Head and Neck: DLBCL
|
|
|
- Coleen Warren
- 6 years ago
- Views:
Transcription
1 Head and Neck: DLBCL Nikhil G. Thaker Chelsea C. Pinnix Valerie K. Reed Bouthaina S. Dabaja Department of Radiation Oncology MD Anderson Cancer Center
2 Case 60 yo male Presented with right cervical LAD PE: large, palpable right neck mass in the submandibular region No other palpable adenopathy
3 PET/CT Scan

4 PET/CT Scan
5 PET/CT Scan
6 PET/CT Scan
7 PET/CT Scan
8 PET/CT Scan
9 Pathology Right excisional LN biopsy Diagnosis DIFFUSE LARGE B CELL LYMPHOMA, Germinal Center-type Ki-67: Greater than 95% Positive for CD45, CD20, PAX-5, CD-10, BCL-6, and CD79a Negative for CD3, CD5, pan keratin, HHV8, ALK-1, EBER, and MIM-1
10 NHL: Epidemiology >70,000 new cases of NHL per year in US ~19,000 estimated deaths NHL is 9 th leading cause of death in men and 6 th leading cause of death in women Most common subtype of NHL is DLBCL Median age at presentation: 60 40% with localized disease 40-50% with extranodal disease Common symptoms: painless LAD (axillary, inguinal, femoral), ~30% have B symptoms Indolent lymphoma: waxing and waning LAD
11 B Symptoms Any of the following: Fevers: T > 38 C (100.4 F) Night sweats (drenching) Weight loss: >10% loss over the past 6 months
12 DLBCL: Workup Excisional biopsy preferred Adequate immunophenotyping to establish diagnosis via IHC or flow cytometry IHC panel: CD20, CD3, CD5, CD10, CD45, BCL2, BCL6, Ki- 67, IRF/MUM1 Cell surface marker analysis by flow: CD45, CD3, CD5, CD19, CD10, CD20 In certain situations: Molecular analysis to detect gene rearrangements via FISH or IHC: BCL2, BCL6, MYC Cytogenetics or FISH: t(14;18), t(8;14), etc.
13 Biopsy Type of Biopsy Advantages Disadvantages FNA Core needle Excisional Easy Relatively painless Office-based procedure Very small needle Easy Relatively painless Office-based procedure Standard histopathology Able to assess tissue architecture Able to obtain cell surface markers Standard histopathology Able to assess tissue architecture Able to obtain cell surface markers Requires expert cytopathologist Unable to evaluate histology Slightly larger needle than FNA Requires procedure suite or OR Larger incision More painful Courtesy of G. Walker
14 DLBCL: Workup B symptoms (fevers, night sweats, weight loss) PE: performance status; attention to node-bearing sites, including waldeyer s ring; note size of liver and spleen. Labs: CBC with diff, LDH, CMP, uric acid, Hep B Imaging: CT of C/A/P with contrast, PET-CT scan Bone marrow biopsy Calculate International Prognostic Index (IPI) Consider: cardiac w/u (MUGU scan, echo) if giving anthracycline based regimen, pregnancy test, beta-2-microglobulin, head and neck MRI, discuss fertility and sperm banking, HIV test LP if paranasal sinus, testicular, epidural, bone marrow with large cell lymphoma, HIV lymphoma, or more than 2 extranodal sites with elevated LDH.
15 Lymphoma Histology B-cell DLBCL Follicular SLL/CLL Lymphoplasmacytic Plasma Cell / Myeloma Marginal zone B-cell Mantle Cell Burkitt s lymphoma Precursor B lymphoblastic T-cell Peripheral T-cell Precursor T lymphoblastic Mycosis Fungoides Anaplastic large cell Adult T-cell
16 Immunophenotype B-Cell: CD19+, CD20+ Mantle Cell: CD5+ Follicular: CD10+ (germinal center) MALT: CD5-, CD10-, CD23- T-Cell: CD2+, CD3+, CD7+, CD8+ Anaplastic large cell: CD30+
17 WHO Histology Indolent Aggressive Very Aggressive Follicular (G1-2) DLBCL Burkitt s Marginal zone Follicular (G3) Precursor B lymphoblastic MALT Mantle Precursor T lymphoblastic Mycosis fungoides Peripheral T cell NK Cell Anaplastic large cell CLL
18 Genotype Translocations t(8;14) Burkitt s lymphoma (c-myc) t(11;14) Mantle cell lymphoma (bcl-1) t(11;18) MALT lymphoma t(14;18) Follicular lymphoma (bcl-2)
19 Ann Arbor Staging I II III IV X E B/A Single lymph node group Multiple lymph node groups on same side diaphragm Multiple lymph node groups on both sides of diaphragm Multiple extranodal sites or lymph nodes and extranodal disease Bulk (> 10cm) Extranodal extension or single isolated site of extranodal disease B symptoms
20 Case 60 yo male Right cervical LAD in 5/2013 No B symptoms Bx: DLBCL Stage IA What else should we focus on in w/u?
21 International Prognostic Index (IPI) Score Age > 60 Performance status 2 LDH > normal Extranodal sites, > 1 Stage 3 or 4 Score Risk Group 5 Year OS (- R) 3 Year OS (+ R) 0-1 Low 76% 91% 2 Low-intermediate 51% 81% 3 High-intermediate 43% 65% 4-5 High 26% 59% Shipp et al NEJM 1993 Rule of thumb: for R-CHOP, add 15% to 5-year OS

22 60 yo male Right cervical LAD No B symptoms Good PS, normal LDH Bx: DLBCL Stage IA IPI = 0 Tx recs? Case
23 Case Treatment recommendations for non-bulky, stage I or II DLBLC, without adverse risk factors: R-CHOP x 3 cycles + RT Or R-CHOP x 6 cycles +/- RT
24 Chemotherapy Regimens in Lymphoma R-CHOP CVAD EPOCH ABVD BEACOPP COPP EBVP MOPP Stanford V rituximab, cyclophosphamide, adriamycin (hydroxydaunorubicin), vincristine (Oncovin), prednisone cyclophosphamide, vincristine, adriamycin, dexamethasone etoposide, prednisone, vincristine (Oncovin), cyclophosphamide, adriamycin (hydroxydaunorubicin) adriamycin, bleomycin, vinblastine, dacarbazine bleomycin, etoposide, doxorubicin (Adriamycin), cyclophosphamide, vincristine (Oncovin), procarbazine, prednisone cyclophosphamide, vincristine (Oncovin), procarbazine, prednisone epirubicin, bleomycin, vinblastine, prednisone mechlorethamine, vincristine (Oncovin), procarbazine, prednisone mechlorethamine, doxorubicin, vinblastine, vincristine, bleomycin, etoposide, prednisone
25 Treatment Summary: DLBCL DLBCL Stage I, II Stage III, IV IPI = 0 RCHOP x 6 or RCHOP x 3 + RT (30 Gy) IPI 0 RCHOP x 6 + RT (30Gy; 36 Gy if bulky; Gy if FDG avid) RCHOP x 6-8, RT in select cases (bulky, paraspinal, refractory, prep for SCT)




26 Treatment Recommendations? 60 yo male Stage IA DLBCL s/p 3 cycles R-CHOP PET CT and CT with contrast demonstrated complete response (CR)
27 If I have a CR, why do I also need RT?
28 Chemo vs. Chemo-RT in the Pre-PET and Pre-R Era TRIAL PT CHARACTERISTICS SWOG 8736 Median age: 59 Normal LDH: 80% PS 0-1: 97% % stage II: 33% Excl. bulky stage II ECOG 1484 Median age: 59 PS 0-1: 92% % stage II: 68% % bulky: 31% GEELA LNH 93-1 Median age: 47 Normal LDH PS 0-1 % stage II: 32% % bulky: 11% GELA LNH 93-4 Median age: 68 Normal LDH PS 0-1 % stage II: 32% % bulky: 9% NO. TREATMENT ARMS RESULTS 401 1) CHOP x 3 + RT 2) CHOP x CHOP x 8 If CR (n=215): 1) RT 2) No RT If PR (n=71) RT 647 1) CHOP x 3 + RT 2) ACVBP 574 1) CHOP x 4 + RT 2) CHOP x 4 RT vs. no RT: 5 yr PFS 77% vs. 64% (p=0.03) 5 yr OS 92% vs. 72% (p=0.02) * 8 yr update: no survival advantage with RT Complete response: RT vs. no RT: 6 yr FFS 70% vs. 53% (p=0.05) 6 yr OS 79% vs. 67% (p=0.23) Partial response: 6 yr FFS 63% 6 yr OS 69% CHOP + RT vs. ACVBP: 5 yr EFS 82% vs. 74% (p=<0.001) 5 yr OS 90% vs. 81% (p=0.001) RT vs. no RT: 5 yr EFS 64% vs. 61% (p=0.56) 5 yr OS 68% vs. 72% (p=0.54)
29 This still doesn t answer the question of needing RT with CR after R-CHOP chemo None of these studies used rituximab: 1) Does rituximab obviate the need for RT? 2) Will improved distant control with rituximab allow the local control benefit of RT to translate to an OS benefit? Will answer this in a moment
30 Local Control with RT after CR to Chemo Study Zinzani, 1999 Kahn, 2006 Halasz, 2010 Phan, 2010 Dorth, 2012 # of pts in CR Chemo Median FU Response assessment RT dose (Gy) 38 MACOP-B 39 mo Gallium % 16 CHOP x R-CHOP 46.5 mo 142 R-CHOP in 70% 79 R-CHOP in 65% 40 mo PET Med: % LC PET Med: % 36 mo PET If no residual CT dz: 30; If > 5cm or residual CT dz: mo Gallium (14%); PET (73%) 100% Med: 25 92% ASTRO 2012
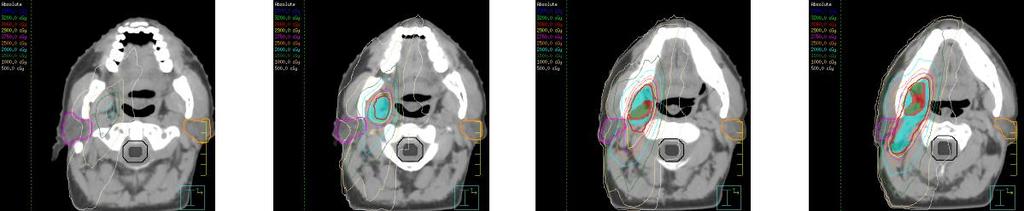
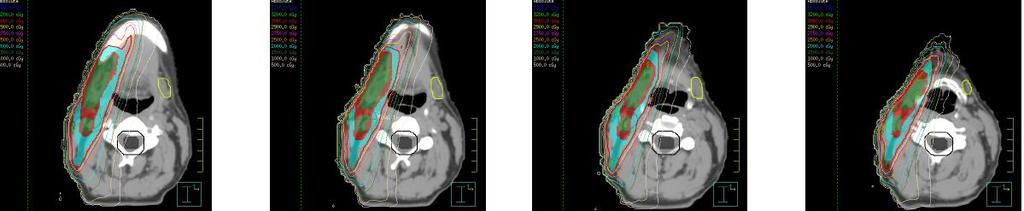
31 Treatment Plan 3060 cgy in 17 fx using IMRT to involved sites
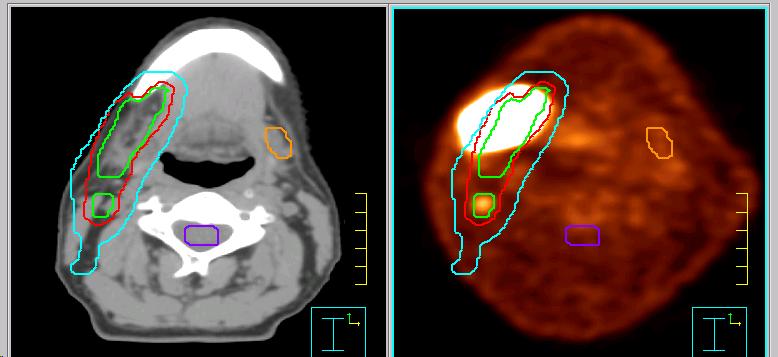

32 Pretreatment PET GTV CTV PTV
33
34 Appendix of Relevant Trials Summary of relevant trials for DLBCL
35 Chemo vs. Chemo-RT in the Pre-PET and Pre-R Era TRIAL PT CHARACTERISTICS SWOG 8736 Median age: 59 Normal LDH: 80% PS 0-1: 97% % stage II: 33% Excl. bulky stage II ECOG 1484 Median age: 59 PS 0-1: 92% % stage II: 68% % bulky: 31% GEELA LNH 93-1 Median age: 47 Normal LDH PS 0-1 % stage II: 32% % bulky: 11% GELA LNH 93-4 Median age: 68 Normal LDH PS 0-1 % stage II: 32% % bulky: 9% NO. TREATMENT ARMS RESULTS 401 1) CHOP x 3 + RT 2) CHOP x CHOP x 8 If CR (n=215): 1) RT 2) No RT If PR (n=71) RT 647 1) CHOP x 3 + RT 2) ACVBP 574 1) CHOP x 4 + RT 2) CHOP x 4 RT vs. no RT: 5 yr PFS 77% vs. 64% (p=0.03) 5 yr OS 92% vs. 72% (p=0.02) * 8 yr update: no survival advantage with RT Complete response: RT vs. no RT: 6 yr FFS 70% vs. 53% (p=0.05) 6 yr OS 79% vs. 67% (p=0.23) Partial response: 6 yr FFS 63% 6 yr OS 69% CHOP + RT vs. ACVBP: 5 yr EFS 82% vs. 74% (p=<0.001) 5 yr OS 90% vs. 81% (p=0.001) RT vs. no RT: 5 yr EFS 64% vs. 61% (p=0.56) 5 yr OS 68% vs. 72% (p=0.54)
36 ECOG 1484 CHOP x 8 If CR, randomized: Arm 1: Observation Arm 2: RT to 30 Gy If PR (28%) 40 Gy Stratified by performance status (0-1), bulk (>10 cm), number of sites (> 3)
37 ECOG 1484 In complete responders: RT improved FFS: 70% vs. 53% (p=0.05) No OS benefit: 79% vs. 67% (p=0.23) In partial responders (all received RT) 6 yr FFS: 63% 6 yr OS: 69%
38 ECOG 1484 Conclusions Patients with CR after CHOP benefit from RT (30 Gy) Improved DFS and local control (53% vs. 70%, p=0.05) No OS benefit Patients with PR treated with RT (40 Gy) had equivalent DFS and OS as patients with CR
39 GELA LNH patients; aggressive lymphoma Age > 60 ( elderly ), but age adjusted IPI = 0 Stage I or II Randomized CHOP x 4, no RT CHOP x Gy IFRT Bonnet et al JCO 2007
40 GELA LNH 93-4 Results CHOP x 4 CHOP x 4 + IFRT p value 5 yr EFS 61% 64% yr OS 72% 68% 0.6 Isolated local relapse 47% 21% - 5 yr OS age > 70 70% 58% 0.1 Bonnet et al JCO 2007
41 GELA LNH 93-4 Conclusions Stopped early: No difference on interim analysis New evidence showing benefit of rituximab No advantage in adding RT GELA abandons RT as 1 st line treatment of localized aggressive lymphoma: now R-CHOP Bonnet et al JCO 2007
42 CHOP +/- RT Summary RT improves LC and possibly DFS, but not OS
43 CHOP-RT vs. Alternative Chemo SWOG 8736 GELA LNH 93-1
44 SWOG 8736 Stage I and IE, Non-bulky stage II NHL (DLBCL, FL, and Burkitt s) Randomized: CHOP x 3 + IFRT to Gy (n=200) CHOP x 8 (n=201) Miller et al. NEJM 1998
45 SWOG 8736 Improved 5 yr PFS and OS in CHOP + RT arm CHOP x 3 + IFRT CHOP x 8 P value 5 yr PFS 76% 67% yr OS 82% 74% 0.02 Miller et al. NEJM 1998
46 SWOG 8736: Update Median follow up 8.2 years Loss of survival advantage in RT arm Conclusion: CHOP x 3 insufficient systemic therapy
47 GELA LNH 93-1 Age < 61, aggressive lymphoma, stage I-II, IPI=0 Randomized CHOP x 3 + IFRT 40 Gy (n=329) ACVBP* x 3 + Consolidation chemo** (n=277) * doxorubicin, cyclophosphamide, vindesin, bleomycin, prednisone ** MTX, Ara-C, etoposide, ifosfamide Reyes et al. NEJM 2005
48 GELA LNH 93-1 Improved EFS and OS with intensified chemotherapy CHOP x 3 + IFRT ACVBP x 3 + consolidation chemo P value 10 yr EFS 74% 82% < yr OS 81% 90% Miller et al. NEJM 1998
49 CHOP-RT vs. alternate chemo: Summary RT cannot compensate for inadequate chemotherapy Ng and Mauch JCO 2007
50 Local Control with RT after CR to R-Chemo Study Zinzani, 1999 Kahn, 2006 Halasz, 2010 Phan, 2010 Dorth, 2012 # of pts in CR Chemo Median FU Response assessment RT dose (Gy) 38 MACOP-B 39 mo Gallium % 16 CHOP x R-CHOP 46.5 mo 142 R-CHOP in 70% 79 R-CHOP in 65% 40 mo PET Med: % LC PET Med: % 36 mo PET If no residual CT dz: 30; If > 5cm or residual CT dz: mo Gallium (14%); PET (73%) 100% Med: 25 92% ASTRO 2012
51 MDACC Retrospective review 469 DLBCL pts, any stage At least 6 cycles of R-CHOP 30% received consolidative RT Median f/u 36 mo Phan et al. JCO 2010
52 MDACC Matched pair analysis: RT improved OS and PFS regardless of stage PFS: hazard ratio 0.29 OS: hazard ratio 0.24 OS benefit observed on multivariate analysis and matched pair analysis 100% LC at sites receiving IFRT Phan et al. JCO 2010
53 MDACC Conclusions Retrospective evidence suggests a benefit for patients who receive R-CHOP followed by RT Among 291 pts treated with R-CHOP and achieved CR, RT was associated with a significantly higher 5 yr PFS and OS Phan et al. JCO 2010
 RCHOP x 6-8, RT in select cases (bulky, paraspinal, refractory, prep for")
54 Treatment Summary: DLBCL DLBCL Stage I, II Stage III, IV IPI = 0 RCHOP x 6 or RCHOP x 3 + RT (30 Gy) IPI 0 RCHOP x 6 + RT (30Gy; 36 Gy if bulky; Gy if FDG avid) RCHOP x 6-8, RT in select cases (bulky, paraspinal, refractory, prep for SCT)
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and
Radiotherapy in DLCL is often worthwhile. Dr. Joachim Yahalom Memorial Sloan-Kettering, New York
 Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
B Cell Lymphoma: Aggressive
 B Cell Lymphoma: Aggressive UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Ibrutinib approved for mantle cell lymphoma as 2nd line therapy. - Aggressive lymphomas are a group of malignant
B Cell Lymphoma: Aggressive UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Ibrutinib approved for mantle cell lymphoma as 2nd line therapy. - Aggressive lymphomas are a group of malignant
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
The treatment of DLBCL. Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona
 The treatment of DLBCL Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona NHL frequency at the IOSI Mantle Cell Lymphoma 6.5 % Diffuse Large B-cell Lymphoma 37%
The treatment of DLBCL Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona NHL frequency at the IOSI Mantle Cell Lymphoma 6.5 % Diffuse Large B-cell Lymphoma 37%
Change Summary - Form 2018 (R3) 1 of 12
 1 of 12") Summary - Form 2018 (R3) 1 of 12 Form Question Number (r3) Type Description New Text Previous Text Today's date was removed 2018 N/A Today's Date Removed from Key Fields 2018 N/A HCT Type 2018 N/A Product
Summary - Form 2018 (R3) 1 of 12 Form Question Number (r3) Type Description New Text Previous Text Today's date was removed 2018 N/A Today's Date Removed from Key Fields 2018 N/A HCT Type 2018 N/A Product
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Aggressive Lymphomas - Current. Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre
 Aggressive Lymphomas - Current Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre Conflicts of interest I have no conflicts of interest to declare Outline What does aggressive lymphoma
Aggressive Lymphomas - Current Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre Conflicts of interest I have no conflicts of interest to declare Outline What does aggressive lymphoma
Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009
 Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations
Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations
Non-Hodgkin Lymphoma in Clinically Difficult Situations
 Winship Cancer Institute of Emory University Non-Hodgkin Lymphoma in Clinically Difficult Situations James Armitage, MD Professor, Department of Internal Medicine Joe Shapiro Distinguished Chair of Oncology
Winship Cancer Institute of Emory University Non-Hodgkin Lymphoma in Clinically Difficult Situations James Armitage, MD Professor, Department of Internal Medicine Joe Shapiro Distinguished Chair of Oncology
Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma:
 1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
HODGKIN LYMPHOMA Updated February 2016 by Dr. Manna (PGY 5 Hematology Resident, University of Calgary)
") HODGKIN LYMPHOMA Updated February 2016 by Dr. Manna (PGY 5 Hematology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff
HODGKIN LYMPHOMA Updated February 2016 by Dr. Manna (PGY 5 Hematology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff
Radiation and Hodgkin s Disease: A Changing Field. Sravana Chennupati Radiation Oncology PGY-2
 Radiation and Hodgkin s Disease: A Changing Field Sravana Chennupati Radiation Oncology PGY-2 History of Present Illness 19 yo previously healthy male college student began having pain in his R shoulder
Radiation and Hodgkin s Disease: A Changing Field Sravana Chennupati Radiation Oncology PGY-2 History of Present Illness 19 yo previously healthy male college student began having pain in his R shoulder
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center
 LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL
 New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
Aggressive NHL and Hodgkin Lymphoma. Dr. Carolyn Faught November 10, 2017
 Aggressive NHL and Hodgkin Lymphoma Dr. Carolyn Faught November 10, 2017 What does aggressive mean? Shorter duration of symptoms Generally need treatment at time of diagnosis Immediate, few days, few weeks
Aggressive NHL and Hodgkin Lymphoma Dr. Carolyn Faught November 10, 2017 What does aggressive mean? Shorter duration of symptoms Generally need treatment at time of diagnosis Immediate, few days, few weeks
ASTRO Refresher Course Lymphoma. Chris Kelsey, M.D. Duke University Medical Center
 ASTRO Refresher Course 2015 Lymphoma Chris Kelsey, M.D. Duke University Medical Center Disclosure Varian Medical Systems Research funding for lung cancer trial Learning Objectives Awareness of Deauville
ASTRO Refresher Course 2015 Lymphoma Chris Kelsey, M.D. Duke University Medical Center Disclosure Varian Medical Systems Research funding for lung cancer trial Learning Objectives Awareness of Deauville
Update: Non-Hodgkin s Lymphoma
 2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
Lymphoma: The Basics. Dr. Douglas Stewart
 Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies
![Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies](/thumbs/90/104309591.jpg "Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies") Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies UNCONTROLLED WHEN PRINTED Note: NOSCAN Haematology MCN has approved the information contained within this document to guide
Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies UNCONTROLLED WHEN PRINTED Note: NOSCAN Haematology MCN has approved the information contained within this document to guide
Indolent Lymphomas. Dr. Melissa Toupin The Ottawa Hospital
 Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Lymphoma 101. Nathalie Johnson, MDPhD. Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University
 Lymphoma 101 Nathalie Johnson, MDPhD Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University Disclosures Consultant and Advisory boards for multiple companies
Lymphoma 101 Nathalie Johnson, MDPhD Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University Disclosures Consultant and Advisory boards for multiple companies
2012 by American Society of Hematology
 2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
PET-imaging: when can it be used to direct lymphoma treatment?
 PET-imaging: when can it be used to direct lymphoma treatment? Luca Ceriani Nuclear Medicine and PET-CT centre Oncology Institute of Southern Switzerland Bellinzona Disclosure slide I declare no conflict
PET-imaging: when can it be used to direct lymphoma treatment? Luca Ceriani Nuclear Medicine and PET-CT centre Oncology Institute of Southern Switzerland Bellinzona Disclosure slide I declare no conflict
Printed by Martina Huckova on 10/3/2011 3:04:43 PM. For personal use only. Not approved for distribution. Copyright 2011 National Comprehensive
 NCCN Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform NCCN consensus. Category 2A: The recommendation
NCCN Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform NCCN consensus. Category 2A: The recommendation
T-cell Lymphomas Biology and Management
 T-cell Lymphomas Biology and Management March-27-2017 Outline Epidemiology Initial Work-up International Prognostic Index Treatment of Diffuse Large B-cell Lymphoma: -Limited Stage -Advanced Stage Frontline:
T-cell Lymphomas Biology and Management March-27-2017 Outline Epidemiology Initial Work-up International Prognostic Index Treatment of Diffuse Large B-cell Lymphoma: -Limited Stage -Advanced Stage Frontline:
1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes on the next page
 COME HOME Non-Hodgkin pathway development worksheet, v6 September 2014 1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes
COME HOME Non-Hodgkin pathway development worksheet, v6 September 2014 1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes
Patient Case Studies & Panel Discussion
 Patient Case Studies & Panel Discussion Panelists: Jeremy S. Abramson, MD, Massachusetts General Hospital Cancer Center; Ranjana H. Advani, MD, Stanford Cancer Institute; Andrew D. Zelenetz, MD, PhD, Memorial
Patient Case Studies & Panel Discussion Panelists: Jeremy S. Abramson, MD, Massachusetts General Hospital Cancer Center; Ranjana H. Advani, MD, Stanford Cancer Institute; Andrew D. Zelenetz, MD, PhD, Memorial
ARRO Case: Pediatric High Risk Classical Hodgkin Lymphoma
 ARRO Case: Pediatric High Risk Classical Hodgkin Lymphoma Steven Seyedin, MD (PGY-3) Faculty Advisor: Dr. John Buatti, MD, FASTRO Department of Radiation Oncology University of Iowa Hospital and Clinics
ARRO Case: Pediatric High Risk Classical Hodgkin Lymphoma Steven Seyedin, MD (PGY-3) Faculty Advisor: Dr. John Buatti, MD, FASTRO Department of Radiation Oncology University of Iowa Hospital and Clinics
Choice of upfront treatment in the management of diffuse large B-cell lymphoma and follicular lymphoma
 Choice of upfront treatment in the management of diffuse large B-cell lymphoma and follicular lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
Choice of upfront treatment in the management of diffuse large B-cell lymphoma and follicular lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphocyte Predominant Hodgkin s Lymphoma. Case Presentation. How would you treat the patient?
 Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Diffuse Large B-Cell Lymphoma (DLBCL)
") Diffuse Large B-Cell Lymphoma (DLBCL) DLBCL/MCL Dr. Anthea Peters, MD, FRCPC University of Alberta/Cross Cancer Institute Disclosures Honoraria from Janssen, Abbvie, Roche, Lundbeck, Seattle Genetics Objectives
Diffuse Large B-Cell Lymphoma (DLBCL) DLBCL/MCL Dr. Anthea Peters, MD, FRCPC University of Alberta/Cross Cancer Institute Disclosures Honoraria from Janssen, Abbvie, Roche, Lundbeck, Seattle Genetics Objectives
THE EORTC-GELA TREATMENT STRATEGY IN CLINICAL STAGES I-II HL Results of the H9-F and H9-U trials (#20982)
") EORTC Lymphoma Group THE EORTC-GELA TREATMENT STRATEGY IN CLINICAL STAGES I-II HL Results of the H9-F and H9-U trials (#20982) J. Thomas, C. Fermé, E.M. Noordijk, H. Eghbali and M. Henry-Amar 7th International
EORTC Lymphoma Group THE EORTC-GELA TREATMENT STRATEGY IN CLINICAL STAGES I-II HL Results of the H9-F and H9-U trials (#20982) J. Thomas, C. Fermé, E.M. Noordijk, H. Eghbali and M. Henry-Amar 7th International
Radiotherapy in aggressive lymphomas. Umberto Ricardi
 Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge. ASH 2012 Atlanta
 Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
MANAGEMENT OF LYMPHOMAS
 MANAGEMENT OF LYMPHOMAS Challenges & Recommendations F. Chite Asirwa, MD. Internal Medicine Physician Medical Oncologist & Hematologist Director-AMPATH Oncology & Hematology @Kenya Physicians Association
MANAGEMENT OF LYMPHOMAS Challenges & Recommendations F. Chite Asirwa, MD. Internal Medicine Physician Medical Oncologist & Hematologist Director-AMPATH Oncology & Hematology @Kenya Physicians Association
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Harmesh Naik, MD. GME Presentation to Family Practice Residents October 16, 2013.
 Harmesh Naik, MD. GME Presentation to Family Practice Residents October 16, 2013. Lymphoma: Lympho-proliferative disorders arising from lymphocytes Heterogeneous group of disorders Differing patterns of
Harmesh Naik, MD. GME Presentation to Family Practice Residents October 16, 2013. Lymphoma: Lympho-proliferative disorders arising from lymphocytes Heterogeneous group of disorders Differing patterns of
Indolent Lymphomas: Current. Dr. Laurie Sehn
 Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Non-Hodgkin lymphoma
 Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Hodgkin's Lymphoma. Symptoms. Types
 Hodgkin's lymphoma (Hodgkin's disease) usually develops in the lymphatic system, a part of the body's immune system. This system carries disease-fighting white blood cells throughout the body. Lymph tissue
Hodgkin's lymphoma (Hodgkin's disease) usually develops in the lymphatic system, a part of the body's immune system. This system carries disease-fighting white blood cells throughout the body. Lymph tissue
Diffuse large B-cell lymphomas. G. Verhoef, MD, PhD University Hospital Leuven BHS, March 9, 2013
 Diffuse large B-cell lymphomas G. Verhoef, MD, PhD University Hospital Leuven BHS, March 9, 2013 Case A 72-year-old previously healthy man presented with acute abdominal pain and a 15 kg weight loss. Positron
Diffuse large B-cell lymphomas G. Verhoef, MD, PhD University Hospital Leuven BHS, March 9, 2013 Case A 72-year-old previously healthy man presented with acute abdominal pain and a 15 kg weight loss. Positron
Aggressive B and T cell lymphomas: Treatment paradigms in 2018
 Aggressive B and T cell lymphomas: Treatment paradigms in 2018 John P. Leonard M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Associate
Aggressive B and T cell lymphomas: Treatment paradigms in 2018 John P. Leonard M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Associate
Mantle Cell Lymphoma
 Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center
 What Is Personalized Medicine For Patients With Lymphoma? Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center DISCLOSURE I have no potential
What Is Personalized Medicine For Patients With Lymphoma? Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center DISCLOSURE I have no potential
PET-CT in Peripheral T-cell Lymphoma: To Be or Not To Be
 PET-CT in Peripheral T-cell Lymphoma: To Be or Not To Be Bruce D. Cheson, M.D. Georgetown University Hospital Lombardi Comprehensive Cancer Center Washington, DC, USA So What is the Question(s)? What is
PET-CT in Peripheral T-cell Lymphoma: To Be or Not To Be Bruce D. Cheson, M.D. Georgetown University Hospital Lombardi Comprehensive Cancer Center Washington, DC, USA So What is the Question(s)? What is
What are the hurdles to using cell of origin in classification to treat DLBCL?
 What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
A CASE OF PRIMARY THYROID LYMPHOMA. Prof Dr.Dilek Gogas Yavuz Marmara University School of Medicine Endocrinology and Metabolism Istanbul, Turkey
 A CASE OF PRIMARY THYROID LYMPHOMA Prof Dr.Dilek Gogas Yavuz Marmara University School of Medicine Endocrinology and Metabolism Istanbul, Turkey 38 year old female She recognized a mass in her right neck
A CASE OF PRIMARY THYROID LYMPHOMA Prof Dr.Dilek Gogas Yavuz Marmara University School of Medicine Endocrinology and Metabolism Istanbul, Turkey 38 year old female She recognized a mass in her right neck
Highlights of ICML 2015
 Highlights of ICML 2015 Jonathan W. Friedberg M.D. Director, James P. Wilmot Cancer Center Statistics, ICML 2015: a global meeting Almost 3700 participants. 90 countries represented. Attendees: USA 465
Highlights of ICML 2015 Jonathan W. Friedberg M.D. Director, James P. Wilmot Cancer Center Statistics, ICML 2015: a global meeting Almost 3700 participants. 90 countries represented. Attendees: USA 465
Lymphomas and multiple myeloma 12/23/2018 1
 60 Lymphomas and multiple myeloma 12/23/2018 1 Lymphomas Lymphoma is cancer of the lymphatic system. Lymphomas are subdivided into two main categories: Hodgkin's lymphoma (HL) and non- Hodgkin's lymphoma
60 Lymphomas and multiple myeloma 12/23/2018 1 Lymphomas Lymphoma is cancer of the lymphatic system. Lymphomas are subdivided into two main categories: Hodgkin's lymphoma (HL) and non- Hodgkin's lymphoma
Non-Hodgkin s Lymphoma
 Non-Hodgkin s Lympoma Non-Hodgkin s Lymphomas Janet H. Van Cleave MSN, ACNP-CS, CS, AOCN Acute Care Nurse Practitioner The Mount Sinai Medical Center of New York City Doctoral Student, Yale University
Non-Hodgkin s Lympoma Non-Hodgkin s Lymphomas Janet H. Van Cleave MSN, ACNP-CS, CS, AOCN Acute Care Nurse Practitioner The Mount Sinai Medical Center of New York City Doctoral Student, Yale University
First Line Management of Classical Hodgkin Lymphoma
 First Line Management of Classical Hodgkin Lymphoma George Follows Cambridge University Hospitals NHS Foundation Trust george.follows@addenbrookes.nhs.uk The controversial areas Early stage non-bulky /
First Line Management of Classical Hodgkin Lymphoma George Follows Cambridge University Hospitals NHS Foundation Trust george.follows@addenbrookes.nhs.uk The controversial areas Early stage non-bulky /
HIV ASSOCIATED LYMPHOMA. Dr N Rapiti
 HIV ASSOCIATED LYMPHOMA Dr N Rapiti HIV ASSOCIATED LYMPHOMA: OVERVIEW Classification Pathogenesis Prognosis cart Chemotherapy/Radiotherapy/SCT Supportive CASE 40 yr old male, Mr BM, p/w Symptomatic anemia
HIV ASSOCIATED LYMPHOMA Dr N Rapiti HIV ASSOCIATED LYMPHOMA: OVERVIEW Classification Pathogenesis Prognosis cart Chemotherapy/Radiotherapy/SCT Supportive CASE 40 yr old male, Mr BM, p/w Symptomatic anemia
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA
 RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
Lymphoma Read with the experts
 Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Lymphomas in Prof Paul Ruff Division of Medical Oncology
 Lymphomas in 2010 Prof Paul Ruff Division of Medical Oncology Most Common Lymphomas: ~90% B-cell and ~10% T-cell T lymphoblastic: 2% Marginal zone, nodal: 2% Other: 9% Burkitt: 2% Anaplastic large cell:
Lymphomas in 2010 Prof Paul Ruff Division of Medical Oncology Most Common Lymphomas: ~90% B-cell and ~10% T-cell T lymphoblastic: 2% Marginal zone, nodal: 2% Other: 9% Burkitt: 2% Anaplastic large cell:
Defined lymphoma entities in the current WHO classification
 Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
SURVIVORSHIP WITH LYMPHOMA APRIL SHAMY MD,CM JEWISH GENERAL HOSPITAL MCGILL UNIVERSITY
 SURVIVORSHIP WITH LYMPHOMA APRIL SHAMY MD,CM JEWISH GENERAL HOSPITAL MCGILL UNIVERSITY Some Statistics Approximately 1 in 2 Canadians develop cancer 25% of Canadians die of cancer 2009: 810,000 Canadians
SURVIVORSHIP WITH LYMPHOMA APRIL SHAMY MD,CM JEWISH GENERAL HOSPITAL MCGILL UNIVERSITY Some Statistics Approximately 1 in 2 Canadians develop cancer 25% of Canadians die of cancer 2009: 810,000 Canadians
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège. 14 th post-ash meeting, January 6 th 2011, Brussels
 Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma
 with classical Hodgkin lymphoma") PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
Interim PET in Diffuse Large B Cell Lymphoma.The GEL/TAMO experience
 Interim PET in Diffuse Large B Cell Lymphoma.The GEL/TAMO experience MD. Caballero, Hospital Universitario, Salamanca, Spain. Chair of The GEL/TAMO Group Menton,9 april 2010 Disclosures for Dolores Caballero
Interim PET in Diffuse Large B Cell Lymphoma.The GEL/TAMO experience MD. Caballero, Hospital Universitario, Salamanca, Spain. Chair of The GEL/TAMO Group Menton,9 april 2010 Disclosures for Dolores Caballero
Traitement des lymphomes diffus à grandes cellules B
 Traitement des lymphomes diffus à grandes cellules B Corinne HAIOUN Unité Hémopathies Lymphoïdes- CHU Henri Mondor Université Paris Est Créteil DES Hématologie Février 2012 On February 10th, the merging
Traitement des lymphomes diffus à grandes cellules B Corinne HAIOUN Unité Hémopathies Lymphoïdes- CHU Henri Mondor Université Paris Est Créteil DES Hématologie Février 2012 On February 10th, the merging
XVIII. Management of nodular lymphocyte predominant Hodgkin lymphoma
 Hematological Oncology Hematol Oncol 2015; 33: 90 95 Published online in Wiley Online Library (wileyonlinelibrary.com).2226 Supplement Article XVIII. Management of nodular lymphocyte predominant Hodgkin
Hematological Oncology Hematol Oncol 2015; 33: 90 95 Published online in Wiley Online Library (wileyonlinelibrary.com).2226 Supplement Article XVIII. Management of nodular lymphocyte predominant Hodgkin
Open questions in the treatment of Follicular Lymphoma. Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland
 Open questions in the treatment of Follicular Lymphoma Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland Survival of major lymphoma subtypes at IOSI 1.00 cause-specific
Open questions in the treatment of Follicular Lymphoma Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland Survival of major lymphoma subtypes at IOSI 1.00 cause-specific
Understanding your diagnosis. Dr Graham Collins Consultant Haemtologist Oxford University Hospitals
 Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
Sally Barrington Martin Hutchings
 Sally Barrington Martin Hutchings Therapeutic implications of BMI Bone marrow involvement means extranodal disease and by definition stage IV BMI detected by BMB is a poor prognostic feature in most lymphomas
Sally Barrington Martin Hutchings Therapeutic implications of BMI Bone marrow involvement means extranodal disease and by definition stage IV BMI detected by BMB is a poor prognostic feature in most lymphomas
Acute Lymphoblastic Leukemia (ALL) Ryan Mattison, MD University of Wisconsin March 2, 2010
 Ryan Mattison, MD University of Wisconsin March 2, 2010") Acute Lymphoblastic Leukemia (ALL) Ryan Mattison, MD University of Wisconsin March 2, 2010 ALL Epidemiology 20% of new acute leukemia cases in adults 5200 new cases in 2007 Most are de novo Therapy-related
Acute Lymphoblastic Leukemia (ALL) Ryan Mattison, MD University of Wisconsin March 2, 2010 ALL Epidemiology 20% of new acute leukemia cases in adults 5200 new cases in 2007 Most are de novo Therapy-related
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113)
") Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
FDG-PET/CT in the management of lymphomas
 FDG-PET/CT in the management of lymphomas Olivier Gheysens, MD, PhD Dept. of Nuclear Medicine, UZ Leuven BHS, Feb 4th 2017 Brussels Dept. of Nuclear Overview Introduction on FDG-PET/CT Staging Response
FDG-PET/CT in the management of lymphomas Olivier Gheysens, MD, PhD Dept. of Nuclear Medicine, UZ Leuven BHS, Feb 4th 2017 Brussels Dept. of Nuclear Overview Introduction on FDG-PET/CT Staging Response
LYSA PET adapted programs. O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France
 LYSA PET adapted programs O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France 3 phase III trials DLBCL LNH 09-1B: aaipi = 0, 18 80y : ongoing GAINED: aaipi = 1-3, 18 60y : ongoing
LYSA PET adapted programs O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France 3 phase III trials DLBCL LNH 09-1B: aaipi = 0, 18 80y : ongoing GAINED: aaipi = 1-3, 18 60y : ongoing
Patient underwent hemicolectomy: 7 x 4.5 cm intusscepted segment of ileum in colon - mucosal
 Extranodal Lymphomas Rena Buckstein Odette Cancer Center Case: JT 69 yo male COO software company PMHx: basal cell back, cholesterol Presents to ER with severe abdominal pain, bloody diarrhea x 2d In ER
Extranodal Lymphomas Rena Buckstein Odette Cancer Center Case: JT 69 yo male COO software company PMHx: basal cell back, cholesterol Presents to ER with severe abdominal pain, bloody diarrhea x 2d In ER
Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES!
 Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES! Christopher Flowers, MD, MSc Associate Professor Director, Lymphoma Program Department of Hematology and Oncology Emory School of Medicine
Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES! Christopher Flowers, MD, MSc Associate Professor Director, Lymphoma Program Department of Hematology and Oncology Emory School of Medicine
CAR-T cell therapy pros and cons
 CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
Non-Hodgkin s Lymphomas Version
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) n-hodgkin s Lymphomas Version 2.2015 NCCN.g Continue Version 2.2015, 03/03/15 National Comprehensive Cancer Netwk, Inc. 2015, All rights
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) n-hodgkin s Lymphomas Version 2.2015 NCCN.g Continue Version 2.2015, 03/03/15 National Comprehensive Cancer Netwk, Inc. 2015, All rights
Alexander Fosså, M.D. PhD.
 Alexander Fosså, M.D. PhD. Current position: Senior Consultant, Department of Medical Oncology Oslo University Hospital Focus of work: - Malignant lymphoma - Chemotherapy, immunotherapy, radiotherapy -
Alexander Fosså, M.D. PhD. Current position: Senior Consultant, Department of Medical Oncology Oslo University Hospital Focus of work: - Malignant lymphoma - Chemotherapy, immunotherapy, radiotherapy -
Aggressive lymphomas ASH Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV
 Aggressive lymphomas ASH 2015 Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV CHOP 1992 2002 R-CHOP For DLBCL High dose chemo With PBSCT Aggressive lymphomas 1.DLBCL 2.Primary Mediastinal Lymphoma 3.CNS
Aggressive lymphomas ASH 2015 Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV CHOP 1992 2002 R-CHOP For DLBCL High dose chemo With PBSCT Aggressive lymphomas 1.DLBCL 2.Primary Mediastinal Lymphoma 3.CNS
Addition of rituximab is not associated with survival benefit compared with CHOP alone for patients with stage I diffuse large B-cell lymphoma
 Original Article Addition of rituximab is not associated with survival benefit compared with CHOP alone for patients with stage I diffuse large B-cell lymphoma Bo Jia 1, Yuankai Shi 1, Suyi Kang 1, Sheng
Original Article Addition of rituximab is not associated with survival benefit compared with CHOP alone for patients with stage I diffuse large B-cell lymphoma Bo Jia 1, Yuankai Shi 1, Suyi Kang 1, Sheng
Lymphatic system component
 Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
Indium-111 Zevalin Imaging
 Indium-111 Zevalin Imaging Background: Most B lymphocytes (beyond the stem cell stage) contain a surface antigen called CD20. It is possible to kill these lymphocytes by injecting an antibody to CD20.
Indium-111 Zevalin Imaging Background: Most B lymphocytes (beyond the stem cell stage) contain a surface antigen called CD20. It is possible to kill these lymphocytes by injecting an antibody to CD20.
Solomon Graf, MD February 22, 2013
 Solomon Graf, MD February 22, 2013 Case Review of FL pathology, prognosis Grading of FL Grade 3 disease High proliferative index in grade 1/2 disease Pediatric FL Future of FL classification 57 yo man
Solomon Graf, MD February 22, 2013 Case Review of FL pathology, prognosis Grading of FL Grade 3 disease High proliferative index in grade 1/2 disease Pediatric FL Future of FL classification 57 yo man
Prognostic Value of Early Introduction of Second Line in Patients with Diffuse Large B Cell Lymphoma
 Med. J. Cairo Univ., Vol. 84, No., December: 443-447, 6 www.medicaljournalofcairouniversity.net Prognostic Value of Early Introduction of Second Line in Patients with Diffuse Large B Cell Lymphoma HAMDY
Med. J. Cairo Univ., Vol. 84, No., December: 443-447, 6 www.medicaljournalofcairouniversity.net Prognostic Value of Early Introduction of Second Line in Patients with Diffuse Large B Cell Lymphoma HAMDY
Comparison of Three Radiation Dose Levels after EBVP Regimen in Favorable Supradiaphragmatic Clinical Stages I-II Hodgkin s Lymphoma (HL):
:") Comparison of Three Radiation Dose Levels after EBVP Regimen in Favorable Supradiaphragmatic Clinical Stages I-II Hodgkin s Lymphoma (HL): Preliminary Results of the EORTC-GELA H9-F Trial H. Eghbali, P.
Comparison of Three Radiation Dose Levels after EBVP Regimen in Favorable Supradiaphragmatic Clinical Stages I-II Hodgkin s Lymphoma (HL): Preliminary Results of the EORTC-GELA H9-F Trial H. Eghbali, P.
Original Article. Introduction
 Original Article Radiat Oncol J 217;35(4):317-324 https://doi.org/1.3857/roj.217.451 pissn 2234-19 eissn 2234-3156 Treatment results of radiotherapy following CHOP or R-CHOP in limited-stage head-and-neck
Original Article Radiat Oncol J 217;35(4):317-324 https://doi.org/1.3857/roj.217.451 pissn 2234-19 eissn 2234-3156 Treatment results of radiotherapy following CHOP or R-CHOP in limited-stage head-and-neck
Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy?
 Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy? Andreas Rosenwald Institute of Pathology, University of Würzburg, Germany Barcelona, June 18, 2010 NEW WHO CLASSIFICATION
Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy? Andreas Rosenwald Institute of Pathology, University of Würzburg, Germany Barcelona, June 18, 2010 NEW WHO CLASSIFICATION
Diagnosis and patient pathway in lymphomas
 The Royal Marsden Diagnosis and patient pathway in lymphomas Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Change Presentation title and date in Footer dd.mm.yyyy
The Royal Marsden Diagnosis and patient pathway in lymphomas Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Change Presentation title and date in Footer dd.mm.yyyy
Targeted Radioimmunotherapy for Lymphoma
 Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
children and young people:
 Hodgkin lymphoma in children and young people: State of the art Professor W. Hamish Wallace RHSC 2016 Childhood Cancer 1971-2010 One-, Five- and Ten-Year Actuarial Survival (%), Children (Aged 0-14),
Hodgkin lymphoma in children and young people: State of the art Professor W. Hamish Wallace RHSC 2016 Childhood Cancer 1971-2010 One-, Five- and Ten-Year Actuarial Survival (%), Children (Aged 0-14),
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs. Nancy P. Caraway, M.D.
 A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
LINFOMA B (INCLASIFICABLE) CON RASGOS INTERMEDIOS ENTRE LINFOMA DE BURKITT Y LINFOMA B DIFUSO DE CÉLULAS GRANDES.
 CON RASGOS INTERMEDIOS ENTRE LINFOMA DE BURKITT Y LINFOMA B DIFUSO DE CÉLULAS GRANDES.") Congreso Nacional SEAP 2013. LINFOMA B (INCLASIFICABLE) CON RASGOS INTERMEDIOS ENTRE LINFOMA DE BURKITT Y LINFOMA B DIFUSO DE CÉLULAS GRANDES. Santiago Montes Moreno Servicio de Anatomía Patológica, HUMV
Congreso Nacional SEAP 2013. LINFOMA B (INCLASIFICABLE) CON RASGOS INTERMEDIOS ENTRE LINFOMA DE BURKITT Y LINFOMA B DIFUSO DE CÉLULAS GRANDES. Santiago Montes Moreno Servicio de Anatomía Patológica, HUMV
Journal of American Science 2016;12(6)
") Role of reduced dose CHOP with Rituximab plus involved field radiotherapy in treatment of early stage diffuse large B cell lymphoma in elderly patients Lobna A. Abdelaziz 1, Reham A. Salem 1, Nabila Hefzi
Role of reduced dose CHOP with Rituximab plus involved field radiotherapy in treatment of early stage diffuse large B cell lymphoma in elderly patients Lobna A. Abdelaziz 1, Reham A. Salem 1, Nabila Hefzi
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas. Original Policy Date
 MP 7.03.13 Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013
MP 7.03.13 Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013
Hodgkin Lymphoma PROVIDING THE LATEST INFORMATION FOR PATIENTS & CAREGIVERS. Revised 2018
 PROVIDING THE LATEST INFORMATION FOR PATIENTS & CAREGIVERS Hodgkin Lymphoma Revised 2018 Supported by an independent educational grant from Merck & Co., Inc. and Seattle Genetics, Inc. A six-word narrative
PROVIDING THE LATEST INFORMATION FOR PATIENTS & CAREGIVERS Hodgkin Lymphoma Revised 2018 Supported by an independent educational grant from Merck & Co., Inc. and Seattle Genetics, Inc. A six-word narrative
Case Report B Cell Lymphoma, Unclassifiable, Transformed from Follicular Lymphoma: A Rare Presentation with Review of the Literature
 Hindawi Publishing Corporation Case Reports in Hematology Volume 2015, Article ID 651764, 9 pages http://dx.doi.org/10.1155/2015/651764 Case Report B Cell Lymphoma, Unclassifiable, Transformed from Follicular
Hindawi Publishing Corporation Case Reports in Hematology Volume 2015, Article ID 651764, 9 pages http://dx.doi.org/10.1155/2015/651764 Case Report B Cell Lymphoma, Unclassifiable, Transformed from Follicular
Prevalent lymphomas in Africa
 Prevalent lymphomas in Africa Dr Zainab Mohamed Clinical Oncologist GSH/UCT Groote Schuur Hospital Disclaimer I declare that I have no conflict of interest Groote Schuur Hospital Denis Burkitt 1911-1993
Prevalent lymphomas in Africa Dr Zainab Mohamed Clinical Oncologist GSH/UCT Groote Schuur Hospital Disclaimer I declare that I have no conflict of interest Groote Schuur Hospital Denis Burkitt 1911-1993
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin s Lymphomas
 Hematopoietic Stem-Cell Transplantation for Non-Hodgkin s Lymphomas Policy Number: 8.01.20 Last Review: 7/2014 Origination: 7/2002 Next Review: 7/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin s Lymphomas Policy Number: 8.01.20 Last Review: 7/2014 Origination: 7/2002 Next Review: 7/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue
Hematopoietic Cell Transplantation for Non-Hodgkin's Lymphomas
 Medical Policy Manual Transplant, Policy No. 45.23 Hematopoietic Cell Transplantation for Non-Hodgkin's Lymphomas Next Review: September 2018 Last Review: December 2017 Effective: January 1, 2018 IMPORTANT
Medical Policy Manual Transplant, Policy No. 45.23 Hematopoietic Cell Transplantation for Non-Hodgkin's Lymphomas Next Review: September 2018 Last Review: December 2017 Effective: January 1, 2018 IMPORTANT
Advanced stage HL The old and new match: BEACOPP
 27.03.2015 1 Advanced stage HL The old and new match: BEACOPP Peter Borchmann German Hodgkin Study Group University of Cologne, Germany Which answer is wrong? For patients with advanced stage HL, treatment
27.03.2015 1 Advanced stage HL The old and new match: BEACOPP Peter Borchmann German Hodgkin Study Group University of Cologne, Germany Which answer is wrong? For patients with advanced stage HL, treatment
C r h ist s op o h p e h r e R. R F l F ow o er e s, s M D, D M S
 1 Christopher R. Flowers, MD, MS Associate Professor of Hematology and Medical Oncology Winship Cancer Institute Emory University School of Medicine Atlanta, Georgia 2 1 Anyone can get blood cancer One
1 Christopher R. Flowers, MD, MS Associate Professor of Hematology and Medical Oncology Winship Cancer Institute Emory University School of Medicine Atlanta, Georgia 2 1 Anyone can get blood cancer One
Barbara Barnes Rogers, CRNP, MN, AOCN, ANP-BC Adult Hematology-Oncology Nurse Practitioner Fox Chase Cancer Center Philadelphia, Pennsylvania
 Barbara Barnes Rogers, CRNP, MN, AOCN, ANP-BC Adult Hematology-Oncology Nurse Practitioner Fox Chase Cancer Center Philadelphia, Pennsylvania Barbara.rogers@fccc.edu Disclosures Barbara Rogers, CRNP, MN,
Barbara Barnes Rogers, CRNP, MN, AOCN, ANP-BC Adult Hematology-Oncology Nurse Practitioner Fox Chase Cancer Center Philadelphia, Pennsylvania Barbara.rogers@fccc.edu Disclosures Barbara Rogers, CRNP, MN,