminal A or B? Actually not proven: depends on prognosis & prediction (and now, I m sorry, the circle is round again)

77 Did you get some order out of chaos?




78 Thanks to the patients and all those who provided me with the presented information, and for inviting me, your attention & discussion The Van t Veer group
79 Intermediate Clinico/Pathological Risk What to do? Treat all patients with chemotherapy? Or be more selective, and treat those patients who benifit (and thus minimizing the risk of losing lives by foregoing chemotherapy)
80 70-gene assay (MammaPrint) Is not just another prognostic factor Is designed from the beginning to tell you the metastatic potential of an individual breast cancer
81 70-gene MammaPrint Functions of many genes are identified and are all related to the process of dissemination including proliferation
82 Validation 4: N = 100 Wittner et al., Clin Cancer Res 14: 2988, 2008 MGH series, Boston; Time to metastasis
83 Aims RASTER study Feasibility of using 70-gene signature in community-based settings Effect of 70-gene signature on adjuvant systemic treatment (AST) decisions AST decision at that time based on restrictive Dutch National Guideline 2004, 70GS result and doctors and patients preferences Outcome after 5 and 10 years of follow-up
84 Current aim RASTER study Outcome after 5 years of follow-up What would the risk estimation of the RASTER cohort be with currently used risk estimation tools to guide AST decisions Adjuvant!Online
85 Inclusion criteria Female ct1-4n0m0 invasive breast cancer Age < 61 years, amended to < 55 years (after 242 patients had been enrolled) Operable, unilateral tumor No history of previous malignancy, except for basal cell carcinoma or cervical carcinoma in situ No neoadjuvant systemic therapy
86 Dutch guideline 2004 RASTER enrollment High risk N+ N0; 35 years except for tumor 1 cm grade I N0; > 35 years: Larger than 1 cm grade III Larger than 2 cm grade II Larger than 3 cm any grade

87 Adjuvant Online version years 9% 10-yrs risk ER pos Low risk defined as 10-year survival Grade I 2-3 cm N0 probability at least 90% 2.6% risk Benefit ET 3%, CT 2%
88 Results 427 patients tested between Median FUP time 61.6 months 33 DDFS events DDFS event = distant recurrence, death (any cause), 2nd primary other than breast 11 deaths 9 breast cancer specific deaths
89 Proportion of patients labeled as high risk High risk Low risk 70-gene signature Adjuvant Online 89
90 With 70GS 29% less patients high risk With 70GS 29% less patients high risk category, compared to AOL High risk Low risk 70-gene signature Adjuvant Online 90
91 5-year DDFS of 427 patients according to 70GS or AOL 5YR DDFS 5YR DDFS 89.8% High risk 92.4% 96.1% Low risk 94.4% 70-gene signature Adjuvant Online 91
92 70GS-AOL risk groups and AST CT & ET ET CT no AST concordant low risk 70GS high- AOL low 70GS low- AOL high concordant high risk
93 Patient characteristics discordant group n=94 patients no AST or ET only Age years 75% pt1 (< 2 cm) 80% Grade II 82% IDC / ILC 72 / 20% ER pos 98% PgR pos 78% HER neg 90%
94 Conclusions AOL high risk and 70GS low risk patients who did not receive adjuvant systemic therapy or hormonal therapy only had an excellent 5-year DDFS (97.8%) This percentage is unlikely to drop below 90% at 10 years of follow-up Of this patient group at least 80% had an ER positive, HER2 negative, grade II tumor of 1 to 2 cm in size The percentage of high risk patients could be reduced by almost 30% when 70GS risk estimation was used

95 Acknowledgements All participating patients

96



97 Multiple answers from a single array MammaPrint 70 x x 5 Molecular subtypes BluePrint 80 x 5 mrna readout ER, PR and HER2 TargetPrint 3 x 5 Research Gene Panel TheraPrint 56 x 3 Normalization 465 x 3 Control probes 536 Drug response profile Drug response profile
The Current Status and the Future Prospects of Multigene testing in Europe
 The Current Status and the Future Prospects of Multigene testing in Europe Emiel J. Rutgers The Netherlands Cancer Institute Antoni Van Leeuwenhoek Hospital Amsterdam St. Gallen Recommendations 2009 =
The Current Status and the Future Prospects of Multigene testing in Europe Emiel J. Rutgers The Netherlands Cancer Institute Antoni Van Leeuwenhoek Hospital Amsterdam St. Gallen Recommendations 2009 =
30 years of progress in cancer research
 Breast Cancer Molecular Knowledge Integrated in Clinical Practice Personalized Medicine Laura J. Esserman UCSF Comprehensive Cancer Center Retreat Breast Cancer Management Advances 80-90s 1) Screening
Breast Cancer Molecular Knowledge Integrated in Clinical Practice Personalized Medicine Laura J. Esserman UCSF Comprehensive Cancer Center Retreat Breast Cancer Management Advances 80-90s 1) Screening
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011
 Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
Breast cancer classification: beyond the intrinsic molecular subtypes
 Breast cancer classification: beyond the intrinsic molecular subtypes Britta Weigelt, PhD Signal Transduction Laboratory CRUK London Research Institute Summary Breast cancer heterogeneity Molecular classification
Breast cancer classification: beyond the intrinsic molecular subtypes Britta Weigelt, PhD Signal Transduction Laboratory CRUK London Research Institute Summary Breast cancer heterogeneity Molecular classification
Adjuvan Chemotherapy in Breast Cancer
 Adjuvan Chemotherapy in Breast Cancer Prof Dr Adnan Aydıner Istanbul University, Oncology Institute aa1 Slide 1 aa1 adnan aydiner; 17.02.2008 15-Year Reductions in Recurrence and Disease-Specific Mortality
Adjuvan Chemotherapy in Breast Cancer Prof Dr Adnan Aydıner Istanbul University, Oncology Institute aa1 Slide 1 aa1 adnan aydiner; 17.02.2008 15-Year Reductions in Recurrence and Disease-Specific Mortality
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer
 The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA
 Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
OVERVIEW OF GENE EXPRESSION-BASED TESTS IN EARLY BREAST CANCER
 OVERVIEW OF GENE EXPRESSION-BASED TESTS IN EARLY BREAST CANCER Aleix Prat, MD PhD Medical Oncology Department Hospital Clínic of Barcelona University of Barcelona esmo.org Disclosures Advisory role for
OVERVIEW OF GENE EXPRESSION-BASED TESTS IN EARLY BREAST CANCER Aleix Prat, MD PhD Medical Oncology Department Hospital Clínic of Barcelona University of Barcelona esmo.org Disclosures Advisory role for
Contemporary Classification of Breast Cancer
 Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
MammaPrint, the story of the 70-gene profile
 MammaPrint, the story of the 70-gene profile René Bernards Professor of Molecular Carcinogenesis The Netherlands Cancer Institute Amsterdam Chief Scientific Officer Agendia Amsterdam The breast cancer
MammaPrint, the story of the 70-gene profile René Bernards Professor of Molecular Carcinogenesis The Netherlands Cancer Institute Amsterdam Chief Scientific Officer Agendia Amsterdam The breast cancer
Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer
 Node Positive Breast Cancer") Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer Kathy S. Albain, MD, FACP Professor of Medicine Dean s Scholar Loyola University Chicago Stritch School of Medicine Cardinal Bernardin
Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer Kathy S. Albain, MD, FACP Professor of Medicine Dean s Scholar Loyola University Chicago Stritch School of Medicine Cardinal Bernardin
UK Interdisciplinary Breast Cancer Symposium. Should lobular phenotype be considered when deciding treatment? Michael J Kerin
 UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
8/8/2011. PONDERing the Need to TAILOR Adjuvant Chemotherapy in ER+ Node Positive Breast Cancer. Overview
 Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Immunohistochemical classification of breast tumours
 Immunohistochemical classification of breast tumours Workshop in Diagnostic Immunohistochemistry September 19 th - 21 th 2018 Anne-Vibeke Lænkholm Department of Surgical Pathology, Zealand University Hospital,
Immunohistochemical classification of breast tumours Workshop in Diagnostic Immunohistochemistry September 19 th - 21 th 2018 Anne-Vibeke Lænkholm Department of Surgical Pathology, Zealand University Hospital,
National Medical Policy
 National Medical Policy Subject: Policy Number: MammaPrint, Prosigna and Other Gene Expression Tests for Breast Cancer NMP520 Effective Date*: May 2013 Updated: June 2017 This National Medical Policy is
National Medical Policy Subject: Policy Number: MammaPrint, Prosigna and Other Gene Expression Tests for Breast Cancer NMP520 Effective Date*: May 2013 Updated: June 2017 This National Medical Policy is
Adjuvant endocrine therapy (essentials in ER positive early breast cancer)
") Adjuvant endocrine therapy (essentials in ER positive early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Picking optimal adjuvant endocrine
Adjuvant endocrine therapy (essentials in ER positive early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Picking optimal adjuvant endocrine
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint
 Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Profili di espressione genica
 Profili di espressione genica Giampaolo Bianchini MD Ospedale San Raffaele, Milan - Italy Gene expression profiles Transcriptomics Gene DNA mrna mirnas Protein metilation Metabolite Genomics Transcriptomics
Profili di espressione genica Giampaolo Bianchini MD Ospedale San Raffaele, Milan - Italy Gene expression profiles Transcriptomics Gene DNA mrna mirnas Protein metilation Metabolite Genomics Transcriptomics
Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers
 日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
Breast Cancer Assays of Genetic Expression in Tumor Tissue
 Breast Cancer Assays of Genetic Expression in Tumor Tissue Policy Number: Original Effective Date: MM.12.009 12/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 12/16/2016
Breast Cancer Assays of Genetic Expression in Tumor Tissue Policy Number: Original Effective Date: MM.12.009 12/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 12/16/2016
Section: Genetic Testing Last Reviewed Date: March Policy No: 42 Effective Date: June 1, 2014
 Medical Policy Manual Topic: Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis In Patients With Breast Cancer Date of Origin: October 5, 2004 Section: Genetic Testing Last
Medical Policy Manual Topic: Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis In Patients With Breast Cancer Date of Origin: October 5, 2004 Section: Genetic Testing Last
Medical Policy. Description. Related Policies. Policy. Effective Date January 1, 2015 Original Policy Date December 1, 2005
 2.04.36 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Section 2.0 Medicine Subsection 2.04 Pathology/Laboratory Effective Date January
2.04.36 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Section 2.0 Medicine Subsection 2.04 Pathology/Laboratory Effective Date January
Breast cancer: Molecular STAGING classification and testing. Korourian A : AP,CP ; MD,PHD(Molecular medicine)
") Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland
 What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
Oncotype DX testing in node-positive disease
 Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
38 years old, premenopausal, had L+snbx. Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI %
 38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
Profili Genici e Personalizzazione del trattamento adiuvante nel carcinoma mammario G. RICCIARDI
 Profili Genici e Personalizzazione del trattamento adiuvante nel carcinoma mammario G. RICCIARDI UOC Oncologia Medica, A.O. Papardo, Messina Dir. Prof. V. Adamo BREAST CANCER Brain Adjuvant Medical Therapies
Profili Genici e Personalizzazione del trattamento adiuvante nel carcinoma mammario G. RICCIARDI UOC Oncologia Medica, A.O. Papardo, Messina Dir. Prof. V. Adamo BREAST CANCER Brain Adjuvant Medical Therapies
Oncotype DX MM /01/2008. HMO; PPO; QUEST 03/01/2014 Section: Other/Miscellaneous Place(s) of Service: Office
 of Service: Office") Oncotype DX Policy Number: Original Effective Date: MM.12.009 12/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 03/01/2014 Section: Other/Miscellaneous Place(s) of Service: Office
Oncotype DX Policy Number: Original Effective Date: MM.12.009 12/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 03/01/2014 Section: Other/Miscellaneous Place(s) of Service: Office
Extended Hormonal Therapy
 Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer
 Medical Policy Manual Genetic Testing, Policy No. 42 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Next Review: December 2018 Last Review:
Medical Policy Manual Genetic Testing, Policy No. 42 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Next Review: December 2018 Last Review:
Postoperative Adjuvant Chemotherapies. Stefan Aebi Luzerner Kantonsspital
 Postoperative Adjuvant Chemotherapies Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Does Chemotherapy Work in Older Patients? ER : Chemotherapy vs nil Age
Postoperative Adjuvant Chemotherapies Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Does Chemotherapy Work in Older Patients? ER : Chemotherapy vs nil Age
Current Status and Future Development of Tools for Prognosis and Prediction - USA
 Current Status and Future Development of Tools for Prognosis and Prediction - USA John H. Ward, MD Professor of Medicine University of Utah School of Medicine Huntsman Cancer Institute October18, 2009
Current Status and Future Development of Tools for Prognosis and Prediction - USA John H. Ward, MD Professor of Medicine University of Utah School of Medicine Huntsman Cancer Institute October18, 2009
A new way of looking at breast cancer tumour biology
 A new way of looking at breast cancer tumour biology Contents Intrinsic subtypes of breast cancer 3 Gene expression assays 3 Basis of the Prosigna test 4 Information provided by Prosigna 5 The accuracy
A new way of looking at breast cancer tumour biology Contents Intrinsic subtypes of breast cancer 3 Gene expression assays 3 Basis of the Prosigna test 4 Information provided by Prosigna 5 The accuracy
Hormone therapyduration: Can weselectthosepatientswho benefitfromtreatmentextension?
 Hormone therapyduration: Can weselectthosepatientswho benefitfromtreatmentextension? Ivana Sestak, PhD Centre for Cancer Prevention Wolfson Institute of Preventive Medicine Queen Mary University London
Hormone therapyduration: Can weselectthosepatientswho benefitfromtreatmentextension? Ivana Sestak, PhD Centre for Cancer Prevention Wolfson Institute of Preventive Medicine Queen Mary University London
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer
 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Policy Number: 2.04.36 Last Review: 9/2018 Origination: 1/2006 Next Review: 9/2019 Policy
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Policy Number: 2.04.36 Last Review: 9/2018 Origination: 1/2006 Next Review: 9/2019 Policy
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer
 The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
Breast Cancer Assays of Genetic Expression in Tumor Tissue
 Breast Cancer Assays of Genetic Expression in Tumor Tissue Policy Number: Original Effective Date: MM.12.009 12/02/2008 Line(s) of Business: Current Effective Date Section: 05/25/2018 Other Miscellaneous
Breast Cancer Assays of Genetic Expression in Tumor Tissue Policy Number: Original Effective Date: MM.12.009 12/02/2008 Line(s) of Business: Current Effective Date Section: 05/25/2018 Other Miscellaneous
Morphological and Molecular Typing of breast Cancer
 Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological
Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological
Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer
 Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY
 Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY Methodology The test is based on the reported 50-gene classifier algorithm originally named PAM50 and is performed on the ncounter Dx Analysis System
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY Methodology The test is based on the reported 50-gene classifier algorithm originally named PAM50 and is performed on the ncounter Dx Analysis System
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY
 Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY GENE EXPRESSION PROFILING WITH PROSIGNA What is Prosigna? Prosigna Breast Cancer Prognostic Gene Signature Assay is an FDA-approved assay which provides
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY GENE EXPRESSION PROFILING WITH PROSIGNA What is Prosigna? Prosigna Breast Cancer Prognostic Gene Signature Assay is an FDA-approved assay which provides
She counts on your breast cancer expertise at the most vulnerable time of her life.
 HOME She counts on your breast cancer expertise at the most vulnerable time of her life. Empowering the right treatment choice for better patient outcomes. The comprehensive genomic assay experts trust.
HOME She counts on your breast cancer expertise at the most vulnerable time of her life. Empowering the right treatment choice for better patient outcomes. The comprehensive genomic assay experts trust.
Relevancia práctica de la clasificación de subtipos intrínsecos en cáncer de mama Miguel Martín Instituto de Investigación Sanitaria Gregorio Marañón
 Relevancia práctica de la clasificación de subtipos intrínsecos en cáncer de mama Miguel Martín Instituto de Investigación Sanitaria Gregorio Marañón Universidad Complutense Madrid The new technologies
Relevancia práctica de la clasificación de subtipos intrínsecos en cáncer de mama Miguel Martín Instituto de Investigación Sanitaria Gregorio Marañón Universidad Complutense Madrid The new technologies
A breast cancer gene signature for indolent disease
 Breast Cancer Res Treat (2017) 164:461 466 DOI 10.1007/s10549-017-4262-0 EPIDEMIOLOGY A breast cancer gene signature for indolent disease Leonie J. M. J. Delahaye 1 Caroline A. Drukker 2,3 Christa Dreezen
Breast Cancer Res Treat (2017) 164:461 466 DOI 10.1007/s10549-017-4262-0 EPIDEMIOLOGY A breast cancer gene signature for indolent disease Leonie J. M. J. Delahaye 1 Caroline A. Drukker 2,3 Christa Dreezen
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives
 Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
The 70-Gene Signature (MammaPrint) As a Guide for the Management of Early Stage Breast Cancer. California Technology Assessment Forum
 As a Guide for the Management of Early Stage Breast Cancer. California Technology Assessment Forum") TITLE: The 70-Gene Signature (MammaPrint) As a Guide for the Management of Early Stage Breast Cancer AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department
TITLE: The 70-Gene Signature (MammaPrint) As a Guide for the Management of Early Stage Breast Cancer AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department
Janet E. Dancey NCIC CTG NEW INVESTIGATOR CLINICAL TRIALS COURSE. August 9-12, 2011 Donald Gordon Centre, Queen s University, Kingston, Ontario
 Janet E. Dancey NCIC CTG NEW INVESTIGATOR CLINICAL TRIALS COURSE August 9-12, 2011 Donald Gordon Centre, Queen s University, Kingston, Ontario Session: Correlative Studies in Phase III Trials Title: Design
Janet E. Dancey NCIC CTG NEW INVESTIGATOR CLINICAL TRIALS COURSE August 9-12, 2011 Donald Gordon Centre, Queen s University, Kingston, Ontario Session: Correlative Studies in Phase III Trials Title: Design
Adjuvant Endocrine Therapy: How Long is Long Enough?
 Adjuvant Endocrine Therapy: How Long is Long Enough? Harold J. Burstein, MD, PhD Dana-Farber Cancer Institute Harvard Medical School Boston, Massachusetts hburstein@partners.org I have no conflicts to
Adjuvant Endocrine Therapy: How Long is Long Enough? Harold J. Burstein, MD, PhD Dana-Farber Cancer Institute Harvard Medical School Boston, Massachusetts hburstein@partners.org I have no conflicts to
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer
 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Policy Number: 2.04.36 Last Review: 1/2019 Origination: 1/2006 Next Review: 9/2019 Policy
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Policy Number: 2.04.36 Last Review: 1/2019 Origination: 1/2006 Next Review: 9/2019 Policy
Corporate Medical Policy
 Corporate Medical Policy Assays of Genetic Expression to Determine Prognosis of Breast File Name: Origination: Last CAP Review: Next CAP Review: Last Review: assays_of_genetic_expression_to_determine_prognosis_of_breast_cancer
Corporate Medical Policy Assays of Genetic Expression to Determine Prognosis of Breast File Name: Origination: Last CAP Review: Next CAP Review: Last Review: assays_of_genetic_expression_to_determine_prognosis_of_breast_cancer
Molecular in vitro diagnostic test for the quantitative detection of the mrna expression of ERBB2, ESR1, PGR and MKI67 in breast cancer tissue.
 Innovation for your breast cancer diagnostics PGR G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C ERBB2
Innovation for your breast cancer diagnostics PGR G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C ERBB2
Prognostic and predictive biomarkers. Marc Buyse International Drug Development Institute (IDDI) Louvain-la-Neuve, Belgium
 Louvain-la-Neuve, Belgium") Prognostic and predictive biomarkers Marc Buyse International Drug Development Institute (IDDI) Louvain-la-Neuve, Belgium marc.buyse@iddi.com 1 Prognostic biomarkers (example: gene signature) 2 PROGNOSTIC
Prognostic and predictive biomarkers Marc Buyse International Drug Development Institute (IDDI) Louvain-la-Neuve, Belgium marc.buyse@iddi.com 1 Prognostic biomarkers (example: gene signature) 2 PROGNOSTIC
MEDICAL POLICY. SUBJECT: GENETIC ASSAY OF TUMOR TISSUE TO DETERMINE PROGNOSIS OF BREAST CANCER (OncotypeDX TM, MammaPrint )
") MEDICAL POLICY PAGE: 1 OF: 8 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
MEDICAL POLICY PAGE: 1 OF: 8 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
William J. Gradishar MD
 Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Introduction. Wilfred Truin 1 Rudi M. H. Roumen. Vivianne C. G. Tjan-Heijnen 2 Adri C. Voogd
 Breast Cancer Res Treat (2017) 164:133 138 DOI 10.1007/s10549-017-4220-x EPIDEMIOLOGY Estrogen and progesterone receptor expression levels do not differ between lobular and ductal carcinoma in patients
Breast Cancer Res Treat (2017) 164:133 138 DOI 10.1007/s10549-017-4220-x EPIDEMIOLOGY Estrogen and progesterone receptor expression levels do not differ between lobular and ductal carcinoma in patients
Rationale For & Design of TAILORx. Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York
 Rationale For & Design of TAILORx Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York Declining Breast Cancer Mortality & Event Rates in Adjuvant
Rationale For & Design of TAILORx Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York Declining Breast Cancer Mortality & Event Rates in Adjuvant
Point of View on Early Triple Negative
 Point of View on Early Triple Negative Valentina Rossi, MD UOSD Oncologia dei Tumori della Mammella Azienda Ospedaliera S.Camillo-Forlanini VRossi@scamilloforlanini.rm.it Outline Neoadjuvant Setting IPSY-2
Point of View on Early Triple Negative Valentina Rossi, MD UOSD Oncologia dei Tumori della Mammella Azienda Ospedaliera S.Camillo-Forlanini VRossi@scamilloforlanini.rm.it Outline Neoadjuvant Setting IPSY-2
ORMONOTERAPIA ADIUVANTE: QUALE LA DURATA OTTIMALE? MARIANTONIETTA COLOZZA
 ORMONOTERAPIA ADIUVANTE: QUALE LA DURATA OTTIMALE? MARIANTONIETTA COLOZZA THE NATURAL HISTORY OF HORMONE RECEPTOR- POSITIVE BREAST CANCER IS VERY LONG Recurrence hazard rate 0.3 0.2 0.1 0 ER+ (n=2,257)
ORMONOTERAPIA ADIUVANTE: QUALE LA DURATA OTTIMALE? MARIANTONIETTA COLOZZA THE NATURAL HISTORY OF HORMONE RECEPTOR- POSITIVE BREAST CANCER IS VERY LONG Recurrence hazard rate 0.3 0.2 0.1 0 ER+ (n=2,257)
Molecular in vitro diagnostic test for the quantitative detection of the mrna expression of ERBB2, ESR1, PGR and MKI67 in breast cancer tissue.
 Innovation for your breast cancer diagnostics Now valid ated on: -Roche cob as z 480 A nalyzer -Roche L ightcycle r 480 II - ABI 750 0 Fast -Versant kpcr Cyc ler PGR ESR1 MKI67 Molecular in vitro diagnostic
Innovation for your breast cancer diagnostics Now valid ated on: -Roche cob as z 480 A nalyzer -Roche L ightcycle r 480 II - ABI 750 0 Fast -Versant kpcr Cyc ler PGR ESR1 MKI67 Molecular in vitro diagnostic
Considerations in Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
Genomic Profiling in Early Stage Breast Cancer. James V. Pellicane, MD, FACS Director of Breast Oncology Bon Secours Cancer Institute Richmond, VA
 Genomic Profiling in Early Stage Breast Cancer James V. Pellicane, MD, FACS Director of Breast Oncology Bon Secours Cancer Institute Richmond, VA 1 Disclosures Speakers Bureau Agendia Focal Therapeutics
Genomic Profiling in Early Stage Breast Cancer James V. Pellicane, MD, FACS Director of Breast Oncology Bon Secours Cancer Institute Richmond, VA 1 Disclosures Speakers Bureau Agendia Focal Therapeutics
A Study to Evaluate the Effect of Neoadjuvant Chemotherapy on Hormonal and Her-2 Receptor Status in Carcinoma Breast
 Original Research Article A Study to Evaluate the Effect of Neoadjuvant Chemotherapy on Hormonal and Her-2 Receptor Status in Carcinoma Breast E. Rajesh Goud 1, M. Muralidhar 2*, M. Srinivasulu 3 1Senior
Original Research Article A Study to Evaluate the Effect of Neoadjuvant Chemotherapy on Hormonal and Her-2 Receptor Status in Carcinoma Breast E. Rajesh Goud 1, M. Muralidhar 2*, M. Srinivasulu 3 1Senior
Manejo do câncer de mama RH+ na adjuvância: o que há de novo?
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
RNA preparation from extracted paraffin cores:
 Supplementary methods, Nielsen et al., A comparison of PAM50 intrinsic subtyping with immunohistochemistry and clinical prognostic factors in tamoxifen-treated estrogen receptor positive breast cancer.
Supplementary methods, Nielsen et al., A comparison of PAM50 intrinsic subtyping with immunohistochemistry and clinical prognostic factors in tamoxifen-treated estrogen receptor positive breast cancer.
Sesiones interhospitalarias de cáncer de mama. Revisión bibliográfica 4º trimestre 2015
 Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Search for Randox, Blueprint, PAM50, Breast Cancer Index, IHC4, Mammostrat, and NPI+ Date limits = 2002 date Filter = human studies only
 Appendix 1 Search strategy Update search for Oncotype DX, and MammaPrint Date limits = January 2009 date Filter = human studies only 1. exp Breast Neoplasms/ 2. exp mammary neoplasms/ 3. exp "Neoplasms,
Appendix 1 Search strategy Update search for Oncotype DX, and MammaPrint Date limits = January 2009 date Filter = human studies only 1. exp Breast Neoplasms/ 2. exp mammary neoplasms/ 3. exp "Neoplasms,
Is Gene Expression Profiling the Best Method for Selecting Systemic Therapy in EBC? Norman Wolmark Miami March 8, 2013
 Is Gene Expression Profiling the Best Method for Selecting Systemic Therapy in EBC? Norman Wolmark Miami March 8, 2013 Changing Phases claudin low Lum A Lum B Basal Her2 NIH Consensus Development Panel,
Is Gene Expression Profiling the Best Method for Selecting Systemic Therapy in EBC? Norman Wolmark Miami March 8, 2013 Changing Phases claudin low Lum A Lum B Basal Her2 NIH Consensus Development Panel,
Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer. Cheol Min Kang 2018/04/05
 Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
The Oncotype DX Assay A Genomic Approach to Breast Cancer
 The Oncotype DX Assay A Genomic Approach to Breast Cancer Pathology: 20 th and 21 st Century Size Age Phenotype Nodal status Protein/Gene Genomic Profiling Prognostic & Predictive Markers Used in Breast
The Oncotype DX Assay A Genomic Approach to Breast Cancer Pathology: 20 th and 21 st Century Size Age Phenotype Nodal status Protein/Gene Genomic Profiling Prognostic & Predictive Markers Used in Breast
Giuseppe Viale for the BIG 1 98 Collaborative and International Breast Cancer Study Groups
 Central Review of ER, PgR and HER2 in BIG 1 98 Evaluating Letrozole vs. Letrozole Tamoxifen vs. Tamoxifen Letrozole as Adjuvant Endocrine Therapy for Postmenopausal Women with Hormone Receptor Positive
Central Review of ER, PgR and HER2 in BIG 1 98 Evaluating Letrozole vs. Letrozole Tamoxifen vs. Tamoxifen Letrozole as Adjuvant Endocrine Therapy for Postmenopausal Women with Hormone Receptor Positive
Current Status of Biomarkers (including DNA Tumor Markers and Immunohistochemistry in the Laboratory Diagnosis of Tumors)
") Current Status of Biomarkers (including DNA Tumor Markers and Immunohistochemistry in the Laboratory Diagnosis of Tumors) Kael Mikesell, DO McKay-Dee Hospital May 14, 2015 Outline Update to DNA Testing
Current Status of Biomarkers (including DNA Tumor Markers and Immunohistochemistry in the Laboratory Diagnosis of Tumors) Kael Mikesell, DO McKay-Dee Hospital May 14, 2015 Outline Update to DNA Testing
Intervention(s) Results primary outcome Results secondary and other outcomes
 Results primary outcome Results secondary and other outcomes") Uitgangsvraag 4: evidence tables Welke nieuwe vormen van risicoprofilering zijn - in tegenstelling tot de traditionele prognostische factoren als tumorgrootte, lymfklierstatus en tumorgradering - van invloed
Uitgangsvraag 4: evidence tables Welke nieuwe vormen van risicoprofilering zijn - in tegenstelling tot de traditionele prognostische factoren als tumorgrootte, lymfklierstatus en tumorgradering - van invloed
Systemic Management of Breast Cancer
 Systemic Management of Breast Cancer Why Who When What How long Etc. Vernon Harvey Rotorua, June 2014 Systemic Management of Breast Cancer Metastatic Disease Adjuvant Therapy Aims of therapy Quality of
Systemic Management of Breast Cancer Why Who When What How long Etc. Vernon Harvey Rotorua, June 2014 Systemic Management of Breast Cancer Metastatic Disease Adjuvant Therapy Aims of therapy Quality of
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 67 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 67 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Journal of Breast Cancer
 Journal of Breast Cancer ORIGINAL ARTICLE J Breast Cancer 211 March; 14(1): 33-38 The 7-Gene Prognostic Signature for Korean Breast Cancer Patients Kuk Young Na, Ku Sang Kim, Jeong Eon Lee 1, Hee Jeong
Journal of Breast Cancer ORIGINAL ARTICLE J Breast Cancer 211 March; 14(1): 33-38 The 7-Gene Prognostic Signature for Korean Breast Cancer Patients Kuk Young Na, Ku Sang Kim, Jeong Eon Lee 1, Hee Jeong
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
FAQs for UK Pathology Departments
 FAQs for UK Pathology Departments This is an educational piece written for Healthcare Professionals FAQs for UK Pathology Departments If you would like to discuss any of the listed FAQs further, or have
FAQs for UK Pathology Departments This is an educational piece written for Healthcare Professionals FAQs for UK Pathology Departments If you would like to discuss any of the listed FAQs further, or have
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY. Dr. Carlos Garbino
 EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
Gene signature for risk stratification and treatment of breast cancer: Incorporating tumor biology in clinical decision-making Drukker, Caroline
 UvA-DARE (Digital Academic Repository) Gene signature for risk stratification and treatment of breast cancer: Incorporating tumor biology in clinical decision-making Drukker, Caroline Link to publication
UvA-DARE (Digital Academic Repository) Gene signature for risk stratification and treatment of breast cancer: Incorporating tumor biology in clinical decision-making Drukker, Caroline Link to publication
Clinical Policy Title: Breast cancer index genetic testing
 Clinical Policy Title: Breast cancer index genetic testing Clinical Policy Number: 02.01.22 Effective Date: January 1, 2017 Initial Review Date: October 19, 2016 Most Recent Review Date: October 19, 2016
Clinical Policy Title: Breast cancer index genetic testing Clinical Policy Number: 02.01.22 Effective Date: January 1, 2017 Initial Review Date: October 19, 2016 Most Recent Review Date: October 19, 2016
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 55 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 55 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Breast Cancer Earlier Disease. Stefan Aebi Luzerner Kantonsspital
 Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?
 as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?") 1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
ADAPT. Adjuvant Dynamic marker- Adjusted Personalized Therapy trial optimizing risk assessment and therapy response prediction in early breast cancer
 ADAPT Adjuvant Dynamic marker- Adjusted Personalized Therapy trial optimizing risk assessment and therapy response prediction in early breast cancer Therapieindikation gesteuert durch prognostische Information
ADAPT Adjuvant Dynamic marker- Adjusted Personalized Therapy trial optimizing risk assessment and therapy response prediction in early breast cancer Therapieindikation gesteuert durch prognostische Information
Update on New Perspectives in Endocrine-Sensitive Breast Cancer. James R. Waisman, MD
 Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
MammaPrint Improving treatment decisions in breast cancer Support and Involvement of EU
 MammaPrint Improving treatment decisions in breast cancer Support and Involvement of EU 1 Bas van der Baan VP Clinical Affairs Irvine, California Amsterdam, The Netherlands 2 Two Crucial Questions in Cancer
MammaPrint Improving treatment decisions in breast cancer Support and Involvement of EU 1 Bas van der Baan VP Clinical Affairs Irvine, California Amsterdam, The Netherlands 2 Two Crucial Questions in Cancer
Ideal neo-adjuvant Chemotherapy in breast ca. Dr Khanyile Department of Medical Oncology, University of Pretoria
 Ideal neo-adjuvant Chemotherapy in breast ca Dr Khanyile Department of Medical Oncology, University of Pretoria When is neo-adjuvant Chemo required? Locally advanced breast ca: - Breast conservative surgery
Ideal neo-adjuvant Chemotherapy in breast ca Dr Khanyile Department of Medical Oncology, University of Pretoria When is neo-adjuvant Chemo required? Locally advanced breast ca: - Breast conservative surgery
Present Role of Immunohistochemistry in the. Subtypes. Beppe Viale European Institute of Oncology University of Milan Milan-Italy
 Present Role of Immunohistochemistry in the Classification of Molecular Subtypes Beppe Viale European Institute of Oncology University of Milan Milan-Italy We know it is many diseases Breast cancer is
Present Role of Immunohistochemistry in the Classification of Molecular Subtypes Beppe Viale European Institute of Oncology University of Milan Milan-Italy We know it is many diseases Breast cancer is
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 47 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 47 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Retrospective analysis to determine the use of tissue genomic analysis to predict the risk of recurrence in early stage invasive breast cancer.
 Retrospective analysis to determine the use of tissue genomic analysis to predict the risk of recurrence in early stage invasive breast cancer. Goal of the study: 1.To assess whether patients at Truman
Retrospective analysis to determine the use of tissue genomic analysis to predict the risk of recurrence in early stage invasive breast cancer. Goal of the study: 1.To assess whether patients at Truman
Gene Expression Profiling for Managing Breast Cancer Treatment. Policy Specific Section: Medical Necessity and Investigational / Experimental
 Medical Policy Gene Expression Profiling for Managing Breast Cancer Treatment Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date:
Medical Policy Gene Expression Profiling for Managing Breast Cancer Treatment Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date:
DIAGNOSTICS ASSESSMENT PROGRAMME
 DIAGNOSTICS ASSESSMENT PROGRAMME Evidence overview Tumour profiling tests to guide adjuvant chemotherapy decisions in people with breast cancer (update of DG10) This overview summarises the key issues
DIAGNOSTICS ASSESSMENT PROGRAMME Evidence overview Tumour profiling tests to guide adjuvant chemotherapy decisions in people with breast cancer (update of DG10) This overview summarises the key issues
Kathy Albain, MD. Chemotherapy in Luminal Breast Cancer: Who Benefits? Loyola University Chicago Stritch School of Medicine
 Chemotherapy in Luminal Breast Cancer: Who Benefits? Kathy Albain, MD Loyola University Chicago Stritch School of Medicine, Director, Breast Clinical Research Program, Cardinal Bernardin Cancer Center,
Chemotherapy in Luminal Breast Cancer: Who Benefits? Kathy Albain, MD Loyola University Chicago Stritch School of Medicine, Director, Breast Clinical Research Program, Cardinal Bernardin Cancer Center,
XII Michelangelo Foundation Seminar
 XII Michelangelo Foundation Seminar The opportunity of the neoadjuvant approach L. Gianni, Milan, I XII Michelangelo Foundation Seminar Milano, October 12, 2012 The opportunity of the neoadjuvant approach
XII Michelangelo Foundation Seminar The opportunity of the neoadjuvant approach L. Gianni, Milan, I XII Michelangelo Foundation Seminar Milano, October 12, 2012 The opportunity of the neoadjuvant approach
Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE
 Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE Neoadjuvant Chemotherapy Indications: Management of locally advanced invasive breast cancers including inflammatory breast
Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE Neoadjuvant Chemotherapy Indications: Management of locally advanced invasive breast cancers including inflammatory breast
Oncotype DX tools User Guide
 Oncotype DX tools User Guide This guide provides an overview of the data and quick access to the Oncotype DX tools Oncotype DX tools offers two quantitative calculator tools that may be used together with
Oncotype DX tools User Guide This guide provides an overview of the data and quick access to the Oncotype DX tools Oncotype DX tools offers two quantitative calculator tools that may be used together with
Early Stage Disease. Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center
 SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
Neoadjuvant therapy a new pathway to registration?
 Neoadjuvant therapy a new pathway to registration? Graham Ross, FFPM Clinical Science Leader Roche Products Ltd Welwyn Garden City, UK (full time employee) Themes Neoadjuvant therapy Pathological Complete
Neoadjuvant therapy a new pathway to registration? Graham Ross, FFPM Clinical Science Leader Roche Products Ltd Welwyn Garden City, UK (full time employee) Themes Neoadjuvant therapy Pathological Complete
Session thématisée Les Innovations diagnostiques en cancérologie
 10 èmes Journées Scientifiques du Cancéropôle Nord-Ouest 10-12 mai 2017, Deauville Session thématisée Les Innovations diagnostiques en cancérologie Les signatures multigéniques pronostiques dans le cancer
10 èmes Journées Scientifiques du Cancéropôle Nord-Ouest 10-12 mai 2017, Deauville Session thématisée Les Innovations diagnostiques en cancérologie Les signatures multigéniques pronostiques dans le cancer