LESSONS LEARNT Melanoma Academic Perspective
|
|
|
- Philomena Davis
- 6 years ago
- Views:
Transcription


1 LESSONS LEARNT Melanoma Academic Perspective Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy
2 Disclosures Employment or Leadership Position: None Consultant/Advisory Role: Bristol-Meyers Squibb, Merck Sharp & Dohme, Roche-Genentech, Ventana, Novartis, Amgen, Array Stock Ownership: None Honoraria: None Research Funding: Bristol-Meyers Squibb, Roche- Genentech, Ventana Expert Testimony: None Other Remuneration: None
3 Meta-analysis of Phase II cooperative group trials in metastatic stage IV melanoma to determine progression-free and overall survival benchmarks for future Phase II trials This metanalysis summarises the outcome of advanced melanoma patients before 2011 Median survival time 6.2 months Alive at 1 year 25.5% Median PFS 1.7 months Progression free at 6 months 14.5% Korn E, et al. J Clin Oncol 2008;26: Reprinted with permission 2008, American Society of Clinical Oncology. All rights reserved
4 Treatment for advanced melanoma approved by EMA after ipilimumab 2012 vemurafenib 2013 dabrafenib 2014 trametinib 2015 nivolumab pembrolizumab combo dabrafenib-trametinib combo vemurafenib-cobimetinib talimogene laherparepvec Agent Company Indication Nivolumab BMS Unresectable or metastatic melanoma Ipilimumab BMS Unresectable or metastatic melanoma pending combo ipilimumabnivolumab Vemurafenib Roche/Genentech Unresectable or metastatic melanoma with BRAF V600E mutation Dabrafenib Novartis Unresectable or metastatic melanoma with BRAF V600E mutation Trametinib Novartis Unresectable or metastatic melanoma with BRAF V600E/K mutation Talimogene laherparepvec Amgen Unresectable melanoma that is regionally or distantly metastatic (Stage IIIB, IIIC, and IVM1a) with no bone, brain, lung, or other visceral disease.
:83")
5 Advanced melanoma: different approaches according to mutational status BRAF V600E/K Q61 NRAS c-kit BRAF wt NRAS wt Ascierto P, et al. J Transl Med May 2;10(1):83



6 Ipilimumab slow action, but it s able to make chronic the disease Two different drugs... Two different concepts Vemurafenib quick action, rapid metabolic shutdown, unfortunately resistance after a median of 6-8 months Oct-2010 Jun-2011 Day 0 Day 15
7 Target Therapy

8 VEMU-PET study Patient # 18 V600E BRAF mutated Day 0 Day 7 Istituto Nazionale Tumori Napoli
9 Different evidences of rapid progression disease after BRAF inhibitors treatment Experience Patients sample (n) % of patients with a rapid disease progression kinetics BRIM % BRIM % Ascierto et al % Ackerman et al % Italian ipilimumab EAP 54 41% Fisher et al % Ascierto et al. J Trans Med 2013

10 BRIM-3: OS Without Censoring at Crossover (ITT Population) DTIC (n = 338) 10.3 ( ) 46.0% 24.5% 18.9% 15.6% DTIC Data cutoff: August 14, DTIC, dacarbazine; ITT, intention-to-treat. Ascierto P, et al. Bridge meeting
11 BRIM-3: OS Was Better for ECOG PS 0 in Vemurafenib Arm Data cutoff: August 14, ECOG PS, Eastern Cooperative Oncology Group performance status. Ascierto P, et al. Bridge meeting
12 BRIM-3: OS Was Better for Normal Baseline LDH in Vemurafenib Arm Data cutoff: August 14, LDH, lactate dehydrogenase. Ascierto P, et al. Bridge meeting







13 Effect of BRAF inhibitors on the immune system BRAF inhibition is associated with increased melanoma antigen expression in tumours of patients with metastatic melanoma CD4+ and CD8+ increase in responder lesion and decrease in lesions which progressed Antitumour activity of combined BRAFi+MEKi plus anti-pd-1 3 MHC and melanoma antigen expression 3 BRAF inhibition is associated with increased CD8+ T-cell infiltrate in tumours of patients with metastatic melanoma Wilmott JS, et al. Clin Cancer Res 2011;18: , Reprinted from Clinical Cancer Research 2012, with permission from AACR Frederick DT, et al. Clin Cancer Res 2013;19: , Reprinted from Clinical Cancer Research 2013, with permission from AACR 3. From Hu-Lieskovan S et al. Sci Transl Med 2015;7:279ra41., Reprinted with permission from AAAS






14 Resistance BRAF-mutant melanomas acquire BRAF inhibitor resistance via upregulation of both MAPK and PI3K AKT pathways. However, MAPK reactivation is the major pathway of acquired BRAF inhibitor resistance in melanoma. Among MAPK-reactivating mechanisms associated with acquired BRAF inhibitor resistance the most frequents are NRAS mutations, mutant BRAF amplification and alternative splice variants, MAP2K1 and CDKN2A mutations Shi H et al. Cancer Discovery 2014; 4:80-93 Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy Day 0 Day 7 Day 15 Day 30
 5 improved response rates and PFS in BRAF")
15 Rationale for the combination of BRAF and MEK inhibitors Rationale Most common mechanism of acquired resistance to vemurafenib is MAPK reactivation through MEK 1,2 MEK + BRAF inhibition prevents the development of acquired resistance in preclinical models 3 MEK + BRAF inhibition (dabrafenib + trametinib 4 phase 3 and vemurafenib + cobimetinib phase 1/2) 5 improved response rates and PFS in BRAF inhibitor naive melanoma patients Reduced incidence of hyperproliferative lesions by blocking paradoxical activation of the MAPK pathway from RAF inhibition 6 BRAF inhibitors vemurafenib dabrafenib encorafenib MEK inhibitors trametinib cobimetinib binimetinib 1. Shi H et al. Cancer Discov Trunzer K et al. J Clin Oncol Paraiso K et al. Br J Cancer Long GV et al. J Clin Oncol Ribas A et al. Lancet Oncol Su F et al. New Engl J Med Gowrishankar et al.; licensee InTech. ISBN: , DOI: / Available from: Open access article distributed under the terms of the Creative Commons Attribution License 3.0
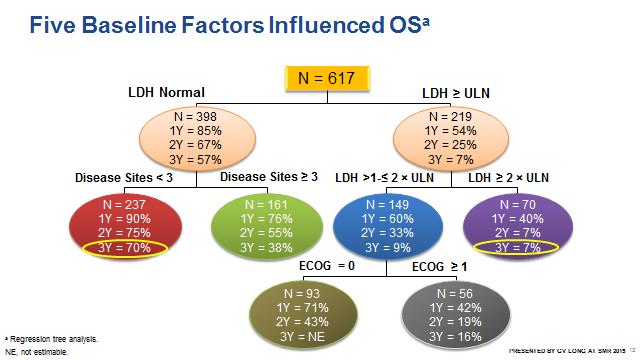
16 Results from the fase I/II dabrafenib/ trametinib Estimated Survival Function Cohort Dabrafenib 150 mg BID Dabrafenib 150 mg BID/trametinib 1 mg QD Dabrafenib 150 mg BID/trametinib 2 mg QD Cohort 150/2 Median: 25 mo 12-mo OS rate: 80% 24-mo OS rate: 51% 36-mo OS rate: 38% 0.0 Patients at Risk Data as of 15 January 2015 Time Since Randomization, months Longer follow-up reveals median OS of 25 months for patients in the 150/2 cohort. Landmark OS results for the 150/2 cohort: 1 year, 80%; 2 year, 51%; 3 year, 38%. Normal LDH and fewer disease sites were associated with prolonged survival. Prior immunotherapy had no effect on OS. No new safety signal observed and no increase in cuscc cases or treatment-emergent malignancies Daud A, et al. ASCO 2015, J Clin Oncol 2015;33 (suppl; abstr 9036) Poster 279 (with permission of Daud A.)


17 BRAFì + MEKì: OS data from phase III clinical trial CoBrim: Overall Survival 1. Long G et al. Lancet Robert C et al. ECC Atkinson V et al. SMR 2015.
18
19
20 Immunotherapy

:viii6 viii9; 2. Eggermont AM. Ann Oncol 2012;23(suppl 8):viii53 viii57; 3. Hodi FS, et al. N Engl J Med 2010;363:711 723; 4. Kantoff PW, et al.")
21 The potential of I-O therapies I-O therapies are being investigated for their potential to provide long-term survival in patients with various solid or haematologic malignancies 1 4 Immune adaptability, and memory offers the potential for long-term survival 1,2,8 Targeting the immune system not the tumour offers the potential for activity across multiple tumour types 2 Potential to improve clinical outcome In various solid and haematologic malignancies Unique MoAs offer the opportunity for combination 7 Unique safety profiles 1. Finn OJ. Ann Oncol 2012;23(suppl 8):viii6 viii9; 2. Eggermont AM. Ann Oncol 2012;23(suppl 8):viii53 viii57; 3. Hodi FS, et al. N Engl J Med 2010;363: ; 4. Kantoff PW, et al. N Engl J Med 2010;363: ; 5. Brahmer JR, et al. IASCL 15th WCLC 2013; Abs MO Hamid O, et al. N Eng J Med 2013;369:






22 Anti-CTLA-4 and anti-pd-1/pd-l1 mechanism of action Immune System T-cell activation Antigens Regulatory molecules (CTLA-4, PD-1)
23 The MDX study: randomized phase III, double blinded, three arms study which compared ipilimumab + gp100 vs ipilimumab + placebo vs gp100 + placebo N. 676 pretreated advanced melanoma patients were enrolled. Randomization was 3:1:1 and the primary endpoint was OS No separation in curves for the first 3 months Separation and survival impact occurs after 3 months (~ 4 months improvement in median OS Near doubling of 1 and 2 years when we start to see durable long-term survivors Median OS ipi + gp100 = 10,0 mos Ipi + placebo = 10,1 mos gp100 + placebo = 6,4 mos Hodi et al New Engl J Med 2010; 363:711-23
24 Pooled OS Analysis Including EAP Data: 4846 Patients 1.0 Proportion Alive Median OS, months (95% CI): 9.5 ( ) 3-year OS rate, % (95% CI): 21 (20 22) Ipilimumab CENSORED Months Patients at Risk Ipilimumab Schadendorf et al. JCO 2015
25 No effect in surrogate endpoints Best Overall Response Rate (BORR) ipi + gp100 = 5,7 % Ipi + placebo = 10,9 % gp100 + placebo = 1,5 % 08/03/ Hodi et al New Engl J Med 2010; 363:711-23


26 New response criteria about immunotherapy? Ribas A et al. Clin Cancer Res 2009;15(23):7116 8) 2009;15:
27 Example Response Patterns Change from baseline SPD (%) Change from baseline SPD (%) Response in baseline lesions PD PR Relative week from first dose date 'Stable disease' with slow, steady decline in total tumor volume 2,894 2,556 2,218 1,881 1,543 1, SPD (mm 2 ) 2,810 2,482 2,154 1,826 1,498 1, Total tumor volume Index lesions New lesions Ipilimumab dosing Relative week from first dose date SPD = Sum of the Product of the perpendicular Diameters (a measure of tumor volume) SPD (mm 2 ) Change from baseline SPD (%) Change from baseline SPD (%) Response after initial increase in total tumor volume 5.2 months 6 months CR 9 months Wolchok et al. Clin Cancer Res 2009;15(23): Relative week from first dose date 19,373 17,242 15,111 12,980 10,849 8,718 6,587 4,456 2, ,937 Response in index and new lesions At or after the appearance of new lesions months 1,272 1, Relative week from first dose date IPI SPD (mm 2 ) SPD (mm 2 ) 27
28 Immunotherapy: evolution of the antitumoral effect ipi ipi ipi ipi ipi ipi ipi Exposure to ipilimumab The T lymphocytes response beyond week 12 was not evaluated Activation of lymphocytes T Total volume of tumor * 25% 50% 100% Basal SD PR CR * Tumoral volume can include infiltrating lymphocytes and tumoral cells PD SD PR CR Models of response The activation and proliferation of the immune-system cells had early The measurable clinical effect occurs in variable times
29
30 Keynote 006: pembrolizumab vs ipilimumab OS Arm 1-yr rate (95% CI), mo HR (95% CI) P Pembro 10 Q2W 74,1% Pembro 10 Q3W 68,4% 0.63 ( ) 0.69 ( ) < < ipilimumab 58,2% Robert et al. NEJM 2015
31 Results from CA and Ca studies Unmet need in metastatic melanoma > 50% patients have BRAF wild-type tumor 1 Only ipilimumab has OS benefit in this group of patients 2,3 Nivolumab A fully human anti-pd-1 monoclonal antibody 4 with clinical benefit 5 8 Phase 1 Study 003 5,6 Phase 3 Study CheckMate-037 7,8 1-Year 2-Year 3-Year 4-Year Nivolumab 3 mg/kg Q2W Investigator s Choice of Chemotherapy OS 63% 48% 42% 32% ORR 32% 11% 1. Long et al. J Clin Oncol 2011; 2. Hodi et al. N Engl J Med 2010; 3. Robert et al. N Engl J Med 2011; 4. Wang et al. Cancer Immunol Res 2014; 5. McDermott et al. ESMO 2014; 6. Hodi et al. SMR 2014; 7. Weber et al. ESMO 2014; 8. D Angelo et al. SMR 2014.
32 Probability of Survival Overall Survival NIVO vs DTIC NIVO DTIC 46.3% 70.7% Months 26.7% 57.7% Number of Patients at Risk NIVO DTIC Median OS, mo (95% CI) NIVO (N = 210) NR (23.1, NR) DTIC (N = 208) 11.2 (9.6, 13.0) HR (95% CI) 0.43 (0.33, 0.57); P < CI = confidence interval, HR = hazard ratio; mo = month Median follow-up was 18.5 months for NIVO and 10.9 months for DTIC Database lock was on July 15,
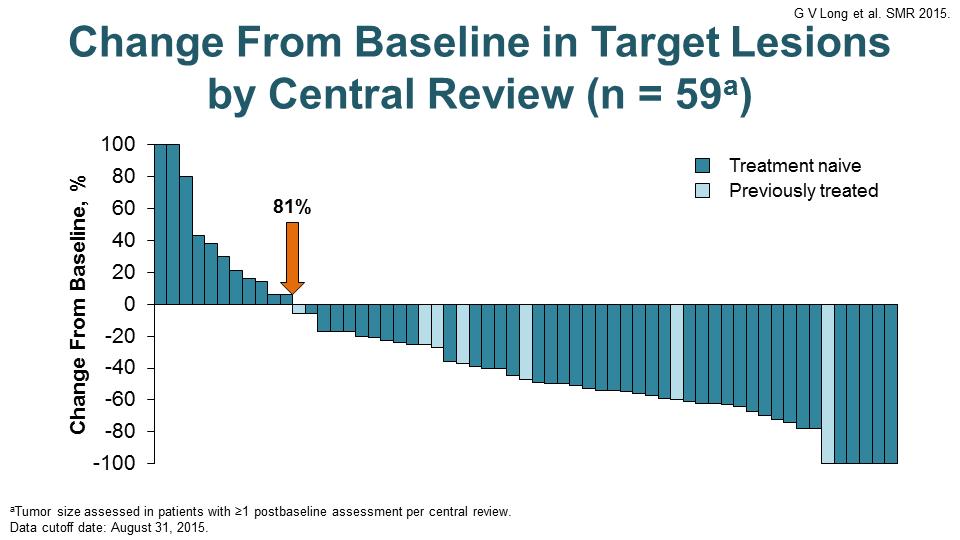
33 Ca : Objective Response by RECIST v1.1 Nivolumab ORR 40% (95% CI, 33 47%) Dacarbazine ORR 14% (95% CI, 10 19%) Maximum Change from Baseline in Target Lesion (%) Truncated to 100% Responder Truncated to 100% Responder -100 Patients -100 Patients Odds ratio for response 4.06 (95% CI, ; P < ) Showing only patients with both baseline and at least one post-baseline measurement of target lesion. Robert et al. N Engl J Med 2015 Jan 22;372(4):320-30
34 Progression-Free Survival NIVO vs DTIC Probability of PFS NIVO DTIC 7.7% 44.3% Number of Patients at Risk NIVO DTIC Months Median PFS, mo (95% CI) NIVO (N = 210) 5.4 (3.7, 12.2) DTIC (N = 208) 2.2 (2.1, 2.5) HR (95% CI) 0.42 (0.32, 0.53); P < NC 39.2% CI = confidence interval; HR = hazard ratio; mo = month; NC = not calculated 34
35 Time to and Durability of Response On Treatment Off Treatment First Tumor Response Ongoing Response NIVO DTIC Patients Patients Weeks NIVO DTIC Duration of response, median (range), mo NR 7.2 (3.9 NR) a At the time of the last follow-up mo = month; NR = not reached Weeks Ongoing response among responders a 73/90 (81%) 15/30 (50%) 35
 there was a 8% of patients who progressed according with RECIST v1.")
 For this reason, together the classical RECIST criteria, we must consider")


36 Unconventional responses in patients treated with nivolumab CA CA In both the two randomised phase III studies (CA and CA ) there was a 8% of patients who progressed according with RECIST v1.1 criteria, but achieved or maintained a 30% reduction in the target lesion tumour burden ( immune-related, unconventional response pattern ) For this reason, together the classical RECIST criteria, we must consider immuno-related criteria even for nivolumab treatment By permission of Weber J, Weber J et al. ESMO 2014 Congress; September 26-30, 2014; Madrid, Spain. Abstract LBA3. Weber J et al. Lancet Oncol 2015; 16:375-84, Reprinted from The Lancet, Copyright 2015, with permission from Elsevier. From Robert C et al. N Engl J Med 20145;372: Supplementary material. Copyright 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
37 Early Pseudoprogression (irrc, Central Review) Presented By Jedd Wolchok at 2015 ASCO Annual Meeting









38 Targeting CTLA-4 and PD-1 pathways Periphery Tumour microenvironment Activation (cytokines, lysis, proliferation, migration to tumour) MHC TCR TCR MHC Dendritic cell B7 CD28 B7 CTLA-4 Anti-CTLA T cell T cell PD-1 PD-L1 Anti-PD-1/PD-L1 PD-1 PD-L2 Tumour cell Anti-PD-1 CTLA-4 pathway PD-1 pathway Wolchock J, et al. JCO 2013 Volume 31, Issue 15_suppl ; abstr 9012^




39 Ipilimumab plus nivolumab - results from the three arms randomized phase 3 study in untreated advanced melanoma patients with ipilimumab/nivolumab or nivolumab alone vs ipilimumab alone (CA ): NIVO + IPI resulted in a longer PFS 39 Larkin J et al. N Engl J Med 2015;373:23-34
40 Candidate Predictive Biomarker: Tumor PD-L1 Expression

 0/17 PD-L1 Positive no. (%) 17/17 PD-L1(-) PD-L1 Negative no.")
 CR/PR 9 (36) 0 9 (21) Nonresponder 16* (64) 17 (100) 33 (79) All Patients 25 17 42 Topalian S, et al.")
41 Correlation of PD-L1 expression in pretreatment tumor biopsies with clinical outcomes 42 pts include 18 MEL, 10 NSCLC, 7 CRC, 5 RCC, and 2 CRPC. Proportion of patients *2 pts still under evaluation Association Between Pretreatment Tumor PD-L1 Expression and Clinical Response Response Status 9/25 16*/25 PD-L1(+) 0/17 PD-L1 Positive no. (%) 17/17 PD-L1(-) PD-L1 Negative no. (%) Total no. (%) CR/PR 9 (36) 0 9 (21) Nonresponder 16* (64) 17 (100) 33 (79) All Patients Topalian S, et al. NEJM 2012;366: PD-L1(+) PD-L1(-) p=0.006 analysis not pre-planned and based on subset of subjects'. * Melanoma RCC NSCLC
42 Tumor PD-L1 Expression as candidate predictive biomarker: response according to PD-L1 expression in NSCLC and melanoma Subsequent experiences showed that there is a 15-20% of patients PD-L1 negative who respond. Moreover, in the phase I study with the combination ipilimumab/nivolumab, the ORR was similar in both the groups (PD-L1 positive and negative). (Simeone et al. Melanoma Manag. 2015; 2:41 50) Tumour PDL1+ Positive ORR n/n (%) PDL1- Negative ORR n/n (%) MPDL3280A (Hamid ASCO 2013) Melanoma 4/15 (27) 3/15 (20) Nivolumab (Weber ASCO 2013) Melanoma 8/12 (67) 6/32 (19) Nivolumab (Grosso ASCO 2013) Melanoma 7/16 (44) 3/18 (17) Nivolumab (Topalian, N Engl J Med, 2012) NSCLC 9/25 (36) 0/17 (0) Nivolumab (Antonia, WCLC 2013) NSCLC 5/31 (16) 4/32 (13) Pembrolizumab (Garon, WCLC 2013) NSCLC 4/7 (57) 2/22 (9) MPDL3280A3 (Horn, WCLC 2013) NSCLC 8/26 (31) 4/20 (20) Nivolumab/ Ipilimumab (Callahan ASCO 2013) NSCLC 4/10 (40) 8/17 (47) Key questions Variability in tissue collection timing, cell sampling, types of assay, IHC criteria 08/03/ Antonia SJ, et al. Poster presentation at WCLC J Thorac Oncol 2013;8(Suppl 2):abstract: P ; 2. Garon EB, et al. Oral presentation at WCLC J Thorac Oncol 2013;8(Suppl 2):abstract: MO18.02; 3. Horn L, et al. Mini-Oral presentation at WCLC J Thorac Oncol. 2013;8(Suppl 2):abstract: MO Bottom table Presented by: Walter J. Urba, MD, PhD 42
43 OS by PD-L1 expression level (5%) NIVO 5% (N = 59) NIVO <5% (N = 127) DTIC 5% (N = 61) DTIC <5% (N = 116) 1.0 Median OS, mo (95% CI) NR (NR, NR) NR (16.6, NR) 1.0 Median OS, mo (95% CI) 9.7 (6.7, 13.5) 11.6 (9.3, 13.0) 0.9 HR (95% CI) a 0.56 (0.32, 0.98); P = HR (95% CI) a 1.16 (0.79, 1.68); P = % 0.8 Probability of Survival % 68.3% 54.2% Probability of Survival % 44.7% 28.9% % NIVO PD-L1 5% NIVO PD-L1 <5% DTIC PD-L1 5% DTIC PD-L1 <5% Months Months a Hazard ratios expressed as PD-L1 5% over PD-L1 <5% CI = confidence interval; HR = hazard ratio; mo = month; NR = not reached 43
44 Slide 13 Presented By Jedd Wolchok at 2015 ASCO Annual Meeting
45 PD-L1 as a potential biomarker: % of Pts PD-L1 positive in the different clinical trials Study Pts PDL1+ Positive (%) CA (Weber J et al. LO 2015) 49 CA (Robert C et al. NEJM 2014) 35 Ca (Larkin J et al. NEJM 2015) ipi/nivo arm 21,7 Ca (Larkin J et al. NEJM 2015) nivo arm 25,3 Keynote 006 (Robert C et al. NEJM 2015) pembro every 2 wks 80,6 Keynote 006 (Robert C et al. NEJM 2015) pembro every 3 wks 79,8 Keynote 002 (Puzanov I et al. ASCO 2015) 69 Keynote 001 (Daud A et al SMR 2014)) 77 Ascierto PA et al. J Trans Med 2015; 13:213
 100 80 60 40 20 0 20 40 60 3 mg/kg 1st occurrence of new lesion Change in target lesions from baseline (%) 200 100 80 60 40 20 0 20 40 60 First occurrence of new lesion 80 80 100 0 10 20 30 40 50")
46 Changes in Target Lesions: Comparing Nivolumab Alone and in Combination Nivolumab monotherapy Nivolumab + ipilimumab mg/kg nivolumab + 3 mg/kg ipilimumab Change in target lesions from baseline (%) mg/kg 1st occurrence of new lesion Change in target lesions from baseline (%) First occurrence of new lesion Weeks since treatment initiation Weeks since treatment initiation Horizontal line at 30% = threshold for defining objective response (partial tumour regression) in absence of new lesions or non-target disease according to RECIST Wolchok JD, et al. J Clin Oncol 2013;31(suppl): abstract 9012^; Sznol M, et al. J Clin Oncol 2013;31(suppl): abstract CRA9006^
47
48
49 Nivolumab monotherapy Changes in Target Lesions: Comparing Nivo/Ipi and Pembro/Epacadostat Nivolumab + ipilimumab mg/kg nivolumab + 3 mg/kg ipilimumab Change in target lesions from baseline (%) First occurrence of new lesion Weeks since treatment initiation Horizontal line at 30% = threshold for defining objective response (partial tumour regression) in absence of new lesions or non-target disease according to RECIST Wolchok JD, et al. J Clin Oncol 2013;31(suppl): abstract 9012^; Sznol M, et al. J Clin Oncol 2013;31(suppl): abstract CRA9006^ SMR, O. Hamid, November 21, 2015

50 Melanoma, Cancer Immunotherapy and Innovative Therapies Unit Istituto Nazionale Tumori Fondazione G. Pascale Chair Paolo A. Ascierto Medical Oncologists Ester Simeone Antonio M. Grimaldi Lucia Festino Dermatologists Fabrizio Ayala Rossella Di Trolio Marco Palla Luigi Scarpato Research Group Rosalba Camerlingo Mariaelena Capone Rosaria Falcone Federica Fratangelo Gabriele Madonna Domenico Mallardo Chiara Botti Study Coordinators/ Data Manager Susy Esposito Miriam Paone Marcello Curvietto Gianni Rinaldi Research Nurses Federica Huber Raffaella Furia Secretary s Office Mariarosaria Cecco Anna Riccio Via Mariano Semmola, 80131, Napoli, Italy Tel ; Fax p.ascierto@istitutotumori.na.it
New treatments in melanoma
 New treatments in melanoma Paolo A. Ascierto, MD Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy Meta-analysis of Phase II cooperative group trials in metastatic stage IV melanoma to determine
New treatments in melanoma Paolo A. Ascierto, MD Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy Meta-analysis of Phase II cooperative group trials in metastatic stage IV melanoma to determine
What we learned from immunotherapy in the past years
 What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
New Systemic Therapies in Advanced Melanoma
 New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
LA QUARTA ARMA CONTRO IL CANCRO
 LA QUARTA ARMA CONTRO IL CANCRO Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure Employment or
LA QUARTA ARMA CONTRO IL CANCRO Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure Employment or
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy. What every patient needs to know. James Larkin
 Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
MELANOMA METASTASICO: NUEVAS COMBINACIONES. Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona
 MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
Combination Approaches in Melanoma: A Balancing Act
 Combination Approaches in Melanoma: A Balancing Act Antoni Ribas, MD, PhD Jonsson Comprehensive Cancer Center University of California Los Angeles Los Angeles, California Advances in the Treatment of Metastatic
Combination Approaches in Melanoma: A Balancing Act Antoni Ribas, MD, PhD Jonsson Comprehensive Cancer Center University of California Los Angeles Los Angeles, California Advances in the Treatment of Metastatic
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology
 Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD
 Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Update on Immunotherapy in Advanced Melanoma. Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017
 Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
What s new in melanoma? Combination!
 DOI 10.1186/s12967-015-0582-1 EDITORIAL Open Access What s new in melanoma? Combination! Paolo A Ascierto 1*, Francesco M Marincola 2 and Michael B Atkins 3 Abstract Melanoma was again a focus of attention
DOI 10.1186/s12967-015-0582-1 EDITORIAL Open Access What s new in melanoma? Combination! Paolo A Ascierto 1*, Francesco M Marincola 2 and Michael B Atkins 3 Abstract Melanoma was again a focus of attention
New Therapeutic Approaches to Malignant Melanoma
 2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
Immunoterapia e melanoma maligno metastatico: siamo partiti da li. Vanna Chiarion Sileni Istituto Oncologico Veneto
 Immunoterapia e melanoma maligno metastatico: siamo partiti da li Vanna Chiarion Sileni Istituto Oncologico Veneto Vanna.chiarion@iov.veneto.it Metastatic Melanoma Available Treatment: 197 217 Zelboraf
Immunoterapia e melanoma maligno metastatico: siamo partiti da li Vanna Chiarion Sileni Istituto Oncologico Veneto Vanna.chiarion@iov.veneto.it Metastatic Melanoma Available Treatment: 197 217 Zelboraf
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Approaches To Treating Advanced Melanoma
 Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Melanoma Clinical Trials and Real World Experience
 Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico
 Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
Melanoma: Immune checkpoints
 ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
ImmunoScore/Immuneprofiling in Melanoma
 ImmunoScore/Immuneprofiling in Melanoma Gabriele Madonna Melanoma, Cancer Immunotherapy and Innovative Therapy Unit Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Tumor microenviroment
ImmunoScore/Immuneprofiling in Melanoma Gabriele Madonna Melanoma, Cancer Immunotherapy and Innovative Therapy Unit Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Tumor microenviroment
Treatment and management of advanced melanoma: Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC
 Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Checkpoint regulators a new class of cancer immunotherapeutics. Dr Oliver Klein Medical Oncologist ONJCC Austin Health
 Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Best Practices in the Treatment and Management of Metastatic Melanoma. Melanoma
 Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Immunotherapy for Metastatic Malignant Melanoma. Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
 Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy for Melanoma. Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France
 Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Outcomes of Patients With Metastatic Melanoma Treated With Immunotherapy Prior to or After BRAF Inhibitors
 Outcomes of Patients With Metastatic Melanoma Treated With Immunotherapy Prior to or After BRAF Inhibitors Allison Ackerman, MD, PhD 1 ; Oliver Klein, MD 2 ; David F. McDermott, MD 1 ; Wei Wang, PhD 3
Outcomes of Patients With Metastatic Melanoma Treated With Immunotherapy Prior to or After BRAF Inhibitors Allison Ackerman, MD, PhD 1 ; Oliver Klein, MD 2 ; David F. McDermott, MD 1 ; Wei Wang, PhD 3
MELANOMA: THE BEST OF THE YEAR Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone
 MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
ASCO 2014: The Future is Here. What I Will Talk About. George W. Sledge MD Stanford University School of Medicine
 ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
The Current Status of Immune Checkpoint Inhibitors: Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb
 The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
6/7/16. Melanoma. Updates on immune checkpoint therapies. Molecularly targeted therapies. FDA approval for talimogene laherparepvec (T- VEC)
") Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Immunotherapies in melanoma: regulatory perspective. Jorge Camarero (AEMPS)
") Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
Update on Targeted Therapy in Melanoma
 Update on Targeted Therapy in Melanoma Seville June 2013 James Larkin FRCP PhD London UK Overview What are the targets in melanoma? BRAF / KIT / NRAS / GNAQ / MEK DNA / microtubules CTLA4 / PD1 / PDL1
Update on Targeted Therapy in Melanoma Seville June 2013 James Larkin FRCP PhD London UK Overview What are the targets in melanoma? BRAF / KIT / NRAS / GNAQ / MEK DNA / microtubules CTLA4 / PD1 / PDL1
Largos Supervivientes, Tenemos datos?
 Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Ipilimumab ASCO Data Review and Discussion Webcast. Monday, June 2, 2008
 Ipilimumab ASCO Data Review and Discussion Webcast Monday, June 2, 2008 Slide 2 Forward Looking Statements Except for historical information, the matters contained in this slide presentation may constitute
Ipilimumab ASCO Data Review and Discussion Webcast Monday, June 2, 2008 Slide 2 Forward Looking Statements Except for historical information, the matters contained in this slide presentation may constitute
The Really Important Questions Current Immunotherapy Trials are Not Answering
 The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
Beyond BRAFi/MEKi: Combination and Sequencing Approaches for in Patients with Metastatic BRAF V600 Mutant Melanoma:
 Beyond BRAFi/MEKi: Combination and Sequencing Approaches for in Patients with Metastatic BRAF V600 Mutant Melanoma: Michael B. Atkins, M.D. Deputy Director Georgetown-Lombardi Comprehensive Cancer Center
Beyond BRAFi/MEKi: Combination and Sequencing Approaches for in Patients with Metastatic BRAF V600 Mutant Melanoma: Michael B. Atkins, M.D. Deputy Director Georgetown-Lombardi Comprehensive Cancer Center
The Immunotherapy of Oncology
 The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3
 ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
A Case Study: Ipilimumab in Pre-treated Metastatic Melanoma
 A Case Study: Ipilimumab in Pre-treated Metastatic Melanoma Tai-Tsang Chen, PhD Global Biometric Sciences, Bristol-Myers Squibb EFSPI Statistical Meeting on Evidence Synthesis Brussels, Belgium November
A Case Study: Ipilimumab in Pre-treated Metastatic Melanoma Tai-Tsang Chen, PhD Global Biometric Sciences, Bristol-Myers Squibb EFSPI Statistical Meeting on Evidence Synthesis Brussels, Belgium November
Immunotherapy for Melanoma. Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center
 Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Melanoma- Fighting the Dark Side
 Melanoma- Fighting the Dark Side Anna C. Pavlick, BSN, MSc, DO, MBA Professor of Medicine and Dermatology Director, NYU Melanoma Program Director, NYU Clinical Trials Office NYU Perlmutter Cancer Center
Melanoma- Fighting the Dark Side Anna C. Pavlick, BSN, MSc, DO, MBA Professor of Medicine and Dermatology Director, NYU Melanoma Program Director, NYU Clinical Trials Office NYU Perlmutter Cancer Center
Histology independent indications in oncology. The BRAF Story. Yibing Yan PhD Roche / Genentech
 Histology independent indications in oncology The BRAF Story Yibing Yan PhD Roche / Genentech 1 Introduction the discovery Case study in BRAF mutant melanoma heterogeneity within the tumour variability
Histology independent indications in oncology The BRAF Story Yibing Yan PhD Roche / Genentech 1 Introduction the discovery Case study in BRAF mutant melanoma heterogeneity within the tumour variability
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
WHY LOOK FOR ADDITIONAL DATA TO ENRICH THE KAPLAN-MEIER CURVES? Immuno-oncology, only an example
 WHY LOOK FOR ADDITIONAL DATA TO ENRICH THE KAPLAN-MEIER CURVES? Immuno-oncology, only an example YIDOU ZHANG Health Economics and Payer Analytics Director Oncology Payer Evidence and Pricing, AstraZeneca
WHY LOOK FOR ADDITIONAL DATA TO ENRICH THE KAPLAN-MEIER CURVES? Immuno-oncology, only an example YIDOU ZHANG Health Economics and Payer Analytics Director Oncology Payer Evidence and Pricing, AstraZeneca
Priming the Immune System to Kill Cancer and Reverse Tolerance. Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics
 Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Treatment of Tumors Resistant to PD-1 inhibitors
 Treatment of Tumors Resistant to PD-1 inhibitors Harriet Kluger, MD Professor of Medicine (Medical Oncology), Yale School of Medicine Deputy Section Chief, Medical Oncology Associate Cancer Center Director
Treatment of Tumors Resistant to PD-1 inhibitors Harriet Kluger, MD Professor of Medicine (Medical Oncology), Yale School of Medicine Deputy Section Chief, Medical Oncology Associate Cancer Center Director
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma
 Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
Review of immunotherapy in melanoma
 Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Array BioPharma Jefferies 2016 Global Healthcare Conference. June 9, 2016
 Array BioPharma Jefferies 216 Global Healthcare Conference June 9, 216 Safe Harbor Statement 2 Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
Array BioPharma Jefferies 216 Global Healthcare Conference June 9, 216 Safe Harbor Statement 2 Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma
 With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma") Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Targeted Therapies in Melanoma
 Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Overall Survival in COLUMBUS: A Phase 3 Trial of Encorafenib (ENCO) Plus Binimetinib (BINI) vs Vemurafenib (VEM) or ENCO in BRAF-Mutant Melanoma
 Plus Binimetinib (BINI) vs Vemurafenib (VEM) or ENCO in BRAF-Mutant Melanoma") Overall Survival in COLUMBUS: A Phase 3 Trial of Encorafenib (ENCO) Plus Binimetinib (BINI) vs Vemurafenib () or ENCO in BRAF-Mutant Melanoma, Paolo A. Ascierto, Helen J. Gogas, Ana Arance, Mario Mandala,
Overall Survival in COLUMBUS: A Phase 3 Trial of Encorafenib (ENCO) Plus Binimetinib (BINI) vs Vemurafenib () or ENCO in BRAF-Mutant Melanoma, Paolo A. Ascierto, Helen J. Gogas, Ana Arance, Mario Mandala,
News from ASCO. Niven Mehra, Medical Oncologist. Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital
 News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
Unmet Need Mucosal and Uveal Melanoma
 Unmet Need Mucosal and Uveal Melanoma Matteo Carlino Crown Princess Mary Cancer Centre Westmead and Blacktown Hospitals Melanoma Institute Australia The University of Sydney. Cutaneous Overall Survival
Unmet Need Mucosal and Uveal Melanoma Matteo Carlino Crown Princess Mary Cancer Centre Westmead and Blacktown Hospitals Melanoma Institute Australia The University of Sydney. Cutaneous Overall Survival
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes. Disclosures
 Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Immuno-Oncology Applications
 Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento
 tra la prima e la seconda linea di trattamento") Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Cancer Progress. The State of Play in Immuno-Oncology
 Cancer Progress The State of Play in Immuno-Oncology Axel Hoos, MD, PhD VP, Oncology R&D, Glaxo Smith Kline Co-Director, Cancer Immunotherapy Consortium Key Drivers in Immuno-Oncology Science Methods Combinations
Cancer Progress The State of Play in Immuno-Oncology Axel Hoos, MD, PhD VP, Oncology R&D, Glaxo Smith Kline Co-Director, Cancer Immunotherapy Consortium Key Drivers in Immuno-Oncology Science Methods Combinations
Melanoma in Focus: Update on Novel Therapy, Emerging Agents, and Optimizing Patient Care Presentation 1
 Presentation 1 The following is a transcript from a web-based CME -certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational
Presentation 1 The following is a transcript from a web-based CME -certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational
Weitere Kombinationspartner der Immunotherapie
 1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER. Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium
 THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
ASCO / COLUMBUS ENCORE PRESENTATION June 4, 2018
 ASCO / COLUMBUS ENCORE PRESENTATION June 4, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions of the Private
ASCO / COLUMBUS ENCORE PRESENTATION June 4, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions of the Private
Evan J. Lipson, M.D.
 Update on treatment for Merkel cell, cutaneous squamous cell and basal cell cancers Evan J. Lipson, M.D. The Johns Hopkins University School of Medicine Bloomberg~Kimmel Institute for Cancer Immunotherapy
Update on treatment for Merkel cell, cutaneous squamous cell and basal cell cancers Evan J. Lipson, M.D. The Johns Hopkins University School of Medicine Bloomberg~Kimmel Institute for Cancer Immunotherapy
The changing landscape of medical management of stage III and IV melanoma Current treatments and what s on the horizon
 The changing landscape of medical management of stage III and IV melanoma Current treatments and what s on the horizon Samantha Bowyer Medical Oncologist Rockingham General Hospital Historical perspective
The changing landscape of medical management of stage III and IV melanoma Current treatments and what s on the horizon Samantha Bowyer Medical Oncologist Rockingham General Hospital Historical perspective
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Overview: Immunotherapy in CNS Metastases
 Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Appendices. Appendix A Search terms
 Appendices Appendix A Search terms Database Search terms Medline 1. Ipilimumab; 2. MDX-010; 3. MDX-101; 4. Yervoy; 5. BMS-734016; 6. Nivolumab; 7. ONO-4538; 8. BMS-936558; 9. MDX-1106; 10. Opdivo; 11.
Appendices Appendix A Search terms Database Search terms Medline 1. Ipilimumab; 2. MDX-010; 3. MDX-101; 4. Yervoy; 5. BMS-734016; 6. Nivolumab; 7. ONO-4538; 8. BMS-936558; 9. MDX-1106; 10. Opdivo; 11.
Principles and Application of Immunotherapy for Cancer: Advanced NSCLC
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
Role of the Pathologist in Guiding Immuno-oncological Therapies. Scott Rodig MD, PhD
 Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Nivolumab in Hodgkin Lymphoma
 Nivolumab in Hodgkin Lymphoma Stephen M. Ansell, MD, PhD Professor of Medicine Chair, Lymphoma Group Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers Squibb Celldex Therapeutics Seattle
Nivolumab in Hodgkin Lymphoma Stephen M. Ansell, MD, PhD Professor of Medicine Chair, Lymphoma Group Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers Squibb Celldex Therapeutics Seattle
Challenges in Distinguishing Clinical Signals to Support Development Decisions: Case Studies
 Challenges in Distinguishing Clinical Signals to Support Development Decisions: Case Studies David Feltquate MD, PhD Head of Early Clinical Development, Oncology Bristol-Myers Squibb, Princeton, NJ Challenges
Challenges in Distinguishing Clinical Signals to Support Development Decisions: Case Studies David Feltquate MD, PhD Head of Early Clinical Development, Oncology Bristol-Myers Squibb, Princeton, NJ Challenges
Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy
 New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology
New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology
Toxicity from Checkpoint Inhibitors. James Larkin FRCP PhD
 Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Melanoma, o status da imunoterapia e o futuro próximo
 III International Symposium on Immuno-Oncology Saturday, October 7 th 9:3 1: am Melanoma, o status da imunoterapia e o futuro próximo Antoni Ribas, M.D., Ph.D. Professor of Medicine, Surgery, Molecular
III International Symposium on Immuno-Oncology Saturday, October 7 th 9:3 1: am Melanoma, o status da imunoterapia e o futuro próximo Antoni Ribas, M.D., Ph.D. Professor of Medicine, Surgery, Molecular
Immunotherapy for Renal Cell Carcinoma. James Larkin
 Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Innovations in Immunotherapy - Melanoma. Systemic Therapies October 27, 2018 Charles L. Bane, MD
 Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
Basic Principles of Tumor Immunotherapy. Ryan J. Sullivan, M.D. Massachusetts General Hospital Cancer Center Boston, MA
 Basic Principles of Tumor Immunotherapy Ryan J. Sullivan, M.D. Massachusetts General Hospital Cancer Center Boston, MA Disclosures Consulting Fees: Biodesix, Novartis Pharmaceuticals Other: Boehringer
Basic Principles of Tumor Immunotherapy Ryan J. Sullivan, M.D. Massachusetts General Hospital Cancer Center Boston, MA Disclosures Consulting Fees: Biodesix, Novartis Pharmaceuticals Other: Boehringer
Breakthrough and Landscape of Acral and Mucosal Melanomas. Jun Guo. M.D., Ph.D Peking University Cancer Hospital & Institute
 Breakthrough and Landscape of Acral and Mucosal Melanomas Jun Guo. M.D., Ph.D Peking University Cancer Hospital & Institute Current status of advanced melanoma Current status of advanced MM Targeted therapy
Breakthrough and Landscape of Acral and Mucosal Melanomas Jun Guo. M.D., Ph.D Peking University Cancer Hospital & Institute Current status of advanced melanoma Current status of advanced MM Targeted therapy
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Checkpoint-Inhibitoren beim Lungenkarzinom. Dr. Helge Bischoff Thoraxklinik Heidelberg
 Checkpoint-Inhibitoren beim Lungenkarzinom Dr. Helge Bischoff Thoraxklinik Heidelberg Survival (%) First-Line: Polychemotherapy vs 9387 patients 778 patients in studies with platinum chemotherapy 1-year
Checkpoint-Inhibitoren beim Lungenkarzinom Dr. Helge Bischoff Thoraxklinik Heidelberg Survival (%) First-Line: Polychemotherapy vs 9387 patients 778 patients in studies with platinum chemotherapy 1-year
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal (STA) Dabrafenib for treating unresectable, advanced or metastatic
 Dabrafenib for treating unresectable, advanced or metastatic") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal (STA) Dabrafenib for treating unresectable, advanced or metastatic BRAF V600 mutation-positive melanoma mutation-positive melanoma
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal (STA) Dabrafenib for treating unresectable, advanced or metastatic BRAF V600 mutation-positive melanoma mutation-positive melanoma
Releasing the Brakes on Tumor Immunity: Immune Checkpoint Blockade Strategies
 Releasing the Brakes on Tumor Immunity: Immune Checkpoint Blockade Strategies Jason Muhitch, PhD MIR 509 October 1 st, 2014 Email: jason.muhitch@roswellpark.org 0 Holy Grail of Tumor Immunity Exquisite
Releasing the Brakes on Tumor Immunity: Immune Checkpoint Blockade Strategies Jason Muhitch, PhD MIR 509 October 1 st, 2014 Email: jason.muhitch@roswellpark.org 0 Holy Grail of Tumor Immunity Exquisite
Principles and Application of Immunotherapy for Cancer: Advanced Melanoma
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced Melanoma This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced Melanoma This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
Cutaneous melanoma: new developments for 2018
 Cutaneous melanoma: new developments for 2018 and beyond KIM MARGOLIN, M.D., FASCO CITY OF HOPE MEDICAL ONCOLOGY CORONADO, CALIFORNIA SEPTEMBER 20, 2018 DISCLOSURE Consultant for ImaginAb, Nektar Therapeutics,
Cutaneous melanoma: new developments for 2018 and beyond KIM MARGOLIN, M.D., FASCO CITY OF HOPE MEDICAL ONCOLOGY CORONADO, CALIFORNIA SEPTEMBER 20, 2018 DISCLOSURE Consultant for ImaginAb, Nektar Therapeutics,