Colorectal Cancer: Novel Insights
|
|
|
- Cornelius Lester
- 5 years ago
- Views:
Transcription
1 Colorectal Cancer: Novel Insights Richard Kim M.D. Associate Professor Service Chief of Medical Oncology Department of Gastrointestinal Oncology Moffitt Cancer Center Tampa, FL
2 Richard Kim, MD Colorectal Cancer: Novel Insights Relevant financial relationships in the past twelve months by presenter or spouse/partner. Grant/Research Support: Bayer, BMS, Taiho Consultant: BMS, Lilly, Bayer Speakers Bureau: Lilly The speaker will directly disclosure the use of products for which are not labeled (e.g., off label use) or if the product is still investigational. 15 th Annual Miami Cancer Meeting
3 Learning Objectives Know the current trend for treatment of advanced colorectal cancer Know the current status of personalized medicine in advanced CRC Know the differences between left vs right sided colon cancer
4 CRC US statistics: Impact of CRC 3 rd highest incidence rate (~135,000/yr) 2 nd highest mortality rate (~49,000/yr) CRC Global statistics: 3 rd highest incidence rate ( ~ 1.2million/yr) 4 th highest mortality rate (~608,000/yr) The burden of disease is clearly evident





5 A High Number of Agents Is Currently Available for the Treatment of mcrc 5-FU Capecitabine Irinotecan Oxaliplatin Bevacizumab Cetuximab Regorafenib Aflibercept Panitumumab TAS-102 Ramucirumab BSC
6 Landscape in mcrc Bevacizumab and EGFR mabs competing for firstline patients in KRAS wt CRC Bevacizumab, ramucirumab and Aflibercept competing for second-line patients with each other, and with EGFR mabs in KRAS wt CRC Best sequence of therapies (VEGFi vs EGFRi) still to be established Regorafenib and TAS 102 as salvage therapy option Immunotherapy for pts with MMR deficient/msi-h tumor
7 Tools for Treatment Selection Age PS Comorbidities Tumor burden Potential for cure? Symptoms? Tumor location Clinical Markers Molecular Markers Histologic grade CEA KRAS NRAS BRAF MSI/MMR Patient characteristics + Tumor characteristics
8 Questions How can biologics be used to their full potential? Prognostic markers -Biomarker that correlates with clinical outcome regardless of therapy Predictive markers-biomarker that is associated with the likelihood of response to therapy Can a patient population be identified which would benefit most from one specific treatment strategy?





9 Overview of EGFR and VEGFR Growth Signaling Pathways Tumor Cell Endothelial Cell VEGF EGFR KIT PDGFR-β VEGFR Targeted by cetuximab and panitumumab RAS Pl3K Targeted by bevacizumab ramucirumab and aflibercept* *Aflibercept also targets PIGF RAF BRAF MEK AKT ERK mtor ONCOGENESIS ANGIOGENESIS TUMOR MICROENVIRONMENT G.SM.ON Krasinskas AM. Patholog Res Int. 2011;2011:932932; Sitohy B, et al. Cancer Res 2012;72: ; Bendardaf R, et al. Anticancer Res. 2008;28: ; Kitadai Y, et al. Am J Pathol. 2006;169: ; Jayson GC, et al. J Clin Oncol. 2005;23:

10 Biomarkers for anti- VEGF Drugs
11 Spectrum of ras mutations KRAS EXON 2 EXON 3 EXON % % 5.6% 146 NRAS EXON 2 EXON 3 EXON % % 0.9% 146

12 Updated Analysis of PRIME study KRAS exon 2 codon 12/13 KRAS exon 3 codon 61 KRAS exon 4 codon 117/146 NRAS exon 2 codon 12/13 NRAS exon 3 codon 61 BRAF exon 15 codon % 4% 6% 3% 4% 8% 17% Oliner et al., ASCO 2013
13 PRIME Biomarker Analysis: OS in Patients With WT KRAS Exon 2 and WT RAS mcrc Proportion Alive, % Proportion Alive, % WT KRAS Exon 2 WT KRAS Exon 2 FOLFOX4 alone (n=331) 100 Panitumumab FOLFOX4 alone + FOLFOX4 (n=331) (n=325) 100 Panitumumab + FOLFOX4 (n=325) HR=0.83 (95% CI, ) 80 HR=0.83 P=0.072 (95% CI, ) P= mos 19.7 mos mos mos Time, Months Time, Months FOLFOX4 alone (n=259) 100 Panitumumab FOLFOX4 alone + FOLFOX4 (n=259) (n=253) Panitumumab + FOLFOX4 (n=253) HR=0.78 (95% CI, ) 80 HR=0.78 P=0.043 (95% CI, ) 70 P= mos 20.2 mos mos mos Time, Months Time, Months Proportion Alive, % Proportion Alive, % WT KRAS/NRAS WT KRAS/NRAS Oliner J, et al. ASCO (abstr 3511). Oliner J, et al. ASCO (abstr 3511)
14 PRIME Biomarker Analysis: OS in Patients With MT RAS or WT KRAS Exon 2/MT Other RAS FOLFOX4 alone (n=276) 100 Panitumumab FOLFOX4 alone + FOLFOX4 (n=276) (n=272) Panitumumab + FOLFOX4 (n=272) HR=1.25 (95% CI, ) HR=1.25 P=0.034 (95% CI, ) 70 P= mos 15.6 mos mos mos Time, Months Time, Months Proportion Alive, % Proportion Alive, % MT RAS MT RAS FOLFOX4 alone (n=57) 100 Panitumumab FOLFOX4 alone + FOLFOX4 (n=57) (n=51) HR=1.29 (95% CI, ) 80 HR= P=0.305 (95% CI, ) 70 P= mos 17.1 mos mos mos Time, Months Time, Months Proportion Alive, % Proportion Alive, % WT KRAS Exon 2/MT Other RAS WT KRAS Exon 2/MT Other RAS Oliner J, et al. ASCO (abstr 3511). Oliner J, et al. ASCO (abstr 3511)
15 Take home point testing for these additional codons could help screen 20% more patients with mcrc for treatment with EGFR inhibitors This method could help to more accurately select patients who will benefit from EGFR inhibitors. NCCN now recommends testing for all RAS mutations
16 BRAF Mutations in CRC BRAF is primary effector of KRAS signaling BRAF mutations: Tumor Cell EGF Occur most frequently in exon 15 (V600E) Found in 4%-14% of patients with CRC P P P P Ras Raf Mutually exclusive with KRAS mutations MEK Tumor cell proliferation and survival Erk Yarden. Nat Rev Mol Cell Biol. 2001;2:127; Di Nicolantonio. J Clin Oncol. 2008;26:5705; Artale. J Clin Oncol. 2008;26:4217.
:466-474. Tol J, et al. N Engl J Med.")
17 The Prognosis of Patients With BRAF V600E Mutations is Poor Roth AD, et al. J Clin Oncol. 2010;28(3): Tol J, et al. N Engl J Med. 2009;361(1):98-99.
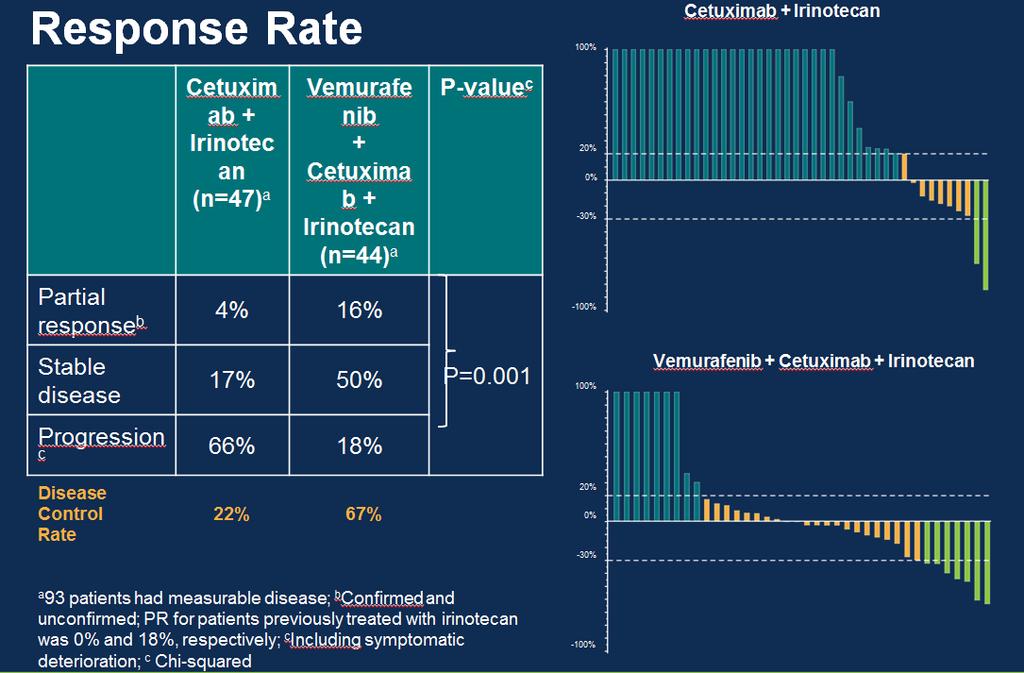
18 Randomized trial of irinotecan and cetuximab with or without vemurafenib in BRAF-mutant metastatic colorectal cancer (SWOG S1406) Scott Kopetz, 1 Shannon McDonough, 2 Heinz-Josef Lenz, 3 Anthony Magliocco, 4 Chloe Atreya, 5 Luis A. Diaz Jr., 6 Carmen Allegra, 7 Kanwal Raghav, 1 Van Morris, 1 Stephen Wang, 8 Christopher Lieu, 9 Katherine A. Guthrie, 2 Howard S. Hochster 10 1 The University of Texas MD Anderson Cancer Center, Houston, TX; 2 Fred Hutchinson Cancer Research Center, Seattle, WA; 3 USC Norris Comprehensive Cancer Center, Los Angeles, CA; 4 H. Lee Moffitt Cancer Center & Research Institute, Tampa, FL; 5 University of California, San Francisco, San Francisco, CA; 6 Memorial Sloan Kettering Cancer Center, NewYork, NY; 7 University of Florida, Gainesville, FL; 8 Kaiser Permanente, Sacramento, CA; 9 University of Colorado School of Medicine, Anschutz Medical Campus, Aurora, CO; 10 Yale Cancer Center, New Haven, CT
19 Study Design R E G I S T R A T I O N Local BRAF testing No local BRAF testing BRAF V600E Mutation Central Testing Performed R A N D O M I Z A T I O N ARM 1: Cetuximab + Irinotecan ARM 2: Vemurafenib + Cetuximab + Irinotecan Progression Progression Off Study STEP 3: Cross-over to add Vemurafenib Off Study Wild-type (off study) Vemurafenib 960mg PO bid continuous Cetuximab 500mg/m2 IV q2weeks Irinotecan 180mg/m2 IV q2weeks Presented by: Scott Kopetz, MD, PhD

20 Primary Endpoint: Progression-free survival Presented by:
21
22
23
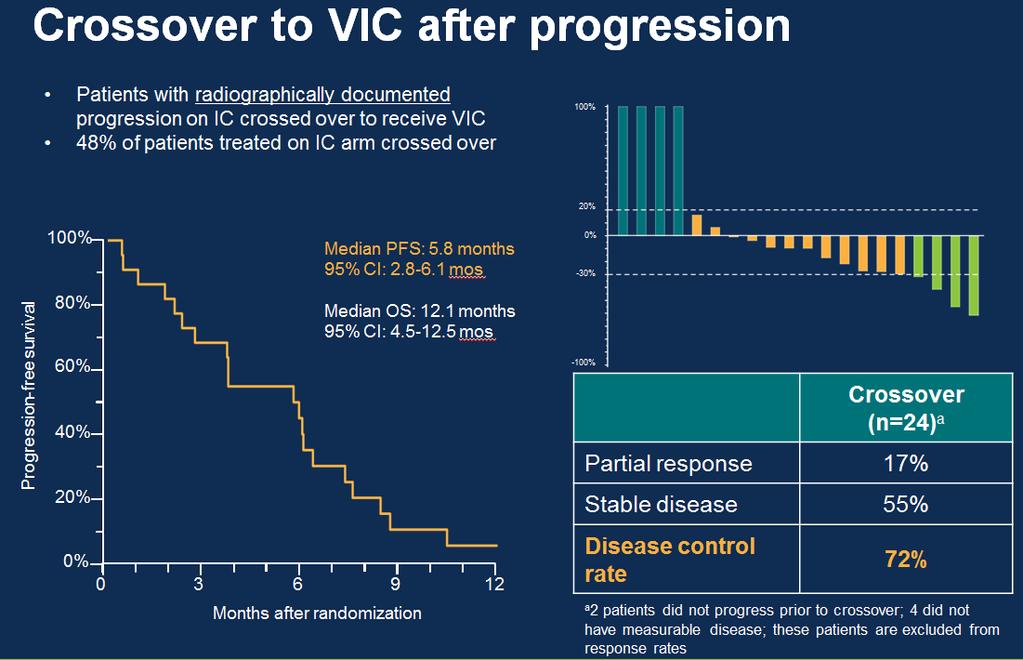
24 Conclusions The combination of vemurafenib, cetuximab, and irinotecan (VIC) met its primary endpoint demonstrating improved progression-free survival in patients with BRAF V600E CRC Addition of Vemurafenib to IC showed activity even after progression on IC VIC represents a new treatment for metastatic BRAF V600E colorectal cancer

25 What is the impact of site of primary tumour?


26 Primary Tumor Location and Potential Treatments Anti-PD1 Right-sided MSI-H Left-sided Bev + Triplet CT BRAF MT HER2+ HER2-targeted agents KRAS MT KRAS WT AREG/EREG Bufill JA. Ann Intern Med. 1990;113: ; Missiaglia E, et al. ASCO Abstract 3526; Brule SY, et al. ASCO Abstract 3528; The Cancer Genome Atlas Network. Nature :61-70; Bendardaf R, et al. Anticancer Res. 2008;28:



27 CALGB/SWOG 80405: KRAS wt 1 ST LINE MET / ADVANCED COLORECTAL KRAS wt Codons 12 & 13 N = 1137 FOLFIRI or FOLFOX MD choice Chemo + Cetuximab Chemo OS = Cetuximab mos PFS = 10.4 mos : NO DIFFERENCE Chemo + Bevacizumab Chemo OS + = Bevacizumab 29.0 mos PFS = 10.8 mos PRESENTED AT THE 2014 ASCO ANNUAL MEETING DATA IS THE PROPERTY OF THE AUTHOR
28


29 Meta-analysis: Sidedness in MCRC Holch et al, Eur J Cancer, 2017 Favors LEFT Presented by:



30 Predictive impact bev versus anti-egfrs Chemo+anti-EGFR vs Chemo+Bev FIRE 3 CALGB PEAK RAS wt FOLFIR I+ BEV FOLFI R I+ CET RAS wt CHEMO + BEV CHEMO + CET RAS wt FOLFO X+ BEV FOLFO X+ PAN
31 FIRE-3 Tejpar et al., JAMA Oncol 2016
 21.0 (6.0 29.0) 0.45 (0.08 2.49) 1: Pmab + FOLFOX left 2: Beva + FOLFOX left 3: Pmab + FOLFOXright 4: Beva + FOLFOX right 0 0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 No.")
32 Right versus Left: PEAK OS Kaplan-Meier estimate Median OS (95% CI), months Pmab + FOLFOX Beva + FOLFOX HR (95% CI) Left 43.4 ( ) 32.0 ( ) 0.84 ( ) Right 17.5 ( ) 21.0 ( ) 0.45 ( ) 1: Pmab + FOLFOX left 2: Beva + FOLFOX left 3: Pmab + FOLFOXright 4: Beva + FOLFOX right No. of subjects: Overall survival (months) 1: : : : Censor indicated by vertical bar Boeckx ESMO 2016; Peeters et al. Ann Oncol Apr 25. Epub ahead of print. Beva, bevacizumab; HR, hazard ratio; OS, overall survival; Pmab, panitumumab



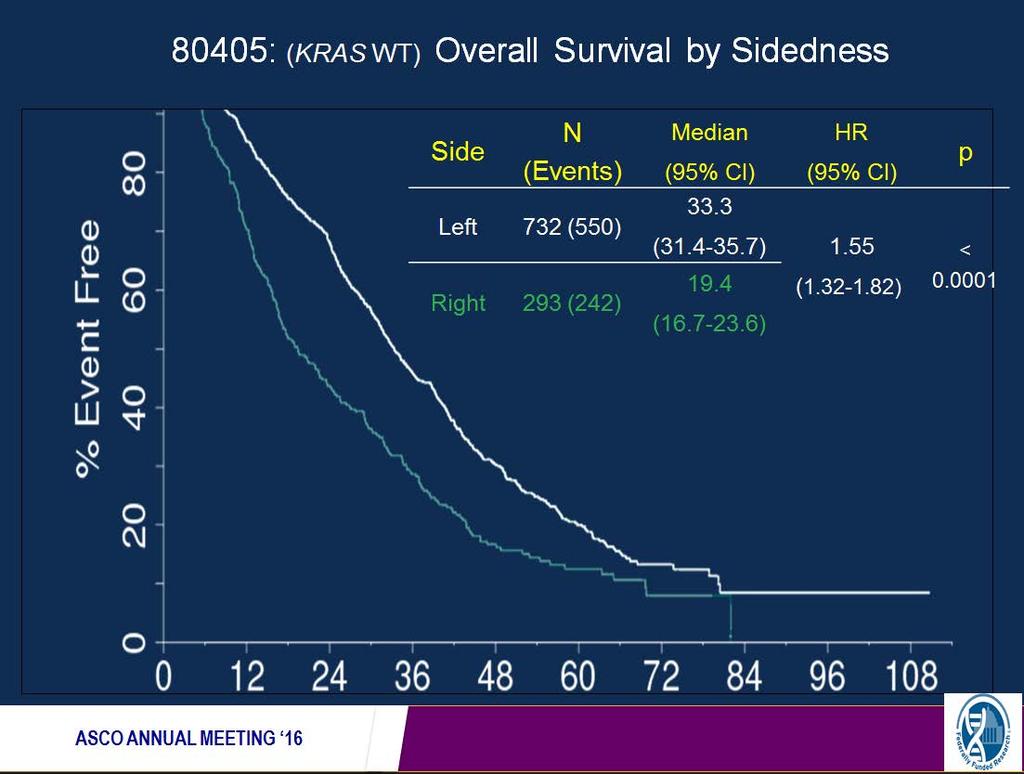
33 Right versus Left: CALGB80405 study - OS 31% p for interaction0.009 Lenz et al. ESMO Congress 2016.
34 Minimal difference between bev and cetux in left sided tumors Venook A, ASCO 2017; abstract 3503
35 Take Home Points Left sided primary colorectal cancers have better prognosis than right sided colon cancers Right sided colorectal cancers do not benefit from anti-egfr therapy but do benefit from bevacizumab Left sided tumors benefit from both bevacizumab and anti- EGFR therapy
36 MSI-high CRC and Immune Checkpoint Blockade
37 Background In non selected colorectal cancer patients PD- 1 blockade seems to be ineffective. Average tumor has dozens of somatic mutations. Mismatch repair deficient tumors harbor thousands of mutations Somatic mutations have the potential to generate neo-antigiens which can be recognized by immune system.
38 Clinical Trial Design: Basket Trial Colorectal Cancer Noncolorectal Cancer Group A Mismatch-repair proficient (n = 25) Group B Mismatch-repair deficient (n = 25) Group C Mismatch-repair deficient (n = 21) Anti PD-1 antibody (Pembrolizumab): 10 mg/kg q 2 week Primary endpoint: Immune-related ORR and the 20-week immune-related PFS rate Mismatch-repair status was assessed in tumors with the use of the MSI Analysis System MSI, Microsatellite Instability Analysis System Le DT, et al. N Engl J Med. 2015;372(26):
39 Best Radiographic Response % Change from Baseline SLD M M R-proficient CRC M M R -deficient CRC -100

40 Objective Responses According to RECIST Criteria RECIST, Response EvaluationCriteria in Solid Tumors Le DT, et al. N Engl J Med. 2015;372(26):
41 Progression-free Survival 100 MMR-deficient (mpfs = not reached) Percent survival 50 MMR-proficient (mpfs = 2.3 mos) Time
42 100 Overall Survival MMR-deficient (mos = Not reached) Percent survival 50 MMR-proficient (mos = 5.98 mos) Time
43
44 Nivolumab ± Ipilimumab in Treatment of Patients With Metastatic Colorectal Cancer With and Without High Microsatellite Instability: CheckMate 142 Interim Results Michael Overman, 1 Scott Kopetz, 1 Ray McDermott, 2 Joseph Leach, 3 Sara Lonardi, 4 Heinz-Josef Lenz, 5 Michael Morse, 6 Jayesh Desai, 7 Andrew Hill, 8 Michael Axelson, 9 Rebecca A. Moss, 9 Chen-Sheng Lin, 9 Monica Goldberg, 9 Thierry Andre 10 1 MD Anderson Cancer Center, Houston, TX, USA; 2 St Vincent s University Hospital, Dublin, Ireland; 3 Allina Health System, Minneapolis, MN, USA; 4 Istituto Oncologico Veneto IOV-IRCSS, Padova, Italy; 5 USC Norris Comprehensive Cancer Center, Los Angeles, CA, USA; 6 Duke University Office of Research Administration, Durham, NC, USA; 7 Royal Melbourne Hospital, Victoria, Australia; 8 Tasman Oncology Research Pty Ltd, Southport, Queensland, Australia; 9 Bristol-Myers Squibb, Princeton, NJ, USA; 10 Hopital Saint Antoine, Paris, France
45 Phase 2 CheckMate 142 Study Design: MSI-H Cohort mstage 1 Responses a mstage 2 MSI-H Second-line colon MSI-H 7/19 Nivo 3 mg/kg (Q2W) 1 prior treatment for metastatic disease 1 target lesion ECOG PS of 0-1 Nivo 3 mg/kg (Q2W) Responses a cstage 1 Responses a cstage 2 b 3 6/19 Nivo 3 mg/kg + Ipi 1 mg/kg (Q3W x 4 doses) Then Nivo 3 mg/kg (Q2W) 7/19 Nivo 3 mg/kg + Ipi 1 mg/kg (Q3W x 4 doses) Then Nivo 3 mg/kg (Q2W) a In patients with centrally confirmed MSI-H status b Currently enrolling cstage 1 = combination therapy stage 1; cstage 2 = combination therapy stage 2; Ipi = ipilimumab; mstage 1 = monotherapy stage 1; mstage 2 = monotherapy stage 2; Nivo = nivolumab; Q2W = every 2 weeks; Q3W = every 3 weeks 47
46 Investigator-Assessed Best Overall Response in Patients With MSI-H Receiving Nivolumab Monotherapy ORR, n (%) (95% exact CI) Nivolumab 3 mg/kg (n = 47) a 12 (25.5) (15.4, 38.1) Nivolumab 3 mg/kg Off treatment Nivolumab treatment ongoing 1 st occurrence of new lesion CR or PR % change truncated to 100 Complete response 0 Partial response 12 (25.5) Stable disease 14 (29.8) Progressive disease 17 (36.2) Change From Baseline (%) Unable to determine 4 (8.5) Median time to response, mo (range) Median duration of response, mo (range) 2.12 ( ) NE (0.0 b 15.2 b ) Weeks Horizontal reference line indicates 30% reduction 48
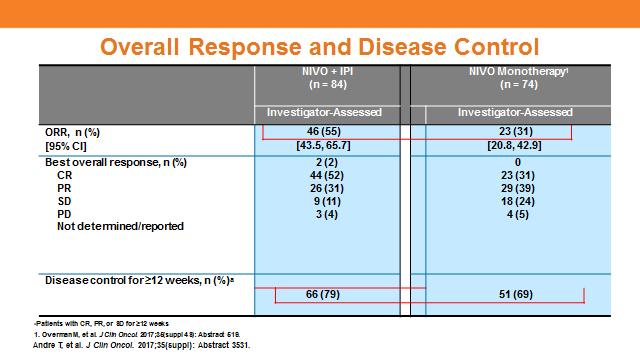
47 Response and Disease Control ORR, n (%) 95% CI dmmr/msi-h per Local Laboratory (N = 74) Investigato r 23 (31.1) 20.8, 42.9 BICR 20 (27.0) 17.4, 38.6 dmmr/msi-h per Central Laboratory (n = 53) Investigato r 19 (35.8) 23.1, 50.2 BICR 17 (32.1) 19.9, 46.3 Best overall response, n (%) CR PR SD PD Unable to determine 0 23 (31.1) 29 (39.2) 18 (24.3) 4 (5.4) 2 (2.7) 18 (24.3) 28 (37.8) 20 (27.0) 6 (11.1) 0 19 (35.8) 21 (39.6) 10 (18.9) 3 (5.7) 1 (1.9) 16 (30.2) 21 (39.6) 12 (22.6) 3 (5.7) Disease control for 12 weeks, n (%) a 51 (68.9) 46 (62.2) 39 (73.6) 37 (69.8) BICR, blinded independent central review. a Patients with CR, PR, or SD for 12 weeks. Presented by: Dr Michael J. Overman
48 Overall Survival Median OS [95% CI], months 12-month OS rate [95% CI], % NR [17.1, NE] 73.8 [59.8, 83.5] Probability of Survival (%) a Months No. at risk NR, not reached. a Patients evaluated as dmmr/msi-h by local laboratory. Presented by: Dr Michael J. Overman
 1% < 1% + Confirmed CR/PR Investigator-Assessed Best Change in Target Lesion Size (%) Rare Intermediate Numerous + Confirmed CR/PR ORR, n/n (%) Investigato r BICR ORR, n/n (%) Investigato r")
49 Reduction in Target Lesion Size Regardless of PD-L1 Expression Tumor PD-L1 Expression Abundance of PD-L1 Expressing Tumor- Associated Immune Cells Investigator-Assessed Best Change in Target Lesion Size (%) 1% < 1% + Confirmed CR/PR Investigator-Assessed Best Change in Target Lesion Size (%) Rare Intermediate Numerous + Confirmed CR/PR ORR, n/n (%) Investigato r BICR ORR, n/n (%) Investigato r BICR Tumor PD-L1 expression 1% < 1% 7/20 (35.0) 6/21 (28.6) 11/45 13/45 (28.9) (24.4) Abundance of PD-L1 expressing immune cells Rare Intermediate Numerous 5/23 (21.7) 5/20 (25.0) 9/23 (39.1) 4/22 (18.2) 4/20 (20.0) 10/23 (43.5) Presented by: Dr Michael J. Overman
50 Patients Study Design Stage 1 Stage 2 Histologica lly confirmed metastatic/ recurrent CRC dmmr/msi-h per local laboratory 1 prior line of therapy MONOTH ERA PY ARM COMBINA TIO N ARM NIVO 3 mg/kg Q2W NIVO 3 mg/kg + IPI 1 mg/kgq3w (4 doses and then NIVO 3 mg/kgq2w) If 7/19 confirmed responders, continue enrollment Primary endpoint: ORR per investigator assessment (RECIST v1.1) If 7/19 confirmed responders, continue enrollment NIVO 3 mg/kg Q2W n = 74 NIVO 3 mg/kg + IPI 1 mg/kgq3w (4 doses and then NIVO 3 mg/kgq2w) n = 84 Other key endpoints: ORR per blinded independent central review (BICR), PFS, OS, and safety Current analysis included all patients (n = 84) who received their first dose 6 months prior to the data cut-off - Median (range) time from first dose to data cut-off: 8.6 ( ) months ORR, overall response; OS, overall survival; PFS, progression-free survival Andre T, et al. J Clin Oncol. 2017;35(suppl): Abstract 3531.
51 Investigator-Assessed Best Overall Response in Patients With MSI-H Receiving Nivolumab + Ipilimumab Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg (n = 27) a Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg ORR, n (%) (95% exact CI) 11 (41.3) (18.6, 50.9) Off treatment Nivolumab + ipilimumab treatment ongoing Complete response st occurrence of new lesion CR or PR Partial response 10(37) Stable disease 14 (51.9) Progressive disease 2(7 ) Unable to determine 0 Change From Baseline (%) Median time to response, mo (range) 2.73 ( ) -75 Median duration of response, mo (range) NE (NE NE) a Patients with 12 weeks of follow-up b Includes censored observations CR = complete response; NE = not estimable; PR = partial response Weeks Horizontal reference line indicates 30% reduction 53
52
53
54 Event, n (%) Treatment-Related Adverse Events in 15% of Patients With MSI-H Nivolumab 3 mg/kg (n = 70) Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg (n = 30) Any grade Grade 3 4 Any grade Grade 3 4 Any event 41 (58.6) a 10 (14.3) 25 (83.3) 8 (26.7) Fatigue 13 (18.6) 1 (1.4) 6 (20.0) 0 Diarrhea 10 (14.3) 1 (1.4) 13 (43.3) 0 Pruritus 8 (11.4) 0 5 (16.7) 1 (3.3) Nausea 5 (7.1) 0 6 (20.0) 0 Pyrexia 3 (4.3) 0 7 (23.3) 0 Any event leading to discontinuation a One Grade 5 event of sudden death 4 (5.7) 2 (2.9) 4 (13.3) 4 (13.3) 57
55 Question?? Can we convert non-immunogenic tumor into immunogenic tumor?

56 PD-L1 and MEK Inhibition: A Rational Combination MEK inhibition alone can result in intratumoral T-cell accumulation and MHC I upregulation, and synergizes with an anti-pdl1 agent to promote durable tumor regression 1 CD8 + T cell per tumor cell Class I MHC P = Tumor volume (mm 3 ) Control Anti-PDL1 MEKi (38963) MEKi + anti-pdl1 ND MEKi ND MEKi Day To examine the possible benefits of MEK inhibition with an anti-pdl1 agent, we evaluated cobimetinib + atezolizumab in patients with advanced solid tumors MHC, major histocompatibility complex; ND, no drug (vehicle alone). CT26 (KRASmt) CRC models. 1. Ebert et al. Immunity Bendell J, et al. Cobimetinib and atezolizumab in CRC. ASCO

57 Cobimetinib + Atezolizumab in CRC: Phase Ib Dose Escalation and Cohort Expansion Study a Cobimetinib was administered on 21 days on/7 days off dosing schedule. Atezo, atezolizumab; cobi, cobimetinib; DLT, drug limited toxicity; ECOG PS, Eastern Cooperative Oncology Group performance status; KRASmt, KRAS mutant; MTD, maximum tolerated dose; NSCLC, non-small cell lung cancer Bendell J, et al. J Clin Oncol. 2016;34(suppl): Abstract 3502.

58 Efficacy: Change Maximum SLD Reduction From Baseline, % PD PD TC 3 PD PD PD PD in Tumor Burden PD PD PD PD PD SD SD SD PD SD SD PR T C0 PR PR T C0 TC N A PR T C0 PD-L1 IC status NA IC0 IC1 IC2 IC3 4 patients had partial responses (confirmed per RECIST v1.1) MSI status of CRC patients was examined by NGS-based scoring: 3 of 4 responders were mismatch-repair proficient (not MSI-H); 1 responder had unknown MSI status and was not evaluable Tumor volume reduction was not associated with PD-L1 status: TC3 (n = 1; PD), TC0 (n = 18), NA (n = 4) PD-L1 IHC status on tumor cells (TC) and tumor-infiltrating immune cells (IC) defined as: TC3 = TC 50% PD-L1+ cells; IC3 = IC 10% PD-L1+ cells; TC2 = TC 5% and < 50% PD-L1+ cells; IC2 = IC 5% and < 10% PD-L1+ cells; TC1 = TC 1% and < 5% PD-L1+ cells; IC1 = IC 1% and < 5% PD-L1+ cells; TC0 = TC < 1% PD-L1+ cells; IC0 = IC < 1% PD-L1+ cells. NA, not available; NGS, next generation sequencing. Efficacy-evaluable patients. 2 patients missing or unevaluable are not included. Data cut-off February 12, Bendell J, et al. Cobimetinib and atezolizumab in CRC. ASCO
59 Efficacy: Change in Tumor Burden Over Time Change in Sum of Longest Diameters from Baseline, % PD SD PR/CR a Discontinued atezolizumab New lesion Median duration of response was not reached (range: 5.4 to mo) Responses are ongoing in 2 of 4 responding patients Time on Study (mo) a Confirmed per RECIST v1.1. CR, complete response; PD, progressive disease; PR, partial response; SD, stable disease. Efficacy-evaluable patients. 2 patients missing or unevaluable are not included. Data cut-off February 12, Bendell J, et al. Cobimetinib and atezolizumab in CRC. ASCO

60 Phase Ib Dose Escalation and Cohort Expansion Study (NCT ) Presented By Johanna Bendell at 2018 Gastrointestinal Cancers Symposium

61 Duration of Response Presented By Johanna Bendell at 2018 Gastrointestinal Cancers Symposium

62 Progression-Free Survival and Overall Survival Presented By Johanna Bendell at 2018 Gastrointestinal Cancers Symposium
63 COTEZO IMblaze-370: Phase 3 Trial Atezolizumab With and Without Cobimetinib vs Regorafenib Atezolizumab + cobimetinib 840 mg IV days 1, mg days 1-21 Eligibility Criteria: mcrc 2 prior therapies Progression on or within 3 months of prior therapy ECOG PS 0-1 N = 360 2:1:1 R Atezolizumab 1200 mg IV on day 1 28 day cycle Treatment until: Disease progression, unacceptable toxicity, or death Regorafenib 160 mg per d Days 1-21; 28 day cycle Outcomes Primary endpoint: OS Secondary endpoint: PFS, ORR, DOR, QoL, safety 1,
64 Summary VEGF and EGFR mabs competing for first-line patients in RAS wt CRC For anti-egfr treatment, all RAS tests are required Primary tumor location is related to effect of cetuximab Bevacizumab, Ramucirumab and Aflibercept competing for second-line patients with each other, and with EGFR mabs in KRAS wt CRC
65 Summary Best sequence of therapies (VEGFi vs EGFRi) still to be established Regorafenib and TAS 102 as salvage therapy option Checkpoint inhibitors are highly active in select molecular subsets Rationale combination maybe able to covert cold tumor to hot tumor
66 Thank you! GI oncology questions
Randomized trial of irinotecan and cetuximab with or without vemurafenib in BRAF-mutant metastatic colorectal cancer (SWOG S1406)
") Randomized trial of irinotecan and cetuximab with or without vemurafenib in BRAF-mutant metastatic colorectal cancer (SWOG S1406) ASCO Annual Meeting 2017 Randomized trial of irinotecan and cetuximab with
Randomized trial of irinotecan and cetuximab with or without vemurafenib in BRAF-mutant metastatic colorectal cancer (SWOG S1406) ASCO Annual Meeting 2017 Randomized trial of irinotecan and cetuximab with
Bristol-Myers Squibb, Braine-l Alleud, Belgium; 12 MD Anderson Cancer Center, Houston, TX, USA
 3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142
 Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142 Abstract #519 Overman MJ, Lonardi S, Leone F, McDermott
Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142 Abstract #519 Overman MJ, Lonardi S, Leone F, McDermott
Carcinoma colorettale: personalizzazione del trattamento
 33 Incontro Oncologico del Triveneto Padova, Aprile 2017 Carcinoma colorettale: personalizzazione del trattamento Fotios Loupakis, MD PhD U.O.C. Oncologia Medica 1 Dipartimento di Oncologia Clinica e Sperimentale
33 Incontro Oncologico del Triveneto Padova, Aprile 2017 Carcinoma colorettale: personalizzazione del trattamento Fotios Loupakis, MD PhD U.O.C. Oncologia Medica 1 Dipartimento di Oncologia Clinica e Sperimentale
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER. Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium
 THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
Κίκα Πλοιαρχοπούλου. Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών
 Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
Presentation Number: LBA18_PR. Lecture Time: 09:15-09:27. Speakers: Heinz-Josef J. Lenz (Los Angeles, US) Background
 Background") LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer
 Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer Axel Grothey, M.D., Professor of Oncology, Clinical and Translational Science Division of Medical Oncology Mayo Clinic, Rochester,
Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer Axel Grothey, M.D., Professor of Oncology, Clinical and Translational Science Division of Medical Oncology Mayo Clinic, Rochester,
Colon Cancer Molecular Target Agents
 Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
AIOM GIOVANI Perugia, Luglio 2017
 AIOM GIOVANI 2017 Perugia, 07-08 Luglio 2017 Scelta delle linee successive nel paziente RAS e BRAF wild-type con particolare accento su nuovi bersagli terapeutici Francesca Battaglin U.O.C. Oncologia Medica
AIOM GIOVANI 2017 Perugia, 07-08 Luglio 2017 Scelta delle linee successive nel paziente RAS e BRAF wild-type con particolare accento su nuovi bersagli terapeutici Francesca Battaglin U.O.C. Oncologia Medica
Colon cancer: Highlights. Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano
 Colon cancer: Highlights Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano Agenda 1) Metastatic colorectal cancer First-line treatment molecularly unselected: FOLFOXIRI-bev (CHARTA trial) Later-line
Colon cancer: Highlights Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano Agenda 1) Metastatic colorectal cancer First-line treatment molecularly unselected: FOLFOXIRI-bev (CHARTA trial) Later-line
Treatment of Advanced Colorectal Cancer
 Treatment of Advanced Colorectal Cancer Alexis D. Leal, M.D. Assistant Professor, GI Medical Oncology University of Colorado Cancer Center Disclosures None Objectives Review the basics of advanced colorectal
Treatment of Advanced Colorectal Cancer Alexis D. Leal, M.D. Assistant Professor, GI Medical Oncology University of Colorado Cancer Center Disclosures None Objectives Review the basics of advanced colorectal
MEETING SUMMARY ESMO 2018, Munich, Germany. Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER
 MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
Right Drug for the Right Colorectal Patient: Select the Best Initial Therapy and What Comes After 5-FU/OXALI/IRINO?
 Right Drug for the Right Colorectal Patient: Select the Best Initial Therapy and What Comes After 5-FU/OXALI/IRINO? Axel Grothey Professor of Oncology Minnesota -> Tennessee The Luxury of So Many Options...
Right Drug for the Right Colorectal Patient: Select the Best Initial Therapy and What Comes After 5-FU/OXALI/IRINO? Axel Grothey Professor of Oncology Minnesota -> Tennessee The Luxury of So Many Options...
Colon Cancer: State of the Art
 Colon Cancer: State of the Art Heinz-Josef Lenz Professor of Medicine and Preventive Medicine Associate Director, Clinical Research J Terrence Lanni Chair in Cancer Research Co-Director, USC Center for
Colon Cancer: State of the Art Heinz-Josef Lenz Professor of Medicine and Preventive Medicine Associate Director, Clinical Research J Terrence Lanni Chair in Cancer Research Co-Director, USC Center for
Colon Cancer ASCO Poster Review
 Rome, February 11 th 2017 AIOM POST ASCO GI Review Colon Cancer ASCO Poster Review Lisa Salvatore UOC Oncologia Policlinico GB Rossi Azienda Ospedaliero Universitaria Integrata di Verona Me Before Me After
Rome, February 11 th 2017 AIOM POST ASCO GI Review Colon Cancer ASCO Poster Review Lisa Salvatore UOC Oncologia Policlinico GB Rossi Azienda Ospedaliero Universitaria Integrata di Verona Me Before Me After
Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO. CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS?
 INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS? V. Alonso Servicio de Oncologia Medica H. U. Miguel Servet Zaragoza MSI-H mcrc Clinical and Pathological
INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS? V. Alonso Servicio de Oncologia Medica H. U. Miguel Servet Zaragoza MSI-H mcrc Clinical and Pathological
ASCO 2017 updates in Colorectal and Gastric Cancers. May Cho, M.D.
 ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression
 Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression Guillermo Méndez, MD Sección Oncología Hospital de Gastroenterología Bonorino Udaondo Carlos B. Udaondo y Fundación
Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression Guillermo Méndez, MD Sección Oncología Hospital de Gastroenterología Bonorino Udaondo Carlos B. Udaondo y Fundación
Management of Patients with Colorectal Cancer
 Management of Patients with Colorectal Cancer Elsevier Office of Continuing Medical Education Independent Conference Highlights of the ASCO-GI 2018 Symposium Disclaimer The views expressed in the following
Management of Patients with Colorectal Cancer Elsevier Office of Continuing Medical Education Independent Conference Highlights of the ASCO-GI 2018 Symposium Disclaimer The views expressed in the following
Novel Molecularly Targeted Therapies and Biomarkers in Advanced Colorectal Cancer. Objectives
 Novel Molecularly Targeted Therapies and Biomarkers in Advanced Colorectal Cancer Michael S. Lee, MD Assistant Professor of Medicine University of North Carolina Objectives Discuss important clinicopathologic
Novel Molecularly Targeted Therapies and Biomarkers in Advanced Colorectal Cancer Michael S. Lee, MD Assistant Professor of Medicine University of North Carolina Objectives Discuss important clinicopathologic
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS
 CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
Colorectal Cancer in 2017: From Biology to the Clinics. Rodrigo Dienstmann
 Colorectal Cancer in 2017: From Biology to the Clinics Rodrigo Dienstmann MOLECULAR CLASSIFICATION Tumor cell Immune cell Tumor microenvironment Stromal cell MOLECULAR CLASSIFICATION Biomarker Tumor cell
Colorectal Cancer in 2017: From Biology to the Clinics Rodrigo Dienstmann MOLECULAR CLASSIFICATION Tumor cell Immune cell Tumor microenvironment Stromal cell MOLECULAR CLASSIFICATION Biomarker Tumor cell
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine
 CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine") ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO. Dra. Ruth Vera Complejo Hospitalario de Navarra
 MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
ADVANCES IN COLON CANCER
 ADVANCES IN COLON CANCER Peter T. Silberstein, M.D., FACP Professor, Creighton University Chief Hematology/Oncology UNIVERSAL SCREENING FOR LYNCH SYNDROME OF ALL PATIENTS WITH COLON CANCER ADOPTED BY CHI
ADVANCES IN COLON CANCER Peter T. Silberstein, M.D., FACP Professor, Creighton University Chief Hematology/Oncology UNIVERSAL SCREENING FOR LYNCH SYNDROME OF ALL PATIENTS WITH COLON CANCER ADOPTED BY CHI
Immunotherapy in Colorectal cancer
 Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD
 METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
The left versus right colon cancer story What is the truth?
 The left versus right colon cancer story What is the truth? Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany Three stages of truth (Schopenhauer) Ridicule
The left versus right colon cancer story What is the truth? Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany Three stages of truth (Schopenhauer) Ridicule
NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO
 Congresso AIOM Giovani Perugia, 9 luglio 2016 NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO Carlotta Antoniotti Polo Oncologico Azienda Ospedaliero-Universitaria Pisana Università di Pisa What
Congresso AIOM Giovani Perugia, 9 luglio 2016 NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO Carlotta Antoniotti Polo Oncologico Azienda Ospedaliero-Universitaria Pisana Università di Pisa What
DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT?
 DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT? By: Dr. Dominik Modest, Medical Department III, Hospital of the University of Munich, Germany Dr. Andrea Sartore-Bianchi, Niguarda Cancer Center,
DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT? By: Dr. Dominik Modest, Medical Department III, Hospital of the University of Munich, Germany Dr. Andrea Sartore-Bianchi, Niguarda Cancer Center,
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
Colorectal Cancer in the Coming Years: What Can We Expect?
 Colorectal Cancer in the Coming Years: What Can We Expect? Clara Montagut, MD, PhD Hospital Universitari del Mar, Barcelona, Spain Memorial Sloan Kettering Cancer Center, New York, United States What Are
Colorectal Cancer in the Coming Years: What Can We Expect? Clara Montagut, MD, PhD Hospital Universitari del Mar, Barcelona, Spain Memorial Sloan Kettering Cancer Center, New York, United States What Are
Immunoterapia en Cáncer colorrectal. Manuel Benavides
 Immunoterapia en Cáncer colorrectal Manuel Benavides Agenda - Cáncer colorrectal / MSI - MSI-H / MSI-L o MSI-S - Inhibidores de Checkpoints Molecular Pathways in Colorectal Cancer tability or MSI (15%)
Immunoterapia en Cáncer colorrectal Manuel Benavides Agenda - Cáncer colorrectal / MSI - MSI-H / MSI-L o MSI-S - Inhibidores de Checkpoints Molecular Pathways in Colorectal Cancer tability or MSI (15%)
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy
: Biomarkers for Immunotherapy") Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Ashita Waterston Beatson West of Scotland Cancer Centre
 Ashita Waterston Beatson West of Scotland Cancer Centre Aim of treatment Scheduling and choice of treatments are dictated by aim: Down staging for resectability: upfront intensive Prolong survival: combination
Ashita Waterston Beatson West of Scotland Cancer Centre Aim of treatment Scheduling and choice of treatments are dictated by aim: Down staging for resectability: upfront intensive Prolong survival: combination
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Royal Marsden Hospital ESMO Colorectal Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role Servier, Celgene, BMS, Five
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Royal Marsden Hospital ESMO Colorectal Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role Servier, Celgene, BMS, Five
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
My name is Dr. David Ilson, Professor of Medicine at Memorial Sloan Kettering Cancer Center and Weill Cornell Medical Center in New York, New York.
 Welcome to this CME/CE-certified activity entitled, Integrating the Latest Advances Into Clinical Experience: Data and Expert Insights From the 2016 Meeting on Gastrointestinal Cancers in San Francisco.
Welcome to this CME/CE-certified activity entitled, Integrating the Latest Advances Into Clinical Experience: Data and Expert Insights From the 2016 Meeting on Gastrointestinal Cancers in San Francisco.
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
Validated and promising predictive factors in mcrc: Recent updates on RAS testing Fotios Loupakis, MD PhD
 Validated and promising predictive factors in mcrc: Recent updates on RAS testing Fotios Loupakis, MD PhD U.O. Oncologia 2 Universitaria Azienda Ospedaliero-Universitaria Pisana Pisa, Italy Learning Objectives
Validated and promising predictive factors in mcrc: Recent updates on RAS testing Fotios Loupakis, MD PhD U.O. Oncologia 2 Universitaria Azienda Ospedaliero-Universitaria Pisana Pisa, Italy Learning Objectives
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy. What every patient needs to know. James Larkin
 Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Highlights STOMACH CANCER
 UPDATES and NEWS from the Gastrointestinal Cancers Symposium in San Francisco Roma, 10-11 Febbraio 2017 Highlights STOMACH CANCER Lorenzo Fornaro, MD Unit of Medical Oncology 2 Azienda Ospedaliero-Universitaria
UPDATES and NEWS from the Gastrointestinal Cancers Symposium in San Francisco Roma, 10-11 Febbraio 2017 Highlights STOMACH CANCER Lorenzo Fornaro, MD Unit of Medical Oncology 2 Azienda Ospedaliero-Universitaria
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
Objectives. Briefly summarize the current state of colorectal cancer
 Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
Colon Cancer Update Christie J. Hilton, DO
 POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
MANAGEMENT OF ADVANCED COLORECTAL CANCER
 MANAGEMENT OF ADVANCED COLORECTAL CANCER Alberto Sobrero IRCCS San Martino IST Genoa Italy Disclosures : Pfizer, Roche, Merck, Amgen, Celgene, Bayer, Sanofi, Nordic, Takeda,BMS, Syrtex, Servier outline
MANAGEMENT OF ADVANCED COLORECTAL CANCER Alberto Sobrero IRCCS San Martino IST Genoa Italy Disclosures : Pfizer, Roche, Merck, Amgen, Celgene, Bayer, Sanofi, Nordic, Takeda,BMS, Syrtex, Servier outline
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Kolorektalni karcinom- novosti u liječenju. PANEL: Maja Banjin, Janja Ocvirk, Borislav Belev, Ivan Nikolić, Anes Pašić
 Kolorektalni karcinom- novosti u liječenju PANEL: Maja Banjin, Janja Ocvirk, Borislav Belev, Ivan Nikolić, Anes Pašić Kolorektalni karcinomnovosti u liječenju PANEL : Maja Banjin, Janja Ocvirk, Borislav
Kolorektalni karcinom- novosti u liječenju PANEL: Maja Banjin, Janja Ocvirk, Borislav Belev, Ivan Nikolić, Anes Pašić Kolorektalni karcinomnovosti u liječenju PANEL : Maja Banjin, Janja Ocvirk, Borislav
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER
 OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux
 Michel Ducreux") Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux 2 ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working groups E Van Cutsem A Sobrero
Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux 2 ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working groups E Van Cutsem A Sobrero
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Daniele Santini University Campus Bio-Medico Rome, Italy
 Daniele Santini University Campus Bio-Medico Rome, Italy Anti EGFR therapy and colorectal cancer Cetuximab or Panitumumab Adapted from Ciardiello F. and Tortora G. NEJM 2008;358:1160-74 Who will benefit
Daniele Santini University Campus Bio-Medico Rome, Italy Anti EGFR therapy and colorectal cancer Cetuximab or Panitumumab Adapted from Ciardiello F. and Tortora G. NEJM 2008;358:1160-74 Who will benefit
MELANOMA METASTASICO: NUEVAS COMBINACIONES. Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona
 MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
Dr. Iain Tan. Senior Consultant GI Medical Oncologist National Cancer Centre Singapore
 ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
Colorectal Cancer: Lumping or Splitting? Jimmy J. Hwang, MD FACP Levine Cancer Institute Carolinas HealthCare System Charlotte, NC
 Colorectal Cancer: Lumping or Splitting? Jimmy J. Hwang, MD FACP Levine Cancer Institute Carolinas HealthCare System Charlotte, NC 2 Epidemiology Colorectal Cancer is the 2 nd Leading Cause of Cancer-related
Colorectal Cancer: Lumping or Splitting? Jimmy J. Hwang, MD FACP Levine Cancer Institute Carolinas HealthCare System Charlotte, NC 2 Epidemiology Colorectal Cancer is the 2 nd Leading Cause of Cancer-related
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
New Systemic Therapies in Advanced Melanoma
 New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
Colon cancer: ASCO poster review. Alfonso De Stefano MD, PhD SC Oncologia Clinica Sperimentale Addome
 Colon cancer: ASCO poster review Alfonso De Stefano MD, PhD SC Oncologia Clinica Sperimentale Addome a.destefano@istitutotumori.na.it 255 poster examined: my selection Clinical Practice Translational &
Colon cancer: ASCO poster review Alfonso De Stefano MD, PhD SC Oncologia Clinica Sperimentale Addome a.destefano@istitutotumori.na.it 255 poster examined: my selection Clinical Practice Translational &
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
What s New in Colon Cancer? Therapy over the last decade
 What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
Squamous Cell Carcinoma Standard and Novel Targets.
 Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options
 Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
Recent Advances in Gastrointestinal Cancers
 Recent Advances in Gastrointestinal Cancers Ursina R. Teitelbaum, MD Section of Hematology/Oncology Abramson Cancer Center PENN 2016 Updates in Oncology June 23, 2016 none Disclosures ASCO 2016 Highlights:
Recent Advances in Gastrointestinal Cancers Ursina R. Teitelbaum, MD Section of Hematology/Oncology Abramson Cancer Center PENN 2016 Updates in Oncology June 23, 2016 none Disclosures ASCO 2016 Highlights:
COMETS: COlorectal MEtastatic Two Sequences
 COMETS: COlorectal MEtastatic Two Sequences A Phase III Multicenter Trial Comparing Two Different Sequences of Second/Third Line Therapy (Irinotecan/Cetuximab Followed By FOLFOX-4 vs. FOLFOX-4 Followed
COMETS: COlorectal MEtastatic Two Sequences A Phase III Multicenter Trial Comparing Two Different Sequences of Second/Third Line Therapy (Irinotecan/Cetuximab Followed By FOLFOX-4 vs. FOLFOX-4 Followed
AACR 2018 Investor Meeting
 AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
NSCLC 2 nd and further line therapies. Egbert F. Smit MD PhD. Dept. Thoracic Oncology, Netherlands Cancer Institute
 NSCLC 2 nd and further line therapies Egbert F. Smit MD PhD. Dept. Thoracic Oncology, Netherlands Cancer Institute e.smit@nki.nl ESMO Guidelines 2016: Treatment of Stage IV nonsquamous NSCLC at progression
NSCLC 2 nd and further line therapies Egbert F. Smit MD PhD. Dept. Thoracic Oncology, Netherlands Cancer Institute e.smit@nki.nl ESMO Guidelines 2016: Treatment of Stage IV nonsquamous NSCLC at progression
First line treatment in metastatic colorectal cancer
 First line treatment in metastatic colorectal cancer Claus-Henning Köhne University Clinic Onkology and Haematology North West German Cancer Center (NWTZ) A non authorised version of ESMO guidelines was
First line treatment in metastatic colorectal cancer Claus-Henning Köhne University Clinic Onkology and Haematology North West German Cancer Center (NWTZ) A non authorised version of ESMO guidelines was
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Management of Brain Metastases Sanjiv S. Agarwala, MD
 Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Nivolumab for previously treated metastatic colorectal cancer with high microsatellite instability or mismatch repair deficiency
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Nivolumab for previously treated metastatic colorectal cancer with high microsatellite instability or mismatch repair deficiency
Immunotherapy for dmmr metastatic colorectal cancer. Prof.dr. Kees Punt Dept. Medical Oncology AUMC
 Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Overview: Immunotherapy in CNS Metastases
 Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
HeavilyTreated mcrc..whats next?
 ESMO Preceptorship Programme Gastrointestinal Cancer 20-22 October 2016,Singapore Dr Surendra Pal Chaudhary Dept of Medical Oncology Dr BR Ambedkar Instituite Rotary Cancer Hospital All India Institute
ESMO Preceptorship Programme Gastrointestinal Cancer 20-22 October 2016,Singapore Dr Surendra Pal Chaudhary Dept of Medical Oncology Dr BR Ambedkar Instituite Rotary Cancer Hospital All India Institute
Eric Van Cutsem University Hospitals Leuven, Belgium
 BEACON CRC Study Safety Lead-in: Assessment of the BRAF Inhibitor Encorafenib + MEK Inhibitor Binimetinib + Anti Epidermal Growth Factor Receptor Antibody Cetuximab for BRAF V600E Metastatic Colorectal
BEACON CRC Study Safety Lead-in: Assessment of the BRAF Inhibitor Encorafenib + MEK Inhibitor Binimetinib + Anti Epidermal Growth Factor Receptor Antibody Cetuximab for BRAF V600E Metastatic Colorectal
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Fighting a Smarter War On Colon Cancer:
 Fighting a Smarter War On Colon Cancer: Value as a new endpoint? John L. Marshall, MD Tel: (202) 444-0275 Fax: (202) 444-1229 http://lombardi.georgetown.edu/gi Stakeholder Motivation Stakeholders FDA CMS/Payers
Fighting a Smarter War On Colon Cancer: Value as a new endpoint? John L. Marshall, MD Tel: (202) 444-0275 Fax: (202) 444-1229 http://lombardi.georgetown.edu/gi Stakeholder Motivation Stakeholders FDA CMS/Payers
ANTI-EGFR IN MCRC? Assoc. Prof. Gerald Prager, Medical University of Vienna, Austria
 IS IT TIME TO RE-CHALLENGE ANTI-EGFR IN MCRC? Assoc. Prof. Gerald Prager, Medical University of Vienna, Austria Dr. Andrea Sartore-Bianchi, Oncologia Clinica Molecolare, Niguarda Cancer Center, Milano,
IS IT TIME TO RE-CHALLENGE ANTI-EGFR IN MCRC? Assoc. Prof. Gerald Prager, Medical University of Vienna, Austria Dr. Andrea Sartore-Bianchi, Oncologia Clinica Molecolare, Niguarda Cancer Center, Milano,
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
News from ASCO. Niven Mehra, Medical Oncologist. Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital
 News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
How to treat a patient with metastatic CRC? Towards personalized treatment strategies
 How to treat a patient with metastatic CRC? Towards personalized treatment strategies Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Progress in the treatment
How to treat a patient with metastatic CRC? Towards personalized treatment strategies Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Progress in the treatment
Keynote Presentation I New Era of CRC Management: Impact of Tumor Sidedness and Molecular Subtypes of CRC
 Keynote Presentation I New Era of CRC Management: Impact of Tumor Sidedness and Molecular Subtypes of CRC Scott Kopetz, MD, PhD, FACP University of Texas MD Anderson Cancer Center Houston, Texas, United
Keynote Presentation I New Era of CRC Management: Impact of Tumor Sidedness and Molecular Subtypes of CRC Scott Kopetz, MD, PhD, FACP University of Texas MD Anderson Cancer Center Houston, Texas, United
Atezolizumab Is a Humanized Anti-PDL1 Antibody That Inhibits the Binding of PD-L1 to PD-1 and B7.1
 Phase II, Single-Arm Trial (BIRCH) of Atezolizumab as First-Line or Subsequent Therapy for Locally Advanced or Metastatic PD-L1-Selected Non-Small Cell Lung Cancer (NSCLC) Abstract 16LBA Besse B, Johnson
Phase II, Single-Arm Trial (BIRCH) of Atezolizumab as First-Line or Subsequent Therapy for Locally Advanced or Metastatic PD-L1-Selected Non-Small Cell Lung Cancer (NSCLC) Abstract 16LBA Besse B, Johnson
Evan J. Lipson, M.D.
 Update on treatment for Merkel cell, cutaneous squamous cell and basal cell cancers Evan J. Lipson, M.D. The Johns Hopkins University School of Medicine Bloomberg~Kimmel Institute for Cancer Immunotherapy
Update on treatment for Merkel cell, cutaneous squamous cell and basal cell cancers Evan J. Lipson, M.D. The Johns Hopkins University School of Medicine Bloomberg~Kimmel Institute for Cancer Immunotherapy
Current experience in immunotherapy for metastatic renal cell carcinoma
 Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Review of the ESMO consensus conference on metastatic colorectal cancer Basic strategies and groups. Chemotherapy and targeted agents in 1st line
 ESMO Preceptorship Programme Colorectal Cancer Valencia, 18th May 2018 Review of the ESMO consensus conference on metastatic colorectal cancer Basic strategies and groups Chemotherapy and targeted agents
ESMO Preceptorship Programme Colorectal Cancer Valencia, 18th May 2018 Review of the ESMO consensus conference on metastatic colorectal cancer Basic strategies and groups Chemotherapy and targeted agents
ESMO GI / BEACON CRC SAFETY LEAD-IN ENCORE PRESENTATION June 23, 2018
 ESMO GI / BEACON CRC SAFETY LEAD-IN ENCORE PRESENTATION June 23, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
ESMO GI / BEACON CRC SAFETY LEAD-IN ENCORE PRESENTATION June 23, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in