Immunotherapy in GI cancers
|
|
|
- Kristina Morris
- 6 years ago
- Views:
Transcription


1 Immunotherapy in GI cancers Julien TAIEB Sorbonne Paris Cité Hopital Européen Georges Pompidou Inserm U97 J Taieb ESDO Leuven 217
2 How to progress in GI cancer treatment Better define subgroups With different prognostic and different treatments Find predictive markers for precision medecine Combine different targeted agents in accordance with the molecular profile of the patients tumor Induce an efficient immune response from the host against the tumor J Taieb ESDO Leuven 217


3 Immunité innée et adaptative Innée : - Rapide - Non spécifique Adaptative : - Plus lente - Spécifique





4 Immunité anti-tumorale Lyse antigens Immature DC mature DC TUMOR Peptide / MHC I Peptide / MHC II CD8 + T Lymphocyte CD4 + T Lymphocyte Terme, Taieb et al. Immunooncology 214
5 Major immunotherapeutic approaches Adoptive transfer Anti-cancer vaccines Checkpoint blockade J Taieb ESDO Leuven 217



6 Anti-CEA T cell transfer CEA decrease (maximum decline 74 99% vs baseline) Radiological response Inflammatory colitis 1. Parkhurst MR, et al. Mol Ther 211;19: J Taieb ESDO Leuven 217
7 Immune check points Mellman I et al., Science, 211 J Taieb ESDO Leuven 217
8 Immune check points Activate The activators Inhibit The inhibitors Mellman I et al., Science, 211 J Taieb ESDO Leuven 217

9 Immune check points. T cell regulation T cell function Pardoll DM et al., Nat Rev Cancer, 212 J Taieb ESDO Leuven 217
10 In 217, Efficacy in phase III Anti-CTLA4 (Ipilimumab, tremelumumab) Anti-PD(L)1 (Nivolumab, Pembro, Atezolizumab, avelumab, darvalumab ) Melanoma M+ (L1, L2) Adjuvant (st III) Ovarian 15% TNBC 2% Mel 3-4% NSCLC 15-2% SCLC 15% Melanoma M+ (L1, L2) Nivo +Ipili +++ Melanoma M+ and Lung M+ (L1 & L2) Lung M+ (L2) Nivo/Atezolizumab Kidney M+ (L2) Nivolumab Squamous Cell Cancer of the Head and Neck (L2). Nivolumab MSI High CRC 6% PD1/PD-L1 Blockade reported ORR RCC 15-2% Hodgkin 65-85% HCC 2% Gastric 2% HNSCC 15-25% Bladder 25% Bladder (phase 2: Atezolizumab)
11 Colon cancer
12 Change From Baseline in Tumor Size, % 1 Melanoma 1 1 NSCLC 2 1 H&N3 Urothelial 4 TNBC Gastric 6 1 chl NHL PMBCL 8 Mesothelioma Ovarian 1 1 SCLC 11 1 Esophageal 12 1 NPC 13 1 Anal Biliary Tract 15 1 Colorectal 16 1 ER + /HER2 BC 17 Cervical 18 Thyroid 19 Salivary

13 J Taieb ESDO Leuven 217
 Radiographic responses* OS in CRC Immune-related ORR in mismatch-repair deficient vs proficient CRC: 4% vs % Adjusted OS HR for mismatch-repair deficient vs")
14 Checkpoint blockers Efficacy signal in MSI-H colorectal cancer Treatment with pembrolizumab (anti-pd-1 antibody) (n=11 mismatch repair-deficient CRC, n=21 mismatch-repair proficient CRC, n=9 mismatch-repair deficient non-crc) Radiographic responses* OS in CRC Immune-related ORR in mismatch-repair deficient vs proficient CRC: 4% vs % Adjusted OS HR for mismatch-repair deficient vs proficient CRC:.18, P =.5 *RECIST-based radiographic response **Adjusted for elapsed time since the initial diagnosis Le DT, et al. N Engl J Med. 215;372(26): J Taieb ESDO Leuven 217

15 Response to Pembrolizumab for MSI-H/dMMR 11 patients achieved a CR and were taken off therapy after 2 years of treatment. No evidence of cancer PD has been observed in those patients with a median time off therapy of 8.3 months. Le DT, Science 217
16 Pembrolizumab for MSI-H/dMMR CRC and Non-CRC Best response MSI-H CRC N = 61 a MSI-H Non-CRC N = 77 b n % (95% CI) n % (95% CI) ORR (95% CI), % 17 28% (17-41) 29 38% (27-49) Complete response 2 3% (-9) Partial response 17 28% (17-41) 27 35% (25-47) Stable disease 14 23% (13-36) 16 21% (12-32) Progressive disease 28 46% (33-59) 24 31% (21-43) DCR (CR+PR+SD) 31 51% (38-64) 45 58% (47-7) Median duration of response (range), months c Not reached (2.9+ to 12.5+) Not reached (2.4+ to 9.2+) Median time to response (range), months 4. (2-1) 2.1 (1-4) Diaz LA, ASCO 217, J Clin Oncol 35l(suppl 15), 3618 J Taieb ESDO Leuven 217
17 ASCO update Keynote 16 Tolerability : Rash prurit 25% Diarrhea/Colitis 11% Arthralgia 15% Thyroïditis/Hypothyroïdia 11%, Fatigue 9% grade 3-4 toxicities : 14% including pancreatitis 4% and diarrhea /colitis / thrombocytopenia / leucopenia /anemia in 2% each Efficacy : MSI : RR 28% with 11%CR ; DCR 51% MSS : RR % ; DCR 16% KEYNOTE 164 is ongoing in MSI-H (phase II, 12 pretreated pts) Le DT et al., ASCO 216, CSS 13 J Taieb ESDO Leuven 217
18 May 23, 217 FDA GRANTS ACCELERATED APPROVAL TO PEMBROLIZUMAB FOR FIRST TISSUE/SITE-AGNOSTIC INDICATION Adult and pediatric patients with unresectable or metastatic, MSI-H or dmmr solid tumors that have progressed following prior treatment and who have no satisfactory alternative treatment options or with MSI-H or dmmr colorectal cancer that has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan Non MSI GI cancer will be treatable by anti-pd1 in the future => MSI testing has to be performed in daily practice J Taieb ESDO Leuven 217
19 Phase 2 CheckMate 142 Study Design: MSI-H Cohort MSI-H mstage 1 Responses a mstage 2 7/19 Nivo 3 mg/kg (Q2W) Second-line colon MSI-H 1 prior treatment for metastatic disease 1 target lesion ECOG PS of -1 Nivo 3 mg/kg (Q2W) Responses a 3 6/19 cstage 1 Nivo 3 mg/kg + Ipi 1 mg/kg (Q3W x 4 doses) Then Nivo 3 mg/kg (Q2W) Responses a 7/19 cstage 2 b Nivo 3 mg/kg + Ipi 1 mg/kg (Q3W x 4 doses) Then Nivo 3 mg/kg (Q2W) a In patients with centrally confirmed MSI-H status b Currently enrolling cstage 1 = combination therapy stage 1; cstage 2 = combination therapy stage 2; Ipi = ipilimumab; mstage 1 = monotherapy stage 1; mstage 2 = monotherapy stage 2; Nivo = nivolumab; Q2W = every 2 weeks; Q3W = every 3 weeks 19 J Taieb ESDO Leuven 217
20
21 Patient Demographics and Disease Characteristics Overman M, Lancet Oncol 217

22 Overall Response and Disease Control CheckMate 142 Nivolumab alone Median time to response is 2,8 (1,4-3,2) Only 3 patients with ORR experiencing progression Median duration of response are not yet reached and are responder are alive at the time of analysis Overman M, Lancet Oncol 217
 months Median DOR: not reached 85% (39/46) of responses ongoing Tt discontinuations 38 pts( 51%) : 27 (36%) for PD 6 (8%)")
23 Changes in Tumor Burden CheckMate 142 Nivolumab alone Median TTR: 2.8 ( ) months Median DOR: not reached 85% (39/46) of responses ongoing Tt discontinuations 38 pts( 51%) : 27 (36%) for PD 6 (8%) Toxicity 5 (7%) other Overman M, Lancet Oncol 217
24 Progression-Free Survival Median PFS, mo 14,3 months PFS rate, % (95% CI) 12 months 5 % (38, 61) CheckMate 142 Nivolumab alone Overall Survival Median OS, mo (95% CI) OS rate, % (95% CI) NR (18, NE) 12 months 73% (62, 82) 36 investigator assessed PD 23 death/74 patients Median Follow up 12 months Overman M, Lancet Oncol 217

25 Investigator-assessed ORR and disease control (n=74) CheckMate 142 Nivolumab alone Overman M, Lancet Oncol 217
26 Safety Summary CheckMate 142 Nivolumab alone dmmr/msi-h per Local Assessment (N = 74) a Patients, n (%) Grade 1 or 2 Grade 3 or 4 Any Event 36 (49%) 15 (21%) TRAE reported in 1% of patients Fatigue Diarrhea Pruritus Hypothyroidism Lipase increased Rash Colitis Adrenal insufficiency Increase ASAT/ALAT 16 (22.%) 15 (2%) 1 (14%) 7 (1%) 3 (4%) 8 (11%) 5 (7%) 1 (1%) 1 (1%) 6 (8%) 1 (1%) 1(%) 1 (1%). Overman M, Lancet Oncol 217
27 Conclusions CheckMate 142: nivolumab alone Nivolumab monotherapy provided durable responses and disease control in patients with dmmr/msi-h CRC Responses and disease control were observed regardless of tumor PD-L1 expression, BRAF or KRAS mutation status, or a clinical history of Lynch syndrome Patient-reported outcome analyses showed clinically meaningful improvements in functioning, symptoms, and QOL Patients who continued treatment for 19 weeks attained a level of health that would be considered as equal to or exceeding the general health of many populations Nivolumab was well tolerated with no new safety signals observed These results suggest that nivolumab could be considered a new standard of care for patients with dmmr/msi-h CRC and warrants further investigation in patients with other dmmr/msi-h tumors Overman M, Lancet Oncol 217
28 FDA grants nivolumab accelerated approval for MSI-H or dmmr colorectal cancer On July 31, 217, the U.S. Food and Drug Administration granted accelerated approval to nivolumab (OPDIVO, Bristol-Myers Squibb Company) for the treatment of patients 12 years and older with mismatch repair deficient (dmmr) and microsatellite instability high (MSI-H) metastatic colorectal cancer that has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan. The approval was based on data from Study CA29142 (CHECKMATE 142; NCT 26188)
29 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer (mcrc): CheckMate 142 Study André T et al; ASCO 217; abst 3531
30 Study Design: CheckMate 142 Study Patients Stage 1 Stage 2 Histologically confirmed metastatic/ recurrent CRC MONOTHERAPY ARM NIVO 3 mg/kg Q2W If 7/19 confirmed responders, continue enrollment NIVO 3 mg/kg Q2W n = 74 pts dmmr/msi-h per local laboratory 1 prior line of therapy COMBINATION ARM NIVO 3 mg/kg + IPI 1 mg/kg Q3W (4 doses and then NIVO 3 mg/kg Q2W) If 7/19 confirmed responders, continue enrollment NIVO 3 mg/kg + IPI 1 mg/kg Q3W (4 doses and then NIVO 3 mg/kg Q2W) n = 84 pts Primary endpoint: ORR per investigator assessment (RECIST v1.1) Current analysis included all patients (n=84) who received their first dose 6 months prior to the data cut-off Median (range) time from first dose to data cut-off: 8.6 ( ) months André T et al; ASCO 217, Abst 3531
31 Patient Demographics and Disease Characteristics CheckMate 142 Study: nivolumab + ipilimumab Age Median (range), years < 65 years, n (%) ECOG performance status, n (%) 1 dmmr/msi-h (n = 84) 57 (21-81) 61 (73) 31 (37) 53 (63) Mutation status, n (%) BRAF/KRAS wild type BRAF mutated KRAS mutated Prior lines of therapy, n (%) (26) 21 (25) 3 (36) 1 (1) 17 (2) 31 (37) 23 (27) 12(14) Prior radiotherapy, n (%) 17 (2) André T et al; ASCO 217, Abst 3531
32 Overall Response and Disease Control: CheckMate 142 Study: nivolumab + ipilimumab ORR, n (%) [95% CI] Best overall response, n (%) CR PR SD PD ND/reported NIVO + IPI (n = 84) Investigator- Assessed 46 (55) [43.5, 65.7] 2 (2) 44 (52) 26 (31) 9 (11) 3 (4) NIVO Monotherapy 1 (n = 74) Investigator-Assessed 23 (31) [2.8, 42.9] 23 (31) 29 (39) 18 (24) 4 (5) Disease control for 12 weeks, n (%) a 66 (79) 51 (69) a Patients with CR, PR, or SD for 12 weeks André T et al; ASCO 217, Abst 3531 Overman M, Lancet Oncol 217
33 Best Reduction From Baseline in Target Lesion (%) Best Reduction From Baseline in Target Lesion (%) Best Change in Target Lesion Size NIVO + IPI (n = 84) NIVO Monotherapy 1 (n = 74) 8% of patients had reduction in tumor burden from baseline 62% of patients had reduction in tumor burden from baseline Confirmed CR or PR per investigator % Change truncated at 1 André T et al; ASCO 217, Abst 3531 Overman M, Lancet Oncol 217-1
34 Best reduction from baseline in target lesion (%) Results Figure 2. Association of best reduction in target lesion size (B) BRAF and KRAS mutation status in patients with dmmr/msi-h mcrc treated with NIVO + IPI B KRAS/BRAF wild type BRAF mutation KRAS mutation Unknown 34
35 Best reduction from baseline in target lesion (%) Results Figure 2. Association of best reduction in target lesion size with (C) Lynch syndrome in patients with dmmr/msi-h mcrc treated with NIVO + IPI C Lynch syndrome (Yes) Lynch syndrome (No) Unknown 35
36 Change in target lesion from baseline, (%) Changes in Tumor Burden CheckMate 142 Study: nivolumab + ipilimumab Median TTR: 2.8 ( ) months Median DOR: not reached 85% (39/46) of responses ongoing On treatment CR or PR 1 st occurrence of new lesion Time since start of treatment (week) André T et al; ASCO 217, Abst 3531 Overman M, Lancet Oncol 217
37 Probability of Progression-Free Survival Progression-Free Survival CheckMate 142 Study: nivolumab + ipilimumab Median PFS, mo (95% CI) NR (11.5, NE) PFS rate, % (95% CI) 6 months 77 (66.5, 85.1) 9 months 77 (66.5, 85.1) Time (months) No. at Risk NE = not estimable; NR = not reached André T et al; ASCO 217, Abst 3531
38 Probability of Survival Overall Survival CheckMate 142 Study: nivolumab + ipilimumab Median OS, mo (95% CI) NR (NE, NE) OS rate, % (95% CI) 6 months 89 (8.2, 94.2) 9 months 88 (78.1, 93.1) Time (months) No. at Risk NE = not estimable; NR = not reached André T et al; ASCO 217, Abst 3531
39 Event, n (%) Checkmate 142 Treatment-Related Adverse Events in 15% of Patients With MSI-H Nivolumab 3 mg/kg (n = 7) Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg (n = 3) Any grade Grade 3 4 Any grade Grade 3 4 Any event 41 (58.6) a 1 (14.3) 25 (83.3) 8 (26.7) Fatigue 13 (18.6) 1 (1.4) 6 (2.) Diarrhea 1 (14.3) 1 (1.4) 13 (43.3) Pruritus 8 (11.4) 5 (16.7) 1 (3.3) Nausea 5 (7.1) 6 (2.) Pyrexia 3 (4.3) 7 (23.3) Any event leading to discontinuation 4 (5.7) 2 (2.9) 4 (13.3) 4 (13.3) a One Grade 5 event of sudden death J Taieb ESDO Leuven
40 Safety Check Mate 142 Study: nivolumab + ipilimumab No treatment-related deaths were reported NIVO + IPI (n = 84) Patients, n (%) Any Grade Grade 3 or 4 Any TRAE 57 (68) 24 (29) Serious TRAEs 15 (18) 14 (17) Discontinuation due to TRAEs 11 (13) 8 (9) TRAEs reported in 1% of patients Diarrhea 2 (24) 1 (1) Fatigue 14 (17) 1 (1) Aspartate aminotransferase increase 14 (17) 8 (9) Pyrexia 13 (16) Pruritus 13 (16) 2 (2) Alanine aminotransferase increase 12 (14) 7 (8) Nausea 12 (14) Hyperthyroidism 11 (13) Hypothyroidism 11 (13) André T et al; ASCO 217, Abst 3531
41 Conclusions Check Mate 142 Study: nivolumab + ipilimumab NIVO + IPI provided durable responses, sustained disease control, and encouraging survival data in pretreated patients with dmmr/msi-h mcrc ORR of 55%, with 79% of patients achieving disease control for 12 weeks 85% of responses ongoing, and the median DOR was not yet reached 88% of patients alive at 9 months, 77% without progression NIVO + IPI demonstrated a manageable safety profile; 29% of patients had grade 3/4 TRAEs This trial is ongoing and patients will continue to be followed for survival 41 patients in this study were treated in St Antoine hospital and translational research are planned (we have primary and metastatic tissue for all) A French study will began in Septempter 217 (GERCOR group) with nivolumab and ipilumumab (55 patients) in the same population and we will collect archival tissue for all patients
42 dmmr/ MSI-H COL-11 Reproduced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) for Colon Cancer V National Comprehensive Cancer Network, Inc. All rights reserved. The NCCN Guidelines and illustrations herein may not be reproduced in any form for any purpose without the express written permission of NCCN. To view the most recent and complete version of the NCCN Guidelines, go online to NCCN.org. The NCCN Guidelines are a work in progress that may be refined as often as new significant data becomes available. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
43 Summary of Efficacy in Patients With MSS Nivolumab ± Ipilimumab in Metastatic CRC Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg (n = 1) Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg (n = 1) ORR, n (%) 1 (1) Median PFS, mo (95% CI) 2.28 (.62, 4.4) 1.31 (.89, 1.71) Median OS, mo (95% CI) (.62, NE) 3.73 (1.22, 5.62) vs NR OS and 14 PFS in MSI-H pts treated with nivolumab alone vs median not reached in MSI-H pts treated with the combo NE = not estimable 43
44 Change in sum of longest diameters from baseline, % Phase Ib: Atezolizumab + cobimetinib in MSS pretreated mcrc Tolerability : No DLT, Diarrhea : 7%, rash: 4%, Fatigue : 52% Grade 3-4 toxicities : 34% incl. diarrhea : 9% Efficacy : Response 17% (4 OR, 5 SD) : 3 MSS/1 statut MSI ukn, 4 to 7 mo Tumor Biopsy : no correlation with PDL1 at D Time on study (mo) PD SD PR/CR Discontinued atazolizumab New lesion Bendell JVC. et al., ASCO 216, OS 352
45 Conclusion Trials are ongoing in mcrc and in the adjuvant setting (soon) Colon cancer probably less easy than others MSI-H tumors : a good target Others may be: PolE, PolD, MSS with immune infiltrates Combination with targeted agents: + chemotherapy, sequence? + radiotherapy? + targeted agents: anti-angiogenics; MEK? J Taieb ESDO Leuven 217
46 After ASCO: even more trials for colorectal cancer Anti-CTLA-4 or anti-pd-1 or anti-pd-l1 Ipilimumab (BMS): anti-ctla-4 Nivolumab (ONO/BMS): anti-pd-1 Pembrolizumab (MSD): anti-pd-1 Perioperative First-line Second-line KEYNOTE-177 Ph III Pembro vs CT MSI-H Third-line + refractory to standard Durvalumab (AZ): anti-pd-l1 Atezolizumab (Roche): anti-pd-l1 Phase III Adjuvant NCI FOLFOX 6 m +/- atezo 1y MSI-H Ph III FOLFOX+B Vs Atezo Vs Atezo+FOLFOX+B MSI-H Phase III Atezo+ cobimetinib vs Atezo vs regorafenib MSS Avelumab (Merck/Pfizer) anti-pd-l1 SAMCO R Phase II Avelumab vs CT MSI-H 1. Study designs available at: (accessed September 217). Agents have not yet received EMA approval for treatment of indication listed
47 Gastric cancer
48 Cumulative survival Rationale for immuno-oncology in GC Pathology of GC associated with immune system evasion PD-L1 in gastric carcinoma 5 Immunosuppressive proteins expressed on immune cells in patients with GC patients, including key checkpoint inhibitors: 1 4 Cytotoxic T-lymphocyte-associated protein-4 (CTLA-4) PD PD-L1 Negative (n=65).2 PD-L1 Positive (n=67) Overall survival 1. Kim JW et al. Gastric Cancer 216;19:42 2; 2. Böger C et al. Oncotarget 216;7: ; 3. Saito H et al. J Surg Oncol 213;17:517 22; 4. Takano S et al. Surg Today 216;46:1341 7; 5. Zhang L et al. Int J Clin Exp Pathol. 215;8:
 ECOG PS ( vs 1) Number of")

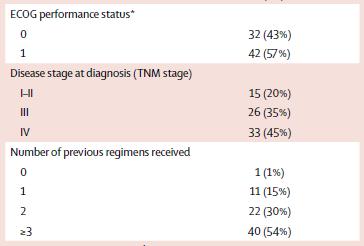
49 Study Design and Endpoints Key eligibility criteria: Age 2 years Unresectable advanced or recurrent gastric or gastroesophageal junction cancer Histologically confirmed adenocarcinoma Prior treatment with 2 regimens and refractory to/intolerant of standard therapy ECOG PS of or 1 R 2:1 Stratification based on: Nivolumab 3 mg/kg IV Q2W Country (Japan vs Korea vs Taiwan) ECOG PS ( vs 1) Number of organs with metastases (< 2 vs 2) Primary endpoint: OS Secondary endpoints: Efficacy (PFS, BOR, ORR, TTR, DOR, DCR) Safety Exploratory endpoint: Biomarkers Placebo Patients were permitted to continue treatment beyond initial RECIST v1.1 defined disease progression, as assessed by the investigator, if receiving clinical benefit and tolerating study drug BOR, best overall response; DCR, disease control rate; DOR, duration of response; ECOG PS, Eastern Cooperative Oncology Group performance status; IV; intravenous; ORR, objective response rate; OS, overall survival; PFS, progression-free survival; Q2W, every 2 weeks; R, randomization; RECIST, Response Evaluation Criteria In Solid Tumors; TTR, time to tumor response. ASCO GI 217 Kang et al. ASCO GI
50 Probability of Survival (%) Overall Survival Patients, n Events, n Median OS [95% CI], months Hazard ratio,.63 (95% CI,.5.78) P <.1 12-Month OS Rate [95% CI], % Nivolumab [ ] 26.6 [ ] Placebo [ ] 1.9 [ ] At risk: Time (months) Nivolumab Placebo ASCO GI 217 Kang et al. ASCO GI 217 5
51 Overall Survival by Subgroup Subgroup Hazard Ratio [95% CI] All.64 [.52.8] Country Japan Korea Taiwan Age, years < Sex Male Female ECOG PS 1 Prior gastrectomy No Yes Primary sites Gastric (fundus, corpus, antrum, and pylorus) Gastroesophageal junction Unknown.63 [.46.85].7 [.51.96].46 [.23.92].75 [.57.98].53 [.38.74].58 [.45.75].83 [ ].59 [.4.87].67 [.52.86].69 [.49.98].6 [.46.79].69 [.55.87].44 [.2.97].52 [ ] Subgroup Histological type (Lauren classification) Intestinal type Diffuse type Mixed Unknown Number of organs with metastasis < 2 2 Peritoneal metastasis No Yes Liver metastasis No Yes Measurable lesion No Yes Number of previous regimens Hazard Ratio [95% CI].59 [.41.85].82 [ ].37 [ ].56 [.37.84].7 [ ].61 [.48.78].63 [.5.81].74 [ ].63 [.5.8].67 [ ].7 [ ].63 [.5.8].82 [ ].87 [ ].44 [.31.61] Favors nivolumab Favors placebo Hazard ratio [95% CI] Favors nivolumab Favors placebo Hazard ratio [95% CI] ASCO GI 217 Kang et al. ASCO GI
52 Maximum Reduction From Baseline in Target Lesions (%) Maximum Reduction in Tumor Burden From Baseline 1 a Nivolumab 1 a Placebo Patients with Tumor reduction: 37.3% Patients with Tumor reduction: 12.4% a Patients with a change in tumor burden that exceeds 1%. 31% ORR ASCO GI 217 Kang et al. ASCO GI
53 Probability of Survival (%) Probability of Survival (%) No strong signal for PDL1 predictive value Overall survival by PD-L1 expression <1% vs 1% PD-L1 <1% PD-L1 1% Median OS, months (95% CI) Nivolumab (n=114) 6.1 ( ) Placebo (n=52) 4.2 (3. 6.9) Median OS, months (95% CI) ONO-4538 Nivolumab (n=16) 5.2 ( ) Placebo Placebo (n=1) 3.8 (.8 5.) Hazard ratio,.71 (95% CI,.5 1.1) Hazard ratio,.58 (95% CI, ) No. at Risk Nivolumab Placebo Months Months PD-L1 evaluable patients (N=192) 53

54 Methods Figure 1. ATTRACTION-4 study design (part 1) a IV oxaliplatin 13 mg/m 2 on day 1 followed by 2 days off and oral S-1 or oral capecitabine twice daily for 14 days followed by 7 days off. S-1 initial dose was 4 mg/m 2 /dose. Capecitabine initial dose was 1, mg/m 2 /dose ECOG PS = Eastern Cooperative Oncology Group performance status; IV = intravenous; Q3W = every 3 weeks; RECIST = Response Evaluation Criteria in Solid Tumors 54

55 Results Table 2. Summary of treatment-related adverse events 55

56 Results Figure 3. Best reduction in tumor burden 56
57 Authors Conclusions Part 1 of this two-part randomized study met its primary and secondary endpoints; nivolumab + chemotherapy regimens (SOX or CapeOX) had manageable safety profiles and demonstrated clinically meaningful antitumor activity Discontinuations due to treatment-related AEs were low ( 1% of patients) and no treatment-related deaths were reported The incidence and type of treatment-related AEs were consistent with AEs known to be associated with chemotherapy regimens and with nivolumab 5 9 Objective responses were observed in more than two-thirds of patients, occurred early, and were durable, with encouraging PFS No substantial differences in clinical activity and safety were observed between the nivolumab + SOX and nivolumab + CapeOX treatment regimens These results suggest that nivolumab in combination with SOX or CapeOX chemotherapy in patients with unresectable advanced or recurrent gastric or gastroesophageal junction cancer may be a first-line therapy option Part 2 of this study is currently recruiting patients 57
58 414: Nivolumab ± ipilimumab in pts with advanced (adv)/metastatic chemotherapy-refractory (CTx-R) gastric (G), esophageal (E), or gastroesophageal junction (GEJ) cancer: CheckMate 32 study Study objective To evaluate the long-term survival, efficacy, and safety of nivolumab alone and in combination with ipilimumab in the oesophagogastric cohort of the CheckMate 32 study Key patient inclusion criteria Advanced/metastatic oesophagogastric cancer Progression on 1 prior chemotherapy Western population (n=16) Nivolumab 3 mg/kg IV q2w (n=59) Nivolumab 1 mg/kg + ipilimumab 3 mg/kg IV q3w* (n=49) PD/death/ toxicity PD/death/ toxicity Nivolumab 3 mg/kg + ipilimumab 1 mg/kg IV q3w* (n=52) PD/death/ toxicity PRIMARY ENDPOINT ORR (RECIST v1.1) SECONDARY ENDPOINTS OS, PFS, TTR, DoR, safety, PD-L1 tumour expression *Administered for 4 cycles followed by nivolumab 3 mg/kg IV q2w Janjigian YY, et al. J Clin Oncol 217;35(Suppl):Abstr 414
59 Probability of survival Probability of progression-free survival 414: Nivolumab ± ipilimumab in pts with advanced (adv)/metastatic chemotherapy-refractory (CTx-R) gastric (G), esophageal (E), or gastroesophageal junction (GEJ) cancer: CheckMate 32 study Janjigian YY, et al 1. OS 1. PFS Time, months mos, months OS rate, % (95%CI) 12-month 18-month Nivolumab 3 mg/kg 6.2 (3.4, 12.4) Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg 6.9 (3.7, 11.5) (3., 8.4) Time, months mpfs, months PFS rate, % (95%CI) 6-month 12-month Nivolumab 3 mg/kg 1.4 (1.2, 1.5) 17 8 Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg 1.4 (1.2, 3.8) (1.4, 2.6) 12 1 Janjigian YY, et al. J Clin Oncol 217;35(Suppl):Abstr 414
60 Best reduction from baseline in target lesions, % 414: Nivolumab ± ipilimumab in pts with advanced (adv)/metastatic chemotherapy-refractory (CTx-R) gastric (G), esophageal (E), or gastroesophageal junction (GEJ) cancer: CheckMate 32 study Janjigian YY, et al Key results (cont.) Best reduction in target lesions Nivolumab 3 mg/kg PD-L1-evaluable patients, 38 of 53 Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg PD-L1-evaluable patients, 38 of 42 Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg PD-L1-evaluable patients, 34 of * * * * -5 * * * * * * * -5 * * * * * * PD-L1 <1% PD-L1 1% PD-L1 not evaluable/missing * * Janjigian YY, et al. J Clin Oncol 217;35(Suppl):Abstr 414
61 KEYNOTE-59: Efficacy and Safety of Pembrolizumab Alone or in Combination With Chemotherapy in Patients With Advanced Gastric or Gastroesophageal Cancer Study Design Cohort 1 2 prior lines of chemotherapy PD-L1 positive or negative Pembrolizumab 2 mg Q3W Cohort 2 No prior therapy PD-L1 positive or negative Pembrolizumab 2 mg Q3W + Cisplatin 8mg/m 2 Q3W + 5-FU 8 mg/m 2 Q3W or Capecitabine 1 mg/m 2 BID Q3W a Treat for up to 35 cycles ( ~ 2 years), or until progression or intolerable toxicity Follow-up for survival by telephone until death, withdrawal, or study end Cohort 3 No prior therapy PD-L1 positive Pembrolizumab 2 mg Q3W Response assessment per RECIST v1.1: First scan 9 weeks after cycle 1, then every 6 weeks for year 1 and every 9 weeks thereafter Primary end points: Safety (all cohorts); ORR by central review per RECIST v1.1 (cohort 1: all patients and patients with PD-L1-positive expression); ORR by central review per RECIST v1.1 (cohort 3) PD-L1 positive: combined positive score (CPS) 1 (previously reported as and equivalent to CPS 1%), where CPS=number of PD-L1-positive cells b (tumor cells, lymphocytes, and macrophages) divided by the total number of tumor cells x 1 Wainberg et al., Abstract LBA28, ESMO 217 a Capecitabine was administered only in Japan b PD-L1 IHC 22C3 pharmadx (Agilent Technologies, Carpinteria, CA,USA)
62 KEYNOTE-59 cohort 1: Efficacy and safety of pembrolizumab monotherapy in patients with previously treated advanced gastric cancer. Study Design Cohort 1 2 prior lines of chemotherapy PD-L1 positive or negative Pembrolizumab 2 mg Q3W Cohort 2 No prior therapy PD-L1 positive or negative Pembrolizumab 2 mg Q3W + Cisplatin 8mg/m 2 Q3W + 5-FU 8 mg/m 2 Q3W or Capecitabine 1 mg/m 2 BID Q3W a Treat for up to 35 cycles ( ~ 2 years), or until progression or intolerable toxicity Follow-up for survival by telephone until death, withdrawal, or study end Cohort 3 No prior therapy PD-L1 positive Pembrolizumab 2 mg Q3W Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217 a Capecitabine was administered only in Japan
63 KEYNOTE-59 cohort 1: Efficacy and safety of pembrolizumab monotherapy in patients with previously treated advanced gastric cancer. Baseline Characteristics Characteristic N=259 Median age (range), years 62 (24-89) Male, n (%) 198 (76) Race, n (%) White Asian Other ECOG, n (%) 1 Number of prior therapies, n (%) Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO (77) 41 (16) 7 (3) 17 (41) 151 (58) 134 (52) 75 (29) 5 (19) Characteristic N=259 Location of primary tumor, n (%) GEJ Gastric Prior gastrectomy, n (%) Total Partial No PD-L1 expression, n (%) Positive Negative Unknown HER2 status, n (%) Positive Negative Intermediate 134 (52) 124 (48) 49 (19) 17 (7) 193 (75) 148 (57) 19 (42) 2 (1) 63 (24) 194 (75) 2 (1)
64 KEYNOTE-59 cohort 1: Efficacy and safety of pembrolizumab monotherapy in patients with previously treated advanced gastric cancer. Response Response b All Patients N = 259 PD-L1 Positive a N = 148 PD-L1 Negative N = 19 % 95% CI % 95% CI % 95% CI ORR DCR c DOR CR PR SD PD Median (range) follow-up: 5.6 ( ) months 134 patients received pembrolizumab as third-line therapy; ORR was 16%, and DCR was 31% 125 patients received pembrolizuman as fourth plus-line therapy; ORR was 7%, and DCR was 23% Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217 a CPS 1 b Only confirmed responses were included c CR + PR + SD 2 months

; assessment was nonevaluable in 1 patient b Longitudinal change")
65 KEYNOTE-59 cohort 1: Efficacy and safety of pembrolizumab monotherapy in patients with previously treated advanced gastric cancer. Best Percentage Change and Longitudinal Change in Target Lesion Size Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217 a Only patients with measurable disease per RECIST v1.1 by central review at baseline who had 1 postbaseline assessment were included (n=223); assessment was nonevaluable in 1 patient b Longitudinal change in the sum of the longest target lesion diameters from baseline in responders (n=31) +No progressive disease at last disease assessment
66 KEYNOTE-59 cohort 1: Efficacy and safety of pembrolizumab monotherapy in patients with previously treated advanced gastric cancer. PFS and OS in All Patients Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217
67 KEYNOTE-59 cohort 1: Efficacy and safety of pembrolizumab monotherapy in patients with previously treated advanced gastric cancer. PFS and OS by PD-L1 Expression Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217
68 KEYNOTE-59 cohort 1: Efficacy and safety of pembrolizumab monotherapy in patients with previously treated advanced gastric cancer. Treatment-Related Adverse Events Event, n (%) N = 259 Any 159 (61) Grades 3-5 Anemia, grade 3 Fatigue, grade 3 Dehydration, grade 3 46 (18) 7 (3) 6 (2) 3 (1) Serious 29 (11) Led to discontinuation a 7 (3) Led to death Acute kidney injury Pleural effusion Median (range) duration of exposure was 2.1 (.-23,7) months 2 (1) 1 (1) 1 (1) Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217 a Abnormal hepatic function, bile duct stenosis, encephalitis, increase blood bilirubin level, hyperglycemia, acute kidney injury, and pneumonitis
69 KEYNOTE-59 cohort 1: Efficacy and safety of pembrolizumab monotherapy in patients with previously treated advanced gastric cancer. Immune-Mediated Adverse Events a and Infusion-Related Reactions Event, n (%) There were no grade 4/5 immune-mediated or infusion reactions N=259 All Grades in >2 Patients Grades 3b Any 5 (19) 13 (5) Hypothyroidism 24 (9) 1 (<1) Hyperthyroidism 9 (4) Colitis 4 (2) 3 (1) Infusion-related reactions 4 (2) Pneumonitis 4 (2) 2 (1) Thyroiditis 3 (1) 1 (<1) Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217 a Based on a list of terms specified by the sponsor and included regardless of attribution to study treatment or immune relatedness by the investigator b 2 (1%) patients experienced grade 3 rash; 1 (<1%) patient experienced grade 3 adverse events: uveitis, hepatitis, jaundice, encephalitis, and maculopapular rash
70 KEYNOTE-59 Cohort 2: Safety and efficacy of pembrolizumab plus 5-fluorouracil and cisplatin for first-line treatment of advanced gastric cancer Study Design Cohort 1 2 prior lines of chemotherapy PD-L1 positive or negative Pembrolizumab 2 mg Q3W Cohort 2 No prior therapy PD-L1 positive or negative Pembrolizumab 2 mg Q3W + Cisplatin 8mg/m 2 Q3W + 5-FU 8 mg/m 2 Q3W or Capecitabine 1 mg/m 2 BID Q3W a Treat for up to 35 cycles ( ~ 2 years), or until progression or intolerable toxicity Follow-up for survival by telephone until death, withdrawal, or study end Cohort 3 No prior therapy PD-L1 positive Pembrolizumab 2 mg Q3W Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217 a Capecitabine was administered only in Japan
71 KEYNOTE-59 Cohort 2: Safety and efficacy of pembrolizumab plus 5-fluorouracil and cisplatin for first-line treatment of advanced gastric cancer Baseline Characteristics Characteristic N=25 Median age (range), years, y 64 (21-82) Male, n (%) 16 (24) Race, n (%) White Asian ECOG PS, n (%) 1 8 (32) 17 (68) 15 (6) 1 (4) Characteristic N=25 Location of primary tumor, n (%) GEJ Gastric Prior gastrectomy, n (%) Total Partial No PD-L1 expression, n (%) Positive Negative Unknown 5 (2) 2 (8) 4 (16) 1 (4) 2 (8) 16 (64) 8 (32) 1 (4) HER2 negative, n (%) 25 (1) Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217
72 KEYNOTE-59 Cohort 2: Safety and efficacy of pembrolizumab plus 5-fluorouracil and cisplatin for first-line treatment of advanced gastric cancer Response Respons e b All Patients N = 25 PD-L1 Positive a N = 16 PD-L1 Negative N = 8 % 95% CI % 95% CI % 95% CI ORR DCR c BOR CR PR SD PD Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217 Median (range) follow-up in cohort 2: 13.8 ( ) months a CPS 1 b Only confirmed responses were included c CR + PR + SD 6 months

; assessment was nonevaluable for 1 patient b Longitudinal change in the sum")
73 KEYNOTE-59 Cohort 2: Safety and efficacy of pembrolizumab plus 5-fluorouracil and cisplatin for first-line treatment of advanced gastric cancer Best Percentage Change and Longitudinal Change in Target Lesion Size Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217 a Only patients with measurable disease per RECIST v1.1 by central review at baseline who had 1 postbaseline assessment were included (n=25); assessment was nonevaluable for 1 patient b Longitudinal change in the sum of the longest target lesion diameters from baseline in patients with 1 postbaseline assessment (n=25) +No progressive disease at last disease assessment
74 KEYNOTE-59 Cohort 2: Safety and efficacy of pembrolizumab plus 5-fluorouracil and cisplatin for first-line treatment of advanced gastric cancer PFS and OS Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217
75 KEYNOTE-59 Cohort 2: Safety and efficacy of pembrolizumab plus 5-fluorouracil and cisplatin for first-line treatment of advanced gastric cancer Treatment-Related Adverse Events Event, n (%) N = 25 Any 25 (1) Grades 3/4 Neutropenia Stomatitis Anemia Decreased platelet count Decreased appetite Fatigue 19 (76) 6 (24) 5 (2) 2 (8) 2 (8) 2 (8) 2 (8) Led to discontinuation 3 (12) Led to death Median (range) duration of exposure was 7.1 ( ) months 3 (12%) patients discontinued treatment because of chemotherapy-related adverse events (stomatitis [grade 3], hypoacusis [grade 2], increased creatinine level [grade 1]) No patients discontinued treatment because of pembrolizumab-related adverse events Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217
76 KEYNOTE-59 Cohort 2: Safety and efficacy of pembrolizumab plus 5-fluorouracil and cisplatin for first-line treatment of advanced gastric cancer Immune-Mediated Adverse Events a Event, n (%) All Grades in >2 Patients There were no grade 4/5 immune-mediated or infusion reactions N=25 Grades 3 in All Patients Any 12 (48) 4 (16) Hyperthyroidism 4 (16) Palmar-plantar erythrodysesthesia 2 (8) 2 (8) Nephrotic syndrome 1 (4) 1 (4) Rash 1 (4) 1 (4) Maculopapular rash 1 (4) 1 (4) Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217 a Based on a list of terms specified by the sponsor and included regardless of attribution to study treatment or immune relatedness by the investigator
77 KEYNOTE-59 Cohort 3: Safety and efficacy of pembrolizumab monotherapy for first-line treatment of patients with PD-L1-positive advanced gastric/gastroesophageal cancer Study Design Cohort 1 2 prior lines of chemotherapy PD-L1 positive or negative Pembrolizumab 2 mg Q3W Cohort 2 No prior therapy PD-L1 positive or negative Pembrolizumab 2 mg Q3W + Cisplatin 8mg/m 2 Q3W + 5-FU 8 mg/m 2 Q3W or Capecitabine 1 mg/m 2 BID Q3W a Treat for up to 35 cycles ( ~ 2 years), or until progression or intolerable toxicity Follow-up for survival by telephone until death, withdrawal, or study end Cohort 3 No prior therapy PD-L1 positive Pembrolizumab 2 mg Q3W Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217 a Capecitabine was administered only in Japan
78 KEYNOTE-59 Cohort 3: Safety and efficacy of pembrolizumab monotherapy for first-line treatment of patients with PD-L1-positive advanced gastric/gastroesophageal cancer Baseline Characteristics Characteristic N=31 Median age (range), years, y 62 (32-75) Male, n (%) 19 (61) Race, n (%) White Asian ECOG PS, n (%) 1 16 (52) 15 (48) 14 (45) 17 (55) No. of prior therapies, n (%) Characteristic N=31 Location of primary tumor, n (%) GEJ Gastric Prior gastrectomy, n (%) Total Partial No 12 (39) 19 (61) 9 (29) 3 (1) 19 (61) PD-L1 positive, n (%) 31 (1) HER2 negative, n (%) 31 (1) Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217
79 KEYNOTE-59 Cohort 3: Safety and efficacy of pembrolizumab monotherapy for first-line treatment of patients with PD-L1-positive advanced gastric/gastroesophageal cancer Response Response a N = 31 % 95% CI ORR DCR b BOR CR PR SD PD Median (range) follow-up in cohort 3: 17.5 ( ) months Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217 a Only confirmed responses were included b CR + PR + SD 6 months Data cutoff: April 21, 217

80 KEYNOTE-59 Cohort 3: Safety and efficacy of pembrolizumab monotherapy for first-line treatment of patients with PD-L1-positive advanced gastric/gastroesophageal cancer Best Percentage Change and Longitudinal Change in Target Lesion Size Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217 a Only patients with measurable disease per RECIST v1.1 by central review at baseline who had 1 postbaseline assessment were included (n=31); assessment were nonevaluable/not evailable in 3 patients b Longitudinal change in the sum of the longest target lesion diameters from baseline in patients with CR or PR (n=3) +No progressive disease at last disease assessment
81 KEYNOTE-59 Cohort 3: Safety and efficacy of pembrolizumab monotherapy for first-line treatment of patients with PD-L1-positive advanced gastric/gastroesophageal cancer PFS and OS Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217
82 KEYNOTE-59 Cohort 3: Safety and efficacy of pembrolizumab monotherapy for first-line treatment of patients with PD-L1-positive advanced gastric/gastroesophageal cancer Treatment-Related Adverse Events Event, n (%) N = 31 Any 24 (77) Grades (23) Led to discontinuation Led to death 1 (3) Pneumonitis a 1 (3) Median (range) duration of exposure was 2.8 (.7-2.3) months 1 patient each experienced grade 3 adverse events (neutropenia, diffuse uveal melanocytic proliferation, colitis, bile duct obstruction, decreased neutrophils, dehydration, hyponatremia, and rash 1 patient died because of a treatment-related adverse events during safety follow-up (pneumonitis) Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217 a death occurred during safety follow-up
83 KEYNOTE-59 Cohort 3: Safety and efficacy of pembrolizumab monotherapy for first-line treatment of patients with PD-L1-positive advanced gastric/gastroesophageal cancer Immune-Mediated Adverse Events a Event, n (%) All Grades in >2 Patients N=31 Grades 3 Grade 5 Any 1 (32) 2 (7) 1 (3) Pneumonitis 4 (13) 1 (3) Colitis 1 (3) 1 (3) Rash 1 (3) 1 (3) Data cutoff: April 21, 217 Wainberg et al., Abstract LBA28, ESMO 217 a Based on a list of terms specified by the sponsor and included regardless of attribution to study treatment or immune relatedness by the investigator
84 KEYNOTE-59 Cohort 3: Safety and efficacy of pembrolizumab monotherapy for first-line treatment of patients with PD-L1-positive advanced gastric/gastroesophageal cancer Summary and Conclusion (I) Updated KEYNOTE-59 results Pembrolizumab continues to demonstrate, in patients with advanced G/GEJ cancer, Promising antitumor activity and durable response as monotherapy in patients whose disease has progressed after 2 prior lines of therapy Encouraging antitumor activity in combination with chemotherapy in previously untreated patients Encouraging antitumor activity as monotherapy in previously untreated patients with PD-L1-positive tumors Responses were regardless of PD-L1 expression, but higher in patients with PD-L1-positive tumors in cohorts 1 and 2 Safety was manageable and consistent with that previous reports: no new safety signals Wainberg et al., Abstract LBA28, ESMO 217
85 KEYNOTE-59 Cohort 3: Safety and efficacy of pembrolizumab monotherapy for first-line treatment of patients with PD-L1-positive advanced gastric/gastroesophageal cancer Summary and Conclusion (II) Results support further development of pembrolizumab for advanced G/GEJ cancer KEYNOTE-61 (NCT237498) is an ongoing, phase 3, randomized clinical study of pembrolizumab versus paclitaxel in patients with advanced G/GEJ cancer whose disease progressed after first-line therapy with platinum and fluoropyrimidine KEYNOTE-62 (NCT ) is an ongoing, phase 3, randomized clinical study of pembrolizumab alone or in combination with chemotherapy versus chemotherapy alone as first-line therapy for advanced PD-L1 positive G/GEJ cancer Wainberg et al., Abstract LBA28, ESMO 217
86 After ESMO: even more trials for oesophagogastric cancer Anti-CTLA-4 or anti-pd-1 or anti-pd-l1 Ipilimumab (BMS): anti-ctla-4 Nivolumab (ONO/BMS): anti-pd-1 Pembrolizumab (MSD): anti-pd-1 Durvalumab (AZ): anti-pd-l1 Atezolizumab (Roche): anti-pd-l1 Avelumab (Merck/Pfizer) anti-pd-l1 Perioperative First-line Second-line Phase III Adjuvant 577 Nivo vs placebo ESO after RCTX Phase II Adjuvant Phase II Perioperative FOLFOX/ FLOT +/- atezolizumab Phase III 649/648 Nivo Ipi vs CTX Phase III 649/648 Nivo Ipi vs CTX KEYNOTE-62 Ph III Pembro vs Pembro, Cis, 5-FU vs Cis, 5-FU Phase II Durvalumab vs placebo JAVELIN GASTRIC 1 Phase III Maintenance after FOLFOX ONO-473 Phase III Nivo vs Taxanes KEYNOTE-181 Phase III Pembro vs standard of care KEYNOTE-61 Phase III Pembro vs paclitaxel Phase Ib/II Durva vs Treme vs Durva+Treme Third-line + refractory to standard ONO Phase II Nivo KEYNOTE-18 Phase II Pembro Phase Ib and II Durva+Treme (Phase I) and Phase III Avelumab JAVELIN GASTRIC 3 1. Study designs available at: (accessed September 217). Agents have not yet received EMA approval for treatment of indication listed
87 HCC
88 All Patients (N = 262) CheckMate 4 Study Design Study Endpoints Dose Escalation Uninfected (n = 23) Sorafenib Experienced (2L) (n = 37) Primary Safety and tolerability (escalation).1 1 mg/kg N = 48 HCV infected (n = 1) HBV infected (n = 15) Sorafenib Naive (1L) (n = 11) Objective response rate a (expansion) Secondary Objective response rate a (escalation) Disease control rate Time to response Duration of response Overall survival Dose Expansion Uninfected (n = 113) Sorafenib Experienced (2L) (n = 145) Other Biomarker assessments 3 mg/kg HCV infected (n = 5) Patient-reported outcomes b N = 214 HBV infected (n = 51) Sorafenib Naive (1L) (n = 69) Disease assessment imaging (CT or MRI) every 6 weeks Interim analysis data cutoff date: August 8, 216 Median follow-up was 13.3 months in the dose-escalation phase and 1.5 months in the dose-expansion phase a RECIST v1.1; b Baseline and every 6 weeks through week 25 using the EQ-5D utility index and visual analog scale (VAS). ASCO GI
89 Safety: Dose-Expansion Phase Patients, n (%) Any Grade Uninfected (n = 113) Grade 3/4 HCV Infected (n = 5) Any Grade Grade 3/4 HBV Infected (n = 51) Any Grade Grade 3/4 All Dose Expansion (N = 214) Any treatment-related AE (TRAE) 84 (74) 22 (19) 4 (8) 15 (3) 35 (69) 3 (6) 159 (74) 4 (19) TRAEs ( 5%) Fatigue 34 (3) 2 (2) 8 (16) 1 (2) 7 (14) 49 (23) 3 (1) Pruritus 18 (16) 14 (28) 1 (2) 13 (25) 45 (21) 1 (<1) Rash 16 (14) 2 (2) 9 (18) 8 (16) 33 (15) 2 (1) Diarrhea 19 (17) 2 (2) 5 (1) 3 (6) 1 (2) 27 (13) 3 (1) Nausea 1 (9) 6 (12) 1 (2) 17 (8) Dry mouth 9 (8) 2 (4) 2 (4) 13 (6) Decreased appetite 6 (5) 2 (4) 1 (2) 3 (6) 11 (5) 1 (<1) Laboratory TRAEs ( 5%) AST increase 9 (8) 4 (4) 6 (12) 5 (1) 1 (2) 16 (7) 9 (4) ALT increase 7 (6) 2 (2) 7 (14) 3 (6) 3 (6) 17 (8) 5 (2) Any Grade Grade 3/4 ASCO GI
 1 mg/kg 1 mg/kg Uninfected (n = 14) HCV (n = 2).3 mg/kg 1 mg/kg HCV (n = 7) CR PR HBV (n = 1).")
 DOR, median (range), mo 17.1 (7.2 32.5+) TTR, median (range), mo 2.7 (1.2 9.6) DOR, median (range), mo NR (1.4 9.")
90 Time to Response and Duration of Response Sorafenib Experienced (2L) Investigator Assessment Dose Escalation Dose Expansion 3 mg/kg Uninfected (n = 3) 1 mg/kg 1 mg/kg Uninfected (n = 14) HCV (n = 2).3 mg/kg 1 mg/kg HCV (n = 7) CR PR HBV (n = 1).1 mg/kg HBV (n = 6) Last dose Last dose when off treatment Censored with ongoing response TTR, median (range), mo 1.9 ( ) DOR, median (range), mo 17.1 ( ) TTR, median (range), mo 2.7 ( ) DOR, median (range), mo NR ( ) NR, not reached. ASCO GI 217 9
91 Probability of Survival Overall Survival Sorafenib Experienced (2L) Dose Expansion: Median OS (95% CI), mo = 13.2 (13.2 NR) Dose Escalation: Median OS (95% CI), mo = 15. (5. 2.2) OS Rate (95% CI), % Dose Escalation (n = 37) Dose Expansion (n = 145) 6 months 67 (49 8) 82 (74 87) 9 months 67 (49 8) 71 (63 78) a 12 months 58 (4 72) NC 18 months 46 (29 62) NC a Data cutoff August 8, 216. NC, not available/not calculated. Months ASCO GI
92 Change in Target Lesion Size From Baseline (%) Response by PD-L1 Expression Sorafenib Experienced (2L) Investigator Assessment 1 Dose Escalation 1 Dose Expansion PD-L1: < 1% 1% NA PD-L1: < 1% 1% NA PD-L1 < 1% PD-L1 1% -5 PD-L1 < 1% PD-L1 1% ORR, n/n (%) 95% CI, % 4/26 (15.4), /9 (22.2), ORR, n/n (%) 95% CI, % 17/99 (17.2) /25 (32.), Patients -1 Patients Responses were observed irrespective of PD-L1 expression on tumor cells ASCO GI
93 Other GI cancer
94 Attraction 1 trial Nivolumab monotherapy for advanced pretreated oesophageal cancer Summary of Clinical Activity (N=64): As of Nov. 17, 216 Best Overall Response/ORR Investigator Central Review Response N % (95% CI) N % (95% CI) Complete response (CR) (.9, 1.7) (1.6, 12.9) Partial response (PR) (11.1, 3.) (6.5, 22.8) Stable disease (SD) (21.2, 43.4) (16., 36.8) Progressive disease (PD) NE * 12.5 ORR (CR+PR) (13.5, 33.4) (9.9, 28.2) *Including subjects who have no target lesion 64 patients were assessable for the primary endpoint as one patient was excluded due to having multiple primary cancers 1
95 Results Figure 2. Progression-Free Survival and Overall Survival (N=64): As of Nov. 17, 216 CI = confidence interval 95


96 Nivolumab in L2+ Anal cancer NCI9673: Primary Endpoint of Response Rate Lancet Oncology 217 Cathy Eng
97 RESULTATS Taux de réponse : 9/37 = 24% (IC95=15-33) en réponse dont 2 réponses complètes, et 1 réponse partielle chez un patient VIH 7/9 des répondeurs (78%) ont maintenu cette réponse jusqu'à l'analyse des données (temps médian 5.8mois IC95= , durée la plus longue à 1.4mois) Réponse radiologique de -7% (IC95=57-9) Taux de stabilisation : 17/37 = 47% (IC95=6-63) en maladie stable, soit au total 72% (IC95=53-84) de contrôle de la maladie à la 1 ère évaluation
98 Bryan S. Balancing cost-effectiveness with other values: the NICE experience - Gesundheitswesen 29; 71: S3-S33

99 Conclusion J Taieb WCGIC Barcelona 216
Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142
 Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142 Abstract #519 Overman MJ, Lonardi S, Leone F, McDermott
Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142 Abstract #519 Overman MJ, Lonardi S, Leone F, McDermott
Bristol-Myers Squibb, Braine-l Alleud, Belgium; 12 MD Anderson Cancer Center, Houston, TX, USA
 3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER. Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium
 THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Royal Marsden Hospital ESMO Colorectal Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role Servier, Celgene, BMS, Five
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Royal Marsden Hospital ESMO Colorectal Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role Servier, Celgene, BMS, Five
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
ASCO 2017 updates in Colorectal and Gastric Cancers. May Cho, M.D.
 ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
Presentation Number: LBA18_PR. Lecture Time: 09:15-09:27. Speakers: Heinz-Josef J. Lenz (Los Angeles, US) Background
 Background") LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS
 CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT
 ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy
: Biomarkers for Immunotherapy") Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Policy. Medical Policy Manual Approved Revised: Do Not Implement until 6/30/2019. Nivolumab
 Medical Manual Approved Revised: Do Not Implement until 6/30/2019 Nivolumab NDC CODE(S) 00003-3772-XX Opdivo 40 MG/4ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3774-XX Opdivo 100 MG/10ML SOLN (B-M SQUIBB
Medical Manual Approved Revised: Do Not Implement until 6/30/2019 Nivolumab NDC CODE(S) 00003-3772-XX Opdivo 40 MG/4ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3774-XX Opdivo 100 MG/10ML SOLN (B-M SQUIBB
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Immunotherapy for Upper GI Cancers
 Immunotherapy for Upper GI Cancers Esophageal Adenocarcinoma GE Junction Adeno Gastric Carcinoma Ahmed Zakari MD Medical Director of GI Cancer Program, Florida Hospital Cancer Institute Associate Professor
Immunotherapy for Upper GI Cancers Esophageal Adenocarcinoma GE Junction Adeno Gastric Carcinoma Ahmed Zakari MD Medical Director of GI Cancer Program, Florida Hospital Cancer Institute Associate Professor
Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration trials and future considerations
 Gong et al. Journal for ImmunoTherapy of Cancer (2018) 6:8 DOI 10.1186/s40425-018-0316-z REVIEW Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration
Gong et al. Journal for ImmunoTherapy of Cancer (2018) 6:8 DOI 10.1186/s40425-018-0316-z REVIEW Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration
Policy. Medical Policy Manual Approved Revised: Do Not Implement Until 3/2/19. Nivolumab (Intravenous)
") Nivolumab (Intravenous) NDC CODE(S) 00003-3772-XX Opdivo 40 MG/4ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3774-XX Opdivo 100 MG/10ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3734-XX Opdivo 240
Nivolumab (Intravenous) NDC CODE(S) 00003-3772-XX Opdivo 40 MG/4ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3774-XX Opdivo 100 MG/10ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3734-XX Opdivo 240
Highlights STOMACH CANCER
 UPDATES and NEWS from the Gastrointestinal Cancers Symposium in San Francisco Roma, 10-11 Febbraio 2017 Highlights STOMACH CANCER Lorenzo Fornaro, MD Unit of Medical Oncology 2 Azienda Ospedaliero-Universitaria
UPDATES and NEWS from the Gastrointestinal Cancers Symposium in San Francisco Roma, 10-11 Febbraio 2017 Highlights STOMACH CANCER Lorenzo Fornaro, MD Unit of Medical Oncology 2 Azienda Ospedaliero-Universitaria
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Keytruda. Keytruda (pembrolizumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.50 Subject: Keytruda Page: 1 of 9 Last Review Date: November 30, 2018 Keytruda Description Keytruda
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.50 Subject: Keytruda Page: 1 of 9 Last Review Date: November 30, 2018 Keytruda Description Keytruda
Immunotherapy for dmmr metastatic colorectal cancer. Prof.dr. Kees Punt Dept. Medical Oncology AUMC
 Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
MEETING SUMMARY ESMO 2018, Munich, Germany. Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER
 MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
Keytruda. Keytruda (pembrolizumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.50 Subject: Keytruda Page: 1 of 9 Last Review Date: September 20, 2018 Keytruda Description Keytruda
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.50 Subject: Keytruda Page: 1 of 9 Last Review Date: September 20, 2018 Keytruda Description Keytruda
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-028 Study
 Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies. Eric H. Rubin, MD Merck Research Laboratories
 Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
Chemotherapy for Advanced Gastric Cancer
 Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
AACR 2018 Investor Meeting
 AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
NOVITA IN TEMA DI CARCINOMA GASTRICO ROSA BERENATO
 NOVITA IN TEMA DI CARCINOMA GASTRICO ROSA BERENATO ONCOLOGIA MEDICA 1 FONDAZIONE IRCCS ISTITUTO NAZIONALE DEI TUMORI MILANO PROGRESS AGAINST METASTATIC GC OS in first-line palliative setting Little progress
NOVITA IN TEMA DI CARCINOMA GASTRICO ROSA BERENATO ONCOLOGIA MEDICA 1 FONDAZIONE IRCCS ISTITUTO NAZIONALE DEI TUMORI MILANO PROGRESS AGAINST METASTATIC GC OS in first-line palliative setting Little progress
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO. CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS?
 INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS? V. Alonso Servicio de Oncologia Medica H. U. Miguel Servet Zaragoza MSI-H mcrc Clinical and Pathological
INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS? V. Alonso Servicio de Oncologia Medica H. U. Miguel Servet Zaragoza MSI-H mcrc Clinical and Pathological
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for Renal Cell Carcinoma. James Larkin
 Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Checkpoint regulators a new class of cancer immunotherapeutics. Dr Oliver Klein Medical Oncologist ONJCC Austin Health
 Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Immunotherapy on the Horizon
 Immunotherapy on the Horizon Andrew L. Coveler Assistant Professor of Medicine, Division of Oncology University of Washington Assistant Member Fred Hutchinson Cancer Research Center Image: NASA.gov 1 2
Immunotherapy on the Horizon Andrew L. Coveler Assistant Professor of Medicine, Division of Oncology University of Washington Assistant Member Fred Hutchinson Cancer Research Center Image: NASA.gov 1 2
Immunotherapy for Metastatic Malignant Melanoma. Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
 Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Tumores esófago-gástricos, tiene algo que decir la inmunoterapia? Dr. Fernando Rivera Herrero Hospital Universitario Marqués de Valdecilla.
 Tumores esófago-gástricos, tiene algo que decir la inmunoterapia? Dr. Fernando Rivera Herrero Hospital Universitario Marqués de Valdecilla. Santander Finantial disclosure Consultor: CELGENE Research fundings:
Tumores esófago-gástricos, tiene algo que decir la inmunoterapia? Dr. Fernando Rivera Herrero Hospital Universitario Marqués de Valdecilla. Santander Finantial disclosure Consultor: CELGENE Research fundings:
Supplementary Online Content
 Supplementary Online Content Powles T, O Donnell PH, Massard C, et al. Efficacy and safety of durvalumab in locally advanced or metastatic urothelial carcinoma: updated results from a phase 1/2 openlabel
Supplementary Online Content Powles T, O Donnell PH, Massard C, et al. Efficacy and safety of durvalumab in locally advanced or metastatic urothelial carcinoma: updated results from a phase 1/2 openlabel
ASCO 2014 Highlights*
 ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Update on the development of immune checkpoint inhibitors
 Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
ESMO 2016 * Investor Meeting October 9, *European Society of Medical Oncology, October 7-11, 2016 ESMO 2016 NOT FOR PRODUCT PROMOTIONAL USE
 ESMO 2016 * Investor Meeting October 9, 2016 *European Society of Medical Oncology, October 7-11, 2016 1 Forward-Looking Information During this meeting, we will make statements about the Company s future
ESMO 2016 * Investor Meeting October 9, 2016 *European Society of Medical Oncology, October 7-11, 2016 1 Forward-Looking Information During this meeting, we will make statements about the Company s future
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Checkpoint-Inhibitoren beim Lungenkarzinom. Dr. Helge Bischoff Thoraxklinik Heidelberg
 Checkpoint-Inhibitoren beim Lungenkarzinom Dr. Helge Bischoff Thoraxklinik Heidelberg Survival (%) First-Line: Polychemotherapy vs 9387 patients 778 patients in studies with platinum chemotherapy 1-year
Checkpoint-Inhibitoren beim Lungenkarzinom Dr. Helge Bischoff Thoraxklinik Heidelberg Survival (%) First-Line: Polychemotherapy vs 9387 patients 778 patients in studies with platinum chemotherapy 1-year
Attached from the following page is the press release made by BMS for your information.
 June 22, 2015 European Commission Approves Bristol-Myers Squibb s Opdivo (nivolumab), the First and Only PD-1 Checkpoint Inhibitor Approved in Europe, for Both First-Line and Previously-Treated Advanced
June 22, 2015 European Commission Approves Bristol-Myers Squibb s Opdivo (nivolumab), the First and Only PD-1 Checkpoint Inhibitor Approved in Europe, for Both First-Line and Previously-Treated Advanced
Prostate cancer Management of metastatic castration sensitive cancer
 18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
Immunotherapy for Melanoma. Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center
 Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Keytruda. Keytruda (pembrolizumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.50 Subject: Keytruda Page: 1 of 7 Last Review Date: December 8, 2017 Keytruda Description Keytruda
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.50 Subject: Keytruda Page: 1 of 7 Last Review Date: December 8, 2017 Keytruda Description Keytruda
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy in Patients with Non-Small Cell Lung Cancer
 LIVE WEBINARS Immunotherapy in Patients with Non-Small Cell Lung Cancer Presented by: Leora Horn, MD, MSc Vanderbilt-Ingram Cancer Center July 14, 216 Moderated by Rose K. Joyce NCCN, Conferences and Meetings
LIVE WEBINARS Immunotherapy in Patients with Non-Small Cell Lung Cancer Presented by: Leora Horn, MD, MSc Vanderbilt-Ingram Cancer Center July 14, 216 Moderated by Rose K. Joyce NCCN, Conferences and Meetings
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Attached from the following page is the press release made by BMS for your information.
 September 28, 2015 Opdivo (nivolumab) Demonstrates Superior Overall Survival in a Phase 3 Trial Compared to Standard of Care in Patients with Previously Treated Advanced Renal Cell Carcinoma (PRINCETON,
September 28, 2015 Opdivo (nivolumab) Demonstrates Superior Overall Survival in a Phase 3 Trial Compared to Standard of Care in Patients with Previously Treated Advanced Renal Cell Carcinoma (PRINCETON,
Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma
 With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma") Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
My name is Dr. David Ilson, Professor of Medicine at Memorial Sloan Kettering Cancer Center and Weill Cornell Medical Center in New York, New York.
 Welcome to this CME/CE-certified activity entitled, Integrating the Latest Advances Into Clinical Experience: Data and Expert Insights From the 2016 Meeting on Gastrointestinal Cancers in San Francisco.
Welcome to this CME/CE-certified activity entitled, Integrating the Latest Advances Into Clinical Experience: Data and Expert Insights From the 2016 Meeting on Gastrointestinal Cancers in San Francisco.
Merck ASCO 2015 Investor Briefing
 Merck ASCO 2015 Investor Briefing Forward-Looking Statement This presentation includes forward-looking statements within the meaning of the safe harbor provisions of the U.S. Private Securities Litigation
Merck ASCO 2015 Investor Briefing Forward-Looking Statement This presentation includes forward-looking statements within the meaning of the safe harbor provisions of the U.S. Private Securities Litigation
Attached from the following page is the press release made by BMS for your information.
 June 2, 2015 Phase I/II Opdivo (nivolumab) Trial Shows Bristol-Myers Squibb s PD-1 Immune Checkpoint Inhibitor is First to Demonstrate Anti-Tumor Activity In Patients With Hepatocellular Carcinoma (PRINCETON,
June 2, 2015 Phase I/II Opdivo (nivolumab) Trial Shows Bristol-Myers Squibb s PD-1 Immune Checkpoint Inhibitor is First to Demonstrate Anti-Tumor Activity In Patients With Hepatocellular Carcinoma (PRINCETON,
Challenges in Distinguishing Clinical Signals to Support Development Decisions: Case Studies
 Challenges in Distinguishing Clinical Signals to Support Development Decisions: Case Studies David Feltquate MD, PhD Head of Early Clinical Development, Oncology Bristol-Myers Squibb, Princeton, NJ Challenges
Challenges in Distinguishing Clinical Signals to Support Development Decisions: Case Studies David Feltquate MD, PhD Head of Early Clinical Development, Oncology Bristol-Myers Squibb, Princeton, NJ Challenges
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy. Raanan Berger MD PhD Sheba Medical Center, Israel
 Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CENTENE PHARMACY AND THERAPEUTICS DRUG REVIEW 3Q17 April May
 BRAND NAME Keytruda GENERIC NAME Pembrolizumab MANUFACTURER Merck & Co., Inc. DATE OF APPROVAL Non-small cell lung cancer (NSCLC) indication: May 10, 2017 Urothelial carcinoma indication: May 18, 2017
BRAND NAME Keytruda GENERIC NAME Pembrolizumab MANUFACTURER Merck & Co., Inc. DATE OF APPROVAL Non-small cell lung cancer (NSCLC) indication: May 10, 2017 Urothelial carcinoma indication: May 18, 2017
Weitere Kombinationspartner der Immunotherapie
 1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
News from ASCO. Niven Mehra, Medical Oncologist. Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital
 News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
Presenter Disclosure Information
 Presenter Disclosure Information Tara C. Gangadhar, M.D. The following relationships exist related to this presentation: Research funding (Institution): Incyte Corporation and Merck & Co., Inc Preliminary
Presenter Disclosure Information Tara C. Gangadhar, M.D. The following relationships exist related to this presentation: Research funding (Institution): Incyte Corporation and Merck & Co., Inc Preliminary
Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma
 Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Colon Cancer Update Christie J. Hilton, DO
 POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
Attached from the following page is the press release made by BMS for your information.
 June 2, 2015 Opdivo (nivolumab) Demonstrates Superior Survival Compared to Standard of Care (docetaxel) for Previously-Treated Squamous Non-Small Cell Lung Cancer in Phase III Trial (PRINCETON, NJ, May
June 2, 2015 Opdivo (nivolumab) Demonstrates Superior Survival Compared to Standard of Care (docetaxel) for Previously-Treated Squamous Non-Small Cell Lung Cancer in Phase III Trial (PRINCETON, NJ, May
Post-ASCO 2017 Cancer du sein Triple Négatif
 Post-ASCO 217 Cancer du sein Triple Négatif A.Ladjeroud, K.Bouzid Centre Pierre et Marie Curie- Alger Oran, 3 Septembre 217 Phase III Investigation of Neoadjuvant Carboplatin ± Veliparib in Combination
Post-ASCO 217 Cancer du sein Triple Négatif A.Ladjeroud, K.Bouzid Centre Pierre et Marie Curie- Alger Oran, 3 Septembre 217 Phase III Investigation of Neoadjuvant Carboplatin ± Veliparib in Combination
Opdivo. Opdivo (nivolumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.53 Subsection: Antineoplastic Agents Original Policy Date: January 16, 2015 Subject: Opdivo Page:
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.53 Subsection: Antineoplastic Agents Original Policy Date: January 16, 2015 Subject: Opdivo Page:
Immunotherapy in Colorectal cancer
 Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
The Immunotherapy of Oncology
 The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
The Current Status of Immune Checkpoint Inhibitors: Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb
 The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
May 31, NCCN Guidelines: T-Cell Lymphomas
 May 31, 2017 Maria Rivas, MD Senior Vice-President Global Medical Affairs Merck & Co. Kenilworth - Galloping Hill, +1 908 740 6533 K6-1624G maria.rivas1@merck.com NCCN Guidelines: T-Cell Lymphomas On behalf
May 31, 2017 Maria Rivas, MD Senior Vice-President Global Medical Affairs Merck & Co. Kenilworth - Galloping Hill, +1 908 740 6533 K6-1624G maria.rivas1@merck.com NCCN Guidelines: T-Cell Lymphomas On behalf
R&D Conference Call. CHUGAI PHARMACEUTICAL CO., LTD. Department Manager of Oncology Lifecycle Management Dept. Megumi Uzu.
 R&D Conference Call CHUGAI PHARMACEUTICAL CO., LTD. Department Manager of Oncology Lifecycle Management Dept. Megumi Uzu July 4, 2016 Forward-Looking Statements This presentation may include forward-looking
R&D Conference Call CHUGAI PHARMACEUTICAL CO., LTD. Department Manager of Oncology Lifecycle Management Dept. Megumi Uzu July 4, 2016 Forward-Looking Statements This presentation may include forward-looking
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Patient Selection: The Search for Immunotherapy Biomarkers
 Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
6/7/16. Melanoma. Updates on immune checkpoint therapies. Molecularly targeted therapies. FDA approval for talimogene laherparepvec (T- VEC)
") Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
PLENARY SESSION 1: CLINICAL TRIAL DESIGN IN AN ERA OF HORIZONTAL DRUG DEVELOPMENT Industry Perspective
 PLENARY SESSION 1: CLINICAL TRIAL DESIGN IN AN ERA OF HORIZONTAL DRUG DEVELOPMENT Industry Perspective Davy Chiodin, VP - Regulatory Science, QA and Compliance, Acerta Pharma (A Member of the AstraZeneca
PLENARY SESSION 1: CLINICAL TRIAL DESIGN IN AN ERA OF HORIZONTAL DRUG DEVELOPMENT Industry Perspective Davy Chiodin, VP - Regulatory Science, QA and Compliance, Acerta Pharma (A Member of the AstraZeneca
MELANOMA METASTASICO: NUEVAS COMBINACIONES. Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona
 MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
New experimental targets for gastric cancer Andrés Cervantes
 New experimental targets for gastric cancer Andrés Cervantes Professor of Medicine Outline Acquired capabilities of Cancer IGFR pathway PI3K-AKT-m-TOR pathway MET pathway FGFR pathway Check point inhibitors
New experimental targets for gastric cancer Andrés Cervantes Professor of Medicine Outline Acquired capabilities of Cancer IGFR pathway PI3K-AKT-m-TOR pathway MET pathway FGFR pathway Check point inhibitors
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
Cancer Immunotherapy Patient Forum. for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015
 Cancer Immunotherapy Patient Forum for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015 Biomarkers and Patient Selection Julie R. Brahmer, M.D. Director
Cancer Immunotherapy Patient Forum for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015 Biomarkers and Patient Selection Julie R. Brahmer, M.D. Director
Immunotherapy in head and neck cancer and MSI in solid tumors
 Immunotherapy in head and neck cancer and MSI in solid tumors Brian Hunis, MD, MBA Associate Medical Director, Memorial Cancer Institute. Hollywood, FL »No disclosures Objectives»Discuss the role of immunology
Immunotherapy in head and neck cancer and MSI in solid tumors Brian Hunis, MD, MBA Associate Medical Director, Memorial Cancer Institute. Hollywood, FL »No disclosures Objectives»Discuss the role of immunology
New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain
 New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain PHC 2018 - www.aphc.info EASL-EORTC Guidelines EASL EORTC Guidelines. J Hepatol. 2012;56:908-43. Systemic
New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain PHC 2018 - www.aphc.info EASL-EORTC Guidelines EASL EORTC Guidelines. J Hepatol. 2012;56:908-43. Systemic
Role of the Pathologist in Guiding Immuno-oncological Therapies. Scott Rodig MD, PhD
 Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate