Lymphoma Read with the experts
|
|
|
- Cecilia Merritt
- 6 years ago
- Views:
Transcription
1 Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology
2 Learning Objectives Recognize common pitfalls and artifacts in interpreting PET/CT in lymphoma Discuss and apply current recommendations for performing a standardized interpretation of PET/CT in response assessment of lymphoma Identify common patterns of spread by lymphoma and recognize subtypes of lymphoma that have variable or low FDG uptake
3 Case 1

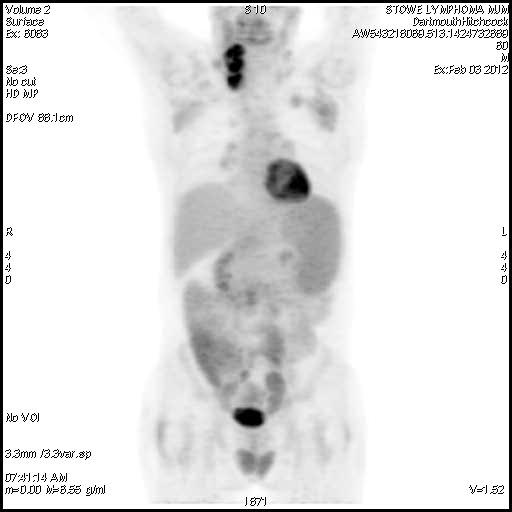
4 22 yom Large B-Cell Lymphoma PET-CT performed 2 days after starting chemotherapy
5
6 On this PET-CT performed 2 days after starting chemotherapy, the most likely explanation for the low FDG uptake in the mediastinal mass is: A. Large B-cell lymphomas are not reliably FDG avid B. The histology of the mediastinal mass was not adequately sampled prior to starting chemotherapy C. The bulk of the mass is comprised of inflammatory tissue D. FDG uptake is suppressed due to 2 days of chemotherapy
7 ?
8 On this PET-CT performed 2 days after starting chemotherapy, the most likely explanation for the low FDG uptake in the mediastinal mass is: A. Large B-cell lymphomas are not reliably FDG avid B. The histology of the mediastinal mass was not adequately sampled prior to starting chemotherapy C. The bulk of the mass is comprised of inflammatory tissue D. FDG uptake is suppressed due to 2 days of chemotherapy

9 22 yom Large B-Cell Lymphoma Restaging PET-CT after 6 cycles of chemotherapy
10
11
12 Restaging PET/CT after 6 cycles of chemotherapy


13 Baseline CT Restaging PET/CT Post 6 cycles of chemo
14 ?
15 The most likely explanation for the high FDG uptake in the residual mediastinal mass is: A. Thymic hyperplasia B. Metastatic lesion from another new primary tumor C. Post-chemotherapy inflammation D. Residual active lymphoma
16 The most likely explanation for the high FDG uptake in the residual mediastinal mass is: A. Thymic hyperplasia B. Metastatic lesion from another new primary tumor C. Post-chemotherapy inflammatory tissue D. Residual active lymphoma
17 Mini-sternotomy after PET-CT Final pathology: Rests of normal thymic tissue No lymphoma present in specimen Findings at pathology consistent with thymic hyperplasia

18 22 yom Large B- Cell Lymphoma Follow-up PET-CT 3 months post sternotomy
19
20
21 3 months after surgical excision with no further treatment: PET Interpretation: No active lymphoma
22 Case 1 Teaching Points FDG avid hyperplastic thymic tissue is commonly seen in children and young adults in the early months following completion of chemotherapy As the thymus normally involutes with aging, the morphologic appearance of thymic hyperplasia can be quite variable ranging from homogeneous and curvilinear, to heterogenous, patchy, asymmetric, and focal.
23 Case 1 Teaching Points Lymphomas can arise within or near the thymus. In such cases, residual active lymphoma cannot always be excluded as the cause of a post-chemotherapy residual hypermetabolic mass without surgical or biopsy proof. While uncommon, high FDG uptake in a postchemotherapy residual mass may be due to inflammation


24 14 year old with anaplastic lymphoma Baseline 4 months post-chemo (NED)
25 Post - Chemotherapy Thymic Hyperplasia
26 Post - Chemotherapy Thymic Hyperplasia
27 Post - Chemotherapy Thymic Hyperplasia
28 Recurrent Lymphoma and Thymic Hyperplasia

29 Recurrent Lymphoma and Thymic Hyperplasia
30 Recurrent Lymphoma and Thymic Hyperplasia
31 Thymus Activity on PET The degree of FDG uptake in thymic hyperplasia is variable but typically greater than or equal to liver activity
32 Case 2
33 History 52-year-old woman with Hodgkin lymphoma referred for a restaging PET/CT after 2 cycles of chemotherapy
34 Baseline Post 2 cycles chemotherapy Marrow Bx: +Diffuse Infiltration? Worse, Stable, Better?
35 Based on the images shown, the BEST interpretation of the PET findings is: A. Worsening of active lymphoma B. Stable active lymphoma C. Improved but residual active lymphoma D. Resolved, no active lymphoma E. Indeterminate for residual active lymphoma

36 Based on the images shown, the BEST interpretation of the PET findings is: A. Worsening of active lymphoma B. Stable active lymphoma C. Improved but residual active lymphoma D. Resolved, no active lymphoma E. Indeterminate for residual active lymphoma
37 Baseline PET/CT Post 2 cycles chemotherapy
38 Baseline L2 body Post- 2 cycles chemo

39 Baseline L2 body Post- 2 cycles chemo
40 Baseline L2 body Post- 2 cycles chemo
41 Baseline para-aortic node Post- 2 cycles chemo
42 Baseline para-aortic node Post- 2 cycles chemo
43 Baseline para-aortic node Post- 2 cycles chemo
44 Based on the images shown, the BEST interpretation of the PET findings is: A. Improved but residual active lymphoma in the left paraaortic lymph node B. Improved but residual active lymphoma in the L4 vertebral body C. No active lymphoma in the L4 vertebral body nor in the left paraaortic lymph node. D. Worsening of active lymphoma (treatment failure)
45 Based on the images shown, the BEST interpretation of the PET findings is: A. Improved but residual active lymphoma in the left paraaortic lymph node B. Improved but residual active lymphoma in the L4 vertebral body C. No active lymphoma in the L4 vertebral body nor in the left paraaortic lymph node. Reactive marrow hyperplasia in the skeleton that was not involved by lymphoma. D. Worsening of active lymphoma (treatment failure)
46 Case 2 Final Diagnosis No active lymphoma in the L4 vertebral body nor in the left paraaortic lymph node. Marrow hyperplasia throughout the skeleton.


47 61F, Hodgkin Lymphoma Baseline Post 2 cycles chemo Post 6 cycles chemo Marrow Bx: +Diffuse Infiltration Treated lesions and Reactive Marrow Probably no active disease Marrow Bx: Negative No active disease
48 Case 2 Teaching Points Marrow hyperplasia on PET/CT is commonly seen in patients receiving granulocyte colony stimulating factor (GCSF) which is given concurrently with chemotherapy. Rebound marrow hyperplasia on PET/CT can also be seen in the early weeks to months after completing chemotherapy.
49 Case 2 Teaching Points The presence of diffuse marrow activity on a followup PET/CT should not be misinterpreted as tumor involvement, particularly when all previously known sites of disease have resolved.

50 Non-Hodgkin s Lymphoma Restaging
51

52 Marrow and Splenic Hyperplasia due to colony stimulating factors
53 PET/CT Initial Staging NSCLC Diffuse marrow activity presumed due to tumor GCSF production

54 Baseline PET/CT Post 4 cycles chemotherapy
55 Baseline PET/CT Post 4 cycles chemotherapy
56 Case 3

57 52-year-old with non-small cell lung cancer undergoing presurgical evaluation
58
59
60
61
62
63
64
65
66
67 The BEST interpretation of the PET findings is: A. Right lung cancer and a second primary neoplastic process such as lymphoma involving the left axilla B. Right lung cancer and unrelated inflammatory process involving the left axilla and left deltoid C. Right lung cancer and contralateral left axillary nodal metastases D. Right lung cancer and infiltrated dose in the left arm
68 The BEST interpretation of the PET findings is: A. Right lung cancer and a second primary neoplastic process such as lymphoma involving the left axilla B. Right lung cancer and unrelated inflammatory process involving the left axilla and left deltoid C. Right lung cancer and contralateral left axillary nodal metastases D. Right lung cancer and infiltrated dose in the left arm
69 Case 3 Diagnosis Right lung cancer and unrelated inflammatory process involving the left axilla and left deltoid. The patient had influenza vaccination in the left deltoid 3 days prior to the PET/CT

70 Flu shot in left arm 3 days before PET/CT
71 Case 3 Teaching Points Recent vaccinations can result in FDG uptake at the injection site and within regional lymph nodes The regional lymph nodes may or may not appear pathologically enlarged Dose infiltration can result in FDG uptake within the draining sentinel lymph nodes on the side of injection. The lymph nodes are typically NOT enlarged and FDG uptake within lymphatic vessels may be seen distal to the injection site.

72 Dose infiltration in right antecubital fossa
73 Follicular lymphoma in left arm and axilla
74 Case 4

75 42 yow Non-Hodgkin s Lymphoma Baseline 6 cycles

76 42 yow Non-Hodgkin s Lymphoma Baseline 6 cycles
77 42 yow Non-Hodgkin s Lymphoma Baseline 6 cycles
78 42 yow Non-Hodgkin s Lymphoma Baseline 6 cycles
79 After 6 cycles of chemotherapy, which of the following is the BEST overall impression of the PET-CT findings: A. No active lymphoma B. Indeterminate for residual active lymphoma C. Suspicious for residual active lymphoma D. New marrow involvement by lymphoma
80 After 6 cycles of chemotherapy, which of the following is the BEST overall impression of the PET-CT findings: a. No active lymphoma b. Indeterminate for residual active lymphoma c. Suspicious for residual active lymphoma d. New marrow involvement by lymphoma
81 42 yow Non-Hodgkin s Lymphoma Baseline 6 cycles 5weeks later Indeterminate

82 42 yow Non-Hodgkin s Lymphoma Baseline 6 cycles 5weeks later
83 42 yow Non-Hodgkin s Lymphoma Baseline 6 cycles 5weeks later
84 42 yow Non-Hodgkin s Lymphoma Baseline 6 cycles 5weeks later?
85 5 weeks after the post cycle 6 PET-CT, which of the following is the BEST overall impression of the PET-CT findings: A. No active lymphoma B. Indeterminate for recurrent active lymphoma C. Recurrent active lymphoma D. New marrow involvement by lymphoma
86 5 weeks after the post cycle 6 PET-CT, which of the following is the BEST overall impression of the PET-CT findings: A. No active lymphoma B. Indeterminate for recurrent active lymphoma C. Recurrent active lymphoma D. New marrow involvement by lymphoma
87 NCCN recommends using which of the following PET imaging criteria to assess treatment response and determine further treatment options in Hodgkin lymphoma? a. PERCIST b. International working group response criteria c. Standardized uptake value criteria d. Deauville criteria e. None of the above: interpretation criteria are not included in NCCN guidelines
88 NCCN recommends using which of the following PET imaging criteria to assess treatment response and determine further treatment options in Hodgkin lymphoma? a. PERCIST b. International working group response criteria c. Standardized uptake value criteria d. Deauville criteria e. None of the above: interpretation criteria are not included in NCCN guidelines
89 Deauville Criteria for PET Guided Response Assessment of Lymphoma
90 Deauville Criteria for PET Guided Response Assessment of Lymphoma

91 Non-Hodgkin s Lymphoma Baseline 6 cycles 5weeks later Deauville 3 or 4 Deauville 4 or 5
92 Non-Hodgkin s Lymphoma Baseline 2 cycles 6 cycles
93 Non-Hodgkin s Lymphoma Baseline 2 cycles 6 cycles
94 Non-Hodgkin s Lymphoma Baseline 2 cycles 6 cycles

95 Non-Hodgkin s Lymphoma Baseline 2 cycles 6 cycles

96 Non-Hodgkin s Lymphoma Baseline 2 cycles 6 cycles

97 Bleomycin induced pneumonitis Baseline 2 cycles 6 cycles Deauville 2 Deauville 2, X
98 The Deauville criteria is included in the NCCN guidelines for BOTH Hodgkin and Non-Hodgkin lymphoma management algorithms? a. True b. False
99 The Deauville criteria is included in the NCCN guidelines for BOTH Hodgkin and Non-Hodgkin lymphoma management algorithms? a. True b. False The Deauville criteria is included in the NCCN guidelines for Hodgkin and DLBCL (2015)

100 The Deauville criteria is included in the NCCN guidelines for Hodgkin and DLBCL (2015)

101 The Deauville criteria is included in the NCCN guidelines for Hodgkin and DLBCL (2015)
102 Which one of the following types of lymphomas is the LEAST likely to be 18 F-FDG-avid? a. Diffuse large B cell b. Follicular c. Marginal zone/ mucosa-associated lymphoid tissue d. Hodgkin e. Mantle Cell
103 Which one of the following types of lymphomas is the LEAST likely to be 18 F-FDG-avid? a. Diffuse large B cell b. Follicular c. Marginal zone/ mucosa-associated lymphoid tissue d. Hodgkin e. Mantle cell
104 Newly Diagnosed MALT Lymphoma of the Stomach
105 Newly Diagnosed MALT Lymphoma of the Stomach
106 Newly Diagnosed MALT Lymphoma of the Stomach
107 Case 5
108 MJM 60 yo male presented with increasing fatique, night sweats and adenopathy. Labs revealed elevated WBC with lymphocyte predominance, anemia, thrombocytopenia and elevated LDH. Flow cytometry confirmed CLL On exam patient had diffuse adenopathy and dominant neck mass PET scan done to help stage disease and guide biopsy
109
110
111 MJM Biopsy of neck mass confirmed transformation of CLL to DLBCL (Richter s Transformation). Patient received 4 cycles of RCHOP with resolution of all PET avid adenopathy Autologous stem cell transplant In remission after 3 years Goal of treatment was to cure the aggressive lymphoma; CLL is likely to relapse in future
112 Thank you and Questions?
113 Bonus Cases (Interpretation Pitfalls)
114 42 yo man, mediastinal adenopathy, suspected lymphoma

115 Final Diagnosis: Disseminated Sarcoidosis
116 19 yow with fevers, night sweats, remote h/o Hodgkin s

117 Acute EBV Infection (confirmed by serum titer)

118 Repeat (new baseline) PET-CT 6 months post EBV Infection

119 PET/CT Restaging Lymphoma??Recurrence
120
121
122
123
124
125

126 PET/CT Restaging Lymphoma Brown Adipose Tissue
127 Brown Adipose Tissue Exists in animals, infants, and adults. Mitochondria rich and highly vascular Sympathetic nervous system activity significantly increases glucose uptake by BAT. FDG uptake is felt to be due to non-shivering thermoregulation caused by sympathetic stimulation BAT on PET scans is more commonly seen in younger, thin, women and seen more frequently during winter months
128 Brown Adipose Tissue FDG uptake in brown adipose tissue can be dramatically reduced by pre-medication with a benzodiazepine or beta blocker Consider pre-medication in any young patient (up to age 40) Oral alprazolam 0.5 mg or diazepam 5 mg given 60 minutes prior to FDG injection CT part of PET-CT helps avoid misinterpretations
129 Thank you
Update in Lymphoma Imaging
 Update in Lymphoma Imaging Victorine V. Muse, MD Lymphoma Update in Lymphoma Imaging Victorine V Muse, MD Heterogeneous group of lymphoid neoplasms divided into two broad histological categories Hodgkin
Update in Lymphoma Imaging Victorine V. Muse, MD Lymphoma Update in Lymphoma Imaging Victorine V Muse, MD Heterogeneous group of lymphoid neoplasms divided into two broad histological categories Hodgkin
Lugano classification: Role of PET-CT in lymphoma follow-up
 CAR Educational Exhibit: ID 084 Lugano classification: Role of PET-CT in lymphoma follow-up Charles Nhan 4 Kevin Lian MD Charlotte J. Yong-Hing MD FRCPC Pete Tonseth 3 MD FRCPC Department of Diagnostic
CAR Educational Exhibit: ID 084 Lugano classification: Role of PET-CT in lymphoma follow-up Charles Nhan 4 Kevin Lian MD Charlotte J. Yong-Hing MD FRCPC Pete Tonseth 3 MD FRCPC Department of Diagnostic
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center
 LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
Understanding your diagnosis. Dr Graham Collins Consultant Haemtologist Oxford University Hospitals
 Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010
 Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Abstracting Hematopoietic Neoplasms
 CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
Hodgkin's Lymphoma. Symptoms. Types
 Hodgkin's lymphoma (Hodgkin's disease) usually develops in the lymphatic system, a part of the body's immune system. This system carries disease-fighting white blood cells throughout the body. Lymph tissue
Hodgkin's lymphoma (Hodgkin's disease) usually develops in the lymphatic system, a part of the body's immune system. This system carries disease-fighting white blood cells throughout the body. Lymph tissue
PET/CT F-18 FDG. Objectives. Basics of PET/CT Imaging. Objectives. Basic PET imaging
 Basics of PET/CT Imaging Kevin Robinson, DO Department of Radiology Michigan State University Objectives Basic PET imaging Evaluating the therapeutic response Evaluating the big 5 Lymphoma Breast Lung
Basics of PET/CT Imaging Kevin Robinson, DO Department of Radiology Michigan State University Objectives Basic PET imaging Evaluating the therapeutic response Evaluating the big 5 Lymphoma Breast Lung
L hyperfixation dans le suivi des lymphomes représente-t-elle toujours une maladie active?
 L hyperfixation dans le suivi des lymphomes représente-t-elle toujours une maladie active? Thierry Vander Borght UCL Mont-Godinne, Belgique FDG-PET in Lymphoma: Mont-Godinne Experience 03/2000 10/2002:
L hyperfixation dans le suivi des lymphomes représente-t-elle toujours une maladie active? Thierry Vander Borght UCL Mont-Godinne, Belgique FDG-PET in Lymphoma: Mont-Godinne Experience 03/2000 10/2002:
Clinical summary. Male 30 year-old with past history of non-seminomous germ cell tumour. Presents with retroperitoneal lymphadenopathy on CT.
 Clinical summary Male 30 year-old with past history of non-seminomous germ cell tumour. Presents with retroperitoneal lymphadenopathy on CT. For restaging PET/CT. PET/CT findings No significant FDG uptake
Clinical summary Male 30 year-old with past history of non-seminomous germ cell tumour. Presents with retroperitoneal lymphadenopathy on CT. For restaging PET/CT. PET/CT findings No significant FDG uptake
Indolent Lymphomas. Dr. Melissa Toupin The Ottawa Hospital
 Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Dr Sneha Shah Tata Memorial Hospital, Mumbai.
 Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
Lymphatic System Disorders
 Lymphatic System Disorders Lymphomas Malignant neoplasms involving lymphocyte proliferation in lymph nodes Specific causes not identified // Higher risk in adults who received radiation during childhood
Lymphatic System Disorders Lymphomas Malignant neoplasms involving lymphocyte proliferation in lymph nodes Specific causes not identified // Higher risk in adults who received radiation during childhood
ROLE OF PET-CT IN BREAST CANCER, GUIDELINES AND BEYOND. Prof Jamshed B. Bomanji Institute of Nuclear Medicine UCL Hospitals London
 ROLE OF PET-CT IN BREAST CANCER, GUIDELINES AND BEYOND Prof Jamshed B. Bomanji Institute of Nuclear Medicine UCL Hospitals London CANCER Key facts Estimated 15.2 million new cases per year in 2015 worldwide
ROLE OF PET-CT IN BREAST CANCER, GUIDELINES AND BEYOND Prof Jamshed B. Bomanji Institute of Nuclear Medicine UCL Hospitals London CANCER Key facts Estimated 15.2 million new cases per year in 2015 worldwide
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
Breast Imaging: Multidisciplinary Approach. Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina
 Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113)
") Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Overview of Cutaneous Lymphomas: Diagnosis and Staging. Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology
 Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
Testicular relapse of non-hodgkin Lymphoma noted on FDG-PET
 Testicular relapse of non-hodgkin Lymphoma noted on FDG-PET Stephen D. Scotti 1*, Jennifer Laudadio 2 1. Department of Radiology, North Carolina Baptist Hospital, Winston-Salem, NC, USA 2. Department of
Testicular relapse of non-hodgkin Lymphoma noted on FDG-PET Stephen D. Scotti 1*, Jennifer Laudadio 2 1. Department of Radiology, North Carolina Baptist Hospital, Winston-Salem, NC, USA 2. Department of
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
New Visions in PET: Surgical Decision Making and PET/CT
 New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
Clinical indications for positron emission tomography
 Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Lymphoma: The Basics. Dr. Douglas Stewart
 Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lymphatic system component
 Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
Yiyan Liu. 1. Introduction
 AIDS Research and Treatment Volume 2012, Article ID 764291, 6 pages doi:10.1155/2012/764291 Clinical Study Concurrent FDG Avid Nasopharyngeal Lesion and Generalized Lymphadenopathy on PET-CT Imaging Is
AIDS Research and Treatment Volume 2012, Article ID 764291, 6 pages doi:10.1155/2012/764291 Clinical Study Concurrent FDG Avid Nasopharyngeal Lesion and Generalized Lymphadenopathy on PET-CT Imaging Is
PET-imaging: when can it be used to direct lymphoma treatment?
 PET-imaging: when can it be used to direct lymphoma treatment? Luca Ceriani Nuclear Medicine and PET-CT centre Oncology Institute of Southern Switzerland Bellinzona Disclosure slide I declare no conflict
PET-imaging: when can it be used to direct lymphoma treatment? Luca Ceriani Nuclear Medicine and PET-CT centre Oncology Institute of Southern Switzerland Bellinzona Disclosure slide I declare no conflict
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
Aggressive Lymphomas - Current. Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre
 Aggressive Lymphomas - Current Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre Conflicts of interest I have no conflicts of interest to declare Outline What does aggressive lymphoma
Aggressive Lymphomas - Current Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre Conflicts of interest I have no conflicts of interest to declare Outline What does aggressive lymphoma
Change Summary - Form 2018 (R3) 1 of 12
 1 of 12") Summary - Form 2018 (R3) 1 of 12 Form Question Number (r3) Type Description New Text Previous Text Today's date was removed 2018 N/A Today's Date Removed from Key Fields 2018 N/A HCT Type 2018 N/A Product
Summary - Form 2018 (R3) 1 of 12 Form Question Number (r3) Type Description New Text Previous Text Today's date was removed 2018 N/A Today's Date Removed from Key Fields 2018 N/A HCT Type 2018 N/A Product
ASPS Recommended Insurance Coverage Criteria for Third- Party Payers
 ASPS Recommended Insurance Coverage Criteria for Third- Party Payers Breast Implant Associated Anaplastic Large Cell Lymphoma BACKGROUND Anaplastic Large Cell Lymphoma (ALCL) is a rare type of cancer of
ASPS Recommended Insurance Coverage Criteria for Third- Party Payers Breast Implant Associated Anaplastic Large Cell Lymphoma BACKGROUND Anaplastic Large Cell Lymphoma (ALCL) is a rare type of cancer of
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL RESPONSE ASSESSMENT LYMPHOMA CHAPTER 11B REVISED: SEPTEMBER 2016
 MANUAL RESPONSE ASSESSMENT LYMPHOMA CHAPTER 11B REVISED: SEPTEMBER 2016") LYMPHOMA Definitions of Response According to Non Hodgkin s Lymphoma (NHL) Criteria Listed below is the new NCI Lymphoma criteria for evaluation and endpoint definitions for Non Hodgkin s Lymphoma response
LYMPHOMA Definitions of Response According to Non Hodgkin s Lymphoma (NHL) Criteria Listed below is the new NCI Lymphoma criteria for evaluation and endpoint definitions for Non Hodgkin s Lymphoma response
Sarajevo (Bosnia Hercegivina) Monday June :30-16:15. PET/CT in Lymphoma
 Monday June :30-16:15. PET/CT in Lymphoma") Sarajevo (Bosnia Hercegivina) Monday June 16 2013 15:30-16:15 PET/CT in Lymphoma FDG-avidity Staging (nodal & extra nodal) Response evaluation Early assessment during treatment / interim (ipet) Remission
Sarajevo (Bosnia Hercegivina) Monday June 16 2013 15:30-16:15 PET/CT in Lymphoma FDG-avidity Staging (nodal & extra nodal) Response evaluation Early assessment during treatment / interim (ipet) Remission
STAGING AND FOLLOW-UP STRATEGIES
 ATHENS 4-6 October 2018 European Society of Urogenital Radiology STAGING AND FOLLOW-UP STRATEGIES Ahmet Tuncay Turgut, MD Professor of Radiology Hacettepe University, Faculty of Medicine Ankara 2nd ESUR
ATHENS 4-6 October 2018 European Society of Urogenital Radiology STAGING AND FOLLOW-UP STRATEGIES Ahmet Tuncay Turgut, MD Professor of Radiology Hacettepe University, Faculty of Medicine Ankara 2nd ESUR
Radiation and Hodgkin s Disease: A Changing Field. Sravana Chennupati Radiation Oncology PGY-2
 Radiation and Hodgkin s Disease: A Changing Field Sravana Chennupati Radiation Oncology PGY-2 History of Present Illness 19 yo previously healthy male college student began having pain in his R shoulder
Radiation and Hodgkin s Disease: A Changing Field Sravana Chennupati Radiation Oncology PGY-2 History of Present Illness 19 yo previously healthy male college student began having pain in his R shoulder
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
FDG PET for therapy response assessment in lymphoma: Beyond Lugano Classification
 FDG PET for therapy response assessment in lymphoma: Beyond Lugano Classification Yan Xuexian, MD, DABNM Department of Nuclear Medicine and PET, SGH National Cancer Center Singapore Duke-NUS Medical School
FDG PET for therapy response assessment in lymphoma: Beyond Lugano Classification Yan Xuexian, MD, DABNM Department of Nuclear Medicine and PET, SGH National Cancer Center Singapore Duke-NUS Medical School
Hematologic Malignancies of the Liver : Spectrum of Disease. Zhou Jian
 Hematologic Malignancies of the Liver : Spectrum of Disease Zhou Jian 2015-7-8 Hematologic malignancies include a wide spectrum of lymphoproliferative and myeloproliferative disorders with nodal and extranodal
Hematologic Malignancies of the Liver : Spectrum of Disease Zhou Jian 2015-7-8 Hematologic malignancies include a wide spectrum of lymphoproliferative and myeloproliferative disorders with nodal and extranodal
The Role of PET / CT in Lung Cancer Staging
 July 2004 The Role of PET / CT in Lung Cancer Staging Vlad Vinarsky, Harvard Medical School Year IV Patient AM HPI: 81 yo F p/w hemoptysis x 1 month LLL lesion on CXR, not responsive to Abx 35 pack-year
July 2004 The Role of PET / CT in Lung Cancer Staging Vlad Vinarsky, Harvard Medical School Year IV Patient AM HPI: 81 yo F p/w hemoptysis x 1 month LLL lesion on CXR, not responsive to Abx 35 pack-year
Mimics of Lymphoma in Routine Biopsies. Mixed follicular and paracortical hyperplasia. Types of Lymphoid Hyperplasia
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes on the next page
 COME HOME Non-Hodgkin pathway development worksheet, v6 September 2014 1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes
COME HOME Non-Hodgkin pathway development worksheet, v6 September 2014 1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Positron Emission Tomography in Lung Cancer
 May 19, 2003 Positron Emission Tomography in Lung Cancer Andrew Wang, HMS III Patient DD 53 y/o gentleman presented with worsening dyspnea on exertion for the past two months 30 pack-year smoking Hx and
May 19, 2003 Positron Emission Tomography in Lung Cancer Andrew Wang, HMS III Patient DD 53 y/o gentleman presented with worsening dyspnea on exertion for the past two months 30 pack-year smoking Hx and
NCCN Practice Guidelines Narrative Summary of Indications for FDG PET and PET/CT
 NCCN Practice Guidelines Narrative Summary of Indications for FDG PET and PET/CT NCCN guidelines were reviewed on 2/14/2016 for utilization of 18F-fluorodeoxyglucose (FDG) PET and PET/CT (available at:
NCCN Practice Guidelines Narrative Summary of Indications for FDG PET and PET/CT NCCN guidelines were reviewed on 2/14/2016 for utilization of 18F-fluorodeoxyglucose (FDG) PET and PET/CT (available at:
FDG PET/CT in Lung Cancer Read with the experts. Homer A. Macapinlac, M.D.
 FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
Head and Neck: DLBCL
 Head and Neck: DLBCL Nikhil G. Thaker Chelsea C. Pinnix Valerie K. Reed Bouthaina S. Dabaja Department of Radiation Oncology MD Anderson Cancer Center Case 60 yo male Presented with right cervical LAD
Head and Neck: DLBCL Nikhil G. Thaker Chelsea C. Pinnix Valerie K. Reed Bouthaina S. Dabaja Department of Radiation Oncology MD Anderson Cancer Center Case 60 yo male Presented with right cervical LAD
Pediatric Oncology. Vlad Radulescu, MD
 Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
Patient underwent hemicolectomy: 7 x 4.5 cm intusscepted segment of ileum in colon - mucosal
 Extranodal Lymphomas Rena Buckstein Odette Cancer Center Case: JT 69 yo male COO software company PMHx: basal cell back, cholesterol Presents to ER with severe abdominal pain, bloody diarrhea x 2d In ER
Extranodal Lymphomas Rena Buckstein Odette Cancer Center Case: JT 69 yo male COO software company PMHx: basal cell back, cholesterol Presents to ER with severe abdominal pain, bloody diarrhea x 2d In ER
Patient Case Studies & Panel Discussion
 Patient Case Studies & Panel Discussion Panelists: Jeremy S. Abramson, MD, Massachusetts General Hospital Cancer Center; Ranjana H. Advani, MD, Stanford Cancer Institute; Andrew D. Zelenetz, MD, PhD, Memorial
Patient Case Studies & Panel Discussion Panelists: Jeremy S. Abramson, MD, Massachusetts General Hospital Cancer Center; Ranjana H. Advani, MD, Stanford Cancer Institute; Andrew D. Zelenetz, MD, PhD, Memorial
ARRO Case: Pediatric High Risk Classical Hodgkin Lymphoma
 ARRO Case: Pediatric High Risk Classical Hodgkin Lymphoma Steven Seyedin, MD (PGY-3) Faculty Advisor: Dr. John Buatti, MD, FASTRO Department of Radiation Oncology University of Iowa Hospital and Clinics
ARRO Case: Pediatric High Risk Classical Hodgkin Lymphoma Steven Seyedin, MD (PGY-3) Faculty Advisor: Dr. John Buatti, MD, FASTRO Department of Radiation Oncology University of Iowa Hospital and Clinics
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Diagnosis and patient pathway in lymphomas
 The Royal Marsden Diagnosis and patient pathway in lymphomas Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Change Presentation title and date in Footer dd.mm.yyyy
The Royal Marsden Diagnosis and patient pathway in lymphomas Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Change Presentation title and date in Footer dd.mm.yyyy
Pathology #07. Hussein Al-Sa di. Dr. Sohaib Al-Khatib. Mature B-Cell Neoplasm. 0 P a g e
 Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
NAACCR Webinar Series 1
 COLLECTING CANCER DATA: HEMATOPOIETIC AND LYMPHOID NEOPLASMS Jim Hofferkamp, CTR (jhofferkam@naaccr.org) Shannon Vann, CTR (svann@naaccr.org) Q&A Please submit all questions concerning webinar content
COLLECTING CANCER DATA: HEMATOPOIETIC AND LYMPHOID NEOPLASMS Jim Hofferkamp, CTR (jhofferkam@naaccr.org) Shannon Vann, CTR (svann@naaccr.org) Q&A Please submit all questions concerning webinar content
Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma:
 1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
UK Musculoskeletal Oncology: Something for All Ages. Lars Wagner, MD Pediatric Hematology/Oncology University of Kentucky
 UK Musculoskeletal Oncology: Something for All Ages Lars Wagner, MD Pediatric Hematology/Oncology University of Kentucky Pediatric-Type Sarcomas of Bone and Soft Tissue The incidence of sarcoma continues
UK Musculoskeletal Oncology: Something for All Ages Lars Wagner, MD Pediatric Hematology/Oncology University of Kentucky Pediatric-Type Sarcomas of Bone and Soft Tissue The incidence of sarcoma continues
Indium-111 Zevalin Imaging
 Indium-111 Zevalin Imaging Background: Most B lymphocytes (beyond the stem cell stage) contain a surface antigen called CD20. It is possible to kill these lymphocytes by injecting an antibody to CD20.
Indium-111 Zevalin Imaging Background: Most B lymphocytes (beyond the stem cell stage) contain a surface antigen called CD20. It is possible to kill these lymphocytes by injecting an antibody to CD20.
2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA
 2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA SUSQUEHANNA HEALTH David B. Nagel, M.D. April 11, 2008 Hodgkin s lymphoma was first described by Thomas Hodgkin in 1832. It remained an incurable malignancy until
2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA SUSQUEHANNA HEALTH David B. Nagel, M.D. April 11, 2008 Hodgkin s lymphoma was first described by Thomas Hodgkin in 1832. It remained an incurable malignancy until
Zydelig. Zydelig (idelalisib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.49 Subject: Zydelig Page: 1 of 6 Last Review Date: June 22, 2018 Zydelig Description Zydelig (idelalisib)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.49 Subject: Zydelig Page: 1 of 6 Last Review Date: June 22, 2018 Zydelig Description Zydelig (idelalisib)
Mimics of Lymphoma in Routine Biopsies. I have nothing to disclose regarding the information to be reported in this talk.
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
What is a hematological malignancy? Hematology and Hematologic Malignancies. Etiology of hematological malignancies. Leukemias
 Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies
 Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Regression of Advanced Gastric MALT Lymphoma after the Eradication of Helicobacter pylori
 Gut and Liver, Vol. 6, No. 2, April 2012, pp. 270-274 CASE REPORT Regression of Advanced Gastric MALT Lymphoma after the Eradication of Helicobacter pylori Soo-Kyung Park, Hwoon-Yong Jung, Do Hoon Kim,
Gut and Liver, Vol. 6, No. 2, April 2012, pp. 270-274 CASE REPORT Regression of Advanced Gastric MALT Lymphoma after the Eradication of Helicobacter pylori Soo-Kyung Park, Hwoon-Yong Jung, Do Hoon Kim,
Non-Hodgkin lymphoma
 Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Indolent Lymphomas: Current. Dr. Laurie Sehn
 Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Approach to Core Biopsy Specimens
 BDIAP 108th Symposium on Haematopathology Joint Meeting of the BDIAP and BLPG at-bristol, Anchor Road, Harbourside, Bristol BS1 5DB 15th - 17th May 2014 Approach to Core Biopsy Specimens Dr Stefan Dojcinov
BDIAP 108th Symposium on Haematopathology Joint Meeting of the BDIAP and BLPG at-bristol, Anchor Road, Harbourside, Bristol BS1 5DB 15th - 17th May 2014 Approach to Core Biopsy Specimens Dr Stefan Dojcinov
ISPUB.COM. Primary Cutaneous Anaplastic Large Cell Lymphoma Long-term Management with Low Dose Methotrexate. S Parker INTRODUCTION
 ISPUB.COM The Internet Journal of Dermatology Volume 7 Number 3 Primary Cutaneous Anaplastic Large Cell Lymphoma Long-term Management with Low Dose S Parker Citation S Parker.. The Internet Journal of
ISPUB.COM The Internet Journal of Dermatology Volume 7 Number 3 Primary Cutaneous Anaplastic Large Cell Lymphoma Long-term Management with Low Dose S Parker Citation S Parker.. The Internet Journal of
Non-Hodgkin Lymphoma. Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract.
 Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
Melanoma Quality Reporting
 Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
ACHIEVING EXCELLENCE IN ABSTRACTING: LYMPHOMA
 ACHIEVING EXCELLENCE IN ABSTRACTING: LYMPHOMA ACHIEVING EXCELLENCE IN ABSTRACTING LYMPHOMA Recoding Audit Performed in 2009 260 cases audited 17 data items audited per case 4420 possible discrepancies
ACHIEVING EXCELLENCE IN ABSTRACTING: LYMPHOMA ACHIEVING EXCELLENCE IN ABSTRACTING LYMPHOMA Recoding Audit Performed in 2009 260 cases audited 17 data items audited per case 4420 possible discrepancies
Aggressive NHL and Hodgkin Lymphoma. Dr. Carolyn Faught November 10, 2017
 Aggressive NHL and Hodgkin Lymphoma Dr. Carolyn Faught November 10, 2017 What does aggressive mean? Shorter duration of symptoms Generally need treatment at time of diagnosis Immediate, few days, few weeks
Aggressive NHL and Hodgkin Lymphoma Dr. Carolyn Faught November 10, 2017 What does aggressive mean? Shorter duration of symptoms Generally need treatment at time of diagnosis Immediate, few days, few weeks
Zydelig. Zydelig (idelalisib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.49 Subject: Zydelig Page: 1 of 6 Last Review Date: June 22, 2017 Zydelig Description Zydelig (idelalisib)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.49 Subject: Zydelig Page: 1 of 6 Last Review Date: June 22, 2017 Zydelig Description Zydelig (idelalisib)
Pediatric Lymphoma Update from the Children s Oncology Group
 Pediatric Lymphoma Update from the Children s Oncology Group Stephan D. Voss, MD, PhD Department of Radiology Boston Children s Hospital Harvard Medical School Staging Assessment Disclosures None Acknowledgements:
Pediatric Lymphoma Update from the Children s Oncology Group Stephan D. Voss, MD, PhD Department of Radiology Boston Children s Hospital Harvard Medical School Staging Assessment Disclosures None Acknowledgements:
FieldStrength. Leuven research is finetuning. whole body staging
 FieldStrength Publication for the Philips MRI Community Issue 40 May 2010 Leuven research is finetuning 3.0T DWIBS for whole body staging The University Hospital of Leuven is researching 3.0T whole body
FieldStrength Publication for the Philips MRI Community Issue 40 May 2010 Leuven research is finetuning 3.0T DWIBS for whole body staging The University Hospital of Leuven is researching 3.0T whole body
Understanding the Diagnostic and Prognostic Role of Imaging in the Evaluation of an Anterior Mediastinal Mass
 Understanding the Diagnostic and Prognostic Role of Imaging in the Evaluation of an Anterior Mediastinal Mass Daniel W. Kim, Harvard Medical School Year III Agenda Mediastinum Menu of tests Anatomy Normal
Understanding the Diagnostic and Prognostic Role of Imaging in the Evaluation of an Anterior Mediastinal Mass Daniel W. Kim, Harvard Medical School Year III Agenda Mediastinum Menu of tests Anatomy Normal
Deppen S, et al. Annals of Thoracic Surgery 2011;92:
 Deppen S, et al. Annals of Thoracic Surgery 2011;92:428-33. http://www.nationmaster.com/graph/ mor_his-mortality-histoplasmosis http://www.humirarems.com/brochure.aspx Baddley, John W., et al. Emerging
Deppen S, et al. Annals of Thoracic Surgery 2011;92:428-33. http://www.nationmaster.com/graph/ mor_his-mortality-histoplasmosis http://www.humirarems.com/brochure.aspx Baddley, John W., et al. Emerging
Dr. Noelle O Rourke Beatson Oncology Centre, Glasgow RADIOTHERAPY FOR LYMPHOMA???
 Dr. Noelle O Rourke Beatson Oncology Centre, Glasgow RADIOTHERAPY FOR LYMPHOMA??? History of Radiotherapy 1895 Rontgen describes X-rays 1896 Becquerel radioactivity 1905 Radiation is used to treat tumours
Dr. Noelle O Rourke Beatson Oncology Centre, Glasgow RADIOTHERAPY FOR LYMPHOMA??? History of Radiotherapy 1895 Rontgen describes X-rays 1896 Becquerel radioactivity 1905 Radiation is used to treat tumours
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Peripheral blood Pleural effusion in a cat
 Tools for the Diagnosis of Lymphoproliferative Diseases When is it difficult to diagnose lymphoproliferative disease? Persistent lymphocytosis consisting of small Lymph node aspirates containing an excess
Tools for the Diagnosis of Lymphoproliferative Diseases When is it difficult to diagnose lymphoproliferative disease? Persistent lymphocytosis consisting of small Lymph node aspirates containing an excess
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Lung Cancer Imaging. Terence Z. Wong, MD,PhD. Department of Radiology Duke University Medical Center Durham, NC 9/9/09
 Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
A CASE OF PRIMARY THYROID LYMPHOMA. Prof Dr.Dilek Gogas Yavuz Marmara University School of Medicine Endocrinology and Metabolism Istanbul, Turkey
 A CASE OF PRIMARY THYROID LYMPHOMA Prof Dr.Dilek Gogas Yavuz Marmara University School of Medicine Endocrinology and Metabolism Istanbul, Turkey 38 year old female She recognized a mass in her right neck
A CASE OF PRIMARY THYROID LYMPHOMA Prof Dr.Dilek Gogas Yavuz Marmara University School of Medicine Endocrinology and Metabolism Istanbul, Turkey 38 year old female She recognized a mass in her right neck
Sally Barrington Martin Hutchings
 Sally Barrington Martin Hutchings Therapeutic implications of BMI Bone marrow involvement means extranodal disease and by definition stage IV BMI detected by BMB is a poor prognostic feature in most lymphomas
Sally Barrington Martin Hutchings Therapeutic implications of BMI Bone marrow involvement means extranodal disease and by definition stage IV BMI detected by BMB is a poor prognostic feature in most lymphomas
IBD-Related Lymphoma
 IBD-Related Lymphoma Larry Burgart MD Staff Pathologist, Allina Health and Minnesota Gastroenterology Clinical Professor of Pathology, University of Minnesota College of Medicine IBD-Related Lymphoma
IBD-Related Lymphoma Larry Burgart MD Staff Pathologist, Allina Health and Minnesota Gastroenterology Clinical Professor of Pathology, University of Minnesota College of Medicine IBD-Related Lymphoma
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Lymphoma is a cancer that develops in the white blood cells (lymphocytes) of the lymphatic system, which is part of the body's immune system.
 of the lymphatic system, which is part of the body's immune system.") Scan for mobile link. Lymphoma Lymphoma is a cancer that develops in the white blood cells of the lymphatic system. Symptoms may include enlarged lymph nodes, unexplained weight loss, fatigue, night sweats
Scan for mobile link. Lymphoma Lymphoma is a cancer that develops in the white blood cells of the lymphatic system. Symptoms may include enlarged lymph nodes, unexplained weight loss, fatigue, night sweats