Clinical features and outcomes of 139 Japanese patients with Hodgkin lymphoma
|
|
|
- Rafe Alexander
- 5 years ago
- Views:
Transcription
1 Original Article Clinical features and outcomes of 139 Japanese patients with Hodgkin lymphoma Authors: Shinichi Makita 1, 4, Dai Maruyama 1, Akiko Miyagi Maeshima 2, Hirokazu Taniguchi 2, Ken-ichi Miyamoto 1, Hideaki Kitahara 1, Suguru Fukuhara 1, Wataru Munakata 1, Yukio Kobayashi 1, Jun Itami 3, and Kensei Tobinai 1, 4 Affiliations: Department of 1 Hematology, 2 Pathology and Clinical Laboratory, and 3 Radiation Oncology, National Cancer Center Hospital, Tokyo, Japan. 4 Course of Advanced Clinical Research of Cancer, Juntendo University Graduate School of Medicine, Tokyo, Japan. Running Title: Treatment outcomes of HL in Japan Correspondence: Dai Maruyama, MD, PhD. Department of Hematology, National Cancer Center Hospital, Tsukiji, Chuo-ku, Tokyo , Japan. 1
2 Tel: Fax:
3 Abstract Hodgkin lymphoma (HL) is a rare subtype of malignant lymphoma in Japan, and there are few reports of HL in Japan in recent years. We retrospectively analyzed the clinical features of 139 patients with HL who were diagnosed and treated at our institution between 1997 and The median age at diagnosis was 34 years with 83 male. Of these patients, 83 (60%) were early-stage and 56 (40%) advanced-stage. Seventy-three patients (88%) with early-stage disease received ABVd followed by irradiation. All of the 56 advanced-stage patients received chemotherapy, mainly ABVd. The 5-year progression-free survival (PFS) rates and overall survival rates were 90% and 94% in patients with early-stage disease, and 71% and 90% in those with advanced-stage disease. The PFS of patients with advanced-stage disease was significantly lower than those with early stage (P = 0.014). In conclusion, the outcomes of Japanese patients with HL in recent years were not improved as compared with the results of previous reports. We confirmed that patients with advanced-stage disease have lower PFS than those with early-stage disease. Prospective studies are needed to establish novel treatment strategies to improve the outcome of HL patients, especially those with advanced disease. Keywords: Hodgkin lymphoma, ABVd, Japanese patient 3
4 Introduction Hodgkin lymphoma (HL) is one of the common subtypes of malignant lymphoma in Western countries [1, 2]. Although the patients with HL showed unsatisfied outcomes in1960s, the clinical development of radiotherapy and chemotherapy based on the several clinical trials in the past decades made HL a curable disease with favorable outcome [2]. In 1970s and 1980s, multi-agent regimen, MOPP (mechlorethamine, vincristine, procarbazine and prednisone) has been developed. Several trials reported the favorable response of MOPP regimen, while the toxicities such as sterility, premature menopause, and leukemogenesis were serious problems [3-5]. To solve these problems, the well-established multi-agent combination regimen, ABVD (doxorubicin, bleomycin, vinblastine, and dacarbazine) has been developed. ABVD with or without involved-field irradiation provides the best balance of effectiveness and minimization of toxicity and regarded as a standard of care in the patients with HL until recently [5, 6]. Although the optimal cycle of ABVD was controversial until early 2000s, 4 cycles of ABVD followed by irradiation was recommended in the early-stage HL, while 6 cycles of ABVD in the advanced-stage HL nowadays [7]. In Japan, HL is a rare subtype of malignant lymphoma; its incidence is approximately one-third of that in Western countries [8]. Therefore, Japanese trials for HL have been less frequently conducted. Three prospective studies for HL were conducted by the 4
5 Lymphoma Study Group of Japan Clinical Oncology Group (JCOG-LSG) from the1980s to 1990s [9-11]. Sequential phase II studies, JCOG8905 and JCOG9305 showed the safety and efficacy of C-MOPP/ABVd (cyclophosphamide, vincristine, procarbazine and prednisone/doxorubicin, bleomycin, vinblastine and dacarbazine) and ABVd regimens. Both regimens used a reduced dose of dacarbazine (250 mg/m 2 ) because of intolerable sever emesis related to dacarbazine in a polot study at that time [9]. As the 4-year progression-free survival (PFS) rate of the patients in JCOG8905 and the 5-year PFS rate in MOPP/ABVD in Cancer and Leukemia Group B (CALGB) study was 65.7% and 65%, respectively, ABVd regimen is supposed to have similar efficacy to original ABVD regimen in Japanese patients [7, 9]. The next phase II study, JCOG9705 investigated the ABV regimen, removing dacarbazine from ABVd, with an increased dose of doxorubicin [11]. The interim analysis revealed that the 2-year PFS with ABV was significantly inferior to that shown by ABVd in JCOG9305, suggesting that dacarbazine is a key agent for the treatment of HL. Based on these 3 studies, ABVd has been regarded as the standard of care in patients with previously untreated HL in Japan. There are few data about clinical characteristics and the outcomes of HL patients, except for the JCOG-LSG trials, especially in recent years. Therefore, this retrospective study was made to clarify the clinical characteristics and outcomes of the Japanese patients with HL 5
6 in recent years. Patients and Methods Patients Among the 205 patients who were diagnosed as having HL at the National Cancer Center Hospital (NCCH) between September 1997 and December 2011, we retrospectively analyzed 139 consecutive patients who were initially treated in the setting of clinical practice at NCCH. All the histopathological diagnoses were made by experienced hemato-pathologists (AMM and HT) according to the WHO classification [12]. The protocol for this retrospective study was approved by the institutional review board of the National Cancer Center. Clinical staging Clinical stage (CS) was determined according to the Ann Arbor classification system [13]. The extent of disease was assessed by chest X-ray, computed tomography (CT) scan from neck to pelvis, and bone marrow aspiration or biopsy. We determined CS I-IIA as early stage and CS IIB-IV as advanced stage. Bulky disease was determined by a mediastinal mass ratio > 0.33 on chest X-ray or a diameter larger than 10 cm on CT-scan. The 6
7 International Prognostic Score (IPS) was also assessed in patients with advanced stage disease [14]. Treatment strategy of HL in the present study In 1990s and early 2000s, The patient with early-stage HL were treated according to the strategy of JCOG9305; the ABVd was scheduled to give 6 cycles or 7-8 cycles, when complete remission (CR) was obtained after 1-4 cycles or 5-6 cycles, respectively. The patient with bulky disease at initial presentation received irradiation after the ABVd. In the late 2000s, 4 cycles of ABVd followed by involved-field irradiation was performed regardless of bulky disease or interim-response. The patients with advanced-stage HL were treated with 6-8 cycles of ABVd. The patiens with bulky disease or with residual disease after the ABVd received irradiation. Statistical analysis Response was assessed after completion of the initial treatment according to the International Workshop response criteria 1999 [15]. Among the patients who received [ 18 F] fluorodeoxyglucose-positron emission tomography (FDG-PET)/CT, the response was assessed according to the revised response criteria for malignant lymphoma 2007 [16]. 7
8 Overall survival (OS) was calculated from the date of diagnosis to the date of death from any cause. PFS was calculated from the date of diagnosis to the date of disease progression or death from any cause. OS and PFS were analyzed by the Kaplan-Meier method [17], with between-group comparisons made using log-rank tests. Multivariate analyses with a Cox proportional multiple regression model were performed to assess the impact of clinical determination on OS and PFS. A P value <0.05 for a two-sided test was considered statistically significant. All statistical analyses were performed using Dr SPSS II software, release J (SPSS Japan, Tokyo, Japan). Results Patient characteristics We analyzed a total of 139 HL patients, and their demographics and clinical characteristics are summarized in Table 1. Median age at diagnosis was 34 years (range, years) with 83 male and 56 female patients. As a histologic distribution, 79 patients (57%) had nodular sclerosis (NS), 29 patients (21%) had mixed cellularity (MC), 5 patients (4%) had lymphocyte depletion (LD), 3 patients (2%) had lymphocyte rich (LR), and 12 patients (8%) had nodular lymphocyte predominant HL (NLPHL). Eleven patients (9%) had 8
9 classical HL, not otherwise specified. The performance status (PS) of the majority of patients was 0 or 1. Bulky disease was present in 31 patients (22%) and 28 of them had mediastinal bulky disease. Early stage and advanced stage were present in 83 (60%) and 56 (40%) patients, respectively. Among the advanced-stage patients, the numbers of patients with an IPS of 0-2 and 3 or higher were 32 (57%) and 24 (42%), respectively. In the present study, fourteen patients received high dose chemotherapy with autologous stem cell transplantation (HDC/ASCT) in first relapse. Five patients received allogeneic stem cell transplantation at the relapse after HDC/ASCT. Initial treatments and responses The details of the initial treatments and responses are shown in table 2. Among the 83 early-stage patients, 73 patients (88%) received chemotherapy followed by irradiation, while 22 (39%) of the 56 advanced-stage patients received chemotherapy followed by irradiation. The reasons for receiving irradiation after the chemotherapy in patients with advanced disease were as follows; clinical stage IIB (14 patients, 24%), initial bulky disease (4 patients, 8%), and residual disease after chemotherapy (4 patients, 8%). The overall response rates after the initial treatment in early-stage and advanced-stage were 97% and 93%, 9
10 respectively. Seventy-six early-stage patients (92%) achieved CR or CRu, while 46 (82%) advanced-stage patients achieved CR or CRu. Among the patients of all stages, 122 (87%) received ABVd therapy and the median number of cycles was 6 in early-stage and 8 in advanced-stage. Toxicities Table 3 lists the acute toxicities observed in the 122 patients who received ABVd therapy. The toxicities were assessed according to the criteria of NCI-CTCAE v4.0. The most frequent hematologic toxicity was neutropenia. Neutropenia with grade 3 and 4 was observed in 47 patients (39%) and 40 patients (33%), respectively. The most frequent non-hematologic toxicity was nausea/vomiting, which was observed in 55 patients (45%). Phlebitis, which was considered to be caused by dacarbazine, was observed in 22 patients (18%), and three of them used a central venous port system to avoid phlebitis. The toxicities caused treatment discontinuation were observed in 10 patients. Grade 3 pneumonitis induced by bleomycin and Pneumocystis jirovecii pneumonia was observed in one patient each. There was no treatment-related death. Secondary malignancies were observed in 5 patients (4%) during the follow-up 10
11 time (median 69 months, range: months). Three patients had solid tumors in the field of radiation therapy; one patient had basal cell carcinoma of the skin, one patient had esophageal cancer, and remaining one patient had mycosis fungoides. These tumors occurred approximately 10 years after the initial treatment of HL. One patient who did not receive irradiation in the initial HL treatment suffered breast cancer 3.6 years after chemotherapy. Hematologic malignancy was observed in 1 patient; the patient developed myelodysplastic syndrome one year after the completion of 8 cycles of ABVd. Cardio-vascular events were observed in 4 patients (3%). One of the 4 patients died of an acute coronary event, which occurred 8 years after thoracic irradiation for mediastinal bulky mass, and one patient had a first-degree atrioventricular block 4 years after thoracic irradiation. The remaining two patients, who had received ABVd without irradiation, had asymptomatic low left ventricular ejection fractions. Survival The PFS of 83 early-stage patients and 56 advanced-stage patients are shown in Fig. 1a and their 5-year PFS rates were estimated to be 90% and 71%, respectively. The PFS of advanced-stage patients was significantly worse than that of early-stage patients (p = 0.014). 11
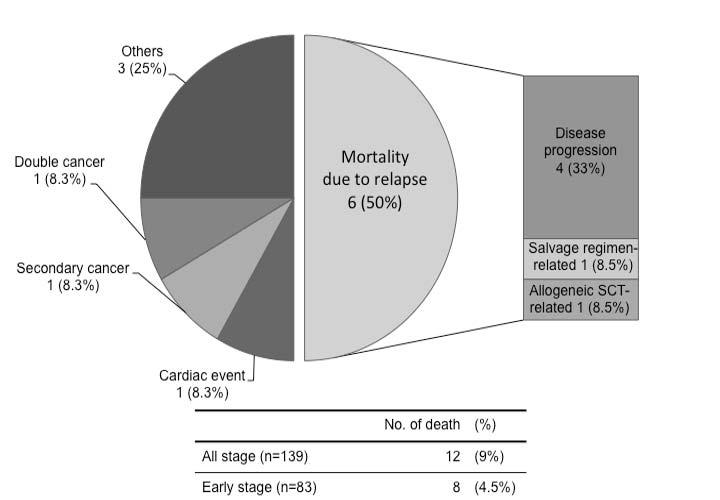
12 The five-year OS rates of early stage and advanced stage patients were estimated at 94% and 91%, respectively, with no significant difference (p = 0.95) (Fig. 1b). There were 12 deaths: 8 patients with early-stage disease and 4 patients with advanced-stage disease. The causes of death were as follows: disease progression in 4 patients (1 with early-stage disease and 3 with advanced-stage disease), a salvage regimen-related mortality (one patient), allogeneic stem cell transplantation-related mortality (one patient), cardiac event (one patient), secondary malignancy (one patient), double cancer; cancer diagnosed before the initial treatment of HL (one patient) and others (three patients) (Fig. 2). The results of univariate and multivariate analyses of various factors affecting PFS and OS are shown in Table 4. Among the early-stage patients, no variables were found to be significant adverse factors related to PFS and OS. On the other hand, in the advanced-stage patients, anemia and aged 70 or older were significant adverse factors related to PFS, but not to OS. Discussion Here, we report the treatment outcome of 139 Japanese patients with HL. The present study is the most recent analysis, with the largest number of patients, regarding the detailed treatment outcomes and clinical features of patients with HL in Japan. The OS and 12
13 PFS in the present study are as favorable as those of previous prospective clinical trials, even though the present study treatments were performed in a clinical practice setting. In other words, it is likely that the survival of HL patients failed to improve sufficiently compared with those previously reported, despite the development of supportive care in the last decade. Therefore, novel treatment strategies to improve the survival of HL patients are needed. The main previous reports on HL are shown in Table 5. In these studies, the 5-year survival rate for patients with early-stage HL has consistently been 90% or higher [18-20]. Our study also showed patients with early-stage HL has significantly high survival rate. Therefore, the late onset treatment-related toxicities, such as secondary malignancies and cardiac events, are thought to be a more significantly problematic issue to resolve in early-stage patients. The German Hodgkin Study Group (GHSG) reported that secondary malignancies occur at an average rate of approximately 1% per year for at least 30 years after treatment [21]. The risk is particularly high among women younger than 30 years of age who receive thoracic radiotherapy; breast cancer develops in 30 to 40% of these patients in the 25 years after treatment [22]. Radiation-related cardiac events are also an important problem. Swerdlow AJ, et al. reported that the risk of death from myocardial infarction is increased 13
14 after thoracic radiotherapy, and that the increased risk persists for more than 25 years [23]. In the present study, we experienced 5 secondary malignancies and 4 cardiac toxicities. Although this incidence was lower than that of previous reports, the median follow up duration, only 70 months, was too short to evaluate the actual incidence of these late-onset toxicities. Therefore, further follow-up is needed. The novel treatment strategy for early-stage HL, aims to reduce the late onset treatment related toxicities. The GHSG reported on a large-scale study that investigated the efficacy of reduced cycles of ABVD with or without reduction in the radiation dose. They concluded that 2 cycles of ABVD followed by 20 Gy of involved-field radiotherapy (IFRT) should be regarded as the standard of care in early favorable HL, with EFS of 91% and OS of 93% at 5 years [20]. On the other hand, advanced-stage HL patients still have a higher relapse rate compared with early-stage disease patients [9, 10, 24]. Several study groups have attempted to improve survival using intensive chemotherapies, such as BEACOPP and Stanford V [25-27]. These regimens may be more effective than ABVD and beneficial for some of the higher risk population; however, the higher rate of toxicities, both acute hematologic toxicities and late toxicities such as secondary malignancies, cardiovascular toxicities and infertility, make us 14
15 hesitate to perform these intensive regimens for all advanced-stage patients. Therefore, a method to reasonably select which of the higher risk population may benefit from intensive chemotherapy is needed. In our study, anemia, which is contained in the International Prognostic Score (IPS), was found to be an adverse risk for PFS. Engert A, et al. showed that the advantage of escalated BEACOPP is seen among all IPS subgroups and is not just restricted to the high-risk group; accordingly, the selection of high-risk patients by IPS is not a reliable strategy to discern the subset of patients who may benefit from dose intensification [28]. Recent studies showed that an interim PET scan after 2 cycles of ABVD predicts the prognosis of advanced-stage HL patients more clearly than IPS [29]. Interim PET-based risk-adapted approaches are expected to be useful for distinguishing between patients with a disease that is curable by ABVD and others who need a novel treatment strategy. Phase II trials to assess an interim PET-based response-adapted therapy with dose-escalated BEACOPP are currently ongoing in the United States (SWOG study; S0816, NCT ) [30] and in Japan (JCOG-LSG study; JCOG1305, UMIN ) [31]. Further refinement of the initial chemotherapeutic regimen combining a novel agent is also expected. Brentuximab vedotin (BV) is an antibody-drug conjugate targeting CD30. It is highly effective for relapsed/refractory HL and a promising treatment option for these 15
16 patients recently [32-34]. A phase I study of BV combined with ABVD or AVD for 51 patients with untreated advanced-stage HL was conducted and the CR rate was 96% with manageable toxicity [35]. Based on this study, a global phase III study to compare the clinical outcomes of ABVD with AVD plus BV is currently ongoing (NCT ) [36]. The optimal frontline treatment of elderly patients with HL is another important controversial issue. In the present study, the age 70 years or older was an adverse factor related to PFS in the patients with advanced-stage HL. Evans et al also reported the outcome of 95 elderly patients with HL (median age 67, range 60-89) and the age more than 70 years were associated to poor outcome [37]. In these populations, frailty and comorbidity are common and doxorubicin-containing regimens such as ABVD or BEACOPP are inappropriate because of their toxicities. Forero-Torres et al conducted a phase II study to assess the efficacy of brentuximab vedotin monotherapy as a frontline treatment in the elderly patients with HL [38]. Overall response rate was 92% among the 26 evaluable patients with 19 patients (73%) achieving complete remission. Further investigations regarding brentuximab vedotin-containing less toxic regimens as a frontline therapy are expected especially in the elderly patients with HL. The present study has several limitations. First, this is a single institutional 16
17 retrospective study; second, the various potential selection biases associated with this kind of retrospective analysis; third, a fewer number of patients compared with the clinical trials conducted in Western countries. Even so, there is no data available regarding Japanese patients with HL in recent years and the number of patients in this study is larger than other clinical studies previously reported in Japan. In conclusion, we showed the treatment outcomes of 139 Japanese patients with HL at a single institution. The treatment outcome was as favorable as previously reported, while the patients with advanced-stage disease still have lower PFS compared to the patients with early-stage disease. The present study will provide reference data in future clinical trials for Japanese patients with HL. A further prospective multicenter study is needed to establish a novel treatment strategy and evidence that supports our daily clinical practice on HL. Acknowledgments This work was supported in part by the National Cancer Center Research and Development Fund [26-A-4], a grant for cancer research (Practical Research for Innovative Cancer Control) from the Japan Agency for Medical Research and Development (AMED) and the Japan Society for the Promotion of Science (JSPS) Grant-in-Aid for Scientific Research 17
18 [C ]. We wish to thank the doctors, nurses and all medical staffs belonging to the Departments of Hematology and Hematopoietic Stem cell Transplantation at the National Cancer Center Hospital. Conflict of interest statement None declared. References 1. Morton LM, Wang SS, Devesa SS, Hartge P, Weisenburger DD, Linet MS. Lymphoma incidence patterns by WHO subtype in the United States, Blood. 2006;107: Connors JM. State-of-the-art therapeutics: Hodgkin's lymphoma. J Clin Oncol. 2005;23: Devita VT Jr, Serpick AA, Carbone PP. Combination chemotherapy in the treatment of advanced Hodgkin's disease. Ann Intern Med. 1970;73: Longo DL, Young RC, Wesley M, Hubbard SM, Duffey PL, Jaffe ES, et al. Twenty years of MOPP therapy for Hodgkin's disease. J Clin Oncol. 1986;4: Viviani S, Santoro A, Ragni G, Bonfante V, Bestetti O, Bonadonna G. Gonadal toxicity 18
19 after combination chemotherapy for Hodgkin's disease. Comparative results of MOPP vs ABVD. Eur J Cancer Clin Oncol. 1985;21: Canellos GP, Anderson JR, Propert KJ, Nissen N, Cooper MR, Henderson ES, et al. Chemotherapy of advanced Hodgkin's disease with MOPP, ABVD, or MOPP alternating with ABVD. N Engl J Med. 1992;327(21): Hoppe RT, Advani RH, Ai WZ, Ambinder RF, Aoun P, Bello CM, et al. Hodgkin lymphoma, version featured updates to the NCCN guidelines. J Natl Compr Canc Netw. 2012;10: Lymphoma Study Group of Japanese Pathologists. The World Health Organization classification of malignant lymphomas in Japan: Incidence of recently recognized entities. Pathol Int. 2000;50: Takenaka T, Mikuni C, Miura A, Sasaki T, Suzuki H, Hotta T, et al. Alternating combination chemotherapy C-MOPP (cyclophosphamide, vincristine, procarbazine, prednisone) and ABVd (adriamycin, bleomycin, vinblastine, dacarbazine) in clinical stage II-IV Hodgkin's disease: a multicenter phase II study (JCOG 8905). The Lymphoma Study Group of the Japan Clinical Oncology Group. Jpn J Clin Oncol. 2000;30:
20 10. Ogura M, Itoh K, Kinoshita T, Fukuda H, Takenaka T, Ohtsu T, et al. Phase II study of ABVd therapy for newly diagnosed clinical stage II-IV Hodgkin lymphoma: Japan Clinical Oncology Group study (JCOG 9305). Int J Hematol. 2010;92: Ogura M, Itoh K, Ishizawa K, Kobayashi Y, Tobinai K, Kinoshita T, et al. Phase II study of ABV (doxorubicin with increased dose, bleomycin and vinblastine) therapy in newly diagnosed advanced-stage Hodgkin lymphoma: Japan Clinical Oncology Group study (JCOG9705). Leuk Lymphoma. 2013;54: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al., editors. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4 th ed. Lyon: IARC Press 2008; Carbone PP, Kaplan HS, Musshoff K, Smithers DW, Tubiana M. Report of the Committee on Hodgkin's Disease staging classification. Cancer Res. 1971;31: Hasenclever D, Diehl V, Armitage JO, Assouline D, Björkholm M, Brusamolinoet E, et al. A prognostic score for advanced Hodgkin's disease. International Prognostic Factors Project on Advanced Hodgkin's Disease. N Eng J Med. 1998;339: Cheson BD, Horning SJ, Coiffier B, Shipp MA, Fisher RI, Connors JM, et al. Report of an International Workshop to standardize response criteria for non-hodgkin's 20
21 lymphomas. J Clin Oncol. 1999;17: Cheson BD, Pfistner B, Juweid ME, Gascoyne RD, Specht L, Horning SJ, et al. Revised response criteria for malignant lymphoma. J Clin Oncol. 2007;25: Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc. 1958;53: Meyer RM, Gospodarowicz MK, Connors JM, Pearcey RG, Bezjak A, Wells WA, et al. Randomized comparison of ABVD chemotherapy with a strategy that includes radiation therapy in patients with limited-stage Hodgkin's lymphoma: National Cancer Institute of Canada Clinical Trials Group and the Eastern Cooperative Oncology Group. J Clin Oncol. 2005;23: Straus DJ, Portlock CS, Qin J, Myers J, Zelenetz AD, Moskowitz C, et al. Results of a prospective randomized clinical trial of doxorubicin, bleomycin, vinblastine, and dacarbazine (ABVD) followed by radiation therapy (RT) versus ABVD alone for stages I, II, and IIIA nonbulky Hodgkin disease. Blood. 2004;104: Engert A, Plütschow A, Eich HT, Lohri A, Dörken B, Borchmann P, et al. Reduced treatment intensity in patients with early-stage Hodgkin's lymphoma. N Eng J Med. 2010;363:
22 21. Franklin J, Pluetschow A, Paus M, Specht L, Anselmo AP, Aviles A, et al. Second malignancy risk associated with treatment of Hodgkin s lymphoma: meta-analysis of the randomized trials. Ann Oncol. 2006;17: Travis LB, Hill D, Dores GM, Gospodarowicz M, van Leeuwen FE, Holowaty E, et al. Cumulative absolute breast cancer risk for young women treated for Hodgkin lymphoma. J Natl Cancer Inst. 2005;97: Swerdlow AJ, Higgins CD, Smith P, Cunningham D, Hancock BW, Horwich A, et al. Myocardial infarction mortality risk after treatment for Hodgkin disease: a collaborative British cohort study. J Natl Cancer Inst. 2007;99: Duggan DB, Petroni GR, Johnson JL, Glick JH, Fisher RI, Connors JM, et al. Randomized comparison of ABVD and MOPP/ABV hybrid for the treatment of advanced Hodgkin's disease: report of an intergroup trial. J Clin Oncol. 2003;21: Diehl V, Franklin J, Pfreundschuh M, Lathan B, Paulus U, Hasenclever D, et al. Standard and increased-dose BEACOPP chemotherapy compared with COPP-ABVD for advanced Hodgkin's disease. N Engl J Med. 2003;348: Gobbi PG, Levis A, Chisesi T, Broglia C, Vitolo U, Stelitano C, et al. ABVD versus modified stanford V versus MOPPEBVCAD with optional and limited radiotherapy in 22
23 intermediate- and advanced-stage Hodgkin's lymphoma: final results of a multicenter randomized trial by the Intergruppo Italiano Linfomi. J Clin Oncol. 2005;23: Viviani S, Zinzani PL, Rambaldi A, Brusamolino E, Levis A, Bonfante V, et al. ABVD versus BEACOPP for Hodgkin's lymphoma when high-dose salvage is planned. N Engl J Med. 2011;365: Engert A, Diehl V, Franklin J, Lohri A, Dörken B, Ludwig WD, et al. Escalated-dose BEACOPP in the treatment of patients with advanced-stage Hodgkin's lymphoma: 10 years of follow-up of the GHSG HD9 study. J Clin Oncol : Gallamini A, Hutchings M, Rigacci L, Specht L, Merli F, Hansen M, et al. Early interim 2-[18F]fluoro-2-deoxy-D-glucose positron emission tomography is prognostically superior to international prognostic score in advanced-stage Hodgkin's lymphoma: a report from a joint Italian-Danish study. J Clin Oncol. 2007;25: Fludeoxyglucose F 18-PET/CT imaging and combination chemotherapy with or without additional chemotherapy and G-CSF in treating patients with stage III or stage IV Hodgkin lymphoma. Accessed October 1, Non-randomized confirmatory study of interim PET-guided ABVD or ABVD/escalated 23
24 BEACOPP regimen for previously untreated advanced stage Hodgkin lymphoma (JCOG1305, INNOVATE-HL study). summary&recptno=r &language=e. Accessed November 20, Younes A, Bartlett NL, Leonard JP, Kennedy DA, Lynch CM, Sievers EL, et al. Brentuximab vedotin (SGN-35) for relapsed CD30-positive lymphomas. N Engl J Med. 2010;363: Younes A, Gopal AK, Smith SE, Ansell SM, Rosenblatt JD, Savage KJ, et al. Results of a pivotal phase II study of brentuximab vedotin for patients with relapsed or refractory Hodgkin's lymphoma. J Clin Oncol. 2012;30: Eichenauer DA, Engert A. Advances in the treatment of Hodgkin lymphoma. Int J Hematol. 2012;96: Younes A, Connors JM, Park SI, Fanale M, O'Meara MM, Hunder NN, et al. Brentuximab vedotin combined with ABVD or AVD for patients with newly diagnosed Hodgkin's lymphoma: a phase 1, open-label, dose-escalation study. Lancet Oncol. 2013;14: Phase 3 Frontline Therapy Trial in Patients With Advanced Classical Hodgkin 24
25 Lymphoma. Accessed October 1, Evens AM, Helenowski I, Ramsdale E, Nabhan C, Karmali R, Hanson B, et al. A retrospective multicenter analysis of elderly Hodgkin lymphoma: outcomes and prognostic factors in the modern era. Blood. 2012;119: Forero-Torres A, Holkova B, Goldschmidt J, Chen R, Olsen G, Boccia RV, et al. Phase 2 study of frontline brentuximab vedotin monotherapy in Hodgkin lymphoma patients aged 60 years and older. Blood. 2015;126:
26 TABLES Table 1. Patient characteristics Table 2. Treatment modalities, regimens and response Table 3. Toxicities of ABVd with or without irradiation Table 4-1. The risk factors in the 83 early-stage patients Table 4-1. The risk factors in the 56 advanced-stage patients Table 5. Previous reports of HL 26
27 FIGURE LEGENDS Figure 1. The progression free survival (PFS) (a) and overall survival (OS) (b) of the patients with Hodgkin lymphoma in the present study with a median follow-up duration of 69 months. The estimated 5-year PFS rates for patients with early-stage disease (solid line) and advanced-stage disease (dashed line) were 90% and 71%, respectively. The 5-year OS rates for patients with early-stage disease (solid line) and advanced-stage disease (dashed line) were 94% and 90%, respectively. The PFS of advanced-stage patients was significantly worse than that of early-stage patients (p = 0.014), whereas the OS was not (p = 0.95). Figure 2. Causes of death in the present study 27
28 Table1 Patient characteristics ( N=139 ) n (%) Age median (years) 34 range Gender male 83 (60%) female 56 (40%) Histology NS 79 (57%) MC 29 (21%) LD 5 (4%) LR 3 (2%) NLPHL 12 (8%) Classical HL, NOS 11 (8%) PS (97%) 2 3 (2%) 3 1 (1%) Clinical stage Early stage IA 27 (20%) IB 3 (2%) IIA 53 (38%) Advanced stage IIB 15 (11%) IIIA 14 (10%) IIIB 3 (2%) IVA 14 (10%) IVB 10 (7%) Bulky disease Yes 31 (22%) mediastinal 28 (20%) non-mediastinal 3 (2%) International Prognostic Score* (N=56) 0 5 (9%) 1 10 (18%) 2 17 (30%) 3 7 (12%) 4 16 (29%) 5 1 (2%) NS nodular sclerosis; MC mixed cellularity; LD lymphocyte depletion; LR lymphocyte-rich; NLPHL nodular lymphocyte predominant HL; PS performance status *Assessed in 61 advanced disease patients
29 Table 2 Treatment modalities, regimens and response Modalities n (%) Early-stage Chemotherapy and RT 73 (88%) (N=83) RT alone 6 (7.2%) Chemotherapy alone 4 (4.8%) Advanced-stage Chemotherapy and RT 22 (39%) (N=56) RT alone 0 Chemotherapy alone 34 (61%) Regimen of chemotherapy n (%) Early-stage ABVd 74 (96%) (N=77) (median 6 cycles, range: 2-8 cycles) Others 3 (4%) Advanced-stage ABVd 48 (86%) (N=56) (median 8 cycles, range: 2-8 cycles) C-MOPP 3 (5%) Others 5 (9%) Response n (%) Early-stage CR/CRu 76 (92%) (N=83) PR 4 (5%) Advanced-stage CR/CRu 46 (82%) (N=56) PR 6 (11%) RT radiotherapy; CR complete remission; CRu complete remission unconfirmed ; PR partial remission; ABVd adriamycin, bleomycin, vinblastine, and dacarbazine; C-MOPP cyclophosphamide, vincristine, procarbazine,and prednisone
30 Table 3 Toxicities of ABVd with or without irradiation (N=122) Grade1/2 Grade 3 Grade 4 Adverse event n (%) n (%) n (%) Leukopenia 108 (89%) 4 (3%) 0 Neutropenia 24 (20%) 47 (39%) 40 (33%) Anemia 107 (88%) 0 0 Thrombocytopenia 7 (8%) 0 0 Febrile Neutropenia - 18 (15%) 2 (2%) Fever 12 (10%) 0 0 Nausea/vomitting 54 (44%) 1 (1%) - Phlebitis 22 (18%) - -
31 Table 4-1 The risk factors in the 83 early-stage patients Univaliate analysis PFS OS Variable n HR (95%CI) P value HR (95%CI) P value Mediastinal bulky disease Yes ( ) ( ).77 No 66 Age ( ) ( ).68 <45 63 LDH Within normal range ( ) ( ).67 Without normal range 41 B symptoms Yes (.42-35) (.53-35).17 No 80 LDH lactate dehydrogenase; HR hazard ratio; CI confidence interval
32 Table 4-2 The risk factors in the 56 advanced-stage patients PFS OS Univariate analysis Multivariate analysis Univariate analysis Variable n HR (95% CI) P value HR (95%CI) P value HR (95% CI) P value Serum albumin <40 g/l ( ).21 ー 2.9 (.30-28) g/l 25 Hemoglobin <105 g/l (1.1-11) (1.1-11) (.31-28) g/l 50 LDH Within normal range ( ).76 ー.39 ( ).41 Without normal range 23 Clinical stage IV Yes ( ).13 ー 4.9 (.50-47).17 No 32 Age 70 years (1.7-22) (1.7-24) (.63-64).12 <70 years 52 WBC count 15 x 10 9 /L ( ).39 ー 1.2 (.13-12).86 <15 x 10 9 /L 44 Lymphocyte count <0.6 x 10 9 /L or <8% ( ).89 ー 2.6 (.27-25) x 10 9 /L 50
33 Table 5 Previous reports of HL Early stage Advanced stage Author Clinical stage year of recruitment Treatment No. of Pts %CR %OS (5yr) %PFS (5yr) Meyer et al. I-IIA ABVD 4-6 cycles 196 NA (JCO 2005, NCIC-CTG) vs SNRT (35Gy) Straus et al. I-IIIA ABVD 6 cycles (Blood 2004, MSKCC) vs ABVD 6cycles + IFRT Engert et al. Early-stage ABVD 4 cycles + IFRT 30Gy (NEJM 2010, GHSGwith low risk ABVD 4 cycles + IFRT 20Gy ABVD 2 cycles + IFRT 30Gy ABVD 2 cycles + IFRT 30Gy Present study I-IIA ABVd etc. ± RT Duggan et al. III/IV - ABVD (JCO 2003, CALGB and ECOG) vs MOPP/ABV Diehl et al. IIB-IV dose-escalated BEACOPP (NEJM 2003, GHSG) standard BEACOPP COPP/ABVD Gobbi et al. IIB-IV ABVD (JCO 2005, Italy) Stanford V MOPPEBVCAD Viviani et al. IIB-IV ABVD (NEJM 2011,Italy ) BEACOPP Takenaka et al. II-IV C-MOPP/ABVD (JJCO 2000, JCOG8905) Ogura et al. II-IV ABVd (Int J Hematol 2010, JCOG9305) Present study IIB-IV ABVd etc NCIC-CTG National Cancer Institute of Canada Clinical Trials Group; ABVD adriamycin, bleomycin, vinblastine, and dacarbazine; SNRT subtotal nodal radiation therapy; MSKCC Memorial Sloan Kettering Cancer Center; IFRT involved-field radiation therapy; MOPP mechlorethamine, vincristine, procarbazine, and prednisone; GHSG German Hodgkin Study Group; CALGB Cancer and Leukemia Group B; ECOG Eastern Cooperative Oncology Group; BEACOPP bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone; COPP cyclophosphamide, vincristine, procarbazine, and prednisone; MOPPEBVCAD mechlorethamine, vincristine, procarbazine, prednisone, epidoxirubicin, bleomycin, vinblastine, lomustine, doxorubicin, and vindesine; C-MOPP cyclophosphamide, vincristine, procarbazine, and prednisone.
34
35
36
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma
 with classical Hodgkin lymphoma") PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
German Hodgkin Study Group
 German Hodgkin Study Group Deutsche Hodgkin Studiengruppe Avoiding Relapse of Hodgkin Lymphoma: Have We Moved The Needle? Andreas Engert, MD Chairman, German Hodgkin Study Group University Hospital of
German Hodgkin Study Group Deutsche Hodgkin Studiengruppe Avoiding Relapse of Hodgkin Lymphoma: Have We Moved The Needle? Andreas Engert, MD Chairman, German Hodgkin Study Group University Hospital of
Advanced stage HL The old and new match: BEACOPP
 27.03.2015 1 Advanced stage HL The old and new match: BEACOPP Peter Borchmann German Hodgkin Study Group University of Cologne, Germany Which answer is wrong? For patients with advanced stage HL, treatment
27.03.2015 1 Advanced stage HL The old and new match: BEACOPP Peter Borchmann German Hodgkin Study Group University of Cologne, Germany Which answer is wrong? For patients with advanced stage HL, treatment
End-of-treatment but not interim PET scan predicts outcome in nonbulky limited-stage Hodgkin s lymphoma
 original article Annals of Oncology 22: 910 915, 2011 doi:10.1093/annonc/mdq549 Published online 15 October 2010 original article End-of-treatment but not interim PET scan predicts outcome in nonbulky
original article Annals of Oncology 22: 910 915, 2011 doi:10.1093/annonc/mdq549 Published online 15 October 2010 original article End-of-treatment but not interim PET scan predicts outcome in nonbulky
PET-Guided Treatment Approach for Advanced Stage Classical Hodgkin Lymphoma. Ranjana H. Advani, MD
 PET-Guided Treatment Approach for Advanced Stage Classical Hodgkin Lymphoma Ranjana H. Advani, MD Stanford Cancer Institute Management of Hodgkin Lymphoma Learning Objectives Review risk adapted strategies
PET-Guided Treatment Approach for Advanced Stage Classical Hodgkin Lymphoma Ranjana H. Advani, MD Stanford Cancer Institute Management of Hodgkin Lymphoma Learning Objectives Review risk adapted strategies
Hodgkin Lymphoma Status of the art of treatment
 11.05.2016 1 Hodgkin Lymphoma Status of the art of treatment Peter Borchmann German Hodgkin Study Group University of Cologne, Germany Question No 1: Which statement regarding 1 st line treatment of early
11.05.2016 1 Hodgkin Lymphoma Status of the art of treatment Peter Borchmann German Hodgkin Study Group University of Cologne, Germany Question No 1: Which statement regarding 1 st line treatment of early
Printed by Martina Huckova on 10/3/2011 3:04:43 PM. For personal use only. Not approved for distribution. Copyright 2011 National Comprehensive
 NCCN Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform NCCN consensus. Category 2A: The recommendation
NCCN Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform NCCN consensus. Category 2A: The recommendation
Serum levels of soluble CD30 improve International Prognostic Score in predicting the outcome of advanced Hodgkin s lymphoma
 Original article Annals of Oncology 13: 1908 1914, 2002 DOI: 10.1093/annonc/mdf333 Serum levels of soluble CD30 improve International Prognostic Score in predicting the outcome of advanced Hodgkin s lymphoma
Original article Annals of Oncology 13: 1908 1914, 2002 DOI: 10.1093/annonc/mdf333 Serum levels of soluble CD30 improve International Prognostic Score in predicting the outcome of advanced Hodgkin s lymphoma
ABVD versus BEACOPP arguments for ABVD. Dr Pauline BRICE Hôpital saint louis Université Paris VII PARIS
 ABVD versus BEACOPP arguments for ABVD Dr Pauline BRICE Hôpital saint louis Université Paris VII PARIS DISCLOSURES HONORARIAS: Takeda, roche GRANT RESEARCH : Millenium Takeda, AMGEN ABVD the standard chemotherapy
ABVD versus BEACOPP arguments for ABVD Dr Pauline BRICE Hôpital saint louis Université Paris VII PARIS DISCLOSURES HONORARIAS: Takeda, roche GRANT RESEARCH : Millenium Takeda, AMGEN ABVD the standard chemotherapy
Radiation therapy has a dramatic effect on lymphomas, and has played an important role in treating Hodgkin
 COUNTERPOINTS Current Controversies in Hematology and Oncology Can Radiotherapy Be Omitted in Patients With Localized Hodgkin Lymphoma? Radiation therapy has a dramatic effect on lymphomas, and has played
COUNTERPOINTS Current Controversies in Hematology and Oncology Can Radiotherapy Be Omitted in Patients With Localized Hodgkin Lymphoma? Radiation therapy has a dramatic effect on lymphomas, and has played
HODGKIN LYMPHOMA Updated February 2016 by Dr. Manna (PGY 5 Hematology Resident, University of Calgary)
") HODGKIN LYMPHOMA Updated February 2016 by Dr. Manna (PGY 5 Hematology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff
HODGKIN LYMPHOMA Updated February 2016 by Dr. Manna (PGY 5 Hematology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff
Relapsed/Refractory Hodgkin Lymphoma
 Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
Limited-Stage Disease: Optimal Use of Chemotherapy and Radiation Treatment
 HODGKIN LYMPHOMA: CLINICAL CHALLENGES Limited-Stage Disease: Optimal Use of Chemotherapy and Radiation Treatment John Radford 1 1 Professor of Medical Oncology, Christie Hospital and The University of
HODGKIN LYMPHOMA: CLINICAL CHALLENGES Limited-Stage Disease: Optimal Use of Chemotherapy and Radiation Treatment John Radford 1 1 Professor of Medical Oncology, Christie Hospital and The University of
Evolving Approaches to Primary Treatment of Hodgkin Lymphoma
 Evolving Approaches to Primary Treatment of Hodgkin Lymphoma Joseph M. Connors Two challenges confront the clinician treating Hodgkin lymphoma today: achieving a high level of effectiveness while minimizing
Evolving Approaches to Primary Treatment of Hodgkin Lymphoma Joseph M. Connors Two challenges confront the clinician treating Hodgkin lymphoma today: achieving a high level of effectiveness while minimizing
XVIII. Management of nodular lymphocyte predominant Hodgkin lymphoma
 Hematological Oncology Hematol Oncol 2015; 33: 90 95 Published online in Wiley Online Library (wileyonlinelibrary.com).2226 Supplement Article XVIII. Management of nodular lymphocyte predominant Hodgkin
Hematological Oncology Hematol Oncol 2015; 33: 90 95 Published online in Wiley Online Library (wileyonlinelibrary.com).2226 Supplement Article XVIII. Management of nodular lymphocyte predominant Hodgkin
ABVD or BEACOPP for advanced Hodgkin lymphoma. Not to BEACOPP. Massimo Federico University of Modena and Reggio Emilia Italy
 ABVD or BEACOPP for advanced Hodgkin lymphoma Not to BEACOPP Massimo Federico University of Modena and Reggio Emilia Italy What is the best Induction Therapy for Advanced Hodgkin Lymphoma? How to treat
ABVD or BEACOPP for advanced Hodgkin lymphoma Not to BEACOPP Massimo Federico University of Modena and Reggio Emilia Italy What is the best Induction Therapy for Advanced Hodgkin Lymphoma? How to treat
Treatment of Forty Adult Patients with Hodgkin Disease; Baghdad Teaching Hospital Experience
 Original Article Treatment of Forty Adult Patients with Hodgkin Disease; Baghdad Teaching * Alaadin S. Naji* Ahmed A. AL - Saffar* Mazin A. Shubbar* Bassam F. Matti* Adil Siwan* Ammar F. Majeed* Ali M.Jawad*
Original Article Treatment of Forty Adult Patients with Hodgkin Disease; Baghdad Teaching * Alaadin S. Naji* Ahmed A. AL - Saffar* Mazin A. Shubbar* Bassam F. Matti* Adil Siwan* Ammar F. Majeed* Ali M.Jawad*
Lymphocyte Predominant Hodgkin s Lymphoma. Case Presentation. How would you treat the patient?
 Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Treatment of Early Stage Hodgkin Lymphoma. Massimo Federico University of Modena and Reggio Emilia Città di Lecce Hospital - GVM Care & Research
 Treatment of Early Stage Hodgkin Lymphoma Massimo Federico University of Modena and Reggio Emilia Città di Lecce Hospital - GVM Care & Research Conflict of Interest Disclosure I hereby declare the following
Treatment of Early Stage Hodgkin Lymphoma Massimo Federico University of Modena and Reggio Emilia Città di Lecce Hospital - GVM Care & Research Conflict of Interest Disclosure I hereby declare the following
Risk, Cure and Complications in Advanced Hodgkin Disease
 Risk, Cure and Complications in Advanced Hodgkin Disease Sandra J. Horning Stanford University, Stanford, CA Current therapy for Hodgkin disease is aimed at high cure rates and optimal survivorship. Although
Risk, Cure and Complications in Advanced Hodgkin Disease Sandra J. Horning Stanford University, Stanford, CA Current therapy for Hodgkin disease is aimed at high cure rates and optimal survivorship. Although
Practical Application of PET adapted Therapy in Hodgkin Lymphoma
 Practical Application of PET adapted Therapy in Hodgkin Lymphoma Matthew Matasar, MD Lymphoma and Adult BMT Services Director, Lymphoma Survivorship Clinic Memorial Sloan Kettering Cancer Center New York,
Practical Application of PET adapted Therapy in Hodgkin Lymphoma Matthew Matasar, MD Lymphoma and Adult BMT Services Director, Lymphoma Survivorship Clinic Memorial Sloan Kettering Cancer Center New York,
Hodgkin Lymphoma-Stage III and IV EVIDENCE TABLE
 . Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed. Lyon, France: IARC Press; 2008. 2. Lister TA, Crowther D, Sutcliffe SB, et al. Report
. Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed. Lyon, France: IARC Press; 2008. 2. Lister TA, Crowther D, Sutcliffe SB, et al. Report
Lymphocyte-Depleted Classical Hodgkin s Lymphoma: A Comprehensive Analysis From the German Hodgkin Study Group
 Published Ahead of Print on September 12, 211 as 1.12/JCO.211.36.473 The latest version is at http://jco.ascopubs.org/cgi/doi/1.12/jco.211.36.473 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R
Published Ahead of Print on September 12, 211 as 1.12/JCO.211.36.473 The latest version is at http://jco.ascopubs.org/cgi/doi/1.12/jco.211.36.473 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R
Interim PET Hodgkin s Disease. Fellows talk Fellow: Shweta Jain Faculty: Ajay Gopal
 Interim PET Hodgkin s Disease Fellows talk Fellow: Shweta Jain Faculty: Ajay Gopal Why is this a Question? Early Advanced ipet ABVD + RT ABVD Pos Neg ABVD Beacopp Escalation Salvage Deescalation Talk outline
Interim PET Hodgkin s Disease Fellows talk Fellow: Shweta Jain Faculty: Ajay Gopal Why is this a Question? Early Advanced ipet ABVD + RT ABVD Pos Neg ABVD Beacopp Escalation Salvage Deescalation Talk outline
Hodgkin Lymphoma in Older Patients
 Hodgkin Lymphoma in Older Patients Andrew M. Evens, DO, MSc March 26 th, 2015 Professor of Medicine Chief, Division of Hematology/Oncology Director, Tufts Cancer Center Tufts Medical Center Elderly Hodgkin
Hodgkin Lymphoma in Older Patients Andrew M. Evens, DO, MSc March 26 th, 2015 Professor of Medicine Chief, Division of Hematology/Oncology Director, Tufts Cancer Center Tufts Medical Center Elderly Hodgkin
Hodgkin Lymphoma Review of characteristics and treatment of elderly patients
 Hodgkin Lymphoma Review of characteristics and treatment of elderly patients Boris Böll M.D. German Hodgkin Study Group (GHSG) University Hospital Cologne OS of HL patients in all stages 1960-1967 Courtesy
Hodgkin Lymphoma Review of characteristics and treatment of elderly patients Boris Böll M.D. German Hodgkin Study Group (GHSG) University Hospital Cologne OS of HL patients in all stages 1960-1967 Courtesy
First Line Management of Classical Hodgkin Lymphoma
 First Line Management of Classical Hodgkin Lymphoma George Follows Cambridge University Hospitals NHS Foundation Trust george.follows@addenbrookes.nhs.uk The controversial areas Early stage non-bulky /
First Line Management of Classical Hodgkin Lymphoma George Follows Cambridge University Hospitals NHS Foundation Trust george.follows@addenbrookes.nhs.uk The controversial areas Early stage non-bulky /
Original Articles. Etoposide, vinblastine, adriamycin and prednisolone (EVAP) combination chemotherapy as first-line treatment for Hodgkin s disease
 combination chemotherapy as first-line treatment for Hodgkin s disease") RUPALI et al. : AETIOLOGY OF PROLONGED FEVER IN HIV-INFECTED ADULTS Original Articles 189 Etoposide, vinblastine, adriamycin and prednisolone (EVAP) combination chemotherapy as first-line treatment for
RUPALI et al. : AETIOLOGY OF PROLONGED FEVER IN HIV-INFECTED ADULTS Original Articles 189 Etoposide, vinblastine, adriamycin and prednisolone (EVAP) combination chemotherapy as first-line treatment for
Elderly Patients with Hodgkin s Lymphoma: FIL experience. Massimo Federico University of Modena and Reggio Emilia
 Elderly Patients with Hodgkin s Lymphoma: FIL experience Massimo Federico University of Modena and Reggio Emilia RESULTS OF VbMp CHEMOTHERAPY REGIMEN IN ELDERLY PATIENTS WITH HODGKIN DISEASE: THE GISL
Elderly Patients with Hodgkin s Lymphoma: FIL experience Massimo Federico University of Modena and Reggio Emilia RESULTS OF VbMp CHEMOTHERAPY REGIMEN IN ELDERLY PATIENTS WITH HODGKIN DISEASE: THE GISL
The Present: Optimizing Therapy Too Much or Too Little?
 CLINICAL ADVANCES IN HODGKIN LYMPHOMA The Present: Optimizing Therapy Too Much or Too Little? Nancy L. Bartlett 1 1 Siteman Cancer Center, Washington University, St. Louis, MO Despite the use of less toxic
CLINICAL ADVANCES IN HODGKIN LYMPHOMA The Present: Optimizing Therapy Too Much or Too Little? Nancy L. Bartlett 1 1 Siteman Cancer Center, Washington University, St. Louis, MO Despite the use of less toxic
Update: Non-Hodgkin s Lymphoma
 2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
Hodgkin Lymphoma. Barbara Pro, MD Robert H. Lurie Comprehensive Cancer Center of Northwestern University Chicago, Illinois
 Hodgkin Lymphoma Barbara Pro, MD Robert H. Lurie Comprehensive Cancer Center of Northwestern University Chicago, Illinois Hodgkin Lymphoma Successes and Challenges The success 80 % of patients achieve
Hodgkin Lymphoma Barbara Pro, MD Robert H. Lurie Comprehensive Cancer Center of Northwestern University Chicago, Illinois Hodgkin Lymphoma Successes and Challenges The success 80 % of patients achieve
2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA
 2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA SUSQUEHANNA HEALTH David B. Nagel, M.D. April 11, 2008 Hodgkin s lymphoma was first described by Thomas Hodgkin in 1832. It remained an incurable malignancy until
2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA SUSQUEHANNA HEALTH David B. Nagel, M.D. April 11, 2008 Hodgkin s lymphoma was first described by Thomas Hodgkin in 1832. It remained an incurable malignancy until
Hodgkin. The PET World. Sally Barrington
 Hodgkin The PET World Sally Barrington PET-CT Staging in HL PET-CT changes stage 15-30% RATHL - Advanced HL 1171 pts Stage by PET-CT compared with cect and BMB 20% stage change; upstaging 14% Most upstaging
Hodgkin The PET World Sally Barrington PET-CT Staging in HL PET-CT changes stage 15-30% RATHL - Advanced HL 1171 pts Stage by PET-CT compared with cect and BMB 20% stage change; upstaging 14% Most upstaging
Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL
 New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
Primary treatment of Hodgkin s disease
 DOI: 10.1093/annonc/mdf653 Primary treatment of Hodgkin s disease G. P. Canellos Dana-Farber Cancer Institute, Harvard Medical School, Boston, Massachusetts, USA Introduction Therapeutic research in human
DOI: 10.1093/annonc/mdf653 Primary treatment of Hodgkin s disease G. P. Canellos Dana-Farber Cancer Institute, Harvard Medical School, Boston, Massachusetts, USA Introduction Therapeutic research in human
Linfoma de Hodgkin. Novos medicamentos. Otavio Baiocchi CRM-SP
 Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
Bleomycin versus Brentuximab in Hodgkin Lymphoma: Don t Hold Your Breath
 Bleomycin versus Brentuximab in Hodgkin Lymphoma: Don t Hold Your Breath Rachel Bubik, PharmD, BCPS PGY-2 Hematology/Oncology Pharmacy Resident January 8 th, 2019 2017 MFMER slide-1 Objectives 1. Explain
Bleomycin versus Brentuximab in Hodgkin Lymphoma: Don t Hold Your Breath Rachel Bubik, PharmD, BCPS PGY-2 Hematology/Oncology Pharmacy Resident January 8 th, 2019 2017 MFMER slide-1 Objectives 1. Explain
Late relapse of Hodgkin s lymphoma is it different in clinical characteristics and outcome?
 JBUON 2017; 22(2): 481-486 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Late relapse of Hodgkin s lymphoma is it different in clinical characteristics
JBUON 2017; 22(2): 481-486 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Late relapse of Hodgkin s lymphoma is it different in clinical characteristics
Hodgkin Lymphoma Which Group of Patients benefits from the use of BEACOPP. Volker Diehl for the German Hodgkin Study Group
 Hodgkin Lymphoma Which Group of Patients benefits from the use of BEACOPP Volker Diehl for the German Hodgkin Study Group Moscow 25.October 2007 HD8 trial design CS IA, IB, IIA,B with risk factors Random
Hodgkin Lymphoma Which Group of Patients benefits from the use of BEACOPP Volker Diehl for the German Hodgkin Study Group Moscow 25.October 2007 HD8 trial design CS IA, IB, IIA,B with risk factors Random
On behalf of the Israel Cooperative Lymphoma Group. A. Avigdor, S. Bulvik, I. Levi, E. Dann, A. Nagler, I. Ben-Bassat and A.
 Two cycles of escalated BEACOPP followed by four cycles of ABVD utilizing early-interim PET/CT scan for patients with advanced highrisk Hodgkin s lymphoma A. Avigdor, S. Bulvik, I. Levi, E. Dann, A. Nagler,
Two cycles of escalated BEACOPP followed by four cycles of ABVD utilizing early-interim PET/CT scan for patients with advanced highrisk Hodgkin s lymphoma A. Avigdor, S. Bulvik, I. Levi, E. Dann, A. Nagler,
Bendamustine for Hodgkin lymphoma. Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service
 Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
For more than a century after Thomas Hodgkin first described
 The new england journal of medicine review article Current Concepts Early-Stage Hodgkin s Lymphoma James O. Armitage, M.D. For more than a century after Thomas Hodgkin first described the disease that
The new england journal of medicine review article Current Concepts Early-Stage Hodgkin s Lymphoma James O. Armitage, M.D. For more than a century after Thomas Hodgkin first described the disease that
Brentuximab Vedotin in Lymphomas
 New Drugs In Hematology Brentuximab Vedotin in Lymphomas Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center Monday, May 9, 2016 9:15-9:45 a.m U.S. Cancer Statistics 2016 300.000
New Drugs In Hematology Brentuximab Vedotin in Lymphomas Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center Monday, May 9, 2016 9:15-9:45 a.m U.S. Cancer Statistics 2016 300.000
Response Adapted treatment of chl using BV in first line. Massimo Federico University of Modena and Reggio Emilia Italy
 Response Adapted treatment of chl using BV in first line Massimo Federico University of Modena and Reggio Emilia Italy From the book of 18FDG-PET in BV treatment patients 1 In the beginning Seattle Genetics
Response Adapted treatment of chl using BV in first line Massimo Federico University of Modena and Reggio Emilia Italy From the book of 18FDG-PET in BV treatment patients 1 In the beginning Seattle Genetics
Hodgkin Lymphoma-Unfavorable Clinical Stage I and II EVIDENCE TABLE
 . Kaplan HS. Evidence for a tumoricidal dose level in the radiotherapy of Hodgkin's disease. Cancer Res. 966;6(6):-4.. Rosenberg SA, Kaplan HS. Evidence for an orderly progression in the spread of Hodgkin's
. Kaplan HS. Evidence for a tumoricidal dose level in the radiotherapy of Hodgkin's disease. Cancer Res. 966;6(6):-4.. Rosenberg SA, Kaplan HS. Evidence for an orderly progression in the spread of Hodgkin's
Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA
 Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA Objectives Describe the current standard approach for patients with relapsed/refractory
Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA Objectives Describe the current standard approach for patients with relapsed/refractory
Comparison of Three Radiation Dose Levels after EBVP Regimen in Favorable Supradiaphragmatic Clinical Stages I-II Hodgkin s Lymphoma (HL):
:") Comparison of Three Radiation Dose Levels after EBVP Regimen in Favorable Supradiaphragmatic Clinical Stages I-II Hodgkin s Lymphoma (HL): Preliminary Results of the EORTC-GELA H9-F Trial H. Eghbali, P.
Comparison of Three Radiation Dose Levels after EBVP Regimen in Favorable Supradiaphragmatic Clinical Stages I-II Hodgkin s Lymphoma (HL): Preliminary Results of the EORTC-GELA H9-F Trial H. Eghbali, P.
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Schaapveld M, Aleman BMP, van Eggermond AM, et al. Second cancer
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Schaapveld M, Aleman BMP, van Eggermond AM, et al. Second cancer
Nodular lymphocyte-predominant Hodgkin lymphoma: a unique disease deserving unique management
 HODGKIN LYMPHOMA: NEW INSIGHTS AND NEW APPROACHES Nodular lymphocyte-predominant Hodgkin lymphoma: a unique disease deserving unique management Dennis A. Eichenauer 1,2 and Andreas Engert 1,2 1 First Department
HODGKIN LYMPHOMA: NEW INSIGHTS AND NEW APPROACHES Nodular lymphocyte-predominant Hodgkin lymphoma: a unique disease deserving unique management Dennis A. Eichenauer 1,2 and Andreas Engert 1,2 1 First Department
Hodgkin's Lymphoma. Symptoms. Types
 Hodgkin's lymphoma (Hodgkin's disease) usually develops in the lymphatic system, a part of the body's immune system. This system carries disease-fighting white blood cells throughout the body. Lymph tissue
Hodgkin's lymphoma (Hodgkin's disease) usually develops in the lymphatic system, a part of the body's immune system. This system carries disease-fighting white blood cells throughout the body. Lymph tissue
NIH Public Access Author Manuscript Expert Opin Pharmacother. Author manuscript; available in PMC 2011 December 1.
 NIH Public Access Author Manuscript Published in final edited form as: Expert Opin Pharmacother. 2010 December ; 11(17): 2891 2906. doi:10.1517/14656566.2010.515979. Hodgkin s Lymphoma Therapy: Past, Present,
NIH Public Access Author Manuscript Published in final edited form as: Expert Opin Pharmacother. 2010 December ; 11(17): 2891 2906. doi:10.1517/14656566.2010.515979. Hodgkin s Lymphoma Therapy: Past, Present,
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin
 What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin Alison Moskowitz, MD Assistant Attending, Lymphoma Service Memorial Sloan Kettering
What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin Alison Moskowitz, MD Assistant Attending, Lymphoma Service Memorial Sloan Kettering
Brentuximab Vedotin. Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center
 Brentuximab Vedotin Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center U.S. Cancer Statistics 2016 300.000 249.260 224.390 200.000 180.890 Incidence 100.000 95.270 76.960
Brentuximab Vedotin Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center U.S. Cancer Statistics 2016 300.000 249.260 224.390 200.000 180.890 Incidence 100.000 95.270 76.960
ROB LOWN SOUTHAMPTON HODGKIN LYMPHOMA IN THE ELDERLY
 ROB LOWN SOUTHAMPTON HODGKIN LYMPHOMA IN THE ELDERLY EPIDEMIOLOGY HODGKIN LYMPHOMA - INCIDENCE EPIDEMIOLOGY HODGKIN LYMPHOMA - MORTALITY EPIDEMIOLOGY HODGKIN LYMPHOMA - MORTALITY BY AGE NUMBER OF PEOPLE
ROB LOWN SOUTHAMPTON HODGKIN LYMPHOMA IN THE ELDERLY EPIDEMIOLOGY HODGKIN LYMPHOMA - INCIDENCE EPIDEMIOLOGY HODGKIN LYMPHOMA - MORTALITY EPIDEMIOLOGY HODGKIN LYMPHOMA - MORTALITY BY AGE NUMBER OF PEOPLE
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
PET-imaging: when can it be used to direct lymphoma treatment?
 PET-imaging: when can it be used to direct lymphoma treatment? Luca Ceriani Nuclear Medicine and PET-CT centre Oncology Institute of Southern Switzerland Bellinzona Disclosure slide I declare no conflict
PET-imaging: when can it be used to direct lymphoma treatment? Luca Ceriani Nuclear Medicine and PET-CT centre Oncology Institute of Southern Switzerland Bellinzona Disclosure slide I declare no conflict
Clinical Characteristics and Treatment Response of Hodgkin s Lymphoma in Taiwan
 ORIGINAL ARTICLE Clinical Characteristics and Treatment Response of Hodgkin s Lymphoma in Taiwan Shang-Ju Wu, 1 Chien-Yuan Chen, 1 Ih-Jen Su, 2 Jih-Luh Tang, 1 Wen-Chen Chou, 1,3 Bo-Sheng Ko, 1 Sheng-Yi
ORIGINAL ARTICLE Clinical Characteristics and Treatment Response of Hodgkin s Lymphoma in Taiwan Shang-Ju Wu, 1 Chien-Yuan Chen, 1 Ih-Jen Su, 2 Jih-Luh Tang, 1 Wen-Chen Chou, 1,3 Bo-Sheng Ko, 1 Sheng-Yi
Lymphology 28 (1995) 73-77
 73-77") 73 Lymphology 28 (1995) 73-77 Lymphological Laboratory (PH), Department of Gynecology, University of Tiibingen, Germany and Fifth Department of Internal Medicine (EZ), Silesian Medical Academy, Poland
73 Lymphology 28 (1995) 73-77 Lymphological Laboratory (PH), Department of Gynecology, University of Tiibingen, Germany and Fifth Department of Internal Medicine (EZ), Silesian Medical Academy, Poland
THE EORTC-GELA TREATMENT STRATEGY IN CLINICAL STAGES I-II HL Results of the H9-F and H9-U trials (#20982)
") EORTC Lymphoma Group THE EORTC-GELA TREATMENT STRATEGY IN CLINICAL STAGES I-II HL Results of the H9-F and H9-U trials (#20982) J. Thomas, C. Fermé, E.M. Noordijk, H. Eghbali and M. Henry-Amar 7th International
EORTC Lymphoma Group THE EORTC-GELA TREATMENT STRATEGY IN CLINICAL STAGES I-II HL Results of the H9-F and H9-U trials (#20982) J. Thomas, C. Fermé, E.M. Noordijk, H. Eghbali and M. Henry-Amar 7th International
RECENT APPROACHES IN THE TREATMENT OF HODGKIN S LYMPHOMA. Luděk Raida
 Volume 142, 1999 13 RECENT APPROACHES IN THE TREATMENT OF HODGKIN S LYMPHOMA Luděk Raida Haemato-oncology Department of University Hospital, I. P. Pavlova 6, 775 20 Olomouc, Czech Republic Received August
Volume 142, 1999 13 RECENT APPROACHES IN THE TREATMENT OF HODGKIN S LYMPHOMA Luděk Raida Haemato-oncology Department of University Hospital, I. P. Pavlova 6, 775 20 Olomouc, Czech Republic Received August
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page
 Vol.69(1), Page") The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1668-1673 Role of Surveillance CT in Detection of Pre-Clinical Relapse in Patients with B- Cell lymphoma: A Retrospective Study
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1668-1673 Role of Surveillance CT in Detection of Pre-Clinical Relapse in Patients with B- Cell lymphoma: A Retrospective Study
Treatment outcomes of IMEP as a front-line chemotherapy for patients with peripheral T-cell lymphomas
 BLOOD RESEARCH VOLUME 51 ㆍ NUMBER 3 September 2016 ORIGINAL ARTICLE Treatment outcomes of IMEP as a front-line chemotherapy for patients with peripheral T-cell lymphomas Ji Young Lee 1, Sang Min Lee 1,
BLOOD RESEARCH VOLUME 51 ㆍ NUMBER 3 September 2016 ORIGINAL ARTICLE Treatment outcomes of IMEP as a front-line chemotherapy for patients with peripheral T-cell lymphomas Ji Young Lee 1, Sang Min Lee 1,
Dr. Andrea Gallamini - Hematology Department Azienda Ospedaliera S. Croce e Carle Cuneo Italy
 High-dose sequential chemotherapy (HDS) followed by autologous stem cell transplantation (ASCT) in relapsed/refractory Hodgkin s lymphoma. Long term results. Dr. Andrea Gallamini - Hematology Department
High-dose sequential chemotherapy (HDS) followed by autologous stem cell transplantation (ASCT) in relapsed/refractory Hodgkin s lymphoma. Long term results. Dr. Andrea Gallamini - Hematology Department
Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL
 Lymphoma & Myeloma 2015 Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL Jeremy S. Abramson, MD Relevant Disclosure Consulting for Seattle
Lymphoma & Myeloma 2015 Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL Jeremy S. Abramson, MD Relevant Disclosure Consulting for Seattle
Role of modern radiation therapy in early stage Hodgkin s lymphoma: A young radiation oncologists perspective
 reports of practical oncology and radiotherapy 1 7 ( 2 0 1 2 ) 246 250 Available online at www.sciencedirect.com jo u r n al hom epage: http://www.elsevier.com/locate/rpor Review Role of modern radiation
reports of practical oncology and radiotherapy 1 7 ( 2 0 1 2 ) 246 250 Available online at www.sciencedirect.com jo u r n al hom epage: http://www.elsevier.com/locate/rpor Review Role of modern radiation
Response-adapted frontline therapy for Hodgkin lymphoma: are we there yet?
 HODGKIN LYMPHOMA: TREATMENT TODAY AND THE CHALLENGE FOR TOMORROW Response-adapted frontline therapy for Hodgkin lymphoma: are we there yet? Peter W. M. Johnson Cancer Research UK Centre, University of
HODGKIN LYMPHOMA: TREATMENT TODAY AND THE CHALLENGE FOR TOMORROW Response-adapted frontline therapy for Hodgkin lymphoma: are we there yet? Peter W. M. Johnson Cancer Research UK Centre, University of
Radiation and Hodgkin s Disease: A Changing Field. Sravana Chennupati Radiation Oncology PGY-2
 Radiation and Hodgkin s Disease: A Changing Field Sravana Chennupati Radiation Oncology PGY-2 History of Present Illness 19 yo previously healthy male college student began having pain in his R shoulder
Radiation and Hodgkin s Disease: A Changing Field Sravana Chennupati Radiation Oncology PGY-2 History of Present Illness 19 yo previously healthy male college student began having pain in his R shoulder
Radiotherapy in aggressive lymphomas. Umberto Ricardi
 Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
AHSCT in Hodgkin lymphoma - indication and challenges. Bastian von Tresckow German Hodgkin Study Group Cologne University Hospital
 AHSCT in Hodgkin lymphoma - indication and challenges Bastian von Tresckow German Hodgkin Study Group Cologne University Hospital AHSCT in Hodgkin Lymphoma The role of AHSCT in HL Mobilisation failure
AHSCT in Hodgkin lymphoma - indication and challenges Bastian von Tresckow German Hodgkin Study Group Cologne University Hospital AHSCT in Hodgkin Lymphoma The role of AHSCT in HL Mobilisation failure
Predictive value of Follicular Lymphoma International Prognostic Index (FLIPI) in patients with follicular lymphoma at first progression
 in patients with follicular lymphoma at first progression") Original article Annals of Oncology 15: 1484 1489, 2004 doi:10.1093/annonc/mdh406 Predictive value of Follicular Lymphoma International Prognostic Index (FLIPI) in patients with follicular lymphoma at
Original article Annals of Oncology 15: 1484 1489, 2004 doi:10.1093/annonc/mdh406 Predictive value of Follicular Lymphoma International Prognostic Index (FLIPI) in patients with follicular lymphoma at
Gruppo Italiano Terapie Innovative nei Linfomi (G.I.T.I.L.) Dr. Andrea Gallamini S.C. Ematologia Az. Ospedaliera S. Croce e Carle, Cuneo
 Dr. Andrea Gallamini S.C. Ematologia Az. Ospedaliera S. Croce e Carle, Cuneo") Sponsor Principal Investigator Protocol Coordinators Coordinating Centre Writing committee CRO Gruppo Italiano Terapie Innovative nei Linfomi (G.I.T.I.L.) Dr. Andrea Gallamini S.C. Ematologia Az. Ospedaliera
Sponsor Principal Investigator Protocol Coordinators Coordinating Centre Writing committee CRO Gruppo Italiano Terapie Innovative nei Linfomi (G.I.T.I.L.) Dr. Andrea Gallamini S.C. Ematologia Az. Ospedaliera
Modified Number of Extranodal Involved Sites as a Prognosticator in R-CHOP-Treated Patients with Disseminated Diffuse Large B-Cell Lymphoma
 ORIGINAL ARTICLE DOI: 10.3904/kjim.2010.25.3.301 Modified Number of Extranodal Involved Sites as a Prognosticator in R-CHOP-Treated Patients with Disseminated Diffuse Large B-Cell Lymphoma Changhoon Yoo
ORIGINAL ARTICLE DOI: 10.3904/kjim.2010.25.3.301 Modified Number of Extranodal Involved Sites as a Prognosticator in R-CHOP-Treated Patients with Disseminated Diffuse Large B-Cell Lymphoma Changhoon Yoo
Hodgkin s Lymphoma: Biology and Treatment Strategies for Primary, Refractory, and Relapsed Disease
 Hodgkin s Lymphoma: Biology and Treatment Strategies for Primary, Refractory, and Relapsed Disease Volker Diehl, Harald Stein, Michael Hummel, Raphael Zollinger, and Joseph M. Connors Hodgkin s lymphomas
Hodgkin s Lymphoma: Biology and Treatment Strategies for Primary, Refractory, and Relapsed Disease Volker Diehl, Harald Stein, Michael Hummel, Raphael Zollinger, and Joseph M. Connors Hodgkin s lymphomas
Role of PET in staging and treatment of lymphomas
 Role of PET in staging and treatment of lymphomas ESMO preceptorship in lymphoma Madrid, 25 November 2016 Martin Hutchings Rigshospitalet, Copenhagen, Denmark EORTC Lymphoma Group PET in lymphoma staging
Role of PET in staging and treatment of lymphomas ESMO preceptorship in lymphoma Madrid, 25 November 2016 Martin Hutchings Rigshospitalet, Copenhagen, Denmark EORTC Lymphoma Group PET in lymphoma staging
Ferrata Storti Foundation
 ARTICLES Introduction Hodgkin s Lymphoma Brentuximab vedotin in relapsed/refractory Hodgkin s lymphoma: the Italian experience and results of its use in daily clinical practice outside clinical trials
ARTICLES Introduction Hodgkin s Lymphoma Brentuximab vedotin in relapsed/refractory Hodgkin s lymphoma: the Italian experience and results of its use in daily clinical practice outside clinical trials
12 th Annual Hematology & Breast Cancer Update Update in Lymphoma
 12 th Annual Hematology & Breast Cancer Update Update in Lymphoma Craig Okada, MD, PhD Assistant Professor, Hematology January 14, 2010 Governors Hotel, Portland Oregon Initial Treatment of Indolent Lymphoma
12 th Annual Hematology & Breast Cancer Update Update in Lymphoma Craig Okada, MD, PhD Assistant Professor, Hematology January 14, 2010 Governors Hotel, Portland Oregon Initial Treatment of Indolent Lymphoma
First line Treatment of HL: Differential Treatment Strategies in Newly Diagnosed Patients with Early versus Advanced Stage Disease Presented
 [Editor s note: Dr. Even's video transcript has been edited to improve readability] you today about the management of Hodgkin lymphoma in 2016. Welcome to Managing Hodgkin Lymphoma. My name is Andy Evens,
[Editor s note: Dr. Even's video transcript has been edited to improve readability] you today about the management of Hodgkin lymphoma in 2016. Welcome to Managing Hodgkin Lymphoma. My name is Andy Evens,
Head and Neck: DLBCL
 Head and Neck: DLBCL Nikhil G. Thaker Chelsea C. Pinnix Valerie K. Reed Bouthaina S. Dabaja Department of Radiation Oncology MD Anderson Cancer Center Case 60 yo male Presented with right cervical LAD
Head and Neck: DLBCL Nikhil G. Thaker Chelsea C. Pinnix Valerie K. Reed Bouthaina S. Dabaja Department of Radiation Oncology MD Anderson Cancer Center Case 60 yo male Presented with right cervical LAD
IAEA Pediatric Radiation Oncology Training Dr Laskar Version 1 June 2009 RADIATION THERAPY FOR PEDIATRIC HODGKIN S DISEASE
 RADIATION THERAPY FOR PEDIATRIC HODGKIN S DISEASE THOMAS HODGKIN 1832 On Some Morbid Appearances of the Absorbent Glands & Spleen GLOBAL INCIDENCE Region Cases per 100,000 children United States 0.5 European
RADIATION THERAPY FOR PEDIATRIC HODGKIN S DISEASE THOMAS HODGKIN 1832 On Some Morbid Appearances of the Absorbent Glands & Spleen GLOBAL INCIDENCE Region Cases per 100,000 children United States 0.5 European
Radiotherapy in DLCL is often worthwhile. Dr. Joachim Yahalom Memorial Sloan-Kettering, New York
 Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
Welcome & Introductions
 Living with Hodgkin Lymphoma Welcome & Introductions Dr. Lamar s slides are available for download at www.lls.org/programs, under the program listing. 1 Living with Hodgkin Lymphoma Living with Hodgkin
Living with Hodgkin Lymphoma Welcome & Introductions Dr. Lamar s slides are available for download at www.lls.org/programs, under the program listing. 1 Living with Hodgkin Lymphoma Living with Hodgkin
CARE at ASH 2014 Lymphoma. Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre
 CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
Hodgkin Lymphoma: Advancing Beyond Standard Management
 J a n u a r y 2 0 0 9 w w w. c l i n i c a l a d v a n c e s. c o m V o l u m e 7, I s s u e 1, S u p p l e m e n t 3 G u e s t E d i t o r Bruce D. Cheson, MD, FACP Head of Hematology Lombardi Comprehensive
J a n u a r y 2 0 0 9 w w w. c l i n i c a l a d v a n c e s. c o m V o l u m e 7, I s s u e 1, S u p p l e m e n t 3 G u e s t E d i t o r Bruce D. Cheson, MD, FACP Head of Hematology Lombardi Comprehensive
Addition of rituximab is not associated with survival benefit compared with CHOP alone for patients with stage I diffuse large B-cell lymphoma
 Original Article Addition of rituximab is not associated with survival benefit compared with CHOP alone for patients with stage I diffuse large B-cell lymphoma Bo Jia 1, Yuankai Shi 1, Suyi Kang 1, Sheng
Original Article Addition of rituximab is not associated with survival benefit compared with CHOP alone for patients with stage I diffuse large B-cell lymphoma Bo Jia 1, Yuankai Shi 1, Suyi Kang 1, Sheng
At initial diagnosis, patients with
 Malignant Lymphomas Decision Making and Problem Solving Current treatment and immunotherapy of Hodgkin s lymphoma Beate Klimm Roland Schnell Volker Diehl Andreas Engert The treatment of Hodgkin s lymphoma
Malignant Lymphomas Decision Making and Problem Solving Current treatment and immunotherapy of Hodgkin s lymphoma Beate Klimm Roland Schnell Volker Diehl Andreas Engert The treatment of Hodgkin s lymphoma
One, the UK RAPID trial, including patients with early stage disease stage 1 and 2A nonbulky.
 Martin Hutchings, MD, PhD Department of Hematology The Finsen Centre, National Hospital Copenhagen University Hospital Copenhagen, Denmark Welcome to Managing Hodgkin Lymphoma. My name is Martin Hutchings.
Martin Hutchings, MD, PhD Department of Hematology The Finsen Centre, National Hospital Copenhagen University Hospital Copenhagen, Denmark Welcome to Managing Hodgkin Lymphoma. My name is Martin Hutchings.
ORIGINAL ARTICLE CHARACTERISTICS AND OUTCOMES OF ANAPLASTIC LARGE CELL LYMPHOMA PATIENTS-A SINGLE CENTRE EXPERIENCE
 ORIGINAL ARTICLE CHARACTERISTICS AND OUTCOMES OF ANAPLASTIC LARGE CELL LYMPHOMA PATIENTS-A SINGLE CENTRE EXPERIENCE Sohail Athar, Neelam Siddiqui, Abdul Hameed Department of Medical Oncology, Shaukat Khanum
ORIGINAL ARTICLE CHARACTERISTICS AND OUTCOMES OF ANAPLASTIC LARGE CELL LYMPHOMA PATIENTS-A SINGLE CENTRE EXPERIENCE Sohail Athar, Neelam Siddiqui, Abdul Hameed Department of Medical Oncology, Shaukat Khanum
Lugano classification: Role of PET-CT in lymphoma follow-up
 CAR Educational Exhibit: ID 084 Lugano classification: Role of PET-CT in lymphoma follow-up Charles Nhan 4 Kevin Lian MD Charlotte J. Yong-Hing MD FRCPC Pete Tonseth 3 MD FRCPC Department of Diagnostic
CAR Educational Exhibit: ID 084 Lugano classification: Role of PET-CT in lymphoma follow-up Charles Nhan 4 Kevin Lian MD Charlotte J. Yong-Hing MD FRCPC Pete Tonseth 3 MD FRCPC Department of Diagnostic
Principles of Chemotherapy in Hodgkin Lymphoma
 Principles of Chemotherapy in Hodgkin Lymphoma 9 Patrice Carde and Peter Johnson Contents 9.1 Historical Introduction... 141 9.2 Chemotherapy Applied to Advanced Stage HL: Theories and Practice... 142
Principles of Chemotherapy in Hodgkin Lymphoma 9 Patrice Carde and Peter Johnson Contents 9.1 Historical Introduction... 141 9.2 Chemotherapy Applied to Advanced Stage HL: Theories and Practice... 142
Rituximab in the Treatment of NHL:
 New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
Outcomes of patients with peripheral T-cell lymphoma in first complete remission: data from three tertiary Asian cancer centers
 Tang et al. (2017) 7:653 DOI 10.1038/s41408-017-0030-y CORRESPONDENCE Outcomes of patients with peripheral T-cell lymphoma in first complete remission: data from three tertiary Asian cancer centers Open
Tang et al. (2017) 7:653 DOI 10.1038/s41408-017-0030-y CORRESPONDENCE Outcomes of patients with peripheral T-cell lymphoma in first complete remission: data from three tertiary Asian cancer centers Open
RADIOLOGY: the chest x-ray
 RADIOLOGY: the chest x-ray A B A case of lymphoma that was treated in September 1901 by W. A. Pusey, Professor of Dermatology in the Medical Department of the University of Illinois. A: The patient on
RADIOLOGY: the chest x-ray A B A case of lymphoma that was treated in September 1901 by W. A. Pusey, Professor of Dermatology in the Medical Department of the University of Illinois. A: The patient on
RT in Hodgkin Lymphoma
 RT in Hodgkin Lymphoma Lesser is better? Philip Poortmans, M.D. Ph.D. Radiation oncologist Tilburg, The Netherlands Radiation dose in Hodgkin Lymphoma Introduction Current evidence Guidelines 1.0 Early
RT in Hodgkin Lymphoma Lesser is better? Philip Poortmans, M.D. Ph.D. Radiation oncologist Tilburg, The Netherlands Radiation dose in Hodgkin Lymphoma Introduction Current evidence Guidelines 1.0 Early
Radiotherapy Alone Versus Combined-Modality Therapy for Initial Treatment of Early Stage Hodgkin's Lymphoma
 Radiotherapy Alone Versus Combined-Modality Therapy for Initial Treatment of Early Stage Hodgkin's Lymphoma Hanan Shawky Gamal El-Deen * and Amr Abd- El Aziz Ghannam Clinical Oncology Department, Tanta
Radiotherapy Alone Versus Combined-Modality Therapy for Initial Treatment of Early Stage Hodgkin's Lymphoma Hanan Shawky Gamal El-Deen * and Amr Abd- El Aziz Ghannam Clinical Oncology Department, Tanta
Advances in CD30- and PD-1-targeted therapies for classical Hodgkin lymphoma
 Wang et al. Journal of Hematology & Oncology (2018) 11:57 https://doi.org/10.1186/s13045-018-0601-9 REVIEW Advances in CD30- and PD-1-targeted therapies for classical Hodgkin lymphoma Yucai Wang 1, Grzegorz
Wang et al. Journal of Hematology & Oncology (2018) 11:57 https://doi.org/10.1186/s13045-018-0601-9 REVIEW Advances in CD30- and PD-1-targeted therapies for classical Hodgkin lymphoma Yucai Wang 1, Grzegorz
Treating Hodgkin Lymphoma
 Treating Hodgkin Lymphoma General treatment information If you (or your child) has been diagnosed with Hodgkin lymphoma, the cancer care team will discuss treatment options with you. It s important to
Treating Hodgkin Lymphoma General treatment information If you (or your child) has been diagnosed with Hodgkin lymphoma, the cancer care team will discuss treatment options with you. It s important to
Supplementary Appendix to manuscript submitted by Trappe, R.U. et al:
 Supplementary Appendix to manuscript submitted by Trappe, R.U. et al: Response to rituximab induction is a predictive marker in B-cell post-transplant lymphoproliferative disorder and allows successful
Supplementary Appendix to manuscript submitted by Trappe, R.U. et al: Response to rituximab induction is a predictive marker in B-cell post-transplant lymphoproliferative disorder and allows successful
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA
 RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin