ACCME/Disclosures 4/13/2016. Clinical History
|
|
|
- Shannon Wiggins
- 5 years ago
- Views:
Transcription

1 ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner have, or have had, within the past 12 months, which relates to the content of this educational activity and creates a conflict of interest. Dr. Yi-Hua Chen declares no conflict of interest to disclose. Clinical History Peripheral blood 70 year-old male with macrocytic anemia for 10 years, became transfusion dependent. Two prior BM biopsie: hypercellular, no specific diagnoses Normal B12, folate, thyroid function test, iron studies; evidence of hemolysis. Splenectomy 3 year ago: congestion & lymphocytosis. WBC 5.6 x10 9 /L Hb 8.0 g/dl MCV 106 fl Plt 485 x10 9 /L Neutrophil 65.0% Lymph 20.0% Monocyte 14.5% Basophil 0.5% Abs. lymph: 1.1 x 10 9 /L 1



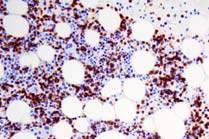
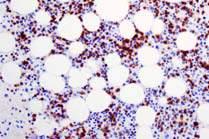
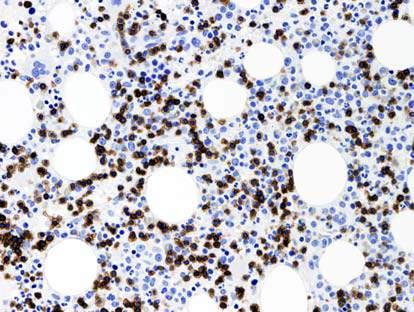
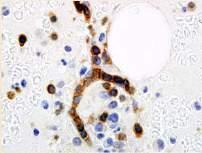
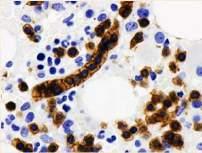
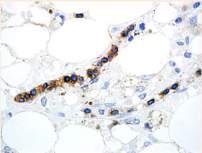
2 Bone Marrow Aspirate Bone Marrow Core Biopsy Low power unremarkable highlights T cell infiltrate: ~30% Example case 2 Intrasinusoidal infiltration (single cell layer) 2





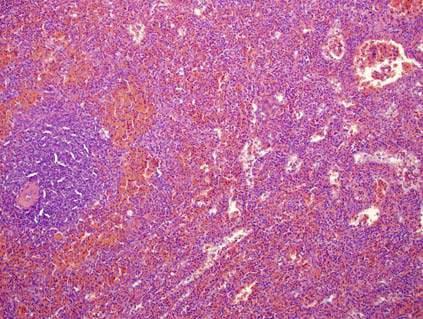
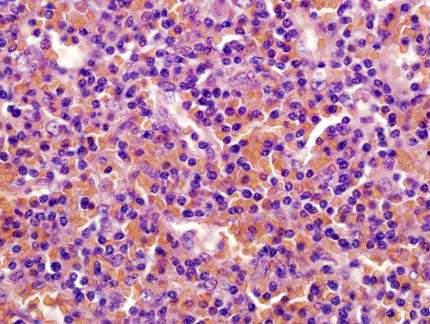
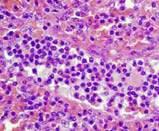


3 Flow Cytometric Analysis CD4-CD8- T cells Normal T cells Spleen CD7 CD5 CD4 CD 3 CD2 CD8 Immunophenotype summary: +, CD2+, CD7+, CD5-, CD4-, CD8-, TCR + TIA-1+ (IHC) CD56-, CD57- (IHC) Red pulp Spleen CD20 3








![46,XY[20] FISH](/docs-images/83/87512648/images/4-8.jpg "Negative for i(7q)")
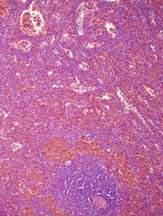
4 Spleen +, CD4-, CD8-, CD5-, TCR Spleen CD4- TIA-1+ Granzyme B+ Perforin+ CD8- CD5- TCR HSTCL: TIA1+, granzyme B-, Perforin- (inactivated cytotoxic T cell) Spleen Ancillary Studies Molecular analysis Identical clonal TCR rearrangement in PB and spleen Cytogenetic studies 46,XY[20] FISH Negative for i(7q) CD56 CD57 Summary: +, CD5, CD4, CD8, TCR +, TIA1+, GrB+, Perforin+, CD56, CD57, EBER 4
5 Diagnosis & Follow-up Diagnosis T-LGL leukemia (CD4-/CD8- +) with associated pure red cell aplasia Follow-up (10 years) Treated with steroids: hemoglobin rose; transfusion independent Survived for 10 years from the diagnosis of T-LGL leukemia and ~20 years from disease onset. Features supporting the diagnosis in this case Morphologic features BM: interstitial and focal intrasinusoidal infiltrate (single-cell layer) Spleen: red pulp involvement Activated cytotoxic T-cell phenotype Clonal TCR gene rearrangement Negative for i7q Clinical picture! Older age (70 years) Long-standing refractory anemia Moderate splenomegaly without lymphadenopathy Associated autoimmunity: AIHA, PRCA Indolent disease course T-LGL leukemia 2-5% of chronic LPD Median age of 60 years, equal M:F ratio Brief review of T-LGL leukemia Clonal proliferation of cytotoxic T cells (most commonly +CD8+) Cytopenias (most commonly neutropenia and anemia) Splenomegaly without adenopathy Often associated with autoimmune disorders especially rheumatoid arthritis 5
:2764 2774 2. Steinway SN, Leblanc F and Loughran T. Blood Rev.")

 * Autoimmune cytopenias (PRCA, AIHA, ITP) 5 10 Cyclic neutropenia Rare Neoplasms <10 Solid tumors <4 Myelodysplasia <4 B cell")

6 Clinical context Cytopenia (Neutropenia, anemia) Splenomegaly Lymphocytosis Autoimmune conditions (e.g. RA) Modified from: 1. Lamy T and Loughran T. Blood. 2011; 117(10): Steinway SN, Leblanc F and Loughran T. Blood Rev. 2014; 28(3):87 94 Diagnosis of T-LGL leukemia BM biopsy IHC FC PB smear / Flow cytometry (FC) LGL < 500/uL phenotype LGL > 500/uL Phenotyping Clonality FC: KIR or V repertoire PCR: TCR gene NK phenotype FC: KIR Disorders Associated with T LGLL Disorder Frequency % Autoimmune diseases Rheumatoid arthritis (RA) Other autoimmune (Sjogren syndrome, polymyocytis, Case reports endocrinopathy, etc.) * Autoimmune cytopenias (PRCA, AIHA, ITP) 5 10 Cyclic neutropenia Rare Neoplasms <10 Solid tumors <4 Myelodysplasia <4 B cell malignancies 5 7 CML treated with desatinib N/A Monoclonal B cell lymphocytosis 16 MGUS 19 Viral infection, s/p organ or HSC transplant Rare Pulmonary hypertension Rare Modified from Lamy T and Loughran T. Blood 2011; 117: Peripheral blood T-LGL leukemia Bone marrow aspirate T-LGL leukemia Interstitial & intrasinusoidal infiltration 6
 Cytopenias (neutropenia and anemia most common) Bone")
 Reactive lymphoid aggregates may be present Spleen Involving")

 CD16 (common but variable) Expression of cytotoxic molecule-associated antigens TIA-1+,")
7 T-LGL Leukemia CD8 Reactive lymphoid aggregate (CD8-, CD4+) CD4 Morphologic features of T-LGL leukemia Peripheral blood Increased LGLs (variable levels) Cytopenias (neutropenia and anemia most common) Bone marrow Slightly hypercellular, normocellular or hypocellular BM involvement often <50% Interstitial & intrasinusoidal infiltration (linear array) Reactive lymphoid aggregates may be present Spleen Involving the red pulp T-LGL Leukemia: Immunophenotype Common type TCR +, +, CD8+ Rare variants: TCR +, +, CD4+ TCR +, +, CD4+, CD8+ TCR +, +, CD8+ TCR +, +, CD4-, CD8- T-LGL leukemia: Immunophenotype Pan T-cell antigens Loss of CD5 (most common) Loss of CD7 Expression of NK-cell associated antigens CD57 (most cases positive) CD56 (small subset) CD16 (common but variable) Expression of cytotoxic molecule-associated antigens TIA-1+, granzyme B+, perforin+ 7

:2764 2774 2. Steinway SN, Leblanc F and Loughran T. Blood Rev. 2014; 28(3):87 94 Clonality FC: KIR or V repertoire PCR: TCR gene FC: KIR 8")
8 TCR V usage T-LGL leukemia: Analysis of clonality T-LGL leukemia: Analysis of clonality CD158 (KIR) expression Forward scatter Vb3 Restricted Usage of Vb7.1 Vb7.1 Restricted expression of CD158b Side Scatter CD5 Vb 5.3 CD158a CD158b CD158e PCR for TCR gene rearrangement Vb7.1 Vb13.6 Vb13.6 Vb3 Vb8 Vb8 Vb 5.3 Vb 13.1 Vb 13.1 Diagnosis of T-LGL leukemia Clinical context Cytopenia (Neutropenia, anemia) Splenomegaly Lymphocytosis Autoimmune conditions (e.g. RA) BM biopsy IHC FC PB smear / Flow cytometry (FC) LGL < 500/uL phenotype LGL > 500/uL Phenotyping NK phenotype Differential diagnosis relevant to this case (CD4-CD8- ) Modified from: 1. Lamy T and Loughran T. Blood. 2011; 117(10): Steinway SN, Leblanc F and Loughran T. Blood Rev. 2014; 28(3):87 94 Clonality FC: KIR or V repertoire PCR: TCR gene FC: KIR 8
9 Peripheral T lymphocytes T cells >90% of T cells (CD4+ or CD8+) T cells % T cells in peripheral blood Rich in skin, mucosa, liver & spleen CD4-/CD8- (90%) A subset CD5- T-LGL leukemia 5% of T-LGL leukemia are + T-LGL leukemia CD8+ (60-70%) CD4-/CD8- (30-40%) Clinical features similar to T-LGL leukemia Bourgault Rouxel AS et al. Leuk Res. 2008; 32:45 48 Sandberg Y et al. Leukemia. 2006;20: CD4-/CD8- T-LGL leukemia Clinical, hematologic, morphologic features similar to but: Increased LGLs in PB rare (1/7) Inconspicuous granules common Red cell aplasia (2/7) and AIHA (3/7) may be more frequent Immunophenotype +, CD4-, CD8-, CD5-, +, TIA1+ (overlaps with HSTCL) Variable expression of CD56 and CD57 Cytogenetics/FISH negative for i7q. Chen et al. Am J Clin Pathol 2011; 136: T-LGL leukemia CD4-/CD8- (8 cases; 67%); CD8+ (4 cases; 33%) More likely to have rheumatoid arthritis Lower absolute neutrophil count Lower platelet count Similar overall survival compared to Yabe et al. Am J Clin Pathol 2015;144:




/CD7+/CD5 dim+ T")

10 HSTCL HSTCL HSTCL HSTCL Clinicopathologic Features of CD4-/CD8- and HSTCL Clinical findings Age/sex T-LGL leukemia, CD4-/CD8- Elderly M=F HSTCL Young adult & children M>F B symptoms, LDH Uncommon Common Hepatosplenomegaly Mild or moderate Marked Clinical course Indolent Highly aggressive Hematological findings Neutropenia/anemia Common, often severe Variable Thrombocytopenia Less common; often mild or moderate Common, often marked Chen YH. et. al. Am J Clin Pathol. 2012;137: T-LGL leukemia, HSTCL CD4-/CD8- Morphology Peripheral blood LGLs; no atypia Variable morphology; blastic cells may be present Bone marrow Interstitial/intrasinusoidal (single cell layer) Prominent intrasinusoidal component Immunophenotype T cell antigens +/CD4 /CD8 /CD7+/CD5 or +/CD4 /CD8( /+)/CD7+/CD5 dim+ T cell receptor CD56/CD57 ( /+)/(+/ ) Often +/ TIA 1/GrB/perforin +/(+/ )/+/ +/ / Molecular/Genetics i7q STAT3 mutation STAT5b mutation Negative 40% T LGL 2% T LGL Majority positive 9% 43% Modified from: Chen YH. et. al. Am J Clin Pathol. 2012;137:
 Reactive T cells may exhibit patterns of T cell antigen expression that mimic T-cell neoplasm!")
11 Expansion of reactive T cells in peripheral blood Reactive expansion of + CD4-CD8- T cells CD5 expression CD5-: 11/62 (18%) Partial CD5-: 4 (6%) Dim CD5+: 1 (2%) CD7 expression Dim CD7: 3 (5%) expression Brighter : 6/62 (10%) Reactive T cells may exhibit patterns of T cell antigen expression that mimic T-cell neoplasm! Associated clinical conditions Clinical conditions Study group Control group Infection/inflammatory 18/36 (50%) 8/39 (21%) disorders Autoimmune 9/36 (25%) 2/39 (5%) diseases Lymphoproliferative 6/36 (17%) 4/39 (10%) disorders Splenectomy 3/36 (8%) 1/39 (2%) Not identified 8/36 (22% 24/39 (62%) Roden AC et al. Arch Pathol Lab Med. 2008;132: (n=29) (60%) (n=7) (15%) Infection inflammation (n=5) (10%) Transplant Data from Northwestern Memorial Hospital, Chicago, IL (n=10) (21%) Others Associated conditions Hematopoietic neoplasm Infection inflammation Reactive expansion of + CD4-CD8- T cells No. of patients Clinical conditions 29 Mature B cell lymphoma/myeloma No. of patients 22 AML/B ALL 6 CML 1 7 HIV 4 Infectious mono 1 Hepatitis C 1 Sarcoidosis 1 Transplant 5 Stem cell 4 Solid organ 1 Others 10 ITP 3 Cyclic neutropenia 1 Chronic oral ulcer 1 Sickle cell disease 1 Unclear 4 Absolute increase in LGL Rare (1/47) CD5 expression CD5+: 27/48 (56%) CD5-: 21/48 (44%) A subset of normal T cells do not express CD5. Spour et. Al. Clin Exp Immunol. 1990;80: Roden AC et al. Arch Pathol Lab Med. 2008;132: Clinical context Cytopenia (Neutropenia, anemia) Splenomegaly Lymphocytosis Autoimmune conditions (e.g. RA) Diagnosis of T-LGL leukemia BM biopsy IHC FC Modified from: 1. Lamy T and Loughran T. Blood. 2011; 117(10): Steinway SN, Leblanc F and Loughran T. Blood Rev. 2014; 28(3):87 94 PB smear / Flow cytometry (FC) LGL < 500/uL phenotype LGL > 500/uL Phenotyping Clonality FC: KIR or V repertoire PCR: TCR gene NK phenotype FC: KIR Data from Northwestern Memorial Hospital, Chicago, IL 11
 harbor STAT3 mutations, resulting in activation of JAK/STAT pathway Constitutive activation of STAT3 is a")

12 Constitutive activation of STAT3 is a unifying feature of LGL leukemia Will new molecular findings help with diagnosis of T-LGL leukemia? 30 to 40% of patients with or chronic lymphoproliferative disorder of NK cells (CLPD-NK) harbor STAT3 mutations, resulting in activation of JAK/STAT pathway Constitutive activation of STAT3 is a unifying feature in all patients with LGL leukemia irrelevant to STAT3 mutation. Alternative mechanisms contribute to activation of JAK/STAT pathway: Elevated IL-6 contributing to STAT3 activation Down-regulated SOCS3 responsible for lack of negative feedback for STAT3 activation Koskela HLM et al. N Engl J Med. 2012; 366: Jerez A et al. Blood. 2012; 120: Teramo A. et al. Blood. 2013; 121(19): Others Will new molecular findings help? Molecular testing for STAT3 mutations: ~40% harbor STAT3 mutations Mutant Stat3 is predictive of earlier time to treatment failure STAT3 Y640F mutation may be associated with a favorable methotrexate response Activation of STAT3 (p-stat3) resulting in nuclear translocation Jerez A. et al. Blood Oct 11; 120(15): of Stat3 IHC for nuclear p-stat3? What we ve learned from this case discussion? CD4-/CD8- T-LGL leukemia is an indolent disease and shows clinical, hematological and morphologic features similar to common. A lower LGL count may be more common in this variant, and a diagnosis is often made on a bone marrow biopsy. CD4-/CD8- T-LGL leukemia demonstrate an immunophenotype overlapping with HSTCL. Awareness of this phenotypic variant is important for an accurate diagnosis, 12
13 Expansion of T-LGLs including T-LGLs occurs in various reactive conditions. Lack of CD5 expression in T cells does not necessarily indicates immunophenotypic aberrancy as a subset of normal T cells does not express CD5. About 40% of patients with harbor STAT3 mutations, but activation of Stat3 is a unifying feature of all. Demonstration of Stat3 activation may provide a useful tool in diagnosis and differential diagnosis of. 13
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
Leukocytosis - Some Learning Points
 Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228
 2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
SESSION 1 Reactive cytopenia and dysplasia
 SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
Hematopathology Specialty Conference Case #1
 Hematopathology Specialty Conference Case #1 Robert (Bob) Ohgami, MD, PhD Assistant Professor Stanford University Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships
Hematopathology Specialty Conference Case #1 Robert (Bob) Ohgami, MD, PhD Assistant Professor Stanford University Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Myelodysplastic Syndrome Case 158
 Myelodysplastic Syndrome Case 158 Dong Chen MD PhD Division of Hematopathology Mayo Clinic Clinical History 86 year old man Persistent borderline anemia and thrombocytopenia. His past medical history was
Myelodysplastic Syndrome Case 158 Dong Chen MD PhD Division of Hematopathology Mayo Clinic Clinical History 86 year old man Persistent borderline anemia and thrombocytopenia. His past medical history was
Case Reports. De Novo CD3 Negative Hepatosplenic T-cell Lymphoma. Diagnostic Challenges and Pitfalls
 Case Reports De Novo CD3 Negative Hepatosplenic T-cell Lymphoma Diagnostic Challenges and Pitfalls Lucy Harn Kapur, MD; Yasser Khaled, MD; Melhem Solh, MD; David Ward, DO; Chung-Che Chang, MD Hepatosplenic
Case Reports De Novo CD3 Negative Hepatosplenic T-cell Lymphoma Diagnostic Challenges and Pitfalls Lucy Harn Kapur, MD; Yasser Khaled, MD; Melhem Solh, MD; David Ward, DO; Chung-Che Chang, MD Hepatosplenic
Morphology Case Study. Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital
 Morphology Case Study Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital 41 year old male presented to GP for routine check-up in May 2011. FBC Results:
Morphology Case Study Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital 41 year old male presented to GP for routine check-up in May 2011. FBC Results:
Test Utilization: Chronic Lymphocytic Leukemia
 Test Utilization: Chronic Lymphocytic Leukemia Initial Evaluation Diagnostic Criteria Selection of Tests for Prognosis Response to Therapy Challenges Assessment for persistent disease Paul J. Kurtin, M.D.
Test Utilization: Chronic Lymphocytic Leukemia Initial Evaluation Diagnostic Criteria Selection of Tests for Prognosis Response to Therapy Challenges Assessment for persistent disease Paul J. Kurtin, M.D.
Extramedullary precursor T-lymphoblastic transformation of CML at presentation
 Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
ADx Bone Marrow Report. Patient Information Referring Physician Specimen Information
 ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
MDS 101. What is bone marrow? Myelodysplastic Syndrome: Let s build a definition. Dysplastic? Syndrome? 5/22/2014. What does bone marrow do?
 101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
The patient had a mild splenomegaly but no obvious lymph node enlargement. The consensus phenotype obtained from part one of the exercise was:
 Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Case Presentation No. 075
 Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls
 Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Patterns of Lymphoid Neoplasia in Peripheral Blood. Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure
 Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
GP CME. James Liang Consultant Haematologist. Created by: Date:
 GP CME James Liang Consultant Haematologist Date: Created by: Scenario 52 year old European male Fit and well Brother recently diagnosed with diabetes PMHx Nil Social Hx Ex-smoker stopped 5 years ago (20
GP CME James Liang Consultant Haematologist Date: Created by: Scenario 52 year old European male Fit and well Brother recently diagnosed with diabetes PMHx Nil Social Hx Ex-smoker stopped 5 years ago (20
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
CASE 106. Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation
 CASE 106 Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation Gabriel C. Caponetti, MD University of Pennsylvania, US Clinical history 69, F peripheral neuropathy, refractory
CASE 106 Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation Gabriel C. Caponetti, MD University of Pennsylvania, US Clinical history 69, F peripheral neuropathy, refractory
Hematopathology Case Study
 www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
MYELODYSPLASTIC SYNDROMES
 MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
Supervisor: Prof. Dr. P Vandenberghe Dr. C Brusselmans
 Contribution of molecular diagnosis in eosinophilia/hypereosinophilia Eosinophilia Hypereosinophilia Hypereosinophilic syndrome Immune mediated hypereosinophilia Chronic eosinophilic leukemia (NOS)/ Idiopathic
Contribution of molecular diagnosis in eosinophilia/hypereosinophilia Eosinophilia Hypereosinophilia Hypereosinophilic syndrome Immune mediated hypereosinophilia Chronic eosinophilic leukemia (NOS)/ Idiopathic
74y old Female with chronic elevation of Platelet count. August 18, 2005 Faizi Ali, MD Hematopathology Fellow
 74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
Tel: Fax: Received: 25, Jul, 2014 Accepted: 16, Dec, 2014
 IJHOSCR International Journal of Hematology- Oncology and Stem Cell Research Original Article T-cell/Natural killer-cell neoplasms presenting as leukemia- Case series from single tertiary care center Shano
IJHOSCR International Journal of Hematology- Oncology and Stem Cell Research Original Article T-cell/Natural killer-cell neoplasms presenting as leukemia- Case series from single tertiary care center Shano
Case Presentation. Attilio Orazi, MD
 Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Persistent lymphocytosis. Persistent lymphocytosis: are there prognostic indicators? Problem. Questions. Basic markers used to identify lymphocytes
 Persistent lymphocytosis Persistent lymphocytosis: are there prognostic indicators? Paul R. Avery VMD, PhD, DACVP Marjorie Williams, DVM Anne C. Avery VMD, PhD Clinical Immunology Laboratory Colorado State
Persistent lymphocytosis Persistent lymphocytosis: are there prognostic indicators? Paul R. Avery VMD, PhD, DACVP Marjorie Williams, DVM Anne C. Avery VMD, PhD Clinical Immunology Laboratory Colorado State
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms
 & Myeloproliferative neoplasms") Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017
 MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017") LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
Ordering Physician CLIENT,CLIENT. Collected REVISED REPORT
 HPWET Hematopathology Consultation, MML Embed Client Hematopathology Consult REVISED INAL DIAGNOSIS Interpretation Peripheral blood, bone marrow aspirate and biopsies, bilateral iliac crests: 1. Normocellular
HPWET Hematopathology Consultation, MML Embed Client Hematopathology Consult REVISED INAL DIAGNOSIS Interpretation Peripheral blood, bone marrow aspirate and biopsies, bilateral iliac crests: 1. Normocellular
Follicular Lymphoma: the WHO
 Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
Hematopathology Case Study
 Hematopathology Case Study AMP Outreach Course 2009 AMP Annual Meeting John Greg Howe Ph.D. Department of Laboratory Medicine Yale University School of Medicine November 19, 2009 HISTORY Case History An
Hematopathology Case Study AMP Outreach Course 2009 AMP Annual Meeting John Greg Howe Ph.D. Department of Laboratory Medicine Yale University School of Medicine November 19, 2009 HISTORY Case History An
Hematology: Challenging Cases with Your Participation COPYRIGHT
 Hematology: Challenging Cases with Your Participation Reed E. Drews, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Question 1 Question 1 64-year-old man is evaluated during
Hematology: Challenging Cases with Your Participation Reed E. Drews, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Question 1 Question 1 64-year-old man is evaluated during
Diagnostic Approach for Eosinophilia and Mastocytosis. Curtis A. Hanson, M.D.
 Diagnostic Approach for Eosinophilia and Mastocytosis Curtis A. Hanson, M.D. 2014 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2014 MFMER slide-2 Molecular Classification
Diagnostic Approach for Eosinophilia and Mastocytosis Curtis A. Hanson, M.D. 2014 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2014 MFMER slide-2 Molecular Classification
ACCME/Disclosures. History. Hematopathology Specialty Conference Case #4 4/13/2016
 Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and
 Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Does Morphology Matter in 2017
 Does Morphology Matter in 2017 ISLH May 2017 Kathryn Foucar Distinguished Professor Emerita kfoucar@salud.unm.edu Objectives Recognize unique RBC and WBC abnormalities in non-neoplastic disorders Learn
Does Morphology Matter in 2017 ISLH May 2017 Kathryn Foucar Distinguished Professor Emerita kfoucar@salud.unm.edu Objectives Recognize unique RBC and WBC abnormalities in non-neoplastic disorders Learn
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi
.ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi") Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
The function of the bone marrow. Living with Aplastic Anemia. A Case Study - I. Hypocellular bone marrow failure 5/14/2018
 The function of the bone marrow Larry D. Cripe, MD Indiana University Simon Cancer Center Bone Marrow Stem Cells Mature into Blood Cells Mature Blood Cells and Health Type Function Term Red Cells Carry
The function of the bone marrow Larry D. Cripe, MD Indiana University Simon Cancer Center Bone Marrow Stem Cells Mature into Blood Cells Mature Blood Cells and Health Type Function Term Red Cells Carry
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms. Daniel A. Arber, MD Stanford University
 Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89
 Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Case Report Two distinct types of clinical characteristics and therapies for T-cell large granular lymphocyte leukemia: a report of seven cases
 Int J Clin Exp Med 2016;9(6):12301-12307 www.ijcem.com /ISSN:1940-5901/IJCEM0022566 Case Report Two distinct types of clinical characteristics and therapies for T-cell large granular lymphocyte leukemia:
Int J Clin Exp Med 2016;9(6):12301-12307 www.ijcem.com /ISSN:1940-5901/IJCEM0022566 Case Report Two distinct types of clinical characteristics and therapies for T-cell large granular lymphocyte leukemia:
6 yr old MC labrador retriever. Peripheral Neutropenia and Occult Lymphoproliferative Disorders. 6 yr old MC labrador retriever.
 Peripheral Neutropenia and Occult Lymphoproliferative Disorders Paul R. Avery VMD, PhD, DACVP Melanie S. Spoor Laurie Bohannon-Worsley Lauren C. Taraba Matthew D. Jones Anne C. Avery VMD, PhD Colorado
Peripheral Neutropenia and Occult Lymphoproliferative Disorders Paul R. Avery VMD, PhD, DACVP Melanie S. Spoor Laurie Bohannon-Worsley Lauren C. Taraba Matthew D. Jones Anne C. Avery VMD, PhD Colorado
Case Report Blasts-more than meets the eye: evaluation of post-induction day 21 bone marrow in CBFB rearranged acute leukemia
 Int J Clin Exp Pathol 2014;7(7):4498-4502 www.ijcep.com /ISSN:1936-2625/IJCEP0000851 Case Report Blasts-more than meets the eye: evaluation of post-induction day 21 bone marrow in CBFB rearranged acute
Int J Clin Exp Pathol 2014;7(7):4498-4502 www.ijcep.com /ISSN:1936-2625/IJCEP0000851 Case Report Blasts-more than meets the eye: evaluation of post-induction day 21 bone marrow in CBFB rearranged acute
HEMATOPATHOLOGY SUMMARY REPORT RL;MMR;
 HEMATOPATHOLOGY SUMMARY REPORT RL;MMR; Page 1 of 1 05/15/20XX HP000000-20XX 05/21/20XX (212) 123-457 (51) 32-3455 (51) 123-457 Age: 78 DOB: 0/05/19XX SS#: 45-45-45 Clinical Information: 78 y/o female with
HEMATOPATHOLOGY SUMMARY REPORT RL;MMR; Page 1 of 1 05/15/20XX HP000000-20XX 05/21/20XX (212) 123-457 (51) 32-3455 (51) 123-457 Age: 78 DOB: 0/05/19XX SS#: 45-45-45 Clinical Information: 78 y/o female with
Hematology 101. Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD
 Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Hemophagocytic Lymphohistiocytosis Secondary to T cell/histiocyte-rich Large B-cell Lymphoma
 Hemophagocytic Lymphohistiocytosis Secondary to T cell/histiocyte-rich Large B-cell Lymphoma Katherine Devitt, M.D., Benjamin Chen, M.D., Ph.D., Hongbo Yu, M.D., Ph.D., Bruce Woda, M.D. 1 1 Department
Hemophagocytic Lymphohistiocytosis Secondary to T cell/histiocyte-rich Large B-cell Lymphoma Katherine Devitt, M.D., Benjamin Chen, M.D., Ph.D., Hongbo Yu, M.D., Ph.D., Bruce Woda, M.D. 1 1 Department
Welcome to Master Class for Oncologists. Session 3: 9:15 AM - 10:00 AM
 Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Borderline cytopenias. Dr Taku Sugai Consultant Haematologist
 Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
CD4-Positive T-Cell Large Granular Lymphocytosis Mimicking Sézary Syndrome in a Patient With Mycosis Fungoides
 Case Report CD4-Positive T-Cell Large Granular Lymphocytosis Mimicking Sézary Syndrome in a Patient With Mycosis Fungoides Ling Zhang, MD, Magali Van den Bergh, MD, and Lubomir Sokol, MD, PhD Summary:
Case Report CD4-Positive T-Cell Large Granular Lymphocytosis Mimicking Sézary Syndrome in a Patient With Mycosis Fungoides Ling Zhang, MD, Magali Van den Bergh, MD, and Lubomir Sokol, MD, PhD Summary:
5000 International Clinical Cytometry Society: Practical Flow Cytometry in Hematopathology A Case-Based Approach
 5000 International Clinical Cytometry Society: Practical Flow Cytometry in Hematopathology A Case-Based Approach Joseph A DiGiuseppe, MD, PhD Hartford Hospital Disclosures In the past 12 months, I have
5000 International Clinical Cytometry Society: Practical Flow Cytometry in Hematopathology A Case-Based Approach Joseph A DiGiuseppe, MD, PhD Hartford Hospital Disclosures In the past 12 months, I have
JMSCR Vol. 03 Issue 06 Page June 2015
 www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x An Indolent Natural Killer Cell Leukemia Presenting with Bilateral Ankle Arthritis and Low Grade Fever Abstract Author Subhash Chandra
www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x An Indolent Natural Killer Cell Leukemia Presenting with Bilateral Ankle Arthritis and Low Grade Fever Abstract Author Subhash Chandra
Anemia (3).ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh
.ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh") Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
Case #16: Diagnosis. T-Lymphoblastic lymphoma. But wait, there s more... A few weeks later the cytogenetics came back...
 Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
Juvenile Myelomonocytic Leukemia (JMML)
") Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
T CELL LYMPHOMA ANALYSIS
 T CELL LYMPHOMA ANALYSIS Charles Goolsby, Ph.D. Floyd E. Patterson Research Professor of Pathology Northwestern Feinberg School of Medicine c-goolsby@northwestern.edu 1 T CELL LYMPHOMA ANALYSIS Diverse
T CELL LYMPHOMA ANALYSIS Charles Goolsby, Ph.D. Floyd E. Patterson Research Professor of Pathology Northwestern Feinberg School of Medicine c-goolsby@northwestern.edu 1 T CELL LYMPHOMA ANALYSIS Diverse
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms. Curtis A. Hanson, MD
 Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Western Health Specialist Clinics Access & Referral Guidelines
 Haematology Specialist Clinics at Western Health: Western Health runs MBS funded Specialist Clinics on a Wednesday and Thursday afternoon at its Sunshine Hospital site for patients who require assessment
Haematology Specialist Clinics at Western Health: Western Health runs MBS funded Specialist Clinics on a Wednesday and Thursday afternoon at its Sunshine Hospital site for patients who require assessment
Complete Blood Count PSI AP Biology
 Complete Blood Count PSI AP Biology Name: Objective Students will examine how the immunological response affects molecules in the blood. Students will analyze three complete blood counts and create diagnoses
Complete Blood Count PSI AP Biology Name: Objective Students will examine how the immunological response affects molecules in the blood. Students will analyze three complete blood counts and create diagnoses
The spectrum of flow cytometry of the bone marrow
 The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
accumulation the blood, marrow, lymph nodes, and spleen.
 Chronic Lymphocytic Leukemia accumulation of mature-appearing appearing lymphocytes in the blood, marrow, lymph nodes, and spleen. CLL cells are: monoclonal l B lymphocytes that express CD19. CD5, and
Chronic Lymphocytic Leukemia accumulation of mature-appearing appearing lymphocytes in the blood, marrow, lymph nodes, and spleen. CLL cells are: monoclonal l B lymphocytes that express CD19. CD5, and
Autoimmunity in CLL. Anne Silva, MD Hematology Fellows Conference
 Autoimmunity in CLL Anne Silva, MD Hematology Fellows Conference Case Presentation Mr. M is a 62 year old male with multiple medical problems including pulmonary sarcoidosis on steroids, was incidentally
Autoimmunity in CLL Anne Silva, MD Hematology Fellows Conference Case Presentation Mr. M is a 62 year old male with multiple medical problems including pulmonary sarcoidosis on steroids, was incidentally
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
Myelodysplastic Syndrome: Let s build a definition
 1 MDS: Diagnosis and Treatment Update Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian Hospital Myelodysplastic
1 MDS: Diagnosis and Treatment Update Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian Hospital Myelodysplastic
MDS: Who gets it and how is it diagnosed?
 MDS: Who gets it and how is it diagnosed? October 16, 2010 Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian
MDS: Who gets it and how is it diagnosed? October 16, 2010 Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian
Collect and label sample according to standard protocols. Gently invert tube 8-10 times immediately after draw. DO NOT SHAKE. Do not centrifuge.
 Complete Blood Count CPT Code: CBC with Differential: 85025 CBC without Differential: 85027 Order Code: CBC with Differential: C915 Includes: White blood cell, Red blood cell, Hematocrit, Hemoglobin, MCV,
Complete Blood Count CPT Code: CBC with Differential: 85025 CBC without Differential: 85027 Order Code: CBC with Differential: C915 Includes: White blood cell, Red blood cell, Hematocrit, Hemoglobin, MCV,
Acute Myeloid Leukemia with RUNX1 and Several Co-mutations
 Case SH2017-0281 Acute Myeloid Leukemia with RUNX1 and Several Co-mutations James Bauer, MD, PhD David Yang, MD Erik Ranheim, MD, PhD Catherine Leith, MB, Bchir Clinical History Chief Complaint: 72 year
Case SH2017-0281 Acute Myeloid Leukemia with RUNX1 and Several Co-mutations James Bauer, MD, PhD David Yang, MD Erik Ranheim, MD, PhD Catherine Leith, MB, Bchir Clinical History Chief Complaint: 72 year
Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data
 Post-HCT Data") Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED
 Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Diseases Of The Blood
 Diseases Of The Blood DR. Associate Professor Of Pathology Faculty Of Medicine Ain Shams University Red Blood Cells and Anemia RBC=4-6 million/mm 2 Hb=12-18 g/dl Oxygen Carrying Molecule Hemoglobin Tetramer:
Diseases Of The Blood DR. Associate Professor Of Pathology Faculty Of Medicine Ain Shams University Red Blood Cells and Anemia RBC=4-6 million/mm 2 Hb=12-18 g/dl Oxygen Carrying Molecule Hemoglobin Tetramer:
Donor-Derived T-Cell Large Granular Lymphocytic Leukemia in a Patient With Peripheral T-Cell Lymphoma
 Molecular Insights in Patient Care 939 Donor-Derived T-Cell Large Granular Lymphocytic Leukemia in a Patient With Peripheral T-Cell Lymphoma Juliana E. Hidalgo Lopez, MD a,* ; Mariko Yabe, MD, PhD a,*
Molecular Insights in Patient Care 939 Donor-Derived T-Cell Large Granular Lymphocytic Leukemia in a Patient With Peripheral T-Cell Lymphoma Juliana E. Hidalgo Lopez, MD a,* ; Mariko Yabe, MD, PhD a,*
Hematology 101. Rachid Baz, M.D. 5/16/2014
 Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Large granular lymphocytic leukaemia
 MEDISIN OG VITENSKAP Medisin og vitenskap Original article Original article Large granular lymphocytic leukaemia Abstract Background. Large granular lymphocytic leukaemia (LGL-leukaemia) is a rare disease.
MEDISIN OG VITENSKAP Medisin og vitenskap Original article Original article Large granular lymphocytic leukaemia Abstract Background. Large granular lymphocytic leukaemia (LGL-leukaemia) is a rare disease.
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the author to give readers additional information about his work. Supplement to: Olnes MJ, Scheinberg P, Calvo KR, et al. Eltrombopag and improved
Supplementary Appendix This appendix has been provided by the author to give readers additional information about his work. Supplement to: Olnes MJ, Scheinberg P, Calvo KR, et al. Eltrombopag and improved
Bone marrow T-cell infiltrates in viral infections and autoimmune diseases Alexander Tzankov
 Bone marrow T-cell infiltrates in viral infections and autoimmune diseases Alexander Tzankov Institute of Pathology, University Hospital Basel Bone marrow T-cell infiltrates Physiological roles of mature
Bone marrow T-cell infiltrates in viral infections and autoimmune diseases Alexander Tzankov Institute of Pathology, University Hospital Basel Bone marrow T-cell infiltrates Physiological roles of mature
Flow cytometric analysis of B-cell lymphoproliferative disorders
 Flow cytometric analysis of B-cell lymphoproliferative disorders David M. Dorfman, M.D., Ph.D. Department of Pathology Brigham and Women s Hospital and Harvard Medical School Boston, MA Objectives Review
Flow cytometric analysis of B-cell lymphoproliferative disorders David M. Dorfman, M.D., Ph.D. Department of Pathology Brigham and Women s Hospital and Harvard Medical School Boston, MA Objectives Review
Spontaneous Regression of Methotrexate-related Lymphoproliferative Disorder with T-cell Large Granular Lymphocytosis
 CASE REPORT Spontaneous Regression of Methotrexate-related Lymphoproliferative Disorder with T-cell Large Granular Lymphocytosis Hiroshi Ureshino 1, Chiho Kadota 1, Kazuya Kurogi 1, Masaharu Miyahara 1
CASE REPORT Spontaneous Regression of Methotrexate-related Lymphoproliferative Disorder with T-cell Large Granular Lymphocytosis Hiroshi Ureshino 1, Chiho Kadota 1, Kazuya Kurogi 1, Masaharu Miyahara 1
Platelet and WBC disorders
 Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
APPROACHING TO PANCYTOPENIA
 APPROACHING TO PANCYTOPENIA P A T C H A R E E K O M V I L A I S A K, M. D. A S S I S T A N T P R O F E S S O R D I V I S I O N O F P E D I A T R I C H E M A T O L O G Y O N C O L O G Y, D E P A R T M E
APPROACHING TO PANCYTOPENIA P A T C H A R E E K O M V I L A I S A K, M. D. A S S I S T A N T P R O F E S S O R D I V I S I O N O F P E D I A T R I C H E M A T O L O G Y O N C O L O G Y, D E P A R T M E
Chronic Idiopathic Myelofibrosis (CIMF)
") Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
This was a multicenter study conducted at 11 sites in the United States and 11 sites in Europe.
 Protocol CAM211: A Phase II Study of Campath-1H (CAMPATH ) in Patients with B- Cell Chronic Lymphocytic Leukemia who have Received an Alkylating Agent and Failed Fludarabine Therapy These results are supplied
Protocol CAM211: A Phase II Study of Campath-1H (CAMPATH ) in Patients with B- Cell Chronic Lymphocytic Leukemia who have Received an Alkylating Agent and Failed Fludarabine Therapy These results are supplied
88-year-old Female with Lymphadenopathy. Faizi Ali, MD
 88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
Case 3. Ann T. Moriarty,MD
 Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Myelodysplastic Syndromes Myeloproliferative Disorders
 Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
One Day BMT Course by Thai Society of Hematology. Management of Graft Failure and Relapsed Diseases
 One Day BMT Course by Thai Society of Hematology Management of Graft Failure and Relapsed Diseases Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital
One Day BMT Course by Thai Society of Hematology Management of Graft Failure and Relapsed Diseases Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital
Adult Acute leukemia. Matthew Seftel. August
 Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
All Wales Lymphoma Panel Lymphoma Course April 2015 Wales Millennium Centre Cardiff
 All Wales Lymphoma Panel Lymphoma Course 23-24 April 2015 Wales Millennium Centre Cardiff Case Histories Online slides at: http://dental.uwcm.ac.uk:82/awlp%20course%202015/view.apml? Professor Sebastian
All Wales Lymphoma Panel Lymphoma Course 23-24 April 2015 Wales Millennium Centre Cardiff Case Histories Online slides at: http://dental.uwcm.ac.uk:82/awlp%20course%202015/view.apml? Professor Sebastian
Anemia. A case-based approach. David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017
 Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
CHALLENGING CASES PRESENTATION
 CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish