Melanoma 6/2/2011. Classification and Prognosis. Melanoma Statistics. American Cancer Society
|
|
|
- Tabitha Rogers
- 5 years ago
- Views:
Transcription

.")
1 University of Pennsylvania, Ben Franklin in front of Charles Addams Building Melanoma Classification and Prognosis Emphasizing Pathology & History David Elder University of Pennsylvania Melanoma Statistics American Cancer Society Cancer of the skin is by far the most common of all cancers. Melanoma accounts for less than 5% of skin cancer cases but causes a large majority of skin cancer deaths. About 70,000 new melanomas are diagnosed in the United States per year (about 40,000 in men and 30,000 in women). About 9,000 people in the US may be expected to die of melanoma per year (about 6,000 men and 3,000 women). (Compare with ~ 2,500 for SCC). The death rate has dropped since the 1990s for those younger than 50, but has been stable or rising in older age groups. 1
 for blacks, and 0.5% (1 in 200) for Hispanics.")
2 Melanoma Statistics - 2 American Cancer Society Incidence rates for melanoma have been rising for at least 30 years. The lifetime risk of getting melanoma is about 2% (1 in 50) for whites, 0.1% (1 in 1,000) for blacks, and 0.5% (1 in 200) for Hispanics. The risk for each person is affected by a number of different factors, including sun susceptibility and exposure, nevi, freckles, family and personal history of melanoma Melanoma occurs in younger as well as older people. Rates increase with age, with the highest incidence at age 85, but melanoma is one of the more common cancers in young adults, and occurs in teenagers. Melanoma and Nevi Nevi are important mainly in relation to melanoma, most importantly as simulants but also as risk markers and, occasionally, as precursors. Although some melanomas may arise in a pre-existing benign nevus, the general tendency in nevi is to regress over time. Nevi and especially dysplastic nevi are among the strongest markers of individuals at increased risk for developing melanoma over time. Nevi are also the most important simulants of melanoma, both clinically and histologically. Gross Pathology of Tumor Progression Compartments (SSM) in Melanoma Junctional Nevus Compound Nevus Dysplastic Nevus RGP RGP+VGP RGP+VGP 6 2


3 ABCDE s of Melanoma A = Asymmetry one half not like the other B = Border irregularity like the map of a small island C = Color variegation shades of tan, brown, black, red, white, blue-gray D = Diameter no lower limit today E = Elevation, and Evolution Ugly duckling a mole out of step with the others Tumorigenic & Nontumorigenic melanoma (Radial & Vertical Growth Phase) ABCD Criteria for RGP Asymmetry Border irregularity Color variegation Diameter > 4-6 mm Vertical Growth Phase balloon-like expansion forms nodule often symmetrical, smooth borders color is often quite uniform diameter often less than 6 mm 9 3
 Metastatic Melanoma As for VGP, capable of metastasis.")

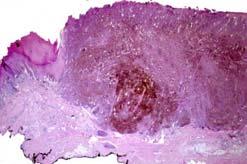
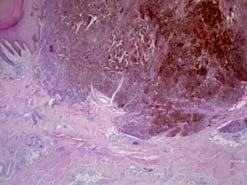
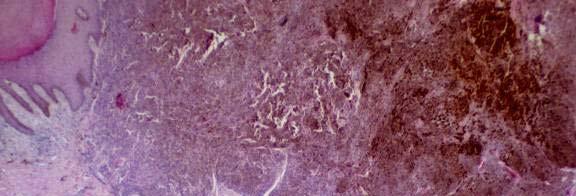
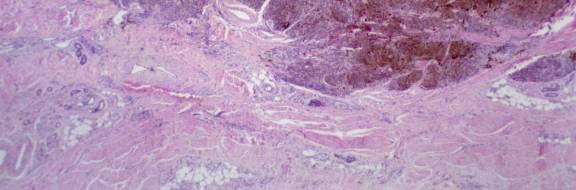
4 Tumor Progression in Melanoma RGP Radial Growth Phase In situ or invasive but nontumorigenic, rarely forms permanent cell lines, does not metastasize Vertical Growth Phase Tumorigenic, forms permanent cell lines. Source of metastatic disease (cytogenetic evidence) Metastatic Melanoma As for VGP, capable of metastasis. VGP Prognosis of Primary Melanoma Clark s levels, Breslow thickness, Ulceration, Mitogenicity, TNM Stage Evidence is presented suggesting that superficial spreading melanoma and lentigo maligna melanoma though evolving at different rates, show a long gperiod of superficial growth, followed by the relatively rapid appearance of nodules or deeper invasion within the primary lesion. This change in the nature of the primary lesion may be due to the appearance of one or more strains of cells of aggressive biologic potential. The subdivision of each of the forms of melanoma into 5 anatomic levels of invasion permits the accurate assignment of prognosis to each case. 4




. Nodal disease may be microscopic, i.e. non-palpable disease detected in sentinel node procedure, or macroscopic, i.")
5 Breslow s Thickness "One possible reason for the lack of reliability of tumor size in estimating prognosis may be that studies to date have considered size in only two dimensions and have neglected tumor volume". "From a retrospective study of 98 invasive i melanomas it was found that both tumor thickness and stage of invasion are of value in determining prognosis. By using these two criteria it was possible to identify a group of 45 patients only one of whom developed recurrent or metastatic disease. These criteria may be of value in selecting patients for prophylactic lymph node dissection." 14 7 th Edition of Melanoma Staging AJCC/UICC Balch et al, 2009 T Stages of primary tumors are based on Breslow s thickness intervals Mitogenicity is an independent factor and a rate >1 is a modifier of stage T1 Ulceration is a modifier of all T stages (T1b-T4b). Nodal disease may be microscopic, i.e. non-palpable disease detected in sentinel node procedure, or macroscopic, i.e. palpable. Cutaneous, nodal and distant metastases have increasingly worse prognosis. 5
6 In patients with localized melanoma, tumor thickness, mitogenicity and ulceration are the most dominant prognostic factors 16 Mitotic rate has replaced Clark Level IV for defining T1b melanomas. MALIGNANT MELANOMAS AND RELATED LESIONS Radial Growth Phase Variants Radial Growth Phase Absent Nodular melanoma (VGP present, RGP absent) Radial Growth Phase Present (with or without VGP) Superficial spreading melanoma Lentigo maligna melanoma Acral-lentiginous melanoma Mucosal-lentiginous melanoma Vertical growth phase variants MALIGNANT MELANOMAS AND RELATED LESIONS Vertical Growth Phase Variants Nodular Melanoma Desmoplastic melanoma Neurotropic melanoma Neurotropic melanoma Malignant blue nevus Melanoma in congenital nevi Minimal deviation melanoma Clear cell sarcoma Malignant melanocytic schwannoma Melanocytic tumor of uncertain malignant potential (MELTUMP) 6
 Chronic continuous exposure Acral (5%) No sun exposure Melanoma Classification Reasons to")


7 Histogenetic Subtypes Superficial Spreading (80%) Intermittent sun exposure Lentigo maligna (10%) Chronic continuous exposure Acral (5%) No sun exposure Melanoma Classification Reasons to Classify All melanomas are not the same Morphological variation affects diagnostic criteria nosologic differences Although no differences in prognostic outcome when other variables are controlled, there are differences in local progression and recurrence Different forms of melanoma have different etiologic and genetic basis, and targeted therapy needs to be tailored to these differences. 7




8 Nodular Melanoma Clinical Features Detectable RGP is absent by definition Tumorigenic melanoma without an adjacent nontumorigenic component short-lived RGP may be obliterated by the developing tumor. ABCD criteria i may not apply lesions are often symmetrical nodules/papules with raised discrete borders, fairly uniform color, diameter not always > 6 mm prognosis is similar to other melanomas when level and thickness are controlled Nodular Melanoma Histologic Features Diagnosis may be tricky especially if there is no highgrade atypia may be quite symmetrical at scanning magnification, but pigmentation and cytology generally vary from side to side. uniform cytologic atypia and mitotic activity in dermis maturation from top to bottom usually absent or imperfect no adjacent radial growth phase by definition epithelial involvement above the tumor may be subtle differential diagnosis includes epidermotropic metastatic melanoma Differential diagnosis includes benign lesions such as atypical compound nevi, Spitz nevi, deep penetrating nevi, cellular blue nevi Nodular Melanoma 8



9 Nodular melanoma Nodular Melanoma Rate of growth in melanomas: characteristics and associations of rapidly growing melanomas. Liu W, Dowling JP, Murray WK, McArthur GA, Thompson JF, Wolfe R, Kelly JW. Arch Dermatol Rapidly growing melanomas were more often symmetrical, elevated, amelanotic, regular in border, and symptomatic, occurred more frequently in elderly men and individuals with fewer nevi and fewer freckles Early detection of thick melanomas in the United States: beware of the nodular subtype. Demierre MF, Chung C, Miller DR, Geller AC. Arch Dermatol Nodular melanoma comprised 9% of all recorded cases but 34% of melanomas 2 mm or larger. A substantial number of thick melanomas in the United States are of the nodular subtype, and median thickness of nodular melanoma has not changed during the 12 years of study. New strategies are needed to decrease the incidence of thick melanoma in the United States. Superficial Spreading Melanoma Clinical Features 70% of all melanoma cases (common melanoma) occurs on usually covered, intermittently exposed skin relatively young adults median yrs of age classic ABCD lesions Asymmetry, Border irregularity, Color variegation, Diameter > 4 mm) highly associated with usual risk factors for melanoma: Dysplastic nevi, total nevi, large nevi, sun exposure habits, sun susceptibility, freckles, family or personal history of melanoma More likely than LMM, ALM or MLM to be associated with mutations of the oncogene BRAF 9

")
, usually high-level")



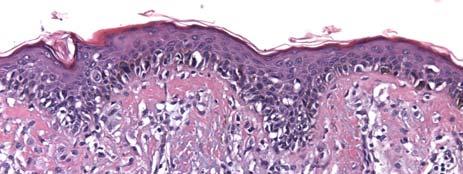
10 Superficial Spreading Melanoma SSM Asymmetry Border irregularity Color variegation Diameter > 4 mm Discrete border Superficial Spreading Melanoma Histologic Features Pagetoid Melanoma (McGovern) essential features of radial growth phase: pagetoid melanocytic proliferation (PMP), usually high-level and extensive breadth, asymmetry, poor circumscription, irregular epithelial hyperplasia uniform moderate to severe atypia, mitoses in about 1/3 invasion without tumor formation ( microinvasive melanoma ) may progress to tumorigenic vertical growth phase melanoma morphology of VGP is similar to nodular and other melanomas 10







11 Lentigo Maligna Melanoma Clinical Features about 10% of all melanoma A lentiginous melanoma occurs on chronically exposed skin especially head and neck elderly population risk for LMM may be increased in outdoor workers slow evolution over many years ABCD criteria are ultimately fulfilled by most evolving lesions border is illdefined and impalpable shades of tan, brown, black, fine reticulated lines within lesion vertical growth phase may develop as exophytic nodule or as endophytic tumor 11






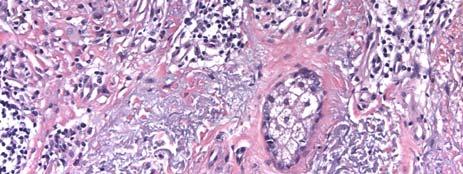
12 Lentigo Maligna Melanoma Histologic Features Lentiginous (basal) melanocytic proliferation pattern mainly near dermal-epidermal junction relatively small cell type nevoid to small epithelioid cells uniformly atypical melanocytes in contiguity with one another continuous proliferation (extends between rete ridges) nested and pagetoid melanocytic proliferation are less prominent nests hang down from interface in droplet pattern, nests above elastotic dermis changes at periphery may be very subtle definition of margin issues Sun-damaged skin elastosis is usually severe, may be associated actinic lentigines epidermis tends to be atrophic, rete ridges are effaced Final common pathway in center of advanced lesions: pagetoid proliferation, epithelial hyperplasia, larger cell type Desmoplastic and/or neurotropic VGP should be considered especially when predominantly spindle cells Lentigo Maligna Melanoma in Situ Illdefined border Lentiginous proliferation 12




13 Lentigo Maligna Melanoma in Situ Epidermal atrophy Lentiginous proliferation Usually also slight pagetoid proliferation Skin appendage extension Actinic elastosis Acral-lentiginous Melanoma Palms, soles, subungual Great toe region most common Incidence similar in all races, thus most common form of melanoma in African, and Asian populations May be deceptively thick even in absence of a raised nodule 13






14 14

 Continuous basal")




15 Acral-lentiginous Melanoma Lentiginous nontumorigenic compartment (radial growth phase) Continuous basal proliferation of uniformly atypical melanocytes Often a spindle cell tumorigenic compartment (vertical growth phase) May be deceptively thick even in absence of a raised nodule Tumorigenic component often desmoplastic and/or neurotropic (local recurrence risk) 15


16 Recurrent melanoma at site of prior biopsy 16




17 Histomorphological signature of mutation status in melanoma Simple histomorphological features and patient characteristics were correlated to the mutation status of BRAF and NRAS in a cohort of 302 primary cutaneous melanomas. Univariate analysis showed positive associations with multiple factors BRAF mutation associated with nesting, scatter, absent chronic solar damage (CSD), young patient age, sharp circumscription, large cell size, heavy pigmentation, truncal location, round cell and nuclear shape, SSM subtype, large nuclear size, little solar elastosis, and a thickened or hyperplastic epidermal contour. Multivariate and prediction analysis showed that a combination of high nesting and scatter, low age, and large cell size predicted BRAF mutation with an error estimate of 13%. Amaya Viros, Jane Fridlyand, Juergen Bauer, John Curtin, Daniel Pinkel, Boris C. Bastian. PLOS Medicine 5: ,


18 BRAF NRAS BRAF NRAS Neither Viros et al,
19 Curing Advanced Disease 70% of Melanomas have activated BRAF oncogene which drives progression Davies et al, Plexxikon Company developed a designer drug that inhibits common V600E mutation that activates BRAF Phase I and II trials of Plexxikon 4032 has been completed. MAP Kinase Pathway in Melanoma Growth Factors (e.g. bfgf) GRB2 SOS RAS GDP N-RAS GTP B-Raf MEK ERK ELK Cdk4 Cyclin D Proliferation Signals MAP Kinase Pathway in Melanoma Growth Factors (e.g. bfgf) GRB2 SOS RAS GDP N-RAS GTP B-Raf MEK ERK ELK Cdk4 Cyclin D Proliferation Signals 19

 The targeted-therapy revolution in oncology could be coming to melanoma, especially if the results of a phase 1 trial of an")


20 Update on PLX4032 phase I trial Keith Flaherty et al, U Penn Similar results with c-kit inhibiters e.g. Gleevec in patients with c-kit mutations A paradigm shift for melanoma therapy From HYPERLINK " Medical News ASCO 2009: Investigational Targeted Therapy for Metastatic Melanoma Shrinks Tumors, Causes Stir at Meeting June 4, 2009 (Orlando, Florida) The targeted-therapy revolution in oncology could be coming to melanoma, especially if the results of a phase 1 trial of an investigational agent are followed by similar results in subsequent trials, according to melanoma experts attending the American Society of Clinical Oncology 45th Annual Meeting. In a dose-escalation, proof-of-concept study, more than half of metastatic melanoma patients with this BRAF mutation who received high doses of PLX4032 had tumor shrinkage, said lead study author Keith T. Flaherty, MD, from the Abramson Cancer Center of the University of Pennsylvania in Philadelphia. "We are on the verge of a paradigm shift for melanoma therapy," said melanoma expert Boris Bastian, MD, from the University of California at San Francisco, who was not involved in the trial. "This is a decisive step toward personalized medicine," he added. 20
21 A Drug Trial Cycle: Recovery, Relapse, Reinvention The New York Times Feb In the weeks leading up to the annual oncologists conference here, several of the patients on the trial of the drug known as PLX4032 had relapsed. One had died. Another, Christopher Nelson, who had made what seemed like a miraculous recovery in March, had lost his appetite again. Dr. Flaherty feared what he might see on Mr. Nelson s scan when he returned to his office at the University of Pennsylvania. The drug s ability to stop the melanoma, on average, he told the crowd, appears to be approximately six months. Summary Early melanoma is curable by simple surgery (complete local excision) Advanced melanoma is not yet curable, but for the first time drugs are available that elicit responses in most eligible patients. Therapy depends on the presence of mutations appropriate for the targeted therapeutic agents personalized medicine. Surgical Pathology Cancer Case Summary y( (Checklist) MELANOMA OF THE SKIN: Biopsy, Excision, Re-Excision (for reference only) 21
22 Grossing Procedure (select all that apply) (Note A) Biopsy, shave Biopsy, punch Biopsy, incisional Excision Re-excision Lymphadenectomy, sentinel node(s) Lymphadenectomy, regional nodes (specify): Other (specify): Not specified Specimen Laterality Right Left Midline Not specified Tumor Site (Note B) Specify (if known): Not specified Tumor Size (required only if tumor is grossly present) Greatest dimension: cm *Additional dimensions: x cm Indeterminate (see Comment ) Macroscopic Satellite Nodule(s) (required for excision specimens only) Not identified Present Indeterminate *Macroscopic Pigmentation * Not identified * Present, diffuse * Present, patchy/focal * Indeterminate Primary Tumor (pt) ptx: Primary tumor cannot be assessed (eg, shave biopsy or regressed melanoma) (see Comment ) pt0: No evidence of primary tumor ptis: Melanoma in situ (ie, not an invasive tumor: anatomic level I) pt1: Melanoma mm or less in thickness, with or without ulceration (see Note D) 1.0 pt1a: Melanoma 1.0 mm or less in thickness, no ulceration, <1 mitoses/mm 2 pt1b: Melanoma 1.0 mm or less in thickness with ulceration and/or 1 or more mitoses/mm 2 pt2: Melanoma to 2 mm in thickness, with or without t ulceration 1.01 pt2a: Melanoma 1.01 mm thickness, no ulceration to 2.0 in pt2b: Melanoma 1.01 to 2.0 mm in thickness, with ulceration pt3: Melanoma to 4.0 mm in thickness, with or without ulceration 2.01 pt3a: Melanoma 2.01 to 4.0 mm in thickness, no ulceration pt3b: Melanoma 2.01 to 4.0 mm in thickness, with ulceration pt4: Melanoma greater than 4.0 mm in thickness, with or without ulceration pt4a: Melanoma greater than 4.0 mm in thickness, no ulceration pt4b: Melanoma greater than 4.0 mm in thickness, with ulceration Microscopic Features Histologic Type Maximum Tumor Thickness Anatomic Level Ulceration Margins (select all that apply) Mitotic Index Microsatellitosis Lymph-Vascular Invasion Perineural Invasion Tumor-Infiltrating Lymphocytes Tumor Regression Growth Phase Pathologic Staging (ptnm) TNM Descriptors 22
23 Metastasis Distant Metastasis (pm) Not applicable pm1: Distant metastasis (documented in this specimen) * pm1a: Metastasis in skin, subcutaneous tissues, or distant lymph nodes * pm1b: Metastasis to lung * pm1c: Metastasis to all other visceral sites or distant metastasis at any site associated with an elevated serum lactic dehydrogenase d (LDH) *Specify site, if known: *Additional Pathologic Findings (select all that apply) * Nevus remnant * Other (specify): *Comment(s) Regional Lymph Nodes (pn) pnx: Regional lymph nodes cannot be assessed pn0: No regional lymph node metastasis pn1: Metastasis in 1 regional lymph node pn1a: Clinically occult (microscopic) metastasis pn1b: Clinically apparent (macroscopic) metastasis pn2: Metastasis in 2 to 3 regional nodes or intralymphatic regional metastasis without nodal metastasis pn2a: Clinically occult (microscopic) metastasis pn2b: Clinically apparent (macroscopic) metastasis pn2c: Satellite or in-transit metastasis without nodal metastasis pn3: Metastasis in 4 or more regional lymph nodes, or matted metastatic nodes, or in-transit metastasis or satellites(s) with metastasis in regional node(s) No nodes submitted or found Number of lymph nodes identified: Number containing metastases identified macroscopically: Number containing metastases identified microscopically: Matted nodes: Present Not identified Lymph Nodes Number of sentinel nodes examined: Total number of nodes examined (sentinel and nonsentinel): Number of lymph nodes with metastases: *Extranodal tumor extension: * Present Present * Not identified * Indeterminate *Size of largest metastatic focus: (mm) (for sentinel node) *Location of metastatic tumor (for sentinel node) * Subcapsular * Intramedullary * Subcapsular and intramedullary 23
24 Margins Peripheral Margins Cannot be assessed Uninvolved by invasive melanoma Distance of invasive melanoma from closest peripheral margin: mm (required for excisions only) Specify location(s), if possible: Involved by invasive melanoma Specify location(s), if possible: Uninvolved by melanoma in situ Distance of melanoma in situ from closest margin: mm (required for excisions only) Specify location(s), if possible: Involved by melanoma in situ Specify location(s), if possible: Deep Margin Cannot be assessed Uninvolved by invasive melanoma Distance of invasive melanoma from margin: mm (required for excisions only) Specify location(s), if possible: Involved by invasive melanoma Specify location(s), if possible: 24
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Springer Healthcare. Staging and Diagnosing Cutaneous Melanoma. Concise Reference. Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone
 Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
An Overview of Melanoma. Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center
 An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Skin Cancer. 5 Warning Signs. American Osteopathic College of Occupational and Preventive Medicine OMED 2012, San Diego, Monday, October 8, 2012 C-1
 Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Michael T. Tetzlaff MD, PhD
 Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Impact of Prognostic Factors
 Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma. Michael T. Tetzlaff MD, PhD
 Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Malignant tumors of melanocytes: Part 1. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Protocol for the Examination of Specimens From Patients With Melanoma of the Skin
 Protocol for the Examination of Specimens From Patients With Melanoma of the Skin Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Protocol for the Examination of Specimens From Patients With Melanoma of the Skin Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
SKIN CANCER. Most common cancer diagnosis 40% of all cancers
 SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
Melanoma Underwriting Presented at 2018 AHOU Conference. Hank George FALU
 Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
NAACCR Webinar Series 1
 Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 2. Variations on the acquired nevus 3. Dermal melanocytosis
 Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Metastatic Melanoma. Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds
 Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
5/21/2018. Disclosures. Consulting: Myriad Genetics SciBase. Superficial Atypical Melanocytic Proliferations. SSM, LMM and (some of) their Simulants
 their Simulants") Disclosures Consulting: Myriad Genetics SciBase Superficial Atypical Melanocytic Proliferations SSM, LMM and (some of) their Simulants 1 Melanomas and Nevi. Nevi are important mainly in relation to melanoma
Disclosures Consulting: Myriad Genetics SciBase Superficial Atypical Melanocytic Proliferations SSM, LMM and (some of) their Simulants 1 Melanomas and Nevi. Nevi are important mainly in relation to melanoma
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG
 Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Living Beyond Cancer Skin Cancer Detection and Prevention
 Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Histopathology of Melanoma
 THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
Cutaneous Malignancies: A Primer COPYRIGHT. Marissa Heller, M.D.
 Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY
 IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD
 Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Racial differences in six major subtypes of melanoma: descriptive epidemiology
 Wang et al. BMC Cancer (2016) 16:691 DOI 10.1186/s12885-016-2747-6 RESEARCH ARTICLE Racial differences in six major subtypes of melanoma: descriptive epidemiology Yu Wang 1, Yinjun Zhao 2 and Shuangge
Wang et al. BMC Cancer (2016) 16:691 DOI 10.1186/s12885-016-2747-6 RESEARCH ARTICLE Racial differences in six major subtypes of melanoma: descriptive epidemiology Yu Wang 1, Yinjun Zhao 2 and Shuangge
Melanoma and Dermoscopy. Disclosure Statement: ABCDE's of melanoma. Co-President, Usatine Media
 Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma 10/6/16. Please submit all questions concerning webinar content through the Q&A panel. Reminder:
 Collecting NAACCR Cancer Data: 2015-2016 Melanoma Webinar Series NAACCR 2016-2017 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
Collecting NAACCR Cancer Data: 2015-2016 Melanoma Webinar Series NAACCR 2016-2017 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ]](/thumbs/71/65936251.jpg "Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ]") MelanomaSkin CS Tumor Size Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ] Code 000 No mass/tumor found Description 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters
MelanomaSkin CS Tumor Size Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ] Code 000 No mass/tumor found Description 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Multiple Primary Melanoma in a Thai Male: A Case Report
 Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival
 MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Malignant Melanoma Early Stage. A guide for patients
 This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 12, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma.
 Melanoma UpToDate: Introduction: Risk Factors: 1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma. Median age = 50 yrs Incidence is rising - Sun exposure: UVB (290-320nm) > UVA
Melanoma UpToDate: Introduction: Risk Factors: 1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma. Median age = 50 yrs Incidence is rising - Sun exposure: UVB (290-320nm) > UVA
Learning Objectives. Tanning. The Skin. Classic Features. Sun Reactive Skin Type Classification. Skin Cancers: Preventing, Screening and Treating
 Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Protocol for the Examination of Specimens From Patients With Melanoma of the Skin
 Protocol for the Examination of Specimens From Patients With Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Based on AJCC/UICC TNM, 7th edition Protocol web posting date:
Protocol for the Examination of Specimens From Patients With Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Based on AJCC/UICC TNM, 7th edition Protocol web posting date:
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Uveal Melanoma. Protocol applies to malignant melanoma of the uvea.
 Uveal Melanoma Protocol applies to malignant melanoma of the uvea. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist) Biopsy (No Accompanying
Uveal Melanoma Protocol applies to malignant melanoma of the uvea. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist) Biopsy (No Accompanying
Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern
 Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern ELIZABETH A. MANCI, M.D., CHARLES M. BALCH, M.D..TARIQ M. MURAD, M.D., PH.D., AND SENG/JAW SOONG, PH.D. Manci, Elizabeth A., Balch, Charles
Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern ELIZABETH A. MANCI, M.D., CHARLES M. BALCH, M.D..TARIQ M. MURAD, M.D., PH.D., AND SENG/JAW SOONG, PH.D. Manci, Elizabeth A., Balch, Charles
Michael T. Tetzlaff MD, PhD
 American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
Contrast with Australian Guidelines A/Pr Pascale Guitera,
 Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Corporate Medical Policy
 Corporate Medical Policy Gene Expression Profiling for Cutaneous Melanoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: gene_expression_profiling_for_cutaneous_melanoma 5/2018
Corporate Medical Policy Gene Expression Profiling for Cutaneous Melanoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: gene_expression_profiling_for_cutaneous_melanoma 5/2018
Normal RAS-RAF (MAPK) pathway signaling
 pathway signaling") BRAF-Mutations in Melanomas L. Mazzucchelli Istituto Cantonale di Patologia, Locarno 77. Annual Meeting Swiss Society of Pathology, Lucerne 2011 Sponsored by Roche Pharma Switzerland Melanoma has increased
BRAF-Mutations in Melanomas L. Mazzucchelli Istituto Cantonale di Patologia, Locarno 77. Annual Meeting Swiss Society of Pathology, Lucerne 2011 Sponsored by Roche Pharma Switzerland Melanoma has increased
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018
 Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Conflict of Interest 9/2/2014. Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma
 Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
Finding Melanoma. Is not easy!
 Finding Melanoma Is not easy! Finding Melanoma Victoria mean depth at diagnosis is 1.5 mm. Melanoma 1.5mm Has Stage 1B Mortality 10% Melanoma Spotting a killer! Spotting a killer Visual Clues What are
Finding Melanoma Is not easy! Finding Melanoma Victoria mean depth at diagnosis is 1.5 mm. Melanoma 1.5mm Has Stage 1B Mortality 10% Melanoma Spotting a killer! Spotting a killer Visual Clues What are
Interesting Case Series. Desmoplastic Melanoma
 Interesting Case Series Desmoplastic Melanoma Anthony Maurice Kordahi, MD, Joshua B. Elston, MD, Ellen M. Robertson, MD, and C. Wayne Cruse, MD Division of Plastic Surgery, Department of Surgery, University
Interesting Case Series Desmoplastic Melanoma Anthony Maurice Kordahi, MD, Joshua B. Elston, MD, Ellen M. Robertson, MD, and C. Wayne Cruse, MD Division of Plastic Surgery, Department of Surgery, University
6/22/2015. Original Paradigm. Correlating Histology and Molecular Findings in Melanocytic Neoplasms
 6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
Management of pediatric melanocytic lesions
 Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
Protocol for the Examination of Specimens From Patients With Merkel Cell Carcinoma of the Skin
 Protocol for the Examination of Specimens From Patients With Merkel Cell Carcinoma of the Skin Protocol applies to Merkel cell carcinoma of cutaneous surfaces only. Based on AJCC/UICC TNM, 7th edition
Protocol for the Examination of Specimens From Patients With Merkel Cell Carcinoma of the Skin Protocol applies to Merkel cell carcinoma of cutaneous surfaces only. Based on AJCC/UICC TNM, 7th edition
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology
 Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Melanoma of the Skin INTRODUCTION SUMMARY OF CHANGES
 24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44.6 Skin of upper limb
24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44.6 Skin of upper limb
Glenn D. Goldman, MD. University of Vermont Medical Center. University of Vermont College of Medicine
 Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Epidemiology. Objectives 8/28/2017
 Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
47. Melanoma of the Skin
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 13, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter.
 Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Melanoma Quality Reporting
 Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
21/07/2017. The «gray zone» of diagnosis is visible. Nevus Atypical nevus Melanoma. Melanoma ex-blue nevus
 Update on the Clinico- Pathological and Molecular Diagnosis of Melanocytic Lesions None to declare Conflicts of interest Belfast pathology Arnaud de la Fouchardière MD, PhD Lyon, France What is new? Today
Update on the Clinico- Pathological and Molecular Diagnosis of Melanocytic Lesions None to declare Conflicts of interest Belfast pathology Arnaud de la Fouchardière MD, PhD Lyon, France What is new? Today
Melanoma of the Skin
 24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44. Skin of upper limb
24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44. Skin of upper limb
HISTOPATHOLOGIC REPORTING OF MELANOCYTIC SKIN LESIONS. Problems, thoughts, proposals
 HISTOPATHOLOGIC REPORTING OF MELANOCYTIC SKIN LESIONS Problems, thoughts, proposals Gerardo Ferrara Anatomic Pathology Unit Macerata General Hospital AV3 ASUR Marche Macerata, I Aims and scope STANDARDIZATION:
HISTOPATHOLOGIC REPORTING OF MELANOCYTIC SKIN LESIONS Problems, thoughts, proposals Gerardo Ferrara Anatomic Pathology Unit Macerata General Hospital AV3 ASUR Marche Macerata, I Aims and scope STANDARDIZATION:
Glenn D. Goldman, MD. Fletcher Allen Health Care. University of Vermont College of Medicine
 Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Guy Perrot (Ги Перро)
") НАУЧНО-ПРАКТИЧЕСКАЯ КОНФЕРЕНЦИЯ (МАСТЕР-КЛАСС) «ПРАКТИЧЕСКИЕ АСПЕКТЫ ДИАГНОСТИКИ И ЛЕЧЕНИЯ МЕЛАНОМЫ КОЖИ» DIAGNOSTIC AND PITFALLS IN MELANOMA Guy Perrot (Ги Перро) MD PHD pathologist, University Hospital
НАУЧНО-ПРАКТИЧЕСКАЯ КОНФЕРЕНЦИЯ (МАСТЕР-КЛАСС) «ПРАКТИЧЕСКИЕ АСПЕКТЫ ДИАГНОСТИКИ И ЛЕЧЕНИЯ МЕЛАНОМЫ КОЖИ» DIAGNOSTIC AND PITFALLS IN MELANOMA Guy Perrot (Ги Перро) MD PHD pathologist, University Hospital
MALIGNANT MELANOMA OF THE HEEL
 MALIGNANT MELANOMA OF THE HEEL Pages with reference to book, From 50 To 53 Fazli M. Qazi ( Departments of Pathology, Khyber Medical College, Peshawar. ) Rahjm Gul ( Departments of Surgery, Khyber Medical
MALIGNANT MELANOMA OF THE HEEL Pages with reference to book, From 50 To 53 Fazli M. Qazi ( Departments of Pathology, Khyber Medical College, Peshawar. ) Rahjm Gul ( Departments of Surgery, Khyber Medical
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
12. Malignant Melanoma of Skin
 KEY FACTS 12. Malignant Melanoma of Skin ICD-9 172 On average 160 melanomas of the skin were registered per year. Twice as common in females than in males. Higher than expected numbers in Southern Board
KEY FACTS 12. Malignant Melanoma of Skin ICD-9 172 On average 160 melanomas of the skin were registered per year. Twice as common in females than in males. Higher than expected numbers in Southern Board
Protocol for the Examination of Specimens From Patients With Merkel Cell Carcinoma of the Skin
 Protocol for the Examination of Specimens From Patients With Merkel Cell Carcinoma of the Skin Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Protocol for the Examination of Specimens From Patients With Merkel Cell Carcinoma of the Skin Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is:
 Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Simulators of melanoma
 Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
MELANOCYTIC LESIONS: EFFECTIVE MANAGEMENT IN PRIMARY CARE: Part 2
 MELANOCYTIC LESIONS: EFFECTIVE MANAGEMENT IN PRIMARY CARE: Part 2 In the second part of our feature on pigmented skin lesions, dermatology specialist Dr Sweta Rai describes the steps to rational decision-making
MELANOCYTIC LESIONS: EFFECTIVE MANAGEMENT IN PRIMARY CARE: Part 2 In the second part of our feature on pigmented skin lesions, dermatology specialist Dr Sweta Rai describes the steps to rational decision-making
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
When Do I Consider Myself Cured?
 The Melanoma Patient Symposium - Science to Survivorship When Do I Consider Myself Cured? 26 September 2009 Jeffrey E. Gershenwald, MD, FACS Professor of Surgery, Dept. of Surgical Oncology Professor,
The Melanoma Patient Symposium - Science to Survivorship When Do I Consider Myself Cured? 26 September 2009 Jeffrey E. Gershenwald, MD, FACS Professor of Surgery, Dept. of Surgical Oncology Professor,
STAGE CATEGORY DEFINITIONS
 CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
Comparison of Melanoma Subtypes among Korean Patients by Morphologic Features and Ultraviolet Exposure
 Comparison of Melanoma Subtypes in Korean Patients Ann Dermatol Vol. 26, No. 4, 2014 http://dx.doi.org/10.5021/ad.2014.26.4.485 ORIGINAL ARTICLE Comparison of Melanoma Subtypes among Korean Patients by
Comparison of Melanoma Subtypes in Korean Patients Ann Dermatol Vol. 26, No. 4, 2014 http://dx.doi.org/10.5021/ad.2014.26.4.485 ORIGINAL ARTICLE Comparison of Melanoma Subtypes among Korean Patients by